

Abstract
Background
Depression is a common mental disorder characterized by disturbances in mood, thoughts, or behaviors. Serious games, which are games that have a purpose other than entertainment, have been used as a nonpharmacological therapeutic intervention for depression. Previous systematic reviews have summarized evidence of effectiveness of serious games in reducing depression symptoms; however, they are limited by design and methodological shortcomings.
Objective
This study aimed to assess the effectiveness of serious games in alleviating depression by summarizing and pooling the results of previous studies.
Methods
A systematic review of randomized controlled trials (RCTs) was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. The search sources included 6 bibliographic databases (eg, MEDLINE, PsycINFO, IEEE Xplore), the search engine “Google Scholar,” and backward and forward reference list checking of the included studies and relevant reviews. Two reviewers independently carried out the study selection, data extraction, risk of bias assessment, and quality of evidence appraisal. Results of the included studies were synthesized narratively and statistically, as appropriate, according to the type of serious games (ie, exergames or computerized cognitive behavioral therapy [CBT] games).
Results
From an initial 966 citations retrieved, 27 studies met the eligibility criteria, and 16 studies were eventually included in meta-analyses. Very low-quality evidence from 7 RCTs showed no statistically significant effect of exergames on the severity of depressive symptoms as compared with conventional exercises (P=.12). Very low-quality evidence from 5 RCTs showed a statistically and clinically significant difference in the severity of depressive symptoms (P=.004) between exergame and control groups, favoring exergames over no intervention. Very low-quality evidence from 7 RCTs showed a statistically and clinically significant effect of computerized CBT games on the severity of depressive symptoms in comparison with no intervention (P=.003).
Conclusions
Serious games have the potential to alleviate depression as other active interventions do. However, we could not draw definitive conclusions regarding the effectiveness of serious games due to the high risk of bias in the individual studies examined and the low quality of meta-analyzed evidence. Therefore, we recommend that health care providers consider offering serious games as an adjunct to existing interventions until further, more robust evidence is available. Future studies should assess the effectiveness of serious games that are designed specifically to alleviate depression and deliver other therapeutic modalities, recruit participants with depression, and avoid biases by following recommended guidelines for conducting and reporting RCTs.
Trial Registration
PROSPERO International Prospective Register of Systematic Reviews CRD42021232969; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=232969
Keywords: serious games, exergames, depression, cognitive behavioral therapy, systematic reviews, meta-analysis
Introduction
Background
An individual's mental health is fundamental to living a healthy and enjoyable lifestyle. Studies estimate that 1 in 3 people may suffer from a mental illness during their lifetime [1]. The World Health Organization (WHO) reports that depression is a “leading cause of disability worldwide and is a major contributor to the overall global burden of disease” affecting more than 264 million people of all ages globally [2]. Depression is a mental health disorder that the Sustainable Development Goals of the United Nations (2015) has listed among its 270 targets and 230 indicators. Depressive disorders account for most of the total disability-adjusted life years globally. Although depressive disorders are global, they particularly affect those living in high and upper-middle-income nations [3]. This heavy toll is exacerbated by the fact that up to one-half (50%) of the people living in high-income countries and 90% of those living in low-resource settings receive no treatment for depressive disorders [4].
Depressive disorders are a family of mental disorders ranging in severity from mild temporary episodes of sadness to more severe and persistent depression [5]. Depressive disorders include disruptive mood dysregulation disorder, premenstrual dysphoric disorder, substance- or medication-induced depressive disorder, and major depressive disorder [6]. Depressive disorders are characterized by disturbances in mood, thoughts, or behaviors. Furthermore, depressive disorders do not affect the mind alone but are reported to impact a person’s body [7,8]. Depression is known to be caused by a number of factors that interact in complex mechanisms: social, genetic, pathological, and chemical [9]. Treatments for depressive disorders are generally classified into either pharmacological or psychosocial (ie, nonpharmacological) interventions. Pharmacological treatments involve the use of drugs (eg, antidepressants) while examples of psychosocial treatments include cognitive behavioral therapy (CBT), exposure therapy, and exercise [10].
The use of serious games, defined as games that have a purpose other than entertainment, has seen a rise in recent years [11]. Serious games use elements unique to gaming in order to educate or influence change in experience or behaviors [12]. Several industries have adopted and continue to use serious games including health care, education, and airlines [13]. Among other things, serious games have been effectively utilized for education, prevention, and treatment of chronic conditions (eg, asthma and diabetes) [14], therapeutic rehabilitation [15], and educational resources for health care professionals [16]. Moreover, serious games have been used as a nonpharmacological therapeutic intervention for mental disorders [17]. Serious games have been utilized as a treatment for various mental disorders, including depression [18,19], anxiety [20], posttraumatic stress disorder [21,22], autism spectrum disorder [23,24], dementia [25,26], alcohol use disorder [27], attention deficit hyperactivity disorder [28], and obsessive-compulsive disorder [13,29].
Gaming as a therapeutic tool in mental health can potentially offer several specific advantages that may be missing from traditional forms of delivery. The gaming industry is, as ever, popular globally [30] and arguably easier to access than even basic mental health services [31]. Games by their very nature have the potential to engage the user in game play that can be rewarding through scoring points or following story arcs that can help improve user involvement and lower attrition rates [32,33]. Additionally, as the technology improves, gaming can utilize accessories to provide richer sensory environments and immersive user experiences that allow users to simulate real-life scenarios more safely and help in educating and achieving cognitive and behavioral changes through overlearning and repetition [33,34].
Research Gap and Aim
Many studies have assessed the effectiveness of serious games to alleviate depression. Aggregating the evidence from these studies is very important to draw more definitive conclusions about the effectiveness of serious games as viable therapeutic interventions in depressive disorders. Several published reviews have summarized the evidence about the effectiveness of serious games for depression [18,19,35-37]. However, these reviews are undermined by certain technical shortcomings that limit the generalization of the findings. Specifically, these reviews (1) focused on a certain type of serious games (ie, exergames) [19,37]; (2) focused on a certain age group (older adults) [37]; (3) included non-randomized controlled trials (RCTs) [19,35]; (4) did not search technical databases (such IEEE Xplore and the ACM Digital Library), thereby including only a few studies [35-37]; (5) did not assess the quality of the evidence [18,19,35-37]; and (6) were outdated publications [18,19,35]. Therefore, this study aimed to assess the effectiveness of serious games for alleviating depression by summarizing and pooling the results of previous studies and providing an up-to-date review.
Methods
We conducted a systematic review in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Multimedia Appendix 1) [38].
Search Strategy
Search Sources
We utilized the following bibliographic databases to retrieve relevant studies: MEDLINE (via Ovid), PsycInfo (via EBSCO), CINAHL (via EBSCO), IEEE Xplore, ACM Digital Library, and Scopus. These databases were searched on March 30, 2021 by the first author. When applicable, we set auto alerts to conduct an automatic search weekly for 12 weeks (ending on June 30, 2021). We also searched the search engine “Google Scholar” to identify grey literature. We checked only the first 10 pages (ie, 100 hits) because Google Scholar retrieved a vast number of studies and it ordered them based on their relevancy. To identify further studies of relevance to the review, we conducted backward reference list checking (ie, screening the reference lists of the included studies and relevant reviews) and forward reference list checking (ie, screening the studies that cited the included studies).
Search Terms
The search query in this review was developed by consulting 2 experts in digital mental health and by checking systematic reviews of relevance to the review. These terms were chosen based on the target intervention (eg, serious games, exergames, and gamification), target outcome (eg, depression and melancholy), and target study design (eg, RCT and clinical trial). Multimedia Appendix 2 shows the detailed search query used to search each of the aforementioned databases.
Study Eligibility Criteria
This review included only RCTs that assessed the effectiveness of serious games for alleviating the severity of depressive symptoms. To be more precise, the intervention of interest in this review was serious games that were delivered on any digital platform such as computers, consoles (eg, Xbox, PlayStation), mobile phones, tablets, handheld devices, or any other computerized devices. The intervention had to utilize elements of gaming as an integral and primary method for therapeutic or prevention purposes. We did not consider nondigital games and those used for other purposes such as monitoring, screening, and diagnosis. We included RCTs whether they were parallel RCTs, cluster RCTs, crossover RCTs, or factorial RCTs but we excluded quasi-experiments, observational studies, and reviews. We focused on studies in which one of the measured outcomes was depression or depressive symptoms regardless of the outcome measures. Only trials in the English language were eligible for inclusion in this review. RCTs published as journal articles, conference proceedings, and dissertations were included, whereas we excluded conference abstracts and posters, commentaries, preprints, proposals, and editorials. We did not apply restrictions related to the population, year of publication, country of publication, comparator, and study settings.
Study Selection
We followed 3 steps to identify the relevant studies. In the first step, we exported the retrieved studies to EndNote to identify and remove duplicates. Then, 2 reviewers (EA and MA) independently screened the titles and abstracts of all retrieved studies. In the last step, the 2 reviewers independently screened the full texts of studies included from the second step. A third reviewer (AA) resolved any disagreements between the 2 reviewers in the second and third steps. Cohen κ in this review indicated a very good level of interrater agreement in the first (0.85) and second (0.90) steps [39].
Data Extraction
Two reviewers (EA and MA) independently extracted data from the included reviews using Microsoft Excel (Microsoft Corporation, Redmond, WA). Multimedia Appendix 3 shows the data extraction form that was used by the 2 reviewers to extract the data precisely and systematically from the included studies. The form was pilot tested using 3 included studies. Any disagreements between the reviewers were resolved by consulting a third reviewer (AA). The interrater agreement between the reviewers was 0.87, indicating a very good level of agreement [39]. Some outcome data (eg, mean, standard deviation, sample size in each group) were missing in 10 studies. Therefore, we contacted their corresponding authors to get them, and 5 corresponding authors did not reply to our emails even after sending 2 reminders.
Risk of Bias Assessment
Two reviewers (EA and MA) independently assessed the risk of bias in the included studies using the Risk-of-Bias 2 (RoB 2) tool, which is recommended by the Cochrane Collaboration [40]. This tool appraises the risk of bias in 5 domains in RCTs: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result [40]. The risk of bias judgments in these domains is used to determine the overall risk of bias for each included study. A third reviewer (AA) resolved any disagreements in judgments between the 2 reviewers. Interrater agreement between the reviewers was very good (Cohen κ=0.93) [39].
Data Synthesis
We utilized narrative and statistical approaches to synthesize the extracted data. Specifically, in narrative synthesis, texts and tables were used to describe the characteristics of the included studies, population, intervention, comparator, and outcome measures. Then, we grouped and summarized the findings of the included studies according to the type of serious games (ie, exergames or computerized CBT games). A meta-analysis was conducted when at least 2 studies of the same type of serious game reported enough data for the analysis (ie, mean, standard deviation, number of participants in each intervention group). When this information was not reported in any included study, we contacted the first and corresponding authors to get the missing information.
