

Abstract
Objectives Social determinants of health (SDoH) can be measured at the geographic level to convey information about neighborhood deprivation. The Ohio Children's Opportunity Index (OCOI) is a composite area-level opportunity index comprised of eight health domains. Our research team has documented the design, development, and use cases of a dashboard solution to visualize OCOI.
Methods The OCOI is a multidomain index spanning the following eight domains: (1) family stability, (2) infant health, (3) children's health, (4) access, (5) education, (6) housing, (7) environment, and (8) criminal justice. Information on these eight domains is derived from the American Community Survey and other administrative datasets. Our team used the Tableau Desktop visualization software and applied a user-centered design approach to developing the two OCOI dashboards—main OCOI dashboard and OCOI-race dashboard. We also performed convergence analysis to visualize the census tracts where different health indicators simultaneously exist at their worst levels.
Results The OCOI dashboard has multiple, interactive components as follows: a choropleth map of Ohio displaying OCOI scores for a specific census tract, graphs presenting OCOI or domain scores to compare relative positions for tracts, and a sortable table to visualize scores for specific county and census tracts. A case study using the two dashboards for convergence analysis revealed census tracts in neighborhoods with low infant health scores and a high proportion of minority population.
Conclusion The OCOI dashboards could assist health care leaders in making decisions that enhance health care delivery and policy decision-making regarding children's health particularly in areas where multiple health indicators exist at their worst levels.
Keywords: data visualization, social determinants of health, geographical information system, area level deprivation, opportunity index
Background and Significance
In children's health nationally, Ohio ranks 31st . Nearly 2.6 million of the 11.5 million population in Ohio are children aged, that is, 0 to 17 years. Of these, approximately 20% live in poverty, 16% are chronically absent from school, over 0.7% are homeless, and 14 to 15% have disabilities. Thirty-one percent of children and adolescents have been classified as overweight or obese, and nearly half (46%) the adolescents and children report not exercising regularly. Further, a considerable health disparity exists in self-reported health between White and Black children, 1 as well as in infant mortality rates between infants born to White and Black mothers. 2 Together, these statistics indicate an abundance of opportunity for improvement in children's health across Ohio.
The literature thoroughly acknowledges the relationship between social determinants of health (SDoH) and health outcomes. 3 Individual-level factors alone have been deemed insufficient for explaining population disease patterns, thereby raising the importance of context. 4 5 6 7 8 Neighborhoods have emerged as relevant contexts as they possess physical and social attributes that could affect health. 6 9 Neighborhood deprivation can be communicated using area-level measures of SDoH which are composite, and often weighted, scores of measures representing different domains of deprivation. Across the world, multidomain indices of deprivation have been computed at the level of census-based geographic units, 10 11 12 13 14 15 16 to be used as guides for resource allocation, community advocacy, and research. 17 These geographic indices consider factors including unemployment, environmental risks, crime, poor educational resources, lack of transportation, low housing availability, unsafe housing, access to health care, and access to food and resources. 10 11 12 13 14 15 16 Many of these indices were constructed to be general purpose measures and may fall short if the research or policy focus of a particular problem is children.
The neighborhood context bears considerably on the development of children. 18 19 20 Neighborhood deprivation is linked with developmental outcomes such as behavioral problems and cognitive ability 21 22 23 24 and is known to specifically affect college attendance and earnings. 25 Risk factors tend to cluster within individuals, families, and communities exacerbating the inverse relationship 26 that already exists between those who need health care and those who have access to it. 27 28 Together, this evidence highlights the importance of appropriate interventions in the early years of development to positively alter life course trajectories of socioeconomic position and health.
The current Public Health 3.0 (PH 3.0) era is characterized by the use of geospatial inferences, nontraditional data sources, and community-level indicators. 29 Insights from this kind of data are expected to serve as communication and policy tools, promote wellness through changing environmental, social, and economic contexts, and lead to action plans that are multisectoral. 29 With the objective of improving birth outcomes in Ohio, the Ohio Department of Medicaid (ODM) collaborated with researchers at the Ohio State University (OSU) to develop area-level measures of deprivation. Troubling disparities in infant mortality in Ohio, 30 31 prompted the creation of the Ohio Opportunity Index (OOI) and the Ohio Children's Opportunity Index (OCOI)—composite scores of measures representing different domains of opportunity. In addition, ODM also required a powerful way to visualize this information for public health activities.
Dashboards are powerful tools supporting public health and clinical efforts. 32 33 34 They offer several advantages over traditional methods of disseminating data, such as the ability to customize data presentations per the user's interest, to more effectively convey information on trends, to facilitate evaluation of the impact of interventions on communities and subpopulations, and to provide easy access to data to anyone with an internet connection. 35 Visualizing the OCOI using dashboards can assist policymakers, public health officials, and health care leaders in making decisions for better health care delivery to reduce disparities in children's health. To this end, we developed two functional and interactive dashboards with training material to display the distribution of the OCOI. We sought to understand the requirements and preferences of the end-users at ODM to develop the dashboards following a user-centered design (UCD) approach. 36
Objective
This study aimed to the below-mentioned objectives:
To understand the requirements of the end-users of the OCOI dashboards.
To develop the main OCOI dashboard bearing in mind two use cases: end-users at ODM and community-based organizations using the dashboard to plan or deliver interventions and health care programs.
To develop a second OCOI dashboard that displays the race/ethnic distribution in census tracts across Ohio.
To develop training material for the use of two OCOI dashboards.
To provide a case study of how the two OCOI dashboards can be used to perform convergence analysis to visualize factors associated with children's health outcomes in combination with data on infant mortality rates in Ohio from the Ohio Department of Health.
Methods
Our approach to developing and deploying the OCOI dashboard followed the principles of UCD ( Supplementary Appendix 1 ; available in the online version) 36 which involved constant engagement with subject matter experts and stakeholders represented by end-users from ODM using informal focus group discussions.
