

Abstract
Background
Children have a higher chance of decreasing health-related physical fitness during periods of school lockdown due to pandemic situations such as with COVID-19 disease.
Aims
To establish the changes in children’s self-perceived physical fitness (SPPF) during pandemic COVID-19 social distancing in a school lockdown and to describe the individual prevalence of changes in SPPF according to sex.
Methods
It is an intervention study with a convenient sample, 67 children (6–13 years old; 50.7% girls). An intervention occurred according to the Brazilian Base Nacional Comum Curricular (BNCC) and the State Education Secretary orientations for remote Physical Education classes. SPPF was evaluated through a questionnaire (QAPA). Generalized estimative equations (GEE) and the prevalence of changes in individual score delta (Δ) from baseline to follow-up determined the effects.
Results
Positive individual changes in SPPF were observed for 21.2% of girls and 26.4% of boys. Older children presented fewer SPPF total points. There was no interaction between the evaluation period, sex, and age. However, higher baseline SPPF values presented a negative association with the individual SPPF variation (β = − 2.52%; CI 95% − 3.97 to − 1.07; p = 0.001).
Conclusion
A remote Physical Education intervention effectively maintained or even increased individual results of children’s SPPF. Thereby, this study suggests that this kind of initiative should be retained for the duration of social distancing and pandemic conditions to help children maintain an active lifestyle and, consequently, achieve health benefits. Improving intervention effectiveness by focusing on girls seems to be a challenge in this matter.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11332-022-00897-1.
Keywords: Self-report; Internet-based intervention; Early intervention, educational; Physical Education and training; SARS-CoV-2
Introduction
Physical fitness is an important set of components related to children’s body health capacities for day-to-day tasks (e.g., walking, playing, and moving from home to school) and better performance in sports [1]. In addition, it is a powerful marker of health in children and youth [2, 3]. Its higher levels are associated with a better profile in cardiometabolic variables [4–6], reduced risk of cardiovascular diseases [7], better cognition [8, 9], increased mental health [10], and it helps the development of a healthy lifestyle in children [11]. Therefore, it is highlighted the importance of evaluating and developing interventions to increase physical fitness levels during childhood and adolescence [12].
However, as a consequence of the COVID-19 pandemic, several preventive measures were adopted, such as social distance, lockdown, and schools’ closure [13]. The adverse effects related to COVID-19 resulted in the increase of sedentary behavior, physical fitness decreasing and lowering the quality of life [13–18]. During this period of restrictions, physical activity was limited, and changes in dietary behaviors were observed, leading to weight gain among children and youth [19]. Consequently, the prevalence of obesity rates which were already alarming tended to increase [20]. Another aspect contributing to this scenario was that the Physical Education classes were not applied in the school environment based on its traditional approach [17, 18, 21–24]. For example, Physical Education classes were done without an open sports court, involving a non-practical methodology with children alone at home. Given that context, it is difficult to establish high-intensity activities to promote an increase in physical fitness levels mainly because of motivational aspects [17, 18, 21–25].
On the other hand, for many children, Physical Education classes are the only opportunity of increasing physical fitness, practicing sports, physical exercise, and evaluating physical fitness [17, 18, 21–24]. In addition, Physical Education improves the general well-being related to body self-perception [22, 23]. In these interventions, it is more probable that boys and young children have better effects than girls and older children/adolescents because it is easier for these groups to reach higher levels of physical activity, less sedentary behavior [17], and most psychological satisfaction with traditional interventions that involve physical activity and sports [24, 25].
However, traditional evaluations of children’s physical fitness have not been applied due to social distancing and lockdown. Thus, previous studies have shown that questionnaires are adequate resources for monitoring indicators related to fitness, physical activity, and health in children in social distancing context, mainly in lockdown [17, 18, 25, 26]. Some cross-sectional diagnoses were made indicating that sedentary behavior, low levels of physical activity, and low levels of physical fitness were evident [14, 17, 18, 27, 28].
However, according to our knowledge, there are no interventions or baseline to follow-up studies with Physical Education, sports, and physical activity at school context in the remote form to improve children’s self-perceived physical fitness (SPPF) during social distancing. In addition, we have evaluated the changes of this indicator during Physical Education classes in the non-presence form at the 2020 scholar year. Likewise, the knowledge about intervention effects on self-perceived health indicators in children during the COVID-19 social distancing is scarce. Thus, the present study hypothesizes that a Physical Education proposal in pandemic COVID-19 can improve SPPF in children. Consequently, this study aims to establish the changes in children’s SPPF during pandemic COVID-19 social distancing in a school lockdown and to describe the individual prevalence of changes in SPPF according to sex.
