

Abstract
Objective:
To evaluate three-dimensional (3D) positional changes of an intruded tooth, a neighboring tooth, and a tooth connected to a mini-implant following intrusion of a single supraerupted molar, using a mini-implant with partial-fixed orthodontic appliances.
Materials and Methods:
The study consisted of 14 adult patients (two males and 12 females, mean age 41.9 years) with a supraerupted molar due to loss of an antagonist. Intrusion was performed using a mini-implant with a partial strap-up. The mean treatment time was 11.9 months, and the mean retention time was 23.3 months. To quantify the positional changes of the teeth, 3D models using a laser-based, dental scanning system and 3D software at pretreatment, posttreatment, and retention were oriented in a coordinate system and superimposed using nonmoved teeth as references. The changes on the x-, y-, and z-axes were measured at the tip of each cusp in the involved teeth.
Results:
A supraerupted molar was intruded by a mean amount of 1.35 ± 0.48 mm and was well maintained during the retention period. The overall change in the neighboring tooth was insignificant, although it showed opposite movement compared to the intruded tooth during the intrusion. The tooth connected to a mini-implant exhibited a secure anchorage.
Conclusion:
3D analysis showed the detailed positional changes of each tooth, and the involved molars were well maintained after intrusion.
Keywords: Supraerupted molar, Intrusion, Mini-implant, 3D analysis
INTRODUCTION
A supraerupted molar is one of the most common clinical findings in adult patients and is due to the consequences of not replacing a missing posterior tooth. While 18% of the patients have no demonstrable supraeruption, 82% may require clinical approaches before replacement of the lost tooth in the opposing arch because of interocclusal space challenges.1 In addition, supraeruptions greater than 2 mm occur in 24% of unopposed teeth.1 For treatment of supraerupted teeth, the most common conventional approach has been restoration in conjunction with intentional root canal treatment if needed.
Recently, however, orthodontic intrusion has gained wide acceptance because orthodontic temporary anchorage devices (TADS) can be a simple and easy means of treatment that doesn't require affecting multiple teeth or additional extraoral anchorage.2–5 Thus, because it is conservative, this approach can provide a valuable alternative as part of a interdisciplinary approach, although it takes additional time to intrude a molar.
There are two basic mechanisms to intrude a supraerupted molar using TADS: the direct and indirect methods. In the direct method, a mini-implant is directly connected to a target tooth using elastics and/or a coil spring for the intrusive force.2 Although the direct method provides absolute anchorage and predictable tooth movement, detailed tooth movement using an orthodontic appliance is nonetheless required in many cases during the later stages of tooth movement. In the indirect method, a mini-implant is connected to an adjacent tooth, which is similar to an ankylosed tooth.6 The tooth connected to a mini-implant appears to provide a strong and stable anchorage, so that orthodontic intrusion can be simultaneously performed with convenience since it can be localized and minimized.
Attempts to intrude teeth remain controversial because of the reaction of the surrounding tissues. Intrusion has been reported to cause loss of alveolar bone or formation of an angular bony defect.7,8 However, intrusion of periodontally damaged teeth improved the periodontal status under controlled inflammation.9 Another study has shown that pressure from the supra-alveolar fibers generated by the intrusion of the segmental molar induced remodeling of the alveolar bone.10 Moreover, a long-term study showed good periodontal status after intrusion of periodontally involved incisors if oral hygiene was well maintained.11
Two-dimensional (2D) studies using lateral cephalograms and parallel periapical radiographs evaluated positional changes of the tooth after intrusion using TADS.12–19 These 2D assessments, however, had difficulty evaluating three-dimensional (3D) dental movements, which may have caused errors associated with the measurement of small distances on the radiographs.20 Furthermore, detailed positional changes of each cusp in a tooth cannot be evaluated because of 2D limitations. Thus, recent advances in 3D analysis have been used for accurate assessment of positional changes after tooth movement.21 Stable structures, including the palatal surface and nonmoved teeth, facilitate accurate superimposition at different treatment time intervals. However, 3D analysis of tooth movement following intrusion of a single supraerupted molar using a mini-implant has not been performed yet. In addition, there is no information related to the positional changes of the neighboring tooth and the tooth connected to the mini-implant after the intrusion using a mini-implant with a partial appliance. Therefore, the aim of this study was to analyze the 3D positional changes of the intruded tooth, the neighboring tooth, and the tooth connected to the mini-implant following the intrusion of a single supraerupted molar using a mini-implant with partial-fixed orthodontic appliances, and to evaluate any positional change during the retention period.
