

Abstract
Introduction
Parents with childhood maltreatment histories are at risk for emotion regulation (ER) problems, which are associated with reduced self-regulation among their offspring. However, gaps remain in the literature regarding this indirect transmission pathway. First, ER consists of multiple dimensions and it is unclear which dimension is most affected by childhood maltreatment. Second, less is known regarding which parental ER dimension is linked to offspring self-regulation. Thus, the present study aimed to examine the direct and indirect associations between parental maltreatment histories and child self-regulatory capacity via dimensions of parental ER.
Methods
In this cross-sectional study, 101 youth (75% African American/Black; 53% female; Mage = 10.28; SD = 1.19) and their primary caregivers were recruited from a low-income community in the Southeastern United States. Structural equation modeling was used to model the effect of parents’ self-reported childhood maltreatment on youth physiological self-regulation (measured by heart rate variability reactivity [HRV-R]), via parents’ self-reported ER.
Results
Parental maltreatment history was significantly associated with five of the six components of ER. Further, the indirect effect of parents’ childhood maltreatment on child HRV-R was significant when parents reported more difficulty engaging goal-directed behaviors. Moderation analyses by sex showed that daughters had greater dysregulation regardless of parental maltreatment histories, while parents’ ER was found to play a more significant role in the intergenerational transmission of dysregulation to sons.
Conclusions
The current study extends the literature on self-regulation development in children of low-income, maltreatment-exposed parents. Our study may inform parent-child interventions for improving self-regulation.
Keywords: emotion regulation, heart rate variability, intergenerational effects of maltreatment, childhood maltreatment history, sex differences, moderated mediation
Introduction
Childhood maltreatment is linked to an increased risk for emotion dysregulation among parents, and these problems with emotion regulation are documented to spill over from parents to their offspring. Parents’ childhood maltreatment and trauma experiences impact their children’s psychosocial outcomes, including self-regulation problems (Collishaw et al., 2007; DiLillo & Damashek, 2003; Miranda et al., 2013), indicating an intergenerational pathway from child maltreatment to future offsprings’ self-regulation. Despite this body of research, mechanisms through which parental maltreatment histories relate to child self-regulation are less clear. Research suggests that parental emotion regulation (ER) is important in the socialization of child self-regulation skills (Morris et al., 2007). However, ER is multifaceted, and different dimensions of parents’ ER have yet to be examined in relation to the development of children’s self-regulation. Furthermore, research indicates there are sex differences in the development of self-regulation capabilities, including the physiological control of emotional experiences (Chaplin et al., 2005; Fiol-Veny et al., 2018; Koenig et al., 2017). Evidence suggests pre-adolescent females demonstrate more neurobiological vulnerability than their male counterparts (Fiol-Veny et al., 2018; Koenig et al., 2017). Thus, the present investigation aims to examine the interplay of parental maltreatment histories, ER, and child sex in the transmission of trauma effects to offspring’s self-regulation.
Childhood Maltreatment and Parents’ Emotion Regulation
Experiences of childhood maltreatment and trauma are associated with ER difficulties across the lifespan (Anda et al., 2006; DiLillo et al., 2000; Felitti et al., 1998). Effective ER is defined as the ability to accurately identify, understand, and modulate emotional experiences in response to socio-environmental input (Kaufman et al., 2016). In parenting roles, effective ER is necessary for parents to respond to stressful situations and to effectively regulate their own emotions across multiple interactions with their offspring. However, maltreated adults in parenting roles are at risk for having problems with ER. For example, research indicates that parents with maltreatment histories are quicker to anger and are less emotionally engaged with their children (DiLillo et al., 2000; Ehrensaft et al., 2015; Kim et al., 2009; Lorber & O’leary, 2005). In one study, adult daughters of incest survivors reported their mothers were emotionally immature and angry (Burkett, 1991). Although childhood maltreatment and trauma have effects on ER that persists into adulthood, it is unclear what facets of ER incur particular risk during parenthood.
The process of ER in adulthood is multifaceted and complex (Gross, 2015a, 2015b). Recent advances in ER measurement among adults suggest that it involves six dimensions (Kaufman et al., 2016), including emotional awareness, acceptance, and clarity, the ability to inhibit prepotent responses, engage regulation strategies, and activate goal-directed behavior (Cole et al., 2019; Soenke et al., 2010). Contextualized within the Extended Process Model of Emotion Regulation, Gross (2015a) suggests that issues with emotional awareness and clarity during the identification stage of ER (i.e., deciding whether to regulate) can lead to ER failure. Similarly, individuals who have fewer ER strategies at their disposal may over rely on harmful ER strategies (i.e., emotion misregulation) and fail to engage goal-directed behavior. Finally, difficulties with inhibiting impulsive responses in favor of particular ER tactics can result in failure to implement ER. Research suggests that childhood maltreatment experiences are linked to issues in adulthood with these dimensions of ER. For example, childhood maltreatment history was linked to issues with impulse control and goal pursuit, which were in turn related to risk behavior in a college-aged sample (Oshri et al., 2015). In another sample of college women, childhood emotional abuse was uniquely associated with worse emotional clarity, acceptance, goal-oriented behavior, and impulse control, with partial indirect ties to post-traumatic stress through all four dimensions (Burns et al., 2010). Thus, childhood maltreatment experiences appear to affect dimensions of ER important to its effective implementation in adulthood. Understanding the dimensions of ER most affected by childhood maltreatment will aid in clarifying which dimensions are then implicated in the transmission of trauma effects to offspring’s self-regulation.
Child Emotional Self-Regulation and HRV-R
In the present study, we measure children’s self-regulation using a physiological measure, heart rate variability reactivity (HRV-R), which operationalizes the stress response in the autonomic nervous system. The autonomic nervous system (ANS), which is functionally divided into the sympathetic and parasympathetic nervous systems, directs cardiac output in response to stress. The sympathetic nervous system (SNS) is purported to prepare the body to deal with threat by pausing digestion and accelerating heart rate, among other actions (Thayer & Lane, 2000). The parasympathetic nervous system (PNS) counterbalances the SNS and works to return the body to a homeostatic state. The PNS is implicated in the motivation of social behavior and becomes activated in response to social stress, resulting in emotional arousal and regulation (Porges, 1995, 2007). Recent reports suggest biomarkers of ANS functioning can serve as a reliable indirect index of self-regulation (Appelhans & Luecken, 2006; Bridgett et al., 2015). Heart rate variability reactivity (HRV-R), for example, is documented to function as an indirect neurobiological index of emotional self-regulation among youth and adults (Beauchaine, 2015; Holzman & Bridgett, 2017). Engaging and disengaging the PNS in response to social environmental threats is reflected through changes in HRV (Appelhans & Luecken, 2006).
According to the polyvagal theory (Porges, 1995, 2007) and the neurovisceral integration model (Thayer & Lane, 2000) the physiological basis of ER involves a coordinated process between the PNS and SNS. The neurovisceral model suggests a broader system of self-regulation, originating from structures in the brain (such as the amygdala and the anterior cingulate cortex) that control cognitive and emotional processes (Thayer & Lane, 2009). These structures direct cardiovascular output through neuroanatomical connections between the brain and the ANS, therefore influencing arousal and regulation (Thayer & Lane, 2009). Polyvagal theory, on the other hand, approaches social threat response from an evolutionary perspective, suggesting that the vagus nerve (the 10th cranial nerve sitting atop the mammalian spine) controls peripheral structures (e.g., facial muscles) involved with emotional expression and regulation through a network of other cranial nerves (Porges, 1995, 2007). Together these theories converge to suggest that HRV-R can serve as a reliable proxy reflecting emotional self-regulation.
Parent Socialization of Child Emotional Self-Regulation
Among the primary responsibilities of parents is to teach children how to handle stressful normative experiences by regulating their emotions. However, parents with ER difficulties may face challenges when fulfilling this task (Bridgett et al., 2015). Morris and colleagues (2007) articulate three key aspects of the family which influence child ER development: parental modeling of ER skills, emotion-related parenting practices and behaviors, and the family emotional climate (Morris et al., 2017; Morris et al., 2007). Based on this tripartite model, there are many paths through which parental ER difficulties may influence children’s self-regulation. For example, parents who show problems accepting their own emotions and engaging ER strategies may be more likely to invalidate their child’s emotions and become overstimulated when their child is upset (Buckholdt et al., 2014; Lorber, 2012; Lorber & O’leary, 2005). Such ER problems can escalate to ineffective parenting strategies such as harsh and negative discipline, aggression and withdrawal in response to child emotion (Buckholdt et al., 2014; Kim et al., 2009). Parents with a history of child maltreatment who experience greater difficulties with ER may model ineffectual regulation strategies to the child. The child may in turn exhibit ER problems, though it should be noted that a history of maltreatment does not predetermine parents’ ER difficulties and subsequent intergenerational impacts.
Research linking parenting and child HRV indicates the emotional quality of the caregiving environment plays a role in transmitting the effects of parents’ maltreatment histories to the physiological ER of their children (Blair & Raver, 2012; El-Sheikh & Erath, 2011). For example, parents with histories of maltreatment have been found to show decreased emotional availability and sensitivity to their children (DiLillo & Damashek, 2003; Fuchs et al., 2016; Moehler et al., 2007). Reduced emotional availability and sensitivity to children is successively linked to children’s suboptimal physiological ER (Perry et al., 2014; Skowron et al., 2011). While higher baseline HRV affords a child more physiological flexibility when faced with stressful situations (Bridgett et al., 2015) and can be protective against later behavioral issues (Hinnant et al., 2015), problems with physiological ER increases risks of later psychopathology (Cole et al., 2019; Oshri et al., 2020; Sheppes et al., 2015). In addition to parenting behaviors, parental modeling of emotion dysregulation is also linked to child emotion dysregulation as early as preschool, in both maltreated and non-maltreated samples (Eisenberg & Fabes, 1994; Melnick & Hinshaw, 2000; Robinson et al., 2009), and to physiological regulation in children as young as 2 months old (Bornstein & Suess, 2000). Conversely, children who have inherited autonomic impulsivity from parents are protected against developing more severe issues in adolescence if their primary caregivers socialize strong ER skills in the home (Beauchaine et al., 2007; Beauchaine et al., 2001). Therefore, if parents are unable to socialize and model effective ER in the home, children may be at increased risk of developing maladaptive physiological self-regulation.
