

This nonrandomized controlled trial examines efficacy of vamorolone treatment for Duchenne muscular dystrophy among boys compared with glucocorticoid treatment.
Key Points
Question
Is long-term treatment with vamorolone associated with sustained disease modification and decrease of glucocorticoid-associated adverse outcomes among patients with Duchenne muscular dystrophy (DMD)?
Findings
In this nonrandomized controlled trial of 46 boys with DMD, higher-dose vamorolone treatment for up to 30 months was not associated with a change in time to stand velocity. Vamorolone was associated with continued disease-modification and similar efficacy compared with glucocorticoid treatment from 2 historical control cohorts, and long-term vamorolone treatment was associated with decreased adverse outcomes compared with traditional glucocorticoid therapy.
Meaning
These findings suggest that vamorolone may have potential as a standard of care disease-modifying treatment for boys with DMD.
Abstract
Importance
Vamorolone is a synthetic steroidal drug with potent anti-inflammatory properties. Initial open-label, multiple ascending dose-finding studies of vamorolone among boys with Duchenne muscular dystrophy (DMD) found significant motor function improvement after 6 months treatment in higher-dose (ie, ≥2.0 mg/kg/d) groups.
Objective
To investigate outcomes after 30 months of open-label vamorolone treatment.
Design, Setting, and Participants
This nonrandomized controlled trial was conducted by the Cooperative International Neuromuscular Research Group at 11 US and non-US study sites. Participants were 46 boys ages 4.5 to 7.5 years with DMD who completed the 6-month dose-finding study. Data were analyzed from July 2020 through November 2021.
Interventions
Participants were enrolled in a 24-month, long-term extension (LTE) study with vamorolone dose escalated to 2.0 or 6.0 mg/kg/d.
Main Outcomes and Measures
Change in time-to-stand (TTSTAND) velocity from dose-finding baseline to end of LTE study was the primary outcome. Efficacy assessments included timed function tests, 6-minute walk test, and NorthStar Ambulatory Assessment (NSAA). Participants with DMD treated with glucocorticoids from the Duchenne Natural History Study (DNHS) and NorthStar United Kingdom (NSUK) Network were matched and compared with participants in the LTE study receiving higher doses of vamorolone.
Results
Among 46 boys with DMD who completed the dose-finding study, 41 boys (mean [SD] age, 5.33 [0.96] years) completed the LTE study. Among 21 participants treated with higher-dose (ie, ≥2.0 mg/kg/d) vamorolone consistently throughout the 6-month dose-finding and 24-month LTE studies with data available at 30 months, there was a decrease in mean (SD) TTSTAND velocity from baseline to 30 months (0.206 [0.070] rises/s vs 0.189 (0.124) rises/s), which was not a statistically significant change (−0.011 rises/s; CI, −0.068 to 0.046 rises/s). There were no statistically significant differences between participants receiving higher-dose vamorolone and matched participants in the historical control groups receiving glucocorticoid treatment (75 patients in DNHS and 110 patients in NSUK) over a 2-year period in NSAA total score change (0.22 units vs NSUK; 95% CI, −4.48 to 4.04]; P = .92), body mass index z score change (0.002 vs DNHS SD/mo; 95% CI, −0.006 to 0.010; P = .58), or timed function test change. Vamorolone at doses up to 6.0 mg/kg/d was well tolerated, with 5 of 46 participants discontinuing prematurely and for reasons not associated with study drug. Participants in the DNHS treated with glucocorticoids had significant growth delay in comparison with participants treated with vamorolone who had stable height percentiles (0.37 percentile/mo; 95% CI, 0.23 to 0.52 percentile/mo) over time.
Conclusions and Relevance
This study found that vamorolone treatment was not associated with a change in TTSTAND velocity from baseline to 30 months among boys with DMD aged 4 to 7 years at enrollment. Vamorolone was associated with maintenance of muscle strength and function up to 30 months, similar to standard of care glucocorticoid therapy, and improved height velocity compared with growth deceleration associated with glucocorticoid treatment, suggesting that vamorolone may be an attractive candidate for treatment of DMD.
Trial Registration
ClinicalTrials.gov Identifier: NCT03038399
Introduction
Duchenne muscular dystrophy (DMD) is a rapidly progressive X-linked recessive disease, with symptom onset before age 6 years in boys. It is the most common form of muscular dystrophy in childhood, occurring among 1 in 3600 to 9300 male newborns worldwide.1 The disease is caused by variants in the DMD gene, which codes for the dystrophin protein.2 The lack of dystrophin results in membrane fragility, necrosis, inflammation, and progressive muscle atrophy.3 Aberrant intracellular signaling cascades also contribute to DMD pathophysiology. Upregulated inflammatory gene expression and activated immune cell infiltrates, at least partially mediated by nuclear factor κ light chain enhancer of activated B cells (NF-κB) activation, are evident during early disease stages and play a significant role in disease progression.3,4,5 NF-κB regulates expression of numerous inflammatory genes in immune cells and muscle fibers,6,7,8,9 and the infiltration and activation of these cells can trigger muscle cell death.10,11
Despite scientific advances, the only medications that have consistently demonstrated efficacy in clinical trials for DMD are glucocorticoids (GCs), such as prednisone and deflazacort.12,13,14,15 Most gene-targeted disease-modifying technologies that are currently in development or have been recently approved focus on subsets of dystrophin variants and therefore do not address the unmet need among all individuals with DMD. Moreover, these treatments are prescribed in combination with and not as alternatives to GCs. The adverse outcomes associated with GCs, including weight gain, appearance associated with Cushing syndrome, short stature, behavior changes, low bone density, bone fractures, and cataracts, negatively impact quality of life among individuals with DMD.16 Other GC-associated safety concerns include adrenal suppression, delayed puberty, insulin resistance, and further muscle damage.17,18 The significant adverse growth and development outcomes associated with GCs hinder their routine administration among children aged younger than 2 years, even though earlier administration may be associated with better overall functional outcomes.19,20,21 A current goal of DMD research is to find a variant-independent treatment that matches or exceeds the efficacy of GC with a significantly better adverse outcome profile.
Vamorolone is a first-in-class steroidal anti-inflammatory drug that differs from conventional GCs in lacking an 11β hydroxy-carbonyl group.22 This difference removes a contact site with the target glucocorticoid receptor and significantly alters structure and activity associations.23 Additionally, unlike GC, vamorolone is not a substrate for 11β-hydroxysteroid dehydrogenase regulatory enzymes and is a potent antagonist of the mineralocorticoid receptor.24
A Phase IIa 2-week (VBP15-002, NCT02760264) multiple ascending dose study25 of vamorolone (developmental code name, VBP) among boys with DMD who were GC naive and aged 4 years to less than 7 years was completed in 2017. Based on clinical safety and pharmacodynamic biomarker analysis, vamorolone showed dose-dependent anti-inflammatory activity. Findings from a Phase IIa 24-week (VBP15-003, NCT02760277) open-label dose-finding study26 suggested efficacy of vamorolone treatment at 2.0 and 6.0 mg/kg/d based on motor outcomes. Interim analysis at 18 months of the vamorolone open-label extension study (VBP15-LTE, NCT03038399)27 found ongoing improvement in motor function and a favorable safety profile. Here, we report on the long-term efficacy, safety, and tolerability of vamorolone among boys with DMD who completed the 6-month dose-finding and 24-month long-term extension trials, with a total of up to 30 months of vamorolone treatment.
