

Abstract
Transthyretin amyloid cardiomyopathy (ATTR‐CM) is caused by the cardiac deposition of insoluble amyloid fibrils formed by misfolded transthyretin proteins and is associated with various cardiac symptoms, such as progressive heart failure, conduction disturbance, and arrhythmia. The implementation of 99mtechnetium (99mTc)‐labelled bone radiotracer scintigraphy for diagnosing ATTR‐CM has enabled accurate diagnosis of the disease with high sensitivity and specificity and positioned this diagnostic modality as an integral part of disease diagnostic algorithms. In 2020, 99mTc‐pyrophosphate scintigraphy received exceptional approval for Japanese national health insurance reimbursement as a diagnostic method of ATTR‐CM. Nevertheless, the utility of 99mTc‐labelled bone radiotracer scintigraphy and the importance of an early diagnosis of suspected ATTR‐CM using this technique have yet to be internalized as common practice by general cardiologists, and guidance on daily clinical scenarios to consider this technique for a diagnosis of suspected ATTR‐CM is warranted. In this review, we discuss the utility of 99mTc‐labelled bone radiotracer scintigraphy for the early diagnosis of ATTR‐CM based on published literature and the outcomes of an advisory board meeting. This review also discusses clinical scenarios that could support early diagnosis of suspected ATTR‐CM as well as common pitfalls, correct implementation, and future perspectives of 99mTc‐labelled bone radiotracer scintigraphy in daily clinical practice. The clinical scenarios to consider 99mTc‐labelled bone radiotracer scintigraphy in daily practice may include, but are not limited to, patients with a family history of the hereditary type of disease; elderly patients (aged ≥60 years) with unexplained cardiac findings (e.g. cardiac hypertrophy associated with abnormalities on an electrocardiogram, heart failure with preserved ejection fraction associated with unexplained left ventricular hypertrophy, and heart failure with reduced ejection fraction associated with atrial fibrillation and left ventricular hypertrophy); and patients with cardiac hypertrophy associated with diastolic dysfunction, right ventricular/interatrial septum/valve thickness, left ventricular sparkling, or apical sparing. Cardiac hypertrophy and persistent elevation in cardiac troponin in elderly patients are also suggestive of ATTR‐CM. 99mTc‐labelled bone radiotracer scintigraphy is also recommended in patients with characteristic cardiac magnetic resonance findings (e.g. diffuse subendocardial late gadolinium enhancement patterns, native T1 increase, and increase in extracellular volume) or patients with cardiac hypertrophy and bilateral carpal tunnel syndrome.
Keywords: Amyloidosis, Cardiomyopathy, Heart failure, 99mTechnetium‐pyrophosphate scintigraphy, Transthyretin
Introduction
Transthyretin (TTR) amyloidosis is a systemic disorder involving various organs and tissues and is caused by the systemic deposition of insoluble amyloid fibrils formed by misfolded TTR proteins. 1 TTR amyloidosis may present as various phenotypes, among which the disease resulting from the deposition of amyloid fibrils in the heart is specifically referred to as TTR amyloid cardiomyopathy (ATTR‐CM). 2 , 3 ATTR‐CM is associated with various cardiac symptoms, such as progressive heart failure, conduction disturbance, and arrhythmia. 2 , 3
The introduction of non‐invasive techniques and the emergence of disease‐modifying therapies (DMTs) have changed the diagnostic methods and treatment outcomes of ATTR‐CM. Developments in non‐invasive diagnostic modalities, such as 99mtechnetium (99mTc)‐labelled bone radiotracer scintigraphy, in addition to the historical gold‐standard endomyocardial biopsy, have enabled the accurate diagnosis of ATTR‐CM. 4 , 5 Society guidelines and expert consensus documents now recommend 99mTc‐labelled bone radiotracer scintigraphy for the diagnosis of ATTR‐CM, 6 , 7 , 8 , 9 , 10 and in 2020, 99mTc‐pyrophosphate (99mTc‐PYP) scintigraphy received exceptional approval for Japanese national health insurance reimbursement as a diagnostic method of ATTR‐CM. 11 As DMTs, several novel options, including the oral TTR stabilizer tafamidis and TTR silencers patisiran and inotersen, are now available for clinical use in many countries. 10 , 12 The introduction of 99mTc‐labelled bone radiotracer scintigraphy as a routine diagnostic test and treatment with a DMT at the National Amyloidosis Centre in the United Kingdom in 2012 resulted in the diagnosis of ATTR‐CM at an earlier stage of the disease and a significant improvement in the survival of diagnosed patients. 13 In addition, the use of bone‐avid radiotracer cardiac imaging allowed physicians to increasingly recognize that ATTR‐CM is an underdiagnosed cause of heart failure in several populations; specifically, ATTR‐CM has been identified in a significant subgroup of patients with heart failure with preserved ejection fraction (HFpEF), aortic stenosis, or hypertrophic cardiomyopathy. 14 , 15 , 16 , 17 Nevertheless, the utility of 99mTc‐labelled bone radiotracer scintigraphy as a diagnostic modality and the importance of early ATTR‐CM diagnosis have not yet been internalized as common practice by general cardiologists. 18 Moreover, the procedures for 99mTc‐labelled bone radiotracer scintigraphy are highly variable among institutions. 19 These findings indicate a need for guidance on daily clinical scenarios to consider 99mTc‐labelled bone radiotracer scintigraphy for a suspected diagnosis of ATTR‐CM, as well as a standardized protocol for imaging.
This review aims to provide an up‐to‐date understanding of ATTR‐CM and 99mTc‐labelled bone radiotracer scintigraphy by summarizing recent findings in the literature. This review also discusses clinical scenarios that could support the early identification of suspected ATTR‐CM cases in daily clinical practice as well as the appropriate use of 99mTc‐labelled bone radiotracer scintigraphy imaging. Clinical scenarios provided in this review are based on the clinical experience of the authors, as discussed in a virtual medical advisory board meeting held in September 2020.
Wild‐type and variant TTR amyloidosis: similarities and differences
Transthyretin amyloidosis may occur in individuals with either a wild‐type or mutated TTR gene [variant TTR (ATTRv) amyloidosis]. 1 , 2 Wild‐type TTR (ATTRwt) amyloidosis is commonly associated with cardiac involvement and is thus also referred to as wild‐type ATTR‐CM (ATTRwt‐CM; formerly known as senile systemic amyloidosis). 1 , 2 Dissociation of the TTR protein and misfolding and aggregation as amyloid fibrils (Figure 1 ) are pathological mechanisms common to ATTRwt and ATTRv amyloidosis. 2 In the variant type of the disease, TTR destabilization is caused by point mutations in the TTR gene, 2 and more than 130 TTR mutations have been identified worldwide. 20 Some TTR gene mutations, including the replacement of valine with methionine at position 30 (Val30Met or p.Val50Met) with a late onset of disease, are commonly associated with various symptoms, including cardiac symptoms. 3 , 21
Figure 1.
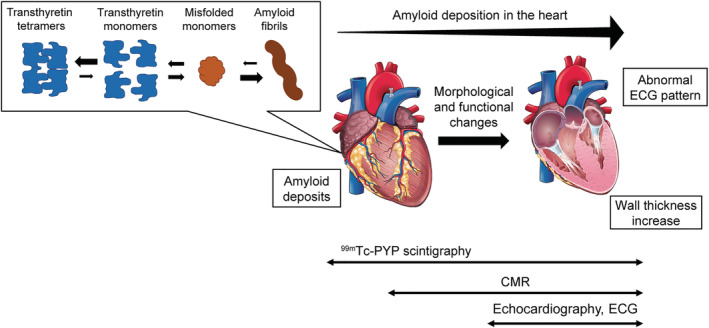
Conceptual diagram for the pathophysiology of transthyretin amyloid cardiomyopathy (ATTR‐CM) and applicability of non‐invasive diagnostic techniques. CMR, cardiac magnetic resonance.
In patients with ATTR‐CM, clinical symptoms such as carpal tunnel syndrome (CTS) and left ventricular hypertrophy (LVH) commonly present months to years before diagnosis, indicating the importance of clinicians' understanding of the most prevalent clinical manifestations of ATTR‐CM. 22 As patient characteristics and pathologies overlap between ATTRwt‐CM and late‐onset ATTRv‐CM, 3 a differential diagnosis aided by genetic testing is necessary.