MATERIALS AND METHODS
Fourteen patients (two males and 12 females; mean age, 41.9 years; range, 22–60.4 years) with a single supraerupted molar due to loss of an antagonist who were treated at the Division of Orthodontics in Ewha Womans University Mokdong Hospital (Seoul, Korea) were recruited for this study. The sample consisted of 14 extruded teeth, including six maxillary first permanent molars, five maxillary second permanent molars, two mandibular second permanent molars, and one maxillary first premolar. The intrusion criteria were as follows: molar intrusion attempted to create interocclusal space for adequate prosthodontic restoration; orthodontic treatment limited to the intrusion of a single extruded molar using TADS; no full-coverage restoration present on the intruded molar; the presence of 30% to 50% horizontal bone loss of a supraerupted molar with a healthy periodontal condition at pretreatment (T1), and maintenance of healthy periodontal conditions at posttreatment (T2) and retention (T3).
The average treatment duration was 11.9 months, with a range of 5 to 20 months, and the average retention period was 23.3 months, with a range of 12 to 35 months. The institutional review board approved the experimental protocol, and all subjects consented to participate.
Orthodontic Treatment Using the Indirect Method with TADS
A partially fixed, 0.022-inch slot, edgewise appliance was placed, and subsequently one mini-implant 1.2 mm in diameter and 6.0 mm in length (Jeil Corp, Seoul, Korea) was implanted onto the buccal alveolar ridges. A rigid 0.019″ × 0.025″ stainless steel wire was bonded to connect the mini-implant and buccal surface of the desired tooth (Figure 1a). In addition, tubes (0.018 × 0.022 inch) or lingual brackets were placed on the palatal (lingual) sides in order to avoid tipping (Figure 1b). The intrusion was undertaken with sequential wire changes using an intrusive force of about 20 g: 0.016″ nickel titanium (NiTi), 0.016″ × 0.022″ NiTi, 0.017″ × 0.025″ beta titanium alloy (TMA), and 0.019″ × 0.025″ stainless steel (SS). At completion of the intrusion, cusps on both the buccal and palatal sides of the intruded molar were well aligned and leveled to create an adequate interocclusal space (Figure 1c). The mini-implant and the appliance were removed after the implant prostheses on the opposing arch were installed (Figure 1d).
Figure 1. .
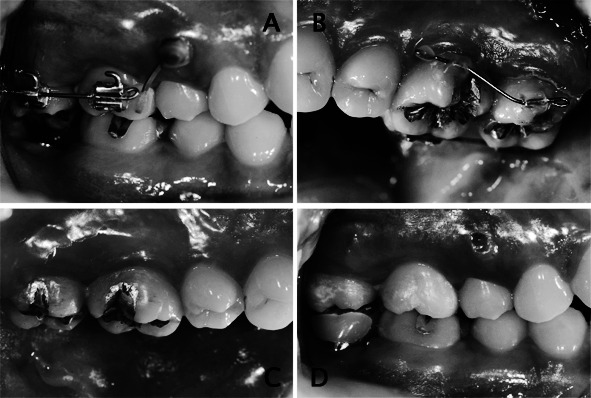
Intrusion process of the maxillary right second permanent molar, which was supraerupted due to the loss of an antagonist. (a) A mini-implant was placed between the maxillary right second premolar and the maxillary right first permanent molar and connected to the maxillary right first permanent molar, and orthodontic appliances were placed on the buccal side of the maxillary right first and second permanent molars. (b) Orthodontic appliances were placed on the palatal side of the maxillary right first and second permanent molars. (c) At the completion of intrusion, cusps on both buccal and palatal sides were well aligned and leveled to create an adequate interocclusal space. (d) After placement of the final restoration on the mandibular right second permanent molar, the mini-implant and orthodontic appliances were removed.