Methods
This nonrandomized clinical study and all studies contributing patients were approved by ethics committees or institutional review boards as required by the participating international academic clinical recruitment sites. Written informed consent was obtained from parents or legal guardians, and assent was obtained from children recruited into each described trial. This report follows the Transparent Reporting of Evaluations With Nonrandomized Designs (TREND) reporting guideline for nonrandomized studies.
The Cooperative International Neuromuscular Research Group (CINRG) conducted 3 consecutive multicenter open-label vamorolone clinical trials.25,26 Participants were recruited from 11 participating centers in the United States, Canada, United Kingdom, Sweden, Israel, and Australia (Figure 1). The 2-week multiple-ascending-dose study25 enrolled 48 boys (ages 4 to <7 years) with DMD who were GC-naive from June 2016 to October 2017. All participants completed the initial study and were enrolled in a 24-week dose-finding trial26; 2 participants subsequently withdrew for reasons unrelated to the study drug. The remaining 46 participants (ages 4.5-7.5 years) who completed the 6-month dose-finding study were eligible to enroll in a 24-month long-term extension (LTE) study, which started in February 2017 and was completed in April 2020.
Figure 1. Flowchart of Vamorolone Long-term Extension (LTE) Study.
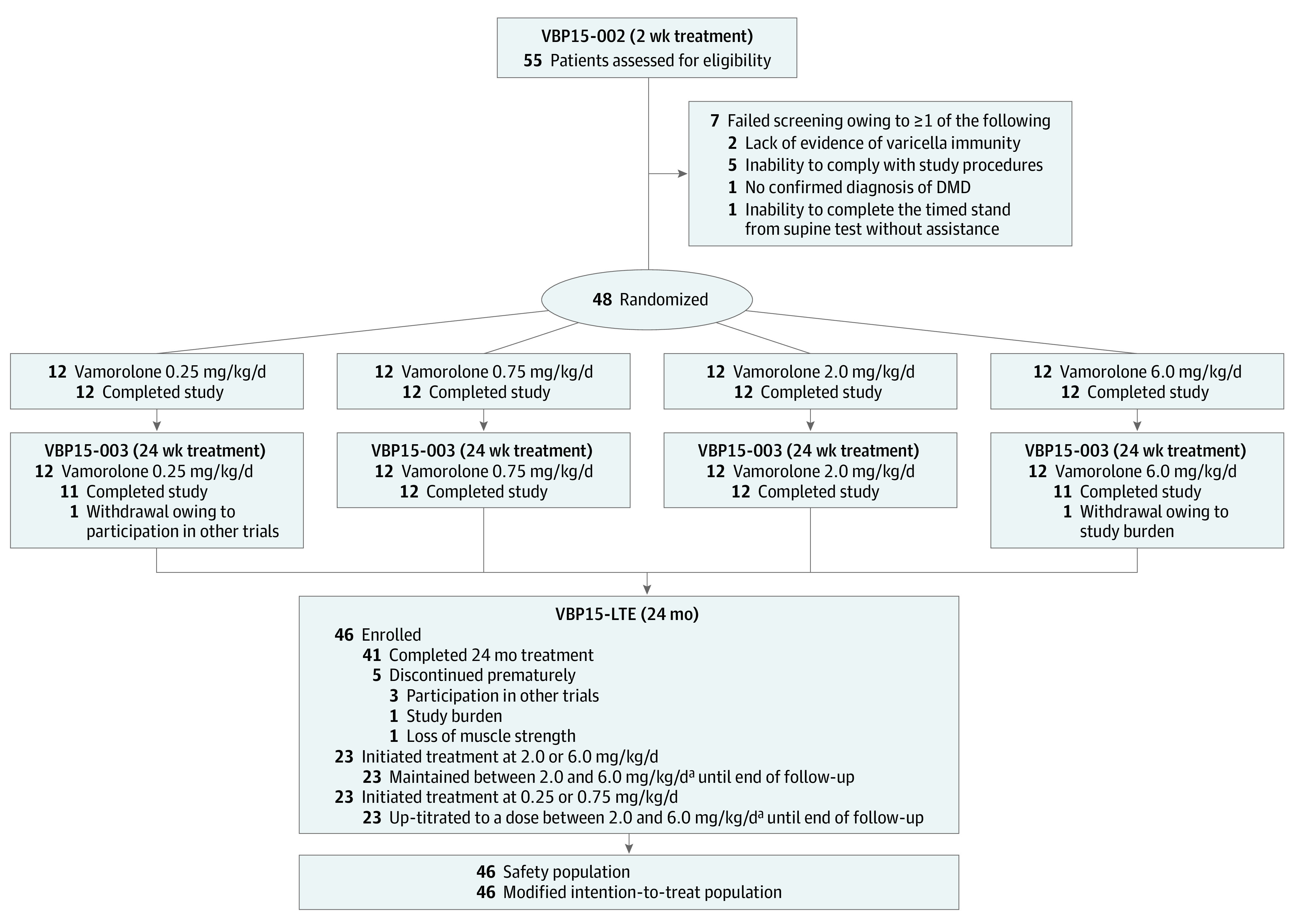
VBP indicates vamorolone.
aTreating physicians were permitted to up-titrate or down-titrate dose according to clinical judgement. There were 3 participants who ended the study at an intermediate dose of 4.0 mg/kg/d.
Study Design
Throughout the studies, vamorolone was provided as a 4% flavored oral suspension taken daily at breakfast with a 240-mL glass of whole milk (approximately 8 g of fat) or equivalent high-fat food portion. Study participants were initially assigned to receive vamorolone at 1 of 4 dose levels (ie, 0.25, 0.75, 2.0, or 6.0 mg/kg/d) (eFigure 1 in Supplement 1) and remained at the same dose level in the 2-week multiple ascending dose and 24-week dose-finding trials. The last visit of the 24-week dose-finding trial coincided with the baseline visit of the 24-month LTE trial. Multiple dose escalations to the highest dose (ie, 6.0 mg/kg/d) were permitted in the LTE protocol (Supplement 2); de-escalations were also allowed in case of intolerability, at the discretion of investigators. Given the variable timing of dose escalations, prespecified analyses of drug-associated efficacy focused on 23 participants who were initially assigned and maintained on a 2.0 mg/kg/d or greater dose of vamorolone (ie, 2 mg/kg/d and 6 mg/kg/d dose groups, hereafter higher-dose groups) for up to 30 months.
