

Abstract
Objective:
To compare arch perimeter and teeth size, number, and shape between the two sides of the dental arch—the canine displacement side (DS) and the nondisplacement side (NDS)—in subjects with unilateral palatally displaced canine (PDC).
Materials and Methods:
Orthopantomograms (OPTs) of 240 subjects with unilateral PDC and 240 OPT matching controls were used. Additionally, study casts of 100 study subjects and 100 controls were used. The age of subjects ranged between 14 and 25 years. Dental casts were digitized and several parameters were recorded.
Results:
The transverse width from midpalatal line to the buccal segment and the palatal area on the DS was larger than that in the NDS (P < .05 to .001), with no difference in tooth size between both sides. Maxillary second premolars, canines, and lateral incisors in the PDC group were smaller than those in control group. Peg-shaped lateral incisors were significantly more frequent in the study group (P < .001).
Conclusions:
The transverse width of the DS was larger than that of the NDS. Both sides were generally smaller than those of the control group. Tooth size in the DS was comparable to that in the NDS but smaller than those of the control group. A missing or peg-shaped lateral incisor was the most common reported anomaly.
Keywords: Unilateral ectopic canine, Arch width
INTRODUCTION
The ectopic eruption of the permanent maxillary canine, whether it results in its subsequent impaction or displacement, is a frequently encountered clinical problem.1 Displacement or ectopic eruption of the canine was defined as divergence from the normal path of eruption; the canine can either erupt in an unusual position or become impacted buccally or palatally.2 It has been reported3 that the prevalence of palatally displaced canines (PDCs) is greater by an almost sixfold measure than labial/buccal displacement.
The etiology of PDC is obscure. Several etiological factors have been suggested,4–6 including arch dimension, mesiodistal width (MD-width) of teeth, tooth morphology, tooth size–arch length relationship, rate of root resorption of deciduous teeth, trauma of the deciduous tooth bud, disturbances in tooth eruption sequence, availability of space in the arch, rotation of tooth buds, and premature root closure.
With regard to arch dimension, some studies reported an association between maxillary excess and PDC7 and other studies reported an association between PDC and maxillary transverse deficiency,8 while still other studies9 reported no difference in arch width and controls. Crowding was reported only in a minority of PDC subjects. On the other hand, several studies10,11 reported excess dental arch space in subjects with PDC.
An association has been established between PDC and various tooth size and shape anomalies. These anomalies may include small or peg-shaped lateral incisors,12 congenitally missing teeth,13 reduced MD-width of maxillary and mandibular incisors,14 and several other features.
Late-developing dentition with insufficiently developed lateral incisors may affect the migration of the developing canine and result in its potential palatal impaction.11 Delayed dental development had also been linked to impacted canines.6
Although several studies have been conducted regarding anomalies associated with PDCs, no studies have been carried out to compare dentoalveolar and arch parameters between displaced (DS) and nondisplaced (NDS) canine sides in subjects with unilateral PDC. Accordingly, the aim of this study was to test the following null hypothesis: In subjects with unilateral PDC, the arch perimeter and teeth size, number, and shape of PDC side are not different from those of the NDS in the same subject.
MATERIALS AND METHODS
Records of 3000 patients available in the archive of the Dental Teaching Center/Jordan University of Science and Technology (JUST) were screened for the presence of unilateral PDC. Diagnosis of PDC was retrieved from patients' files as reported by the treating orthodontist with the aid of different methods, as appropriate (two periapical radiographs, an occlusal radiograph and periapical radiographs, or cone beam computed tomography scans, when needed). Records of patients with all types of PDCs, erupted or impacted, were involved. Ethical approval to access patients' records was obtained from the Institutional Research Board/JUST.
Study Group
Orthopantomograms (OPTs) of 240 subjects (180 females and 60 males) with unilateral maxillary PDC were used in this study to evaluate the prevalence of missing teeth in the study group (SG). Of those, the orthodontic study casts were available and in good condition for only 100 subjects (60 females and 40 males). These casts were used to measure tooth size and arch parameter. Ages of these subjects ranged from 14 to 25 years (with an average of 17.93 ± 2.56 years). All subjects were in their permanent dentition stage. However, some of subjects had their maxillary primary canine retained on the side on which the permanent canine was palatally displaced.
Control Group
The OPTs of 240 subjects (180 females, 60 males) with no maxillary canine displacement were selected as a control group (CG). They matched the SG by age, gender, and type of malocclusion. Age ranged from 14 to 25 years, with an average of 18.09 ± 2.39 years. The 100 casts in the SG were also matched with 100 casts for subjects (60 females, 40 males) from the CG by age, gender, and malocclusion.