Epidemiology of ATTRwt‐CM and applicability of non‐invasive diagnostic techniques for early patient identification
Epidemiology and natural history of ATTRwt‐CM
Although the true prevalence of ATTRwt‐CM remains unclear, previous research has reported that ATTRwt‐CM was found in 3.1–25% of autopsied elderly cases, 23 , 24 , 25 , 26 13% of elderly patients (aged ≥60 years) with heart failure with preserved ejection fraction, 14 and 16% of elderly patients with severe aortic stenosis. 27 The median survival for patients with ATTRwt‐CM is approximately 5 years from diagnosis, 13 , 28 and the disease may be associated with unexpected deaths among the elderly. 23
Approximately 85% of patients with biopsy‐proven ATTRwt‐CM have New York Heart Association (NYHA) functional Class ≥II symptoms. 29 , 30 These findings indicate that amyloid deposition in the heart does occur in patients at NYHA functional Class I or II stage. With the use of non‐invasive scintigraphy, identification of patients with an early‐stage (NYHA functional Class I or II) disease is occurring with increasing frequency. 31 A conceptual diagram representing the pathophysiology of ATTR‐CM and applicability of non‐invasive diagnostic techniques is shown in Figure 1 .
99mTc‐labelled bone radiotracer scintigraphy
For non‐invasive, disease‐specific diagnosis of ATTR‐CM at an early stage of the disease (NYHA functional Class I or II), the utility of cardiac scintigraphy using 99mTc‐labelled tracers, including 99mTc‐PYP, 99mTc‐3,3‐diphosphono‐1,2‐propanodicarboxylic acid (99mTc‐DPD), and 99mTc‐hydroxymethylene diphosphonate (99mTc‐HMDP), has been suggested in the literature. 32 , 33 In a previous study involving patients with suspected cardiac amyloidosis, Grade 2 or 3 myocardial uptake along with the absence of monoclonal gammopathy on serum and urine analysis demonstrated a specificity and positive predictive value of 100% for ATTR‐CM. 34 In a multicentre study that applied planar 99mTc‐PYP scintigraphy to patients with ATTR‐CM (including both ATTRwt‐CM and ATTRv‐CM), the heart‐to‐contralateral (H/CL) ratio (ratio of heart regions of interest mean counts to contralateral chest region of interest mean counts 35 ) in patients with NYHA functional Class I or II symptoms showed no difference from that in patients with Class III or IV symptoms. 32 Moreover, a follow‐up study of 11 asymptomatic individuals carrying a TTR gene mutation (i.e. asymptomatic carriers of ATTRv‐CM) revealed that 99mTc‐DPD scintigraphy measurement successfully detected cardiac involvement earlier than electrocardiogram (ECG), echocardiography, or biomarkers, although the number of subjects was low. 33 Subjects with Grade ≥1 cardiac 99mTc‐DPD uptake showed a statistically significant increase in interventricular septal thickness (IVST) on echocardiography vs. subjects without cardiac uptake (12.2 ± 2.3 mm vs. 9.1 ± 0.9 mm; P = 0.001) as well as a statistically significant increase in left ventricular wall thickness (11.6 ± 1.7 mm vs. 8.9 ± 0.8 mm; P = 0.0001). 33
Cardiac magnetic resonance, echocardiography, and ECG
Cardiac magnetic resonance (CMR) helps differentiate cardiac amyloidosis from other causes of LVH, such as hypertension and hypertrophic cardiomyopathy, 36 and can identify patients with cardiac amyloidosis, independent of the type of amyloid protein. However, the results are not specific to ATTR‐CM, and there is no consensus as to whether this diagnostic modality is suitable for early detection of the disease. In a pilot study that assessed the phenotypes of 49 patients (aged >65 years) with HFpEF, including 26 (53%) patients with NYHA functional Class II symptoms, 15 (31%) patients showed a characteristic infiltrative pattern on CMR. 37 Of these 15 patients, 9 had cardiac uptake in 99mTc‐DPD scintigraphy and were diagnosed with ATTRwt‐CM by genetic testing, while the remaining 6 had no significant cardiac 99mTc‐DPD uptake and were diagnosed with biopsy‐proven or suspected light‐chain (AL) amyloidosis 37 (amyloidosis characterized by the deposition of misfolded monoclonal immunoglobulin light chains 38 ). Late gadolinium enhancement (LGE) 39 is an established, commonly used CMR technique to evaluate cardiac amyloid burden and cardiac involvement. Native T1 and extracellular volume (ECV) measurement are quantitative assessments that can detect cardiac involvement with high sensitivity, 40 , 41 but research demonstrating their utility in early diagnosis of the disease is limited. Of note, LGE is not recommended in individuals with renal impairment because of safety concerns around the development of nephrogenic systemic fibrosis associated with the use of a gadolinium‐based contrast agent. 42
An echocardiographic increase in IVST can also be an indicator of ATTR‐CM, irrespective of NYHA functional class. According to an analysis of the global Transthyretin Amyloidosis Outcomes Survey (THAOS) registry, the proportion of patients with ATTR‐CM presenting with NYHA functional Class II–IV symptoms was not significantly different across patients with normal, mild, moderate, and severe IVST on echocardiography (75%, 75%, 89%, and 93%, respectively; P = 0.0866). 43 An apical sparing pattern is also indicative of ATTR‐CM, although its detection does not necessarily contribute to early diagnosis of the disease.
Electrocardiogram may be less sensitive in detecting ATTR‐CM at an early stage of the disease (Figure 1 ). In the aforementioned analysis of the THAOS registry, the proportion of patients with abnormal ECG findings, such as low voltage and pathological Q waves, was significantly lower among patients with normal or mildly increased IVST vs. patients with moderately or severely increased IVST. 43
Utility of 99mTc‐labelled bone radiotracer scintigraphy in the diagnosis of ATTR‐CM, guideline recommendations, and limitations
Evidence has been established regarding the utility of cardiac scintigraphy using 99mTc‐labelled tracers for the diagnosis of ATTR‐CM. 44 A meta‐analysis of six studies on 99mTc‐labelled bone radiotracer scintigraphy for ATTR‐CM (99mTc‐PYP, 99mTc‐DPD, and 99mTc‐HMDP) yielded a pooled sensitivity of 92.2% (95% confidence interval, 89–95%) and specificity of 95.4% (95% confidence interval, 77–99%) and found no statistically significant differences in diagnostic performance among the radiotracers used. 45 The risk of developing future cancer attributable to 99mTc‐PYP scintigraphy is low and estimated to be <1% of total future cancers. 46 By using positive cardiac uptake of the 99mTc‐labelled tracer as an indicator, suspected ATTRwt‐CM was found in 2.8% of individuals (aged ≥75 years; no prior clinical suspicion of ATTR‐CM) visiting a university hospital in Spain, 47 0.36% of individuals aged ≥65 years (estimated to be up to 1.4% of men in the ninth decade), 48 and 0.06% of individuals (aged >30 years) who underwent scintigraphy for non‐cardiac reasons at a university hospital in South Korea. 49 In an Australian general population, the prevalence of positive 99mTc‐HMDP cardiac uptake increased with age and reached 6.15% in men and 1.69% in women aged ≥85 years. 50
99mTc‐labelled bone radiotracer scintigraphy is now included in the diagnostic algorithms in the Japanese Circulation Society (JCS) guidelines for the diagnosis and treatment of cardiac amyloidosis 6 and in expert consensus recommendations assembled by the American Society of Nuclear Cardiology (ASNC), 7 Amyloidosis Research Consortium, 8 , 9 and European Society of Cardiology. 10 A detailed approach for planar 99mTc‐PYP scintigraphy with visual grading assessment and H/CL ratio‐based quantitative assessment is described in the JCS guidelines 6 and ASNC expert consensus recommendations for multi‐modality imaging in cardiac amyloidosis. 7 The assessment of planar 99mTc‐PYP scintigraphy is performed on the basis of 1‐ or 3‐h imaging (imaging assessed 1 or 3 h after radiotracer injection). Imaging should be followed by an H/CL ratio assessment and visual grading assessment. The cardiac uptake results are categorized as Grade 0 (no uptake), 1 (mild uptake, less than rib uptake), 2 (moderate uptake, equal to rib uptake), or 3 (high uptake, greater than rib uptake); Grades 2 and 3 are deemed positive for ATTR‐CM. 6 An H/CL ratio of >1.5 on 1‐h images or >1.3 on 3‐h images in 99mTc‐PYP scintigraphy has a high diagnostic accuracy in distinguishing ATTR‐CM from AL amyloidosis. 32 , 34 , 51 The 1‐h imaging has advantages in terms of patient comfort, fast throughput, and sensitivity of visual assessment, which is higher than that of the 3‐h imaging (95% vs. 58%); however, the specificity is relatively low (79%), requiring single‐photon emission computed tomography (SPECT) or SPECT/computed tomography (CT) imaging to differentiate true myocardial uptake from radiotracer activity associated with myocardial infarctions, rib fractures, or blood pools. 52 By contrast, the 3‐h imaging requires a longer interval between the radiotracer injection and imaging but enables reduction in blood pools and myocardial radiotracer activity, leading to an enhanced specificity (100%) in visual assessment. 52 Discordance between the 1‐ and 3‐h planar imaging results can be minimized by additionally obtaining SPECT or SPECT/CT images. 51 , 53 The authors recommend further planar imaging at 3 h, as visual grading is easy to use, and SPECT imaging is not feasible in all institutions across Japan.
