

Abstract
Background
Disruptions in global surgery educational routines by the COVID-19 pandemic have elicited demands for alternative formats for rendering qualitative neurosurgical education. This study presents application of a novel model of online neurosurgical course, the Lecture-Panel-Discussion Model (LPDM).
Methods
This is a cross-sectional survey of participants who attended the Swedish African Neurosurgery Collaboration (SANC)-100A course. Participants evaluated the course through an online self-administered questionnaire using a 5-point Likert scale ranging from very poor—1, poor—2, average (fair)—3, good—4, to excellent—5. SANC-100A comprises a tripod of Lectures, Panel review, and interactive case Discussion. This model (LPDM) was innovated by SANC and applied at the Enugu International Neurosurgery course in February 2021.
Results
There were 71 attendees, 19 were course faculty, while 52 were participants. Thirty-five attended from Nigeria, 11 from Sweden, 3 from Malawi, 2 from Senegal, and 1 from the UK. Among 44 participants who completed the questionnaire, there were 9 fellows and 35 residents. The overall median course Likert rating was 4.65 ± 0.1. The median overall rating for course events was similar between day 1 (Likert score = 4.45) and day 2 (Likert score = 4.55), U = 55, Z score = 1.10, P = 0.27. The median rating for lectures was 4.50 ± 0.2 and varied from 4.40 on day 1 to 4.55 on day 2. The median rating for panel review was 4.60 ± 0.1 and varied from 4.55 on day 1 to 4.65 on day 2. Interactive case discussions were rated 4.80 on both course days. There was a significant variability in the rating profiles of the course tripod: U = 24.5, P = 0.03. Fifty-one (98%) participants believe LPDM was COVID-19-compliant, while 90% believe the course was beneficial to training and practice.
Conclusion
Initial application of LPDM is rewarded with both high acceptance and high rating among participants.
Keywords: Andragogy, Global surgery; Lecture-Panel-Discussion Model, Neurosurgical education, Pedagogy
Background
The COVID-19 pandemic has caused unprecedented disruptions to established unit-based neurosurgical educational routines and practice [14, 17, 20]. It has perhaps dealt a more devastating harm to global neurosurgical educational and clinical partnerships leading to a near complete cessation of global collaborative surgical offerings. The effects of these disruptions are both seismic and disproportionately experienced by underserved locations within developing countries already encumbered by fragile health systems and critical infrastructure shortages [5, 21]. The impact of the COVID-19 pandemic has also led to significant transformation in the mode of delivery of neurosurgical education and training as the global neurosurgery retools for survival [8, 11, 24]. Prominent among the innovative measures are online modules and simulation laboratories [15, 24]. Prior to the eruption of the COVID-19 pandemic, two collaborative global surgery missions were scheduled by SANC in collaboration with the neurosurgery unit of the University of Nigeria Teaching Hospital Enugu to be held in March and November 2020. However, these 2 missions were postponed indefinitely as a result of the pandemic. In their place, weekly collaborative virtual meetings were established between SANC and the neurosurgery unit in Enugu, Nigeria, to offset the effects of mission postponement by delivering salient educational offerings. In addition, an International Neurosurgery course based on the tripod of lectures, panel and case discussions were held to maximize the opportunity of the online meetings and extend the recipient field of the global surgery educational project using emerging video conferencing capabilities. Our index study presents this new model of global collaborative neurosurgical education innovated to mitigate an observed gap in our twinning neurosurgical educational partnership.
Methods
This is a cross-sectional survey of participants who attended the first Enugu International Neurosurgery course (SANC-100A) organized by SANC in collaboration with the neurosurgery unit of the University of Nigeria Teaching Hospital and the Nigerian Academy of Neurological Surgeons. Following ethical approval, the survey was administered to participants using an online semi validated questionnaire modified from a similar questionnaire applied for the evaluation of the blended integrated course in clinical surgery of the West African College of Surgeons (WACS) in 2020. SANC-100A is an online collaborative neurosurgical course that comprises a tripod of online Lectures, a Panel providing an in depth practical review of lectures, and finally interactive case based Discussions led by a separate team of experts. This novel paradigm provided a comprehensive didactic exchange through a triphasic module that focuses all three phases of learning on a specific neurosurgical theme to achieve a synchronized experiential outcome.
