

Abstract
Objectives:
Posttraumatic stress disorder (PTSD) is characterized in part by negative alterations of cognition or mood, including alterations in emotional expressivity, or the extent to which one outwardly displays emotions. Yet, research in this area has relied on predominantly White samples and neglected to consider the potential role of gender, despite there being demonstrated gender differences in both PTSD symptom severity and emotional expressivity, separately. The goal of the current study was to fill a critical gap in the literature by examining the moderating role of gender in the relation between PTSD symptom severity and emotional expressivity in a sample of trauma-exposed Black adults.
Methods:
Participants were 207 Black individuals enrolled in a historically Black university in the Southern United States (68.6% female; Mage = 22.32 years).
Results:
Findings provided support for the moderating role of gender in the association between PTSD symptom severity and emotional expressivity. Specifically, greater PTSD symptom severity was inversely related to emotional expressivity among trauma-exposed Black males and positively associated with emotional expressivity among trauma-exposed Black females.
Discussion:
These results suggest the potential need for gender-specific assessment and treatment techniques for PTSD symptom severity among trauma-exposed Black college students.
Keywords: Trauma, posttraumatic stress disorder, emotional expressivity, gender differences, historically Black university
Trauma exposure is common among individuals in the United States, with a national prevalence rate of 89.7% (Kilpatrick et al., 2013). Trauma exposure has been linked to deleterious mental, physical, and behavioral health outcomes (Golding, 1999; Klonsky & Moyer, 2008; Norman et al., 2012), most notably the development of posttraumatic stress disorder (PTSD) symptoms (Kilpatrick et al., 2013). PTSD symptoms include intrusions (e.g., nightmares, flashbacks), avoidance of both internal (e.g., thoughts) and external (e.g., places) trauma-related stimuli, negative alterations in cognitions and mood (e.g., difficulty expressing positive affect, self-blame), and alterations in arousal and reactivity (e.g., hypervigilance; American Psychiatric Association [APA], 2013). PTSD symptoms are a serious clinical concern, associated with considerable functional impairment and high rates of co-occurring conditions (Goldstein et al., 2016). This research underscores the need for research on factors linked to the development, maintenance, and/or exacerbation of PTSD symptoms among trauma-exposed populations.
Theoretical and empirical literature has linked PTSD to emotional expressivity. Emotional expressivity refers to the behavioral changes (e.g., facial, postural) that typically accompany an emotion (e.g., crying, frowning; Kring et al., 1994). Existing cross-sectional research in predominantly White military samples has demonstrated that PTSD symptoms are associated with diminished emotional expressivity. For instance, Litz et al. (2000) found that predominantly White combat veterans with (versus without) PTSD exhibited suppressed physiological responses to negative and positive emotionally valenced images. Similarly, in a sample of predominantly White combat veterans, Roemer et al. (2001) reported that most exhibited strategic, or intentional, withholding of negative and positive emotions. Likewise, among trauma-exposed community individuals, PTSD symptoms are associated with elevated negative affect across a wide array of populations, including trauma-exposed Black college students (Boyraz et al., 2015). Tull et al. (2007) proposed that diminished negative and positive emotional expressivity may develop subsequent to PTSD symptoms as a means of dampening the effects of PTSD-related distress. However, these effects are likely only temporary, as reductions in emotional expressivity impede emotional processing, interfering with PTSD recovery in the long-term (Foa & Kozak, 1986). Thus, the effect of diminished emotional expressivity may be paradoxical, exacerbating PTSD symptoms in the long-term. In terms of positive emotional expressivity specifically, evidence suggests that individuals with more severe PTSD symptoms may be motivated to diminish any emotional experience, including that linked to positive emotions (Weiss et al., 2018; Weiss, Contractor, et al., 2020). For instance, through stimulus generalization, individuals may negatively evaluate physiological arousal originally linked only with trauma-related emotions that has generalized over time to other sources (e.g., negative or positive emotions), increasing efforts to down-regulate both negative and positive emotions (Weiss, Forkus, et al., 2020; Weiss et al., 2021).
In examining the relation between PTSD symptom severity and emotional expressivity, it may be important to consider the role of gender. Previous literature has found gender differences in PTSD symptom severity and emotional expressivity, separately. Regarding PTSD in a national study of United States adults, the lifetime prevalence was 12.8% in women, compared to 5.7% in men (Kilpatrick et al., 2013). One explanation for this difference is that women and men experience different types of trauma. For example, in a national study of United States adults, women were more likely to experience traumas that increase the likelihood of PTSD (e.g., sexual violence; Kilpatrick et al., 2013). In a qualitative review of research conducted over the past 25 years, Tolin and Foa (2006) alternatively suggested that higher rates of PTSD among women may be due to symptom presentation and reports during psychiatric evaluation. For instance, PTSD symptom presentation for women may be more recognizable, with past research across diverse samples of trauma-exposed individuals indicating that women are more likely to report sleep disturbances, difficulties with concentration, negative beliefs, anhedonia, and distress (Carragher et al., 2016; King et al., 2013; Murphy et al., 2019). Finally, there is evidence that college women from racially and ethnically diverse backgrounds are more likely to delay disclosure of their trauma, and delayed disclosure among women (but not men) has been shown to be associated with greater PTSD symptom severity (Ullman & Filipas, 2005).
In terms of gender differences in emotional expressivity, the literature has demonstrated that predominantly White college women generally express more negative and positive emotions than their male counterparts (Kring & Gordon, 1998). Predominantly White and Asian American male college students tend to inhibit both facial and verbal expressions of negative and positive emotions (Gross & John, 1998), with laboratory research in an international sample indicating that men are more likely to refrain from expressing facial cues of negative and positive emotions despite having a greater physiological response to arousal as compared to females (McDuff et al., 2017). Explanations for this phenomenon may have more to do with social constructs surrounding the expression of emotion (Block, 1973). Research among Black students shows that gender differences in emotional expressivity are socialized in accordance with display rules, or the social norms that dictate how, when, and why emotions can be expressed by men and women (Underwood et al., 1992). Gender-specific stereotypes about emotion are learned as early as pre-school age, with predominantly White samples of college students and children showing that young girls are encouraged to cry and show how they feel, while young boys are discouraged from expressing how they feel (Kuebli & Fivush, 1992). As documented in predominately White college students, the expression of emotions that are viewed as “unmanly,” such as sadness, shame, or fear, may lead men to be more negatively evaluated than women (Siegel & Alloy, 1990). It is therefore not surprising that men and women express emotions differently.