Methods
Design
It is an intervention study [29] based on a distancing Physical Education proposal due to COVID-19. It was developed considering a quantitative approach [29]. Baseline evaluations occurred in the first week of May, and follow-up took place in the second week of December 2020 (the research lasted approximately 28 weeks).
Ethics procedures
The study was approved by the National Research and Ethics Committee from Universidade Estácio de Sá (CEP: 25315518.4.0000.5357—NP: 3.758.311). Parents and legal guardians signed the consent form, the children signed the assent form, and the school allowed the study. The terms of the Helsinki Declaration were followed according to the standardization of research with humans [30].
Population and sample description
The population consists of 750 schoolchildren from a public school in Santa Catarina, southern Brazil. The present study was composed of a convenient sample of 67 children (6–13 years old), 34 girls with a mean age of 9.41 (±1.74), and 33 boys aged 9.39 (±1.81) years. The sample was selected due to the need of the school to improve the Physical Education methodology for children during pandemic times. The sample size was estimated according to statistical power [31], considering the criteria described as follows.
Inclusion criteria
(1) to be enrolled in a participant school; (2) to be a student between first (1st) to fifth (5th) grade from early years of elementary education; (3) to have access to google classroom, to attend, and participate effectively in Physical Education classes regularly with a minimum of three times a week; (4) to access to the google formulary about “self-perceived physical fitness questionnaire– QAPA” in May and December; (5) to answer all ten items of the questionnaire.
Exclusion criteria
(1) Children under 8 years of age who did not respond to the survey instruments without the supervision of their parents, legal guardians, or teachers (control carried out through contact between parents and teacher through the WhatsApp application and google classroom).
Physical Education classes in remote form during pandemic COVID-19
The Physical Education classes were carried on at Google Classroom, and the printed material was sent to the children and families without internet access through schools. The general objectives of the classes were established according to the Base Nacional Comum Curricular (BNCC) [32], aligned to Santa Catarina State Education Secretary specific orientations [33], and needs for social distancing [35]. In the present Physical Education intervention, the objectives were:
To be competent to maintain daily physical activity (body movement practices) as part of the routine during pandemic COVID-19 social distancing;
To learn to browser and to make Physical Education tasks through Google Suite digital media, forms, and Google classroom;
To develop basic skills to perform Physical Education tasks using the digital resources (Google Suite) provided by the education department;
Being autonomous and knowing how to request support from an adult in the family to use digital media to take Physical Education classes at home;
To do the physical exercises, body movement practices, to play sports, dance, games, and physical activity at home;
To motivate children, parents, and family to be physically active during social distancing using concepts, orientations, and comprehension.
The classes were organized by themes through time (supplementary table). Parents and family were invited to learn along with the children to promote the intervention’s effectiveness. All orientations were given to promote movements and organized physical exercises at home. In addition, it was elaborated and sent to parents and families an E-book with orientations about how to practice physical activity and physical exercises at home with a didactic, practical, and pedagogical approach [35]. The classes were developed and shared in google classroom on Monday. The teacher guided children and parents during the week about the movies, texts, and tasks (supplementary table).
Outcome measure: QAPA—Self-Perceived Physical Fitness (SPPF)
The SPPF was estimated according to the QAPA (in Portuguese: Questionário de Aptidão Física Auto relatada), a questionnaire proposed and validated in Brazil by Lemes et al. [18], which proved to be easily applicable in Brazilian Physical Education classes. The QAPA is a short questionnaire created specifically to facilitate the children’s understanding regarding self-perception of physical fitness in strength, flexibility, body weight, general fitness, and cardiorespiratory fitness. The questions were written originally in Portuguese based on another questionnaire [26, 36]. The QAPA presents a consistency and reliability of 0.70–0.80 [18] and a significative (β’s = − 0.17 and 0.45; p=0.001) association with body mass index and cardiorespiratory fitness, suggesting that it is a valid instrument to measure SPPF [18].
Parents and legal guardians were invited to help children under 8 years old to answer the questions of QAPA applied in Google Classroom using an automatic formulary according to teacher instructions. Thus, children answered ten closed questions. The answers were marked in an ordinal scale, which, when summed, should present a general SPPF score ranging from 10 to 30 points. A score greater than 24 indicated children with high SPPF, while children with lower scores were classified with low SPPF [18]. The content of the questionnaire is presented below. An expert translated it from the Portuguese language into English (supplementary file).
Statistical analysis
First, a confirmatory factorial analysis to estimate the reliability of QAPA in the present sample was performed according to Ômega of McDonald (Mc-ω) and Cronbach’s alpha (C-α) [37], with sex and periods of evaluation analyzed separately. Descriptive statistics were performed (mean/standard deviation) to characterize the sample.
Considering that the QAPA points did not present a parametric distribution in post-test in girls, we established the changes according to a generalized estimative equation (GEE model) with a transformation matrix in log distribution, a robust estimator, sex, and age as intervenient effects on QAPA raw points in baseline versus follow-up period.