This model (LPDM) was innovated by SANC and applied for the first time at the Enugu International Neurosurgery course on the 12th and 13th of February 2021. The course theme was Adaptation of Modern Neurosurgical Techniques and Applications to sub-Saharan Settings. Each course day lasted 8 h and comprised 5 lectures each lasting 45 min for lecture delivery and 15 min for question and answer (Q/A). The lectures were succeeded by 1 h of three expert panel review and 1 h of case review by different experts interacting with participants. Case reviews provided a robust practical illustration of lecture nuggets with relevant clinical cases, images, and operative videos in an interactive web-based learning environment. Each course day was concluded by an expert summary of salient key points over an hour period. Course components were rated by participants through an online questionnaire using a 5-point Likert scale ranging from very poor—1, poor—2, average (fair)—3, good—4, to excellent—5. Course data and evaluations were acquired and analyzed using Statistical Package for Social Sciences (SPSS) version 23, Chicago, IL, USA. Mann Whitney U test was used to evaluate the median Likert ratings and test for significant association or variability between median Likert ratings of course events. Associations were adjudged significant if P value < 0.05.
Results
Course population
Seventy-one persons attended the course. Fifty-two of those were participants, while 19 were course faculty (Fig. 1). Nigeria with 35 participants and Sweden with 11 accounted for majority of attendees. Other countries represented include Malawi 3, Senegal 2, and the UK 1 participant, respectively (Fig. 1). Neurosurgical residents (n = 41) accounted for majority of participants, whereas 9 fellows and 2 nurses were in attendance as well. There were 3 females among participants and 49 males with F to M = 1:16.3. The mean age of participants was 35.9 ± 2.7 with a range of 31 to 55 years. For each course day, ten (10) highly experienced neurosurgical experts functioned as faculty. One (1) course faculty functioned on both days. Sweden with 6 expert neurosurgeons, Nigeria with 13, and the UK with 1 faculty were practice locations of course faculty. Two women were course faculty resulting in a F to M ratio of 1:8.5. Forty-four (84.6%) participants completed the questionnaire; 35 residents and 9 fellows were among those who completed the questionnaire.
Fig. 1.

Participant status and country profile, n = 71
Course content rating
The median Likert rating ranged from 4.45 ± 0.2 on course day 1 to 4.55 ± 0.2 on course day 2. There was no difference between the median ratings of the different course days using Mann–Whitney U test, U = 55, Z score = 1.10, P = 0.27 (Table 1). The median lecture rating was 4.45 on day 1 and 4.65 on day 2. For panel review, the median Likert rating varied from 4.55 on day 1 to 4.65 on day 2. The Likert rating for interactive case review was 4.80 on both day 1 and day 2. On course day 1, lecture ratings ranged from 4.20 to 4.70 with a median of 4.45, whereas on day 2, it ranged from 4.40 to 4.90 with a median of 4.65. The panel rating varied from 4.30 to 4.80 on day 1 with a median of 4.55, whereas on day 2, it ranged from 4.50 to 4.80 with a median of 4.65. The Likert ratings of the different course modules on course day 1 and course day 2 are profiled in Table 2 and Table 3, respectively. Figure 2 is a bar chart showing the graphical profile of the Likert ratings of the three course components as well as the overall rating, while Fig. 3 is a line graph depicting the comparative Likert ratings of the course modules on both course days. A Mann–Whitney U test performed to evaluate the median ratings of the course modules showed a significant variability in the rating profiles of the three course modules with interactive case review achieving the highest overall rating on both course days, U = 24.5, Z = 1.86, P = 0.03. Fifty-one (98%) participants rated the course as COVID-19-compliant, 47 (90.4%) believe the course delivered high-quality competency-based neurosurgical training as well as knowledge relevant both to training and practice, whereas 46 (88.5%) will recommend the course to colleagues as well as attend a future course.
Table 1.