Despite evidence for gender differences in both PTSD symptom severity and emotional expressivity, separately, no studies have examined the moderating role of gender in their association. Additionally, as is noted in the above literature review, past studies exploring the relation between PTSD symptom severity and emotional expressivity, as well as the influence of gender on PTSD symptom severity and emotional expressivity, separately, have relied on predominantly White samples, limiting our ability to generalize across other racial groups. The absence of research in this area using non-White racial samples is particularly notable given evidence for racial differences in both PTSD symptom severity and emotional expressivity. Black individuals have the highest rate of PTSD (8.7%), significantly higher than the rates for White (7.4%), Hispanic (7.0%), and Asian (4.0%) individuals (Roberts et al., 2011). Differential exposure and differential vulnerability are two prominent theories that have been set forth to explain racial differences in PTSD symptom severity (Perilla et al., 2002). According to the differential exposure theory, Black individuals are at increased risk for trauma exposure, subsequently heightening their severity of PTSD symptoms. Yet, even when accounting for differences in demographic and trauma characteristics, Black individuals in a national sample of adults were more likely to develop PTSD as compared to other racial groups (Roberts et al., 2011). Alternatively, the differential vulnerability theory purports that Black individuals demonstrate more severe PTSD symptoms because they are more affected by stressors, regardless of the severity of their trauma exposure. For instance, Black individuals may not have equal access to economic and social resources that may buffer the impact of trauma exposure (Andrews et al., 2015; Norris et al., 1992). These findings highlight the importance of further examinations of trauma and PTSD symptom severity among Black individuals. Examination of PTSD within a sample of Black college students at a historically Black university is of particular importance because historically Black universities educate a higher percentage of low-income Black students and Black students from underserved communities as compared to predominately White institutions (Hardy et al., 2019; Walker, 2015). Black individuals from low-income households and underserved communities are at elevated risk for traumatic exposure and subsequent PTSD symptoms (Breslau et al., 1998).
Racial differences are also implicated in the literature on emotional expressivity. There is growing evidence that Black individuals are less likely to display outward expression of negative emotions (e.g., as evidenced among primary care patients; Brantley et al., 2002) and are more likely to engage in negative emotional restraint (e.g., women mammogram patients; Consedine et al., 2004). Family socialization of “appropriate” emotional displays may provide context for this difference. Previous literature has noted that Black parents often teach their children to suppress emotional expression and engage in emotional vigilance (Dunbar et al., 2017), perhaps due to racial biases that may lead individuals to view displays of emotion, particularly by Black males, as threatening (Thomas et al., 2009). Thus, the socialization of emotional expressivity may be an attempt by Black parents to help their children safely navigate social interactions (Dodge et al., 2005). Further, greater exposure to socioeconomic stressors have been purported to play a role in the socialization of emotion among Black individuals. According to the literature, psychological stressors associated with poverty may result in decreased tolerance of and support for Black children’s expression of negative emotion (Shaffer et al., 2012). Given that historically Black universities are constructed to provide a protective space for Black individuals, the need for emotional vigilance may be lower, thus resulting in a transient sense of safety (Albritton, 2012; Kennedy, 2012). This period of time may, consequently, provide more opportunities for emotional expressivity. These factors suggest the importance of research on emotional expressivity in Black individuals attending a historically Black university.
The current study addresses a critical gap in the research by examining the moderating role of gender in the relation between emotional expressivity and PTSD symptom severity among trauma-exposed Black college students attending a historically Black university. The decision to study the moderating role of gender stemmed from past literature supporting the moderating role of gender in relations between PTSD symptom severity and other emotion-based variables. For instance, Schick et al. (2020) found that PTSD symptom severity was significantly positively associated with positive emotional avoidance among men but not women. Conversely, Weiss et al. (2013) found that probable PTSD diagnosis (present/absent) was positively related to emotion dysregulation among women but not men. Given the dearth of research on the role of gender in relations between PTSD symptom severity and emotional expressivity, and the mixed findings for those few studies, we had no a priori hypotheses for the current study.
Methods
Participants & Procedures
All procedures were reviewed and approved by the University of Rhode Island’s Institutional Review Board. Data were collected as part of a larger study examining mental health and emotional responding among Black college students attending a historically Black university. An email was sent to instructors in the psychology department, at the University of Rhode Island, requesting study recruitment and data collection during a class period. The principal investigator (graduate student at the time) provided details about the study in classes. Interested students completed pencil-and-paper surveys in a group format and received course credit for their participation. The survey took approximately 30 minutes to complete. The sample for the present study was drawn from a larger sample of 258 undergraduate students from a historically Black university in the southern United States. Individuals were excluded if they (a) identified as a race/ethnicity other than Black (n = 13) or (b) did not endorse a trauma (n = 37). Thus, 207 trauma-exposed Black college students were included in the present study. Participants were primarily female (68.9%, n = 142) with a mean age of 22.32 years (SD = 5.44, range = 17–46). Most participants were unemployed (n = 113, 54.6%), and 94.7 % of participants were full-time college students (n = 196). See Table 1 for further demographic details for the total sample and by gender.
Table 1.