Delta (Δ) values were calculated: (individual follow-up values) – (baseline values), and transformed in percentage considering individual baseline values as 100% [29, 38, 39]. It was applied as a dependent variable in the GEE model to verify the b-effects on Δ% considering baseline values, sex, and age as independent factors.
Finally, the individual pedagogical effects were estimated, considering a variation of about 10% as a relevant individual effect [29, 38, 39]. Thus, children that increased three points or more of Δ SPF were classified as “positive change”, and a decrease of fewer than three points was classified as “negative change”. Children that showed Δ SPPF variation between − 2 and 2 points were classified as “without changes”. Data were presented by a graphic specific for responders and non-responders to intervention with Physical Education [39, 40].
The sample size was estimated according G*Power software, a posteriori [31]. This calculation was perfomed considering the following parameters: a GEE test, with an interchanged matrix, for repeated outcome, non-parametric (log) distribution, robust estimator, a small to moderate effect of 0.10–0.40, 5% of error, and 95% of power test (1-b). This resulted in a minimum sample size of 60 children, enabling a statistical division by sex to verify the aimed effects. Thus, 67 children were included in the present sample considering about 10% of possible missing on the follow-up period.
Results
Table 1 shows the McDonald’s ω and Cronbach’s α and descriptive statistics in the total sample, baseline, and follow-up periods for boys and girls. This analysis presents that QAPA is a reliable and consistent questionnaire, considering high-reliability values, between 0.71 and 0.77 for both sexes. Regarding the descriptive characteristics, for girls, QAPA07 had the lowest average (1.796) and QAPA01 the highest (2.551), both in the follow-up period. Boys presented the most homogenous mean distributions, ranging between 2.082 in QAPA07 and 2.475 in QAPA10 at follow-up.
Table 1.
QAPA reliability and sample characteristics by sexes and evaluation period
| Reliability | Total | Girls (n = 34) | Boys (n = 33) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up (28 weeks) | Baseline | Follow-up (28 weeks) | |||||||
| Mc-ω | C-α | Mc-ω | C-α | Mc-ω | C-α | Mc-ω | C-α | Mc-ω | C-α | |
| Estimate | 0.752 | 0.742 | 0.736 | 0.712 | 0.771 | 0.768 | 0.775 | 0.771 | 0.731 | 0.718 |
| 95% CI lower | 0.718 | 0.705 | 0.677 | 0.642 | 0.676 | 0.648 | 0.724 | 0.713 | 0.632 | 0.595 |
| 95% CI upper | 0.786 | 0.776 | 0.796 | 0.771 | 0.866 | 0.853 | 0.826 | 0.819 | 0.831 | 0.809 |
| QAPA item | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| QAPA01 | 2.356 | 0.976 | 2.442 | 0.869 | 2.551 | 0.843 | 2.232 | 1.077 | 2.295 | 1.038 |
| QAPA02 | 2.306 | 0.854 | 2.264 | 0.859 | 2.367 | 0.755 | 2.335 | 0.895 | 2.279 | 0.819 |
| QAPA03 | 2.032 | 0.902 | 1.896 | 0.953 | 2.122 | 0.726 | 2.104 | 0.950 | 2.115 | 0.709 |
| QAPA04 | 2.425 | 0.788 | 2.350 | 0.843 | 2.367 | 0.755 | 2.494 | 0.755 | 2.475 | 0.744 |
| QAPA05 | 2.189 | 0.805 | 2.012 | 0.816 | 2.327 | 0.658 | 2.274 | 0.801 | 2.311 | 0.827 |
| QAPA06 | 2.194 | 0.906 | 2.092 | 0.922 | 2.143 | 0.791 | 2.268 | 0.894 | 2.295 | 0.972 |
| QAPA07 | 2.030 | 0.918 | 1.969 | 0.906 | 1.796 | 0.935 | 2.134 | 0.950 | 2.082 | 0.822 |
| QAPA08 | 2.326 | 0.843 | 2.387 | 0.849 | 2.408 | 0.762 | 2.317 | 0.835 | 2.131 | 0.903 |
| QAPA09 | 2.288 | 0.842 | 2.123 | 0.935 | 2.449 | 0.738 | 2.384 | 0.779 | 2.344 | 0.772 |
| QAPA10 | 2.356 | 0.772 | 2.325 | 0.823 | 2.265 | 0.670 | 2.366 | 0.776 | 2.475 | 0.698 |
Mc-ω McDonald’s ω, C-α Cronbach’s α, 95% CI confidence interval, SD standard deviation, QAPA 01 to 10 are questions in QAPA measured in points
Table 2 and Fig. 1 presents results from the same GEE model. In Fig. 1, it is possible to perceive that QAPA means and β effects from the transition of baseline to follow-up periods are impacted only by children’s age. Older children have fewer total raw points in QAPA. There was no interaction between the evaluation period, sexes, and age.