Additionally, participants from the CINRG Duchenne Natural History Study (DNHS) treated with GC were selected to serve as a historical control group for timed function tests and anthropometric measurements. The DNHS (NCT00468832) included 440 participants with DMD, with data collected from December 2005 to November 2016.28,29,30 Participants in DNHS were first eligible for inclusion in the control group after they had experienced 6 months of continuous GC exposure, with similar ages (ie, 4.5-7.5 years) as participants in the LTE study who had 6 months of vamorolone exposure at baseline after completing the dose-finding trial. For statistical matching between participants receiving higher-dose vamorolone and those in the DNHS, prespecified criteria (eAppendix 1 in Supplement 1) were defined for coarsened exact matching (CEM).31,32
In addition, participants from the NorthStar United Kingdom (NSUK) Network were selected for inclusion in a second historical control group to allow for comparison of NorthStar Ambulatory Assessment (NSAA) scores, given that NSAA was not assessed for most participants in DNHS. Participants in NSUK33 included in this comparison were recruited from August 2005 to October 2019. Like participants from the DNHS, they were started on GC (any type or dose) for 6 months before the comparison baseline visit, with similar ages (4.5-7.5 years) at baseline compared with participants in the LTE, and were continuously maintained on GC (eAppendix 2 in Supplement 1).
Measurements
Study visits took place quarterly and included clinical and laboratory assessments with adverse event reporting. Standing height and weight were assessed at each study visit; height percentile, body mass index (BMI; calculated as weight in kilograms divided by height in meters squared) and BMI z score were calculated centrally.34 Clinical efficacy evaluations were performed at baseline (ie, multiple ascending dose entry), 6 months (ie, LTE baseline), 18 months (ie, LTE month 12), and 30 months (ie, LTE month 24) of treatment with vamorolone. Assessment of efficacy included timed function tests (ie, time to stand from supine [TTSTAND], time to run or walk 10 m [TTRW], time to climb 4 stairs [TTCLIMB]),35 distance covered in 6-minute walk test (6MWT),36 NSAA score (total NSAA score is made up of the sum of scores on 17 ordinal tests, scored as 0, 1, or 2, with a 2 indicating normal activity with no obvious modification)37 and quantitative muscle testing (QMT) using the CINRG Quantitative Measurement System (measurements in pounds done unilaterally using the dominant side, if known, for each muscle group [ie, knee extension, knee flexion, elbow extension, and elbow flexion]).38 TTSTAND change from the multiple ascending dose study baseline to LTE month 24 was the primary efficacy end point. For TTSTAND, TTRW, and TTCLIMB, results in seconds were converted to velocities (ie, rises per second for TTSTAND, meters per second for TTRW, and tasks per second for TTCLIMB); participants unable to perform tests owing to disease progression had a velocity score imputed as 0.25,26 Clinical evaluators were trained according to operating procedures that were standardized in the NSUK Network33 and vamorolone and DNHS participating centers.39
Patient-reported outcomes and health-related quality of life were assessed by the Pediatric Outcomes Data Collection Instrument (PODCI)40 as an exploratory efficacy end point. The PODCI standardized Upper Extremity and Physical Function score is calculated using at least 4 items with valid nonmissing responses, with a possible range of 0 to 100. The standardized Transfer and Basic Mobility score is calculated using at least 7 items with valid nonmissing response, with a possible range of 0 to 100. Safety measurements included physical exam with weight and height, BMI, clinical laboratory tests, 12-lead electrocardiogram, bone age, lateral thoracolumbar spine x-ray, and adverse event (AE) reporting. All AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA, versions 19.0, 20.1, 21.0, and 21.1) system for reporting. Intensity of AEs was graded using the Common Terminology Criteria for Adverse Events version 4.03.
Statistical Analysis
A statistical analysis plan prespecified the longitudinal within-study (based on paired t test) analyses of motor outcomes, biomarkers, and safety analyses (Supplement 2). Summaries for TTSTAND, TTRW, TTCLIMB, 6MWT, NSAA, and QMT included descriptive statistics on observed values and changes from baseline values at each time.
Comparison of participants in the LTE study receiving higher doses with the historical control group consisting of participants from DNHS receiving GC was based on longitudinal outcome data using a mixed-effect model with repeated measures (MMRM). Owing to NSUK participant-level data sharing restrictions, NSAA data were analyzed separately by NSUK researchers and summaries of change were compared with the higher-dose LTE cohort using independent t tests and a relative risk analysis of NSAA scores.41 Nonparametric maximum likelihood estimation (NPMLE) was used to estimate the observed survival curve (median time to event and bootstrapped CIs) for the first TTSTAND milestone of 10 or more seconds to assess the risk associated with future loss of ambulation for each cohort.30
For the post hoc delayed-start analysis, 23 participants initially assigned to the vamorolone low-dose groups (ie, 0.25 and 0.75 mg/kg/d) during the first 6 months of the dose-finding study were considered to have delayed starts. Outcomes for these participants were compared with outcomes among 23 participants who were initially assigned to and retained on higher-dose vamorolone (ie, 2.0 and 6.0 mg/kg/d) throughout their follow-up and were considered to have early starts. Estimates and standard errors were calculated using MMRM.
Data manipulation, tabulation of descriptive statistics, and graphical representations were performed primarily using statistical software SAS version 9.4 or higher (SAS Institute) and R version 4.1.0 (R Project for Statistical Computing). The following R packages were used: interval,42 lme4,43 lmerTest,44 sjPlot,45 visreg,46 and vistime.47 All statistical tests were 2-sided, and a resultant P value ≤ .05 was considered statistically significant. No adjustments for multiplicity on inferential statistics were made as per the statistical analysis plan (Supplement 2). Data were analyzed from July 2020 through November 2021. More details regarding statistical modeling, as well as real-world comparator populations (ie, historical control groups with different GCs [prednisone or deflazacort], and regimen [daily or intermittent]) are provided in eAppendix 3 in Supplement 1.
Results
Among 46 boys with DMD who completed the dose-finding study, 41 participants (89.1%; baseline mean [SD] age, 5.33 [0.96] years) completed the 2-year LTE treatment period; 5 participants withdrew for reasons unrelated to the study drug (Figure 1). At the LTE month 24 visit, 11 participants, 3 participants, and 27 participants were being treated at 2.0 mg/kg/d, 4.0 mg/kg/d, and 6.0 mg/kg/d, respectively (eFigure 1 in Supplement 1). Analysis of treatment efficacy focused on 23 participants receiving higher-dose vamorolone who were initially assigned and maintained on 2.0 mg/kg/d or more for up to 30 months during the dose-finding study (6 months) and LTE study (24 months). Demographic and clinical characteristics of participants in the LTE study receiving higher doses are summarized in Table 1. The mean (SD) baseline age was 5.83 (0.88) years in the higher-dose LTE group. In the higher-dose LTE group, 3 participants (13.0%) withdrew before the LTE month 24 study visit. The subsets of participants receiving higher doses who completed all planned outcomes are summarized in eAppendix 3 in Supplement 1.