Course day Likert summary
| Course day | Median Likert rating |
|---|---|
| Day 1 | 4.45 ± 0.1 |
| Day 2 | 4.55 ± 0.2 |
| Overall | 4.65 ± 0.1 |
| U = 55, Z score = 1.10, P = 0.27 |
Table 2.
Course day 1 performance profile
| Course day 1 | Median Likert rating |
|---|---|
| A. Lectures | |
| Microneurosurgery tips and tricks | 4.70 |
| Intraventricular endoscopy | 4.20 |
| Skull base endoscopy | 4.50 |
| Intraoperative ultrasound as a neurosurgical tool | 4.50 |
| Potentials and limitations of neuronavigation | 4.60 |
| Median lecture rating | 4.45 |
| B. Panel review | |
| Morning session | 4.80 |
| Afternoon session | 4.30 |
| Median panel rating | 4.55 |
| C. Interactive case discussion | 4.8 |
Data in italics were used to identify the median score of the lecture, panel and case discussion ratings
Table 3.
Course day 2 ratings
| Course day 2 | Median Likert rating |
|---|---|
| A. Lectures | |
| Bone modeling and fusion | 4.65 |
| Spinal fixation techniques 1 (basic principles) | 4.65 |
| Spinal fixation techniques (ACDF and lumbar spinal fusion) | 4.55 |
| Challenges of technical maintenance of neurosurgical equipment in sub-Saharan Africa | 4.0 |
| Global neurosurgery in sub-Saharan Africa; navigating the challenges to harness salient benefits | 4.90 |
| Median lecture rating | 4.65 |
| B. Panel review | |
| Morning session | 4.80 |
| Afternoon session | 4.50 |
| Median panel rating | 4.65 |
| C. Interactive case discussion | 4.80 |
Data in italics were used to identify the median score of the lecture, panel and case discussion ratings
Fig. 2.
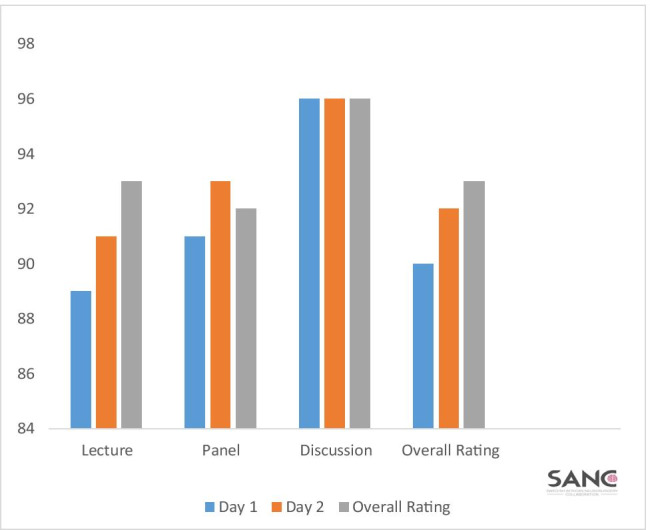
Course day ratings (median scores of daily course events (%))
Fig. 3.
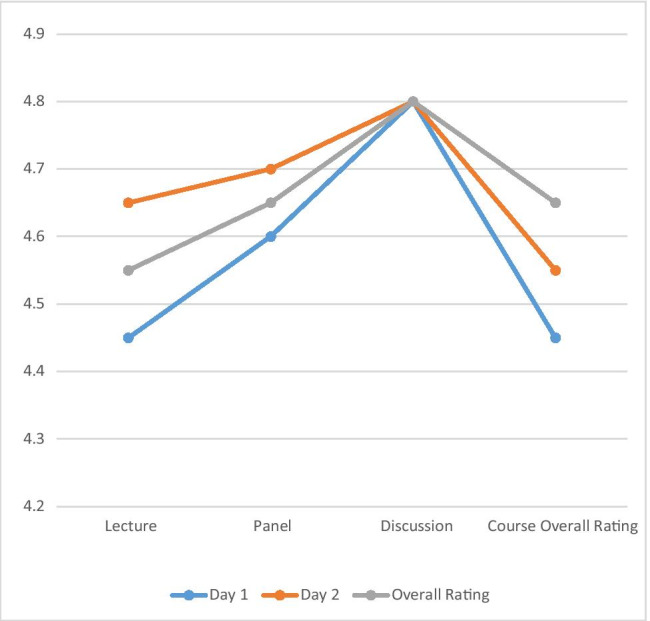
Line graph showing course module median Likert ratings (max = 5) U = 24.5, Z = 1.86, P = 0.03
Discussion
In this survey, a new online model of didactic and competency-based neurosurgical education—LPDM—was evaluated by a cross section of participants who attended the course from 5 different countries located within 2 continents. The ability of participants to attend from these locations obviated the need for travel at the time of global lockdown presenting the participants and faculty with a salient benefit (Table 1).