Table 2.
GEE model for β-effects considering periods (baseline x follow-up), with sex and age interaction on levels of SPPF in QAPA (continues in Fig. 1)
| Independent factors | QAPA Raw points |
95% CI | GEE test | |||
|---|---|---|---|---|---|---|
| β | SE | Lower | Upper | Wald (× 2) | p value | |
| Model | ||||||
| (intercept) | 30.394 | 3.851 | 22.845 | 37.942 | 62.279 | 0.001 |
| Intervention period | ||||||
| Baseline | 0.812 | 2.038 | − 3.182 | 4.806 | 0.159 | 0.690 |
| Follow-up | (Ref) | |||||
| Sex | ||||||
| Girls | − 7.381 | 5.382 | − 17.929 | 3.168 | 1.881 | 0.170 |
| Boys | (Ref) | |||||
| Age | − 0.810 | 0.407 | − 1.609 | − 0.012 | 3.954 | 0.047 |
| Baseline × girls × age | 0.710 | 0.608 | − 0.482 | 1.901 | 1.362 | 0.243 |
| Interaction | ||||||
| Baseline × boys × age | − 0.002 | 0.216 | − 0.426 | 0.423 | 0.000 | 0.994 |
| Follow-up × girls × age | 0.747 | 0.553 | − 0.336 | 1.830 | 1.826 | 0.177 |
| Follow-up × boys × age | (Ref) | |||||
SPPF self-perceived physical fitness, 95% CI confidence interval, SE standard error, GEE generalized estimative equation, QAPA self-perceived physical fitness questionnaire. Bold values are statistically significant for p < 0.05
Fig. 1.
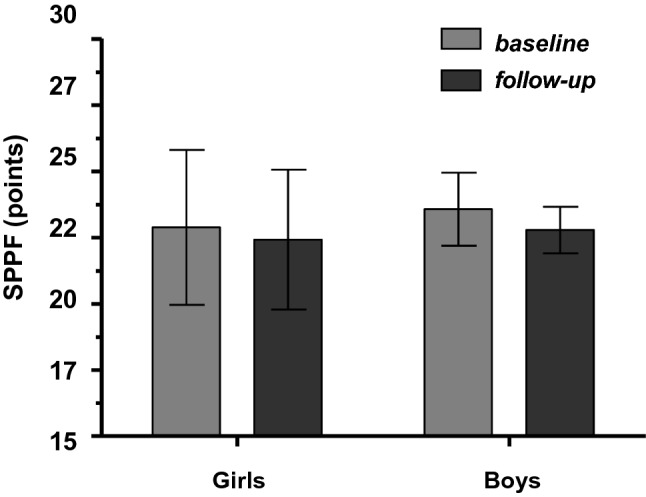
GEE model for means variability comparison considering intervention periods (baseline × follow-up), with sex and age interaction on levels of SPPF in QAPA (Table 1 continued); QAPA self-perceived physical fitness questionnaire, GEE general estimative equations
Figure 1 indicates no statistical differences for the means variability between baseline and follow-up periods for boys and girls (p=0.690, for both sexes). There were no sex differences (p=0.243/0.177). The exact mean and standard errors (SE) values (Fig. 1) considered the interaction GEE model (Table 2): girls—mean at baseline 22,88 (SE=16.80), mean at follow-up 22.42 (SE=15.16); for boys, these values are, respectively, 23.57 (SE=8.07) and 22.78 (SE=5.14).
Table 3 presents the effects of sex, age, and baseline values in changes of SPPF measured by Δ%. Results indicated that an increase of one point in QAPA in baseline represents a significant decreasing about − 2.52% of QAPA-SPPF at the follow-up period. Age and sex showed no significant effects on QAPA-SPPF Δ%.
Table 3.
Effects of sex, age, and baseline values in SPPF changes (Δ%) considering the GEE model
| Δ% SPPF (dependent) | 95% CI | GEE test | ||||
|---|---|---|---|---|---|---|
| Independent factors | β | SE | Lower | Upper | Wald (× 2) | p value |
| (Intercept) | 74.629 | 21.514 | 32.462 | 116.796 | 12.03 | 0.001 |
| Categorical | ||||||
| Girls | − 2.072 | 4.503 | − 10.898 | 6.754 | 0.21 | 0.645 |
| Boys (ref) | ||||||
| Continuous | ||||||
| Age (years) | − 1.238 | 1.085 | − 3.366 | 0.890 | 1.31 | 0.254 |
| QAPA baseline values (points) | − 2.522 | 0.738 | − 3.97 | − 1.074 | 11.65 | 0.001 |
SPPF self-perceived physical fitness, SE standard error, 95% CI confidence interval, GEE general estimative equations, QAPA self-perceived physical fitness questionnaire. Bold values are statistically significant for p < 0.05
Figure 2 presents the individual variation (Δ) of each child from baseline to follow-up evaluation in crude scores of SPPF in QAPA. Results indicated that 26.4% (nine boys) and 21.2% (seven girls) presented an increase in SPPF. In addition, most children presented no pedagogical/clinical changes (19 girls and 21 boys did not present consistent changes in SPPF Δ). Therefore, 24.2% (8) of girls decreased SPPF, and only three boys (8.8%) showed this negative effect.