Table 1. Participant Demographic and Baseline Characteristics for External Comparisonsa.
| Characteristic | Participants | ||
|---|---|---|---|
| Higher-dose VBP15-LTE (N = 23)b | GC in CINRG DNHS (N = 75) | GC in NorthStar UK Network (N = 110)c | |
| Age at baseline comparison visit, y | |||
| Mean (SD) | 5.83 (0.88) | 6.08 (0.81) | 6.00 (0.77) |
| Median (range) | 5.65 (4.60-7.29) | 5.97 (4.50-7.48) | 5.94 (NA) |
| Steroid exposure at baseline comparison visit, mean (SD), d | 200.57 (7.54) | 227.73 (61.91) | 264.84 (57.39) |
| Duration of follow up from baseline visit, mean (SD), yd | 1.85 (0.46) | 1.36 (0.49) | NA |
| Participants with >18 mo follow-up after initial 6 mo of steroid exposure, No. (%) | 21 (91.3) | 30 (40.0) | NA |
| Weight (kg), No. | 23 | 73 | NA |
| Mean (SD) | 21.98 (3.78) | 20.35 (3.55) | NA |
| Median (range) | 22.50 (16.30-32.60) | 20.10 (14.80-32.60) | NA |
| Height (cm), No. | 22 | 73 | NA |
| Mean (SD) | 111.80 (6.94) | 109.86 (6.86) | NA |
| Median (range) | 113.05 (100.60-123.00) | 110.00 (96.10-126.30) | NA |
| Body Mass Index, No. | 22 | 72 | NA |
| Mean (SD) | 17.68 (1.23) | 16.68 (1.55) | NA |
| Median (range) | 17.65 (15.90-21.50) | 16.56 (12.19-20.44) | NA |
Abbreviations: CINRG, Cooperative International Neuromuscular Research Group; DNHS, Duchenne Natural History Study; GC, glucocorticoid; LTE, long-term extension; NA, not applicable; VBP, vamorolone.
Based on baseline comparator visit, which corresponds to approximately 6 months of steroid exposure for participants in the NorthStar UK Network and CINRG DNHS.
The higher-dose cohort refers to participants assigned to vamorolone 2.0 and 6.0 mg/kg/d from initial dose-finding (VBP15-002/-003) studies and maintained at 2.0 mg/kg/d or more from long-term extension (VBP15-LTE) baseline.
Owing to NorthStar UK Network participant-level data-sharing restrictions, limited summary information was available.
Reported for time to stand velocity.
Changes in Functional Outcomes Among Participants in LTE With Higher Doses
Among 23 participants started on higher-dose vamorolone, 21 individuals were treated throughout the dose-finding and LTE studies and had available data at 30 months (3 individuals dropped out, but for 1 individual, terminal visit data was available close to 30 months and counted as such based on procedures). In these individuals, there was a decrease from baseline to 30 months in mean (SD) TTSTAND velocity (0.206 [0.070] rises/s vs 0.189 [0.124] rises/s), which was not a statistically significant change (−0.011 rises/s; 95% CI, −0.068 to 0.046 rises/s). Similarly, there were no significant changes from baseline to 30 months in TTCLIMB velocity score among 18 participants with TTCLIMB data (0.035 tasks/s; 95% CI, −0.051 to 0.121 tasks/s), TTRW velocity score among 18 participants with TTRW data (0.061 m/s; 95% CI, −0.272 to 0.394 m/s), 6MWT total distance among 15 participants with 6MWT data (32.0 m; 95% CI, −18.95 to 82.95 m), and total NSAA score among 18 participants with NSAA data (1.6; 95% CI, −2.92 to 6.14). There was no statistically significant change in PODCI transfer and basic mobility scores from baseline to 30 months (eTable 2 in Supplement 1), and interpretation of QMT was limited by few observations after 30 months (eTable 3 in Supplement 1).
In a delayed start analysis, participants initiated on higher-dose vamorolone (ie, those with early starts) had better clinical outcomes at 6 months compared with those initially treated with low doses (ie, those with delayed starts). At 6, 18, and 30 months, the means of all 5 motor outcome measures were increased for participants with early starts compared with those with delayed starts, although not all differences were statistically significant. At 30 months, no means were statistically significantly different (Figure 2).
Figure 2. Efficacy of Vamorolone in Motor Function Assessments by High vs Low Starting Dose.

6MWT indicates 6-minute walk test; high, a starting dose of 2.0 mg/kg/d or greater; low, a starting dose of less than 2.0 mg/kg/d; points, means; whiskers, standard error of the mean. Mean estimated differences between participants treated at higher dose and low dose, as well as P values, are provided at 6 months (ie, prior to LTE) and 30 months (ie, at conclusion of LTE).
Efficacy of Higher-Dose Vamorolone Compared With GC Treatment in Historical Control Groups
The mean (SD) baseline age was 6.08 (0.81) years among 75 participants in the DNHS control group and 6.00 (0.77) years among 110 participants in the NorthStar UK Network control group. An increased proportion of participants in the higher-dose LTE group had more than 18 months of follow-up after the initial 6 months of steroid exposure compared with participants in the DNHS control group (21 participants [91.3%] vs 30 participants [40.0%]). As noted previously, 75 participants from DNHS and 23 participants from the LTE study receiving higher doses were criteria-matched and subjected to CEM, yielding a smaller subset of matched comparator group (including 29 participants from DNHS and 20 participants from the LTE study). However, participants from DNHS who were CEM-matched had limited follow-up data, and the baseline characteristics of these participants with approximately 2 years of long-term follow-up (which would inform longitudinal analysis) were dissimilar to those from participants in the LTE study who were CEM-matched, resulting in unsuccessful CEM for longitudinal comparison (eTable 1 in Supplement 1). Hence, we conducted a prespecified sensitivity analysis among 75 participants from DNHS and 23 participants from LTE; we present these comparisons in Table 1 and Table 2.
Table 2. Comparison of Study Primary Efficacy and Safety Outcome Measures.