Measurement
To quantify the positional changes, the maxillary dental casts at T1, T2, and T3 were scanned by a laser-based, dental scanning system and virtually constructed with the 3Txer program (Orapix, Seoul, Korea). To determine the positional changes of the teeth, 3D models were oriented in a coordinate system, where the x-axis represented the buccopalatal plane, the y-axis the mesiodistal plane, and the z-axis the vertical plane. The anchored tooth was defined as the tooth connected to a mini-implant providing an indirect skeletal anchorage, and the neighboring tooth was defined as the tooth adjacent to the intruded tooth. For example, to intrude the maxillary first permanent molar, a mini-implant was placed between the roots of the maxillary second premolar and the maxillary first permanent molar, due to sufficient space between the roots, and then connected to the maxillary second premolar. In this case, the maxillary second premolar was defined as the anchored tooth, the maxillary first permanent molar as the intruded tooth, and the maxillary second permanent molar as the neighboring tooth. If the maxillary/mandibular second permanent molar needed to be intruded, the first permanent molar was the anchored tooth, and there would be no neighboring tooth. To compare the movement of the cusp tips, serial models were superimposed using teeth that were not involved in the orthodontic treatment as references. The changes on the x-, y-, and z-axes were measured at the tip of the mesiobuccal cusp, mesiopalatal cusp, distobuccal cusp, and distopalatal cusp of the molars as well as the buccal and palatal cusps of the premolars (Figure 2). The positive sign on the z-axis indicated intrusion, and the negative sign indicated extrusion. The positive sign on the x-axis indicated movement in the buccal direction, and the negative sign indicated movement in the palatal direction. The positive sign on the y-axis indicated movement in the mesial direction, and the negative sign indicated movement in the distal direction.
Figure 2. .
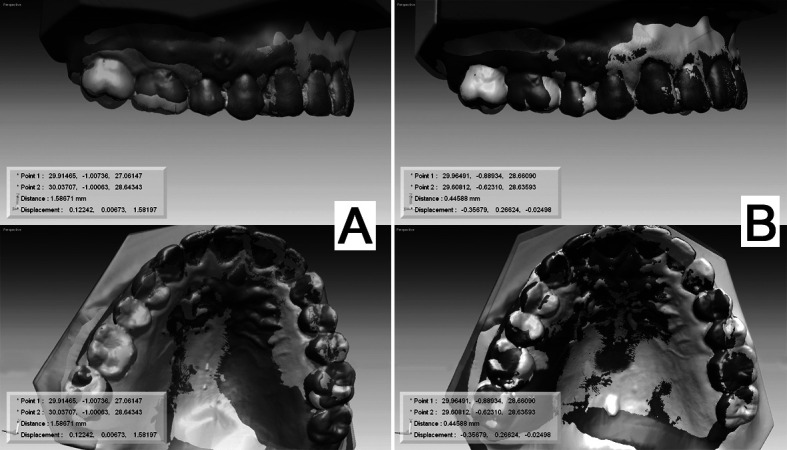
3D superimposition after intrusion of the maxillary first permanent molar. (a) Superimposition between pre- and posttreatment (T1–T2) at the mesiobuccal cusp of the maxillary right first permanent molar showed three values on the z-, x-, and y-axes. (b) Superimposition between post-treatment and retention (T2–T3) at the mesiobuccal cusp of the maxillary right first permanent molar showed three values on the z-, x-, and y-axes.
Statistical Analysis
A single examiner who was blinded to the treatment measured the 3D positional changes of the intruded, neighboring, and anchored teeth. To evaluate intra-examiner reproducibility, the same examiner remeasured values at T1, T2, and T3 for 90 randomly selected measurements after a 2-week interval. Language R22 was used to perform the data analysis. Paired t-tests were implemented to investigate the difference in the 3D positional changes between the T1 and T2 (T1–T2) and T2 and T3 (T2–T3) periods. The level of statistical significance was set at P < .05.
RESULTS
There was no statistically significant difference in the intra-examiner error at a 95% confidence level (P = .180). The intraclass classification coefficient for repeated measurements was 0.943. The value indicated a high reliability of the measurements.