Descriptive characteristics in the total sample and by gender
| Total Sample (N = 207) | Male Subsample (N = 64) | Female Subsample (N = 142) | ||||
|---|---|---|---|---|---|---|
| M, SD, Range | n (%) | M, SD, Range | n (%) | M, SD, Range | n (%) | |
| 22.32, 5.44, 18–46 | 23.27, 6.49, 18–42 | 21.93, 4.87, 18–46 | ||||
| Gender a | ||||||
| Female | 142 (68.9%) | |||||
| Male | 64 (31.1%) | |||||
| Employment Status | ||||||
| Unemployed | 113 (54.6%) | 38 (59.4%) | 75 (52.8%) | |||
| Part-Time | 74 (35.7%) | 16 (25.0%) | 57 (40.1%) | |||
| Full-Time | 20 (9.7%) | 10 (15.6%) | 10 (7.0%) | |||
| Income b | ||||||
| Less than $9,999 | 30 (14.5%) | 8 (12.7%) | 22 (15.7%) | |||
| $10,000 to $19,999 | 28 (13.5%) | 9 (14.3%) | 19 (13.6%) | |||
| $20,000 to $29,999 | 37 (17.9%) | 10 (15.9%) | 27 (19.3%) | |||
| $30,000 to $39,999 | 17 (8.2%) | 4 (6.3%) | 13 (9.3%) | |||
| $40,000 to $49,999 | 21 (10.1%) | 6 (9.5%) | 14 (10.0%) | |||
| $50,000 to $59,999 | 13 (6.3%) | 5 (7.9%) | 8 (5.7%) | |||
| $60,000 to $69,999 | 18 (8.7%) | 7 (11.1%) | 11 (7.9%) | |||
| $70,000 to $79,999 | 10 (4.8%) | 5 (7.9%) | 5 (3.6%) | |||
| $80,000 to $89,999 | 7 (3.4%) | 1 (1.6%) | 6 (4.3%) | |||
| $90,000 to $99,999 | 5 (2.4%) | 2 (3.2%) | 3 (2.1%) | |||
| $100,000 and more | 18 (8.7%) | 6 (9.5%) | 12 (18.6%) | |||
| College Status | ||||||
| Full-Time | 196 (94.7%) | 62 (96.9%) | 133 (93.7%) | |||
| Part-Time | 11 (5.3%) | 2 (3.1%) | 9 (6.3%) | |||
| Probable PTSD | ||||||
| No PTSD | 164 (79.2%) | 48 (75.0%) | 115 (81.0%) | |||
| PTSD | 43 (20.8%) | 16 (25.0%) | 27 (19.0%) | |||
| PTSD Severity | 30.77, 15.16, 17–81 | 32.29, 15.07, 17–69 | 30.07, 15.26, 17–81 | |||
| Emotional Expressivity | 50.54, 18.98, 7–99 | 47.39, 17.33, 7–80 | 52.11, 19.63, 11–99 | |||
| Total Lifetime Traumas | 9.83, 6.01, 1–17 | 10.66, 5.80, 1–17 | 9.51, 6.06, 1–17 | |||
| Index Trauma Type (% Interpersonal) | 161 (77.8%) | 52 (81.3%) | 109 (76.8%) | |||
Note. PTSD = posttraumatic stress disorder.
One missing case, utilized valid percentages.
Three missing cases, utilized valid percentages.
Measures
Lifetime Trauma Exposure.
Exposure to lifetime trauma was measured using the Life Events Checklist for DSM IV (LEC; Gray et al., 2004). The LEC is a 17-item self-report measure that assesses lifetime exposure to 16 traumas and includes one item assessing any other extraordinarily stressful lifetime event not captured in the first 16 items. For each item, the participant is asked to indicate if: (a) they personally experienced a trauma, (b) they witnessed a trauma, or (c) they learned about the trauma through other means. Participants who reported direct (i.e., the lifetime event personally happened to them) or indirect (i.e., they witnessed or learned of a lifetime trauma) exposure to at least one lifetime event were also asked to indicate which of the lifetime events was most traumatic (i.e., index trauma). They were also asked to indicate whether or not they experienced fear, helplessness, and/or horror as a result of their lifetime trauma. This measure was utilized to determine whether or not participants met DSM-IV Criterion A trauma exposure for PTSD (APA, 2000), which has been consistent with past research (Tull et al., 2007; Weiss et al., 2012), and thus were eligible for this study. To control for confounding variables, the following covariates were created utilizing this measure: (a) total number of lifetime traumatic events experienced by the participants, and (b) index lifetime trauma type (i.e., interpersonal vs. non-interpersonal). The total number of lifetime traumatic events covariate was created by summing the number of lifetime traumatic events experienced. The index lifetime trauma type covariate was created by recoding the index lifetime trauma to indicate whether it was interpersonal (i.e., items 6–9 and 11) or non-interpersonal (i.e., items 1–5, 10, and 12–17). The LEC has demonstrated convergent validity with measures assessing varying levels of exposure to traumas and psychopathology known to relate to trauma (Gray et al., 2004). Internal consistency in this sample was excellent (α = 0.95).
PTSD Symptom Severity.
PTSD symptom severity was measured by the PTSD Checklist – Civilian Version for DSM-IV (PCL-C; Weathers et al., 1993). The PCL-C is a 17-item self-report measure of severity of avoidance, hyperarousal, and re-experiencing symptoms of PTSD. Participants referred to the lifetime event that they rated as most stressful on the LEC when completing the PCL-C. Participants were asked to rate the extent to which each symptom had bothered them in the past month on a 5-point Likert-type scale (1 = not at all, 5 = extremely). Higher scores on the PCL-C indicated more severe PTSD symptoms, with a score of 44 or higher indicating a probable diagnosis of PTSD (Blanchard et al., 1996; Ruggiero et al., 2003). The PCL-C has been found to have excellent test-retest reliability and internal consistency in college students (Ruggiero et al., 2003). Internal consistency in this sample was excellent (α = .95).
Emotional Expressivity.
Emotional expressivity was measured by the Emotional Expressivity Scale (EES; Kring et al., 1994). The EES is a 17-item questionnaire assessing general emotional expressivity across manner of expression and valence of emotion (i.e., negative or positive). Participants were asked to rate the extent to which they outwardly expressed their emotions on a 6-point Likert-type scale (1 = never true, 6 = always true). Higher scores on the EES are associated with increased emotional expressivity. The EES has been found to demonstrate adequate discriminant, construct, and convergent validity (Kring et al., 1994). The EES is significantly correlated with spontaneous emotional expressiveness in the laboratory and has been found to have good test-retest reliability (Kring et al., 1994). Internal consistency in this sample was good (α = 0.87).
Demographics.
Participants reported on age, gender, race, ethnicity, employment, annual income, and student status.
Analytic Plan
As recommended by Tabachnick and Fidell (2007), all study variables were assessed for assumptions of normality, including any possible violations to skewness, kurtosis, or linearity. Following this, Pearson product-moment correlations were calculated to explore the bivariate association between PTSD symptom severity and emotional expressivity in the total sample and male and female subsamples. Then, the PROCESS SPSS macro (Hayes, 2012) was utilized to explore whether the unstandardized primary variables (i.e., PTSD symptom severity, gender, and their interaction) could predict emotional expressivity. The PROCESS procedures use bootstrapping methodology and ordinary least squares regression, which confers more statistical power than standard approaches to statistical inference (Edwards & Lambert, 2007; Weidemann et al., 2009) and do not rely on distributional assumptions. Bootstrapping was done with 1,000 random samples generated from the observed covariance matrix to estimate bias-corrected 95% confidence intervals (CIs) and significance values. As described by Aiken and West (1991), these methods produced regression slopes that were plotted at one standard deviation above and below mean levels of emotional expressivity. Follow-up analyses examined whether the slopes of the regression lines differed significantly from zero.