| Outcome | Unique participants (longitudinal samples used), No. (No.) | Baseline mean (SD)a | End of follow up mean (SD)b | Statistical model or test P value (2-sided 95% CI) |
|---|---|---|---|---|
| Efficacy | ||||
| TTSTAND velocity, rises/s | ||||
| Higher-dose vamorolone LTEc | 23 (66) | 0.25 (0.10) | 0.20 (0.13) | vs DNHS (MMRM) |
| GC in DNHS | 75 (313) | 0.25 (0.10) | 0.25 (0.13) | Quadratic comparisond: >.99 (−0.30 to 0.30); linear comparison: .10 (−0.66 to 0.05) |
| With ≥1.5 y follow-up)e | 30 (153) | 0.24 (0.09) | 0.24 (0.12) | |
| TTCLIMB velocity, tasks/s | ||||
| Higher-dose vamorolone LTEc | 23 (63) | 0.31 (0.13) | 0.32 (0.19) | vs DNHS (MMRM) |
| GC in DNHS | 75 (311) | 0.32 (0.14) | 0.33 (0.18) | Quadratic comparison: >.99 (–0.36 to 0.36) linear comparison: .93 (−0.41 to 0.44) |
| With ≥1.5 y follow-up) | 30 (153) | 0.31 (0.13) | 0.32 (0.16) | |
| TTRW velocity, meters/s | ||||
| Higher-dose vamorolone LTEc | 23 (63) | 1.90 (0.34) | 1.87 (0.63) | vs DNHS (MMRM) |
| GC in DNHS | 75 (317) | 1.91 (0.52) | 1.89 (0.71) | Quadratic comparison: .90 (−1.24 to 1.41) Linear comparison: .94 (−1.57 to 1.46) |
| With ≥1.5 years follow-up) | 30 (153) | 1.85 (0.37) | 1.85 (0.64) | |
| 6MWT, m walked | ||||
| Higher-dose vamorolone LTEc | 20 (37) | 377.9 (64.77) | 369.9 (77.81) | Paired sample (within group) t test: .20 (−18.95 to 82.95) |
| NSAA scoref | ||||
| Higher-dose vamorolone LTEc | 23 (41) | 22.3 (4.72) | 21.78 (7.86) | vs NorthStar UK cohort (independent t test on change over 2 y)f |
| GC in NSUK Network | 110 (159) | 26.63 (5.65)g | 26.24 (7.2) | .92 (−4.48 to 4.04) |
| Height percentile | ||||
| Higher-dose vamorolone LTEc | 23 (65) | 32.26 (26.87) | 37.03 (31.14) | vs DNHS (MMRM) |
| GC in DNHS | 75 (312) | 19.88 (21.70) | 13.42 (18.62) | 8.94 × 10−7 (0.23 to 0.52) |
| BMI z score | ||||
| Higher-dose vamorolone LTEc | 23 (65) | 1.28 (0.51) | 1.52 (0.66) | vs DNHS (MMRM) |
| GC in DNHS | 75 (309) | 0.65 (1.03) | 0.79 (1.11) | .58 (−0.01 to 0.01) |
Abbreviations: DNHS, Duchenne Natural History Study; GC, glucocorticoid; LTE, long-term extension; MMRM, mixed-effect model with repeated measures; NSAA, NorthStar Ambulatory Assessment; NSUK, NorthStar United Kingdom; TTCLIMB, time to climb 4 stairs; TTRW, time to run or walk 10 m; TTSTAND, time to stand from supine position; 6MWT, 6-minute walk test distance.
Baseline values after approximately 6 months of continual treatment with vamorolone or GC.
Last visit of participants is used. One participant in vamorolone LTE had 1 measurement and was included in baseline comparator and end of follow-up summaries.
Participants assigned to higher-dose vamorolone (ie, 2.0 and 6.0 mg/kg/d) at start of study and maintained at 2.0 mg/kg/d or more at follow up.
The multivariable model included a quadratic term in addition to model trajectories (ie, Duchenne muscular dystrophy natural history during the age range of interest includes periods of improvement followed by stability and deterioration); P values are provided for comparisons between comparator cohorts.
DNHS is a natural history study with different participants followed up for different durations in the age range of comparison. Summary characteristics are also provided for participants in DNHS with 1.5 years or more of follow-up in the age range of interest.
Owing to NorthStar UK Network participant-level data sharing restrictions, NSAA data was analyzed separately by UK Network researchers and summaries were shared for comparison with the vamorolone LTE cohort. NSAA data had a possible range from 0 to 34.
Owing to the use of independent t test for change in NSAA over 2 years, the baseline mean is provided for 49 participants with 2 years of follow-up.
In longitudinal comparison of mean TTSTAND, TTRW, and TTCLIMB velocity from baseline to end of follow-up, the LTE group and DNHS group were not significantly different (Table 2, Figure 3; eFigure 2 in Supplement 2). Mean TTSTAND velocity trajectories were not significantly different (estimates of difference from interaction of orthogonal polynomial terms with cohort: quadratic term coefficient estimate, 0.001; 95% CI, −0.30 to 0.30; P > .99; linear term coefficient estimate, −0.30; 95% CI, −0.66 to 0.05; P = .10). There was no significant difference in the NPMLE estimate of time to reach a TTSTAND milestone of 10 seconds or more between 22 participants in the higher-dose LTE not beyond 10 seconds at baseline (median age, >9.31 years; 95% CI, 7.51 to ∞ years) and 74 participants in the DNHS group not beyond 10 seconds at baseline (median age, >9.31 years; 95% CI, 8.29 to ∞ years) (asymptotic log-rank 2-sample test P = .74).
Figure 3. Outcome Comparisons of Vamorolone Long-term Extension (LTE) and Duchenne Natural History (DNHS) Study Cohorts.

BMI indicates body mass index. Trajectories based on model estimates, along with 95% CIs, are plotted for an individual with fixed baseline values.
Change in mean total NSAA score for 18 participants receiving higher-dose vamorolone with NSAA data (−0.61; 95% CI, −4.65 to 3.43) vs 49 participants in NSUK receiving GC with NSAA data (–0.39; 95% CI, −1.91 to 1.13) at 2-years of follow-up was not statistically significantly different (0.22 units; 95% CI, −4.48 to 4.04; P = .92) (Table 2). Additionally, body mass index z score change (0.002 SD/mo; 95% CI, −0.006 to 0.010; P = .58) was not significantly different between the higher-dose vamorolone group vs the DNHS group. The NPMLE estimate of time to reach a TTSTAND milestone of 10 seconds or more for 108 participants in NSUK who had not experienced this event by baseline (median age, 9.55 years; 95% CI, 8.87 to ∞ years) was similar to that for participants in DNHS and participants in the LTE study receiving higher doses. Additionally, a relative risk analysis of NSAA scores showed no significant difference in the risk of losing a motor function (ie, change from a function score of a 1 or 2 at baseline to a 0 at the end of follow-up) between participants in NSUK and participants in the LTE study receiving higher doses (139 of 1734 functions lost [8.0%] vs 26 of 335 functions lost [7.8%]; relative risk, 1.033 [95% CI, 0.691 to 1.544]).
Safety Analysis of LTE Cohort
During the 24-month LTE treatment period, all 46 participants experienced at least 1 treatment-emergent AE (eTable 4 in Supplement 1). Among 41 participants receiving vamorolone at 6.0 mg/kg/d, 10 participants (24.4%) deescalated to 2.0 mg/kg/d owing to a treatment-emergent AE of weight gain. The AE abated among 6 participants after dose reduction. Among the 46 LTE participants, 6 participants (13.0%) were observed to have a total of 7 clinical fracture events according to local site AE reporting, including 1 participant with a vertebral fracture and a foot fracture on 2 separate occasions, 3 participants with an upper limb fracture, 1 participant with a vertebral compression fracture, and 1 participant with multiple vertebral fractures. There were 2 serious treatment-emergent AEs: moderate pneumonia in 1 participant and severe myoglobinuria, which occurred twice in 1 participant; 1 participant withdrew from the study owing to moderate muscle weakness. These treatment-emergent AEs were considered by the investigators to not be associated with the study drug.
