

Abstract
Objective:
To determine the effects of linear force vector(s) from interradicular miniscrews on the distalization pattern of the maxillary arch in adult Class II patients.
Materials and Methods:
Twenty-five adult patients with mild to moderate Class II dentition and minimal crowding were collected. Either single (group A, n = 12) or dual (group B, n = 13) miniscrews were inserted on the posterior interradicular area to deliver a distalizing force to the main archwire. The displacement patterns of maxillary incisors and molars were measured and compared.
Results:
Significant distalization in the molars and incisors was shown in both groups. Significantly greater distalization and intrusion of the first molar and intrusive displacement of the incisor, together with significant reduction of the mandibular plane, were noted in group B, in contrast to the rotation of the occlusal plane in group A.
Conclusions:
Interradicular miniscrews predictably induced total arch distalization, leading to the correction of Class II. Additional miniscrews in the premolar area appear to facilitate intrusion and distalization of the entire arch according to the position of the force vectors.
Keywords: Maxillary arch, Class II, Interradicular, Miniscrew, Distalization
INTRODUCTION
The application of monocortical miniscrew-type temporary anchorage devices (TADs) to various clinical situations demanding movement of either a single tooth or teeth segment has been largely successful, with the ease and minimal invasiveness at insertion and removal.1–3 The miniscrews placed at the interdental alveolar bone can deliver forces directly to the tooth or archwire, eliminating the need for additional connectors. This versatility of the miniscrews can be very helpful, especially for the posterior segment control, for which extraoral appliances used to be indicated.4,5 Additionally, the consistency of force may contribute to the predictability of outcome, unlike conventional extraoral appliances or intermaxillary elastics, which demanded the patients' compliance.6,7 In particular, use of extraoral appliances is not favored by adult patients.
The majority of Class II molar relationships tend to be accompanied with an underlying anteroposterior skeletal discrepancy, Class II canine relationship, and excessive overjet. With molar distalization being a prerequisite for nonextraction treatment of Class II patients, various intraoral appliances and techniques such as distalizing arches,8 distal jet appliances,9 and pendulum appliances,10 have been shown to be effective. Nevertheless, significant forward movement of the premolars and incisors was found to be inevitable in response to molar distalization.11,12 Once maxillary molars are distalized, they are prone to relapse during the retraction of premolars and incisors,13 making overcorrection of the molars to a Class III position crucial. In conventional Class II treatment, efficient treatment necessitated predictable molar distalization and subsequent incisor retraction without “burning anchorage.” In this regard, segmental distalization using either miniplates or miniscrews can be meaningful14,15 in that they could eliminate the possibility of round-tripping the anterior teeth. Accordingly, the possibility of en-masse distalization using interradicular miniscrews or miniplates has been proposed.16
Interradicular miniscrews allow immediate loading onto the main archwire,17 which is in contrast to miniplates or palatal implants that demand highly surgical procedures and/or fabrication of complex connecting parts.18 However, considering the relatively low magnitude of force that a miniscrew can withstand,19 empirical studies on the effectiveness of the use of interradicular miniscrew(s) for distalization of the entire arch have been scarce.
The purpose of this study was to investigate how single or dual interradicular miniscrews with respective linear force vectors would affect the amount and pattern of distalization of the maxillary arch in the Class II patients.
MATERIALS AND METHODS
Subjects
The subjects were selected among the patients at the Orthodontic Department at Yonsei University Dental Hospital according to the following criteria: (1) adult individuals with normal or mild skeletal Class II skeletal relationship, (2) no significant craniofacial defects or asymmetries, (3) intact maxillary permanent dentition including second molars, (4) moderate Class II occlusion, and (5) minimal crowding (<3 mm) in the maxilla. This study was performed with the permission of the University's ethical committee (institutional review board).
A total of 25 subjects (3 male, 22 female) were collected by one of the investigators who had not been informed of the purpose of this study regardless of the treatment outcome. Subjects were randomly allocated to either group A (12 patients, 1 male and 11 female, mean age 23.58 ± 6.92 years) or group B (13 patients, 2 male and 11 female, mean age 22.92 ± 7.1 years) (Table 1).
Table 1. .