Sex differences in ER and associated outcomes across the transition to adolescence are frequently reported (see Zahn-Waxler et al., 2008). A recent review found pre-adolescent and early adolescent girls demonstrated greater parasympathetic vulnerability (i.e., lower vagal activity) than boys (Koenig et al., 2017). However, the research becomes mixed when youth’s physiological self-regulation is contextualized within the family’s emotional environment. For example, greater RSA reactivity was found to be protective against the effects of marital conflict on later externalizing problems for boys in a pre-adolescent sample (El- Sheikh et al., 2001), while this same marker of regulation protected girls from internalizing problems in a longitudinal assessment (El-Sheikh & Whitson, 2006). Children of parents with compromised ER skills may similarly be exposed to a familial emotional environment that is unsupportive of their ER development.
The Current Study
In sum, there is abundant theoretical and empirical support for the transmission of parents’ childhood maltreatment histories to youth self-regulation through parental ER. Neither the unique contributions of each ER dimension, nor the role of children’s sex, in this transmission pathway have been empirically tested to date. However, a stronger understanding of this intergenerational pathway will have important implications for researchers and practitioners concerned with the intergenerational effects of childhood maltreatment.
The first aim of the present study was to examine the direct and indirect associations between parental history of childhood maltreatment (i.e., in their own childhood) and children’s emotional self-regulation (measured physiologically by HRV-R), through six facets of parental ER. We hypothesized that greater difficulties for parents in each domain of ER would act as an indirect mechanism linking parents’ experiences of maltreatment with their children’s physiological dysregulation. Due to a lack of consensus on the unique roles of ER dimensions in the intergenerational transmission of trauma effects, this stage in the design was strictly exploratory. Thus, no specific mediational hypotheses were made as they relate to each dimension of ER. The second aim was to examine child sex as a moderator in the transmission of parent’s ER to child’s physiological dysregulation. In light of the evidence for early sex differences in physiological ER (Chaplin et al., 2005; Fiol-Veny et al., 2018; Koenig et al., 2017), we hypothesized that pre-adolescent daughters would be more physiologically dysregulated than their male counterparts and would be more affected by parental ER in the home. For a conceptual model of study hypotheses, see Figure 1.
Fig. 1.
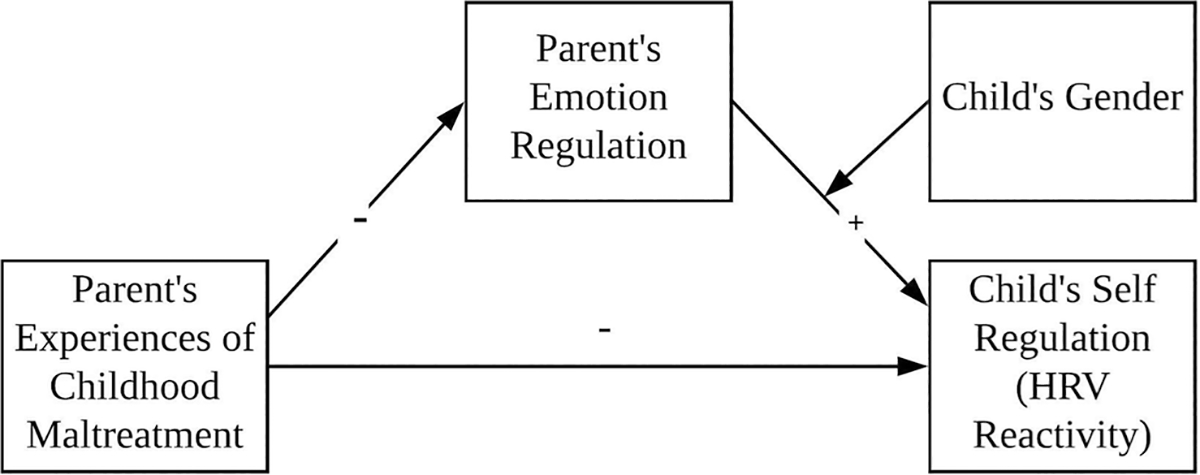
Conceptual model of study hypotheses
Methods
Sample
A community sample of 101 youth (52.5% female) aged 9 to 12 (M = 10.28, SD = 1.19) and their primary caregivers (N = 101; 95.0% female) was obtained from a non-metropolitan region of the Southeastern United States. See Table 1 for demographic information. Families were eligible if they had a household income below 200% of the federal poverty level (i.e., less than $48,600 annually for a family of four) and were English proficient. Due to collection of HRV data as part of the full study, ineligibility criteria included the presence of a heart condition or pregnancy for either the youth or caregiver. The sample was racially and ethnically diverse, with the majority of participants identifying as African American or Black (75.2%), followed by non-Hispanic White (10.9%), Latinx (8.9%), Native-American (1.0%), and Other (4.0%). Parents self-reported on their current involvement with Child Protective Services. Approximately 8.8% (n = 8) and 16.5% (n = 16) of families had an ope n or closed case, respectively, with child services. The majority of primary caregivers identified as the child’s biological mother (n = 91). Other relationships to the child included father (n = 4), grandmother (n = 1), aunt or uncle (n = 1), and other (n = 2).
Table 1.
Demographic characteristics of study sample (N = 101)
| N | % | |
|---|---|---|
|
| ||
| Child’s race/ethnicity | ||
| African American | 76 | 75.2 |
| White | 11 | 10.9 |
| Native American | 1 | 1.0 |
| Other | 4 | 4.0 |
| Child’s sex | ||
| Female | 53 | 52.5 |
| Male | 48 | 47.5 |
| Primary caregiver’s race/ethnicity | ||
| African American | 79 | 78.2 |
| Caucasian/ White | 14 | 13.9 |
| Hispanic/Latinx | 7 | 6.9 |
| Other | 1 | 1.0 |
| Primary caregiver’s sex | ||
| Female | 96 | 95.0 |
| Male | 5 | 5.0 |
| Primary caregiver’s marital status | ||
| Married | 34 | 33.7 |
| Widowed | 2 | 2.0 |
| Divorced | 18 | 17.8 |
| Separated | 5 | 5.0 |
| Never married | 42 | 41.6 |
| Primary caregiver’s education level | ||
| Some High School | 21 | 20.8 |
| Completed High School | 25 | 24.8 |
| Some College | 38 | 37.6 |
| Completed College | 16 | 15.8 |
| Advanced Degree | 1 | 1.0 |
Procedures
All study procedures were approved by the Institutional Review Board for ethical conduct in research. Participants were recruited to the study via paid community recruiters and online and in-person flyers. Community recruiters were individuals who resided in low-income neighborhoods and who held leadership roles in a local, neighborhood coalition group. Recruiters were informed by study personnel of the study aims, recruitment process, and procedures to maintain contact for future waves of data collection and were paid $100 for each family they recruited to the study. Further, research assistants purposefully placed flyers in a local office for the Division of Child and Family Services to recruit families with histories of maltreatment. Caregivers provided informed consent and permission for their child to participate in the study, and youth provided their assent before participating in study activities. Study activities took place in private rooms at a university clinical research unit with trained research staff and pediatric nurses on site. Participants completed questionnaires and several tasks, and several biological samples were obtained from the child.
To measure HRV-R, a mobile electrocardiogram was utilized with seven attached pediatric dermal ECG electrodes placed on both sides of the child’s clavicle and lower rib cage, on the sternum, and on the upper and lower spine. Resting-state PNS system activity was obtained while participants were listening to a five-minute video of nature sounds. Following the baseline period, a five-minute modified version of the Trier Social Stress Task (Kirschbaum et al., 1993) was utilized in which youth were instructed to complete a series of mental arithmetic problems in front of an audience of researchers and their primary caregiver. In order to account for differences in math abilities, the difficulty of the task was adjusted based on youth response accuracy and speed. Throughout the task, researchers were trained to remain neutral and abstain from giving feedback. This task has been shown to reliably elicit psychological (e.g., negative emotion) and physiological (ANS activation) stress reactions (Gruenewald et al., 2004).
Measures
Parental History of Childhood Maltreatment
To assess maltreatment experiences in the caregiver’s childhood, the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) was utilized. In the present study, the five subscales used measured different types of childhood maltreatment: physical neglect (α = .77), emotional abuse, (α = .87), physical abuse (α = .77), sexual abuse (α = .97), and emotional neglect (α = .89). Responses were on a Likert-type scale from “1” (never true) to “5” (very often true), and higher scores represented a higher severity of childhood maltreatment. Due to their high correlation (r = .69) and conceptual overlap, scores for physical neglect and emotional neglect were summed to create a subscale representing total severity of neglect experiences. Using recommended cut-off scores for mild, moderate, and severe maltreatment (Bernstein & Fink, 1998), we found that 60.40% of caregivers experienced mild maltreatment during their childhood, 8.10% experienced moderate maltreatment, and 27.72% of caregivers experienced at least one type of severe maltreatment.