Mean changes in hematology, chemistry, liver function, lipid profile, urinalysis, and electrocardiogram parameters were minimal and clinically unremarkable. There was no significant difference in changes to mean BMI z scores between participants receiving higher-dose vamorolone and those from DNHS (Figure 3D). In comparison of participants receiving higher-dose vamorolone with participants from DNHS treated with GC, there was a statistically significant difference in change in mean height percentile change (0.37 percentile/mo; 95% CI, 0.23 to 0.52 percentile/mo), with no evidence of growth deceleration in the vamorolone group (Figure 3E; eFigure 3 in Supplement 1). Among 41 participants in LTE who finished the 2-year LTE period, 39 participants (95.1%) had a hand and wrist x-ray at month 24; the mean bone age to chronologic age difference was −1.1 years (95% CI, −1.5 to −0.7 years). Results on serum biomarkers of safety including insulin resistance, adrenal suppression, and bone turnover will be presented in a separate report.
Discussion
The results of this nonrandomized clinical trial extend the findings of previous reports on open-label vamorolone treatment among boys with DMD to a total treatment duration of 30 months.25,26,27 We found that vamorolone treatment was not associated with a change in TTSTAND velocity from baseline to 30 months among boys with DMD aged 4 to 7 years at enrollment. However, based on clinical and laboratory results, long-term vamorolone treatment at doses up to 6.0 mg/kg/d appeared to be safe and well-tolerated. While there was an overall decline after initial improvement in TTSTAND velocity observed among boys treated with vamorolone over 2 years, vamorolone showed similar treatment efficacy as GC in DMD,48 and the decline was slower compared with that of untreated patients.26,27 Moreover, participants receiving higher doses (ie, ≥2 mg/kg/d) of vamorolone had persistent improvement in motor function as measured by TTCLIMB, TTRW, NSAA, and 6MWT distance over a 30-month treatment period.
Vamorolone treatment was associated with fewer adverse outcomes compared with GC therapy. Continuous treatment with vamorolone for up to 30 months was not associated with linear growth deceleration, whereas growth delay is a well-recognized adverse outcome associated with traditional GC, which can be distressing to boys with DMD as they mature through adolescence.49,50,51 We observed that boys treated with vamorolone had minimal bone age delay relative to chronological age. In this setting of improved growth velocity with vamorolone, the slight bone age delay is anticipated to be favorable for these patients to attain increased adult height associated with greater residual growth potential. Although some participants receiving high-dose vamorolone had dose reduction to address undesired weight gain, the change in mean BMI z score was not significantly different between participants receiving vamorolone compared with participants in DNHS receiving GC.27 To date, pharmacodynamic biomarker data suggest that vamorolone is not associated with short-term detrimental bone outcomes.25 Additionally, vamorolone does not have the same association with insulin resistance as classic GC therapy; however, long-term vamorolone treatment may be associated with adrenal suppression.27
Limitations
This study has several limitations. The open-label study design and use of prospectively collected real-world observational control data sets with different GCs (ie, prednisone or deflazacort), dose, and regimen (ie, daily or intermittent as per clinical practice16,52) require cautious interpretation of the study results. The comparator data sets included patients with DMD who had been on GC for a variable amount of time before the baseline comparator visits. There was also considerable attrition in the data of participants in comparator groups over time (eg, 91.3% of participants in LTE vs 40.0% of participants in DNHS had >18 months of follow-up data for TTSTAND velocity). Despite strict subset enrollment criteria and adjustment for baseline characteristics, confounding is still possible. We could not look for association between height and motor function among patients treated with vamorolone and GC owing to the nonrandomized study design and small sample size; the risk of adrenal insufficiency will require additional studies.
Conclusions
We found that vamorolone, a novel dissociative steroidal anti-inflammatory drug, was not associated with a change in TTSTAND velocity from baseline to 30 months among boys with DMD aged 4 to 7 at enrollment. However, vamorolone was associated with similar efficacy and maintenance of muscle function comparable to historical cohorts of patients with DMD treated with GC after treatment for 30 months. Vamorolone appeared to be well-tolerated, with fewer safety concerns that are typically seen with standard-of-care GC treatment for ambulatory patients with DMD. A randomized double-blind vamorolone study (VBP15-004; NCT03439670) is near completion; results from this study will provide class I evidence for vamorolone efficacy and safety.
eTable 1. Comparison of Coarsened Exact Matched Participants in Duchenne Natural History Study (DNHS) and Higher-Dose VBP15 Long-term Extension (LTE) Study
eTable 2. Pediatric Outcomes Data Collection Instrument (PODCI) Scores
eTable 3. Quantitative Muscle Testing (QMT) Scores
eTable 4. Adverse Events by Dose at Time of Event From 30 mo of Vamorolone Treatment
eFigure 1. Patient-Level Dose Regimen Schematic
eFigure 2. Timed Motor Function Comparisons of Vamorolone Long-term Extension vs Duchenne Natural History Study With Individual Trajectories
eFigure 3. Body Mass Index z Score and Height Percentile Comparisons of Vamorolone Long-term Extension vs Duchenne Natural History Study With Individual Trajectories
eAppendix 1. Duchenne Natural History Study Cohort External Comparison Workflow Plan
eAppendix 2. NorthStar United Kingdom Network Cohort External Comparison Workflow Plan
eAppendix 3. Supplemental Text on Statistical Analysis
Trial Protocol
Group Authors
Data Sharing Statement
References
- 1.Mah JK, Korngut L, Dykeman J, Day L, Pringsheim T, Jette N. A systematic review and meta-analysis on the epidemiology of Duchenne and Becker muscular dystrophy. Neuromuscul Disord. 2014;24(6):482-491. doi: 10.1016/j.nmd.2014.03.008 [DOI] [PubMed] [Google Scholar]
- 2.Hoffman EP, Brown RH Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell. 1987;51(6):919-928. doi: 10.1016/0092-8674(87)90579-4 [DOI] [PubMed] [Google Scholar]
- 3.Evans NP, Misyak SA, Robertson JL, Bassaganya-Riera J, Grange RW. Immune-mediated mechanisms potentially regulate the disease time-course of Duchenne muscular dystrophy and provide targets for therapeutic intervention. PM R. 2009;1(8):755-768. doi: 10.1016/j.pmrj.2009.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen YW, Nagaraju K, Bakay M, et al. Early onset of inflammation and later involvement of TGFbeta in Duchenne muscular dystrophy. Neurology. 2005;65(6):826-834. doi: 10.1212/01.wnl.0000173836.09176.c4 [DOI] [PubMed] [Google Scholar]