There were no statistically significant differences either between the buccal and palatal cusps or between the mesial and distal cusps of the intruded tooth in the positional changes of the z-, x-, and y-axes (Tables 1 and 2). The same characteristics were found in the neighboring and anchored teeth (data not shown). Therefore, the combined data of all cusps in the involved teeth were used.
Table 1. .
The Positional Changes of Buccal and Palatal Cusps in the Intruded Tootha

Table 2. .
The Positional Changes of Mesial and Distal Cusps in the Intruded Tootha

The intruded tooth showed a mean intrusion (z-axis) of 1.35 ± 0.48 mm at T1–T2, which was statistically significant (Table 3 and Figure 3). The positional changes of the intruded tooth on the x-axis and the y-axis were 0.08 ± 0.96 mm and −0.02 ± 0.62 mm, respectively, at T1–T2. However, a high standard deviation in the positional changes on the x-axis and y-axis was observed at T1–T2.
Table 3. .
The Positional Changes of the Intruded, Anchored, and Neighboring Teeth Between T1–T2 and T2–T3a

Figure 3. .

Positional changes of the intruded, anchored, and neighboring teeth on the z-, x-, and y-axes.
Comparing T2 and T3, there were no statistically significant differences in the positional changes of the intruded tooth except for those on the x-axis.
The neighboring tooth had opposite movement on the z- and x-axes compared to the that of intruded tooth at T1–T2, meaning extrusive and palatal movements (Table 3 and Figure 3). On the other hand, the neighboring tooth exhibited opposite positional changes at T2–T3 compared to those at T1–T2, which were intrusive, buccal, and mesial movements. Thus, the positional changes between T1 and T3 were insignificant. As found in the intruded tooth, a high standard deviation in the positional changes was observed for the neighboring tooth at T1–T2.
The anchored tooth exhibited very slight positional changes in any direction at both T1–T2 and T2–T3 (Table 3 and Figure 3).
DISCUSSION
The present study showed that there were no significant differences in intrusion either between the buccal and palatal cusps or between the mesial and distal cusps of the intruded tooth. It indicated that the intrusion was achieved without tipping in any direction. A supraerupted molar was intruded at an average of 1.35 mm (z-axis), and the total movement length was 1.74 scalar (data not shown) in this study. This is consistent with the finding that 76% of supraerupted molars show less than 2 mm.1 In addition, some studies using 2D analyses showed that the amount of intrusion varied, ranging from 1.2 to 2.3 mm,12 1.8 mm,13 2.1 mm,14 2.4 mm,15 2.6 mm,16 3 mm,17 3.6 mm,18 and up to 5 mm.19 The different amounts of intrusion can be partly explained by the different required amounts of intrusion and/or the difference between 2D and 3D measurements. In addition, high variation on the x-axis and y-axis of the supraerupted molar at T1–T2 resulted from the different amounts of tilting before orthodontic treatment.
The intruded tooth was well maintained: −0.03 ± 0.19 mm on the z-axis, −0.16 ± 0.08 mm on the x-axis, and −0.11 ± 0.30 mm on the y-axis. This finding was consistent with other studies showing good stability after intrusion.17,23 However, relapse after intrusion has been reported in some studies, in which a 0.4-mm relapse occurred after a mean intrusion of 2.1 mm in a single supraerupted molar.14 The difference can be partly explained by either the use of a removable retainer or the 2D measurement in one study. Moreover, the bite force between a single intruded tooth and the prosthesis in the opposing arch after reconstruction of the proper occlusion appeared to be helpful for prevention of any extrusion. Only the fact that the positional change on the x-axis, which was movement toward the palatal side, was statistically significant implies that buccally tipped molars during intrusion could relapse. In some cases, buccal tipping of molars occurred during intrusion because the point of force application was on the buccal side of the molars, although orthodontic appliances were placed on the palatal sides to avoid tipping.
Based on the law of action and reaction, extrusion of the neighboring unit is expected during intrusion in conventional methods. In this study, the neighboring tooth showed extrusion and palatal movement, the opposite positional changes on the z- and x- axes, compared to that of the intruded tooth, although the amount appeared to be clinically insignificant. In addition, these positional changes at T1-T2 were reversed at T2-T3, leading to almost no net change at T1–T3. The presence of teeth in the opposing arch as well as a partial strap-up on both buccal and palatal sides appears to be beneficial for this insignificant positional change.