Setting
This project is an extension of the Infant Mortality Research Project that was set up to improve birth outcomes in Ohio. Researchers at OSU compiled the pertinent data and constructed the OCOI. 37
Data
Data were collected at the census tract level because they are small and relatively homogenous areal units about which the needed data were available. Of the 2,952 census tracts in Ohio, study data pertain to 2,940 tracts with nonzero population. Data were collected from the U.S. Census based American Community Survey (ACS), and other state-level agency administrative datasets (e.g., Medicaid claims and Department of Education school report card data). Information was compiled across these sources and linked with census tract Federal Information Processing Standard (FIPS) codes—numeric and two-letter alphabetic codes to identify U.S. states and associated geographic areas. Finally, datasets corresponding to two different time periods, period I (2010–2014) and period II (2013–2017), were collated for developing respective OCOIs. 37
Domains and Measures of Ohio Children's Opportunity Index
Well-being in children is based on economic, material, and psychosocial conditions in which they grow. 18 19 20 25 These socioeconomic conditions relate to their parents or caregivers, housing units, and the neighborhood in which they live. 38 Guided by these findings and input from subject matter experts, the study team, outlined several domains from which eight were finalized for use: (1) family stability, (2) infant health, (3) children's health, (4) access (to health care and food), (5) education, (6) housing, (7) environment, (8) and criminal justice. 37 39 40 These domains are consistent with the SDoH attributes outlined by the Centers for Disease Control and Prevention (CDC) such as food supply, housing, transportation, education, and health care. 41 42
The OCOI is composed of eight equally weighted domains. Each of the eight domains was measured by multiple variables also referred to as constituent measures. A total of 53 variables were proposed for use; however, information on only 37 variables was available for period I. As a result, for the purpose of comparison, the period-II dataset was treated in two ways; period II (reduced) comprising the same 37 variables as in period I (reduced) and period II (complete) with all 53 variables. Consequently, three datasets, period I (reduced), period II (reduced), and period II (complete), were used for study analyses. Additionally, a fourth dataset captured the differences between period I (reduced) and period II (reduced) measures, referred to as the “Change” dataset to illustrate shifts in area-level SDoH over time. Table 1 presents a summary of the domains and constituent measures. 37 Seminal studies 43 44 informed the stepwise approach used to construct the OCOI ( Supplementary Appendix 2 ; available in the online version), the details of which are available elsewhere. 37
Table 1. Description of domain and variables used in OCOI construction.
| Domain | Constituent measure descriptions |
|---|---|
| Family stability | 1. Proportion of parents enrolled in Medicaid with a primary serious mental illness diagnosis |
| 2. Proportion of children living in a household with below-poverty income | |
| 3. Proportion of births that include no father's first/middle/last name | |
| 4. Proportion of families with a parent served by Medicaid who has an substance use disorder diagnosis | |
| 5. Labor market engagement index (HUD; reversed) | |
| Infant health | 1. Proportion of births that resulted in an infant mortality |
| 2. Proportion of Medicaid infants who had an injury or poisoning in the first year of life | |
| 3. Medicaid-enrolled infants with neonatal abstinence syndrome | |
| 4. Medicaid-enrolled infants with NICU stay | |
| 5. Proportion of infants born preterm | |
| 6. Medicaid children with six or more well-child visits in first 15 months of life (reversed) | |
| 7. Proportion of infants born to Medicaid-enrolled women with severe maternal morbidity | |
| Children's health (noninfant) | 1. Proportion of Medicaid-enrolled children ages 1–5 with a diagnosis of developmental delay including sight and hearing impairment |
| 2. Proportion of Medicaid children age 3–6 meeting continuous enrollment criteria with one or more well-child visits with a primary care physician (reversed) | |
| 3. Proportion of Medicaid-enrolled children ages 6–17 with a diagnosis of asthma | |
| 4. Proportion of Medicaid-enrolled children ages 6–17 with a diagnosis of mental illness | |
| 5. Proportion of Medicaid enrolled children ages 6–17 with a diagnosis of a developmental disability | |
| 6. Proportion of Medicaid enrolled children ages 6–17 with a diagnosis of diabetes | |
| 7. Proportion of Medicaid enrolled children ages 6–17 who received psychotropic BH medication | |
| 8. Proportion of Medicaid-enrolled children ages 6–17 with a diagnosis of obesity | |
| Access | 1. Proportion of Medicaid behavioral health visits for children that meet the access standards of CMS (reversed) |
| 2. Proportion of primary care visits for children that meet the access standards (driving time and driving distance) of CMS (reversed) | |
| 3. Geographic isolation (rurality) of the Census tract | |
| 4. Low transportation cost index | |
| 5. Percent occupied housing units in tract without a vehicle | |
| 6. Percent tract population within a distance from the supermarket | |
| 7. Distance to nearest elementary school | |
| Education | 1. Percent youth who have dropped out |
| 2. Percent of adults in the tract with more than high school education | |
| 3. Percent of youth (age: 5–17 years) not enrolled in school | |
| 4. Proportion of children not meeting third grade reading standards | |
| 5. Free lunch distribution (reversed) | |
| 6. Graduation rate (reversed) | |
| 7. School performance index (reversed) | |
| 8. School's value-added score (reversed) | |
| Housing | 1. Percentage putting 50% of income toward mortgage |
| 2. Percentage of households with less than one person per room | |
| 3. Percentage putting 50% of income toward rent | |
| 4. Percent housing identified as vacant | |
| 5. Percent renting | |
| 6. Percentage living in same housing unit for less than 1 year | |
| 7. Rate of evictions among renters | |
| Environment | 1. Tract land area not covered by vegetation |
| 2. Tract land area covered by open development (e.g., pavement, parking) | |
| 3. Percent of housing units constructed prior to 1980 | |
| 4. Annual average of daily pm25 measurements | |
| 5. Count of tobacco retail outlets within a 3/4 mile buffered tract boundary | |
| 6. Environmental health hazard index (air quality) | |
| Criminal justice | 1. Average number of homicide, assault, and sexual assault incidents per person reported to police each year during the period 2017–2018 |
| 2. The average number of robbery incidents per person reported to police each year during the period 2017–2018 | |
| 3. The average number of burglary, larceny-theft, and motor-vehicle theft incidents per person reported to police each year during the period 2017–2018 | |
| 4. The average number of drunkenness and driving under the influence incidents per person reported to police each year during the period 2017–2018 | |
| 5. The average number of drug crime incidents per person reported to police each year during the period 2017–2018 |
Abbreviations: BH, behavioral health; CMS, Centers for Medicare & Medicaid Services; HUD, Department of Housing and Urban Development; NICU, neonatal intensive care unit; OCOI, the Ohio Children's Opportunity Index.
Additional Area-Level Indicators
We used ACS data aggregated over two 5-year periods, 2010 to 2014 and 2013 to 2017, to obtain the race/ethnic distribution across census tracts in the state of Ohio. Our study visualized the percentage of White, Black, Hispanic individuals, and minority individuals in the state of Ohio.