- 5.Rosenberg AS, Puig M, Nagaraju K, et al. Immune-mediated pathology in Duchenne muscular dystrophy. Sci Transl Med. 2015;7(299):299rv4. doi: 10.1126/scitranslmed.aaa7322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kumar A, Boriek AM. Mechanical stress activates the nuclear factor-kappaB pathway in skeletal muscle fibers: a possible role in Duchenne muscular dystrophy. FASEB J. 2003;17(3):386-396. doi: 10.1096/fj.02-0542com [DOI] [PubMed] [Google Scholar]
- 7.Acharyya S, Villalta SA, Bakkar N, et al. Interplay of IKK/NF-kappaB signaling in macrophages and myofibers promotes muscle degeneration in Duchenne muscular dystrophy. J Clin Invest. 2007;117(4):889-901. doi: 10.1172/JCI30556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dogra C, Changotra H, Wergedal JE, Kumar A. Regulation of phosphatidylinositol 3-kinase (PI3K)/Akt and nuclear factor-kappa B signaling pathways in dystrophin-deficient skeletal muscle in response to mechanical stretch. J Cell Physiol. 2006;208(3):575-585. doi: 10.1002/jcp.20696 [DOI] [PubMed] [Google Scholar]
- 9.Pahl HL. Activators and target genes of Rel/NF-kappaB transcription factors. Oncogene. 1999;18(49):6853-6866. doi: 10.1038/sj.onc.1203239 [DOI] [PubMed] [Google Scholar]
- 10.Spencer MJ, Montecino-Rodriguez E, Dorshkind K, Tidball JG. Helper (CD4(+)) and cytotoxic (CD8(+)) T cells promote the pathology of dystrophin-deficient muscle. Clin Immunol. 2001;98(2):235-243. doi: 10.1006/clim.2000.4966 [DOI] [PubMed] [Google Scholar]
- 11.Spencer MJ, Tidball JG. Do immune cells promote the pathology of dystrophin-deficient myopathies? Neuromuscul Disord. 2001;11(6-7):556-564. doi: 10.1016/S0960-8966(01)00198-5 [DOI] [PubMed] [Google Scholar]
- 12.Griggs RC, Moxley RT III, Mendell JR, et al. ; Clinical Investigation of Duchenne Dystrophy Group . Prednisone in Duchenne dystrophy: a randomized, controlled trial defining the time course and dose response. Arch Neurol. 1991;48(4):383-388. doi: 10.1001/archneur.1991.00530160047012 [DOI] [PubMed] [Google Scholar]
- 13.Mendell JR, Moxley RT, Griggs RC, et al. Randomized, double-blind six-month trial of prednisone in Duchenne’s muscular dystrophy. N Engl J Med. 1989;320(24):1592-1597. doi: 10.1056/NEJM198906153202405 [DOI] [PubMed] [Google Scholar]
- 14.Malik V, Rodino-Klapac LR, Mendell JR. Emerging drugs for Duchenne muscular dystrophy. Expert Opin Emerg Drugs. 2012;17(2):261-277. doi: 10.1517/14728214.2012.691965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Matthews E, Brassington R, Kuntzer T, Jichi F, Manzur AY. Corticosteroids for the treatment of Duchenne muscular dystrophy. Cochrane Database Syst Rev. 2016;2016(5):CD003725. doi: 10.1002/14651858.CD003725.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bello L, Gordish-Dressman H, Morgenroth LP, et al. ; CINRG Investigators . Prednisone/prednisolone and deflazacort regimens in the CINRG Duchenne Natural History Study. Neurology. 2015;85(12):1048-1055. doi: 10.1212/WNL.0000000000001950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kauh E, Mixson L, Malice MP, et al. Prednisone affects inflammation, glucose tolerance, and bone turnover within hours of treatment in healthy individuals. Eur J Endocrinol. 2012;166(3):459-467. doi: 10.1530/EJE-11-0751 [DOI] [PubMed] [Google Scholar]
- 18.Schakman O, Kalista S, Barbé C, Loumaye A, Thissen JP. Glucocorticoid-induced skeletal muscle atrophy. Int J Biochem Cell Biol. 2013;45(10):2163-2172. doi: 10.1016/j.biocel.2013.05.036 [DOI] [PubMed] [Google Scholar]
- 19.Pane M, Mazzone ES, Sivo S, et al. Long term natural history data in ambulant boys with Duchenne muscular dystrophy: 36-month changes. PLoS One. 2014;9(10):e108205. doi: 10.1371/journal.pone.0108205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kim S, Zhu Y, Romitti PA, et al. ; MD STARnet . Associations between timing of corticosteroid treatment initiation and clinical outcomes in Duchenne muscular dystrophy. Neuromuscul Disord. 2017;27(8):730-737. doi: 10.1016/j.nmd.2017.05.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Connolly AM, Zaidman CM, Golumbek PT, et al. ; MDA DMD Clinical Research Network . Twice-weekly glucocorticosteroids in infants and young boys with Duchenne muscular dystrophy. Muscle Nerve. 2019;59(6):650-657. doi: 10.1002/mus.26441 [DOI] [PubMed] [Google Scholar]
- 22.Reeves EKM, Hoffman EP, Nagaraju K, Damsker JM, McCall JM. VBP15: preclinical characterization of a novel anti-inflammatory delta 9,11 steroid. Bioorg Med Chem. 2013;21(8):2241-2249. doi: 10.1016/j.bmc.2013.02.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liu X, Wang Y, Gutierrez JS, et al. Disruption of a key ligand-H-bond network drives dissociative properties in vamorolone for Duchenne muscular dystrophy treatment. Proc Natl Acad Sci U S A. 2020;117(39):24285-24293. doi: 10.1073/pnas.2006890117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Heier CR, Yu Q, Fiorillo AA, et al. Vamorolone targets dual nuclear receptors to treat inflammation and dystrophic cardiomyopathy. Life Sci Alliance. 2019;2(1):1-16. doi: 10.26508/lsa.201800186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Conklin LS, Damsker JM, Hoffman EP, et al. Phase IIa trial in Duchenne muscular dystrophy shows vamorolone is a first-in-class dissociative steroidal anti-inflammatory drug. Pharmacol Res. 2018;136:140-150. doi: 10.1016/j.phrs.2018.09.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hoffman EP, Schwartz BD, Mengle-Gaw LJ, et al. ; Cooperative International Neuromuscular Research Group . Vamorolone trial in Duchenne muscular dystrophy shows dose-related improvement of muscle function. Neurology. 2019;93(13):e1312-e1323. doi: 10.1212/WNL.0000000000008168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Smith EC, Conklin LS, Hoffman EP, et al. ; CINRG VBP15 and DNHS Investigators . Efficacy and safety of vamorolone in Duchenne muscular dystrophy: an 18-month interim analysis of a non-randomized open-label extension study. PLoS Med. 2020;17(9):e1003222. doi: 10.1371/journal.pmed.1003222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McDonald CM, Henricson EK, Abresch RT, et al. ; CINRG Investigators . The cooperative international neuromuscular research group Duchenne natural history study—a longitudinal investigation in the era of glucocorticoid therapy: design of protocol and the methods used. Muscle Nerve. 2013;48(1):32-54. doi: 10.1002/mus.23807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Henricson EK, Abresch RT, Cnaan A, et al. ; CINRG Investigators . The cooperative international neuromuscular research group Duchenne natural history study: glucocorticoid treatment preserves clinically meaningful functional milestones and reduces rate of disease progression as measured by manual muscle testing and other commonly used clinical trial outcome measures. Muscle Nerve. 2013;48(1):55-67. doi: 10.1002/mus.23808 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.McDonald CM, Henricson EK, Abresch RT, et al. ; CINRG Investigators . Long-term effects of glucocorticoids on function, quality of life, and survival in patients with Duchenne muscular dystrophy: a prospective cohort study. Lancet. 2018;391(10119):451-461. doi: 10.1016/S0140-6736(17)32160-8 [DOI] [PubMed] [Google Scholar]