Parent Emotion Regulation
The Difficulties with Emotion Regulation Scale Short Form (DERS-SF; Kaufman et al. 2016) was used to measure levels of parental ER across six domains. Parents responded to a total of 18 items on a Likert scale from “1” (almost never) to “5” (almost always). A total of five subscales were calculated: strategies (e.g., “When I’m upset, it takes me a long time to feel better”; α = .82), non-acceptance (e.g., “When I’m upset, I feel guilty for feeling that way”; α = .83), impulse (e.g., “When I’m upset, I become out of control”; α = .93), goals (e.g., “When I’m upset, I have difficulty focusing on other things”; α = .88), awareness (e.g., “I am clear about my feelings” [reverse coded]; α = .78), and clarity (e.g., “I have no idea how I am feeling”; α = .87). Higher scores indicate greater difficulties across ER domains.
HRV-R
HRV was measured using the BioNex system from MindWare Technologies (Gahanna, OH), and the MindWare HRV 3.1.4 Software module was utilized to digitize heart rate data. The high-frequency band pass was set at .12 to .40, with a sample rate set of 1000 Hz. The high-frequency components of HRV were obtained via power spectrum analysis in order to isolate the influence of parasympathetic activity on HRV (Akselrod et al., 1981). Research has indicated that high frequency components of HRV are a valid measure of parasympathetic activity (Akselrod et al., 1981; Appelhans & Luecken, 2006). Baseline cardiography and respiration was calculated using spectral analysis of thoracic impedance, in order to account for noise in data collection (Ernst et al., 1999). Trained researchers also inspected and removed severe inadvertent cardiac fluctuations caused by participants’ physical movement or breath. An interpolation algorithm was utilized to convert inter-beat intervals into 120s segments, and a MAD/MED algorithm was utilized to detect physically improbable IBIs. To calculate HRV-R, a residualized difference score was calculated using the youth’s mean HRV during the rest period and the stress task. This type of calculation allowed us to adjust for the variance in baseline HRV (Berntson et al., 1997). Lower HRV residualized change scores indicate a decrease from baseline to the stress task, and are indicative of high levels of HRV-R and more self-regulation.
Covariates
Parent income and race were controlled for in the pathway from parent’s experiences of maltreatment to their self-reported emotion regulation, to avoid potential confounding effects. Prior research shows that both income and race are associated with child maltreatment and subsequent adult ER, as well as with children’s psychosocial outcomes (Kim & Drake, 2018; Morelen et al., 2013; Raver et al., 2017). Children’s BMI was controlled for in the association between parent’s ER and child’s HRV-R, as per recommendations for using HRV in psychophysiological research (Laborde et al., 2017).
Analysis
Hypotheses were tested using a structural equation modeling framework in Mplus Version 7.4 (Muthén & Muthén, 1998–2012). Missing data were minimal and ranged from 0% to 5%. The variable with the most missing data was HRV-R, which was missing three cases due to administration errors, one case due to faulty heart rate data, and one case due to an unknown reason. The Little’s test (1988) indicated data were not missing completely at random (MCAR), χ2 = 36.059 (df = 20), p = .015. Further analysis showed that missingness on CTQ variables were correlated with parents’ level of ER (impulsivity and non-acceptance). Thus, missing data were assumed to be missing at random (MAR) and were analyzed with full information maximum likelihood (FIML).
A confirmatory factor analysis (CFA) was conducted to confirm the factor structure of parental experiences of childhood maltreatment, made up of four observed variables that were subscales of the CTQ. Study hypotheses were tested using structural equation models (SEM). In all models, non-significant covariates were trimmed to increase model parsimony, as per recommendations in the SEM literature (Kline, 2015). First, a model was tested in which the latent factor for parental experiences of childhood maltreatment predicted facets of parent ER. In this model, race and income were controlled for. Second, models were tested in which parental ER predicted child’s self-regulation, as measured by HRV-R, and in which child sex moderated the pathways from the parental ER dimensions to child’s self-regulation. To test moderation by child sex, interaction terms were created for each DERS subscale with child sex (e.g., DERS impulsivity * sex). Lastly, a moderated mediation SEM was created to test the conditional indirect effect of parental history of childhood maltreatment on children’s self-regulation through parental ER, conditional upon the sex of the child. Child’s BMI was controlled for in all SEM that included the HRV-R variable. The CFA and SEM results were evaluated based on a variety of fit indices. Models were determined to have good fit if they exhibited CFI and TLI values over 0.95, RMSEA values below 0.06, and SRMR values below 0.08 (Hu & Bentler, 1999). The indirect effect and conditional indirect effect were evaluated using the product-of-coefficients approach (Fritz & MacKinnon, 2007). Significant moderation effects were probed via the simple slopes technique using an Excel tool for plotting interaction effects available online (Dawson, 2014).
Results
Descriptive Statistics and Correlations
Table 2 presents the descriptive statistics and bivariate correlations of study variables. Notably, youth HRV-R was significantly correlated with parents’ experiences of sexual abuse, and with their goal-related ER.
Table 2.
Bivariate Correlations, Means, and Standard Deviations (N = 101)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||||||
| 1. CTQ – Emotional abuse | — | |||||||||||||||
| 2. CTQ – Physical abuse | .65** | — | ||||||||||||||
| 3. CTQ – Sexual abuse | .47** | .48** | — | |||||||||||||
| 4. CTQ – Emotional neglect | .71** | .45** | .45** | — | ||||||||||||
| 5. CTQ – Physical neglect | .56** | .29** | .47** | .69** | — | |||||||||||
| 6. DERS Strategies | .27** | .15 | .27** | .21* | .26** | — | ||||||||||
| 7. DERS Non acceptance | .30** | .19 | .31** | .24* | .19 | .48** | — | |||||||||
| 8. DERS Impulse | .26** | .09 | .28** | .10 | .29** | .65** | .24* | — | ||||||||
| 9. DERS Goals | .40** | .16 | .28** | .22* | .19 | .65** | .31** | .68** | — | |||||||
| 10. DERS Awareness | .12 | .17 | .12 | .23* | .17 | .31** | .13 | .11 | .04 | — | ||||||
| 11. DERS Clarity | .22* | .10 | .35** | .19 | .34** | .63** | .42** | .52** | .53** | .32** | — | |||||
| 12. Youth HRV reactivity | .15 | .18 | .20* | .08 | .09 | .20 | .05 | .14 | .27** | −.02 | .08 | — | ||||
| 13. Child’s sex | .24* | .18 | .13 | .20* | .20* | .12 | .15 | −.07 | .02 | .16 | .08 | .16 | — | |||
| 14. Child’s BMI | −.04 | .02 | .13 | −.05 | −.06 | .05 | .03 | .02 | .04 | −.05 | .09 | .05 | .12 | — | ||
| 15. Parent’s race | −.08 | .07 | −.06 | −.12 | −.15 | .05 | .11 | .10 | .15 | −.02 | .02 | −.03 | −.11 | .02 | — | |
| 16. Income | −.11 | −.02 | −.16 | .00 | −.11 | −.13 | .01 | −.22 | −.12 | −.01 | −.06 | −.04 | .18 | .19 | −.07 | — |
|
| ||||||||||||||||
| Mean | 8.81 | 7.52 | 7.47 | 10.24 | 7.37 | 5.26 | 5.12 | 3.87 | 5.55 | 7.74 | 4.27 | −.10 | 1.52 | 21.96 | 1.96 | 21.74 |
| SD | 4.67 | 3.40 | 5.18 | 5.04 | 3.52 | 2.48 | 2.43 | 1.94 | 2.56 | 3.43 | 2.01 | 1.38 | .50 | 6.41 | .55 | 12.80 |
| Skewness | 1.4 | 2.03 | 2.23 | .87 | 1.89 | 1.58 | 1.64 | 3.04 | 1.67 | .32 | 2.46 | −.05 | −.10 | 1.46 | 1.47 | .73 |
| Kurtosis | 1.7 | 4.24 | 4.08 | −.21 | 2.91 | 3.00 | 3.39 | 11.54 | 3.54 | −.95 | 8.33 | .94 | −2.03 | 2.46 | 9.48 | .19 |
| Range | 20.00 | 16.00 | 20.00 | 18.00 | 14.00 | 12.00 | 12.00 | 12.00 | 12.00 | 12.00 | 12.00 | 8.28 | 1.00 | 33.42 | 4.00 | 52.50 |
Note. CTQ = Childhood Trauma Questionnaire, DERS = Difficulties in Emotion Regulation Scale, HRV = heart rate variability, BMI = body mass index
p < .05
p < .01
Direct and Indirect Effects
The CFA supported a single latent factor representing parents’ experiences of childhood maltreatment, represented by four indicators for neglect, emotional abuse, physical abuse, and sexual abuse (see Figure 2). The model exhibited excellent fit (CFI = .964, SRMR = .033), and all standardized factor loadings were significant (p < .001) and ranged from .568 to .914.
Fig. 2.