Fig. 2.

Individual changes in SPPF (Δ points) from baseline to follow-up period, considering more than two points (10%) as a cut-point (–) to a pedagogical and clinically relevant effect [29, 39, 40]
Discussion
The main results of this study showed that 26.4% of boys and 21.2% of girls improved the SPPF. On the other hand, 54.6% of girls and 64.8% of boys presented no individual changes in SPPF, which considering the pandemic context is a satisfactory result.
The relevance of the present study lays down on the fact that it is one of the first to propose and describe an adaptation of the SPPF assessment to school Physical Education, possible to be applied in remote means in children aged 6–13 years. In addition, we present a new perspective of intervention with Physical Education classes in the remote form, considering changes in health indicators of schoolchildren.
The present research suggests that there are situations and contexts in which the direct evaluation of certain variables is not feasible or possible, and the application of questionnaires becomes a good alternative [41, 42]. In this sense, our study pointed out QAPA as a reliable and consistent questionnaire to assess the SPPF of children from 6 to 13 years old. Corroborating these findings, other studies were developed with this age group showing acceptable values of consistency and reliability in using similar instruments [18, 25, 43].
The findings that pointed out that younger children present higher SPPF compared to older ones are supported by the literature. A study with Swedes [44] between 8 and 12 years old showed the same result, and that greater SPPF was associated with better self-perception in Physical Education classes, reinforcing the importance of strategies for the continuity of the discipline even in the current scenario [44]. It is possible to perceive the psychological maturity factor here [25, 44]. In addition, physical fitness measured objectively increased according to advances in sexual maturation, and it is not directly associated with chronological age [45, 46].
The benefits of the traditional Physical Education classes are well documented in the literature [12, 29, 39, 40, 47, 48]. However, due to social distance in school lockdown, the traditional methodology had to undergo modifications. This new approach also adopted in the present study led to consistent positive changes in the SPPF for about 21.2% in girls and 26.4% in boys. Similar effects have been presented qualitatively or in average effects by other researchers [49, 50], although traditional Physical Education classes provide more facilities for improving physical fitness and social interaction [12, 29, 39, 40, 47, 48]. In another way, the online classes were adequate for some children, mainly when students create autonomy to learn and practice Physical Education at home, maintaining and improving healthy habits [51].
In addition, our study showed that some children had no improvements in SPPF. There was a decrease in this perception, mainly in children who had higher levels in baseline (Table 3). This finding may be explained by the fact that many behaviors that interfere with children’s physical fitness have changed during social distance, such as decreased time in general physical activity, inappropriate sleep time, increased sedentary behavior and intake of unhealthy foods [41, 42, 50–53]. In this context, studies indicate that the best practices in traditional interventions with Physical Education for health [17, 18, 21–25] involve activity in small groups, with direct guidance from the teacher, encouragement to students, formed by classes with well-structured parts and defined by the teacher, which could not happen in the present study due to pandemic circumstances. However, we highlight that considering the social distancing and the remote classes, no changing SPPF must be interpreted as a positive result.
This research has great social and pedagogical relevance as a proposal of intervention and evaluation of changes in the SPPF in distance classes. It can be completed in digital media such as Google Forms, made available in a virtual environment, or even sent in printed form at the student’s home, becoming a diagnostic assessment to tracking children’s SPPF and health variables in distancing situation, a tool applied to Physical Education assessment sets. Besides, online classes are highlighted as an alternative for improving and maintaining physical fitness.
Some limitations must be acknowledged, as the convenient sample of a single school and the impossibility to make inferences to external children. The results presented here should be cautiously interpreted, once some intervenient variables were not considered as body mass index, sexual and biological age maturation. There are possible influences of the subjective bias of QAPA arising from the parents’ opinion about their children and regarding children’s self-perceptions. The QAPA is an alternative measure, but there is no way to replace objective measures of physical fitness.