User-Centered Informal Focus Group Discussions to Create Ohio Children's Opportunity Index Dashboards
We leveraged prior end-user feedback for the OOI dashboard. 45 We conducted informal focus group discussions with six end users to obtain feedback on the content, aesthetics, and function of the prototype dashboards (sample questions in the Supplementary Appendix 3 ; available in the online version). This process of prototyping the OCOI dashboard entailed reconciling iterative feedback from the end users. We repeated this cycle a minimum of two times or until saturation of feedback about the dashboard design was reached. 46 47
Use of Tableau to Visualize Ohio Children's Opportunity Index
ODM required the use of Tableau for constructing the dashboards. Tableau offers notable strengths over commonly used statistical software packages. Tableau uses VizQL, a visual query language that converts drag-and-drop actions into queries. Another advantage of Tableau is its ability to automatically recognize various geographical fields, like state, county, and ZIP code, to generate the corresponding latitude and longitude coordinates. We imported shape files of Ohio that had vector data for the latitude and longitude for each census tract, county, and neighborhood in Ohio. The OCOI dashboards in their current form are intended for project-affiliated researchers and end users and are therefore password protected on an online server. ODM intends to release public versions in the future.
Results
End-User Requirements
ODM requisitioned a dashboard similar to the OOI 45 48 (previously developed by our team) for the OCOI with the goal of having dashboards that were similar in aesthetics, content, and functionality. ODM had three additional requirements: visualization of change in OCOI based on data aggregated between period I and period II; grouping of census tracts into ZIP codes, neighborhoods, and cities, as end users tend to be more familiar with places in these terms rather than census tract numbers; and the creation of an additional dashboard to visualize OCOI and the race/ethnic distribution of the Ohio population. The dashboards were completed between January and December 2020 ( Fig. 1 ). Activities during April 2020 were suspended due to the novel corona virus disease 2019 (COVID-19) pandemic.
Fig. 1.
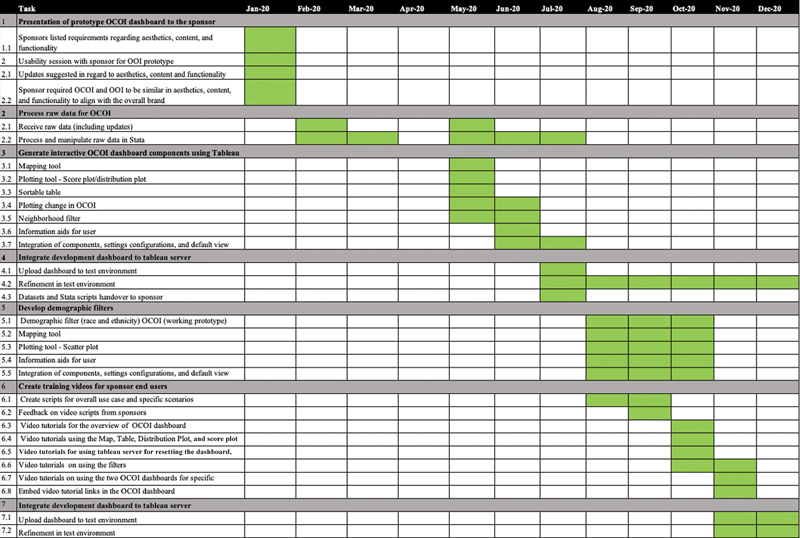
Key milestones and project timeline for the Ohio Children's Opportunity Index.
Iterative Feedback from Focus Group Discussions
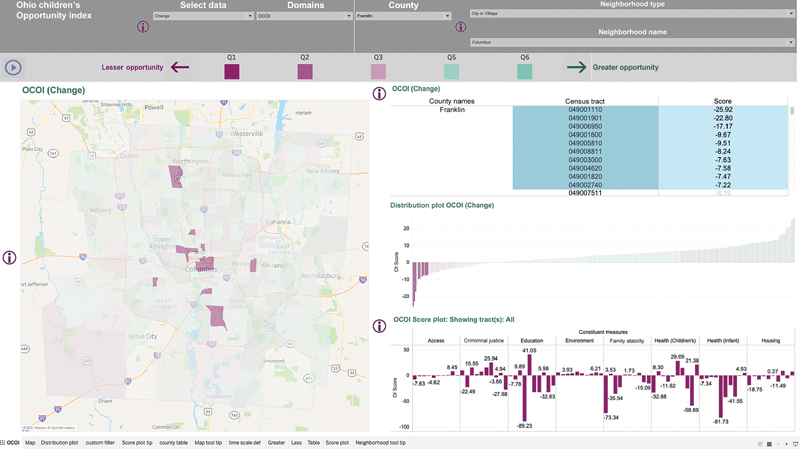
Our team applied prior end-user feedback on the OOI dashboard to the OCOI dashboard ( Fig. 2 ). 45 First, briefly, in terms of content, the OCOI like the OOI is a score of opportunity and not deprivation for easier interpretation and a positive connotation. Second, the scores are visualized as septile groups on a choropleth map of Ohio to provide adequate contrast between OCOI scores. Third, the dashboard displays the actual OCOI values on the Y-axis of the distribution plot to facilitate easier interpretation of the distribution of OCOI scores across census tracts. Further, a breakdown of the domain scores in the score plot as standard deviations from the mean for every census tract is included which facilitates detailed comparison between selected tracts. In regard to aesthetics, we retained the divergent color scheme for the map approved for the OOI dashboard. As in the OOI dashboard, the score plot is presented as a bar graph rather than a line plot to effectively communicate scores across domains or domain variables.
Fig. 2.

Ten lowest ranked census tracts in terms of the Ohio Children's Opportunity Index (OCOI) and Infant Health in Columbus, Ohio, United States,. ( A ) The ten lowest ranked census tracts in terms of OCOI in Columbus, Ohio, United States. ( B ) The ten census tracts with lowest OCOI in Columbus, Ohio, United States, in terms of the Infant Health domain and subdomains of Infant Health.