Review Manager (RevMan 5.4) was used to conduct the meta-analysis. We measured the effect of each trial and the overall effect using the standardized mean difference (SMD; Cohen d) because the outcome data (severity of depressive symptoms) were continuous and tools used to measure the outcome were different between the included studies. The random effects model was used in the analysis given the clinical heterogeneity between the meta-analyzed studies in terms of serious game characteristics (eg, types, duration, frequency, and period), population characteristics (eg, sample size, mean age, and health condition), and outcome measures (ie, tools and follow-up period).
When the meta-analysis showed a statistically significant difference between groups, we examined whether this difference was clinically important. A minimal clinically important difference (MCID) is defined as the smallest change in a measured outcome that a patient would consider as worthy and significant and which mandates a change in a patient’s treatment. The MCID boundaries for an outcome were calculated as ±0.5 times the SMD of the meta-analyzed studies.
We checked the characteristics of participants, interventions, comparator, and outcomes in studies included in the meta-analysis to assess their clinical heterogeneity. We also examined the statistical heterogeneity of the meta-analyzed studies by calculating a Chi-square P value and I2, which measures the statistical significance of heterogeneity and the degree of heterogeneity, respectively. A Chi-square P value ≤.05 indicates heterogeneous meta-analyzed studies [41]. The degree of heterogeneity was considered unimportant, moderate, substantial, or considerable when I2 was 0%-40%, 30%-60%, 50%-90%, or 75%-100%, respectively [41].
We assessed the overall quality of evidence from the meta-analyses using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach, which assesses the quality of evidence based on 5 domains: risk of bias, inconsistency (ie, heterogeneity), indirectness, imprecision, and publication bias [42]. Two reviewers (CT and AA) independently assessed the overall quality of meta-analyzed evidence, and any disagreements were resolved through discussion and consensus. Interrater agreement between the reviewers was very good (Cohen κ=0.88) [39].
Results
Search Results
As shown in Figure 1, we retrieved 966 citations from searching the 7 electronic databases. Using the software EndNote, we identified and removed 225 duplicates of the retrieved citations. Screening titles and abstracts of the remaining 741 citations led to excluding 592 citations because (1) they did not use serious games (n=354); (2) the severity of depressive symptoms was not a measured outcome (n=69); (3) they were not RCTs (n=119); (4) they were not peer-reviewed articles, theses, nor conference proceedings (n=39); and (5) they were published in non-English languages (n=11). Reading the full text of the remaining 149 publications led to excluding 127 publications because (1) they did not use serious games (n=39), (2) the severity of depressive symptoms was not a measured outcome (n=32), (3) they were not RCTs (n=53), and (4) they were published in non-English languages (n=3). We identified 5 additional RCTs through backward and forward reference list checking. In total, 27 RCTs were included in the current review [43-69]. Of those, 16 RCTs were included in the meta-analyses [45-52,54,59-65].
Figure 1.
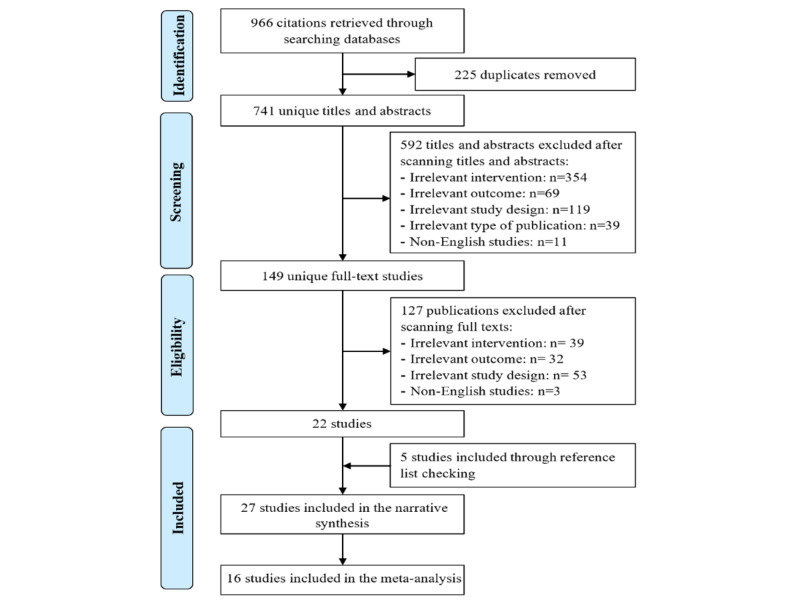
Flow chart of the study selection process.
Characteristics of Included Reviews
The included studies were published between 2012 and 2021 (Table 1). The years that witnessed the largest number of included studies were 2018 (n=5) and 2020 (n=5). The included studies were carried out in 15 different countries, as shown in Table 1. The country that published the largest number of the included studies was Germany (n=5). All included papers were papers published in peer-reviewed journals. The trial type used in the most included studies was parallel RCTs (n=24).
Table 1.
Characteristics of studies and population.
| Author(s), year | Country | Publication type | RCTa type | Sample size, n | Mean age (years) | Sex (male), % | Health condition | Setting |
| Ruivo et al [43], 2017 | Ireland | Journal article | Parallel | 32 | 59.9 | 81.3 | Cardiovascular diseases | Clinical, community, educational |
| Ferraz et al [44], 2018 | Brazil | Journal article | Parallel | 62 | 69 | 59.7 | Parkinson disease | Clinical |
| Song and Park [45], 2015 | South Korea | Journal article | Parallel | 40 | 50.1 | 55.0 | Stroke | Clinical |
| Schumacher et al [46], 2018 | Germany | Journal article | Parallel | 42 | 56.3 | 59.5 | Hematopoietic stem cell transplantation recipients | Clinical |
| Meldrum et al [47], 2015 | Ireland | Journal article | Parallel | 71 | 54.1 | 38.0 | Unilateral peripheral vestibular loss | Clinical |
| Zhou et al [48], 2020 | Qatar | Journal article | Parallel | 73 | 64.6 | 45.2 | Diabetes and end-stage renal disease | Clinical |
| Vieira et al [49], 2017 | Portugal | Journal article | Parallel | 46 | 57.7 | -b | Coronary artery disease | Clinical |
| Tollár et al [50], 2018 | Hungary | Journal article | Parallel | 74 | 69.4 | 48.6 | Parkinson disease | Clinical |
| Ozdogar et al [51], 2020 | Turkey | Journal article | Parallel | 60 | 40.1 | 27.1 | Multiple sclerosis | Clinical |
| Kempf and Martin [52], 2013 | Germany | Journal article | Parallel | 220 | 61.1 | 45.9 | Type 2 diabetes | Clinical, community |
| Rendon et al [53], 2012 | United States | Journal article | Parallel | 40 | 84.5 | 35.0 | Older adults | Clinical |
| Jahouh et al [54], 2021 | Spain | Journal article | Parallel | 80 | 84.2 | 44.0 | Older adults | Clinical |
| Rica et al [55], 2019 | Brazil | Journal article | Parallel | 50 | - | 0.0 | Older adults | Clinical, community |
| Andrade et al [56], 2020 | Brazil | Journal article | Cluster | 140 | 9.41 | 42.1 | Elementary students | Educational |
| Shin et al [57], 2015 | South Korea | Journal article | Parallel | 35 | 54 | 75 | Stroke | Clinical |
| Adomavičienė et al [58], 2019 | Lithuania | Journal article | Parallel | 60 | 64.6 | 66.7 | Stroke | Clinical |
| Fleming et al [59], 2012 | New Zealand | Journal article | Crossover | 32 | 14.9 | 56 | Depression | Educational |
| Merry et al [60], 2012 | New Zealand | Journal article | Parallel | 187 | 15.6 | 34.2 | Depression | Clinical, educational |
| Donker et al [61], 2019 | Netherlands | Journal article | Parallel | 193 | 41.3 | 33.2 | Acrophobia | Community |
| Perry et al [62], 2017 | Australia | Journal article | Cluster | 540 | 16.7 | 36.9 | Secondary students | Educational |
| Cooney et al [63], 2017 | Ireland | Journal article | Parallel | 52 | 40.6 | 38.8 | Anxiety, depression, and/or intellectual disability | Clinical |
| Poppelaars et al [64], 2016 | Netherlands | Journal article | Parallel | 208 | 13.4 | 0.0 | Depression | Educational |
| Välimäki et al [65], 2018 | Finland | Journal article | Parallel | 90 | 41 | 50.0 | Traumatic brain injury | Clinical |
| Wijnhoven et al [66], 2020 | Netherlands | Journal article | Parallel | 109 | 11.1 | 77.1 | Anxiety and autism spectrum disorder | Clinical, educational |
| Haberkamp et al [67], 2021 | Germany | Journal article | Parallel | 68 | 22.8 | 13.0 | Arachnophobia | Educational |
| Butler et al [68], 2020 | Germany | Journal article | Parallel | 40 | 33.4 | 100 | Posttraumatic stress disorder | Clinical |
| David et al [69], 2018 | Germany | Journal article | Parallel | 165 | 12.9 | 35.9 | Stroke | Educational |
aRCT: randomized controlled trial.
bNot reported.
The sample size in the included studies varied from 32 to 540, with an average of 104. The mean age of participants in the included studies ranged between 9.41 years and 84.5 years, with an average of 43.9 years. The percentage of the sample who were men reported in 26 studies ranged from 0% to 100%, with an average of 46.1%. Participants’ health conditions were varied between studies, and depression and stroke were the most common (n=4 each). Participants in most studies were recruited from clinical settings (n=20).
The intervention in the included studies was only serious games in 19 studies, serious games plus occupational therapy in 2 studies, and serious games plus psychotherapy in 1 study (Table 2). The most common games used in the included studies were SPARX (n=4) and Wii Fit (n=4). There were 5 types of serious games based on the therapeutic modality that they deliver: exergames (n=16), computerized CBT games (n=8), exposure therapy games (n=1), brain training games (n=1), rational emotive behavioral therapy (REBT) and rational emotive behavioral therapy education (REBE)–based game (n=1). Although games were designed with a “serious” purpose from the beginning (designed serious games) in 14 studies, they were not designed as serious games but were being used for a serious purpose (purpose-shifted games) in the remaining 13 studies. The most common platforms used for playing the games were computers (n=12) and video game consoles and their accessories (eg, balance board; n=12). The duration of the games in the included studies ranged between 5 minutes and 85 minutes, but it ranged between 20 minutes and 45 minutes in most studies (n=14). The frequency of playing the games varied between once a week and once a day, but it ranged between once a week and 3 times a week in 20 studies. The period of the intervention varied between 1 week and 24 weeks, but it ranged from 4 to 8 weeks in 19 studies.