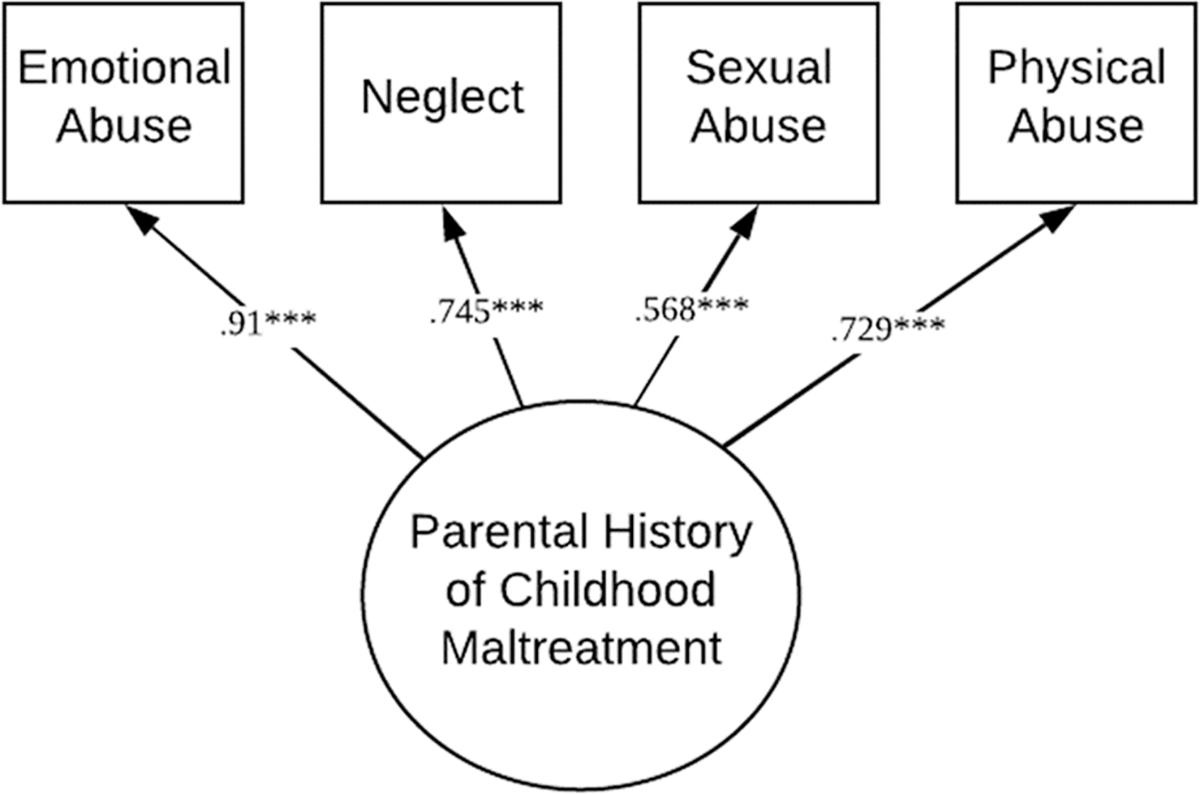
Measurement model for the latent factor representing parental history of childhood maltreatment from the four subscales of the Childhood Trauma Questionnaire
Note. Model fit was good: χ2(2) = 7.578, p < .05, CFI = .964, SRMR = .033. Standardized parameter estimates are shown in the figure
*p < .05, **p < .01, ***p < .001
Using this aforementioned latent factor, an SEM was fit in which parental history of childhood maltreatment predicted different facets of their ER difficulties (see Figure 3). The resulting model fit was good (CFI = .974, TLI = .951, RMSEA = .054, SRMR = .068). Overall, the model showed that parents’ experiences of maltreatment in childhood was related to more non-acceptance of emotional responses (β = .297, SE = .098, p < .01, 95% CI [.104, .490]), impulse control difficulties (β = .290, SE = .101, p < .01, 95% CI [.093, .487]), difficulty engaging in goal-directed behaviors (β = .385, SE = .092, p < .001, 95% CI [.206, .565]), lack of emotional clarity (β = .321, SE = .098, p < .01, 95% CI [.129, .513]), and limited access to ER strategies (β = .291, SE = .098, p < .01, 95% CI [.098, .484]). Race (coded as 1 = African American and 0 = Other) was associated with non-acceptance of emotional responses (β = −.234, SE = .087, p < .01, 95% CI [−.404, −.064]).
Fig. 3.
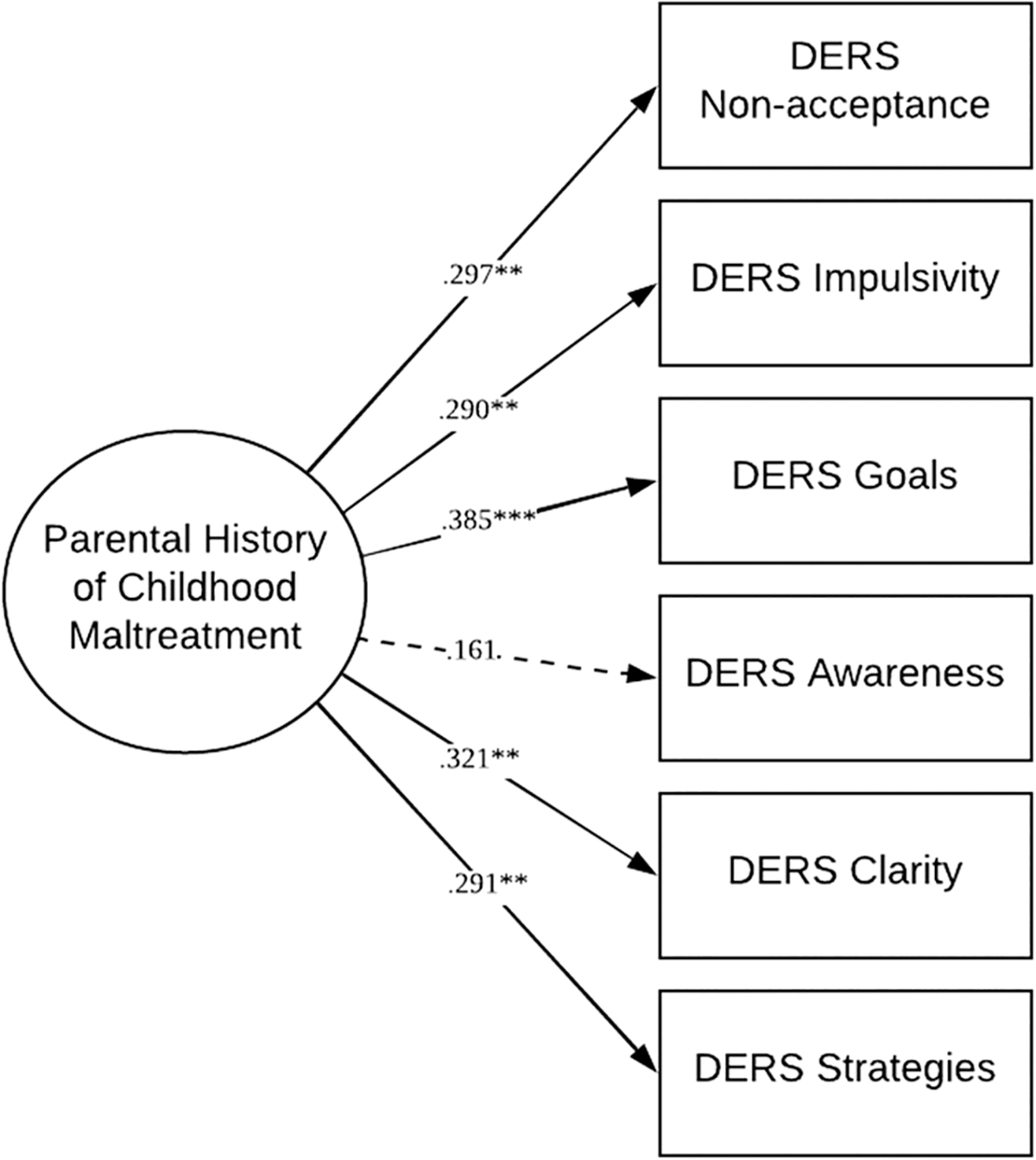
Structural equation model of the association between parental history of childhood maltreatment and their emotion regulation
Note. Model fit was good: CFI = .974, TLI = .951, RMSEA = .054, SRMR = .068. Race and income were controlled for in the analysis and non-significant paths were trimmed. Race (African American = 1, Other = 0) was significantly related to DERS non-acceptance (β = −.234, SE = .087, p < .01). Standardized parameter estimates are shown in the figure
*p < .05, **p < .01, ***p < .001
Second, we modeled the association between DERS subscales and child’s self-regulation (measured by HRV-R), moderated by child sex. The final model (see Figure 4) exhibited excellent model fit (CFI = 1.000, TLI = 1.000, RMSEA < .001, SRMR < .001). Parental difficulty engaging in goal-directed behaviors was significantly associated with child HRV-R (β = .293, SE = .146, p < .05, 95% CI [.007, .578]). Additionally, child sex was significantly associated with HRV-R (β = .328, SE = .146, p < .05, 95% CI [.042, .615]). The interaction between parental goal-directed behaviors and child sex was associated with child’s HRV-R (β = −.238, SE = .147, p = .10, 95% CI [−.526, .050]).
Fig. 4.