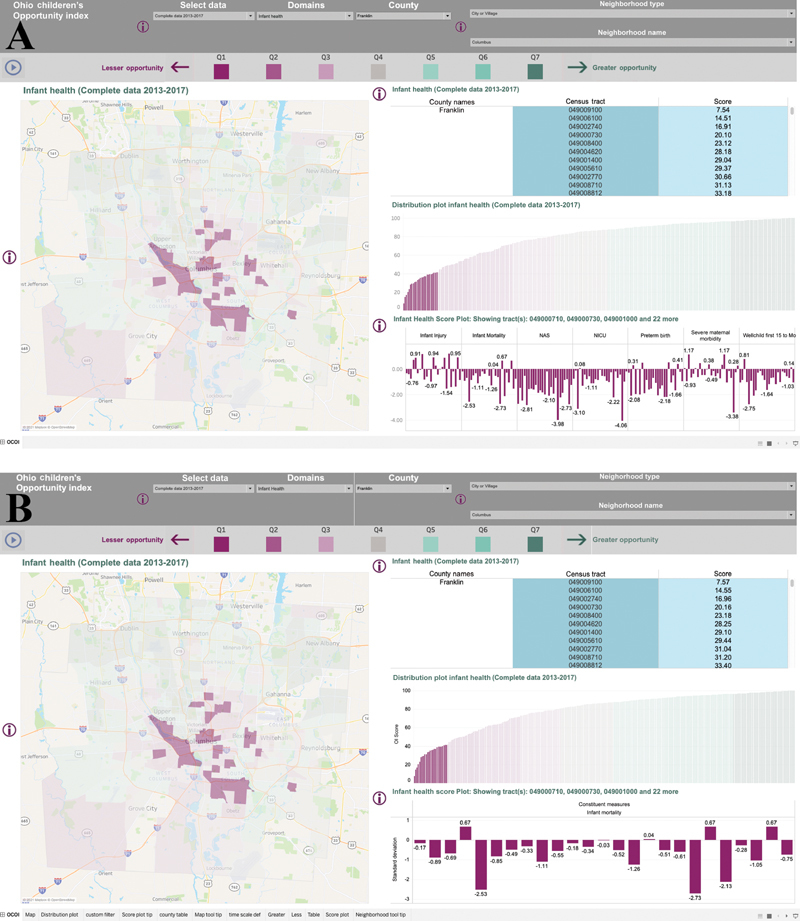
In terms of dashboard function, we displayed street and highway patterns to better orient the end users to the communities within a census tract. Further, users could select a county from a dropdown list to assess census tracts within a specific county. We also incorporated information icons by each dashboard component to aid the end user. We visualized change in OCOI score based on aggregate data between period I and period II. When users visualize change in OCOI, the distribution plot shows a distribution of income-adjusted differences in OCOI and absolute differences for the domains. The score plot displays absolute changes for OCOI domains and Z -scores for constituent measures ( Fig. 3 ). In terms of aesthetics, we ensured that the size of the map was sufficiently large to facilitate zooming in on a specific county.
Fig. 3.
Ten census tracts in Columbus, Ohio, United States, with the most negative change in the Ohio Children's Opportunity Index (OCOI).
To permit visualization of the OCOI and area-level race/ethnic distribution in Ohio, we created an additional dashboard following UCD. 36 Six end-users representing ODM participated in informal focus group discussions. For the race OCOI dashboard, the opportunity scores are visualized as quartiles using four newly approved colors that are accessible to people with colorblindness. While the components differ from the main OOI and OCOI dashboards, the layout, font size, map size, and other interactive features aligned with the overall vision for the Opportunity Index dashboards.
Dashboard Structure
The six components of the main OCOI dashboard were as follows: (1) choropleth map of Ohio with OCOI scores for specific census tracts; (2) filter for users to visualize the OCOI or any of its domains; (3) plots of OCOI and/or individual domain scores to compare relative positions for census tracts with the ability to sort scores and select specific variables within domains; (4) a sortable table to view OCOI or individual domain scores for specific census tracts; (5) information available from four data sources for users to select the reduced data compiled over two different time periods 2010 to 2014 and 2013 to 2017, complete data compiled from 2013 to 2017, change in OCOI and the individual domain scores between 2010 to 2014 and 2013 to 2017 based on the reduced dataset; and (6) a neighborhood filter that end users can use to filter census tracts corresponding to familiar geographies like cities, neighborhoods, or ZIP codes. These six components are interactive permitting an end user to select a city like Columbus, Ohio, United States, in the neighborhood filter, visualize the OCOI across all the census tracts in Columbus from 2013 to 2017, sort the tracts in ascending or descending order using the Table feature, select tracts of interest for visual analysis using the distribution plot, and compare the selected tracts in terms of the eight domains of the OCOI based on the score plot. This process can be repeated using each of the four datasets, for each of the domains of the OCOI, and for a variety of geographies like counties, cities, townships, and neighborhoods.
The race-OCOI dashboard also has the choropleth map of Ohio, filters for OCOI and its domains, choice of data sources, and the neighborhood filter from the main OCOI dashboard. Additional features include a menu with options to visualize the race/ethnic distribution; a scatter plot with OCOI and domain scores on the X-axis and the frequency of the race/ethnic distribution on the Y-axis, as well as the categorization of the OCOI score and the race/ethnic distribution into four discrete categories. The race OCOI dashboard can be adapted in the future to display information about other area-level indicators. Table 2 summarizes the modifications we made in response to feedback on the initial prototype.
Table 2. Modifications to OCOI—race dashboard based on end-user feedback.
| Modification | Rationale |
|---|---|
| Content | |
| •Creation of four categories for each race/ethnic group. These were 0 to 25, 25 to 50, 50 to 75, and >75% | Using quantiles to create categories for race/ethnic group gave rise to very skewed categories. Therefore, the categories requested by the end-user were created |
| •Switch from septile to quartile groups of the OCOI score to use in the state-level heat map | Using septile groups gave rise to too many categories and was visually busy. It was therefore decided that the quartile distribution was easier for interpretation |
| •Scatterplot of OCOI and its domain scores with the X-axis showing the OCOI scores and the Y-axis showing the frequency of the SDoH factor | The scatterplot allows the end users to see the scores for all census tracts at a glance. Each census tract is represented as a circle, which when selected highlights the census tract on the map |
| •Discrete categories represented as tiles showing 16 combinations of the four OCOI categories and the four SDoH factors and the number of census tracts with each combination | End users can at a glance see how many tracts have low opportunity and how many have high opportunity based on the race/ethnic distribution of the census tract |
| Function | |
| •Selection of county results by filtering dashboard content to only the census tracts within that county | This helped the end users specifically assess the census tracts within a county of interest |
| •Selection of neighborhood results by filtering dashboard content to census tracts within a city, neighborhood, or township | This helped end users find census tracts by specifying geographies that were more familiar to them such as the neighborhood, city, township, or ZIP codes |
| •Provide an information icon by each component to help the end user understand it | Provide end users with a conveniently located icon to quickly understand what the information a specific component can provide them, such as the source of the data |
| •Display street and highway patterns | Allow end users to get a better sense of the communities present within a census tract by locating them using streets and highways |
| Aesthetics | |
| •Use a divergent color scheme for the heat map | Attempts to preserve the color scheme used on the main dashboard proved inefficient because the original dashboard used three colors and the need was for four colors in the OCOI dashboard with other area-level indicators. We used shades of blue, orange, purple, and green. We avoided using certain shades of red and green to minimize the probability that end users would have trouble perceiving the colors |
| •Linking the color-coded tiles and the circles on the scatter plot | End users can select any combination of OCOI and area-level indicator of interest. This selection unselects all other census tracts from the scatter plot and at the same time highlights the census tracts in that particular category on the map. Alternatively, users can select any circle on the scatterplot and the selected tract is highlighted on the map and the color-coded tile that it corresponds to is highlighted as well |
Abbreviations: OCOI, Ohio Children's Opportunity Index; SDoH, social determinants of health.