Of note, however, it is advisable to not rely solely on 99mTc‐PYP scintigraphy results for the diagnosis of ATTR‐CM. As patients with AL amyloidosis may also test positive with 99mTc‐PYP scintigraphy, 34 , 54 the serum free light chain assay and serum and urine protein electrophoresis with immunofixation to confirm the absence of monoclonal protein, concurrently with bone‐avid tracer imaging, are essential for a non‐invasive, accurate diagnosis of ATTR‐CM. 6 , 8 , 9 , 34 For a definite diagnosis of ATTR‐CM, endomyocardial, abdominal fat pad, surgical skin, gastrointestinal, or salivary glands biopsy followed by amyloid typing and genetic testing may also be required. 6 , 8 , 9 Caution is advised for the selection of the biopsy site in patients with ATTRwt‐CM, as the sensitivity of fat pad biopsy (14–15%) is not as high as that of endomyocardial biopsy (approximately 100%) for detecting ATTR deposits. 55 , 56
Clinical scenarios to consider 99mTc‐PYP scintigraphy for a diagnosis of suspected ATTR‐CM
Presenting scenarios in daily clinical practice where 99mTc‐PYP scintigraphy should be considered for suspected ATTR‐CM helps cardiologists further understand the recommendations provided in existing guidelines or expert consensus documents. 6 , 7 , 8 , 9 This section summarizes the clinical scenarios to consider 99mTc‐PYP scintigraphy for suspected ATTR‐CM, as discussed in the virtual advisory board meeting.
Typical indicators for suspected ATTR‐CM are summarized in Figure 2 , and representative images of patients with ATTR‐CM are depicted in Figure 3A–3F . Detailed clinical scenarios for considering 99mTc‐PYP scintigraphy in daily clinical practice are shown in Table 1 . 99mTc‐PYP scintigraphy should be considered in patients with a family history of ATTRv amyloidosis or elderly patients (aged ≥60 years) with unexplained cardiac findings. Typical unexplained cardiac findings in elderly patients include cardiac hypertrophy on echocardiography, 57 abnormal ECG findings (e.g. progressive conduction disturbance, low QRS voltage or low voltage‐to‐mass ratio, and poor R‐wave progression), 43 , 58 , 59 HFpEF associated with LVH, 14 and heart failure with reduced ejection fraction (HFrEF) associated with atrial fibrillation and LVH. 99mTc‐PYP scintigraphy should be also considered in patients showing cardiac hypertrophy on echocardiography associated with diastolic dysfunction, right ventricular/interatrial septum/valve thickness, 43 left ventricular sparkling, or apical sparing. 60 , 61 Advanced age (≥60 years) associated with cardiac hypertrophy and persistent elevation in high‐sensitivity cardiac troponin (hs‐cTn) 62 , 63 and characteristic CMR findings, such as diffuse subendocardial LGE, 39 increased native T1, 40 and increased ECV, are also suggestive of ATTR‐CM. Moreover, 99mTc‐PYP scintigraphy should be considered in elderly patients with cardiac hypertrophy and CTS (especially bilateral CTS). 28 , 64 , 65
Figure 2.
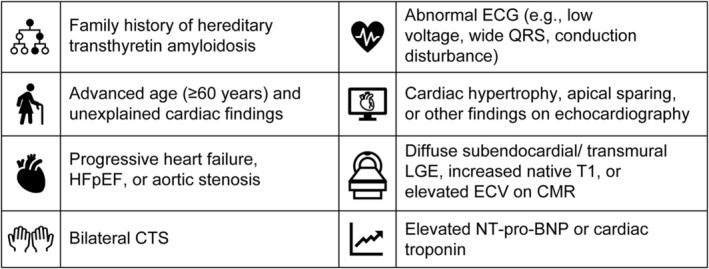
Typical indicators to suspect transthyretin amyloid cardiomyopathy (ATTR‐CM) and consider 99mTc‐PYP scintigraphy in daily clinical practice. CMR, cardiac magnetic resonance; CTS, carpal tunnel syndrome; ECV, extracellular volume; ECG, electrocardiogram; LGE, late gadolinium enhancement; NT‐pro‐BNP, N‐terminal pro–B‐type natriuretic peptide; HFpEF, heart failure with preserved ejection fraction.
Figure 3.
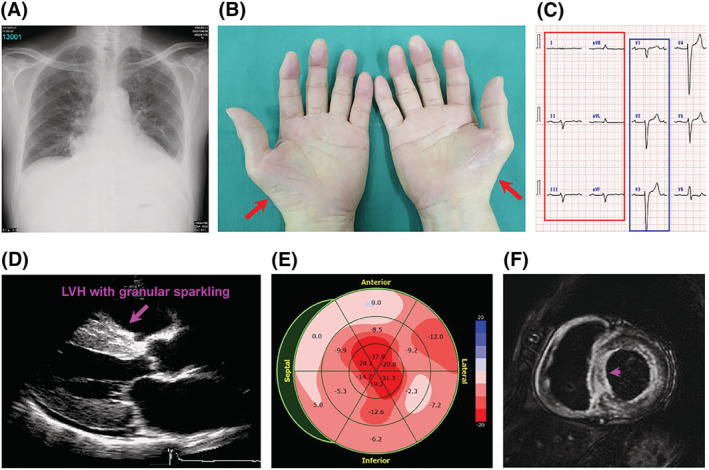
Representative images of patients with transthyretin amyloid cardiomyopathy (ATTR‐CM). (A) Heart failure with pulmonary congestion and pleural effusion, (B) carpal tunnel syndrome (CTS) with thenar muscle atrophy (red arrows) and numbness in the thumb to the thumb side of the ring finger (area served by the median nerve), (C) electrocardiogram with low voltage (red box) and pseudo‐infarct pattern (blue box), (D) cardiac hypertrophy [left ventricular hypertrophy (LVH) with granular sparkling] on echocardiography, (E) apical sparing on echocardiography, (F) cardiac magnetic resonance (CMR) with subendocardial late gadolinium enhancement (LGE). A ring‐shaped subendocardial contrast is observed, consistent with the endocardium. The septal site has transmural enhancement (arrow), and the right ventricle also shows contrast enhancement.
Table 1.
Typical clinical scenarios to consider 99mTc‐PYP scintigraphy for suspected ATTR‐CM
| Serial number | Clinical scenario |
|---|---|
| 1 | Family history of ATTRv amyloidosis |
| 2 | Age ≥60 years; cardiac hypertrophy on echocardiography associated with conduction disturbance, low voltage, or poor R‐wave progression on ECG |
| 3 | Age ≥60 years with HFpEF associated with unexplained LVH |
| 4 | Age ≥60 years with HFrEF associated with atrial fibrillation and LVH |
| 5 | Cardiac hypertrophy on echocardiography associated with diastolic dysfunction, right ventricular/interatrial septum/valve thickness, left ventricular sparkling, or apical sparing |
| 6 | Age ≥60 years; cardiac hypertrophy on echocardiography associated with persistently elevated hs‐cTn |
| 7 | Cardiac hypertrophy with diffuse subendocardial LGE patterns, native T1 increase, or increased ECV on CMR |
| 8 | Cardiac hypertrophy with CTS |
99mTc‐PYP, 99mtechnetium‐pyrophosphate; ATTR‐CM, transthyretin amyloid cardiomyopathy; ATTRv, variant transthyretin; CMR, cardiac magnetic resonance; CTS, carpal tunnel syndrome; ECG, electrocardiogram; ECV, extracellular volume; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; hs‐cTn, high‐sensitivity cardiac troponin; LGE, late gadolinium enhancement; LVH, left ventricular hypertrophy.
However, deviations from these clinical scenarios do not always exclude suspected ATTR‐CM. For example, the absence of a restrictive pattern or low QRS voltage on ECG should not rule out the diagnosis of ATTR‐CM, as these findings were not commonly observed in patients with moderate‐to‐severe increase in IVST (restrictive pattern, 18%; low QRS voltage, 33%). 43
99mTc‐PYP scintigraphy can be considered with a high priority when a patient presents with an elevated level (≥0.0308 ng/mL) of hs‐cTnT, increased left ventricular posterior wall thickness (≥13.6 mm), and wide QRS (≥120 ms); the 99mTc‐PYP positivity rates were 96%, 63%, 21%, and 13% when 3, 2, 1, and no criteria were met, respectively (Kumamoto criteria). 66 In another study that aimed to validate the Kumamoto criteria, the 99mTc‐PYP positivity rates were 89%, 69%, 39%, and 4% when 3, 2, 1, and none of the aforementioned criteria were met, respectively. 67
Data interpretation and common pitfalls of 99mTc‐PYP scintigraphy
Cardiologists may face difficulties in data interpretation and diagnosis of ATTR‐CM while implementing 99mTc‐PYP scintigraphy in daily clinical practice. In this section, guidance on the correct implementation and data interpretation of 99mTc‐PYP scintigraphy and common pitfalls of this diagnostic modality are discussed in detail.