Results
Correlations among the Primary Variables
At zero-order, PTSD symptom severity was found to be non-significantly correlated with emotional expressivity in the total sample (r = 0.07, p = .33). Among the Black male subsample, PTSD symptom severity was significantly negatively correlated with emotional expressivity (r = −0.33, p = 0.01), whereas among the Black female subsample, PTSD symptom severity was significantly positively correlated with emotional expressivity (r = 0.22, p = 0.02).
Preliminary Analyses
A moderation analysis examined the main and interactive effects of PTSD symptom severity and gender on emotional expressivity (see Table 2). Both PTSD symptom severity, B = −0.28, SE = 0.12, t = −2.29, p = .02, 95% CI [−0.52, −0.04], and gender, B= −19.75, SE = 5.18, t = −3.81, p = .0002, 95% CI [−29.97, −9.52], were found to be significantly associated with emotional expressivity. Moreover, the interaction between PTSD symptom severity and gender was significant, B = 0.50, SE = 0.15, t = 3.37, p = .001, 95% CI [0.21, 0.79] (see Figure 1). The R2 increase due to the interaction was significant, ΔR2 = .06, F = 11.35, p =.001. Analysis of simple slopes revealed that the direction of the relation between PTSD symptom severity and emotional expressivity was significant and negative among Black males (+1 SD), B = −0.28, SE= 0.12, t = −2.29, p = 0.02, 95% CI: [−0.52, −0.04], and significant and positive among Black females (−1 SD), B = 0.22, SE = 0.08, t = 2.62, p = 0.01, 95% CI: [0.05, 0.39], providing support for moderation.
Table 2.
Moderation analyses examining the main and interactive effects of PTSD symptom severity and gender on emotional expressivity
| B | SE | t | p | 95% CI | R 2 | F | |
|---|---|---|---|---|---|---|---|
| 0.08 | 5.22* | ||||||
| PTSD Symptom Severity | −0.28 | 0.12 | −2.29 | .02 | −0.52, −0.04 | ||
| Gender | −19.75 | 5.18 | −3.81 | < .001 | −29.97, −9.52 | ||
| PTSD Symptom Severity x Gender | 0.50 | 0.15 | 3.37 | .001 | 0.21, 0.79 |
Note: PTSD = posttraumatic stress disorder.
p <.05.
Figure 1.
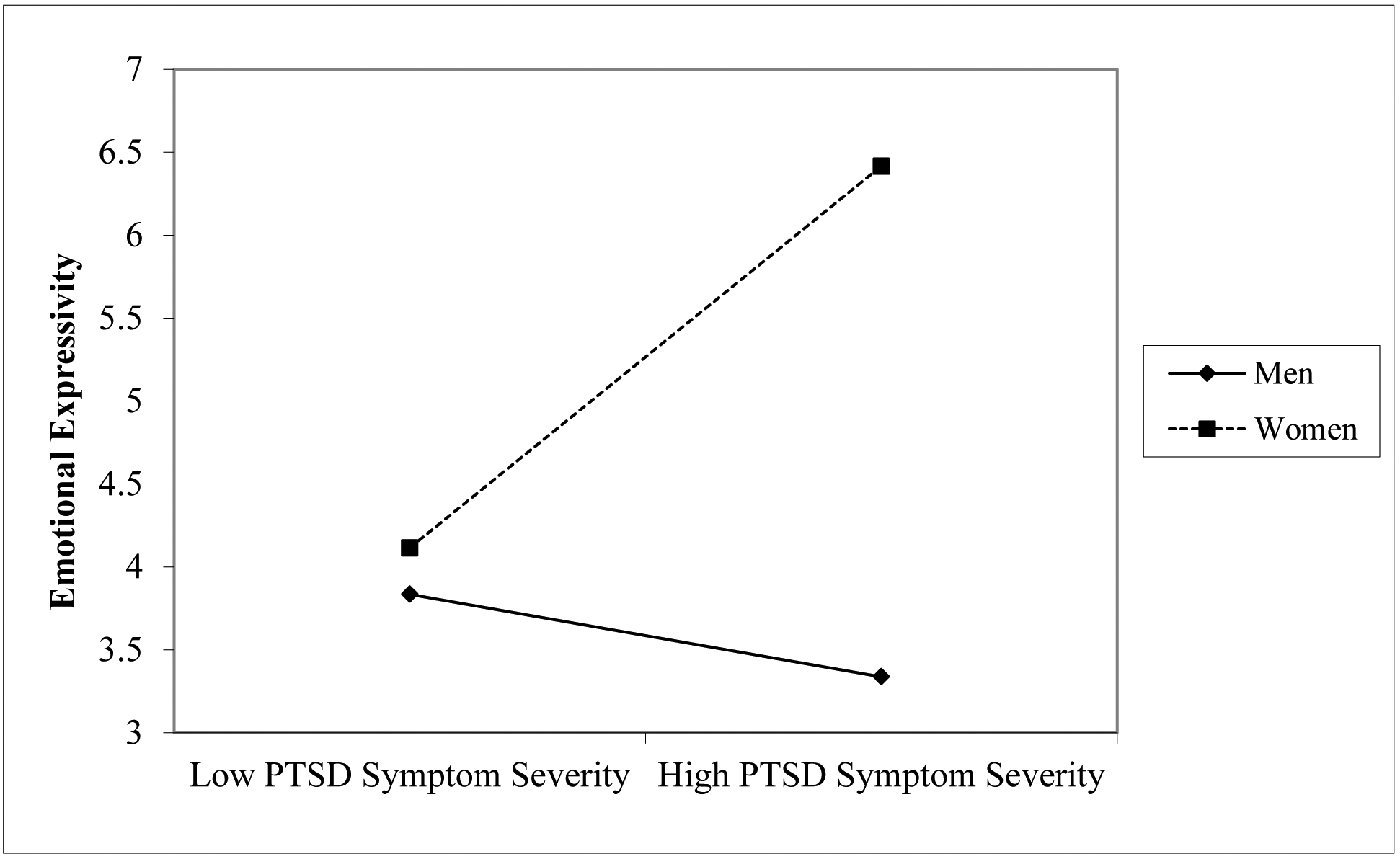
PTSD symptom severity by gender interaction for emotional expressivity
Note. PTSD = posttraumatic stress disorder.