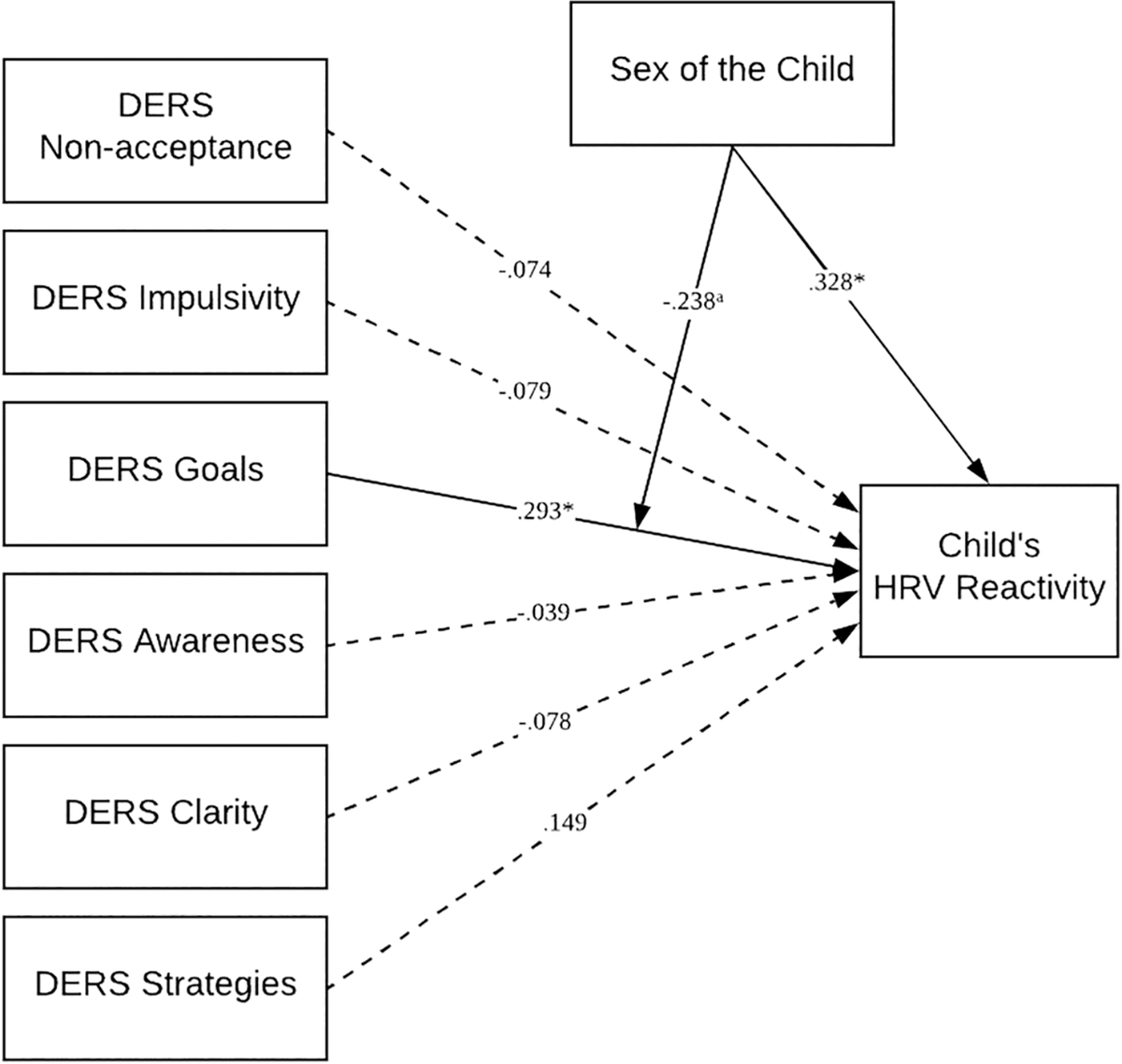
Structural equation model of the association between parent’s emotion regulation and children’s self-regulation as measured by HRV reactivity, moderated by child’s sex
Note. Child sex is coded as 1 = male and 2 = female. BMI was controlled for. Model fit was good: CFI = 1.000, TLI = 1.000, RMSEA < .001, SRMR < .001. Standardized parameter estimates are shown in the figure
ap < .10, *p < .05, **p < .01, ***p < .001
Lastly, a moderated mediation was tested to examine the indirect effect between parents’ experiences of childhood maltreatment and youth HRV-R, through parental ER, dependent on child sex (see Figure 5). The model showed excellent fit (CFI = .977, TLI = .965, RMSEA = .044, SRMR = .053). Parental childhood maltreatment history was significantly associated with the DERS scale representing difficulty engaging in goal-directed behaviors (β = .373, SE = .092, p < .001, 95% CI [.192, .554]), and difficulty engaging in goal-directed behaviors in turn was associated with their child’s self-regulation, as measured by HRV-R (β = .261, SE = .100, p < .01, 95% CI [.064, .457]). Child sex had a significant association with child HRV-R, such that girls had higher HRV-R scores, representing less self-regulation (β = .326, SE = .147, p < .05, 95% CI [.037, .614]). The interaction term (DERS goals * Sex) had a near significant association with child HRV-R (β = −.241, SE = .145, p = .096 95% CI [−.525, .043]). The indirect association between parents’ experiences of childhood maltreatment and child HRV-R, through parental ER (difficulty engaging in goal-directed behaviors), was significant (β = .097, SE = .045, p < .05, 95% CI [.009, .186]).
Fig. 5.
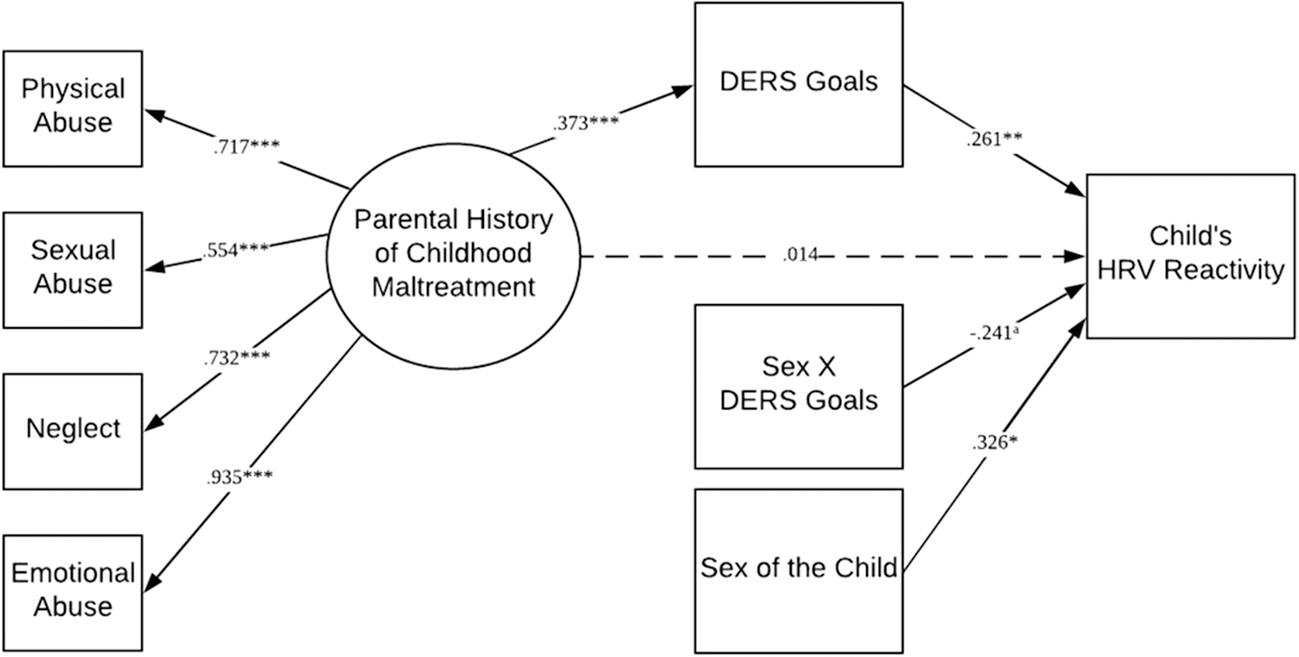
Structural equation model of the indirect association between parental history of childhood maltreatment and child’s HRV reactivity, through parent’s emotion regulation, and moderated by the sex of the child
Note. Sex of the child is coded as 1 = male and 2 = female. Model fit was good: CFI = .977, TLI = .965, RMSEA = .044, SRMR = .053. Standardized parameter estimates are shown in the figure
ap < .10, *p < .05, **p < .01, ***p < .001
A post hoc power analysis was conducted using a Monte Carlo simulation method in Mplus (Muthén & Muthén, 1998–2012, 2002). Using the parameter estimates obtained from the final moderated mediation model, the Monte Carlo approach estimated the obtained power for each unique path using 500 random samples of simulated data. The power for all significant paths were high, as expected. Of interest, the power for the effect of the near-significant interaction term on child HRV-R was .96, indicating that the effect was significant at the .05 level in 96% of the replications. Additionally, the power of the indirect effect was equal to 1.00, which exceeds the accepted standard of .80.
Finally, the association between parental ER and child HRV-R, moderated by sex of the child, was probed (see Figure 6). Results revealed that parents’ level of ER (specifically their difficulty engaging in goal-directed behaviors) was associated with HRV-R for sons but did not have an influence on HRV-R for daughters.
Fig. 6.