Diagnostic algorithm for patients with Grade 1 myocardial tracer uptake and a negative monoclonal protein detection test
In daily clinical practice, patients sometimes present with Grade 1 myocardial tracer uptake (mild uptake less than rib uptake) and a negative monoclonal protein detection test. To distinguish cardiac blood pool activity from true myocardial uptake, 54 not only planar images but also SPECT or SPECT/CT images should be evaluated (Figure 4 A ). Figure 4 B depicts our proposed algorithm for diagnosing patients with Grade 1 myocardial tracer uptake and a negative monoclonal protein detection test. The next step after the SPECT or SPECT/CT image evaluation is to review CMR data (LGE, native T1, and ECV) or order CMR tests if no data are available. After thorough review of the available CMR data, ECG, echocardiography, and clinical findings, if ATTR‐CM is suspected, ATTR deposition should be evaluated with a biopsy. An endomyocardial biopsy is recommended when ATTR‐CM is strongly suspected; however, other sites (e.g. abdominal fat pad and upper gastrointestinal tract) can also be considered for a biopsy depending on the patient's condition, as a diagnosis of ATTR‐CM can be formed in Japan if amyloid deposition is detected in non‐cardiac biopsies. 68 As the sensitivity of non‐cardiac biopsies is low (14–15%), 55 , 56 the JCS guidelines recommend performing biopsies at multiple sites other than the endocardium. 6 In view of the progressive nature of the disease (median survival of approximately 5 years from diagnosis 13 , 28 ), a follow‐up with scintigraphy after 6 months–1 year is advisable in patients without ATTR deposition on biopsy or those not (or weakly) suspected of ATTR‐CM.
Figure 4.
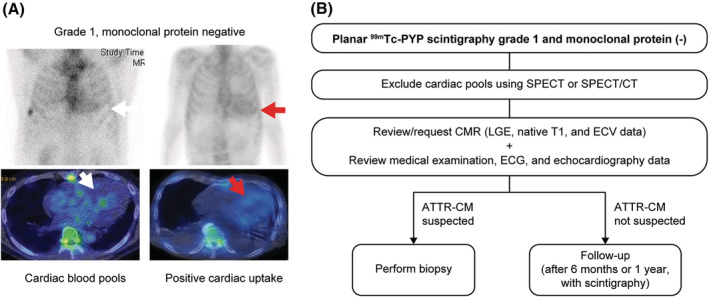
(A) Representative planar (top) and single‐photon emission computed tomography/computed tomography (SPECT/CT; bottom) images of patients with Grade 1 myocardial tracer uptake and negative monoclonal protein test. White and red arrows indicate cardiac blood pools and positive cardiac uptake, respectively. (B) Flow chart of transthyretin amyloid cardiomyopathy (ATTR‐CM) diagnosis in patients with planar 99mTc‐PYP scintigraphy Grade 1 and a negative monoclonal protein detection test. Endomyocardial, abdominal fat pad, or upper gastrointestinal tract biopsy is recommended. For patients who test negative with a biopsy, it is advisable to schedule regular follow‐up with scintigraphy after 6 months–1 year. Grade 1 in 99mTc‐PYP scintigraphy refers to mild uptake less than rib uptake.
False positives, false negatives, and inconsistencies between 99mTc‐PYP scintigraphy and biopsy findings
False‐positive cases in 99mTc‐PYP scintigraphy for ATTR‐CM may include Grade 2 or 3 myocardial uptake; a recent history of acute myocardial infarction 54 ; AL amyloidosis 34 , 54 , 69 , 70 , 71 , 72 , 73 ; apolipoprotein AI amyloidosis (AApoAI), apolipoprotein AII amyloidosis (AApoAII), apolipoprotein A‐IV amyloidosis (ApoAAIV), or β2‐microglobulin amyloidosis (Aβ2M) 10 ; hypertrophic cardiomyopathy 74 , 75 ; hydroxychloroquine toxicity 76 ; and cardiac blood pools. 54 Case reports on false‐positive myocardial uptake following intravenous iron injections have been published for 99mTc‐DPD and 99mTc‐HMDP scintigraphy. 77 , 78 In contrast, Grade 0 or 1 myocardial uptake, an insufficient amount of amyloid deposits, 79 rib fractures, 10 valvular/annular calcifications, 10 recent myocardial infarction, 10 delayed or premature acquisition in 99mTc‐PYP scintigraphy, 10 ATTRv‐CM with a low sensitivity for 99mTc‐labelled bone radiotracer scintigraphy (Ser77Tyr or Phe64Leu mutation), 10 , 80 and initial diagnosis of cardiac pools with myocardial deposits 81 are examples of possible false‐negative cases (Table 2 ). In case of inconsistencies between planar 99mTc‐PYP scintigraphy results and biopsy findings, potential causes should be suspected and investigated, such as errors in scintigraphy imaging time or interpretation, errors in biopsy sampling or pathological diagnosis, deposits of proteins other than TTR (e.g. AL), and ATTRv‐CM with a low sensitivity in 99mTc‐PYP scintigraphy (Table 3 ).
Table 2.
Typical false‐positive and false‐negative cases in planar 99mTc‐PYP scintigraphy for the diagnosis of ATTR‐CM
| Planar 99mTc‐PYP scintigraphy results | Potential causes of false results |
|---|---|
| False positive |
|
| False negative |
|
A positive 99mTc‐PYP scintigraphy result refers to Grade 2 (moderate cardiac uptake equal to rib uptake) or Grade 3 (high cardiac uptake greater than rib uptake), and a negative result refers to Grade 0 (no cardiac uptake) or Grade 1 (mild cardiac uptake less than rib uptake).
99mTc‐PYP, 99mtechnetium‐pyrophosphate; Aβ2M, β2‐microglobulin amyloidosis; AApoAI, apolipoprotein AI amyloidosis; AApoAII, apolipoprotein AII amyloidosis; AApoAIV, apolipoprotein A‐IV amyloidosis; AL, light chain; ATTR‐CM, transthyretin amyloid cardiomyopathy; ATTRv‐CM, variant ATTR‐CM.
Table 3.
Potential causes of inconsistencies between planar 99mTc‐PYP scintigraphy and biopsy findings in suspected ATTR‐CM
| Planar 99mTc‐PYP scintigraphy | Biopsy | Potential causes of inconsistencies |
|---|---|---|
| Positive | Negative |
|
| Negative | Positive |
|
A positive 99mTc‐PYP scintigraphy result refers to Grade 2 (moderate cardiac uptake equal to rib uptake) or Grade 3 (high cardiac uptake greater than rib uptake), and a negative result refers to Grade 0 (no cardiac uptake) or Grade 1 (mild cardiac uptake less than rib uptake).
99mTc‐PYP, 99mtechnetium‐pyrophosphate; AL, light chain; ATTR‐CM, transthyretin amyloid cardiomyopathy; ATTRv‐CM, variant ATTR‐CM.
Guide for appropriate implementation of 99mTc‐PYP scintigraphy in daily clinical practice
For appropriate implementation of 99mTc‐PYP scintigraphy, in addition to planar imaging, SPECT or SPECT/CT fusion imaging is necessary to differentiate myocardial uptake from blood pools or overlying bone uptake. 6 , 7 A standardized protocol (practice points document) for planar 99mTc‐PYP scintigraphy and SPECT data acquisition has been published by the ASNC. 35 In brief, the dose of 99mTc‐PYP intravenous injection is set at 10–20 mCi, a rest scan is recommended for data acquisition, and the time between 99mTc‐PYP injection and data acquisition is set at 1 or 3 h. 35 If persistent blood pool activity is noted on 1‐h SPECT and planar images, 3‐h images may also be obtained. 35
Future perspectives
Recent clinical research has positioned 99mTc‐labelled bone radiotracer scintigraphy as a highly sensitive and specific diagnostic tool for ATTR‐CM and suggests its potential as a quantitative diagnostic tool for ATTR‐CM. For example, the use of quantitative metrics for 99mTc‐PYP imaging (SPECT/CT or SPECT) showed a higher diagnostic accuracy compared with the traditional visual grading approach 82 , 83 as well as its potential as a non‐invasive marker for prognosis. 83 Nevertheless, challenges remain in terms of appropriate implementation of this technique in daily clinical practice. A low level of familiarity with 99mTc‐labelled bone radiotracer scintigraphy 18 and standardization of imaging procedures, such as tracer compound dose, time from injection to imaging, and data interpretation and quantification, 19 are challenges that need to be overcome by cardiologists. Despite its high sensitivity and specificity, 99mTc‐labelled bone radiotracer scintigraphy is not suitable to form a diagnosis of ATTR‐CM as a stand‐alone technique, and exclusion of monoclonal protein components through a careful haematological assessment is required for a definitive diagnosis to avoid misdiagnosis and inappropriate treatment. 6 , 7 , 10 Moreover, research is warranted to elaborate the mechanism of myocardial 99mTc‐labelled tracer uptake in patients with ATTR‐CM. 57 , 84 Lastly, the cost‐effectiveness of 99mTc‐labelled bone radiotracer scintigraphy needs further investigation in the era of treatment with DMTs. 85 , 86
Conclusions
The ATTR‐CM remains an under‐recognized disease owing to its non‐specific clinical manifestation. Cardiac changes are not disease specific, which makes differential diagnosis challenging. Awareness of the disease has been low, but is expected to increase with advances in the treatment strategy. Moreover, a highly accurate diagnosis is warranted as ATTR‐CM is a progressive and fatal disorder. The introduction of 99mTc‐labelled bone radiotracer scintigraphy as a non‐invasive diagnostic modality with high sensitivity and specificity and the coverage of 99mTc‐PYP scintigraphy by the Japanese health insurance have enabled an early and definitive diagnosis of ATTR‐CM. We anticipate that the clinical scenarios associated with ATTR‐CM and common pitfalls of 99mTc‐PYP scintigraphy imaging discussed in this review will help cardiologists establish an early and accurate diagnosis of ATTR‐CM in daily clinical practice.