Supplemental Analyses
To control for confounding variables, moderation analyses were re-ran adjusting for the total number of lifetime traumatic events and the index lifetime trauma type (i.e., interpersonal or non-interpersonal). In the adjusted analyses, neither the total number of lifetime traumatic events, B = 0.03, SE = 0.04, t = 0.72, p = 0.47, 95% CI [−0.05, 0.10], nor the index lifetime trauma type, B = −0.07, SE = 0.11, t = −0.69, p = 0.49, 95% CI [−0.29, 0.14], were significantly associated with emotional expressivity. In this adjusted model, the primary study results remained the same in strength and direction.
Discussion
The primary aim of this study was to examine the moderating role of gender in the relationship between PTSD symptom severity and emotional expressivity among trauma-exposed Black college students attending a historically Black university. Our results provided support for a significant interaction between PTSD symptom severity and gender on emotional expressivity. Specifically, the directionality of the relation between PTSD symptom severity and emotional expressivity was found to differ as a function of gender, such that this association was significant and positive for Black women and significant and negative for Black men. While preliminary, these findings suggest the potentially important role of gender in the link between PTSD symptom severity and emotional expressivity among trauma-exposed Black individuals.
Results of the moderation analysis indicated that Black women were more likely to express emotions when they endorsed higher (versus lower) PTSD symptom severity, whereas Black men were less likely to express emotions when they endorsed higher (versus lower) PTSD symptom severity. These results might be explained by theories regarding the socialization of emotional expression. Past research among predominantly White samples of college students and children has demonstrated that women are socialized from a young age to outwardly express negative and positive emotions, while men are often deterred from showing such emotions (Kuebli & Fivush, 1992). There is some evidence to suggest that this socialization practice may be even more predominant among Black individuals. For example, research has shown that Black individuals are more likely to be socialized in ways that result in reduced negative and positive emotional expressivity (Eid & Diener, 2001), with emotional displays being more likely to be minimized and punished (Halberstadt & Lozada, 2011). According to Nelson et al. (2012), Black men may be socialized to be even more restrictive of emotional expressions given the perception of more negative social consequences for these displays by Black men compared to Black women. These harsher socialization practices may stem from the disproportionately negative experiences that Black men face for displaying emotions (Gregory, 1997). Alternatively, it may be that Black men employ other coping mechanisms apart from outward expression of emotion to process distressing feelings, such as increased self-reliance (Levant & Richmond, 2007), substance use as a form as self-medication (Bonn-Miller et al., 2007; Ullman et al., 2013), and/or avoidance coping (Hayes et al., 1996). Investigations that further explain the relation between PTSD symptom severity and emotional expressivity among Black men and Black women are needed.
The findings of the current study suggest that the relationship between PTSD symptom severity and emotional expressivity may differ by gender among trauma-exposed Black college students attending a historically Black university. Specifically, the direction of this association was found to differ among Black men and Black women, such that Black men who were less outwardly expressive endorsed higher levels of PTSD symptom severity, whereas Black women who were more outwardly expressive endorsed higher levels of PTSD symptom severity. If replicated, these findings could have important implications for the assessment of PTSD symptom severity among Black men and Black women. For instance, our findings may suggest that Black men are less likely to display outward expressions of their emotions during evaluation, whereas Black women may be more likely to outwardly express their emotions. One potentially important implication then is that the degree of emotional expression during evaluation may not correspond with the severity of PTSD symptoms among both Black men and Black women. Specifically, outward emotional responses may be understated among Black men and exaggerated among Black women. Comprehensive and multimethod evaluation of emotional distress may allow for greater context when assessing PTSD symptom severity.
Although preliminary, our findings may also have implications for the prevention and treatment of PTSD among Black men and Black women. For instance, following traumatic exposure, the presence of more severe PTSD symptoms among Black men may result in greater emotional inexpressivity, which may maintain and exacerbate PTSD symptoms over time. Specifically, the suppression of emotional experiences may interfere with the ability to emotionally process a trauma, perhaps by increasing attentional bias toward trauma-related stimuli (Buckley et al., 2000); preventing habituation to fear responses associated with trauma such as the activation of the traumatic memory and the introduction of new information that is incompatible with the existing memory (Foa & Kozak, 1986); and/or interfering with the extinction of conditioned fear responses (McLaughlin et al., 2010). That said, one’s racial status cannot be ignored when considering the relation between PTSD symptom severity and emotional expressivity. Social racial bias plays a role in the way emotional expression among Black individuals is perceived by others, such that displays of negative emotional states in Black men are viewed as more threatening (Kang & Chasteen, 2009; Thomas et al., 2009). Moreover, there is evidence that Black men are more likely to suppress negative experiences during exchanges with individuals of other racial groups to reduce the likelihood of race-related discrimination (Dunbar et al., 2017). Thus, lack of emotional expression among Black men may be viewed as a way to navigate problems associated with racial discrimination and bias (Labella, 2018). Considering the findings of the current study in this context, Black men with greater severity of PTSD symptoms may have been employing adaptive tactics intended to reduce interracial tension. Thus, while emotional expressivity has been found to be generally associated with positive outcomes in other samples, our findings underscore the need for considering the social and racial contexts when teaching Black men with greater severity of PTSD symptoms skills for expressing their emotions. For instance, given strong evidence for the benefits of emotional expression in PTSD recovery (Foa & Kozak, 1986), it might be beneficial to encourage the expression of emotions within safe spaces, such as the home (Dunbar et al., 2017). This might include methods for emotional approach (see Gratz et al., 2014), or getting in touch with one’s emotions, such as through journaling and sharing emotional content with trusted people. Increased efficacy in expressing emotions broadly may generalize to trauma-specific emotions over time. Ecological investigations such as with experience sampling methods are needed to better understand the specific contexts in which emotional expression is adaptive and maladaptive for Black men and Black women. Finally, this knowledge may be important to identifying barriers to efficacious PTSD treatment, particularly salient to Black individuals who are less likely to complete (Lester et al., 2010) and respond to PTSD treatment (Sripada et al., 2019). Specifically, given above evidence that emotional expressivity is key to PTSD treatment, deficits in expressivity may predict treatment dropout or nonresponse.