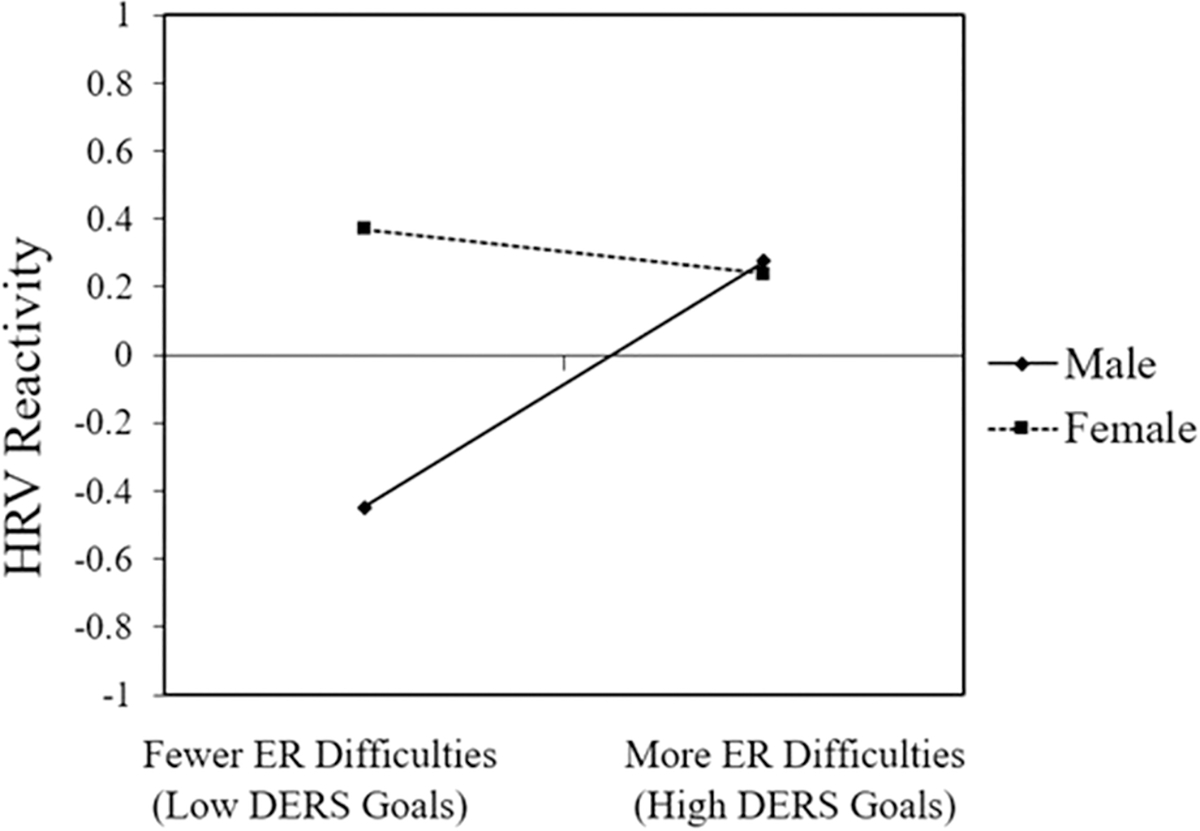
Graph depicting the association between parent’s ER difficulties (high scores on the Goals subscale of the DERS ) and child’s HRV reactivity, moderated by the sex of the child
Note. Variables were centered before the moderation analysis
Discussion
This study examined the intergenerational transmission of trauma effects from parents with histories of childhood maltreatment to offspring self-regulation, measured using a neurobiological proxy (HRV-R), via six separate dimensions of parental ER. Extending prior research on ER strategies and parenting (Lorber, 2012; Lorber & O’leary, 2005), the present study is the first to examine the multidimensionality of ER as it relates to the intergenerational transmission of parental maltreatment histories to child self-regulation outcomes. Findings showed parental maltreament in childhood was significantly related to greater difficulties in five of the six facets of ER: emotional non-acceptance, poor emotional clarity, behavioral impulsivity, inability to engage regulatory strategies, and inability to pursue goal-oriented behaviors. In addition, difficulty engaging in goal-directed behaviors was implicated as an indirect mechanism transmitting risk to offspring self-regulation. As expected, girls in this sample displayed greater problems with self-regulation (higher HRV residualized change scores) than boys, regardless of their parents’ maltreatment histories or ER. Contrary to our hypothesis, however, sons rather than daughters demonstrated greater vulnerability to parental ER difficulties and therefore incurred greater risk from the aforementioned transmission pathway. These findings serve to elucidate the role parents’ ER difficulties may play in the intergenerational transmission of trauma effects to offspring self-regulation among pre-adolescent children in low-income families.
Consistent with prior research and in line with our first hypothesis, maltreatment in childhood significantly predicted an array of emotion regulatory difficulties for parents (Lilly et al., 2014; Maughan & Cicchetti, 2002; Shields & Cicchetti, 1998). Specifically, parents who experienced maltreatment in childhood reported having a more challenging time controlling impulses, accepting negative emotions, pursuing goal-directed behaviors, clarifying emotional experiences, and utilizing ER strategies. Furthermore, greater difficulties in ER served as an indirect mechanism transmitting parental maltreatment effects to offspring HRV-R, specifically through the Goals subscale of the DERS. This is in line with prior research in the field indicating dominance of this ER domain over others when identifying group-level differences in ER and stress responses (Verkuil et al., 2010; Williams et al., 2015). For instance, Gross and colleagues (2015a) classify goal activation as a defining feature of emotion regulation. Although goal-directed behavior can serve as a tool to regulate mood, having a goal in mind may be what motivates an individual to implement ER in the first place. Thus, goal activation is both a part of the ER process (i.e., through affect regulation) and the desired outcome. For example, one might use the goal of getting work done to redirect focus from a negative emotional experience, thereby increasing task focus while modulating the negative feeling. The inability to engage in task-oriented behavior in pursuit of one’s goals may indicate that the negative emotion has overwhelmed the individual’s other ER faculties, therefore influencing the salience of this dimension over the others.
In support of our second hypothesis, child sex was significantly associated with child self-regulation, with daughters demonstrating more physiological dysregulation than their male counterparts. Prior research indicates pre-adolescent and adolescent females are more likely to show low baseline HRV and greater parasympathetic vulnerability, both of which have been implicated in internalizing psychopathology (Bongers et al., 2003; Fiol-Veny et al., 2018; Koenig et al., 2017). The results presented here extend this literature to include self-regulation processes occurring during a social stress task (Hinnant et al., 2015). A potential explanation for this is the increased salience of peer influence occurring for females at this stage in development as they mature more rapidly towards puberty than their male counterparts (Bongers et al., 2003; Negriff & Susman, 2011). Indeed, increased peer influence has been found to intensify stress reactivity in adolescents (Doom et al., 2017). Meanwhile, increases in estrogen and progesterone, particularly for females, stifle negative feedback loops involved in stress regulation (Zahn-Waxler et al., 2008), making the transition to puberty particularly demanding on female self-regulation.
Contrary to our expectations, parents’ ER did not significantly influence daughters’ physiological self-regulation as it did for sons. However, having a parent with fewer ER difficulties was protective for the sons in this sample. It may be that emotion-related socialization behaviors provided to girls early in life become ingrained faster than with boys, thus diminishing the influence of parental ER on neurobiological self-regulatory systems by the time they reach puberty (Bongers et al., 2003; Morris et al., 2017). Additionally, girls are more likely than boys to receive emotion socialization messages from other socializing agents in their lives aside from their parents (i.e., older siblings; Dunn et al., 1987), while parents may be the primary source of emotion socialization for boys. Thus, when emotion coaching from parents is not present, boys may display worse outcomes (Barnett & Scaramella, 2013; Eisenberg et al., 1998). Interestingly, in a sample of mothers with maltreatment histories, Fuchs and colleagues (2016) found that mothers showed attunement in basal cortisol levels (a key hormone in the neurobiological regulation of stress) with their sons, but not with their daughters, when compared to a group of mothers without a history of abuse. The child’s sex alone did not predict cortisol levels, once more suggesting that the transmission of effects from parental trauma to child neurobiological self-regulatory systems may have specific effects for sons (Fuchs et al., 2016). The current study adds to this evidence base, indicating that factors more proximal to the child, such as parental ER, should also be considered when examining sex-specific transmission pathways.
Limitations and Future Directions
The present study’s sample was comprised predominantly of African American families living in poverty. Though the ethnic distribution of this study’s sample is certainly a strength, limits to generalizability must be noted. African American families are documented to experience social strains, such as discrimination, in addition to those placed on low-income families (Brody et al., 2013). Additionally, sex-specific rearing strategies are culturally bound, as are cultural norms surrounding emotion socialization (Eisenberg et al., 1998; Morris et al., 2017). Thus, researchers are cautioned against generalizing these results to majority White samples or families living in low-income conditions generally. An additional limitation to this study includes the saturation of mother-child dyads in the sample. To examine the unique and combined effects of mothers and fathers on child self-regulation and HRV-R, the recruitment of fathers is necessary. In light of research indicating differential effects of fathering behaviors in the ER development of their daughters, the specific role of father ER and dysregulation in female neurobiological ER development deserves more attention (Eisenberg et al., 1998). All the data presented here were collected at the same timepoint, limiting the ability to detect the developmental effects of parental maltreatment history on child ER. Similarly, the directionality from parental ER to child HRV-R is based on established theory and the cross-sectional design does not afford us the ability to partition these dynamic associations. Lastly, this study’s sample size may limit the power to examine sex differences in the transmission of trauma effects through parental ER. In line with recommendations proposed by Zahn-Waxler et al. (2008), the interaction between child sex and the Goals subscale of the DERS is presented and discussed here in the hopes that future research will replicate and fortify these findings within larger samples and longitudinal designs.
Strengths and Implications
The results presented here add to the literature on the transmission of trauma effects by identifying one of six dimensions of parental ER that poses a risk to child neurobiological self-regulatory outcomes. Future research seeking to replicate these finding should note the community-recruited, low-income nature of the sample. Furthermore, trauma-informed interventions aiming to support low-income parents in these communities should consider prioritizing ER skills development in their programs. For example, the Unified Protocol for the transdiagnostic treatment of emotional disorders (Barlow et al., 2018)—an evidence-based intervention that focuses on the role of ER for treating a broad range of disorders—is broadly applicable and could be useful in trauma-informed interventions for low-income parents (Bullis et al., 2018). The differences in effects observed for girls and boys in this study suggest that behavioral interventions aimed at children of parents with maltreatment histories should consider targeting daughters before they transition to puberty. Meanwhile, prioritizing self-regulatory instruction may be particularly beneficial for boys whose parents struggle with ER. It is also important to note that the perpetuation of adversity within poverty contexts may sustain the heightened physiological reactions seen in children of parents with maltreatment histories (Boyce & Ellis, 2005). Policies to address gross inequalities in wealth for families can ameliorate additional stressors influencing ER for parents and self-regulation development in children.
Acknowledgments
Funding: This study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health (grant number UL1TR002378- Oshri PI), and partially supported through the National Institute on Drug Abuse (grant number 5K01DA045219–02-PI Oshri).
Conflict of Interest: Author A and Author B declare that they have no conflict of interest. Author C and Author D have received research grants from the National Center for Advancing Translational Sciences of the National Institutes of Health and Author D has received research grants from the National Institute on Drug Abuse.
Footnotes
Compliance with Ethical Standards
Ethical approval: All procedures performed in studies involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent: Informed consent was obtained from all individual participants included in the study.