Conflict of interest
Nobuhiro Tahara, Jin Endo, and Atsushi Okada have received consulting fees or honoraria from Pfizer Japan Inc. for the submitted work. Olivier Lairez has received consulting fees or honoraria from Pfizer Japan Inc. for the submitted work and reports financial relationships outside of the submitted work with Alnylam, Amicus Therapeutics, Pfizer, Sanofi‐Genzyme, and Takeda. Mitsuharu Ueda has received consulting fees or honoraria, support for travel to meetings, and administrative support for writing assistance, medicines, or equipment from Pfizer Japan Inc. for the submitted work and reports financial relationships outside of the submitted work with Pfizer Japan Inc. and Alnylam Japan Co., Ltd. Tomonori Ishii, Yoshinobu Kitano, Hahn‐Ey Lee, and Eleonora Russo are full‐time employees of Pfizer Japan Inc. Toru Kubo has received consulting fees or honoraria and remuneration for lecture from Pfizer Japan Inc. for the submitted work.
Funding
The conduct of the virtual medical advisory board meeting was supported by Pfizer Japan Inc.
Acknowledgements
Medical writing and editorial assistance for the development of this manuscript was provided by Mami Hirano, MS, of Cactus Life Sciences (part of Cactus Communications) and funded by Pfizer Japan Inc.
Tahara, N. , Lairez, O. , Endo, J. , Okada, A. , Ueda, M. , Ishii, T. , Kitano, Y. , Lee, H.‐E. , Russo, E. , and Kubo, T. (2022) 99mTechnetium‐pyrophosphate scintigraphy: a practical guide for early diagnosis of transthyretin amyloid cardiomyopathy. ESC Heart Failure, 9: 251–262. 10.1002/ehf2.13693.
References
- 1. Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. Lancet 2016; 387: 2641–2654. [DOI] [PubMed] [Google Scholar]
- 2. Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy: JACC state‐of‐the‐art review. J Am Coll Cardiol 2019; 73: 2872–2891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Ruberg FL, Berk JL. Transthyretin (TTR) cardiac amyloidosis. Circulation 2012; 126: 1286–1300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28: 10–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rapezzi C, Lorenzini M, Longhi S, Milandri A, Gagliardi C, Bartolomei I, Salvi F, Maurer MS. Cardiac amyloidosis: the great pretender. Heart Fail Rev 2015; 20: 117–124. [DOI] [PubMed] [Google Scholar]
- 6. Kitaoka H, Izumi C, Izumiya Y, Inomata T, Ueda M, Kubo T, Koyama J, Sano M, Sekijima Y, Tahara N, Tsukada N, Tsujita K, Tsutsui H, Tomita T, Amano M, Endo J, Okada A, Oda S, Takashio S, Baba Y, Misumi Y, Yazaki M, Anzai T, Ando Y, Isobe M, Kimura T, Fukuda K, Japanese Circulation Society Joint Working Group . JCS 2020 guideline on diagnosis and treatment of cardiac amyloidosis. Circ J 2020; 84: 1610–1671. [DOI] [PubMed] [Google Scholar]
- 7. Dorbala S, Ando Y, Bokhari S, Dispenzieri A, Falk RH, Ferrari VA, Fontana M, Gheysens O, Gillmore JD, Glaudemans AWJM, Hanna MA, Hazenberg BPC, Kristen AV, Kwong RY, Maurer MS, Merlini G, Miller EJ, Moon JC, Murthy VL, Quarta CC, Rapezzi C, Ruberg FL, Shah SJ, Slart RHJA, Verberne HJ, Bourque JM. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: part 1 of 2–evidence base and standardized methods of imaging. J Nucl Cardiol 2019; 26: 2065–2123. [DOI] [PubMed] [Google Scholar]
- 8. Maurer MS, Bokhari S, Damy T, Dorbala S, Drachman BM, Fontana M, Grogan M, Kristen AV, Lousada I, Nativi‐Nicolau J, Quarta CC, Rapezzi C, Ruberg FL, Witteles R, Merlini G. Expert consensus recommendations for the suspicion and diagnosis of transthyretin cardiac amyloidosis. Circ Heart Fail 2019; 12: e006075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Gertz M, Adams D, Ando Y, Beirão JM, Bokhari S, Coelho T, Comenzo RL, Damy T, Dorbala S, Drachman BM, Fontana M, Gillmore JD, Grogan M, Hawkins PN, Lousada I, Kristen AV, Ruberg FL, Suhr OB, Maurer MS, Nativi‐Nicolau J, Quarta CC, Rapezzi C, Witteles R, Merlini G. Avoiding misdiagnosis: expert consensus recommendations for the suspicion and diagnosis of transthyretin amyloidosis for the general practitioner. BMC Fam Pract 2020; 21: 198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Garcia‐Pavia P, Rapezzi C, Adler Y, Arad M, Basso C, Brucato A, Burazor I, Caforio ALP, Damy T, Eriksson U, Fontana M, Gillmore JD, Gonzalez‐Lopez E, Grogan M, Heymans S, Imazio M, Kindermann I, Kristen AV, Maurer MS, Merlini G, Pantazis A, Pankuweit S, Rigopoulos AG, Linhart A. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2021; 42: 1554–1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Japanese Circulation Society . Notification of approval of 99mTc‐PYP scintigraphy for the diagnosis of transthyretin cardiac amyloidosis (10 November 2020, website in Japanese). https://www.j‐circ.or.jp/topics/99tc_pyp/ (11 March 2021).