The LPDM course format and its components were highly rated, suggesting participants satisfaction with this model (Tables 1, 2, and 3). Although the tripod—lectures, panels, and case discussions—has often been used informally, to our knowledge, our study represents the first application of this andragogical sequence of content delivery under evaluable conditions. In our application of the LPDM model, a focused predetermined neurosurgical content was sequentially delivered and escalated in scope through the use of a tripod of modules—lecture, panel review, and interactive case discussion presented via a synchronized online learning interface [18]. This innovation is in part the reward of a compelling search by the course directors for a reliable tool for delivering interactive collaborative neurosurgical education to local neurosurgeons in a twinning training location during the global COVID-19 lockdown. The scope of participants was however widened to include participants from other locations other than the initially intended recipients. Online and virtual courses allow interactive exchange between participants and course faculty during courses with minimal risk of contracting or spreading contagious infections such as COVID-19 [18]. Furthermore, web-based courses have proven to be as effective as face-to-face learning [1, 22]. Prior to the COVID-19 era, web-based education had started gaining ascendancy over traditional in-site pulpit modules [1, 22]. The advent of COVID-19 pandemic however compelled an abrupt transition from face-to-face formats to online course modules [2, 7, 10, 18, 19]. Digital-based platforms of neurosurgical education have been proposed as a potentially salient bridge capable of addressing the wide knowledge gap between the developed and underdeveloped countries [19] (Table 4).
Table 4.
Participants’ views
| Course goal | Participant rating (%) |
|---|---|
| Adherence to COVID 19 guidelines | 98% compliance |
| Delivery of competency-based learning | 90.4% |
| Delivery of neurosurgical knowledge relevant to practice | 90.4% |
| Recommendability of course to colleagues | 88.5% |
| Likelihood of attending a future course by SANC | 88.5 |
The precession from lecture to panel review and finally interactive case-based discussion was carefully planned to create a dynamic learning path with incremental enhancement of participants’ grasp of the subject as they migrate from passive learning during lectures to a phase of interactive exchange involving active participation during case reviews and discussions (Figs. 2 and 3).
This model in some ways resemble the andragogical foundations of the Matrix and Milestone curriculum of neurosurgical education popularized by the US Accreditation Council for Graduate Medical Education review committee for Neurological Surgery. Its similarity to Matrix and Milestone draws from the provision of an escalable pathway for training and content delivery using a modifiable web-based platform [19]. However, LPDM differs from Matrix and Milestone by combining three sequential modules in a synchronous digital interface [19]. It is our considered opinion that the progression of participant’s index of satisfaction across the tripod modules from lecture to case discussion may signify a synergy of benefits rather than isolated demonstration of the relative strengths of individual course components (Fig. 3). There is an increasing trend in recent times towards applying pedagogical and andragogical tools to neuroscience educational content [3, 4, 6, 9, 12, 13]. As virtual and online educational offerings evolve to become choice platforms for delivery of COVID-19 compliant education, their efficacy can be further cultivated by applying pedagogic and andragogic tools to the course curriculum as in the index course. Although, we have not compared LPD with traditional paradigms. Our result suggests that application of LPD may hold promise for a broader and potentially more rewarding course experience relative to lecture-only formats. Our optimism is supported by current opinion in neuropedagogy and andragogy that highlight the inadequacy of oral and pulpit modules alone in today’s learning methods. The significance of interactive, image-based teaching and digital delivery of learning modules are currently thought to offer superior results in contemporary teaching and learning. There are suggestions that digital tools in the information age are capable of reconfiguring human brains through neuronal plasticity to dynamically adapt to the evolving learning milieu [3, 9]. To this end, we believe LPD offers a “brain-friendly learning” strategy with strong andragogical foundations represented by the significant role of prior experience, self-directed learning, problem solving, and internal motivation. For example, the previous experience offered by a preceding lecture is believed to provide the motivation for the participant to actively perform tasks during the interactive case discussion. To prevent the Dunning-Kruger effect of overestimating what participants learnt from the course, daily feedback was incorporated into the curriculum of the course and we believe this contributed to improving the overall quality of experiential learning achieved by the course participants [3, 4, 9]. We would welcome other researchers to evaluate LPD so as to determine its external validity and applicability in other environments. More courses have been planned in the future by SANC to further evaluate LPD as well.