Table 2.
Characteristics of interventions.
| Author(s) | Intervention | Serious game name | Serious game type | Serious game genre | Platform | Duration (minutes) | Frequency (times/week) | Period (weeks) |
| Ruivo et al [43] | Serious game | Wii-Sports | Exergame | Purpose-shifted | Wii console and Kinect | 60 | 2 | 6 |
| Ferraz et al [44] | Serious game | Kinect Adventures | Exergame | Purpose-shifted | Xbox console and Kinect | 50 | 3 | 8 |
| Song and Park [45] | Serious game | Kinect Sport, Kinect Sport Season 2, Kinect Adventure, and Kinect Gunstringer | Exergame | Purpose-shifted | Computer and Xbox Kinect | 30 | 5 | 8 |
| Schumacher et al [46] | Serious game | Wii Fit and Wii-Sports | Exergame | Purpose-shifted | Wii console and balance board | 30 | 5 | 2 |
| Meldrum et al [47] | Serious game | Wii Fit Plus | Exergame | Purpose-shifted | Wii console and balance board and Frii Board | 15 | 5 | 6 |
| Zhou et al [48] | Serious game | N/Ra | Exergame | Designed | Computer and wearables (sensors) | 30 | 3 | 4 |
| Vieira et al [49] | Serious game | Kinect-RehabPlay | Exergame | Designed | Computer and Xbox Kinect | 70-85 | 3 | 24 |
| Tollár et al [50] | Serious game | Reflex Ridge, Space Pop, Just Dance | Exergame | Purpose-shifted | Xbox console and Kinect | 60 | 5 | 5 |
| Ozdogar et al [51] | Serious game | Kinect Sports Rivals | Exergame | Purpose-shifted | Xbox console and Kinect | 45 | 1 | 8 |
| Kempf and Martin [52] | Serious game | Wii Fit Plus | Exergame | Purpose-shifted | Wii console and balance board | ≥30 | 1 | 12 |
| Rendon et al [53] | Serious game | Wii Fit | Exergame | Purpose-shifted | Wii console and balance board | 35-45 | 3 | 6 |
| Jahouh et al [54] | Serious game | Step, Nodding | Exergame | Purpose-shifted | Wii console | 40-45 | 2-3 | 8 |
| Rica et al [55] | Serious game | Kinect Sports Ultimate Collection, Your Shape Fitness Evolved, Dance Central, and Kinect Training | Exergame | Purpose-shifted | Xbox console and Kinect | 60 | 3 | 12 |
| Andrade et al [56] | Serious game | Just Dance 2015 | Exergame | Purpose-shifted | Xbox console and Kinect | 40 | 2 | 1 |
| Shin et al [57] | Serious game + occupational therapy | RehabMaster | Exergame | Designed | Computer, sensors, and infrared projector | 60 | 5 | 4 |
| Adomavičienė et al [58] | Serious game | N/R | Exergame | Designed | Computer and Kinect | 45 | Once a day | 2 |
| Fleming et al [59] | Serious game | SPARX | Computerized CBTb game | Designed | Computer | 30 | 1-2 | 5 |
| Merry et al [60] | Serious game | SPARX | Computerized CBT game | Designed | Computer | 20-40 | 1-2 | 4-7 |
| Donker et al [61] | Serious game | ZeroPhobia | Computerized CBT game | Designed | Smartphone and wearables (VRc goggles) | 5-40 | 2 | 3 |
| Perry et al [62] | Serious game | SPARX-R | Computerized CBT game | Designed | Computer | 20-30 | 1-2 | 5-7 |
| Cooney et al [63] | Serious game | Pesky Gnats: The Feel Good Island | Computerized CBT game | Designed | Computer | 60 | 1 | 7 |
| Poppelaars et al [64] | Serious game | SPARX | Computerized CBT game | Designed | Computer | 20-40 | 1 | 7 |
| Välimäki et al [65] | Serious game | CogniFit | Computerized CBT game | Designed | Computer | ≥30 | Once a day | 8 |
| Wijnhoven et al [66] | Serious game | MindLight | Computerized CBT game | Designed | Computer and wearable (headset) | 60 | 1 | 6 |
| Haberkamp et al [67] | Serious game | Spider App | Exposure therapy game | Designed | Smartphone | 12 | 2 | 1 |
| Butler et al [68] | Serious game + psychotherapy | Tetris | Brain-training game | Purpose-shifted | Nintendo DS XL console | 60 | 2 | 6 |
| David et al [69] | Serious game | REThink | REBTd- and REBEe-based game | Designed | Tablet | 50 | 3 | 4 |
aN/R: not reported.
bCBT: cognitive behavioral theory.
cVR: virtual reality.
dREBT: rational emotive behavioral therapy.
eREBE: rational emotive behavioral education.
As shown in Table 3, the comparison groups received inactive interventions in 15 studies, while they received active interventions in 18 studies (eg, conventional exercises, CBT programs, video games, and psychotherapy). Note that the numbers do not add up because 6 studies delivered both active and inactive interventions as comparators. The duration of the active comparators ranged between 12 minutes and 100 minutes. The frequency of playing the active comparators varied between once a week and once a day. The period of the active comparators varied between 1 week and 24 weeks. The outcome of interest (eg, severity of depressive symptoms) was measured using 18 different tools, but the most common tool used by the included studies was the Beck Depression Inventory (BDI; n=6), followed by the Hospital Anxiety and Depression Scale (HADS; n=4). The outcome of interest was measured immediately after the intervention in all included studies, and the most common follow-up period was 3 months (n=6). Participant attrition was reported in 24 studies and ranged from 0 to 134.
Table 3.
Characteristics of comparators and outcomes.
| Author(s) | Comparator | Duration (minutes) | Frequency (times/week) | Period (weeks) | Outcome measures | Follow up | Attrition, n |
| Ruivo et al [43] | Conventional exercises (functional training), conventional exercises (bicycle exercise) | 50 | 3 | 8 | GDSa | Postintervention | 10 |
| Ferraz et al [44] | Robot-assisted trainings | 45 | Once a day | 2 | HADSb | Postintervention | 18 |
| Song and Park [45] | Conventional exercises | 30 | 5 | 8 | BDIc | Postintervention | N/Rd |
| Schumacher et al [46] | Conventional exercises | 30 | 5 | 2 | HADS-De | Postintervention, 30-day follow-up, 100-day follow-up | 11 |
| Meldrum et al [47] | Conventional exercises | 15 | 5 | 6 | HADS-D | Postintervention | 9 |
| Zhou et al [48] | Conventional exercises | 30 | 3 | 4 | CES-Df | Postintervention | 0 |
| Vieira et al [49] | Conventional exercises, control | 70-85 | 3 | 24 | DASS-21g | Postintervention, mid-intervention (3 months) | 13 |
| Tollár et al [50] | Conventional exercises | 60 | 2 | 6 | HADS | Postintervention, 2-month follow-up | 4 |
| Ozdogar et al [51] | Conventional exercises, control | 45 | 1 | 8 | BDI | Postintervention | 3 |
| Kempf and Martin [52] | Control | N/Ah | N/A | N/A | WHO-5i, PAIDj, ADS-Lk | Postintervention | 44 |
| Rendon et al [53] | Control | N/A | N/A | N/A | GDS | Postintervention | 6 |
| Jahouh et al [54] | Control | N/A | N/A | N/A | GDS, GADSl | Postintervention | N/R |
| Rica et al [55] | Conventional exercises, control | 60 | 5 | 5 | BDI | Postintervention | 0 |
| Andrade et al [56] | Physical education | 40 | 2 | 1 | BMSm | Postintervention | 0 |
| Shin et al [57] | Occupational therapy | 60 | 5 | 4 | HAMDn | Postintervention | 3 |
| Adomavičienė et al [58] | Conventional exercises, control | 60 | 5 | 5 | BDI | Postintervention | 0 |
| Fleming et al [59] | Control | N/A | N/A | N/A | CDRS-Ro, RADS-2p | Postintervention | 5 |
| Merry et al [60] | Control | N/A | N/A | N/A | CDRS-R, RADS-2 | Postintervention, 3-month follow-up | 17 |
| Donker et al [61] | Control | N/A | N/A | N/A | PHQ-9q | Postintervention, 3-month follow-up | 59 |
| Perry et al [62] | Interactive online program | 20-30 | 1-2 | 5-7 | MDIr | Postintervention, 6-month follow-up, 18-month follow-up | 134 |
| Cooney et al [63] | Control | N/A | N/A | N/A | GAS-LDs | Postintervention, 3-month follow-up | 3 |
| Poppelaars et al [64] | CBTt program + serious game, CBT program, control | CBT program + serious game (80-100), CBT program (60) | 1 | 7 | RADS-2 | Postintervention, 3-month follow-up, 6-month follow-up, 12-month follow-up | 10 |
| Välimäki et al [65] | Video game, control | ≥30 | Once a day | 8 | PHQ-9 | Postintervention, 3-month follow-up | 20 |
| Wijnhoven et al [66] | Video game | 60 | 1 | 6 | CDI-2u | Postintervention, 3-month follow-up | 35 |
| Haberkamp et al [67] | Video game | 12 | 2 | 1 | BDI-II | Postintervention, 2-week follow-up | 6 |
| Butler et al [68] | Psychotherapy | 60 | 2 | 6 | BDI-II | Postintervention, 6-month follow-up | 0 |
| David et al [69] | Rational emotive behavioral therapy and education, control | 50 | 3 | 4 | EATQ-Rv | Postintervention | 23 |
aGDS: Geriatric Depression Scale.
bHADS: Hospital Anxiety and Depression Scale.
cBDI: Beck Depression Inventory.
dN/R: not reported.
eHADS-D: depression subscale of the HADS.
fCES-D: Center for Epidemiologic Studies Depression Scale.
gDASS-21: Depression, Anxiety and Stress Scale 21.
hN/A: not applicable.
iWHO-5: WHO 5-item Well-Being Index.
jPAID: Problem Areas in Diabetes.
kADS-L: Allgemeine Depressionsskala.
lGADS: Goldberg Anxiety and Depression Scale.
mBMS: Brunel’s Mood Scale.
nHAMD: Hamilton Depression Rating Scale.
oCDRS-R: Children’s Depression Rating Scale-Revised.
pRADS-2: Reynolds Adolescent Depression Scale.
qPHQ-9: Patient Health Questionnaire-9.
rMDI: Major Depression Inventory.
sGAS-LD: Glasgow Depression Scale for people with a learning disability.
tCBT: cognitive behavioral therapy.
uCDI-2: Child Depression Inventory 2.
vEATQ-R: Early Adolescent Temperament Questionnaire-Revised.