In the SG, PDCs were found on the left side in 54 subjects and on the right side in 46 subjects. Accordingly, all measured variables from the casts of the CG were taken from the left side of 54 subjects and the right side of 46 subjects to correspond to the DS and from the contralateral side to correspond to the NDS.
Methods
Dental casts for subjects in the SG and CG were digitized using a scanner (HP Scanjet G4050, Hewlett Packard Company, Palo Alto, Calif). Images with 300-dpi resolution were obtained. The position of the dental casts on the scanner was established using a millimetric translucent paper designed specifically for this purpose.15 The transparent sheet was placed between the scanner glass surface and the occlusal plane of the dental cast so that the posterior edge of the dental cast would coincide with the abscissa axis (x). An ordinate axis (y) creating a Cartesian system was constructed by the perpendicular line on the x-axis passing through the midpoint between the two central incisors (Figure 1). For each cast image, 12 points were determined on the dental arch, representing the center of the clinical crown of incisors, canines, buccal cusp of premolars, and mesiobuccal cusps in the first molars, using special software (Curve Expert version 1.4, Hyams Development, URL: http://www.curveexpert.net/). The perpendicular distance to the midline from each point was analyzed to x and y components and measured in millimeters.
Figure 1. .
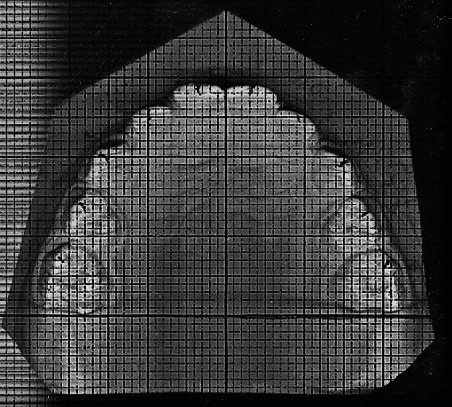
A representation of the Cartesian system and the x and y measurements corresponding to the points used to establish the dental arch form.
Measurements
Scanned images
Intercanine width. The intercanine width was measured between cusp tips of the right and left maxillary canines. The canine tip in the DS was allocated to the proposed correct canine position by bisecting the line connecting the lateral incisor and the first premolar. Additionally, the perpendicular distance from the cusp tip of each canine to the midpalatal line was measured.
Inter–first premolar width
The inter–first premolar width was measured between the cusp tips of the maxillary right and left first premolars. The perpendicular distance from the buccal cusp tip of each first premolar to the midpalatal line was measured.
Intermolar width
The intermolar width was measured between the mesiobuccal cusp tips of the maxillary right and left first molars. The perpendicular distance from the mesiobuccal cusp tip of each molar to the midpalatal line was also measured.
Palatal area
Measurements of x and y coordinates of the 12 points of each dental cast image were plotted to obtain the polynomial function that best described the curve corresponding to the dental arch form (Figure 2). Right and left halves of palatal areas were calculated using the same program.
Figure 2. .
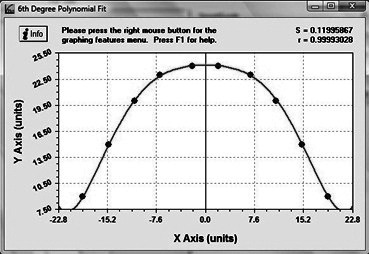
The curve generated using the function generated by the interpolation process.
Dental casts
Palatal depth. The palatal depth was measured as the perpendicular distance from the palatal vault opposite the first molars to a line connecting palatal points located on the first molar at the gingival level.16 An electronic sliding digital depth caliper with an accuracy of 0.01 mm and a steel pipe of 3-mm diameter with a sliding steel pin inside was used to perform depth measurements.
Anterior segment length
The length of a line from the maxillary canine cusp tip to the mesial tip of the central incisor17 was measured as the anterior segment length. For the DS, a constructed point in the line of the arch midway between the lateral incisor and the first premolar was considered.
Posterior segment length
The length of a line from the cusp tip of the maxillary canine to the mesiobuccal cusp tip of the first molar17 was considered as the posterior segment length.
MD-width of teeth
Tooth MD-widths were measured between the contact points using an electronic sliding caliper.
Space condition
Space condition was calculated by subtracting the total tooth size from the arch perimeter (anterior and posterior segment lengths). The MD-width of the PDC was estimated using Tanaka and Johnston's18 analysis for mixed dentition. Arch perimeter was measured by dividing the dental arch into four straight-line segments.17 An arch-length tooth-size discrepancy was not calculated for subjects with congenitally missing teeth.