Finally, SANC-100A offered participating fellows and residents in sub-Saharan Africa an opportunity to socialize and network with their counterparts from Europe. A large proportion of participants benefitted from the course and are willing to attend a future course as well as recommend it to their colleagues. We believe the linkages established between participants and course faculty are healthy seeds sown on the fertile grounds of global neurosurgery. It is our considered opinion and expectation that they will yield a harvest of immense dividends in the future providing further proof of the potentially overarching long-term reward of LPD. The SANC course and the Young African Neurosurgeon Forum (YANF) educational programs are among currently active global neurosurgical educational initiatives within sub-Saharan Africa [23]. Dating back to February 2021, YANF has organized on a monthly basis continuing medical educational webinars on neurosurgical conditions that commonly define the sub-Saharan practice setting [16, 23]. The multidimensional profiles of the SANC and YANF educational offerings are commendable and should represent the beginning steps of more robust collaborations aimed at comprehensively improving the status of neurosurgery care and training in the subregion.
Footnotes
This article is part of the Topical Collection on Neurosurgery Training
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Abdous MH, Yoshimura M. Learner outcomes and satisfaction: a comparison of live video-streamed instruction, satellite broadcast instruction, and face-to-face instruction. Comput Educ. 2010;55(2):733–741. doi: 10.1016/j.compedu.2010.03.006. [DOI] [Google Scholar]
- 2.Affouneh S, Salha SN, Khlaif Z. Designing quality e-learning environments for emergency remote teaching in coronavirus crisis. Interdiscip J Virtual Learn Med Sci. 2020;11(2):1–3. [Google Scholar]
- 3.Alkhatib H (2009) How has pedagogy changed in the digital age. Eur J Open Dist E-Learning; n2.
- 4.Applying Educational Theory to Neurosurgery Residency Training. AANS Neurosurgeon August 2, 2020. https://aansneurosurgeon.org/feature/applying
- 5.Bong CL, Brasher C, Chikumba E, McDougall R, Mellin-Olsen J, Enright A. The COVID-19 pandemic: effects on low- and middle-income countries. Anesth Analg. 2020;131(1):86–92. doi: 10.1213/ANE.0000000000004846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Boon H. Neuroscience for old pedagogy. Conference: In: Proceedings of Australian Association for Research in Education Conference. From: AARE 2013: Australian Association for Research in Education Conference, 1–5 December 2013, Adelaide, SA, Australia At: Adelaide. 10.13140/2.1.5030.5923
- 7.Carey K (2020) Is everybody ready for the big migration to online college? Actually, no. The New York Times. https://www.nytimes.com
- 8.Cenzato M, DiMeco F, Fontanella M, Locatelli D, Servadei F. Editorial. Neurosurgery in the storm of COVID-19: suggestions from the Lombardy region, Italy (ex malobonum) [e-pub ahead of print]. J Neurosurg. 10.3171/2020.3.JNS20960 [DOI] [PMC free article] [PubMed]
- 9.Chojak M (2018) Neuropedagogy as a scientific discipline: interdisciplinary description of the theoretical basis for the development of a research field. World Acad Sci Eng Technol Int J Educ Pedagog Sci 12(8)
- 10.Dhawan S. Online learning: a panacea in the time of COVID-19 crisis. J Educ Technol Syst. 2020;49(1):5–22. doi: 10.1177/0047239520934018. [DOI] [Google Scholar]