Comparison of Pretreatment Age and Treatment Duration Between Group A (Single Miniscrew) and B (Dual Miniscrews)a

Appliances
All patients were bonded with preadjusted 0.018 × 0.025-inch slot edgewise appliances with Roth prescription (Tomy, Tokyo, Japan). Molar tubes were attached for identification of tooth position on the lateral cephalogram. Following initial leveling and alignment, a 0.016 × 0.022-inch stainless steel archwire was tied into the bracket-slots with wire ligatures.
In group A, miniscrews 7.0 mm in length, 1.8 mm in coronal diameter, and with a tapered body (Orlus 18107, Ortholution, Seoul, Korea) were inserted between the maxillary second premolar and first molar. In group B, additional miniscrews were placed between the maxillary first and second premolars (Figure 1). All miniscrews were inserted at the midpoint between adjacent teeth with 45° angulation relative to the occlusal plane and on the mucogingival junction.
Figure 1. .
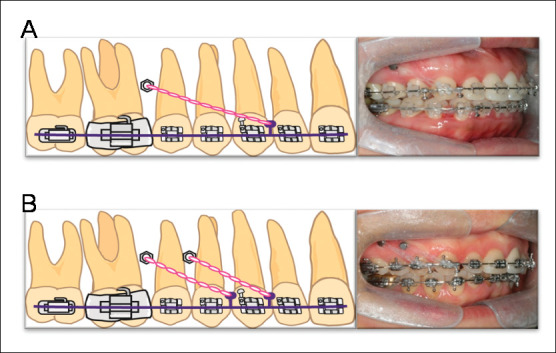
Schematic figure of appliances. (A) Group A. (B) Group B.
Crimpable hooks (TP Orthodontics, La Porte, Ind) were attached on the main archwire. Elastic chains (Ormco, Glendora, Calif) were stretched from each miniscrew head to corresponding crimpable hooks with a force magnitude of approximately 200 g each, meaning 400 g in each side of group B. Elastic chains were renewed every 4 weeks.
Cephalometric Measurements
Lateral cephalograms were taken before (T0) and after (T1) arch retraction using the Cranex3+ Ceph (Soredex, Milwaukee, Wis) machine. The V-Ceph software (Cybermed, Seoul, South Korea) was used to obtain cephalometric measurements. The radiographic magnification of the cephalograms was standardized as 100% of the actual size, with a 100-mm metal ruler image captured in the digital film as a reference.
Two reference lines were constructed for horizontal and vertical measurements.7,15 In the pretreatment lateral cephalogram, a line parallel to the initial occlusal plane (OP) was drawn through the anterior nasal spine (ANS), which was named the horizontal reference (HR) (Figure 2A). The pretreatment angle between the HR and the sella-nasion line (SN) was transferred to the posttreatment lateral cephalogram (Figure 2). In both pretreatment and posttreatment cephalograms, a line perpendicular to HR was drawn through the sella as the vertical reference line (VR).
Figure 2. .

Cephalometric measurements. (A) Linear. (B) Angular measurements.
Distal movement was measured perpendicular from the VR to the edge of the upper central incisor crown, and to the distal cusp tip of the upper first molar. Differences between T0 and T1 were calculated (T1–T0, Figure 2A). Intrusion was measured perpendicular from HR to the edge of the upper central incisor crown, and to the distal cusp tip of the upper first molar. Differences were calculated as described above (Figure 2A).
Angulation of the upper incisor and the molar relative to HR, and changes to the OP were also measured (Figure 2B). The vertical position of the miniscrew head from the OP and the angles between the vector and the OP were also measured in each group.
Statistics
All statistical analyses were performed using SPSS software (SPSS version 14.0, Chicago, Ill). With a 2-week interval, all cephalometric digitizing and analyses were repeated by the same examiner. Intraexaminer reliability was assessed using a paired sample t-test between the two sets of measurements, and no significant differences between the two sets were found.
The mean and standard deviation for each cephalometric variable were determined in each group. The Kolmogorov-Smirnov method was used to confirm the normal distribution of the measurements. A two-tailed paired t-test was then performed to determine the significance of treatment changes (T1–T0) in the groups. An unpaired t-test was performed to determine the differences of the two groups between T0 and T1. The statistical significance was determined at 5% confidence level.
RESULTS
A comparison of age at treatment start (T0) and of the duration of treatment showed no significant differences between the two groups (Table 1). Selected values for sagittal and vertical facial patterns were not significantly different between the two groups (Table 2).
Table 2. .