In conclusion, the present findings showed that a remote Physical Education intervention effectively maintained or even increased individual results of children’s SPPF. Therefore, this study suggests that Physical Education classes in a remote form that promote physical exercises, body movement practices, sports practice, dance, games, and physical activity at home, along with the family’s participation, could be a relevant strategy to increase SPPF in schoolchildren. Indeed, adopting this kind of initiative while last the social distancing and pandemic could benefit children’s health. As the COVID-19 pandemic led to adaptions in Physical Education classes, this study could serve as a model of efficient classes in a remote form.
Supplementary Information
Below is the link to the electronic supplementary material.
Declarations
Conflict of interest
There is no conflict of interest to disclose.
Ethical approval and Informed consent
The present study was approved by Ethics Committee of Estácio de Sá University. All parents, legal guardians, school and participants authorized the study according informed free consent (Number: CEP25315518400005357 - NP3758311).
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Vanilson Batista Lemes, Email: vanilson.lemes@hotmail.com.
Camila Felin Fochesatto, Email: camila-fochesatto@hotmail.com.
Caroline Brand, Email: carolbrand@hotmail.com.
Adroaldo Cezar Araujo Gaya, Email: adroaldogaya@hotmail.com.
Carlos Cristi-Montero, Email: carlos.cristi.montero@gmail.com.
Anelise Reis Gaya, Email: anegaya@gmail.com.
References
- 1.Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–131. [PMC free article] [PubMed] [Google Scholar]
- 2.Ortega FB, Ruiz JR, Castillo MJ, Sjöström M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. 2008;32:1–11. doi: 10.1038/sj.ijo.0803774. [DOI] [PubMed] [Google Scholar]
- 3.Andersen LB, Lauersen JB, Brond JC, et al. A new approach to define and diagnose cardiometabolic disorder in children. J Diabetes Res. 2015;2015:539835. doi: 10.1155/2015/539835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Artero EG, Lee D, Lavie CJ, et al. Effects of muscular strength on cardiovascular risk factors and prognosis. J Cardiopulm Rehabil Prev. 2012;32:351–358. doi: 10.1097/HCR.0b013e3182642688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Earnest CP, Johannsen NM, Swift DL, et al. Aerobic and strength training in concomitant metabolic syndrome and type 2 diabetes. Med Sci Sports Exerc. 2014;46:1293–1301. doi: 10.1249/MSS.0000000000000242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dos Santos FK, Prista A, Gomes TNQF, et al. Body mass index, cardiorespiratory fitness and cardiometabolic risk factors in youth from Portugal and Mozambique. Int J Obes (Lond) 2015;39:1467–1474. doi: 10.1038/ijo.2015.110. [DOI] [PubMed] [Google Scholar]
- 7.Reuter CP, De Moura R, Valim A, Gaya AR, et al. FTO polymorphism, cardiorespiratory fitness, and obesity in Brazilian youth. Am J Hum Biol. 2015 doi: 10.1002/ajhb.2279. [DOI] [PubMed] [Google Scholar]
- 8.Valkenborghs SR, Noetel M, Hillman CH, et al. The impact of physical activity on brain structure and function in youth: a systematic review. Pediatrics. 2019 doi: 10.1542/peds.2018-4032. [DOI] [PubMed] [Google Scholar]
- 9.Kvalø SE, Dyrstad SM, Bru E, Brønnick K. Relationship between aerobic fitness and academic performance: the mediational role of executive function. J Sports Med Phys Fitness. 2019;59:1397–1404. doi: 10.23736/S0022-4707.18.08971-5. [DOI] [PubMed] [Google Scholar]
- 10.Oeland A, Laessoe U, Olesen AV, Munk-Jørgensen P. Impact of exercise on patients with depression and anxiety. Nord J Psychiatry. 2010;64:210–217. doi: 10.3109/08039480903511373. [DOI] [PubMed] [Google Scholar]
- 11.Ortega FB, Cadenas-Sanchez C, Migueles JH, et al. Role of physical activity and fitness in the characterization and prognosis of the metabolically healthy obesity phenotype: a systematic review and meta-analysis. Prog Cardiovasc Dis. 2018 doi: 10.1016/J.PCAD.2018.07.008. [DOI] [PubMed] [Google Scholar]
- 12.Garciá-Hermoso A, Alonso-Martínez AM, Ramírez-Vélez R, et al. Association of physical education with improvement of health-related physical fitness outcomes and fundamental motor skills among youths: a systematic review and meta-analysis. JAMA Pediatr. 2020 doi: 10.1001/jamapediatrics.2020.0223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rundle AG, Park Y, Herbstman JB, et al. COVID-19 related school closings and risk of weight gain among children. Obesity (Silver Spring) 2020 doi: 10.1002/oby.22813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brito LMS, Boguszewski MCS, de Souza MTR MTR, et al. Indoor physical activities, eating and sleeping habits among school adolescents during COVID-19 pandemic. Rev Bras Atividade Física Saúde. 2020;25:1–6. doi: 10.12820/rbafs.25e0117. [DOI] [Google Scholar]