The anchored tooth, which is the tooth connected to a mini-implant, showed insignificant positional changes: 0.15 ± 0.28 mm on the z-axis, −0.02 ± 0.54 mm on the x-axis, and 0.08 ± 0.22 on the y-axis at T1–T2. This may imply that the anchored tooth provides a secure anchorage as long as a mini-implant remains stable and the connection between a mini-implant and the anchored tooth is tight.6 Further study with a large sample size is needed to verify the absolute anchorage of the anchored tooth in the absence of teeth in the opposing arch.
The average treatment duration in the present study was 11.9 ± 5.2 months. The treatment duration in this study appeared to be longer than that in other studies.12–19 The reason being this study included the intrusion of the mandibular molar, which took a longer time for complete intrusion compared to the maxillary molar due to the anatomical difference. It is also due to the loosening of a mini-implant, resulting in the displacement of the anchored tooth. Moreover, this study included a few cases in which the neighboring tooth, usually the maxillary second molar, was wedged under the distal height of the contour of the supraerupted molar, causing the prevention of intrusion. On the other hand, the patients' ages, ranging from 22 to 60.4 years, did not affect the average treatment duration (P = .667).
To assess the amount of intrusion, 3D analysis in this study provided detailed information related to the positional changes of all the cusps in the horizontal, transverse, and vertical directions. This made it possible to compare the positional changes of the buccal and palatal cusps of the molars, and those of the mesial and distal cusps of the molars in three directions, so that the characteristics of the tooth movement during intrusion can be identified. Further studies using a large sample size would be required to provide information related to the status of the surrounding tissues, which is still in controversy.
CONCLUSION
3D analysis showed the detailed positional changes of each tooth during intrusion: a supraerupted molar with successful intrusion, the neighboring tooth with insignificant positional changes, and the anchored tooth providing a secure anchorage.
During the retention period, the intruded molar was well maintained, and the neighboring and anchored teeth showed negligible positional changes.
REFERENCES
- 1.Kiliaridis S, Lyka I, Friede H, Carlsson GE, Ahlqvist M. Vertical position, rotation, and tipping of molars without antagonists. Int J Prosthodont. 2000;13:480–486. [PubMed] [Google Scholar]
- 2.Park YC, Lee SY, Kim DH, Jee SH. Intrusion of posterior teeth using mini-screw implants. Am J Orthod Dentofacial Orthop. 2003;123:690–694. doi: 10.1016/s0889-5406(03)00047-7. [DOI] [PubMed] [Google Scholar]
- 3.Chang YJ, Lee HS, Chun YS. Microscrew anchorage for molar intrusion. J Clin Orthod. 2004;38:325–330. [PubMed] [Google Scholar]
- 4.Yao CC, Wu CB, Wu HY, Kok SH, Chang HF, Chen YJ. Intrusion of the overerupted upper left first and second molars by mini-implants with partial-fixed orthodontic appliances: a case report. Angle Orthod. 2004;74:550–557. doi: 10.1043/0003-3219(2004)074<0550:IOTOUL>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Bae SM, Kyung HM. Mandibular molar intrusion with miniscrew anchorage. J Clin Orthod. 2006;40:107–108. [PubMed] [Google Scholar]
- 6.Yun SW, Lim WH, Chun YS. Molar control using indirect miniscrew anchorage. J Clin Orthod. 2005;39:661–664. [PubMed] [Google Scholar]
- 7.Reitan K. Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod. 1967;53:721–745. doi: 10.1016/0002-9416(67)90118-2. [DOI] [PubMed] [Google Scholar]