Comparison of Skeletal Measurements Before Retraction Treatment (T0) Between Group A (Single Miniscrew) and B (Dual Miniscrews)a

The overall success rate of the miniscrews during the given treatment time was 86.6% (66/76 screws), with 87.5% (21/24 screws) in group A, and 86.5% (45/52 screws) in group B. All failures were found near the end of distalization, possibly due to the root proximity.20 Replacement was made by placing the new miniscrew in the same interradicular area with 2-mm clearance from the initial insertion sites for the continuity of treatment. The success rate of the miniscrews in this study was comparable to previous reports, indicating that the attempt to move the total arch may not decrease the success rate of miniscrews.17,21,22
Statistically significant distal movement was achieved for all measured parameters (incisor crown, molar crown, and distal molar root) in both groups, indicating clinically meaningful total arch distalization, regardless of the number of miniscrews used. In the group comparison, significantly greater horizontal and vertical movement of the molar was noted in group B (Figure 3; Table 3). Horizontal incisor displacement did not show any statistical difference between groups (Figure 3; Table 3). Group B showed statistically significant intrusive displacement of the incisor tip, which was in contrast to extrusive changes to the incisor tip in group A. Slight distal or lingual tipping of both molars and incisors was found in both groups, with no significant differences between groups. Occlusal plane change was noted in both groups, according to the mean value, but there was no significance. Change in the SN-MP angle was significant in group B, indicating a vertical skeletal change related to intrusive displacement.
Figure 3. .
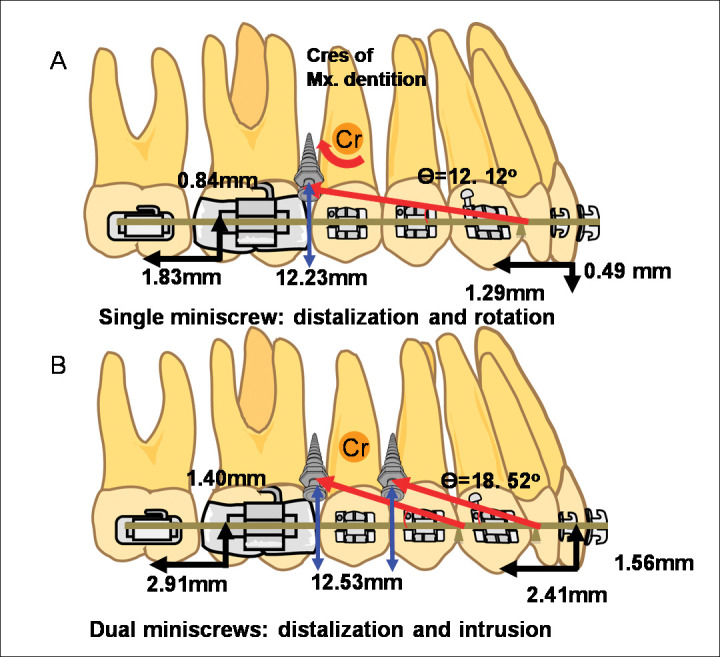
Schematized distalization pattern induced by force vector(s) from the miniscrews. (A) Group A indicating rotation of the occlusal plane. (B) Group B indicating intrusive movement of the dentition.
Table 3. .
Dental and Skeletal Measurements Before Total Arch Movement (T0) and Changes Due to Total Arch Movement (T1–T0) in Group A (Single Miniscrew) and B (Dual Miniscrews)a

In group A, the displacement of molars and incisors was correlated with treatment time, indicating that the amount of the displacement may be a function of treatment time, while group B exhibited a correlation between tooth displacement and skeletal change (Table 4).
Table 4.
Correlation Coefficient Between the Net Amount of Displacement and Skeletal Measurements/Treatment (Tx) Time in Each Groupa

DISCUSSION
Molar distalization in adults has been considered difficult, which is contrasted by recent evidence of molar distalization using miniplates fixed with multiple bone screws,14,23 with a major advantage being the elimination of side effects such as forward movement of premolars and incisors.11,12 This study was designed to clarify the clinical effect of multiple miniscrews implicating the change in both the direction and the magnitude of force vector(s) given to the arch.