Results should be considered within the context of study limitations. First, the cross-sectional and correlational nature of the data precludes causal determination of the associations examined. Future research is needed to investigate the nature and direction of these relations through prospective, longitudinal investigations, as it is possible that bi-directional relationships may exist between PTSD symptom severity and emotional expressivity. It is not clear whether PTSD symptom severity is a risk factor for emotional expressivity (i.e., PTSD symptom severity increases risk for later emotional inexpressivity) or whether emotional expressivity is a risk factor for PTSD symptom severity (i.e., the presence of emotional inexpressivity increases the likelihood of developing PTSD symptoms following trauma). Second, this study relied exclusively on self-report measures. These may be influenced by one’s willingness or ability to report accurately. Thus, future investigations should include objective measures of emotional expressivity. Third, our measure of PTSD symptom severity in the present study was based on the DSM-IV classification of PTSD. Thus, research is needed to replicate these findings using DSM-5 guidelines for the assessment of PTSD symptom severity. Of note, there is evidence that most of the discrepancy (60%) between DSM-IV and DSM-5 PTSD is due to the revised Criterion A definition; another 37% is due to the avoidance criterion, 2% to the negative alterations in cognitions and mood criterion, and 1% to the arousal and reactivity criterion (Kilpatrick et al., 2013). Thus, based on these findings, it is not expected that our findings for emotional expressivity – particularly salient to the negative alterations in cognitions and mood criterion – would drastically change using the DSM-5 classification of PTSD.
Next, although we were able to account for some trauma characteristics such as total number of lifetime traumatic events and type of lifetime index trauma, we did not examine other trauma-related characteristics, such as time passed since the traumatic event, age at which the traumatic event was experienced, and perpetrator type in the case of interpersonal trauma. Future investigations in this area should assess for and explore these trauma characteristics. Lastly, while use of a sample of Black college students attending a historically Black university is a strength of the current study, replication of these findings in larger, more diverse samples is warranted, including clinical samples. For instance, research is needed to explore the potential moderating role of gender in the relation between PTSD symptom severity and emotional expressivity in other racial and ethnic groups (e.g., White and Asian individuals). Further, it will be important for future research to explore the role of cultural factors such as religiosity and socioeconomic status, in the association of PTSD symptom severity to emotional expressivity among Black individuals. Additionally, examination of the relations examined here among samples of Black college students attending predominantly White institutions is needed. These latter findings may specify whether emotional expressivity varies among trauma-exposed Black college students at historically Black universities versus predominantly White institutions. Such findings may help inform the understanding and treatment of PTSD symptom severity in this population.
Acknowledgments
Work on this paper by the last author (NHW) was supported by National Institutes of Health grants K23DA039327 and P20GM125507.
References
- Ahrens CE, Abeling S, Ahmad S, & Hinman J (2010). Spirituality and well-being: The relationship between religious coping and recovery from sexual assault. Journal of Interpersonal Violence, 25, 1242–1263. [DOI] [PubMed] [Google Scholar]
- Aiken LS, & West SG (1991). Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Sage. [Google Scholar]
- Albritton TJ (2012). Educating our own: The historical legacy of HBCUs and their relevance for educating a new generation of leaders. The Urban Review, 44(3), 311–331. [Google Scholar]
- American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th edition, Text Revision) (DSM-IV-TR). Washington, DC: American Psychiatric Pub. [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Washington, DC: American Psychiatric Pub. [Google Scholar]
- Andrews AR, Jobe-Shields L, López CM, Metzger IW, De Arellano MA, Saunders B, & Kilpatrick DG (2015). Polyvictimization, income, and ethnic differences in trauma-related mental health during adolescence. Social psychiatry and psychiatric epidemiology, 50(8), 1223–1234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Badour CL, Resnick HS, & Kilpatrick DG (2017). Associations between specific negative emotions and DSM-5 PTSD among a national sample of interpersonal trauma survivors. Journal of Interpersonal Violence, 32, 1620–1641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blanchard EB, Jones-Alexander J, Buckley TC, & Forneris CA (1996). Psychometric properties of the PTSD Checklist (PCL). Behaviour Research and Therapy, 34, 669–673. [DOI] [PubMed] [Google Scholar]
- Bonn-Miller M, Vujanovic A, Feldner M, Bernstein A, Zvolensky M (2007). Posttraumatic stress symptom severity predicts marijuana use coping motives among traumatic event-exposed marijuana users. Journal of Traumatic Stress, 20, 577–586. [DOI] [PubMed] [Google Scholar]
- Boyraz G, Horne SG, Armstrong AP, & Owens AC (2015). Posttraumatic stress predicting depression and social support among college students: Moderating effects of race and gender. Psychological Trauma: Theory, Research, Practice, and Policy, 7, 259–268. [DOI] [PubMed] [Google Scholar]
- Brantley PJ, O’hea EL, Jones G, & Mehan DJ (2002). The influence of income level and ethnicity on coping strategies. Journal of Psychopathology and Behavioral Assessment, 24, 39–45. [Google Scholar]
- Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, & Andreski P (1998). Trauma and posttraumatic stress disorder in the community: The 1996 Detroit Area Survey of Trauma. Archives of General Psychiatry, 55, 626–632. [DOI] [PubMed] [Google Scholar]
- Buckley TC, Blanchard EB, & Neill WT (2000). Information processing and PTSD: A review of the empirical literature. Clinical Psychology Review, 20, 1041–1065. [DOI] [PubMed] [Google Scholar]
- Carmassi C, Akiskal HS, Bessonov D, Massimetti G, Calderani E, Stratta P, Dell L (2014). Gender differences in DSM-5 versus DSM-IV-TR PTSD prevalence and criteria comparison among 512 survivors to the L′ Aquila earthquake. Journal of Affective Disorders, 160, 55–6. [DOI] [PubMed] [Google Scholar]
- Carragher N, Sunderland M, Batterham PJ, Calear AL, Elhai JD, Chapman C, & Mills K (2016). Discriminant validity and gender differences in DSM-5 posttraumatic stress disorder symptoms. Journal of Affective Disorders, 190, 56–67. [DOI] [PubMed] [Google Scholar]