Bolton ratios
Anterior and overall Bolton ratios were calculated for each group.19
Radiographs and dental casts:
The following anomalies were recorded: missing teeth, impacted teeth, peg-shaped laterals, dilacerated roots, and missing third molars.
Error of the Method
Twenty randomly selected casts were reanalyzed and the arch parameters were remeasured after a 1-month interval. Dahlberg's error ranged from 0.07 mm for maxillary central incisor width to 0.65 mm for space condition. Houston's coefficients of reliability were above 90%.
Statistical Analysis
Data analysis was carried out using SPSS computer software (SPSS 17.0, SPSS Inc, Chicago, Ill). Means and standard deviations (SDs) were calculated for the measured variables. The t-test was used to compare the arch parameters in DS and NDS in each group and to compare the SG and CG. The chi-square test was employed to investigate if there are differences in the frequency of dental anomalies between the two groups. The P value was set at the .05 level.
RESULTS
Maxillary Arch Dimensions
The means, SDs, and mean differences in maxillary arch dimensions between the DS and the NDS for the two groups are shown in Table 1.
Table 1. .
Means, Standard Deviations (SDs), and Mean Differences of the Maxillary Dental Arch Dimensions Between the Displacement Side (DS) and the Nondisplacement Side (NDS) in Study and Control Groupsa

Arch Dimensions
In the PDC group, the palatal area (P < .001) and transverse width from the midpalatal line to the first premolar (P < .01) and molar teeth (P < .05) in the DS were larger than in the NDS. In the CG, no significant differences were detected between the two sides corresponding to the DS and NDS.
Comparing the DS in the SG to its corresponding side in the CG, the distances from the canine (P < .05) to the midline were shorter in the SG. The canine (P < .05), first premolar (P < .01), and first molar (P < .001) on the NDS in the SG were also at a shorter distance to the midline when compared to the corresponding side in the CG. The area of the DS in the SG was larger than that of its corresponding side in the CG (P < .001), while the area of the NDS was significantly smaller than its corresponding side in the CG (P < .001).
Total arch width and depth were smaller in the PDC group than similar values in the CG (P < .05 to <.001), except for the distance between the lateral incisors, for which no difference was noted (Table 2).
Table 2. .
Means, Standard Deviations (SDs), and Mean Differences Between Study and Control Groups Regarding the Maxillary Arch Dimensions and Space Conditiona

Tooth Size
No significant differences were detected in the size of teeth between the DS and the NDS for the PDC group (Table 3). However, small but significant differences in tooth size between the SG and the CG were detected. Maxillary second premolars, canines, and lateral incisors in the SG exhibited a smaller size than did those in the CG on both the DS and NDS (P < .05 to <.01).
Table 3. .
Means, Standard Deviations (SDs), and Mean Differences Between the Study and Control Groups in Terms of Teeth Sizea

Bolton Ratios and Space Condition
There was significantly more space available in the SG than in the CG. No significant differences were noted with regard to Bolton ratios (Table 2).
Dental Anomalies
Peg-shaped lateral incisor (35 teeth, 14.6%) and missing teeth (10.4%, including 11 lateral incisor teeth, eight lower and two upper second premolar teeth, three lower central incisor teeth, and one first upper premolar tooth) were the most common anomalies in the SG. A significant difference was found between the SG and the CG (P < .001) (Table 4).
Table 4. .
Number and Frequency of the Different Dental Anomalies in the Study and Control Groups

DISCUSSION
Several studies9,20,21 have been conducted to compare arch dimensions in subjects with PDC and normal subjects. No previous studies, however, compared dental arch dimensions between displacement and normal sides of unilateral PDC within the same individual.
In this study, the premolar and molar distance to the midline was significantly longer on the DS than on the NDS in the SG but not in the CG. A wider half of the arch on the DS might be explained by displacement of the midline toward the NDS by the ectopic canine. A point that should be taken into consideration is that as the result of a possible discrepancy in the mesiodistal molar position between the two sides (as a result of canine exclusion from the dental arch), the constructed Cartesian system might be skewed, thereby affecting this result, a point that could not be avoided. When the DS in the SG was compared with its corresponding side in the CG, however, the distance from the canine to the midline was smaller in the SG. The difference was small but significant. For the NDS, posterior arch width was smaller in the SG than in the CG. When the total maxillary width was compared between the SG and the CG, the SG exhibited smaller dimensions. An assumption can be made about underdevelopment of the alveolar ridge as a result of the displacement of the canine.21 McConnell et al.8 reported transverse maxillary deficiency in subjects with PDC. Additionally, Schindel and Duffy22 reported a higher frequency of unilateral PDC in subjects with transverse maxillary discrepancy than in their controls. On the other hand, Langberg and Peck9 observed no difference in the anterior and posterior maxillary arch widths between subjects with PDCs and a comparison sample. Saiar et al.20 suggested that maxillary skeletal width is not a primary contributing factor in PDC. Other authors23 reported that the anterior and posterior maxillary transverse dimensions were significantly greater in the PDC group than in their control. Differences in the results might be attributed to the sample characteristics or the method of measurement used.