Results of Risk of Bias Appraisal
The random allocation sequence for the randomization process was appropriate in 23 included studies. However, only 10 studies concealed the allocation sequence until participants were enrolled and assigned to interventions, and groups were not comparable in 4 studies. Accordingly, the risk of bias due to the randomization process was rated as low for only 8 studies (Figure 2).
Figure 2.
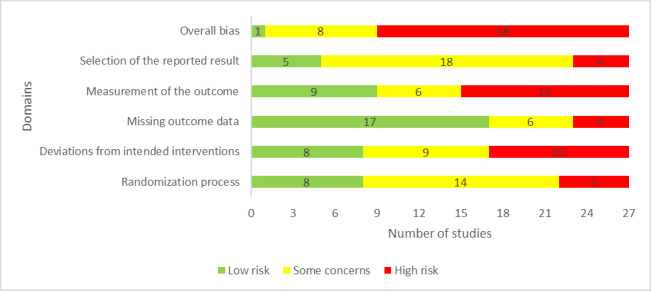
Review authors’ judgments about each “risk of bias” domain.
Participants and individuals delivering the interventions were aware of assigned interventions during the experiment in 22 and 20 studies, respectively. Deviation from the intended intervention occurred in 2 studies due to the experimental contexts. Only 14 studies used an appropriate analysis (intention-to-treat or modified intention-to-treat analyses) to estimate the effect of assignment to intervention. Therefore, the risk of bias due to the deviations from the intended interventions was judged as low in only 8 studies (Figure 2).
Outcome data were not available for all or nearly all participants in 21 studies, and there was evidence that the findings were not biased by missing outcome data in only 5 studies. The reasons for missing outcome data could not be related to the true value of the outcome in 18 studies. As a result, 17 studies were judged as having a low risk of bias in the “missing outcome data” domain.
All included studies assessed the outcome of interest (ie, depression level) using appropriate measures and used measurement methods comparable across intervention groups. However, the assessor of the outcome was blinded in only 9 studies. For this reason, only these studies were rated as low risk of bias in the “measuring the outcome” domain (Figure 2).
In 17 studies, a prespecified analysis plan (ie, protocol) was not published. Only 4 studies reported outcome measurements different from those specified in the analysis plan. There is no evidence that all included studies selected their results from many results produced from multiple eligible analyses of the data. Accordingly, the risk of bias due to the selection of the reported results was considered low in 4 studies (Figure 2).
In the last domain “overall bias,” the risk of bias was considered high in 20 studies as they were judged as having a high risk of bias in at least one domain; 6 studies were judged to have some concerns in the domain of overall bias as they had some concerns in at least one of the domains and were not at high risk for any domain. The remaining study was judged to be at low risk of bias for the domain of overall bias given that it was rated to be at low risk of bias for all domains. Reviewers’ judgments about each “risk of bias” domain for each included study are presented in Multimedia Appendix 4.
Results of Studies
Types of Serious Games
As mentioned earlier, we identified 5 types of serious games based on the therapeutic modality that they deliver in the included studies. The first type is exergames, which refer to video games that require physical exercises (eg, fitness and balance exercises) in order to be played. The second type is computerized CBT games, which are video games that provide CBT for the users. The third type is exposure therapy games, which are video games that apply exposure principles to reduce anxiety in users with phobias. The fourth type is brain training games, which are video games that are based on cognitive interference tasks to reconsolidate traumatic memories. The last type is REBT- and REBE-based games, which are video games that enable users to replace irrational beliefs (eg, demandingness, intolerance, and frustration) with rational beliefs (eg, unconditional acceptance and tolerance). Results of the included studies were grouped into 3 categories based on the types of serious games.
Exergames
Exergames were the intervention in 16 studies [43-58]. Exergames were compared with conventional exercises, no intervention, physical education, and occupational therapy. The results of these comparisons are summarized in the following sections.
Exergames Versus Conventional Exercises
In 9 studies, the effect of exergames was compared with that of conventional exercises on the severity of depressive symptoms [43-51]. Although 1 study did find a statistically significant difference in the severity of depressive symptoms between the groups [45], the remaining 8 studies did not [43,44,46-51]. Specifically, Song and Park [45] compared the effect of exergames (Kinect Sport, Kinect Sport Season 2, Kinect Adventure, and Kinect Gunstringer) with that of conventional exercises (ergometer bicycle training) on the severity of depressive symptoms (measured using the BDI) among patients with stroke. The study found a statistically significant difference (P<.05) in depressive symptoms between the groups, favoring exergames over ergometer training. Another study assessed the effect of exergames (Wii Fit Plus) on the severity of depressive symptoms (measured using the HADS-D) among patients with unilateral peripheral vestibular loss [47]. The study did not find any statistically significant difference (P=.49) in the severity of depressive symptoms between the exergame group and conventional exercise group [47]. Schumacher et al [46] assessed the effects of exergames (Wii Fit and Wii-Sports) and conventional exercises on depression symptoms (measured using the HADS-D) among hematopoietic stem cell transplantation recipients and found no significant difference (P=.07) between both groups in the severity of depressive symptoms. A study by Ozdogar et al [51] examined the effects of exergames (Kinect Sports Rivals) and conventional exercises on the severity of depressive symptoms among patients with multiple sclerosis, and there was no significant difference (P>.05) in the severity of depressive symptoms between the 2 groups. A study examining the effect of exergames (Kinect-RehabPlay) on the severity of depressive symptoms (measured using the BDI) among patients with coronary artery disease in comparison with conventional exercises found no significant difference in the severity of depressive symptoms between the 2 groups [49]. In another study [48], no significant difference in the severity of depressive symptoms (measured using the Center for Epidemiologic Studies Depression Scale in patients with diabetes and end-stage renal disease) was detected between the exergame group and conventional exercise group. Tollár et al [50] compared the effect of exergames (Reflex Ridge, Space Pop, Just Dance) with that of conventional exercises (ergometer bicycle training) on the severity of depressive symptoms (measured using the BDI) among patients with Parkinson disease. The study showed no statistically significant difference (P=.27) in the severity of depressive symptoms between the 2 groups. A study assessed the effects of exergames (Wii-Sports) and conventional exercises on the severity of depressive symptoms (measured by HADS) among patients with a high risk of cardiovascular diseases [43]. No statistically significant difference between the groups was reported in the study [43]. In the last study, no significant difference in the severity of depressive symptoms (measured using the Geriatric Depression Scale [GDS] in patients with Parkinson disease) was detected between the exergame group (Kinect Adventures) and 2 conventional exercise groups (functional training and bicycle exercises) [44].
Results of 7 studies were meta-analyzed as shown in Figure 3 [45-49,51]. No statistically significant difference (P=.12) in the severity of depressive symptoms was found between the exergame group and conventional exercise group (SMD –0.32, 95% CI –0.71 to 0.08). There was substantial heterogeneity in the evidence (P=.005; I2=67%). The quality of the evidence was very low, as it was downgraded by 5 levels due to a high risk of bias, heterogeneity, and imprecision (Multimedia Appendix 5).
Figure 3.
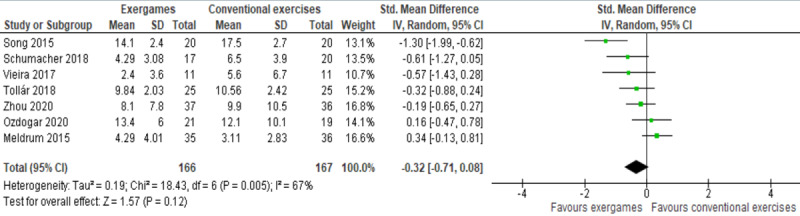
Forest plot of 7 studies comparing the effect of exergames with that of conventional exercises on the severity of depressive symptoms.
Exergames Versus No Intervention
In 7 studies, the effect of exergames was compared with that of no intervention on the severity of depressive symptoms [49-55]. Although 4 studies showed a statistically significant difference in the severity of depressive symptoms between the groups [50-52,55], 3 studies did not [49,53,54]. Specifically, Kempf and Martin [52] compared the effect of exergames (Wii Fit Plus) with that of no intervention on the severity of depressive symptoms (measured using the WHO 5-item Well-Being Index [WHO-5], Problem Areas in Diabetes [PAID], and Allgemeine Depressionsskala [ADS-L]) in patients with type 2 diabetes. The study found a statistically significant effect of exergames over no intervention on the severity of depressive symptoms as measured using the WHO-5 (P<.001), PAID (P=.007), and ADS-L (P=.002) [52]. A study conducted by Ozdogar et al [51] examined the effects of exergames (Kinect Sports Rivals) and no intervention on the severity of depressive symptoms (measured using the BDI) among patients with multiple sclerosis. Interestingly, the study demonstrated a statistically significant difference (P<.05) between the groups, favoring no intervention over exergames [51]. In another study [55], the influence of exergames (Kinect Sports Ultimate Collection, Your Shape Fitness Evolved, Dance Central, Kinect Training) and no intervention on the severity of depressive symptoms (measured using the BDI) among older women was investigated, and a statistically significant difference in the severity of depressive symptoms between groups was detected, favoring exergames over no intervention. Tollár et al [50] compared the effect of exergames (Reflex Ridge, Space Pop, Just Dance) with that of no intervention on the severity of depressive symptoms (measured using the BDI) among patients with Parkinson disease. The study showed a statistically significant difference (P<.001) in the severity of depressive symptoms between the 2 groups, favoring exergames over no intervention. Jahouh et al [54] assessed the effect of exergames (Wii Fit game) on the severity of depressive symptoms (measured using the GDS and Goldberg Anxiety and Depression Scale [GADS]) among older adults. No significant difference in the severity of depressive symptoms as measured using the GDS (P=.43) and GADS (P=.21) was detected between the exergame group and the control group [54]. Another study examining the effect of exergames (Kinect-RehabPlay) on the severity of depressive symptoms (measured using the BDI) among patients with coronary artery disease in comparison with no intervention found no significant difference (P>.05) in the severity of depressive symptoms between the 2 groups [49]. The effects of exergames and no intervention on the severity of depressive symptoms (measured by GDS) among older adults were compared in another study [53], and no significant difference (P=.09) was found in the severity of depressive symptoms between the 2 groups [53].