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of a an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
References
- Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger A, & Cohen RJ (1981). Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science, 213(4504), 220–222. 10.1126/science.6166045 [DOI] [PubMed] [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, Dube SR, & Giles WH (2006, Apr). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. 10.1007/s00406-005-0624-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Appelhans BM, & Luecken LJ (2006). Heart rate variability as an index of regulated emotional responding. Review of General Psychology, 10(3), 229–240. 10.1037/1089-2680.10.3.229 [DOI] [Google Scholar]
- Barlow DH, Farchione TJ, Sauer-Zavala S, Murray Latin H, Ellard KK, Bullis JR, Bentley KH, Boettcher HT, & Cassiello-Robbins C (2018). Unified protocol for transdiagnostic treatment of emotional disorders (Second ed.). Oxford University Press. [Google Scholar]
- Barnett MA, & Scaramella LV (2013). Mothers’ parenting and child sex differences in behavior problems among African American preschoolers. Journal of Family Psychology, 27(5), 773–783. 10.1037/a0033792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP (2015). Respiratory sinus arrhythmia: A transdiagnostic biomarker of emotion dysregulation and psychopathology. Current opinion in psychology, 3, 43–47. 10.1016/j.copsyc.2015.01.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp L, & Mead HK (2007). Polyvagal Theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology, 74(2), 174–184. 10.1016/j.biopsycho.2005.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Katkin ES, Strassberg Z, & Snarr J (2001). Disinhibitory psychopathology in male adolescents: Discriminating conduct disorder from attention-deficit/hyperactivity disorder through concurrent assessment of multiple autonomic states [Periodical]. Journal of Abnormal Psychology, 110(4), 610–624. 10.1037/0021-843X.110.4.610 [DOI] [PubMed] [Google Scholar]
- Bernstein DP, & Fink L (1998). Childhood trauma questionnaire: A retrospective self-report: Manual. Harcourt Brace & Company. [Google Scholar]
- Berntson GG, Bigger JT Jr., Eckberg DL, Grossman P, Kaufmann PG, Malik M, Nagaraja HN, Porges SW, Saul JP, Stone PH, & van der Molen MW (1997). Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology, 34(6), 623–648. 10.1111/j.1469-8986.1997.tb02140.x [DOI] [PubMed] [Google Scholar]
- Blair C, & Raver CC (2012). Individual development and evolution: Experiential canalization of self-regulation. Developmental Psychology, 48(3), 647–657. 10.1037/a0026472 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bongers IL, Koot HM, Van der Ende J, & Verhulst FC (2003). The normative development of child and adolescent problem behavior. Journal of Abnormal Psychology, 112(2), 179–192. 10.1037/0021-843X.112.2.179 [DOI] [PubMed] [Google Scholar]
- Bornstein MH, & Suess PE (2000). Child and mother cardiac vagal tone: Continuity, stability, and concordance across the first 5. Developmental Psychology, 36(1), 54–65. 10.1037/0012-1649.36.1.54 [DOI] [PubMed] [Google Scholar]
- Boyce WT, & Ellis BJ (2005). Biological sensitivity to context: I. An evolutionary–developmental theory of the origins and functions of stress reactivity. Development and Psychopathology, 17(2), 271–301. https://doi.org/10.10170S0954579405050145 [DOI] [PubMed] [Google Scholar]
- Bridgett DJ, Burt NM, Edwards ES, & Deater-Deckard K (2015). Intergenerational transmission of self-regulation: A multidisciplinary review and integrative conceptual framework. Psychological Bulletin, 141(3), 602–654. 10.1037/a0038662 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, Yu T, Chen Y. f., Kogan SM, Evans GW, Beach SRH, Windle M, Simons RL, Gerrard M, Gibbons FX, & Philibert RA (2013). Cumulative socioeconomic status risk, allostatic load, and adjustment: A prospective latent profile analysis with contextual and genetic protective factors. Developmental Psychology, 49(5), 913–927. 10.1037/a0028847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckholdt KE, Parra GR, & Jobe-Shields L (2014). Intergenerational transmission of emotion dysregulation through parental invalidation of emotions: Implications for adolescent internalizing and externalizing behaviors. Journal of Child and Family Studies, 23(2), 324–332. 10.1007/s10826-013-9768-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bullis JR, Bentley KH, & Kennedy KA (2018). Group treatment applications of the Unified Protocol. In Barlow DH & Farchione TJ (Eds.), Applications of the Unified Protocol for transdiagnostic treatment of emotional disorders (pp. 252–267). Oxford University Press. [Google Scholar]
- Burkett LP (1991). Parenting behaviors of women who were sexually abused as children in their families of origin. Family Process, 30(4), 421–434. 10.1111/j.1545-5300.1991.00421.x [DOI] [PubMed] [Google Scholar]
- Burns EE, Jackson JL, & Harding HG (2010). Child maltreatment, emotion regulation, and posttraumatic stress: The impact of emotional abuse. Journal of Aggression, Maltreatment & Trauma, 19(8), 801–819. 10.1080/10926771.2010.522947 [DOI] [Google Scholar]
- Chaplin TM, Cole PM, & Zahn-Waxler C (2005). Parental socialization of emotion expression: Gender differences and relations to child adjustment. Emotion, 5(1), 80–88. 10.1037/1528-3542.5.1.80 [DOI] [PubMed] [Google Scholar]
- Cole PM, Ram N, & English MS (2019). Toward a unifying model of self-regulation: A developmental approach. Child Development Perspectives, 13(2), 91–96. 10.1111/cdep.12316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collishaw S, Dunn J, O’Connor TG, Golding J, & Team t. A. S. (2007). Maternal childhood abuse and offspring adjustment over time. Development and Psychopathology, 19(2), 367–383. 10.1017/S0954579407070186 [DOI] [PubMed] [Google Scholar]
- Dawson JF (2014). Moderation in management research: What, why, when, and how. Journal of Business and Psychology, 29(1), 1–19. 10.1007/s10869-013-9308-7 [DOI] [Google Scholar]
- DiLillo D, & Damashek A (2003). Parenting characteristics of women reporting a history of childhood sexual abuse. Child Maltreatment, 8(4), 319–333. 10.1177/1077559503257104 [DOI] [PubMed] [Google Scholar]
- DiLillo D, Tremblay GC, & Peterson L (2000). Linking childhood sexual abuse and abusive parenting: The mediating role of maternal anger. Child Abuse and Neglect, 24(6), 767–779. 10.1016/S0145-2134(00)00138-1 [DOI] [PubMed] [Google Scholar]
- Doom JR, Doyle CM, & Gunnar MR (2017). Social stress buffering by friends in childhood and adolescence: Effects on HPA and oxytocin activity. Social Neuroscience, 12(1), 8–21. 10.1080/17470919.2016.1149095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn J, Bretherton I, & Munn P (1987). Conversations about feeling states between mothers and their young children. Developmental Psychology, 23(1), 132–139. 10.1037/0012-1649.23.1.132 [DOI] [Google Scholar]
- Ehrensaft MK, Knous-Westfall HM, Cohen P, & Chen H (2015). How does child abuse history influence parenting of the next generation? Psychology of Violence, 5(1), 16–25. 10.1037/a0036080 [DOI] [Google Scholar]
- Eisenberg N, Cumberland A, & Spinrad TL (1998). Parental socialization of emotion. Psychological Inquiry, 9(4), 241–273. 10.1207/s15327965pli0904_1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, & Fabes RA (1994). Mothers’ reactions to children’s negative emotions: Relations to children’s temperament and anger behavior. Merrill-Palmer Quarterly, 40(1), 138–156. https://www.jstor.org/stable/23087912 [Google Scholar]
- El-Sheikh M, & Erath SA (2011). Family conflict, autonomic nervous system functioning, and child adaptation: State of the science and future directions. Development and Psychopathology, 23(2), 703–721. 10.1017/S0954579411000034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Sheikh M, & Whitson SA (2006). Longitudinal relations between marital conflict and child adjustment: Vagal regulation as a protective factor. Journal of Family Psychology, 20(1), 30. 10.1037/0893-3200.20.1.30 [DOI] [PubMed] [Google Scholar]
- El- Sheikh M, Harger J, & Whitson SM (2001). Exposure to interparental conflict and children’s adjustment and physical health: The moderating role of vagal tone. Child Development, 72(6), 1617–1636. 10.1111/1467-8624.00369 [DOI] [PubMed] [Google Scholar]
- Ernst JM, Litvack DA, Lozano DL, Cacioppo JT, & Berntson GG (1999). Impedance pneumography: Noise as signal in impedance cardiography. Psychophysiology, 36(3), 333–338. 10.1017/S0048577299981003 [DOI] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, & Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. 10.1016/S0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- Fiol-Veny A, De la Torre-Luque A, Balle M, & Bornas X (2018). Diminished heart rate complexity in adolescent girls: A sign of vulnerability to anxiety disorders? Anxiety, Stress, & Coping, 31(4), 1–12. 10.1080/10615806.2018.1475004 [DOI] [PubMed] [Google Scholar]
- Fritz MS, & MacKinnon DP (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. 10.1111/j.1467-9280.2007.01882.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuchs A, Möhler E, Resch F, & Kaess M (2016). Sex-specific differences in adrenocortical attunement in mothers with a history of childhood abuse and their 5-month-old boys and girls. Journal of Neural Transmission, 123(9), 1085–1094. 10.1007/s00702-016-1525-6 [DOI] [PubMed] [Google Scholar]
- Gross JJ (2015a). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. 10.1080/1047840X.2014.940781 [DOI] [Google Scholar]
- Gross JJ (2015b). The extended process model of emotion regulation: Elaborations, applications, and future directions. Psychological Inquiry, 26(1), 130–137. 10.1080/1047840X.2015.989751 [DOI] [Google Scholar]