- 31.Iacus SM, King G, Porro G. Multivariate matching methods that are monotonic imbalance bounding. J Am Stat Assoc. 2011;106(493):345-361. doi: 10.1198/jasa.2011.tm09599 [DOI] [Google Scholar]
- 32.Iacus SM, King G, Porro G, Nielsen R. CEM: coarsened exact matching. The Comprehensive R Archive Network. Accessed December 8, 2021. https://cran.r-project.org/package=cem
- 33.Ricotti V, Ridout DA, Pane M, et al. ; UK NorthStar Clinical Network . The NorthStar Ambulatory Assessment in Duchenne muscular dystrophy: considerations for the design of clinical trials. J Neurol Neurosurg Psychiatry. 2016;87(2):149-155. doi: 10.1136/jnnp-2014-309405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Centers for Disease Control and Prevention . Percentile data files with LMS values. National Center for Health Statistics. Accessed December 8, 2021. https://www.cdc.gov/growthcharts/percentile_data_files.htm
- 35.Brooke MH, Griggs RC, Mendell JR, Fenichel GM, Shumate JB, Pellegrino RJ. Clinical trial in Duchenne dystrophy: I. the design of the protocol. Muscle Nerve. 1981;4(3):186-197. doi: 10.1002/mus.880040304 [DOI] [PubMed] [Google Scholar]
- 36.McDonald CM, Henricson EK, Han JJ, et al. The 6-minute walk test as a new outcome measure in Duchenne muscular dystrophy. Muscle Nerve. 2010;41(4):500-510. doi: 10.1002/mus.21544 [DOI] [PubMed] [Google Scholar]
- 37.Scott E, Eagle M, Mayhew A, et al. ; North Star Clinical Network for Paediatric Neuromuscular Disease . Development of a functional assessment scale for ambulatory boys with Duchenne muscular dystrophy. Physiother Res Int. 2012;17(2):101-109. doi: 10.1002/pri.520 [DOI] [PubMed] [Google Scholar]
- 38.Escolar DM, Henricson EK, Mayhew J, et al. Clinical evaluator reliability for quantitative and manual muscle testing measures of strength in children. Muscle Nerve. 2001;24(6):787-793. doi: 10.1002/mus.1070 [DOI] [PubMed] [Google Scholar]
- 39.Dang UJ, Ziemba M, Clemens PR, Hathout Y, Conklin LS, Hoffman EP; CINRG Vamorolone 002/003 Investigators . Serum biomarkers associated with baseline clinical severity in young steroid-naïve Duchenne muscular dystrophy boys. Hum Mol Genet. 2020;29(15):2481-2495. doi: 10.1093/hmg/ddaa132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McDonald CM, McDonald DA, Bagley A, et al. Relationship between clinical outcome measures and parent proxy reports of health-related quality of life in ambulatory children with Duchenne muscular dystrophy. J Child Neurol. 2010;25(9):1130-1144. doi: 10.1177/0883073810371509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.McDonald CM, Campbell C, Torricelli RE, et al. ; Clinical Evaluator Training Group; ACT DMD Study Group . Ataluren in patients with nonsense mutation Duchenne muscular dystrophy (ACT DMD): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390(10101):1489-1498. doi: 10.1016/S0140-6736(17)31611-2 [DOI] [PubMed] [Google Scholar]
- 42.Fay MP, Shaw PA. Exact and asymptotic weighted logrank tests for interval censored data: the interval R package. J Stat Softw. 2010;36(2):io2. doi: 10.18637/jss.v036.i02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bates D, Mächler M, Bolker BM, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67(1):1-48. doi: 10.18637/jss.v067.i01 [DOI] [Google Scholar]
- 44.Kuznetsova A, Brockhoff PB, Christensen RHB. lmerTest Package: Tests in Linear Mixed Effects Models. J Stat Softw. 2017;82(13). doi: 10.18637/jss.v082.i13 [DOI] [Google Scholar]
- 45.Lüdecke D. sjPlot—data visualization for statistics in social science. GitHub. Accessed December 8, 2021. https://strengejacke.github.io/sjPlot/
- 46.Breheny P, Burchett W.. Visualization of regression models using visreg. R J. 2017;9(2):56-71. doi: 10.32614/RJ-2017-046 [DOI] [Google Scholar]
- 47.Raabe S. Vistime: pretty timelines in R. R package version 1.2.1. The Comprehensive R Archive Network. Accessed December 8, 2021. https://CRAN.R-project.org/package=vistime
- 48.Arora H, Willcocks RJ, Lott DJ, et al. Longitudinal timed function tests in Duchenne muscular dystrophy: ImagingDMD cohort natural history. Muscle Nerve. 2018;58(5):631-638. doi: 10.1002/mus.26161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ward LM, Weber DR. Growth, pubertal development, and skeletal health in boys with Duchenne muscular dystrophy. Curr Opin Endocrinol Diabetes Obes. 2019;26(1):39-48. doi: 10.1097/MED.0000000000000456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Joseph S, Wang C, Bushby K, et al. ; UK NorthStar Clinical Network . Fractures and linear growth in a nationwide cohort of boys with Duchenne muscular dystrophy with and without glucocorticoid treatment: results from the UK NorthStar database. JAMA Neurol. 2019;76(6):701-709. doi: 10.1001/jamaneurol.2019.0242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wood CL, Straub V, Guglieri M, Bushby K, Cheetham T. Short stature and pubertal delay in Duchenne muscular dystrophy. Arch Dis Child. 2016;101(1):101-106. doi: 10.1136/archdischild-2015-308654 [DOI] [PubMed] [Google Scholar]
- 52.Griggs RC, Herr BE, Reha A, et al. Corticosteroids in Duchenne muscular dystrophy: major variations in practice. Muscle Nerve. 2013;48(1):27-31. doi: 10.1002/mus.23831 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Comparison of Coarsened Exact Matched Participants in Duchenne Natural History Study (DNHS) and Higher-Dose VBP15 Long-term Extension (LTE) Study
eTable 2. Pediatric Outcomes Data Collection Instrument (PODCI) Scores
eTable 3. Quantitative Muscle Testing (QMT) Scores
eTable 4. Adverse Events by Dose at Time of Event From 30 mo of Vamorolone Treatment
eFigure 1. Patient-Level Dose Regimen Schematic
eFigure 2. Timed Motor Function Comparisons of Vamorolone Long-term Extension vs Duchenne Natural History Study With Individual Trajectories
eFigure 3. Body Mass Index z Score and Height Percentile Comparisons of Vamorolone Long-term Extension vs Duchenne Natural History Study With Individual Trajectories
eAppendix 1. Duchenne Natural History Study Cohort External Comparison Workflow Plan
eAppendix 2. NorthStar United Kingdom Network Cohort External Comparison Workflow Plan
eAppendix 3. Supplemental Text on Statistical Analysis
Trial Protocol
Group Authors
Data Sharing Statement