Statistically significant distalization of molars and incisors was found in both groups (Table 3). The average amount of molar distalization in group A was comparable to or less than those in the previous studies.14,15,24 Greater molar distalization in group B may be related to double magnitude force from using dual screws, supporting the study of Oh et al.24 The prospective selection of subjects and individual variation caused by the cortical bone thickness, pattern of sinus pneumatization, and occlusal force25 may explain the discrepancy among studies. Considering the insufficiency of force from single miniscrew, the results of this study may reflect the practical outcome when using interradicular miniscrews for whole arch distalization, suggesting the use of dual miniscrews to achieve clinically meaningful distalization to correct end-to-end Class II molar relation. Furthermore, simultaneous incisor retraction in both groups is encouraging, indicating the elimination of round-tripping of the premolar and incisor segments exhibited by conventional intraoral distalizers.26,27 Simultaneous movement of the total arch using monocortical miniscrews may therefore be a strong treatment option for nonextraction treatment of Class II in terms of treatment efficiency.
Two subjects in group B required relocation of miniscrews due to proximity with the roots, without spontaneous failure. Apical tilting of the insertion path or approximating the miniscrew toward the tooth on the distal side may help in avoiding root contact.16 However, positioning of the interradicular miniscrews is still technique-sensitive. Moreover, interradicular miniscrews for the correction of a full cusp Class II relationship will inevitably need to be removed and reinserted during treatment,28,29 which can be cumbersome for both the operator and patient. Hence, this technique would well be indicated for the correction of end-to-end Class II, rather than full cusp Class II. It has been shown that the damage to the root surface by the titanium miniscrew during tooth movement is reversible.30 Therefore, distalization using interradicular miniscrews, once placed in appropriate positions, may be regarded as relatively safe.
Tipping of the molars was found to be minimal in both groups, with slightly less tipping in group B. This result was similar to that of other skeletal anchorage devices14 and in contrast to that of conventional distalizers.11 Considering that the translation of a single molar using palatal miniscrews usually takes high accuracy of appliance design,31 this consistent finding is inspiring. Choy et al.32 proposed that the tendency for tooth tipping is associated with the s2 value and demonstrated the increase of s2 according to the blunting of the root, implying greater resistance to tipping. A splinted whole arch with a rectangular stainless steel wire could be compared to an anteroposteriorly long segment, which is expected to show a higher s2 value and greater resistance to tipping than a single tooth. Taking all of this into consideration, the advantage of simultaneous distalization of the whole arch using interradicular miniscrews may surpass the risk of interradicular miniscrew insertion.
An interesting finding was the vertical displacement of the maxillary occlusal plane. While group A displayed a clockwise rotation of the occlusal plane, which was similar to Yamada et al.,15 group B showed significantly less rotation. The center of resistance of the maxillary dentition has been shown to be located around the middle area of premolar roots.33,34 Moreover, the vector angles in group B were measured higher than in group A (Figure 3; Table 2). Applying these notions to the nonextraction model, the force system in group B could induce intrusive translation of the whole arch (Figure 3; Table 3). Accordingly, the SN-MP angle was significantly reduced in group B. This whole arch intrusion was a novel finding in this study, implying that arbitrary arch rotation may be achievable by adjusting the amount and direction of force by changing the miniscrew position. Miniscrew position and number may be the determinants for selective vertical control for long face (Figure 4),7 unlike the conventional intrusion archwires causing extrusion of the posterior segment.35 However, selective intrusion of the incisor segment for gummy smile may be facilitated by the miniscrews inserted close to the incisors, according to our previous study.7
Figure 4. .

A case in group B demonstrating the reduction of anterior facial height.
The correlation pattern between the two groups (Table 4) reveal that the amount of tooth displacement is more related to the duration of retraction in group A, which implies that single miniscrews may take more time to achieve desired anteroposterior correction. In contrast, the effect of dual miniscrews appears to be influenced by other host responses such as bond quality.
Overall, it is conceivable from this study that the resultant pattern of maxillary arch displacement may be closely associated with the relationship between the center of resistance and the line of force. Due to force consistency and configuration of the arch segment, the clinical outcome is expected to be relatively consistent and less technique-sensitive.
CONCLUSIONS
According to the effects of linear force vector(s) from interradicular miniscrews on the distalization pattern of the entire maxillary arch in adult Class II patients:
Significant distal movement of the incisors and molars implies the simultaneous movement of the whole arch was observed in both groups.
The dual-screw group displayed significantly greater molar distalization and intrusion and incisor retraction than did the single-screw group.
Acknowledgments
This work was supported by Korea Research Foundation Grant funded by the Korean Government (KRF-2009-0075637).