- Gruenewald TL, Kemeny ME, Aziz N, & Fahey JL (2004). Acute threat to the social self: Shame, social self-esteem, and cortisol activity. Psychosomatic Medicine, 66(6), 915–924. 10.1097/01.psy.0000143639.61693.ef [DOI] [PubMed] [Google Scholar]
- Hinnant JB, Erath SA, & El-Sheikh M (2015). Harsh parenting, parasympathetic activity, and development of delinquency and substance use. Journal of Abnormal Psychology, 124(1), 137–151. 10.1037/abn0000026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holzman JB, & Bridgett DJ (2017). Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: A meta-analytic review. Neuroscience and Biobehavioral Reviews, 74, 233–255. 10.1016/j.neubiorev.2016.12.032 [DOI] [PubMed] [Google Scholar]
- Hu L. t., & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Kaufman E, Xia M, Fosco G, Yaptangco M, Skidmore C, & Crowell S (2016). The Difficulties in Emotion Regulation Scale Short Form (DERS-SF): Validation and replication in adolescent and adult samples [Article]. Journal of Psychopathology & Behavioral Assessment, 38(3), 443–455. 10.1007/s10862-015-9529-3 [DOI] [Google Scholar]
- Kim H, & Drake B (2018). Child maltreatment risk as a function of poverty and race/ethnicity in the USA. International Journal of Epidemiology, 47(3), 780–787. 10.1093/ije/dyx280 [DOI] [PubMed] [Google Scholar]
- Kim HK, Pears KC, Capaldi DM, & Owen LD (2009). Emotion dysregulation in the intergenerational transmission of romantic relationship conflict. Journal of Family Psychology, 23(4), 585–595. 10.1037/a0015935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke K-M, & Hellhammer DH (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1–2), 76–81. 10.1159/000119004 [DOI] [PubMed] [Google Scholar]
- Kline RB (2015). Principles and practice of structural equation modeling. Guilford publications. [Google Scholar]
- Koenig J, Rash JA, Campbell TS, Thayer JF, & Kaess M (2017). A meta-analysis on sex differences in resting-state vagal activity in children and adolescents. Frontiers in Physiology, 8, 1–11. 10.3389/fphys.2017.00582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laborde S, Mosley E, & Thayer JF (2017). Heart rate variability and cardiac vagal tone in psychophysiological research–Recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, 1–18. 10.3389/fpsyg.2017.00213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lilly MM, London MJ, & Bridgett DJ (2014). Using SEM to examine emotion regulation and revictimization in predicting PTSD symptoms among childhood abuse survivors. Psychological Trauma: Theory, Research, Practice and Policy, 6(6), 644–651. 10.1037/a0036460 [DOI] [Google Scholar]
- Little RJ (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American statistical Association, 83(404), 1198–1202. 10.1080/01621459.1988.10478722 [DOI] [Google Scholar]
- Lorber MF (2012). The role of maternal emotion regulation in overreactive and lax discipline. Journal of Family Psychology, 26(4), 642–647. 10.1037/a0029109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorber MF, & O’leary SG (2005). Mediated paths to overreactive discipline: Mothers’ experienced emotion, appraisals, and physiological responses. Journal of Consulting and Clinical Psychology, 73(5), 972–981. 10.1037/0022-006X.73.5.972 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maughan A, & Cicchetti D (2002). Impact of child maltreatment and interadult violence on children’s emotion regulation abilities and socioemotional adjustment. Child Development, 73(5), 1525–1542. 10.1111/1467-8624.00488 [DOI] [PubMed] [Google Scholar]
- Melnick SM, & Hinshaw SP (2000). Emotion regulation and parenting in AD/HD and comparison boys: Linkages with social behaviors and peer preference. Journal of Abnormal Child Psychology, 28(1), 73–86. 10.1023/A:1005174102794 [DOI] [PubMed] [Google Scholar]
- Miranda JK, de la Osa N, Granero R, & Ezpeleta L (2013). Multiple mediators of the relationships among maternal childhood abuse, intimate partner violence, and offspring psychopathology. Journal of interpersonal violence, 28(14), 2941–2965. 10.1177/0886260513488686 [DOI] [PubMed] [Google Scholar]
- Moehler E, Biringen Z, & Poustka L (2007). Emotional availability in a sample of mothers with a history of abuse. American Journal of Orthopsychiatry, 77(4), 624–628. 10.1037/0002-9432.77.4.624 [DOI] [PubMed] [Google Scholar]
- Morelen D, Jacob ML, Suveg C, Jones A, & Thomassin K (2013). Family emotion expressivity, emotion regulation, and the link to psychopathology: Examination across race. British Journal of Psychology, 104(2), 149–166. 10.1111/j.2044-8295.2012.02108.x [DOI] [PubMed] [Google Scholar]
- Morris AS, Criss MM, Silk JS, & Houltberg BJ (2017). The impact of parenting on emotion regulation during childhood and adolescence. Child Development Perspectives, 11(4), 233–238. 10.1111/jora.12586 [DOI] [Google Scholar]
- Morris AS, Silk JS, Steinberg L, Myers SS, & Robinson LR (2007). The Role of the Family Context in the Development of Emotion Regulation. Social development (Oxford, England), 16(2), 361–388. 10.1111/j.1467-9507.2007.00389.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2012). Mplus user’s guide Seventh edition. Muthén & Muthén. [Google Scholar]
- Muthén LK, & Muthén BO (2002). How to use a Monte Carlo study to decide on sample size and determine power. Structural equation modeling, 9(4), 599–620. 10.1207/S15328007SEM0904_8 [DOI] [Google Scholar]
- Negriff S, & Susman EJ (2011). Pubertal timing, depression, and externalizing problems: A framework, review, and examination of gender differences. Journal of Research on Adolescence, 21(3), 717–746. 10.1111/j.1532-7795.2010.00708.x [DOI] [Google Scholar]
- Oshri A, Liu S, Huffman LG, & Koss KJ (2020). Firm parenting and youth adjustment: Stress reactivity and dyadic synchrony of respiratory sinus arrhythmia. Developmental Psychobiology. 10.1002/dev.22019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri A, Sutton TE, Clay-Warner J, & Miller JD (2015). Child maltreatment types and risk behaviors: Associations with attachment style and emotion regulation dimensions. Personality and Individual Differences, 73, 127–133. 10.1016/j.paid.2014.09.015 [DOI] [Google Scholar]
- Perry NB, Mackler JS, Calkins SD, & Keane SP (2014). A transactional analysis of the relation between maternal sensitivity and child vagal regulation. Developmental Psychology, 50(3), 784–793. 10.1037/a0033819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porges SW (1995). Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A Polyvagal Theory. Psychophysiology, 32(4), 301–318. 10.1111/j.1469-8986.1995.tb01213.x [DOI] [PubMed] [Google Scholar]
- Porges SW (2007). The polyvagal perspective. Biological Psychology, 74(2), 116–143. 10.1016/j.biopsycho.2006.06.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raver CC, Roy AL, Pressler E, Ursache AM, & Charles McCoy D (2017). Poverty-related adversity and emotion regulation predict internalizing behavior problems among low-income children ages 8–11. Behavioral sciences, 7(1), 1–12. 10.3390/bs7010002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson LR, Morris AS, Heller SS, Scheeringa MS, Boris NW, & Smyke AT (2009). Relations between emotion regulation, parenting, and psychopathology in young maltreated children in out of home care. Journal of Child and Family Studies, 18(4), 421–434. 10.1007/s10826-008-9246-6 [DOI] [Google Scholar]
- Sheppes G, Suri G, & Gross JJ (2015). Emotion regulation and psychopathology. 11(1), 379–405. 10.1146/annurev-clinpsy-032814-112739 [DOI] [PubMed] [Google Scholar]
- Shields A, & Cicchetti D (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27(4), 381–395. 10.1207/s15374424jccp2704_2 [DOI] [PubMed] [Google Scholar]
- Skowron EA, Loken E, Gatzke-Kopp LM, Cipriano-Essel EA, Woehrle PL, Van Epps JJ, Gowda A, & Ammerman RT (2011). Mapping cardiac physiology and parenting processes in maltreating mother-child dyads [Periodical]. Journal of Family Psychology, 25(5), 663–674. 10.1037/a0024528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soenke M, Hahn KS, Tull MT, & Gratz KL (2010). Exploring the relationship between childhood abuse and analogue generalized anxiety disorder: The mediating role of emotion dysregulation. Cognitive Therapy and Research, 34(5), 401–412. 10.1007/s10608-009-9264-8 [DOI] [Google Scholar]
- Thayer JF, & Lane RD (2000). A model of neurovisceral integration in emotion regulation and dysregulation. Journal of Affective Disorders, 61(3), 201–216. 10.1016/S0165-0327(00)00338-4 [DOI] [PubMed] [Google Scholar]
- Thayer JF, & Lane RD (2009). Claude Bernard and the heart–brain connection: Further elaboration of a model of neurovisceral integration. Neuroscience and Biobehavioral Reviews, 33(2), 81–88. 10.1016/j.neubiorev.2008.08.004 [DOI] [PubMed] [Google Scholar]
- Verkuil B, Brosschot JF, Gebhardt WA, & Thayer JF (2010). When worries make you sick: a review of perseverative cognition, the default stress response and somatic health. Journal of Experimental Psychopathology, 1(1), 87–118. 10.5127/jep.009110 [DOI] [Google Scholar]
- Williams DP, Cash C, Rankin C, Bernardi A, Koenig J, & Thayer JF (2015). Resting heart rate variability predicts self-reported difficulties in emotion regulation: A focus on different facets of emotion regulation. Frontiers in Psychology, 6, 1–8. 10.3389/fpsyg.2015.00261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahn-Waxler C, Shirtcliff EA, & Marceau K (2008). Disorders of childhood and adolescence: Gender and psychopathology. Annual Review of Clinical Psychology, 4(1), 275–303. 10.1146/annurev.clinpsy.3.022806.091358 [DOI] [PubMed] [Google Scholar]