Training Videos
Continuous improvements were made to the dashboard throughout this project but there is still a learning curve for those unfamiliar with data visualization tools. Therefore, we created training videos to help end users understand the basic functions of Tableau along with the displayed features of the OCOI. Training videos were developed by first obtaining feedback on the video scripts from the six end users. We created training videos on the following: the Tableau toolbar; the map feature; filtering the right data source, neighborhood, county, and measure of interest; and a video on sorting the information. The use of all these features was then illustrated as a case study of how the dashboards can be used by end users at ODM and community-based organizations. Sample scripts are available in Supplementary Appendix 4 (available in the online version).
Case Study
We present a case study where a health program manager in Columbus, Ohio, United States seeks to gain a better understanding of children's opportunity in tracts across Columbus with high infant mortality and high disparity in infant mortality between infants born to White and Black mothers. The health program manager has to strategically allocate resources to the Columbus area and wants to optimize them by identifying areas that have the lowest infant health scores and highest infant mortality rates.
Using the OCOI dashboard, the program manager selects Franklin County in Ohio and examines the Columbus area. They first examine the OCOI and its domains and note the 10 tracts with the lowest scores for all the domains ( Fig. 2A ). Because this program is targeting infant health disparities, they then examine the infant health domain. After looking at the 10 worst tracts for infant health, it is noted that many census tracts scoring low for infant health do not have significantly higher infant mortality, but their scores are low because of neonatal abstinence syndrome, maternal morbidity, neonatal intensive care unit stays, or other factors ( Fig. 2B ). Finally, in the score plot, the official clicks to keep only infant mortality to find the worst scoring tracts for infant mortality ( Fig. 4A ). They highlight the 25 worst ranked infant health scores in the table, and look at the score plot ( Fig. 4B ). They find that the two worst tracts for infant mortality, 049001400, and 049007511, are both in the South Linden area ( Fig. 5A ).
Fig. 4.
Twenty-five tracts with the lowest scores for the Infant Health in Columbus, Ohio, United States; ( A ) 25 of the lowest scoring census tracts in terms of Infant Health in Columbus, Ohio, United States; ( B ) 25 census tracts with the lowest scores for the Infant Mortality subdomain of the Infant Health domain of the Ohio Children's Opportunity Index (OCOI).
Fig. 5.
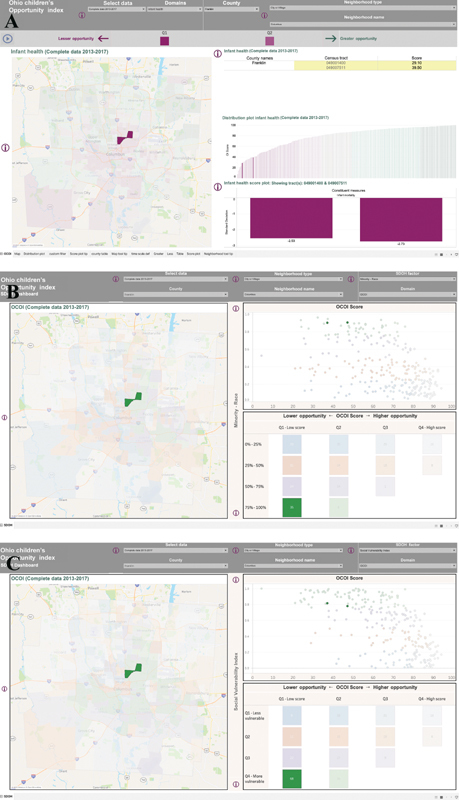
Two lowest-ranked census tracts in terms of Infant Mortality in Columbus, Ohio, United States. ( A ) The two census tracts ranked the lowest in terms of Infant Mortality in Columbus, Ohio, United States. (B) The race distribution for the two lowest-scoring census tracts in terms of Infant Mortality in Columbus, Ohio, United States, in the South Linden neighborhood.
The program manager decides to further examine the two lowest scoring tracts (049001400 and 049007511) which also score poorly for preterm birth but not on the other subdomains of infant health. Both tracts are in the lowest quantile of overall OCOI score, criminal justice, and education, and score poorly in regard to the constituent measures like food access, asthma, free lunch access, high school graduation rates, reading ability, amount of green area, air quality, tobacco exposure, paternal involvement, poverty, crowding, evictions, and percentage renting. The health program manager examines the race/ethnic makeup of the census tracts using the second OCOI dashboard. Both the census tracts have low opportunity scores and over 75% minority population ( Fig. 5B ). The health program manager decides to direct infant mortality prevention resources toward community-based organizations and public health programs in the South Linden area. Programs should be prepared to provide referrals for help in access to food, educational resources, social services, drug and tobacco cessation, and housing.
Discussion
Our team developed the OCOI dashboards following the 10 principles of UCD. 36 The OCOI dashboard visually summarizes and communicates quantitative information about SDoH through 53 measures organized into eight domains, showing opportunity for infants and children in the state of Ohio. This representation of SDoH can help characterize individual census tracts throughout the state and help policy makers, practitioners, and researchers assess their level of need.
In accordance with the UCD approach, 36 our team engaged end users at the beginning and throughout the project to understand their requirements, met regularly to obtain iterative feedback, defined the contexts for use, shared data and working prototypes with instructions for use with the end users, continuously refined the prototypes, and evaluated whether the dashboard met the end-users requirements. Involving end users and inviting qualitative feedback are associated with efficient and effective dashboards tailored to the population that will use them. 49 50 51 The design team and stakeholders included people with different kinds of expertise, including informatics experts, maternal and child health subject matter experts, scientific editors, and government employees that organize community health programs to ensure the tool would be accessible across users.