We meta-analyzed results of 5 studies, as they reported enough and appropriate data for the analysis [49-52,54]. Of the 5 studies, 2 assessed the severity of depressive symptoms using more than one measure (ie, WHO-5, PAID, and ADS-L [52]; GDS and GADS [54]); therefore, we included the results of all these measures in the meta-analysis. The meta-analysis showed a statistically significant difference in the severity of depressive symptoms (P=.004) between exergame and control groups, favoring exergames over no intervention (SMD –0.39, 95% CI –0.65 to –0.12; Figure 4). This difference was also clinically important as the overall effect was outside the MCID boundaries (–0.195 to 0.195) and its CI did not cross the “no effect” line (zero effect) and both MCID boundaries. The statistical heterogeneity of the evidence was substantial (P=.003; I2=68%). The quality of the evidence was very low, as it was downgraded by 6 levels due to a high risk of bias, heterogeneity, and imprecision (Multimedia Appendix 5).
Figure 4.
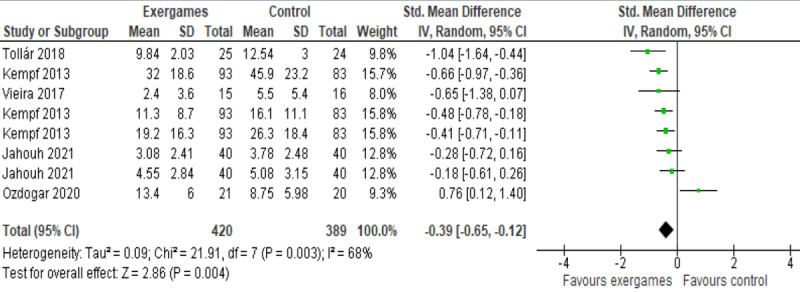
Forest plot of 5 studies (8 comparisons) comparing the effect of exergames with that of no intervention on the severity of depressive symptoms.
Exergames Versus Other Active Interventions
In 3 studies, the effect of exergames was compared with that of active interventions on the severity of depressive symptoms, and no statistically significant difference was found between the groups [56-58]. To be more precise, the first study examined the effects of an exergame (Just Dance 2015) and physical education on the severity of depressive symptoms (measured with the Brunel Mood Scale) among elementary students and demonstrated no statistically significant difference (P=.13) in the severity of depressive symptoms between the exergame group and physical education group [56]. The second study compared the effect of exergames (RehabMaster) with that of occupational therapy on the severity of depressive symptoms (measured using the Hamilton Depression Rating Scale) among patients with stroke. The study found no statistically significant difference (P=.56) in the severity of depressive symptoms between the exergame group and occupational therapy group [57]. The third study compared the effect of exergames with that of robot-assisted training on the severity of depressive symptoms (measured using the HADS) among patients with stroke and did not find any statistically significant difference between the groups [58].
Computerized CBT Games
Computerized CBT games were the intervention in 8 studies [59-66]. Computerized CBT games were compared with no intervention, video games, and conventional CBT. The results of these comparisons are summarized in the following sections.
Computerized CBT Games Versus No Intervention
In 7 studies, the effect of computerized CBT games was compared with that of no intervention on the severity of depressive symptoms [59-65], and 4 of these studies assessed the effect of a computerized CBT game (SPARX) on the severity of depressive symptoms among patients with depression [59,60,64]. The first study found a statistically significant effect of the computerized CBT game over no intervention on the severity of depressive symptoms as measured using the Children’s Depression Rating Scale-Revised (CDRS-R; P=.001) but not the Reynolds Adolescent Depression Scale (RADS-2; P=.08) [59]. In the second study [62], the effect of a computerized CBT game (SPARX-R) on the severity of depressive symptoms (measured using the Major Depression Inventory) among secondary students was compared with placebo, an interactive online program (LIFESTYLE) that provides information about several topics unrelated to mental health. The study found a statistically significant difference in the severity of depressive symptoms (as measured postintervention, P<.001, and at a 6-month follow-up, P=0.01) between the groups, favoring SPARX-R over LIFESTYLE [62]. In contrast, the third study found no statistically significant difference between the 2 groups in the severity of depressive symptoms as measured with the CDRS-R (P=.26) and RADS-2 (P=.16) [60]. Similarly, the fourth study did not show any statistically significant difference (P=.96) in the severity of depressive symptoms between the SPARX group and the control group [64]. Another study examined the effects of a computerized CBT game (Pesky Gnats: The Feel Good Island) and no intervention on the severity of depressive symptoms (measured using the Glasgow Depression Scale for people with a learning disability) among patients with anxiety, depression, or intellectual disability [63]. No statistically significant difference (P=.25) in the severity of depressive symptoms was detected between the groups [63]. Välimäki et al [65] compared the effect of a computerized CBT game (CogniFit) with that of no intervention on the severity of depressive symptoms (measured using the Patient Health Questionnaire-9 [PHQ-9]) among patients with traumatic brain injury and found no statistically significant difference (P=.76) between the groups. In the last study in this comparison, the effects of a computerized CBT game (ZeroPhobia) and no intervention on the severity of depressive symptoms (measured using the PHQ-9) among patients with acrophobia were investigated [61]. No statistically significant difference (P=.12) in the severity of depressive symptoms was found between the 2 groups [61].
Results of these 7 studies were meta-analyzed, as shown in Figure 5. Because 2 of these studies assessed the severity of depressive symptoms using 2 different measures (CDRS-R and RADS-2), we included the results of both measures of each study in the meta-analysis. The overall effect was statistically significant (P=.003) indicating that computerized CBT games are more effective than no intervention in alleviating depressive symptoms: (SMD –0.20, 95% CI –0.34 to –0.07). This difference was also clinically important as the overall effect was outside the MCID boundaries (–0.10 to 0.10) and its CI did not cross the “no effect” line (zero effect) and both MCID boundaries. For this outcome, MCID boundaries were calculated as ±0.5 times the SMD value (–.20). The heterogeneity of the evidence was not a concern (P=.26; I2= 20%). The quality of the evidence was very low, as it was downgraded by 3 levels due to the high risk of bias and impression (Multimedia Appendix 5).
Figure 5.
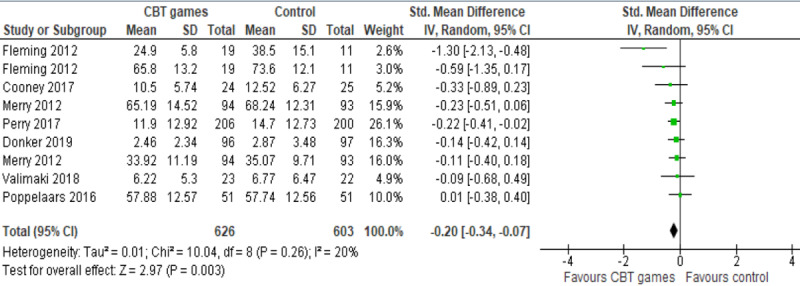
Forest plot of 7 studies (9 comparisons) comparing the effect of CBT games with that of no intervention on depression.
Computerized CBT Games Versus Active Interventions
Välimäki et al [65] compared the effect of a computerized CBT game (CogniFit) with that of entertainment video games on the severity of depressive symptoms (measured using the PHQ-9) among patients with traumatic brain injury and found no statistically significant difference (P=.36) between the groups. Another study compared the effect of a computerized CBT game (MindLight) with that of an entertainment video game (Triple Town) on the severity of depressive symptoms (Child Depression Inventory 2) among patients with autism spectrum disorder and anxiety [66]. No statistically significant difference (P>.05) in the severity of depressive symptoms was detected between the groups [66]. A study carried out by Poppelaars et al [64] assessed the effects of a computerized CBT game (SPARX) and a conventional CBT program on the severity of depressive symptoms (measured using the RADS-2) among patients with depression. The study did not detect a statistically significant difference (P=.58) in the severity of depressive symptoms between the groups.
Other Types of Serious Games
One study compared the effect of an exposure therapy game (Spider App) with that of an entertainment video game (Bubble Shooter) on the severity of depressive symptoms (measured using the BDI-II) among patients with arachnophobia [67]. No statistically significant difference (P=.95) in the severity of depressive symptoms was detected between the groups [67]. Butler et al [68] examined the effects of brain training games and psychotherapy on the severity of depressive symptoms (measured using the BDI) among patients with posttraumatic stress disorder. No statistically significant difference (P=.95) in the severity of depressive symptoms between the 2 groups was detected [68]. In another study, the effect of REBT- and REBE-based games on the severity of depressive symptoms (measured using the Early Adolescent Temperament Questionnaire-Revised) among patients with stroke was compared with conventional REBE and no intervention [69]. The study found a statistically significant difference in the severity of depressive symptoms between the groups, favoring REBT- and REBE-based games over conventional REBE (P=.03) and no intervention (P<.001).
Discussion
Principal Findings
This review assessed the effectiveness of serious games on the severity of depressive symptoms as reported by RCTs. Although 27 RCTs were included in the current review, 16 studies were included in the meta-analysis. Very low-quality evidence from 7 RCTs showed no statistically significant effect of exergames on the severity of depressive symptoms as compared with conventional exercises. Furthermore, 3 studies that compared the effect of exergames with that of other active interventions (eg, occupational therapy and robot-assisted training) on the severity of depressive symptoms and were not included in the meta-analyses found no statistically significant difference between the groups. These findings indicate that exergames are as effective as active interventions, which are usually delivered and supervised by health care providers (eg, physiotherapists, occupational therapists, and psychologists).
Very low-quality evidence from 5 RCTs showed a statistically and clinically significant effect of exergames on the severity of depressive symptoms when compared with no intervention.
Findings in this review are comparable to other reviews. Specifically, a recently published meta-analysis of 5 RCTs conducted by Yen and Chiu [37] showed an overall statistically significant effect (P<.001) of exergames on depression. Additionally, another recent meta-analysis of 8 RCTs conducted by Li et al [19] showed a significant effect of exergames on depression. However, both reviews [19,37] compared the effect of exergames with the effects of different active and inactive interventions through one meta-analysis, while our review conducted 2 separate meta-analyses to compare exergames with conventional exercises and no intervention respecting the uniqueness of these 2 interventions. Further, in contrast to our review, 5 of the 8 studies included in the review by Li et al were not RCTs (quasi-experimental or pre-post one-group trials) [19].
Very low-quality evidence from 6 RCTs showed a statistically and clinically significant effect of computerized CBT games on the severity of depressive symptoms when compared with no intervention. In contrast, 3 studies that compared the effect of computerized CBT games with those of active interventions (eg, video games and conventional CBT) on depressive symptoms and were not included in the meta-analyses found no statistically significant difference between the groups. This insignificant effect can be attributed to the fact that conventional CBT is comparable to the active interventions, thereby comparing the effect of 2 comparable interventions usually produces no significant difference, which indicates that computerized CBT games are at least as effective as these active interventions. None of the previous reviews [18,19,35-37] assessed the effect of computerized CBT games on depression.