- Consedine NS, Magai C, & Neugut AI (2004). The contribution of emotional characteristics to breast cancer screening among women from six ethnic groups. Preventive Medicine, 38, 64–77. [DOI] [PubMed] [Google Scholar]
- Dodge KA, McLoyd VC, & Lansford JE (2005). The Cultural Context of Physically Disciplining Children. In McLoyd VC, Hill NE, & Dodge KA (Eds.), Duke Series in Child Development and Public Policy. African American family life: Ecological and cultural diversity (pp. 245–263). New York, NY: Guilford Press. [Google Scholar]
- Dunbar AS, Leerkes EM, Coard SI, Supple AJ, Calkins S (2017). An integrative model of parental racial/ethnic and emotion socialization and links to social-emotional development among African American families. Child Development Perspectives, 11, 16–22. [Google Scholar]
- Edwards JR, & Lambert LS (2007). Methods for integrating moderation and mediation: a general analytical framework using moderated path analysis. Psychological Methods, 12. [DOI] [PubMed] [Google Scholar]
- Eid M, & Diener E (2009). Norms for experiencing emotions in different cultures: Inter- and intranational differences. In Diener E (Ed.), Culture and well-being: The collected works of Ed Diener. (pp. 169–202). New York, NY: Springer Science + Business Media. [DOI] [PubMed] [Google Scholar]
- Foa EB, & Kozak MJ (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99, 20–35. [PubMed] [Google Scholar]
- Garrison CZ, Bryant ES, Addy CL, Spurrier PG, Freedy JR, Kilpatrick DG (1995). Posttraumatic stress disorder in adolescents after Hurricane Andrew. Journal of the American Academy of Child & Adolescent Psychiatry, 34, 1193–1201. [DOI] [PubMed] [Google Scholar]
- Golding JM (1999). Intimate partner violence as a risk factor for mental disorders: A meta-analysis. Journal of Family Violence, 14, 99–132. [Google Scholar]
- Goldstein RB, Smith SM, Chou SP, Saha TD, Jung J, Zhang H, … & Grant BF, (2016). The epidemiology of DSM-5 posttraumatic stress disorder in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Social Psychiatry and Psychiatric Epidemiology, 51, 1137–1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray MJ, Litz BT, Hsu JL, & Lombardo TW (2004). Psychometric properties of the life events checklist. Assessment, 11, 330–341. [DOI] [PubMed] [Google Scholar]
- Gregory JF (1997). Three strikes and they’re out: African American boys and American schools’ responses to misbehavior. International Journal of Adolescence and Youth, 7, 25–34. [Google Scholar]
- Gross JJ, & John OP (1998). Mapping the domain of expressivity: Multimethod evidence for a hierarchical model. Journal of Personality and Social Psychology, 7, 170–191. [DOI] [PubMed] [Google Scholar]
- Halberstadt AG, & Lozada FT (2011). Emotion Development in Infancy through the Lens of Culture. Emotion Review, 3, 158–168. [Google Scholar]
- Hardy PM, Kaganda EJ, & Aruguete MS (2019). Below the surface: HBCU performance, social mobility, and college ranking. Journal of Black Studies, 50(5), 468–483. [Google Scholar]
- Hayes SC, Wilson KG, Gifford EV, Follette VM, & Strosahl K (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64, 1152–1168. [DOI] [PubMed] [Google Scholar]
- Kang SK, & Chasteen AL (2009). The moderating role of age-group identification and perceived threat on stereotype threat among older adults. The International Journal of Aging and Human Development, 69, 201–220. [DOI] [PubMed] [Google Scholar]
- Kennedy JL (2012). The HBCU experience: Liberating or not?. The Urban Review, 44(3), 358–377. [Google Scholar]
- Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, & Friedman MJ (2013). National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress, 26, 537–547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King MW, Street AE, Gradus JL, Vogt DS, & Resick PA (2013). Gender differences in posttraumatic stress symptoms among OEF/OIF veterans: An item response theory analysis. Journal of Traumatic Stress, 26, 175–183. [DOI] [PubMed] [Google Scholar]
- Klonsky ED, & Moyer A (2008). Childhood sexual abuse and non-suicidal self-injury: Meta- analysis. The British Journal of Psychiatry, 192, 166–170. [DOI] [PubMed] [Google Scholar]
- Kring AM, & Gordon AH (1998). Sex differences in emotion: Expression, experience, and physiology. Journal of Personality and Social Psychology, 74, 686–703. [DOI] [PubMed] [Google Scholar]
- Kring AM, Smith DA, & Neale JM (1994). Individual differences in dispositional expressiveness: Development and validation of the Emotional Expressivity Scale. Journal of Personality and Social Psychology, 66, 934–949. [DOI] [PubMed] [Google Scholar]
- Kuebli J, & Fivush R (1992). Gender differences in parent-child conversations about past emotions. Sex Roles, 27, 683–698. [Google Scholar]
- Labella MH (2018). The sociocultural context of emotion socialization in African American families. Clinical Psychology Review, 59, 1–15. [DOI] [PubMed] [Google Scholar]
- Lester K, Artz C, Resick PA, & Young-Xu Y (2010). Impact of race on early treatment termination and outcomes in posttraumatic stress disorder treatment. Journal of Consulting and Clinical Psychology, 78, 480. [DOI] [PubMed] [Google Scholar]
- Levant RF, & Richmond K (2007). A review of research on masculinity ideologies using the male role norms inventory. Journal of Men’s Studies, 15, 130–146. [Google Scholar]
- Litz BT, Orsillo SM, Kaloupek D, & Weathers F (2000). Emotional processing in posttraumatic stress disorder. Journal of Abnormal Psychology, 109, 26–39. [DOI] [PubMed] [Google Scholar]
- Marx BP, & Sloan DM (2002). The role of emotion in the psychological functioning of adult survivors of childhood sexual abuse. Behavior Therapy, 33, 563–577. [Google Scholar]
- McDuff D, Kodra E, el Kaliouby R, & LaFrance M (2017). A large-scale analysis of sex differences in facial expressions. PLoS ONE, 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Conron KJ, Koenen KC, & Gilman SE (2010). Childhood adversity, adult stressful life events, and risk of past-year psychiatric disorder: a test of the stress sensitization hypothesis in a population-based sample of adults. Psychological Medicine, 40, 1647–1658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy S, Elklit A, Chen YY, Ghazali SR, & Shevlin M (2019). Sex differences in PTSD symptoms: A differential item functioning approach., Psychological Trauma: Theory, ResearchPractice, and Policy, 11, 319. [DOI] [PubMed] [Google Scholar]
- Nelson JA, Leerkes EM, O’Brien M, Calkins SD, Marcovitch S (2012). African American and European American mothers’ beliefs about negative emotions and emotion socialization practices. Parenting: Science and Practice, 12, 22–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norman RE, Byambaa M, De R, Butchart A, Scott J, & Vos T (2012). The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Medicine, 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norris FH (1992). Epidemiology of trauma: Frequency and impact of different potentially traumatic events on different demographic groups. Journal of Consulting and Clinical Psychology, 60, 409–418. [DOI] [PubMed] [Google Scholar]