- 12. Kittleson MM, Maurer MS, Ambardekar AV, Bullock‐Palmer RP, Chang PP, Eisen HJ, Nair AP, Nativi‐Nicolau J, Ruberg FL, American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology . Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation 2020; 142: e7–e22. [DOI] [PubMed] [Google Scholar]
- 13. Lane T, Fontana M, Martinez‐Naharro A, Quarta CC, Whelan CJ, Petrie A, Rowczenio DM, Gilbertson JA, Hutt DF, Rezk T, Strehina SG, Caringal‐Galima J, Manwani R, Sharpley FA, Wechalekar AD, Lachmann HJ, Mahmood S, Sachchithanantham S, Drage EPS, Jenner HD, McDonald R, Bertolli O, Calleja A, Hawkins PN, Gillmore JD. Natural history, quality of life, and outcome in cardiac transthyretin amyloidosis. Circulation 2019; 140: 16–26. [DOI] [PubMed] [Google Scholar]
- 14. González‐López E, Gallego‐Delgado M, Guzzo‐Merello G, de Haro‐Del Moral FJ, Cobo‐Marcos M, Robles C, Bornstein B, Salas C, Lara‐Pezzi E, Alonso‐Pulpon L, Garcia‐Pavia P. Wild‐type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J 2015; 36: 2585–2594. [DOI] [PubMed] [Google Scholar]
- 15. Longhi S, Lorenzini M, Gagliardi C, Milandri A, Marzocchi A, Marrozzini C, Saia F, Ortolani P, Biagini E, Guidalotti PL, Leone O, Rapezzi C. Coexistence of degenerative aortic stenosis and wild‐type transthyretin‐related cardiac amyloidosis. JACC Cardiovasc Imaging 2016; 9: 325–327. [DOI] [PubMed] [Google Scholar]
- 16. Damy T, Costes B, Hagège AA, Donal E, Eicher JC, Slama M, Guellich A, Rappeneau S, Gueffet JP, Logeart D, Planté‐Bordeneuve V, Bouvaist H, Huttin O, Mulak G, Dubois‐Randé JL, Goossens M, Canoui‐Poitrine F, Buxbaum JN. Prevalence and clinical phenotype of hereditary transthyretin amyloid cardiomyopathy in patients with increased left ventricular wall thickness. Eur Heart J 2016; 37: 1826–1834. [DOI] [PubMed] [Google Scholar]
- 17. Zampieri M, Nardi G, Del Monaco G, Allinovi M, Gabriele M, Zocchi C, Casagrande S, Fumagalli C, Di Mario C, Olivotto I, Perfetto F, Cappelli F. Changes in the perceived epidemiology of amyloidosis: 20 year‐experience from a tertiary referral centre in Tuscany. Int J Cardiol 2021; 335: 123–127. [DOI] [PubMed] [Google Scholar]
- 18. Mircsof D. Diagnosis of amyloidosis: a survey of current awareness and clinical challenges among cardiologists in Switzerland. Cardiol Ther 2020; 9: 127–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Harb SC, Haq M, Flood K, Guerrieri A, Passerell W, Jaber WA, Miller EJ. National patterns in imaging utilization for diagnosis of cardiac amyloidosis: a focus on Tc99m‐pyrophosphate scintigraphy. J Nucl Cardiol 2017; 24: 1094–1097. [DOI] [PubMed] [Google Scholar]
- 20. Sekijima Y, Ueda M, Koike H, Misawa S, Ishii T, Ando Y. Diagnosis and management of transthyretin familial amyloid polyneuropathy in Japan: red‐flag symptom clusters and treatment algorithm. Orphanet J Rare Dis 2018; 13: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Rapezzi C, Quarta CC, Obici L, Perfetto F, Longhi S, Salvi F, Biagini E, Lorenzini M, Grigioni F, Leone O, Cappelli F, Palladini G, Rimessi P, Ferlini A, Arpesella G, Pinna AD, Merlini G, Perlini S. Disease profile and differential diagnosis of hereditary transthyretin‐related amyloidosis with exclusively cardiac phenotype: an Italian perspective. Eur Heart J 2013; 34: 520–528. [DOI] [PubMed] [Google Scholar]
- 22. Papoutsidakis N, Miller EJ, Rodonski A, Jacoby D. Time course of common clinical manifestations in patients with transthyretin cardiac amyloidosis: delay from symptom onset to diagnosis. J Card Fail 2018; 24: 131–133. [DOI] [PubMed] [Google Scholar]
- 23. Shiozaki T, Sato N, Hayashi T, Kobayashi K, Asamura H. Wild‐type ATTR amyloidosis may be associated with unexpected death among the elderly. Leg Med (Tokyo) 2019; 41: 101634. [DOI] [PubMed] [Google Scholar]
- 24. Ueda M, Horibata Y, Shono M, Misumi Y, Oshima T, Su Y, Tasaki M, Shinriki S, Kawahara S, Jono H, Obayashi K, Ogawa H, Ando Y. Clinicopathological features of senile systemic amyloidosis: an ante‐ and post‐mortem study. Mod Pathol 2011; 24: 1533–1544. [DOI] [PubMed] [Google Scholar]
- 25. Tanskanen M, Peuralinna T, Polvikoski T, Notkola IL, Sulkava R, Hardy J, Singleton A, Kiuru‐Enari S, Paetau A, Tienari PJ, Myllykangas L. Senile systemic amyloidosis affects 25% of the very aged and associates with genetic variation in alpha2‐macroglobulin and tau: a population‐based autopsy study. Ann Med 2008; 40: 232–239. [DOI] [PubMed] [Google Scholar]
- 26. Krishnappa D, Dykoski R, Can I, Mbai M, Anand IS, Florea V, Chandrashekar YS, Li JM, Tholakanahalli VN. Atrial fibrillation in the elderly: the role of sub‐clinical isolated cardiac amyloidosis. Sci Rep 2019; 9: 16584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Castaño A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, Rubin J, Chiuzan C, Nazif T, Vahl T, George I, Kodali S, Leon MB, Hahn R, Bokhari S, Maurer MS. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J 2017; 38: 2879–2887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Yamada T, Takashio S, Arima Y, Nishi M, Morioka M, Hirakawa K, Hanatani S, Fujisue K, Yamanaga K, Kanazawa H, Sueta D, Araki S, Usuku H, Nakamura T, Suzuki S, Yamamoto E, Ueda M, Kaikita K, Tsujita K. Clinical characteristics and natural history of wild‐type transthyretin amyloid cardiomyopathy in Japan. ESC Heart Fail 2020; 7: 2829–2837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Connors LH, Doros G, Sam F, Badiee A, Seldin DC, Skinner M. Clinical features and survival in senile systemic amyloidosis: comparison to familial transthyretin cardiomyopathy. Amyloid 2011; 18(Suppl 1): 157–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Connors LH, Sam F, Skinner M, Salinaro F, Sun F, Ruberg FL, Berk JL, Seldin DC. Heart failure resulting from age‐related cardiac amyloid disease associated with wild‐type transthyretin: a prospective, observational cohort study. Circulation 2016; 133: 282–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Canepa M, Tini G, Musumeci B, Cappelli F, Milandri A, Mussinelli R, Autore C, Perfetto F, Rapezzi C, Perlini S. Real‐world versus trial patients with transthyretin amyloid cardiomyopathy. Eur J Heart Fail 2019; 21: 1479–1481. [DOI] [PubMed] [Google Scholar]
- 32. Castano A, Haq M, Narotsky DL, Goldsmith J, Weinberg RL, Morgenstern R, Pozniakoff T, Ruberg FL, Miller EJ, Berk JL, Dispenzieri A, Grogan M, Johnson G, Bokhari S, Maurer MS. Multicenter study of planar technetium 99m pyrophosphate cardiac imaging: predicting survival for patients with ATTR cardiac amyloidosis. JAMA Cardiol 2016; 1: 880–889. [DOI] [PubMed] [Google Scholar]
- 33. Minutoli F, Di Bella G, Mazzeo A, Laudicella R, Gentile L, Russo M, Vita G, Baldari S. Serial scanning with 99mTc‐3, 3‐diphosphono‐1, 2‐propanodicarboxylic acid (99mTc‐DPD) for early detection of cardiac amyloid deposition and prediction of clinical worsening in subjects carrying a transthyretin gene mutation. J Nucl Cardiol 2019; 10.1007/s12350-019-01950-2. Published online ahead of print 18 November 2019. [DOI] [PubMed] [Google Scholar]
- 34. Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, Wechalekar AD, Berk JL, Quarta CC, Grogan M, Lachmann HJ, Bokhari S, Castano A, Dorbala S, Johnson GB, Glaudemans AW, Rezk T, Fontana M, Palladini G, Milani P, Guidalotti PL, Flatman K, Lane T, Vonberg FW, Whelan CJ, Moon JC, Ruberg FL, Miller EJ, Hutt DF, Hazenberg BP, Rapezzi C, Hawkins PN. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation 2016; 133: 2404–2412. [DOI] [PubMed] [Google Scholar]
- 35. American Society of Nuclear Cardiology . ASNC cardiac amyloidosis practice points: 99mtechnetium‐pyrophosphate imaging for transthyretin cardiac amyloidosis (version 2.0, updated February 2019). https://www.asnc.org/cardiacamyloidosis (11 March 2021).