The palatal area of the DS was significantly larger than that of the NDS in the SG. It could be speculated that this difference might have been caused by a displacement of the midline toward the NDS by the ectopic canine. Nevertheless, this difference should be looked upon carefully. Measuring the flat projection of a curved area, as in the palatal vault, might be questionable, taking into consideration the different height and inclination of the alveolar bone on the DS and the NDS.
The SG exhibited smaller arch depth than did the CG. Anic-Milosevic et al.21 found no significant difference between the PDC and the CG. This might diminish the role of palatal height in the etiology of PDC.21 On the contrary, a reduced palatal height might be referred to as an effect of canine displacement rather than a cause. Such an effect would be reflected as an alveolar ridge height underdevelopment.
No differences were recorded in tooth size between the DS and the NDS in the SG. However, lateral incisors, canines, and premolar teeth in the SG were smaller than their counterparts in the CG. Tooth size reduction has been reported24 as a characteristic associated with the PDC anomaly. On the other hand, Brenchley and Oliver25 suggested that PDCs were not associated with diminutive maxillary lateral incisors.
In agreement with other studies,9,11 in our study there was an association between PDC and a spaced dentition. Other studies,23 on the other hand, reported no difference in the degree of crowding or in the number of subjects with crowding between the PCD group and matched controls.
Peg-shaped lateral incisor was the most common anomaly in the unilateral PDC group, followed by missing teeth. Several studies20,21 reported a clear association between PDC and small-sized upper lateral incisors and anomalous or congenital tooth absence compared with the controls. Additionally, Baccetti12 reported that PDCs are genetically reciprocally associated with anomalies such as enamel hypoplasia, infraocclusion of primary molars, aplasia of the second premolars, and small maxillary lateral incisors.
All of the above factors, discussed as potential etiologies for explaining the occurrence of PDCs, explained only a small percentage of PDCs. The genetic theory for PDC, however, seems to explain a larger number of these displaced canines. In a review of the literature, Peck et al.26 stated that the evidence points to genetic factors as the primary origin of most palatal impactions, concluding that PDC appears to be a product of polygenic multifactorial inheritance.
CONCLUSIONS
The transverse width of the DS was larger than that of the NDS in the PDC group.
Total intercanine and intermolar widths were reduced in the unilateral PDC group compared to the controls.
No difference in tooth size between the DS and the NDS was noted in unilateral PDC.
The MD-width of teeth was reduced in PDCs compared to the controls.
In the PDC group, peg-shaped lateral incisor was the most common anomaly (15%), followed by missing teeth (10%).
Acknowledgments
This study was supported by a grant from the Deanship of Research/JUST (Reference 108/2010).
REFERENCES
- 1.Shah R, Boyd M, Vakil T. Studies of permanent tooth anomalies in 7886 Canadian individuals. J Can Dent Assoc. 1978;44:262–264. [PubMed] [Google Scholar]
- 2.Chaushu S, Bongart M, Aksoy A, Ben-Bassat Y, Becker A. Buccal ectopia of maxillary canines with no crowding. Am J Orthod Dentofacial Orthop. 2009;136:218–223. doi: 10.1016/j.ajodo.2007.10.047. [DOI] [PubMed] [Google Scholar]
- 3.Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987;91:483–492. doi: 10.1016/0889-5406(87)90005-9. [DOI] [PubMed] [Google Scholar]
- 4.Bishara S. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992;101:159–171. doi: 10.1016/0889-5406(92)70008-X. [DOI] [PubMed] [Google Scholar]
- 5.Peck S, Peck L, Kataja M. Concomitant occurrence of canine malposition and tooth agenesis: evidence of orofacial genetic fields. Am J Orthod Dentofacial Orthop. 2002;122:608–613. doi: 10.1067/mod.2002.129915. [DOI] [PubMed] [Google Scholar]