- 8.Ericsson I, Thilander B, Lindhe J. Periodontal conditions after orthodontic tooth movements in the dog. Angle Orthod. 1978;48:210–218. doi: 10.1043/0003-3219(1978)048<0210:PCAOTM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Melsen B, Agerbaek N, Eriksen J, Terp S. New attachment through periodontal treatment and orthodontic intrusion. Am J Orthod Dentofacial Orthop. 1988;94:104–116. doi: 10.1016/0889-5406(88)90358-7. [DOI] [PubMed] [Google Scholar]
- 10.Kanzaki R, Daimaruya T, Takahashi I, Mitani H, Sugawara J. Remodeling of alveolar bone crest after molar intrusion with skeletal anchorage system in dogs. Am J Orthod Dentofacial Orthop. 2007;131:343–351. doi: 10.1016/j.ajodo.2006.04.025. [DOI] [PubMed] [Google Scholar]
- 11.Re S, Corrente G, Abundo R, Cardaropoli D. The use of orthodontic intrusive movement to reduce infrabony pockets in adult periodontal patients: a case report. Int J Periodontics Restorative Dent. 2002;22:365–371. [PubMed] [Google Scholar]
- 12.Carrillo R, Rossouw E, Franco PF, Opperman LA, Buschang PH. Intrusion of multiradicular teeth and related root resorption with miniscrew implant anchorage. A radiographic evaluation. Am J Orthod Dentofacial Orthop. 2007;132:647–655. doi: 10.1016/j.ajodo.2006.08.017. [DOI] [PubMed] [Google Scholar]
- 13.Xun C, Zeng X, Wang X. Microscrew anchorage in skeletal anterior openbite treatment. Angle Orthod. 2007;77:47–56. doi: 10.2319/010906-14R.1. [DOI] [PubMed] [Google Scholar]
- 14.Heravi F, Bayani S, Madani AS, Radvar M, Anbiaee N. Intrusion of supra-erupted molars using miniscrews: clinical success and root resorption. Am J Orthod Dentofacial Orthop. 2011;139(suppl 4):S170–S175. doi: 10.1016/j.ajodo.2009.06.032. [DOI] [PubMed] [Google Scholar]
- 15.Baek MS, Choi YJ, Yu HS, Lee KJ, Kwak J, Park YC. Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. 2010;138:396.e391–e399. doi: 10.1016/j.ajodo.2010.04.023. [DOI] [PubMed] [Google Scholar]
- 16.Erverdi N, Keles A, Nanda R. The use of skeletal anchorage in openbite treatment: a cephalometric evaluation. Angle Orthod. 2004;74:381–390. doi: 10.1043/0003-3219(2004)074<0381:TUOSAI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Kuroda RS, Sakai Y, Tamamura N, Deguchi T, Takano-Yamamoto T. Treatment of severe anterior open bite with skeletal anchorage in adults: comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2007;132:599–605. doi: 10.1016/j.ajodo.2005.11.046. [DOI] [PubMed] [Google Scholar]
- 18.Erverdi N, Usumez S, Solak A, Koldas T. Noncompliance open-bite treatment with zygomatic anchorage. Angle Orthod. 2007;77:986–990. doi: 10.2319/101206-422.1. [DOI] [PubMed] [Google Scholar]
- 19.Umemori M, Sugawara J, Mitani H, Nagaka, Kawamura H. Skeletal anchorage system for openbite correction. Am J Orthod Dentofacial Orthop. 1999;115:166–174. doi: 10.1016/S0889-5406(99)70345-8. [DOI] [PubMed] [Google Scholar]
- 20.Mavropoulos A, Karamouzos A, Kiliaridis S, Papadopoulos MA. Efficiency of noncompliance simultaneous first and second upper molar distalization: a three-dimensional tooth movement analysis. Angle Orthod. 2005;75:532–539. doi: 10.1043/0003-3219(2005)75[532:EONSFA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Joffe L. OrthoCAD: digital models for a digital era. J Orthod. 2004;31:344–347. doi: 10.1179/146531204225026679. [DOI] [PubMed] [Google Scholar]
- 22.R Development Core Team. R A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2010. [Google Scholar]
- 23.Kuroda S, Sugawara Y, Tamamura N, Yamomoto TT. Anterior open bite with temporomandibular disorder treated with titanium screw anchorage: evaluation of morphological and functional improvement. Am J Orthod Dentofacial Orthop. 2007;131:550–560. doi: 10.1016/j.ajodo.2006.12.001. [DOI] [PubMed] [Google Scholar]