REFERENCES
- 1.Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod. 1997;31:763–767. [PubMed] [Google Scholar]
- 2.Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchorage for treatment of skeletal Class I bialveolar protrusion. J Clin Orthod. 2001;35:417–422. [PubMed] [Google Scholar]
- 3.Lee KJ, Park YC, Hwang WS, Seong EH. Uprighting mandibular second molars with direct miniscrew anchorage. J Clin Orthod. 2007;41:627–635. [PubMed] [Google Scholar]
- 4.Park YC, Lee SY, Kim DH, Jee SH. Intrusion of posterior teeth using mini-screw implants. Am J Orthod Dentofacial Orthop. 2003;123:690–694. doi: 10.1016/s0889-5406(03)00047-7. [DOI] [PubMed] [Google Scholar]
- 5.Park HS, Lee SK, Kwon OW. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod. 2005;75:602–609. doi: 10.1043/0003-3219(2005)75[602:GDMOTU]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Upadhyay M, Yadav S, Patil S. Mini-implant anchorage for en-masse retraction of maxillary anterior teeth: a clinical cephalometric study. Am J Orthod Dentofacial Orthop. 2008;134:803–810. doi: 10.1016/j.ajodo.2006.10.025. [DOI] [PubMed] [Google Scholar]
- 7.Lee KJ, Park YC, Hwang CJ, et al. Displacement pattern of the maxillary arch depending on miniscrew position in sliding mechanics. Am J Orthod Dentofacial Orthop. 2011;140:224–232. doi: 10.1016/j.ajodo.2010.05.020. [DOI] [PubMed] [Google Scholar]
- 8.Muse DS, Fillman MJ, Emmerson WJ, Mitchell RD. Molar and incisor changes with Wilson rapid molar distalization. Am J Orthod Dentofacial Orthop. 1993;104:556–565. doi: 10.1016/s0889-5406(05)80439-1. [DOI] [PubMed] [Google Scholar]
- 9.Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod. 1996;30:374–380. [PubMed] [Google Scholar]
- 10.Fuziy A, Rodrigues de Almeida R, Janson G, Angelieri F, Pinzan A. Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2006;130:502–510. doi: 10.1016/j.ajodo.2004.12.031. [DOI] [PubMed] [Google Scholar]
- 11.Byloff FK, Darendeliler MA. Distal molar movement using the pendulum appliance. Part 1: clinical and radiological evaluation. Angle Orthod. 1997;67:249–260. doi: 10.1043/0003-3219(1997)067<0249:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Byloff FK, Darendeliler MA, Clar E, Darendeliler A. Distal molar movement using the pendulum appliance. Part 2: the effects of maxillary molar root uprighting bends. Angle Orthod. 1997;67:261–270. doi: 10.1043/0003-3219(1997)067<0261:DMMUTP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Cetline NM, Spena R, Vanarsdall RL. Orthodontics Current Principles and Techniques 3rd ed. St Louis, Mo: Mosby; 2000. [Google Scholar]
- 14.Sugawara J, Kanzaki R, Takahashi I, Nagasaka H, Nanda R. Distal movement of maxillary molars in nongrowing patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2006;129:723–733. doi: 10.1016/j.ajodo.2005.08.036. [DOI] [PubMed] [Google Scholar]
- 15.Yamada K, Kuroda S, Deguchi T, Takano-Yamamoto T, Yamashiro T. Distal movement of maxillary molars using miniscrew anchorage in the buccal interradicular region. Angle Orthod. 2009;79:78–84. doi: 10.2319/020408-68.1. [DOI] [PubMed] [Google Scholar]
- 16.Jeon JM, Yu HS, Baik HS, Lee JS. En-masse distalization with miniscrew anchorage in Class II nonextraction treatment. J Clin Orthod. 2006;40:472–476. [PubMed] [Google Scholar]
- 17.Miyawaki S, Koyama I, Inoue M, et al. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2003;124:373–378. doi: 10.1016/s0889-5406(03)00565-1. [DOI] [PubMed] [Google Scholar]
- 18.Wehrbein H, Merz BR, Diedrich P, Glatzmaier J. The use of palatal implants for orthodontic anchorage. Design and clinical application of the orthosystem. Clin Oral Implants Res. 1996;7:410–416. doi: 10.1034/j.1600-0501.1996.070416.x. [DOI] [PubMed] [Google Scholar]
