

Abstract
Objective
This study aimed to assess the determinants of accessing healthcare among reproductive-age women in Sub-Saharan Africa (SSA).
Design, setting and analysis
Cross-sectional data were sourced from recent Demographic and Health Surveys in 36 SSA countries. We employed mixed-effect analysis to identify the determinants of accessing healthcare in SSA. OR and its 95% CI were reported for determinants associated with accessing healthcare.
Outcome
The outcome for this study was whether accessing healthcare was a ‘big problem’ or ‘not a big problem’. Responses to these questions were categorised as a big problem and not a big problem.
Participants
A total weighted sample of 500 439 reproductive-age (15–49 years) women from each country’s recent Demographic and Health Surveys from 2006 to 2018 were included in this study.
Results
The pooled prevalence of healthcare access among reproductive-age women in SSA was 42.56% (95% CI 42.43% to 42.69%). The results of the mixed-effect analysis revealed that the determinants of accessing healthcare were urban residence (adjusted OR (AOR)=1.25, 95% CI 1.34 to 1.73), ability to read and write (AOR=1.15, 95% CI 1.22 to 1.28), primary education (AOR=1.08, 95% CI 1.07 to 1.12), secondary education and above (AOR=1.12, 95% CI 1.10 to 1.14), husband with primary education (AOR=1.06, 95% CI 1.07 to 1.1.12), husband with secondary education and above (AOR=1.22, 95% CI 1.18 to 1.27), middle wealth index (AOR=1.43, 95% CI 1.40 to 1.47), rich wealth index (AOR=2.19, 95% CI 2.13 to 2.24) and wanted pregnancy (AOR=1.27, 95% CI 1.19 to 1.29).
Conclusion
Healthcare access in SSA was found at 42.56%, which is very low even if Sustainable Development Goal 3.8 targeted universal health coverage for everyone so they can obtain the health services they need. The major determinants of healthcare access among reproductive-age women in SSA were urban residence, higher educational level, higher wealth index and wanted pregnancy. The findings of this study suggest and recommend strengthening and improving healthcare access for women who reside in the countryside, women with low level of education and women of low socioeconomic status.
Keywords: quality in health care, public health, epidemiology, international health services
Strengths and limitations of this study.
The study included 36 Sub-Saharan African countries and each country’s Demographic and Health Survey data set is representative of the country and is generalisable.
The study used mixed-effect analysis which considers clustering effect in order to provide reliable estimates.
Incorporating a large sample size with adequate power allows detection of the true effect of independent variables.
This study has its own limitation, that is, the findings do not establish a cause and effect relationship due to the cross-sectional nature of the data/surveys.
Introduction
Globally, 50% of people are unable to access basic health services, as reported by the World Bank and the WHO in 2017.1 In Africa, 11 million people are in poverty as a result of using their household income to access essential healthcare services.2 There is wide discrepancy in accessibility and availability of essentials in Sub-Saharan Africa (SSA) and in Southern Asia.3
Healthcare access indicates the affordability, accessibility, availability and acceptability of services in order to achieve the best health outcome.4 Access to maternal health services is different among women due to them having less land, wealth and properties despite carrying a higher burden of labour, which has a significant role in the society. Also, in most situations, girls are less fed and educated and physically restricted in certain contexts.5–7
Globally, women suffer from healthcare inequalities, which lead to excess mortality in all periods of life.8 Maternal health service refers to providing health service to women during pregnancy, childbearing and postpartum period, and includes antenatal care visits, delivery care and postnatal care services.9 Although Sustainable Development Goal (SDG) target 3.8 aims to provide universal health coverage, 400 million people in the world lack access to essential health services.10 Previous studies have provided some evidence on the factors associated with healthcare access, including social, demographic and economic determinants such as marital status,11 residence,12 age,13 literacy,14 education,14 wealth index,15 birth order,16 wanted pregnancy17 and women empowerment.18
Different empirical evidence related to healthcare access among reproductive-age women has been explored at the country level. Meanwhile, accessing healthcare is a big challenge. There are limited studies that have incorporated all SSA countries and multicountry Demographic and Health Survey (DHS) data sets. This study attempted to generate new evidence by including data from all countries in SSA from 2006 to 2018.
This study aimed to identify the potential factors associated with healthcare access among the reproductive age group in SSA. The results will help improve coverage of access to healthcare and to design an intervention strategy to address issues of poor maternal health status and outcomes.
Methods
Data source
Data for this study were sourced from the most recent surveys in 36 SSA countries from 2006 to 2018. The DHS programme collects data that are comparable across low-income and middle-income countries. The programme designs the same manual, code, value level, variable name and procedure in more than 90 countries across the world. The SSA countries included in this study are listed in table 1. Details can be found in our previously published work.19–21 The inclusion and exclusion criteria for SSA countries are shown in figure 1. Data were collected from each country’s survey year 5 years preceding the survey. The DHS collects data on HIV/AIDS, nutrition, child health, child nutrition, reproductive health, family planning, marriage, fertility and mortality. Individual record files were used in this study.