Strengths and Limitations
Strengths
This review bridged the gaps of previous reviews by focusing on all types of serious games, including only RCTs, targeting all age groups, searching technical databases, assessing the quality of evidence, and synthesizing the data statistically. Therefore, it is more comprehensive than previous reviews [18,19,35-37]. As we followed highly recommended guidelines (ie, PRISMA) to conduct this review, it can be considered a robust and high-quality review.
The risk of publication bias in this review is minimal, as we searched the most popular databases in information technology and health fields; conducted backward and forward reference list checking; used a comprehensive search query; searched grey literature databases; and did not restrict our search to a certain country, year, setting, population, and comparator.
The risk of selection bias in this review is minimal because 2 reviewers independently performed the study selection, data extraction, risk of bias assessment, and quality of evidence evaluation with a very good interrater agreement for all processes. The quality of the evidence was appraised to enable the reader to draw more accurate conclusions. When possible, we synthesized data statistically, and this improved the power of studies and increased the estimates of the likely size of the effect of serious games on depression.
Limitations
The intervention of interest in this review was restricted to serious games delivered on any digital platform and used as a therapeutic intervention. Thus, this review cannot comment on the effectiveness of nondigital serious games and those used for other purposes such as monitoring, screening, or diagnosis. The outcome of interest in this review was depression; therefore, we cannot comment on the effectiveness of serious games on other mental health outcomes.
The review was restricted to RCTs written in the English language; therefore, many studies were excluded because they were quasi-experiments or written in other languages. This restriction was necessary because RCTs have higher internal validity than any other study design [70] and owing to practical constraints, it was not feasible to translate all non-English studies.
Most included studies recruited patients without depression; thereby, the effect of serious games on the severity of depression symptoms was not significant. Further, the overall risk of bias was high in most included studies, and the quality of evidence for the meta-analyses was very low. Accordingly, findings in this review must be interpreted with caution.
Research and Practical Implications
Research Implications
Although the severity of depression was one of the measured outcomes in all included studies, only 5 studies recruited patients with depression. This might lead to underestimating the effect of serious games. Therefore, future studies need to recruit participants with depression to assess the effectiveness of serious games on depression.
The therapeutic modalities provided by serious games in most included studies were either exercises or CBT. Further, serious games were not designed specifically to alleviate depression in about half of the studies. Thus, there is a pressing need to assess the effectiveness of serious games that are designed specifically to alleviate depression and deliver other therapeutic modalities such as art therapy, psychotherapy, relaxation-based exercises, psychoeducation, rational emotive behavioral therapy, and exposure therapy, and the list goes on.
Most included studies were carried out in high-income countries; thereby, our findings may not be generalizable to low-income countries. Researchers should conduct more studies to assess the effectiveness of serious games in low-income countries. We excluded many studies that assessed the effectiveness of serious games on other mental disorders such as anxiety and dementia. Further systematic reviews need to be carried out to investigate the effectiveness of serious in alleviating other mental disorders.
The overall risk of bias was high in most included studies mainly due to issues in the randomization process, deviations from the intended outcomes, and selection of the reported result. Further, several studies were not included in the meta-analysis due to missing outcome data. For this reason, we encourage researchers to follow recommended guidelines or tools (eg, RoB 2 [40]) when conducting and reporting RCTs to avoid such biases.
This review hopefully augurs the possible potential of serious games in mental health disorders, but it also underlines that this field, albeit full of potential, is still in its infancy. More studies are needed to prove the significant role of serious games in alleviating depression.
Practical Implications
Overall, this study showed that serious games can be effective in alleviating depression in comparison with no intervention, and they can be comparable to other traditional therapeutic interventions for alleviating depressive symptoms. However, findings in this review must be interpreted with caution because the overall risk of bias was high in most included studies, the quality of evidence in the meta-analyses was very low, few studies recruited patients with depression, and serious games in half of the studies were purpose-shifted. Therefore, we can only recommend health care providers consider offering serious games as an adjunct to existing interventions until further, more robust evidence is available.
As mentioned before, serious games in more than half of the studies were not designed to specifically alleviate depression and did not deliver other therapeutic modalities such as art therapy, REBT, and psychoeducation. This may be attributed to the lack of such serious games in real life. Accordingly, there is a need to develop more serious games that are designed to specifically alleviate depression and deliver other therapeutic modalities.
The most common platforms used for playing the games were computers and video game consoles and their accessories, which are relatively more expensive and less accessible than smartphones that were the platform for serious games in only 1 study. The number of smartphone users in the world exceeded 6.4 billion in 2021 [71], which forms about 82% of the global population (7.8 billion) [72]. We encourage developers to develop serious games that can be played through smartphones.
Most studies were carried out in high-income countries, and this may indicate the lack of serious games in low-income countries. People in low-income countries may be more in need of serious games than those in high-income countries because low-income countries have a greater shortage of mental health professionals than high-income countries (0.1 per 1,000,000 people vs 90 per 1,000,000 people) [73,74]. Serious games should be exploited to alleviate depression in low-income countries.
Gaming and mental health have traditionally been two distinctly separate fields and come with their own unique pedagogy and praxis. The potential of utilizing the advantages inherent to gaming, as described earlier, from its reach to its transformative potential in mental health holds a lot of promise in theory. However, to achieve this potential, experts from the two disciplines need to work together in order to understand the unique strengths and limitations of each field when designing serious games.
Conclusion
Overall, serious games can be better than no intervention in alleviating depression and as effective in alleviating depression as other active interventions (eg, conventional CBT, exposure therapy, conventional exercise). However, definitive conclusions regarding the effectiveness of serious games could not be drawn in this review because the overall risk of bias was high in most included studies, the quality of the meta-analyzed evidence was very low, and few studies recruited patients with depression. Therefore, we can only recommend health care providers consider offering serious games as an adjunct to existing interventions until further, more robust evidence is available. To have sufficient evidence, future studies should assess the effectiveness of serious games that are designed specifically to alleviate depression and deliver other therapeutic modalities, recruit participants with depression, and avoid biases by following recommended guidelines for conducting and reporting RCTs (eg, RoB 2).
Abbreviations
- ADS-L
Allgemeine Depressionsskala
- BDI
Beck Depression Inventory
- CBT
Cognitive behavioral therapy
- CDRS-R
Children’s Depression Rating Scale-Revised
- GADS
Goldberg Anxiety and Depression Scale
- GDS
Geriatric Depression Scale
- GRADE
Grading of Recommendations Assessment, Development and Evaluation
- HADS
Hospital Anxiety and Depression Scale
- MCID
minimal clinically important difference
- PAID
Problem Areas in Diabetes
- PHQ-9
Patient Health Questionnaire-9
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RADS-2
Reynolds Adolescent Depression Scale
- RCT
randomized controlled trial
- REBE
rational emotive behavioral education
- REBT
rational emotive behavioral therapy
- RoB 2
Risk-of-Bias 2
- SMD
standardized mean difference
- WHO
World Health Organization
- WHO-5
WHO 5-item Well-Being Index
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist.
Search strategy.
Data extraction form.
Reviewers’ judgements about each “risk of bias” domain for each included study.
Grading of Recommendations Assessment, Development and Evaluation (GRADE) Profile for comparison of serious games to control or conventional exercises for depression.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, Silove D. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980-2013. Int J Epidemiol. 2014 Apr;43(2):476–93. doi: 10.1093/ije/dyu038. http://europepmc.org/abstract/MED/24648481 .dyu038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Depression. World Health Organization. [2022-01-09]. https://www.who.int/news-room/fact-sheets/detail/depression .
- 3.Rehm J, Shield KD. Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep. 2019 Feb 07;21(2):10. doi: 10.1007/s11920-019-0997-0.10.1007/s11920-019-0997-0 [DOI] [PubMed] [Google Scholar]
- 4.Roland J, Lawrance E, Insel T, Christensen H. The digital mental health revolution: Transforming care through innovation and scale-up. World Innovation Summit for Health. 2020. [2021-01-09]. https://www.wish.org.qa/reports/the-digital-mental-health-revolution-transforming-care-through-innovation-and-scale-up/
- 5.Hall-Flavin DK. What does the term "clinical depression" mean? Mayo Clinic. 2017. May 13, [2022-01-09]. https://www.mayoclinic.org/diseases-conditions/depression/expert-answers/clinical-depression/faq-20057770 .