- 19.Chung K, Kim SH, Kook Y. C-orthodontic microimplant for distalization of mandibular dentition in Class III correction. Angle Orthod. 2005;75:119–128. doi: 10.1043/0003-3219(2005)075<0119:CMFDOM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Kuroda S, Yamada K, Deguchi T, et al. Root proximity is a major factor for screw failure in orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2007;131(4 suppl):S68–S73. doi: 10.1016/j.ajodo.2006.06.017. [DOI] [PubMed] [Google Scholar]
- 21.Lim HJ, Eun CS, Cho JH, Lee KH, Hwang HS. Factors associated with initial stability of miniscrews for orthodontic treatment. Am J Orthod Dentofacial Orthop. 2009;136:236–242. doi: 10.1016/j.ajodo.2007.07.030. [DOI] [PubMed] [Google Scholar]
- 22.Park HS, Jeong SH, Kwon OW. Factors affecting the clinical success of screw implants used as orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2006;130:18–25. doi: 10.1016/j.ajodo.2004.11.032. [DOI] [PubMed] [Google Scholar]
- 23.Sugawara J, Daimaruya T, Umemori M, et al. Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004;125:130–138. doi: 10.1016/j.ajodo.2003.02.003. [DOI] [PubMed] [Google Scholar]
- 24.Oh YH, Park HS, Kwon TG. Treatment effects of microimplant-aided sliding mechanics on distal retraction of posterior teeth. Am J Orthod Dentofacial Orthop. 2011;139:470–481. doi: 10.1016/j.ajodo.2009.05.037. [DOI] [PubMed] [Google Scholar]
- 25.Sebaoun JD, Kantarci A, Turner JW, et al. Modeling of trabecular bone and lamina dura following selective alveolar decortication in rats. J Periodontol. 2008;79:1679–1688. doi: 10.1902/jop.2008.080024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Papadopoulos MA, Papageorgiou SN, Zogakis IP. Clinical effectiveness of orthodontic miniscrew implants: a meta-analysis. J Dent Res. 2011;90:969–976. doi: 10.1177/0022034511409236. [DOI] [PubMed] [Google Scholar]
- 27.Papadopoulos MA, Melkos AB, Athanasiou AE. Noncompliance maxillary molar distalization with the first class appliance: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2010;137:586.e1–586.e13; discussion 86–87. doi: 10.1016/j.ajodo.2009.10.033. [DOI] [PubMed] [Google Scholar]
- 28.Chung KR, Choo H, Kim SH, Ngan P. Timely relocation of mini-implants for uninterrupted full-arch distalization. Am J Orthod Dentofacial Orthop. 2010;138:839–849. doi: 10.1016/j.ajodo.2009.02.035. [DOI] [PubMed] [Google Scholar]
- 29.Choi YJ, Lee JS, Cha JY, Park YC. Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion. Am J Orthod Dentofacial Orthop. 2011;139:823–833. doi: 10.1016/j.ajodo.2009.07.026. [DOI] [PubMed] [Google Scholar]
- 30.Asscherickx K, Vannet BV, Wehrbein H, Sabzevar MM. Root repair after injury from mini-screw. Clin Oral Implants Res. 2005;16:575–578. doi: 10.1111/j.1600-0501.2005.01146.x. [DOI] [PubMed] [Google Scholar]
- 31.Kyung SH, Hong SG, Park YC. Distalization of maxillary molars with a midpalatal miniscrew. J Clin Orthod. 2003;37:22–26. [PubMed] [Google Scholar]
- 32.Choy K, Pae EK, Park Y, Kim KH, Burstone CJ. Effect of root and bone morphology on the stress distribution in the periodontal ligament. Am J Orthod Dentofacial Orthop. 2000;117:98–105. doi: 10.1016/s0889-5406(00)70254-x. [DOI] [PubMed] [Google Scholar]
- 33.Stockli PW, Teuscher UM. Combined activator headgear orthopedics. In: Graber TM, Vanarsdall RL, editors. Orthodontics Current Principles and Techniques 2nd ed. St Louis, Mo: Mosby; 1994. p. 448. [Google Scholar]
- 34.Jeong GM, Sung SJ, Lee KJ, Chun YS, Mo SS. Finite-element investigation of the center of resistance of the maxillary dentition. Korean J Orthod. 2009;39:83–94. [Google Scholar]
- 35.Burstone C. J. Biomechanics of deep overbite correction. Semin Orthod. 2001;7:26–33. [Google Scholar]