With the reorientation of the health care system on value-based integrated health care, the CDC developed a framework that conceptualizes integration across traditional clinical prevention, provision of services outside of the clinical setting, and the implementation of population or community-wide interventions. 52 PH 3.0 focuses on the latter two areas. 53 The requirements of PH 3.0 include engagement with public and private community stakeholders; innovative funding models; timely, granular, and actionable data; health department accreditation; and working to address “upstream” SDoH. 53 One key barrier to the PH 3.0 model is the availability of tools for data, analytics, and metrics. 54 The development and visualization of the OCOI is consistent with the infrastructure requirements for PH 3.0, 29 the information is as follows: geographically granular at the census tract level; reflects information from two time points; action-oriented as its appropriate use can influence allocation of resources spanning multiple sectors as noted in the case study; and is a representation of SDoH to promote health equity and will be available publicly in the future.
There are many geographic tools displaying deprivation across adult populations 10 11 12 13 14 15 16 but fewer focused on children. 55 56 The Opportunity Atlas, national in scope, shows the average outcomes in adulthood for people based on where they grew up with a greater focus on economic opportunity than health. 55 The Child Opportunity Index 2.0, comprises 29 indicators grouped into three domains (education, health and environment, social, and economic), available for all U.S. neighborhoods at the census tract level for the years 2010 and 2015. 56 Unlike the OCOI, the COI 2.0 has a national focus, the indicators used to construct the COI have varying weights, the environment domain includes toxic exposures like proximity to hazardous waste dump sites, and there is no separate criminal justice domain. The OCOI has more domains, change data, and more specificity to the state of Ohio, allowing state policymakers to have a deeper understanding of the distribution of opportunity.
Limitations
The OCOI has some notable limitations. This dashboard reflects average neighborhood measures and is thus subject to the ecological fallacy of assuming everyone in a tract and well characterized by average characteristics of the tract. Users should use caution against ignoring a problem because the average looks good or inundating an area with resources because an average looks bad. The OCOI sheds light on the distribution of opportunity across Ohio which we hope will be used for good. But as always, new knowledge can be used in a variety of ways, even harmful ones. All stakeholders are responsible for ensuring harmful uses (malicious or not) are discouraged which is a profound challenge to be addressed outside of the scope of this manuscript. Another limitation arises from the static nature of the data. Delays are introduced as the OCOI has to be reconstructed every time updated administrative data becomes available. Finally, indices like the OCOI may impact rural and urban areas in different ways, 57 and policymakers should take the constituent measures into account when developing interventions instead of attempting a one-size-fits-all approach for low domain scores.
Future Research
Future use of the OCOI will include monitoring change in neighborhood opportunity over time. Positive changes in opportunity in specific census tracts may point to improvements due to public health support, the actions of community programs, and movement of people and businesses to an area. Alternatively, decrease in opportunity due to crime, loss in property value, movement of residents, and closing of businesses, schools, and public buildings will also be reflected. Changes in SDoH may predict changes in health outcomes in an area. Researchers will be able to use the OCOI to study potential relationships between specific SDoH and infant and child health outcomes, further adding to public health knowledge about area-level predictors of health. ODM has been using the OCOI dashboard to carry out hot spotting for the distribution of the COVID-19 vaccines and lead screening. Renewed focus on the “place” effect on health has shifted the conversation to innovation in health care delivery and collaboration between healthcare organizations, public health, and social services.
Conclusion
The communication of OCOI through dashboard tools presents an opportunity to help increase awareness about pressing SDoH-related challenges faced by infants and children with potential, immediate, and long-term implications for their development and health. The dashboards facilitate analysis of information from multiple perspectives. Users of the dashboards can make informed decisions about allocating resources to individuals and their communities to ameliorate disparities in health care, with the goal of increasing health equity.
Clinical Relevance Statement
Even though universal and comprehensive screening for social determinants of health (SDoH) during the clinical encounter continues to be debated, 58 area-level measures of SDoH, like the OCOI, represent a rich resource of readily available data that can be incorporated into electronic health records and may be used to improve health care delivery. 59 60 For instance, tools, like the Population Health Assessment Engine (PHATE), combine data from the electronic health record and neighborhood characteristics to identify the geographic distribution of patients at risk of food insecurity. 61 Previously, systematic screening of mothers in the clinic for individual-level SDoH led to the receipt of more community resources to children and families. 62 Compiling a more complete picture of patients' neighborhood risk can help health care providers provide patients with more tailored assistance.
Multiple Choice Questions
-
What was the primary reason for including neighborhood filters with ZIP codes, cities, and neighborhoods on the two Ohio Children's Opportunity Index (OCOI) dashboards?
The information happened to be available
To allow for easier navigation for end users
The OCOI was recalculated at the ZIP code, city, and neighborhood levels
By popular demand
Correct Answer: The correct answer is option b. End users of the dashboard are likely to be more familiar names of neighborhoods, cities, and ZIP codes rather than census tracts. A neighborhood filter allows the end users to easily locate an area of interest for further exploration.
-
How was the change in OCOI score visualized on the Ohio Children's Opportunity Index dashboard?
Absolute difference
Standard deviations
Income adjusted difference
Logged values
Correct Answer : The correct answer is option c. End users of the dashboard are able to obtain more precise comparisons of OCOI change after income adjustments, which reflect differences in economic circumstances over time.
Conflict of Interest
None declared.
Funding Statement
Funding This study was funded by the Ohio Department of Medicaid.
Note
The project was administered by the Ohio College of Medicine Government Resource Center. The views expressed in this paper are solely those of the authors and do not represent the views of the Ohio Department of Medicaid (ODM). This study includes data provided by ODM which should not be considered an endorsement of this study or its conclusions.
Protection of Human and Animal Subjects
Our study was reviewed by our institutional review board and deemed exempt.