- 15.Lippi G, Henry BM, Sanchis-Gomar F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19) Eur J Prev Cardiol. 2020;2019:1–3. doi: 10.1177/2047487320916823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020 doi: 10.3390/ijerph17051729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lemes VB, Fochesatto CF, Gaya AR. Reliability and consistency of movement behavior questionnaire (MBQ) in children at COVID-19 social distancing. J Mov Heal. 2020;18:1–11. doi: 10.5027/jmh-Vol18-Issue1(2021)art99. [DOI] [Google Scholar]
- 18.Lemes VB, Gaya ACA, Gaya AR. Confiabilidade de um escore de aptidão física autorrelatada em 2020, e associação com a aptidão física de crianças no ano 2019. Ambient Gestão e Desenvolv. 2020;1:10–24. doi: 10.24979/ambiente.v1i1.809. [DOI] [Google Scholar]
- 19.Stavridou A, Kapsali E, Panagouli E, et al. Obesity in children and adolescents during COVID-19 Pandemic. Children. 2021;8:135. doi: 10.3390/children8020135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.An R. Projecting the impact of the coronavirus disease-2019 pandemic on childhood obesity in the United States: a microsimulation model. J Sport Heal Sci. 2020;9:302–312. doi: 10.1016/j.jshs.2020.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vidoni C, Ferraz OL. An analysis of national physical education curriculum initiatives in Brazil. Phys Educ. 2019;76:1342–1356. doi: 10.18666/tpe-2019-v76-i5-9201. [DOI] [Google Scholar]
- 22.Speck RM, Gross CR, Hormes JM, et al. Changes in the Body Image and Relationship Scale following a one-year strength training trial for breast cancer survivors with or at risk for lymphedema. Breast Cancer Res Treat. 2010;121:421–430. doi: 10.1007/s10549-009-0550-7. [DOI] [PubMed] [Google Scholar]
- 23.Seabra AFCFC, Seabra AFCFC, Brito J, et al. Effects of a 5-month football program on perceived psychological status and body composition of overweight boys. Scand J Med Sci Sports. 2014;24:10–16. doi: 10.1111/sms.12268. [DOI] [PubMed] [Google Scholar]
- 24.Hilland TA, Ridgers ND, Stratton G, Fairclough SJ. Associations between selected demographic, biological, school environmental and physical education based correlates, and adolescent physical activity. Pediatr Exerc Sci. 2011;23:61–71. doi: 10.1123/pes.23.1.61. [DOI] [PubMed] [Google Scholar]
- 25.Lemes VB, Araujo Gaya AC, Brand C, et al. Associations among psychological satisfaction in Physical Education, sports practice, and health indicators with physical activity: direct and indirect ways in a structural equation model proposal. Int J Pediatr Adolesc Med. 2020 doi: 10.1016/j.ijpam.2020.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cossio-Bolaños M, Vasquez P, Luarte-Rocha C, et al. Assessment of self-perception of physical fitness and proposal for standards among Chilean adolescent students: the EAPAF study. Arch Argent Pediatr. 2016;114:319–328. doi: 10.5546/aap.2016.eng.319. [DOI] [PubMed] [Google Scholar]
- 27.Silva LCB, Noaves CRMN, da Lima Júnior RA, et al. Sleep, sedentary behavior and physical activity: changes on children’s routine during the COVID-19. Rev Bras Atividade Física Saúde. 2020;25:1–9. doi: 10.12820/rbafs.25e0143. [DOI] [Google Scholar]
- 28.Pietrobelli A, Pecoraro L, Ferruzzi A, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity. 2020 doi: 10.1002/oby.22861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lemes VB, Brand C, Moreira RB, et al. Efeitos da Educação Física nos níveis de aptidão cardiorrespiratória e no índice de massa corporal na Educação de Jovens e Adultos – EJA. Rev Bras Educ Física e Esporte. 2019;33:639–647. doi: 10.11606/1807-5509201900040639. [DOI] [Google Scholar]
- 30.World Medical Association HD World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:1–5. doi: 10.1001/jama.2013.281053. [DOI] [PubMed] [Google Scholar]
- 31.Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. doi: 10.3758/BF03193146. [DOI] [PubMed] [Google Scholar]
- 32.BNCC (2019) Base Nacional Comum Curricular. Ministério da Educ. do Bras
- 33.Santa Catarina (2019) Currículo base da educação infantil e do ensino fundamental do território catarinense. Secr. Estado da Educ. 492
- 34.CEE, Ramos O PARECER CEE/SC No 146. Cons Estadual Educ St Catarina. 2020;146:5–10. [Google Scholar]