- Park CL, Holt CL, Le D, Christie J, & Williams BR (2018). Positive and negative religious coping styles as prospective predictors of well-being in African Americans. Psychology of Religion and Spirituality, 10, 318–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perilla JL, Norris FH, & Lavizzo EA (2002). Ethnicity, culture, and disaster response: Identifying and explaining ethnic differences in PTSD six months after Hurricane Andrew. Journal of Social and Clinical Psychology, 21, 20–45. [Google Scholar]
- Pulcino T, Galea S, Ahern J, Resnick H, Foley M, Vlahov D (2003). Posttraumatic stress in women after the September 11 terrorist attacks in New York City. Journal of Women’s Health, 12, 809–820. [DOI] [PubMed] [Google Scholar]
- Roberts AL, Gilman SE, Breslau J, Breslau N, & Koenen KC (2011). Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychological medicine, 41, 71–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roemer L, Litz BT, Orsillo SM, & Wagner AW (2001). A preliminary investigation of the role of strategic withholding of emotions in PTSD. Journal of Traumatic Stress, 14,149–156. [Google Scholar]
- Ruggiero KJ, Del Ben K, Scotti JR, & Rabalais AE (2003). Psychometric properties of the PTSD Checklist—Civilian version. Journal of Traumatic Stress, 16, 495–502. [DOI] [PubMed] [Google Scholar]
- Schick MR, Weiss NH, Contractor AA, Suazo NC, & Spillane NS (2020). Post-traumatic stress disorder’s relation with positive and negative emotional avoidance: The moderating role of gender. Stress and Health, 36, 172–178. [DOI] [PubMed] [Google Scholar]
- Shaffer A, Suveg C, Thomassin K, Bradbury LL (2012). Emotion socialization in the context of family risks: Links to child emotion regulation. Journal of Child and Family Studies, 21, 917–924. [Google Scholar]
- Siegel SJ, & Alloy LB (1990). Interpersonal perceptions and consequences of depressive- significant other relationships: A naturalistic study of college roommates. Journal of Abnormal Psychology, 99, 361. [DOI] [PubMed] [Google Scholar]
- Sripada RK, Blow FC, Rauch SA, Ganoczy D, Hoff R, Harpaz-Rotem I, & Bohnert KM (2019). Examining the nonresponse phenomenon: Factors associated with treatment response in a national sample of veterans undergoing residential PTSD treatment. Journal of Anxiety Disorders, 63, 18–25. [DOI] [PubMed] [Google Scholar]
- Sullivan TJ, Leifker FR, & Marshall AD (2018). Observed emotional expressivity, posttraumatic stress disorder symptoms, and intimate partner violence perpetration among community couples. Journal of Traumatic Stress. 31, 352–361. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, & Fidell LS (2007). Using multivariate statistics. Boston, MA: Pearson. [Google Scholar]
- Taylor RJ, Chatters LM, & Levin J (2003). Religion in the lives of African Americans: Social, psychological, and health perspectives. Thousand Oaks, CA: Sage. [Google Scholar]
- Thomas DE, Coard SI, Stevenson HC, Bentley K, Zamel P (2009). Racial and emotional factors predicting teachers’ perceptions of classroom behavioral maladjustment for urban African American male youth. Psychology in the Schools, 46, 184–196. [Google Scholar]
- Tolin DF, & Foa EB (2006). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132, 959–992. [DOI] [PubMed] [Google Scholar]
- Tull MT, Barrett HM, McMillan ES, & Roemer L (2007). A preliminary investigation of the relationship between emotion regulation difficulties and posttraumatic stress symptoms. Behavior Therapy, 38, 303–313. [DOI] [PubMed] [Google Scholar]
- Tull MT, Jakupcak M, Paulson A, & Gratz KL (2007). The role of emotional inexpressivity and experiential avoidance in the relationship between posttraumatic stress disorder symptom severity and aggressive behavior among men exposed to interpersonal violence. Anxiety, Stress, and Coping, 20, 337–351. [DOI] [PubMed] [Google Scholar]
- Ullman SE, Relyea M, Peter-Hagene L, & Vasquez AL (2013). Trauma histories, substance use coping, PTSD, and problem substance use among sexual assault victims. Addictive Behaviors, 38, 2219–2223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Underwood MK, Coie JD, & Herbsman CR (1992). Display rules for anger and aggression in school-age children. Child Development, 63, 366–380. [PubMed] [Google Scholar]
- Walker LJ (2015). Trauma, environmental stressors, and the African-American college student: Research, practice, and HBCUs. Penn Center for Minority Serving Institutions, Philadelphia, PA, available at: www2.gse.upenn.edu/cmsi/content/reports. [Google Scholar]
- Weathers F, Litz B, Herman D, Huska J, & Keane T (1993). The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Paper presented at the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX. [Google Scholar]
- Wiedemann AU, Schüz B, Sniehotta F, Scholz U, & Schwarzer R (2009). Disentangling the relation between intentions, planning, and behaviour: A moderated mediation analysis. Psychology and Health, 24(1), 67–79. [DOI] [PubMed] [Google Scholar]
- Weiss NH, Contractor AA, Forkus SR, Goncharenko S, & Raudales AM (2020). Positive emotion dysregulation among community individuals: The role of trauma exposure and posttraumatic stress disorder. Journal of Traumatic Stress, 33, 741–749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss NH, Dixon-Gordon KL, Peasant C, & Sullivan TP (2018). An examination of the role of difficulties regulating positive emotions in posttraumatic stress disorder. Journal of Traumatic Stress, 31, 775–780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss NH, Forkus SR, Raudales AM, Schick MR, & Contractor AA (2020). Alcohol misuse to down-regulate positive emotions: A cross-sectional multiple mediator analysis among US military veterans. Addictive Behaviors, 105, 106322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss NH, Goncharenko S, Raudales AM, Schick MR, & Contractor AA (2021). Alcohol to down-regulate negative and positive emotions: Extending our understanding of the functional role of alcohol in relation to posttraumatic stress disorder. Addictive Behaviors, 115, 106777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss NH, Tull MT, Dixon-Gordon KL, & Gratz KL (2013). Extending findings of a relation between posttraumatic stress disorder and emotion dysregulation among African American individuals: A preliminary examination of the moderating role of gender. Journal of Traumatic Stress Disorders & Treatment, 3(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss NH, Tull MT, Davis LT, Dehon EE, Fulton JJ, & Gratz KL (2012). Examining the association between emotion regulation difficulties and probable posttraumatic stress disorder within a sample of African Americans. Cognitive Behaviour Therapy, 41, 5–14. [DOI] [PubMed] [Google Scholar]