- 11.Deora H, Mishra S, Tripathi M, Gard K, Tandon V, Borkar S, Varshney N, Raut R, et al. Adapting neurosurgery practice during the COVID-19 pandemic in the Indian subcontinent. World Neurosurg. 2020;142:e396–406. doi: 10.1016/j.wneu.2020.07.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Furlong J. Educationalists must do better. Times Higher Education 2013. May 2 http://www.timeshighereducation.co.uk/features/educationalists-must-do-better/2003518.fullarticle
- 13.Geake J, Cooper P (2003) Cognitive neuroscience: implications for education? Westminster Stud Educ 26(1):7–20 (2). Available from: https://www.researchgate.net/publication/264707874_NEUROSCIENCE_FOR_OLD_PEDAGOGY [accessed Sep 03 2021]
- 14.Guadix SW, Winston GM, Chae JK, Haghdel A, Chen J, Younus I, et al. Medical student concerns relating to neurosurgery education during COVID-19 [published online ahead of print, 2020 May 16] World Neurosurg. 2020;139:e836–47. doi: 10.1016/j.wneu.2020.05.090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Haji F. Simulation in neurosurgical education during the COVID 19 pandemic and beyond. Can J Neu Sci. 2021;48(2):152–154. doi: 10.1017/cjn.2020.234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kanmounye US, Robertson FC, Thango NS, Doe AN, Bankole NDA, Ginette PA, et al. Needs of young African neurosurgeons and residents: a cross-sectional study. Front Surg. 2021;8:150. doi: 10.3389/fsurg.2021.647279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Khalafallah AM, Jimenez AE, Lee RP, Weingart JD, Theodore N, Cohen AR, et al. Impact of COVID-19 on an academic neurosurgery department: the Johns Hopkins experience [published online ahead of print, 2020 May 24] World Neurosurg. 2020;139:e877–84. doi: 10.1016/j.wneu.2020.05.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khalil R, Mansour AE, Fadda WA, et al. The sudden transition to synchronized online learning during the COVID-19 pandemic in Saudi Arabia: a qualitative study exploring medical students’ perspectives. BMC Med Educ. 2020;20:285. doi: 10.1186/s12909-020-02208-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kim J, Burchiel MD. Neurosurgical education: a new paradigm for curriculum, core, and subspecialty training. Neurosurgery. 2016;63(1):88–90. doi: 10.1227/NEU.0000000000001304. [DOI] [PubMed] [Google Scholar]
- 20.Panayiotis E, Pelargos PE, Chakraborty A, Zhao YD, Smith ZA, Dunn IF, Bauer AM. An evaluation of neurosurgical resident education and sentiment during coronavirus disease 2019 pandemic: a North American survey. World Neurosurg. 2020;140:e381–e386. doi: 10.1016/j.wneu.2020.05.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Park KB, Kanmounye US, Lartigue JW (2020) Global neurosurgery in the time of COVID-19. Neurospine 17(2):348–350. 10.14245/ns.2040246.123 [DOI] [PMC free article] [PubMed]
- 22.Soffer T, Nachmias R. Effectiveness of learning in online academic courses compared with face-to-face courses in higher education. J Comp Ass Learn. 2018;34(5):534–543. doi: 10.1111/jcal.12258. [DOI] [Google Scholar]
- 23.Thango N, Laeke T, Jokonya L, Konan L, Sekabunga J, Jabang J, Nicolosi F, et al. Young African Neurosurgeons’ Forum: a symbiotic approach to global education and research. 2021 (https://wfns.org/WFNSData/Uploads/files/7_CAANS_YNS_Report.pdf?a=123
- 24.Wittayanakorn N, Nga VDW, Sobana M, Bahuri NFA, Baticulon RE. Impact of COVID-19 on neurosurgical training in Southeast Asia. World Neurosurg. 2020;144:e164–e177. doi: 10.1016/j.wneu.2020.08.073. [DOI] [PMC free article] [PubMed] [Google Scholar]