- 36. Banypersad SM. The evolving role of cardiovascular magnetic resonance imaging in the evaluation of systemic amyloidosis. Magn Reson Insights 2019; 12: 1178623x19843519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bennani Smires Y, Victor G, Ribes D, Berry M, Cognet T, Méjean S, Huart A, Roussel M, Petermann A, Roncalli J, Carrié D, Rousseau H, Berry I, Chauveau D, Galinier M, Lairez O. Pilot study for left ventricular imaging phenotype of patients over 65 years old with heart failure and preserved ejection fraction: the high prevalence of amyloid cardiomyopathy. Int J Cardiovasc Imaging 2016; 32: 1403–1413. [DOI] [PubMed] [Google Scholar]
- 38. Grogan M, Dispenzieri A, Gertz MA. Light‐chain cardiac amyloidosis: strategies to promote early diagnosis and cardiac response. Heart 2017; 103: 1065–1072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Martinez‐Naharro A, Treibel TA, Abdel‐Gadir A, Bulluck H, Zumbo G, Knight DS, Kotecha T, Francis R, Hutt DF, Rezk T, Rosmini S, Quarta CC, Whelan CJ, Kellman P, Gillmore JD, Moon JC, Hawkins PN, Fontana M. Magnetic resonance in transthyretin cardiac amyloidosis. J Am Coll Cardiol 2017; 70: 466–477. [DOI] [PubMed] [Google Scholar]
- 40. Fontana M, Banypersad SM, Treibel TA, Maestrini V, Sado DM, White SK, Pica S, Castelletti S, Piechnik SK, Robson MD, Gilbertson JA, Rowczenio D, Hutt DF, Lachmann HJ, Wechalekar AD, Whelan CJ, Gillmore JD, Hawkins PN, Moon JC. Native T1 mapping in transthyretin amyloidosis. JACC Cardiovasc Imaging 2014; 7: 157–165. [DOI] [PubMed] [Google Scholar]
- 41. Oda S, Utsunomiya D, Morita K, Nakaura T, Yuki H, Kidoh M, Hirata K, Taguchi N, Tsuda N, Shiraishi S, Namimoto T, Hirakawa K, Takashio S, Izumiya Y, Yamamuro M, Hokimoto S, Tsujita K, Ueda M, Yamashita T, Ando Y, Yamashita Y. Cardiovascular magnetic resonance myocardial T1 mapping to detect and quantify cardiac involvement in familial amyloid polyneuropathy. Eur Radiol 2017; 27: 4631–4638. [DOI] [PubMed] [Google Scholar]
- 42. Perez‐Rodriguez J, Lai S, Ehst BD, Fine DM, Bluemke DA. Nephrogenic systemic fibrosis: incidence, associations, and effect of risk factor assessment—report of 33 cases. Radiology 2009; 250: 371–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Damy T, Maurer MS, Rapezzi C, Planté‐Bordeneuve V, Karayal ON, Mundayat R, Suhr OB, Kristen AV. Clinical, ECG and echocardiographic clues to the diagnosis of TTR‐related cardiomyopathy. Open Heart 2016; 3: e000289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Hanna M, Ruberg FL, Maurer MS, Dispenzieri A, Dorbala S, Falk RH, Hoffman J, Jaber W, Soman P, Witteles RM, Grogan M. Cardiac scintigraphy with technetium‐99m‐labeled bone‐seeking tracers for suspected amyloidosis: JACC review topic of the week. J Am Coll Cardiol 2020; 75: 2851–2862. [DOI] [PubMed] [Google Scholar]
- 45. Treglia G, Glaudemans AWJM, Bertagna F, Hazenberg BPC, Erba PA, Giubbini R, Ceriani L, Prior JO, Giovanella L, Slart RHJA. Diagnostic accuracy of bone scintigraphy in the assessment of cardiac transthyretin‐related amyloidosis: a bivariate meta‐analysis. Eur J Nucl Med Mol Imaging 2018; 45: 1945–1955. [DOI] [PubMed] [Google Scholar]
- 46. Einstein AJ, Shuryak I, Castaño A, Mintz A, Maurer MS, Bokhari S. Estimating cancer risk from 99mTc pyrophosphate imaging for transthyretin cardiac amyloidosis. J Nucl Cardiol 2020; 27: 215–224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Mohamed‐Salem L, Santos‐Mateo JJ, Sanchez‐Serna J, Hernández‐Vicente Á, Reyes‐Marle R, Castellón Sánchez MI, Claver‐Valderas MA, Gonzalez‐Vioque E, Haro‐Del Moral FJ, García‐Pavía P, Pascual‐Figal DA. Prevalence of wild type ATTR assessed as myocardial uptake in bone scan in the elderly population. Int J Cardiol 2018; 270: 192–196. [DOI] [PubMed] [Google Scholar]
- 48. Longhi S, Guidalotti PL, Quarta CC, Gagliardi C, Milandri A, Lorenzini M, Potena L, Leone O, Bartolomei I, Pastorelli F, Salvi F, Rapezzi C. Identification of TTR‐related subclinical amyloidosis with 99mTc‐DPD scintigraphy. JACC Cardiovasc Imaging 2014; 7: 531–532. [DOI] [PubMed] [Google Scholar]
- 49. Kim HM, Sohn DW, Paeng JC. Prevalence of positive 99 mTc‐DPD scintigraphy as an indicator of the prevalence of wild‐type transthyretin amyloidosis in the elderly. Int Heart J 2019; 60: 643–647. [DOI] [PubMed] [Google Scholar]
- 50. Cuscaden C, Ramsay SC, Prasad S, Goodwin B, Smith J. Estimation of prevalence of transthyretin (ATTR) cardiac amyloidosis in an Australian subpopulation using bone scans with echocardiography and clinical correlation. J Nucl Cardiol 2020; 10.1007/s12350-020-02152-x. Published online ahead of print 8 May 2020. [DOI] [PubMed] [Google Scholar]
- 51. Sperry BW, Burgett E, Bybee KA, McGhie AI, O'Keefe JH, Saeed IM, Thompson RC, Bateman TM. Technetium pyrophosphate nuclear scintigraphy for cardiac amyloidosis: imaging at 1 vs 3 hours and planar vs SPECT/CT. J Nucl Cardiol 2020; 27: 1802–1807. [DOI] [PubMed] [Google Scholar]
- 52. Singh V, Falk R, Di Carli MF, Kijewski M, Rapezzi C, Dorbala S. State‐of‐the‐art radionuclide imaging in cardiac transthyretin amyloidosis. J Nucl Cardiol 2019; 26: 158–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Régis C, Harel F, Martineau P, Grégoire J, Abikhzer G, Juneau D, Pelletier‐Galarneau M. Tc‐99m‐pyrophosphate scintigraphy for the diagnosis of ATTR cardiac amyloidosis: comparison of quantitative and semi‐quantitative approaches. J Nucl Cardiol 2020; 27: 1808–1815. [DOI] [PubMed] [Google Scholar]
- 54. Wehbe RM, Kansal P, Holly TA. Cases from a busy nuclear cardiology laboratory: potential pitfalls in the interpretation of cardiac scintigraphy for ATTR cardiac amyloidosis. J Nucl Cardiol 2021; 28: 653–660. [DOI] [PubMed] [Google Scholar]
- 55. Fine NM, Arruda‐Olson AM, Dispenzieri A, Zeldenrust SR, Gertz MA, Kyle RA, Swiecicki PL, Scott CG, Grogan M. Yield of noncardiac biopsy for the diagnosis of transthyretin cardiac amyloidosis. Am J Cardiol 2014; 113: 1723–1727. [DOI] [PubMed] [Google Scholar]
- 56. Quarta CC, Gonzalez‐Lopez E, Gilbertson JA, Botcher N, Rowczenio D, Petrie A, Rezk T, Youngstein T, Mahmood S, Sachchithanantham S, Lachmann HJ, Fontana M, Whelan CJ, Wechalekar AD, Hawkins PN, Gillmore JD. Diagnostic sensitivity of abdominal fat aspiration in cardiac amyloidosis. Eur Heart J 2017; 38: 1905–1908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Tsutsui Y, Kubota T, Kato S, Nozoe M, Suematsu N, Okabe M, Yamamoto Y, Tsutsui H. Utility of 99mTc‐pyrophosphate scintigraphy in diagnosing transthyretin cardiac amyloidosis in real‐world practice. Circ Rep 2019; 1: 277–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Rapezzi C, Merlini G, Quarta CC, Riva L, Longhi S, Leone O, Salvi F, Ciliberti P, Pastorelli F, Biagini E, Coccolo F, Cooke RM, Bacchi‐Reggiani L, Sangiorgi D, Ferlini A, Cavo M, Zamagni E, Fonte ML, Palladini G, Salinaro F, Musca F, Obici L, Branzi A, Perlini S. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation 2009; 120: 1203–1212. [DOI] [PubMed] [Google Scholar]
- 59. Donnellan E, Wazni OM, Saliba WI, Hanna M, Kanj M, Patel DR, Wilner B, Kochar A, Jaber WA. Prevalence, incidence, and impact on mortality of conduction system disease in transthyretin cardiac amyloidosis. Am J Cardiol 2020; 128: 140–146. [DOI] [PubMed] [Google Scholar]
- 60. Phelan D, Collier P, Thavendiranathan P, Popović ZB, Hanna M, Plana JC, Marwick TH, Thomas JD. Relative apical sparing of longitudinal strain using two‐dimensional speckle‐tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart 2012; 98: 1442–1448. [DOI] [PubMed] [Google Scholar]
- 61. Arvidsson S, Henein MY, Wikström G, Suhr OB, Lindqvist P. Right ventricular involvement in transthyretin amyloidosis. Amyloid 2018; 25: 160–166. [DOI] [PubMed] [Google Scholar]