- 6.Naser D, Abu Alhaija E, Al-Khateeb S. Dental age assessment in patients with maxillary canine displacement. Am J Orthod Dentofacial Orthop. 2011;140:848–855. doi: 10.1016/j.ajodo.2011.04.027. [DOI] [PubMed] [Google Scholar]
- 7.Kuftinec M, Stom D, Shapira Y. The impacted maxillary canine: I. Review of concepts. ASDC J Dent Child. 1995;62:317–324. [PubMed] [Google Scholar]
- 8.McConnell T, Hoffman D, Forbes D, Jensen E, Wientraub N. Maxillary canine impaction in patients with transverse maxillary deficiency. J Dent Child. 1996;63:190–195. [PubMed] [Google Scholar]
- 9.Langberg B, Peck S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am J Orthod Dentofacial Orthop. 2000;118:220–223. doi: 10.1067/mod.2000.104819. [DOI] [PubMed] [Google Scholar]
- 10.Jacoby H. The etiology of maxillary canine impactions. Am J Orthod. 1983;84:125–132. doi: 10.1016/0002-9416(83)90176-8. [DOI] [PubMed] [Google Scholar]
- 11.Zilberman Y, Cohen B, Becker A. Familial trends in palatal canines, anomalous lateral incisors, and related phenomena. Eur J Orthod. 1990;12:135–139. doi: 10.1093/ejo/12.2.135. [DOI] [PubMed] [Google Scholar]
- 12.Baccetti T. A controlled study of associated dental anomalies. Angle Orthod. 1998;68:267–274. doi: 10.1043/0003-3219(1998)068<0267:ACSOAD>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Peck S, Peck L, Kataja M. Prevalence of tooth agenesis and peg shaped maxillary lateral incisor associated with palatally displaced canine (PDC) anomaly. Am J Orthod Dentofacial Orthop. 1996;110:441–443. doi: 10.1016/s0889-5406(96)70048-3. [DOI] [PubMed] [Google Scholar]
- 14.Langberg B, Peck S. Tooth-size reduction associated with occurrence of palatal displacement of canines. Angle Orthod. 2000;70:126–128. doi: 10.1043/0003-3219(2000)070<0126:TSRAWO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Aljayousi M. Maxillary and Mandibular Dental Arch Forms in a Jordanian Population with Normal Occlusion [thesis] Irbid-Jordan: Jordan University of Science and Technology; 2009. [Google Scholar]
- 16.Laine T, Alvesalo L. Size of the alveolar arch of the mandible in relation to that of the maxilla in 45,X females. J Dent Res. 1986;65:1432–1434. doi: 10.1177/00220345860650121101. [DOI] [PubMed] [Google Scholar]
- 17.Proffit WR, Fields HW. Contemporary Orthodontics. St Louis, Mo: Mosby; 1992. [Google Scholar]
- 18.Tanaka MM, Johnston LE. The prediction of the size of unerupted canines and premolars in a contemporary orthodontic population. J Am Dent Assoc. 1974;88:798–801. [PubMed] [Google Scholar]
- 19.Bolton W. Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. Angle Orthod. 1958;28:113–130. [Google Scholar]
- 20.Saiar M, Rebellato J, Sheats R. Palatal displacement of canines and maxillary skeletal width. Am J Orthod Dentofacial Orthop. 2006;129:511–519. doi: 10.1016/j.ajodo.2005.03.021. [DOI] [PubMed] [Google Scholar]
- 21.Anic-Milosevic S, Varga S, Mestrovic S, Lapter-Varga M, Slaj M. Dental and occlusal features in patients with palatally displaced maxillary canines. Eur J Orthod. 2009;31:367–373. doi: 10.1093/ejo/cjp014. [DOI] [PubMed] [Google Scholar]
- 22.Schindel R, Duffy SL. Maxillary transverse discrepancies and potentially impacted maxillary canines in mixed-dentition patients. Angle Orthod. 2007;77:430–435. doi: 10.2319/0003-3219(2007)077[0430:MTDAPI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Al-Nimri K, Gharaibeh T. Space conditions and dental and occlusal features in patients with palatally impacted maxillary canines: an aetiological study. Eur J Orthod. 2005;27:461–465. doi: 10.1093/ejo/cji022. [DOI] [PubMed] [Google Scholar]
- 24.Oliver R, Mannion J, Robinson J. Morphology of the lateral incisor in cases of unilateral impaction of the maxillary canine. Br J Orthod. 1989;19:9–16. doi: 10.1179/bjo.16.1.9. [DOI] [PubMed] [Google Scholar]
- 25.Brenchley Z, Oliver R. Morphology of anterior teeth associated with displaced canines. Br J Orthod. 1997;24:41–45. doi: 10.1093/ortho/24.1.41. [DOI] [PubMed] [Google Scholar]
- 26.Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994;64:249–256. doi: 10.1043/0003-3219(1994)064<0249:WNID>2.0.CO;2. [DOI] [PubMed] [Google Scholar]