- 6.Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Washington, DC: American Psychiatric Publishing; 2013. [Google Scholar]
- 7.Haller H, Anheyer D, Cramer H, Dobos G. Complementary therapies for clinical depression: an overview of systematic reviews. BMJ Open. 2019 Aug 05;9(8):e028527. doi: 10.1136/bmjopen-2018-028527. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=31383703 .bmjopen-2018-028527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Riccelli R, Passamonti L, Cerasa A, Nigro S, Cavalli SM, Chiriaco C, Valentino P, Nisticò R, Quattrone A. Individual differences in depression are associated with abnormal function of the limbic system in multiple sclerosis patients. Mult Scler. 2016 Jul;22(8):1094–105. doi: 10.1177/1352458515606987.1352458515606987 [DOI] [PubMed] [Google Scholar]
- 9.Ohrnberger J, Fichera E, Sutton M. The relationship between physical and mental health: A mediation analysis. Soc Sci Med. 2017 Dec;195:42–49. doi: 10.1016/j.socscimed.2017.11.008. https://linkinghub.elsevier.com/retrieve/pii/S0277-9536(17)30663-9 .S0277-9536(17)30663-9 [DOI] [PubMed] [Google Scholar]
- 10.Park S, Oh HS, Oh D, Jung SA, Na K, Lee H, Kang R, Choi Y, Lee M, Park YC. Evidence-based, non-pharmacological treatment guideline for depression in Korea. J Korean Med Sci. 2014 Jan;29(1):12–22. doi: 10.3346/jkms.2014.29.1.12. https://jkms.org/DOIx.php?id=10.3346/jkms.2014.29.1.12 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dias L, Barbosa J, Vianna H. Gamification and serious games in depression care: A systematic mapping study. Telematics and Informatics. 2018 Apr;35(1):213–224. doi: 10.1016/j.tele.2017.11.002. doi: 10.1016/j.tele.2017.11.002. [DOI] [Google Scholar]
- 12.Chatham RE. Games for training. Commun. ACM. 2007 Jul;50(7):36–43. doi: 10.1145/1272516.1272537. [DOI] [Google Scholar]
- 13.Hwang H, Bae S, Hong JS, Han DH. Comparing effectiveness between a mobile app program and traditional cognitive behavior therapy in obsessive-compulsive disorder: evaluation study. JMIR Ment Health. 2021 Jan 19;8(1):e23778. doi: 10.2196/23778. https://mental.jmir.org/2021/1/e23778/ v8i1e23778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Charlier N, Zupancic N, Fieuws S, Denhaerynck K, Zaman B, Moons P. Serious games for improving knowledge and self-management in young people with chronic conditions: a systematic review and meta-analysis. J Am Med Inform Assoc. 2016 Jan;23(1):230–9. doi: 10.1093/jamia/ocv100. http://europepmc.org/abstract/MED/26186934 .ocv100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wiemeyer J, Kliem A. Serious games in prevention and rehabilitation—a new panacea for elderly people? Eur Rev Aging Phys Act. 2011 Dec 08;9(1):41–50. doi: 10.1007/s11556-011-0093-x. [DOI] [Google Scholar]
- 16.Wang R, DeMaria S, Goldberg A, Katz D. A systematic review of serious games in training health care professionals. Simul Healthc. 2016 Feb;11(1):41–51. doi: 10.1097/SIH.0000000000000118. [DOI] [PubMed] [Google Scholar]
- 17.Zayeni D, Raynaud J, Revet A. Therapeutic and preventive use of video games in child and adolescent psychiatry: a systematic review. Front Psychiatry. 2020;11:36. doi: 10.3389/fpsyt.2020.00036. doi: 10.3389/fpsyt.2020.00036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Li J, Theng Y, Foo S. Game-based digital interventions for depression therapy: a systematic review and meta-analysis. Cyberpsychol Behav Soc Netw. 2014 Aug;17(8):519–27. doi: 10.1089/cyber.2013.0481. http://europepmc.org/abstract/MED/24810933 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Li J, Theng Y, Foo S. Effect of exergames on depression: a systematic review and meta-analysis. Cyberpsychol Behav Soc Netw. 2016 Jan;19(1):34–42. doi: 10.1089/cyber.2015.0366. [DOI] [PubMed] [Google Scholar]
- 20.Matthyssens L, Vanhulle A, Seldenslach L, Vander Stichele G, Coppens M, Van Hoecke E. A pilot study of the effectiveness of a serious game CliniPup® on perioperative anxiety and pain in children. J Pediatr Surg. 2020 Feb;55(2):304–311. doi: 10.1016/j.jpedsurg.2019.10.031. doi: 10.1016/j.jpedsurg.2019.10.031.S0022-3468(19)30766-3 [DOI] [PubMed] [Google Scholar]
- 21.Radkowski R, Huck W, Domik G, Holtmann M. Serious Games for the Therapy of the Posttraumatic Stress Disorder of Children and Adolescents. In: Shumaker R, editor. Virtual and Mixed Reality - Systems and Applications. VMR 2011. Lecture Notes in Computer Science, vol 6774. Berlin, Germany: Springer; 2011. pp. 44–53. [Google Scholar]
- 22.Jones M, Denisova A, Mitchell S, Owen T. Acceptability of a plasticity-focused serious game intervention for posttraumatic stress disorder: user requirements analysis. JMIR Serious Games. 2019 Apr 16;7(2):e11909. doi: 10.2196/11909. https://games.jmir.org/2019/2/e11909/ v7i2e11909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Barajas AO, Osman HA, Shirmohammadi S. A Serious Game for children with Autism Spectrum Disorder as a tool for play therapy. IEEE 5th International Conference on Serious Games and Applications for Health (SeGAH); April 2-4, 2017; Perth, Western Australia. 2017. https://ieeexplore.ieee.org/document/7939266 . [DOI] [Google Scholar]
- 24.Tang JSY, Falkmer M, Chen NTM, Bӧlte S, Girdler S. Designing a serious game for youth with ASD: perspectives from end-users and professionals. J Autism Dev Disord. 2019 Mar;49(3):978–995. doi: 10.1007/s10803-018-3801-9.10.1007/s10803-018-3801-9 [DOI] [PubMed] [Google Scholar]
- 25.McCallum S, Boletsis C. Dementia Games: A Literature Review of Dementia-Related Serious Games. In: Ma M, Oliveira MF, Petersen S, Hauge JB, editors. Serious Games Development and Applications. SGDA 2013. Lecture Notes in Computer Science, vol 8101. Berlin, Germany: Springer; 2013. pp. 15–27. [Google Scholar]
- 26.Zhao Y, Feng H, Wu X, Du Y, Yang X, Hu M, Ning H, Liao L, Chen H, Zhao Y. Effectiveness of exergaming in improving cognitive and physical function in people with mild cognitive impairment or dementia: systematic review. JMIR Serious Games. 2020 Jun 30;8(2):e16841. doi: 10.2196/16841. https://games.jmir.org/2020/2/e16841/ v8i2e16841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Verduin ML, LaRowe SD, Myrick H, Cannon-Bowers J, Bowers C. Computer simulation games as an adjunct for treatment in male veterans with alcohol use disorder. J Subst Abuse Treat. 2013 Mar;44(3):316–22. doi: 10.1016/j.jsat.2012.08.006.S0740-5472(12)00141-9 [DOI] [PubMed] [Google Scholar]
- 28.Dovis S, Van der Oord S, Wiers RW, Prins PJM. Improving executive functioning in children with ADHD: training multiple executive functions within the context of a computer game. a randomized double-blind placebo controlled trial. PLoS One. 2015;10(4):e0121651. doi: 10.1371/journal.pone.0121651. https://dx.plos.org/10.1371/journal.pone.0121651 .PONE-D-14-16366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hong JS, Kim SM, Aboujaoude E, Han DH. Investigation of a mobile "serious game" in the treatment of obsessive-compulsive disorder: a pilot study. Games Health J. 2018 Oct;7(5):317–326. doi: 10.1089/g4h.2017.0158. [DOI] [PubMed] [Google Scholar]
- 30.Cruz R. The Modern Economics of the Video Games Industry. University of Miami. [2022-01-09]. https://com.miami.edu/wp-content/uploads/2021/06/mma_2021_firstplace.pdf .
- 31.Mental health. World Health Organization. [2022-01-09]. https://www.who.int/health-topics/mental-health#tab=tab_1 .
- 32.Eyal N. Hooked: How to build habit-forming products. Brentford, Middlesex, United Kingdom: Portfolio; 2014. [Google Scholar]
- 33.Fleming TM, Bavin L, Stasiak K, Hermansson-Webb E, Merry SN, Cheek C, Lucassen M, Lau HM, Pollmuller B, Hetrick S. Serious games and gamification for mental health: current status and promising directions. Front Psychiatry. 2016;7:215. doi: 10.3389/fpsyt.2016.00215. doi: 10.3389/fpsyt.2016.00215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cheek C, Fleming T, Lucassen MF, Bridgman H, Stasiak K, Shepherd M, Orpin P. Integrating health behavior theory and design elements in serious games. JMIR Ment Health. 2015;2(2):e11. doi: 10.2196/mental.4133. https://mental.jmir.org/2015/2/e11/ v2i2e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fleming TM, Cheek C, Merry SN, Thabrew H, Bridgman H, Stasiak K, Shepherd M, Perry Y, Hetrick S. Juegos serios para el tratamiento o la prevención de la depresión: una revisión sistemática. RPPC. 2015 Jan 15;19(3):227. doi: 10.5944/rppc.vol.19.num.3.2014.13904. [DOI] [Google Scholar]
- 36.Lau HM, Smit JH, Fleming TM, Riper H. Serious games for mental health: are they accessible, feasible, and effective? A systematic review and meta-analysis. Front Psychiatry. 2016;7:209. doi: 10.3389/fpsyt.2016.00209. doi: 10.3389/fpsyt.2016.00209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yen H, Chiu H. Virtual reality exergames for improving older adults' cognition and depression: a systematic review and meta-analysis of randomized control trials. J Am Med Dir Assoc. 2021 May;22(5):995–1002. doi: 10.1016/j.jamda.2021.03.009.S1525-8610(21)00305-4 [DOI] [PubMed] [Google Scholar]
- 38.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009 Jul 21;339(jul21 1):b2700–b2700. doi: 10.1136/bmj.b2700. http://europepmc.org/abstract/MED/19622552 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Altman DG. Practical statistics for medical research. Boca Raton, FL: CRC press; 1990. [Google Scholar]
- 40.Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;366:l4898. doi: 10.1136/bmj.l4898. [DOI] [PubMed] [Google Scholar]
- 41.Deeks JJ, Higgins JPT, Altman DG, Cochrane Statistical Methods Group . Analysing data and undertaking meta-analyses. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Sussex, UK: John Wiley & Sons; 2008. pp. 243–296. [Google Scholar]
- 42.Schunemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, Guyatt GH, Cochrane Applicability and Recommendations Methods Group . Interpreting results and drawing conclusions. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Sussex, UK: John Wiley & Sons; 2008. pp. 359–87. [Google Scholar]
- 43.Ruivo JMADS, Karim K, OʼShea R, Oliveira RCS, Keary L, OʼBrien C, Gormley JP. In-class active video game supplementation and adherence to cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2017 Jul;37(4):274–278. doi: 10.1097/HCR.0000000000000224. [DOI] [PubMed] [Google Scholar]
- 44.Ferraz DD, Trippo KV, Duarte GP, Neto MG, Bernardes Santos KO, Filho JO. The effects of functional training, bicycle exercise, and exergaming on walking capacity of elderly patients with Parkinson cisease: A pilot randomized controlled single-blinded trial. Arch Phys Med Rehabil. 2018 May;99(5):826–833. doi: 10.1016/j.apmr.2017.12.014.S0003-9993(18)30009-1 [DOI] [PubMed] [Google Scholar]