- 62. Takashio S, Yamamuro M, Izumiya Y, Hirakawa K, Marume K, Yamamoto M, Ueda M, Yamashita T, Ishibashi‐Ueda H, Yasuda S, Ogawa H, Ando Y, Anzai T, Tsujita K. Diagnostic utility of cardiac troponin T level in patients with cardiac amyloidosis. ESC Heart Fail 2018; 5: 27–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Ochi Y, Kubo T, Nakashima Y, Baba Y, Hirota T, Yamasaki N, Yamashita T, Ueda M, Ando Y, Kitaoka H. Integrated diagnostic approach to wild‐type transthyretin cardiac amyloidosis with the use of high‐sensitivity cardiac troponin T measurement and 99mTc‐pyrophosphate scintigraphy. J Cardiol 2020; 75: 12–19. [DOI] [PubMed] [Google Scholar]
- 64. Sueyoshi T, Ueda M, Jono H, Irie H, Sei A, Ide J, Ando Y, Mizuta H. Wild‐type transthyretin‐derived amyloidosis in various ligaments and tendons. Hum Pathol 2011; 42: 1259–1264. [DOI] [PubMed] [Google Scholar]
- 65. Vianello PF, La Malfa G, Tini G, Mazzola V, Miceli A, Santolini E, Briano S, Porto I, Canepa M. Prevalence of transthyretin amyloid cardiomyopathy in male patients who underwent bilateral carpal tunnel surgery: the ACTUAL study. Int J Cardiol 2021; 329: 144–147. [DOI] [PubMed] [Google Scholar]
- 66. Marume K, Takashio S, Nishi M, Hirakawa K, Yamamoto M, Hanatani S, Oda S, Utsunomiya D, Shiraishi S, Ueda M, Yamashita T, Sakamoto K, Yamamoto E, Kaikita K, Izumiya Y, Yamashita Y, Ando Y, Tsujita K. Combination of commonly examined parameters is a useful predictor of positive 99mTc‐labeled pyrophosphate scintigraphy findings in elderly patients with suspected transthyretin cardiac amyloidosis. Circ J 2019; 83: 1698–1708. [DOI] [PubMed] [Google Scholar]
- 67. Ochi Y, Kubo T, Baba Y, Ueda M, Miyagawa K, Noguchi T, Hirota T, Yamasaki N, Kitaoka H. Validation of the Kumamoto criteria for prediction of 99mtechnetium pyrophosphate scintigraphy positivity as a strategy for diagnosis of transthyretin cardiac amyloidosis: a retrospective cohort study in Kochi. J Cardiol 2021; 77: 124–130. [DOI] [PubMed] [Google Scholar]
- 68. Endo J, Sano M, Izumiya Y, Tsujita K, Nakamura K, Tahara N, Kuwahara K, Inomata T, Ueda M, Sekijima Y, Ando Y, Tsutsui H, Isobe M, Fukuda K. A statement on the appropriate administration of tafamidis in patients with transthyretin cardiac amyloidosis. Circ J 2019; 84: 15–17. [DOI] [PubMed] [Google Scholar]
- 69. Quarta CC, Zheng J, Hutt D, Grigore SF, Manwani R, Sachchithanantham S, Mahmood SA, Whelan CJ, Fontana M, Martinez‐Naharro A, Chacko L, Lachmann HJ, Gillmore JD, Rapezzi C, Hawkins PN, Wechalekar AD. 99mTc‐DPD scintigraphy in immunoglobulin light chain (AL) cardiac amyloidosis. Eur Heart J Cardiovasc Imaging 2021; 22: 1304–1311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Persia‐Paulino YR, Cuevas‐Perez J, Fernandez‐Asensio R, Junco‐Vicente A, Rozado‐Castano J, Colunga S, Cigarran H, Calvo J, Laverde A, Persia O, Capin‐Sampedro E. Unusual high 99mTc‐3,3‐diphosphono‐1,2‐propanodicarboxylic acid (99mTc‐DPD) tracer deposition on a heart scintigraphy in a patient with AL amyloidosis: a case report. J Nucl Cardiol 2021; 28: 1117–1125. [DOI] [PubMed] [Google Scholar]
- 71. Zeng Y, Poterucha TJ, Einstein AJ, Zhang Q, Chen Y, Xie H, Wan K, Liang Y, Chen J, Tang G. False positive technetium‐99m pyrophosphate scintigraphy in a patient with cardiac amyloidosis light chain: case report. Medicine (Baltimore) 2021; 100: e25582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. de Miguel C, Llorente L, de Haro‐del Moral FJ, García‐Pavía P, González‐López E, Segovia J, Krsnik I. Myocardial uptake of 99mTc‐DPD in patients with AL amyloidosis. Amyloid 2017; 24(Suppl 1): 48–49. [DOI] [PubMed] [Google Scholar]
- 73. Okada A, Tateishi E, Ohta‐Ogo K, Izumi C. Grade 3 myocardial uptake in 99mtechnetium‐pyrophosphate scintigraphy in light chain cardiac amyloidosis. Eur Heart J Case Rep 2021; 5: ytab321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Schafer EB, Tushak Z, Trankle CR, Rao K, Cartagena LC, Shah KB. False‐positive 99mtechnetium‐pyrophosphate scintigraphy in two patients with hypertrophic cardiomyopathy. Circ Heart Fail 2021; 14: e007558. [DOI] [PubMed] [Google Scholar]
- 75. Chimenti C, Alfarano M, Maestrini V, Galea N, De Vincentis G, Verardo R, Fedele F, Frustaci A. False‐positive bone scintigraphy denoting transthyretin amyloid in elderly hypertrophic cardiomyopathy. ESC Heart Fail 2021; 8: 3387–3391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Chang ICY, Bois JP, Bois MC, Maleszewski JJ, Johnson GB, Grogan M. Hydroxychloroquine‐mediated cardiotoxicity with a false‐positive 99mtechnetium‐labeled pyrophosphate scan for transthyretin‐related cardiac amyloidosis. Circ Cardiovasc Imaging 2018; 11: e007059. [DOI] [PubMed] [Google Scholar]
- 77. Shin E, Oh M, Sung C, Kim KH, Ryu JS. Altered biodistribution of 99mTc‐DPD on bone scan after intravenous iron supplement. Nucl Med Mol Imaging 2017; 51: 347–349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Lades G, Carpenet H, Benoit U, Aboyans V, Monteil J. Tc‐99m HMDP bone scintigraphy for cardiac amyloidosis diagnosis: a false positive case. J Nucl Cardiol 2021; 10.1007/s12350-020-02451-3. Published online ahead of print 3 January 2021. [DOI] [PubMed] [Google Scholar]
- 79. Grigoratos C, Aimo A, Rapezzi C, Genovesi D, Barison A, Aquaro GD, Vergaro G, Pucci A, Passino C, Marzullo P, Gimelli A, Emdin M. Diphosphonate single‐photon emission computed tomography in cardiac transthyretin amyloidosis. Int J Cardiol 2020; 307: 187–192. [DOI] [PubMed] [Google Scholar]
- 80. Musumeci MB, Cappelli F, Russo D, Tini G, Canepa M, Milandri A, Bonfiglioli R, Di Bella G, My F, Luigetti M, Grandis M, Autore C, Perlini S, Perfetto F, Rapezzi C. Low sensitivity of bone scintigraphy in detecting Phe64Leu mutation‐related transthyretin cardiac amyloidosis. JACC Cardiovasc Imaging 2020; 13: 1314–1321. [DOI] [PubMed] [Google Scholar]
- 81. Ochi Y, Kubo T, Nakashima Y, Takahashi A, Baba Y, Hirota T, Yamasaki N, Kitaoka H. A case report of an uncommon presentation of 99mtechnetium pyrophosphate scintigraphy in transthyretin cardiac amyloidosis: a potential diagnostic pitfall, pseudo‐positive or pseudo‐negative? J Cardiol Cases 2020; 21: 50–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Dorbala S, Park MA, Cuddy S, Singh V, Sullivan K, Kim S, Falk RH, Taqueti VR, Skali H, Blankstein R, Bay C, Kijewski MF, Di Carli MF. Absolute quantitation of cardiac 99mTc‐pyrophosphate using cadmium‐zinc‐telluride‐based SPECT/CT. J Nucl Med 2021; 62: 716–722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Miller RJH, Cadet S, Mah D, Pournazari P, Chan D, Fine NM, Berman DS, Slomka PJ. Diagnostic and prognostic value of technetium‐99m pyrophosphate uptake quantitation for transthyretin cardiac amyloidosis. J Nucl Cardiol 2021; 10.1007/s12350-021-02563-4. Published online ahead of print 3 January 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Bravo PE, Dorbala S. Targeted nuclear imaging probes for cardiac amyloidosis. Curr Cardiol Rep 2017; 19: 59. [DOI] [PubMed] [Google Scholar]
- 85. Ruiz‐Negrón N, Nativi‐Nicolau J, Maurer MS, Moran AE, Kovacsovics T, Bellows BK. Cost‐effectiveness of technetium pyrophosphate scintigraphy versus heart biopsy for the diagnosis of transthyretin amyloidosis. Amyloid 2019; 26(Suppl 1): 71–72. [DOI] [PubMed] [Google Scholar]
- 86. Kyriakou P, Mouselimis D, Tsarouchas A, Rigopoulos A, Bakogiannis C, Noutsias M, Vassilikos V. Diagnosis of cardiac amyloidosis: a systematic review on the role of imaging and biomarkers. BMC Cardiovasc Disord 2018; 18: 221. [DOI] [PMC free article] [PubMed] [Google Scholar]