Supplementary Material
References
- 1.Selected KIDS COUNT Indicators for State in OhioAccessed August 21, 2021:https://datacenter.kidscount.org/data/customreports/37/any
- 2.The Ohio Department of Health The 2019 infant mortality reportAccessed August 21, 2021:https://odh.ohio.gov/wps/portal/gov/odh/know-our-programs/infant-and-fetal-mortality/reports/2019-Ohio-Infant-Mortality-Report
- 3.Braveman P, Egerter S, Williams D R. The social determinants of health: coming of age. Annu Rev Public Health. 2011;32:381–398. doi: 10.1146/annurev-publhealth-031210-101218. [DOI] [PubMed] [Google Scholar]
- 4.Marmot M, Allen J J. Social determinants of health equity. Am J Public Health. 2014;104 04:S517–S519. doi: 10.2105/AJPH.2014.302200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kirby R S, Delmelle E, Eberth J M. Advances in spatial epidemiology and geographic information systems. Ann Epidemiol. 2017;27(01):1–9. doi: 10.1016/j.annepidem.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 6.Diez Roux A V. New York, NY: Oxford University Press; 2018. Neighborhoods and Health. 2nd ed. [Google Scholar]
- 7.Diez-Roux A V. Bringing context back into epidemiology: variables and fallacies in multilevel analysis. Am J Public Health. 1998;88(02):216–222. doi: 10.2105/ajph.88.2.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blakely T A, Woodward A J. Ecological effects in multi-level studies. J Epidemiol Community Health. 2000;54(05):367–374. doi: 10.1136/jech.54.5.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Diez Roux A V. Neighborhoods and health: where are we and were do we go from here? Rev Epidemiol Sante Publique. 2007;55(01):13–21. doi: 10.1016/j.respe.2006.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Atkinson J, Salmond C, Crampton P.NZDep2013 index of deprivationAccessed December 15, 2021:https://www.otago.ac.nz/wellington/otago069936.pdf
- 11.McLennan D, Noble S, Noble M, Plunkett E, Wright G, Gutacker N.The English Indices of Deprivation 2019: technical reportAccessed December 15, 2021:https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/833951/IoD2019_Technical_Report.pdf
- 12.Singh G K. Area deprivation and widening inequalities in US mortality, 1969-1998. Am J Public Health. 2003;93(07):1137–1143. doi: 10.2105/ajph.93.7.1137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kind A JH, Buckingham W R. Making neighborhood-disadvantage metrics accessible - the neighborhood atlas. N Engl J Med. 2018;378(26):2456–2458. doi: 10.1056/NEJMp1802313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention CDC/ATSDR social vulnerability indexAccessed December 15, 2021:https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
- 15.Butler D C, Petterson S, Phillips R L, Bazemore A W.Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery Health Serv Res 201348(2, pt. 1):539–559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Delaney T, Dominie W, Dowling H.California healthy places index technical report (HPI 2.0)Accessed December 15, 2021:https://healthyplacesindex.org/wp-content/uploads/2021/04/HPI2Documentation2018-02-20-FINALrev2021-04-22.pdf
- 17.Phillips R L, Liaw W, Crampton P. How other countries use deprivation indices-and why the united states desperately needs one. Health Aff (Millwood) 2016;35(11):1991–1998. doi: 10.1377/hlthaff.2016.0709. [DOI] [PubMed] [Google Scholar]
- 18.Larson K, Halfon N. Family income gradients in the health and health care access of US children. Matern Child Health J. 2010;14(03):332–342. doi: 10.1007/s10995-009-0477-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Béatrice N, Lise G, Victoria Z M, Louise S. Longitudinal patterns of poverty and health in early childhood: exploring the influence of concurrent, previous, and cumulative poverty on child health outcomes. BMC Pediatr. 2012;12(01):141. doi: 10.1186/1471-2431-12-141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Probst J C, Barker J C, Enders A, Gardiner P. Current state of child health in Rural America: how context shapes children's health. J Rural Health. 2018;34 01:s3–s12. doi: 10.1111/jrh.12222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singh G K, Ghandour R M.Impact of neighborhood social conditions and household socioeconomic status on behavioral problems among US children Matern Child Health J 201216(01, Suppl 1):S158–S169. [DOI] [PubMed] [Google Scholar]
- 22.Jeon L, Buettner C K, Hur E. Family and neighborhood disadvantage, home environment, and children's school readiness. J Fam Psychol. 2014;28 05:718–727. doi: 10.1037/fam0000022. [DOI] [PubMed] [Google Scholar]
- 23.Caughy M O, Nettles S M, O'Campo P J.The effect of residential neighborhood on child behavior problems in first grade Am J Community Psychol 200842(1,2):39–50. [DOI] [PubMed] [Google Scholar]
- 24.Sampson R J, Sharkey P, Raudenbush S W. Durable effects of concentrated disadvantage on verbal ability among African-American children. Proc Natl Acad Sci U S A. 2008;105(03):845–852. doi: 10.1073/pnas.0710189104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chetty R, Hendren N, Katz L F. The effects of exposure to better neighborhoods on children: new evidence from the moving to opportunity experiment. Am Econ Rev. 2016;106(04):855–902. doi: 10.1257/aer.20150572. [DOI] [PubMed] [Google Scholar]
- 26.Hart J T.The inverse care law Lancet 19711(7696):405–412. [DOI] [PubMed] [Google Scholar]
- 27.Fiscella K, Shin P. The inverse care law: implications for healthcare of vulnerable populations. J Ambul Care Manage. 2005;28(04):304–312. doi: 10.1097/00004479-200510000-00005. [DOI] [PubMed] [Google Scholar]
- 28.Cookson R, Doran T, Asaria M, Gupta I, Mujica F P.The inverse care law re-examined: a global perspective Lancet 2021397(10276):828–838. [DOI] [PubMed] [Google Scholar]
- 29.Wang Y C, DeSalvo K. Timely, Granular, and Actionable: Informatics in the Public Health 3.0 Era. Am J Public Health. 2018;108(07):930–934. doi: 10.2105/AJPH.2018.304406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ohio Department of Health 2018 Infant Mortality ReportAccessed August 21, 2021 at:https://odh.ohio.gov/wps/portal/gov/odh/know-our-programs/infant-and-fetal-mortality/reports/2018-ohio-infant-mortality-report
- 31.Centers for Disease Control and Prevention Infant mortality rates by statesAccessed August 21, 2021:https://www.cdc.gov/nchs/pressroom/sosmap/infant_mortality_rates/infant_mortality.htm