- 45.Song GB, Park EC. Effect of virtual reality games on stroke patients' balance, gait, depression, and interpersonal relationships. J Phys Ther Sci. 2015 Jul;27(7):2057–60. doi: 10.1589/jpts.27.2057. http://europepmc.org/abstract/MED/26311925 .jpts-2015-142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Schumacher H, Stüwe S, Kropp P, Diedrich D, Freitag S, Greger N, Junghanss C, Freund M, Hilgendorf I. A prospective, randomized evaluation of the feasibility of exergaming on patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018 May;53(5):584–590. doi: 10.1038/s41409-017-0070-8.10.1038/s41409-017-0070-8 [DOI] [PubMed] [Google Scholar]
- 47.Meldrum D, Herdman S, Vance R, Murray D, Malone K, Duffy D, Glennon A, McConn-Walsh R. Effectiveness of conventional versus virtual reality-based balance exercises in vestibular rehabilitation for unilateral peripheral vestibular loss: results of a randomized controlled trial. Arch Phys Med Rehabil. 2015 Jul;96(7):1319–1328.e1. doi: 10.1016/j.apmr.2015.02.032.S0003-9993(15)00289-0 [DOI] [PubMed] [Google Scholar]
- 48.Zhou H, Al-Ali F, Kang GE, Hamad AI, Ibrahim RA, Talal TK, Najafi B. Application of wearables to facilitate virtually supervised intradialytic exercise for reducing depression symptoms. Sensors (Basel) 2020 Mar 12;20(6):1. doi: 10.3390/s20061571. https://www.mdpi.com/resolver?pii=s20061571 .s20061571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Vieira A, Melo C, Machado J, Gabriel J. Virtual reality exercise on a home-based phase III cardiac rehabilitation program, effect on executive function, quality of life and depression, anxiety and stress: a randomized controlled trial. Disabil Rehabil Assist Technol. 2018 Feb;13(2):112–123. doi: 10.1080/17483107.2017.1297858. [DOI] [PubMed] [Google Scholar]
- 50.Tollár J, Nagy F, Hortobágyi T. Vastly different exercise programs similarly improve Parkinsonian symptoms: a randomized clinical trial. Gerontology. 2019;65(2):120–127. doi: 10.1159/000493127.000493127 [DOI] [PubMed] [Google Scholar]
- 51.Ozdogar AT, Ertekin O, Kahraman T, Yigit P, Ozakbas S. Effect of video-based exergaming on arm and cognitive function in persons with multiple sclerosis: A randomized controlled trial. Mult Scler Relat Disord. 2020 May;40:101966. doi: 10.1016/j.msard.2020.101966.S2211-0348(20)30042-0 [DOI] [PubMed] [Google Scholar]
- 52.Kempf K, Martin S. Autonomous exercise game use improves metabolic control and quality of life in type 2 diabetes patients - a randomized controlled trial. BMC Endocr Disord. 2013 Dec 10;13:57. doi: 10.1186/1472-6823-13-57. https://bmcendocrdisord.biomedcentral.com/articles/10.1186/1472-6823-13-57 .1472-6823-13-57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rendon AA, Lohman EB, Thorpe D, Johnson EG, Medina E, Bradley B. The effect of virtual reality gaming on dynamic balance in older adults. Age Ageing. 2012 Jul;41(4):549–52. doi: 10.1093/ageing/afs053.afs053 [DOI] [PubMed] [Google Scholar]
- 54.Jahouh M, González-Bernal JJ, González-Santos J, Fernández-Lázaro D, Soto-Cámara R, Mielgo-Ayuso J. Impact of an intervention with Wii video games on the autonomy of activities of daily living and psychological-cognitive components in the institutionalized elderly. Int J Environ Res Public Health. 2021 Feb 07;18(4):1. doi: 10.3390/ijerph18041570. https://www.mdpi.com/resolver?pii=ijerph18041570 .ijerph18041570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rica RL, Shimojo GL, Gomes MC, Alonso AC, Pitta RM, Santa-Rosa FA, Pontes Junior FL, Ceschini F, Gobbo S, Bergamin M, Bocalini DS. Effects of a Kinect-based physical training program on body composition, functional fitness and depression in institutionalized older adults. Geriatr Gerontol Int. 2020 Mar;20(3):195–200. doi: 10.1111/ggi.13857. [DOI] [PubMed] [Google Scholar]
- 56.Andrade A, Cruz WMD, Correia CK, Santos ALG, Bevilacqua GG. Effect of practice exergames on the mood states and self-esteem of elementary school boys and girls during physical education classes: A cluster-randomized controlled natural experiment. PLoS One. 2020;15(6):e0232392. doi: 10.1371/journal.pone.0232392. https://dx.plos.org/10.1371/journal.pone.0232392 .PONE-D-19-24839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Shin J, Bog Park S, Ho Jang S. Effects of game-based virtual reality on health-related quality of life in chronic stroke patients: A randomized, controlled study. Comput Biol Med. 2015 Aug;63:92–8. doi: 10.1016/j.compbiomed.2015.03.011.S0010-4825(15)00089-X [DOI] [PubMed] [Google Scholar]
- 58.Adomavičienė A, Daunoravičienė K, Kubilius R, Varžaitytė L, Raistenskis J. Influence of new technologies on post-stroke rehabilitation: a comparison of Armeo Spring to the Kinect system. Medicina (Kaunas) 2019 Apr 09;55(4):98. doi: 10.3390/medicina55040098. https://www.mdpi.com/resolver?pii=medicina55040098 .medicina55040098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Fleming T, Dixon R, Frampton C, Merry S. A pragmatic randomized controlled trial of computerized CBT (SPARX) for symptoms of depression among adolescents excluded from mainstream education. Behav Cogn Psychother. 2012 Oct;40(5):529–41. doi: 10.1017/S1352465811000695.S1352465811000695 [DOI] [PubMed] [Google Scholar]
- 60.Merry SN, Stasiak K, Shepherd M, Frampton C, Fleming T, Lucassen MFG. The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ. 2012 Apr 18;344(apr18 3):e2598–e2598. doi: 10.1136/bmj.e2598. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=22517917 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Donker T, Cornelisz I, van Klaveren C, van Straten A, Carlbring P, Cuijpers P, van Gelder J. Effectiveness of self-guided app-based virtual reality cognitive behavior therapy for acrophobia: a randomized clinical trial. JAMA Psychiatry. 2019 Jul 01;76(7):682–690. doi: 10.1001/jamapsychiatry.2019.0219. http://europepmc.org/abstract/MED/30892564 .2728184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Perry Y, Werner-Seidler A, Calear A, Mackinnon A, King C, Scott J, Merry S, Fleming T, Stasiak K, Christensen H, Batterham PJ. Preventing depression in final year secondary students: school-based randomized controlled trial. J Med Internet Res. 2017 Nov 02;19(11):e369. doi: 10.2196/jmir.8241. https://www.jmir.org/2017/11/e369/ v19i11e369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Cooney P, Jackman C, Coyle D, O'Reilly G. Computerised cognitive-behavioural therapy for adults with intellectual disability: randomised controlled trial. Br J Psychiatry. 2017 Aug;211(2):95–102. doi: 10.1192/bjp.bp.117.198630.S0007125000281877 [DOI] [PubMed] [Google Scholar]
- 64.Poppelaars M, Tak YR, Lichtwarck-Aschoff A, Engels RCME, Lobel A, Merry SN, Lucassen MFG, Granic I. A randomized controlled trial comparing two cognitive-behavioral programs for adolescent girls with subclinical depression: A school-based program (Op Volle Kracht) and a computerized program (SPARX) Behav Res Ther. 2016 May;80:33–42. doi: 10.1016/j.brat.2016.03.005.S0005-7967(16)30041-9 [DOI] [PubMed] [Google Scholar]
- 65.Välimäki M, Mishina K, Kaakinen JK, Holm SK, Vahlo J, Kirjonen M, Pekurinen V, Tenovuo O, Korkeila J, Hämäläinen H, Sarajuuri J, Rantanen P, Orenius T, Koponen A. Digital gaming for improving the functioning of people with traumatic brain injury: randomized clinical feasibility study. J Med Internet Res. 2018 Mar 19;20(3):e77. doi: 10.2196/jmir.7618. https://www.jmir.org/2018/3/e77/ v20i3e77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Wijnhoven LA, Creemers DH, Vermulst AA, Lindauer RJ, Otten R, Engels RC, Granic I. Effects of the video game 'Mindlight' on anxiety of children with an autism spectrum disorder: A randomized controlled trial. J Behav Ther Exp Psychiatry. 2020 Sep;68:101548. doi: 10.1016/j.jbtep.2020.101548.S0005-7916(18)30277-5 [DOI] [PubMed] [Google Scholar]
- 67.Haberkamp A, Walter H, Althaus P, Schmuck M, Rief W, Schmidt F. Testing a gamified Spider App to reduce spider fear and avoidance. J Anxiety Disord. 2021 Jan;77:102331. doi: 10.1016/j.janxdis.2020.102331.S0887-6185(20)30145-6 [DOI] [PubMed] [Google Scholar]
- 68.Butler O, Herr K, Willmund G, Gallinat J, Kühn S, Zimmermann P. Trauma, treatment and Tetris: video gaming increases hippocampal volume in male patients with combat-related posttraumatic stress disorder. J Psychiatry Neurosci. 2020 Jul 01;45(4):279–287. doi: 10.1503/jpn.190027. https://www.jpn.ca/lookup/pmidlookup?view=long&pmid=32293830 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.David OA, Cardoș RAI, Matu S. Is REThink therapeutic game effective in preventing emotional disorders in children and adolescents? Outcomes of a randomized clinical trial. Eur Child Adolesc Psychiatry. 2019 Jan 10;28(1):111–122. doi: 10.1007/s00787-018-1192-2.10.1007/s00787-018-1192-2 [DOI] [PubMed] [Google Scholar]
- 70.Bhattacherjee A. Social science research: Principles, methods, and practices. Scotts Valley, CA: CreateSpace Independent Publishing Platform; 2012. [Google Scholar]
- 71.Ericsson Mobility Report. Ericsson. 2021. Jun 23, [2022-01-09]. https://www.ericsson.com/en/mobility-report/mobility-visualizer?f=1&ft=1&r=1&t=8&s=1&u=1&y=2016,2021&c=1 .
- 72.Worldometer Current World Population. 2021 July 23, 2021. Jul 23, [2022-01-09]. https://www.worldometers.info/world-population/
- 73.Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabé E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fèvre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FGR, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gonzalez-Medina D, Gosselin R, Grainger R, Grant B, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo J, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Laden F, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Levinson D, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer A, Miglioli V, Miller M, Miller TR, Mitchell PB, Mock C, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KMV, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O'Donnell M, O'Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leòn FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJC, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiebe N, Wiersma ST, Wilkinson JD, Williams HC, Williams SRM, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh P, Zaidi AKM, Zheng Z, Zonies D, Lopez AD, AlMazroa MA, Memish ZA. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012 Dec 15;380(9859):2197–223. doi: 10.1016/S0140-6736(12)61689-4.S0140-6736(12)61689-4 [DOI] [PubMed] [Google Scholar]
- 74.Oladeji BD, Gureje O. Brain drain: a challenge to global mental health. BJPsych Int. 2016 Aug 02;13(3):61–63. doi: 10.1192/s2056474000001240. http://europepmc.org/abstract/MED/29093905 .S2056474000001240 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist.
Search strategy.
Data extraction form.
Reviewers’ judgements about each “risk of bias” domain for each included study.
Grading of Recommendations Assessment, Development and Evaluation (GRADE) Profile for comparison of serious games to control or conventional exercises for depression.