- 35.Lemes V. Orientações em Educação Física não presencial para pais e alunos (Período distanciamento social COVID-19) Res Gate. 2020 doi: 10.13140/RG.2.2.14177.94562/2. [DOI] [Google Scholar]
- 36.Sánchez-López M, Martínez-Vizcaíno V, García-Hermoso A, et al. Construct validity and test-retest reliability of the International Fitness Scale (IFIS) in Spanish children aged 9–12 years. Scand J Med Sci Sport. 2015;25:543–551. doi: 10.1111/sms.12267. [DOI] [PubMed] [Google Scholar]
- 37.McDonald RP. The theoretical foundations of principal factor analysis, canonical factor analysis, and alpha factor analysis. Br J Math Stat Psychol. 1970;23:1–21. doi: 10.1111/j.2044-8317.1970.tb00432.x. [DOI] [Google Scholar]
- 38.RochaLemes DRSVB, Moreira R. Efeitos dos jogos pré- desportivos e da recreação sobre níveis de aptidão física de crianças na educação infantil. Rev Ciência e Conhecimento. 2017;11:57–65. [Google Scholar]
- 39.Brand C, Martins CMDL, Lemes VB, et al. Effects and prevalence of responders after a multicomponent intervention on cardiometabolic risk factors in children and adolescents with overweight/obesity: action for health study. J Sports Sci. 2020;38:682–691. doi: 10.1080/02640414.2020.1725384. [DOI] [PubMed] [Google Scholar]
- 40.Lemes VB, Brand C, Dias AF, et al. Jump gymnastic at school physical education for adolescents and adults: changes and prevalence of success in health-related physical fitness. Rev Bras Atividade Física Saúde. 2018;23:1–10. doi: 10.12820/rbafs.23e0054. [DOI] [Google Scholar]
- 41.Ammar A, Brach M, Trabelsi K, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of ECLB-COVID19 International Online Survey. Nutrients. 2020;12(6):1583. doi: 10.3390/nu12061583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hallal PC, Andersen LB, Bull FC, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380:247–257. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- 43.Hidding LM, Altenburg TM, Mokkink LB, et al. Systematic review of childhood sedentary behavior questionnaires: What do we know and What is next? Sport Med. 2017;47:677–699. doi: 10.1007/s40279-016-0610-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sollerhed A-C, Ejlertsson G. Physical benefits of expanded Physical Education in primary school: findings from a 3-year intervention study in Sweden. Scand J Med Sci Sports. 2008;18:102–107. doi: 10.1111/j.1600-0838.2007.00636.x. [DOI] [PubMed] [Google Scholar]
- 45.Lloyd RS, Oliver JL. The youth physical development model: a new approach to long-term athletic development. Strength Cond J. 2012;34:61–72. doi: 10.1519/SSC.0b013e31825760ea. [DOI] [Google Scholar]
- 46.Hills AP, Byrne NM. An overview of physical growth and maturation. Med Sport Sci. 2010 doi: 10.1159/000321968. [DOI] [PubMed] [Google Scholar]
- 47.de Oliveira LCV, Braga FCC, Lemes VB, et al. Effect of an intervention in Physical Education classes on health related levels of physical fitness in youth. Rev Bras Atividade Física Saúde. 2017;22:46–53. doi: 10.12820/rbafs.v.22n1p46-53. [DOI] [Google Scholar]
- 48.Brand C, Lima RA, Silva TF, et al. Effect of a multicomponent intervention in components of metabolic syndrome: a study with overweight/obese low-income school-aged children. Sport Sci Health. 2019 doi: 10.1007/s11332-019-00590-w. [DOI] [Google Scholar]
- 49.Jeong HC, Lee EJ, Youn HS, So WY. Development and implementation of a “music beeps” program to promote physical fitness in adolescents. Int J Environ Res Public Health. 2020;17:1–12. doi: 10.3390/ijerph17176148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Yang Y, Koenigstorfer J. Determinants of physical activity maintenance during the COVID-19 pandemic: a focus on fitness apps. Transl Behav Med. 2020;10:835–842. doi: 10.1093/tbm/ibaa086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Schwendinger F, Pocecco E. Counteracting physical inactivity during the COVID-19 pandemic: evidence-based recommendations for home-based exercise. Int J Environ Res Public Health. 2020;17:2–6. doi: 10.3390/ijerph17113909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.López-Bueno R, López-Sánchez GF, Casajús JA, et al. Potential health- related behaviors for pre-school and school-aged children during COVID-19 lockdown: a narrative review. Prev Med (Baltim) 2021;143:106349. doi: 10.1016/j.ypmed.2020.106349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dunton GF, Do B, Wang SD. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the US. BMC Public Health. 2020;20:1–13. doi: 10.1186/s12889-020-09429-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.