- 32.Joshi A, Amadi C, Katz B, Kulkarni S, Nash D. A human-centered platform for HIV infection reduction in New York: development and usage analysis of the Ending the Epidemic (ETE) dashboard. JMIR Public Health Surveill. 2017;3(04):e95. doi: 10.2196/publichealth.8312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dowding D, Randell R, Gardner P. Dashboards for improving patient care: review of the literature. Int J Med Inform. 2015;84(02):87–100. doi: 10.1016/j.ijmedinf.2014.10.001. [DOI] [PubMed] [Google Scholar]
- 34.Wahi M M, Dukach N. Visualizing infection surveillance data for policymaking using open source dashboarding. Appl Clin Inform. 2019;10(03):534–542. doi: 10.1055/s-0039-1693649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nash D. Designing and disseminating metrics to support jurisdictional efforts to end the public health threat posed by HIV epidemics. Am J Public Health. 2020;110(01):53–57. doi: 10.2105/AJPH.2019.305398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Still B Crane K. CRC Press; 2017. Fundamentals of User-Centered Design: A Practical Approach. Boca Raton, FL. [Google Scholar]
- 37.Fareed N, Singh P, Jonnalagadda P, Swoboda C M, Odden C, Doogan N.Construction and validation of the Ohio Children's Opportunity Index. medRxiv 20212021.2005.2012.21257062 [DOI] [PMC free article] [PubMed]
- 38.Pearce A, Dundas R, Whitehead M, Taylor-Robinson D. Pathways to inequalities in child health. Arch Dis Child. 2019;104(10):998–1003. doi: 10.1136/archdischild-2018-314808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.The Area Based Analysis Unit of NS . Understanding patterns of deprivation. Regional Trends. 2009;41(01):93–114. [Google Scholar]
- 40.Smith T, Noble M, Noble S, Wright G, McLennan D, Plunket E.The English Indices of Deprivation 2015Accessed December 15, 2021:https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015
- 41.Centers for Disease Control and Prevention NCHHSTP Social Determinants of Health. Frequently asked questionsAccessed August 21, 2021:https://www.cdc.gov/nchhstp/socialdeterminants/faq.html
- 42.Seaman R, Riffe T, Leyland A H, Popham F, van Raalte A. The increasing lifespan variation gradient by area-level deprivation: a decomposition analysis of Scotland 1981-2011. Soc Sci Med. 2019;230:147–157. doi: 10.1016/j.socscimed.2019.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Noble M, Wright G, Smith G, Dibben C. Measuring multiple deprivation at the small-area level. Environ Plann A. 2006;38(01):169–185. [Google Scholar]
- 44.Exeter D J, Zhao J, Crengle S, Lee A, Browne M. The New Zealand indices of multiple deprivation (IMD): a new suite of indicators for social and health research in Aotearoa, New Zealand. PLoS One. 2017;12(08):e0181260. doi: 10.1371/journal.pone.0181260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Fareed N, Swoboda C M, Jonnalagadda P, Griesenbrock T, Gureddygari H R, Aldrich A. Visualizing opportunity index data using a dashboard application: a tool to communicate infant mortality-based area deprivation index information. Appl Clin Inform. 2020;11(04):515–527. doi: 10.1055/s-0040-1714249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Fusch P I, Ness L R. Are we there yet? Data saturation in qualitative research. Qual Rep. 2015;20(09):1408–1416. [Google Scholar]
- 47.Wu D TY, Vennemeyer S, Brown K. Usability testing of an interactive dashboard for surgical quality improvement in a large congenital heart center. Appl Clin Inform. 2019;10(05):859–869. doi: 10.1055/s-0039-1698466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ohio Opportunity Index Consortium The Ohio opportunity indexAccessed November 24, 2021:https://grc.osu.edu/Projects/OhioOpportunityIndex
- 49.Vázquez-Ingelmo A, Garcia-Peñalvo F J, Therón R. Information dashboards and tailoring capabilities - a systematic literature review. IEEE Access. 2019;7:109673–109688. [Google Scholar]
- 50.Yigitbasioglu O M, Velcu O. A review of dashboards in performance management: Implications for design and research. Int J Account Inf Syst. 2012;13(01):41–59. [Google Scholar]
- 51.Richter Lagha R, Burningham Z, Sauer B C. Usability testing a potentially inappropriate medication dashboard: a core component of the dashboard development process. Appl Clin Inform. 2020;11(04):528–534. doi: 10.1055/s-0040-1714693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Auerbach J. The 3 buckets of prevention. J Public Health Manag Pract. 2016;22(03):215–218. doi: 10.1097/PHH.0000000000000381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.DeSalvo K B, Wang Y C, Harris A, Auerbach J, Koo D, O'Carroll P. Public health 3.0: A call to action for public health to meet the challenges of the 21st century. Prev Chronic Dis. 2017;14:E78. doi: 10.5888/pcd14.170017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Meeting proceedings: Public Health 3.0 roundtable on data, metrics and predictive modelingAccessed December 15, 2021:https://www.healthypeople.gov/sites/default/files/PH3.0_Roundtable-Summary.pdf
- 55.Chetty R, Friedman J, Hendren N, Jones M R, Porter S.The opportunity atlas: mapping the childhood roots of social mobilityAccessed December 15, 2021:https://www.nber.org/papers/w25147
- 56.Noelke C, McArdle N, Baek M.Child opportunity index 2.0: technical documentAccessed December 15, 2021:http://new.diversitydatakids.org/sites/default/files/2020-01/ddk_coi2.0_technical_documentation_20200115_1.pdf
- 57.Fecht D, Jones A, Hill T. Inequalities in rural communities: adapting national deprivation indices for rural settings. J Public Health (Oxf) 2018;40(02):419–425. doi: 10.1093/pubmed/fdx048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Garg A, Boynton-Jarrett R, Dworkin P H. Avoiding the unintended consequences of screening for social determinants of health. JAMA. 2016;316(08):813–814. doi: 10.1001/jama.2016.9282. [DOI] [PubMed] [Google Scholar]
- 59.Jonnalagadda P, Swoboda C M, Fareed N. Using area-level measures of social determinants of health to deliver improved and effective health care. J Hosp Manag Health Policy. 2020 doi: 10.21037/jhmhp-20-100. [DOI] [Google Scholar]
- 60.Bazemore A W, Cottrell E K, Gold R. “Community vital signs”: incorporating geocoded social determinants into electronic records to promote patient and population health. J Am Med Inform Assoc. 2016;23(02):407–412. doi: 10.1093/jamia/ocv088. [DOI] [PubMed] [Google Scholar]
- 61.Lichkus J, Liaw W R, Phillips R L. Utilizing PHATE: a population health-mapping tool to identify areas of food insecurity. Ann Fam Med. 2019;17(04):372–372. doi: 10.1370/afm.2387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Garg A, Toy S, Tripodis Y, Silverstein M, Freeman E. Addressing social determinants of health at well child care visits: a cluster RCT. Pediatrics. 2015;135(02):e296–e304. doi: 10.1542/peds.2014-2888. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.