Table 1.
Pooled Demographic and Health Survey (DHS) data from 36 Sub-Saharan African countries
| Country | DHS year | Sample size (500 439) |
| Southern region of Africa | 30 140 | |
| Lesotho | 2014 | 6621 |
| Namibia | 2013 | 10 081 |
| Swaziland | 2006/2007 | 4987 |
| South Africa | 2016 | 8514 |
| Central region of Africa | 88 207 | |
| Angola | 2015/2016 | 14 379 |
| Democratic Republic of Congo | 2013/2014 | 18 379 |
| Congo | 2011/2012 | 10 819 |
| Cameroon | 2011 | 15 426 |
| Gabon | 2012 | 8422 |
| Sao Tome and Principe | 2008/2009 | 2615 |
| Chad | 2014/2015 | 17 719 |
| Eastern region of Africa | 193 949 | |
| Burundi | 2010 | 17 269 |
| Ethiopia | 2016 | 15 683 |
| Kenya | 2014 | 31 079 |
| Comoros | 2012 | 5329 |
| Madagascar | 2008/2009 | 17 375 |
| Malawi | 2015/2016 | 24 562 |
| Mozambique | 2011 | 13 745 |
| Rwanda | 2014/2015 | 13 497 |
| Tanzania | 2015/2016 | 13 266 |
| Uganda | 2011 | 18 266 |
| Zambia | 2018 | 13 683 |
| Zimbabwe | 2013/2014 | 9955 |
| Western region of Africa | 188 143 | |
| Burkina Faso | 2010 | 17 087 |
| Benin | 2017 | 15 928 |
| Cote d’Ivoire | 2011 | 10 060 |
| Ghana | 2014 | 9396 |
| Gambia | 2013 | 10 233 |
| Guinea | 2018 | 10 233 |
| Liberia | 2013 | 9239 |
| Mali | 2018 | 10 519 |
| Nigeria | 2018 | 41 821 |
| Niger | 2012 | 11 160 |
| Sierra Leone | 2010/2011 | 16 658 |
| Senegal | 2010/2011 | 15 688 |
| Togo | 2013/2014 | 9480 |
Figure 1.
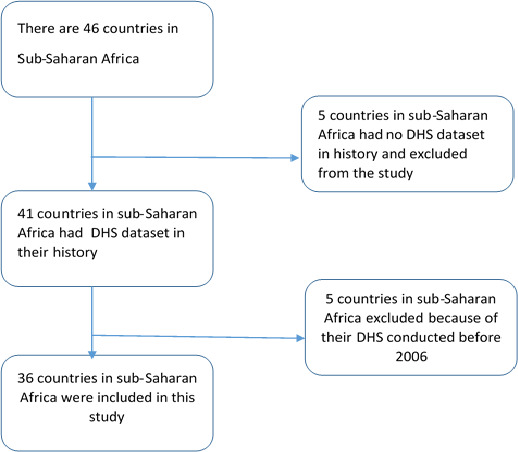
Diagrammatic representation of Sub-Saharan African countries included in the study. DHS, Demographic and Health Survey.
A two-stage stratified sampling method was used to select study participants. First, the enumeration area was selected based on each country frame developed from the previous census conducted. Second, households from each enumeration area were selected. The full sampling procedure is found elsewhere.22 A total of 500 439 reproductive-age women were eligible for this study. Due to the observational nature of the study, the Strengthening the Reporting of Observational Studies in Epidemiology checklist was used and is provided in online supplemental file 1.
bmjopen-2021-054397supp001.pdf (43.1KB, pdf)
Measurement of variables
Outcome variable
The outcome variable was accessibility. Most studies have ignored travel time and transport cost when looking at access to health facilities. In the DHS data, women were asked whether a range of factors would be a big problem for them when accessing healthcare. We generated a composite outcome variable using each country’s DHS standard question. The questions included the following:
Getting the money needed for treatment (big problem/not a big problem).
Distance to a healthcare facility (big problem/not a big problem).
Having to take transport (big problem/not a big problem).
Not wanting to go alone (big problem/not a big problem).
The responses to the questions asked are ‘big problem’ and ‘not a big problem’. If a woman faces at least one problem, access to healthcare is considered a big problem and is coded 1 or 0 otherwise.
Explanatory variables
After reviewing different types of literature,12 13 17 23–25 variables were retrieved from the DHS data set. Variables at the individual, community and regional levels were considered in this study. Individual-level variables include age group, literacy level, women’s educational status, marital status, husband’s educational status, maternal occupation status, media exposure, wealth status, birth order and wanted pregnancy, whereas residence was a community-level variable and region a regional-level variable.
Analytical procedure
In this study, both descriptive and inferential analyses were done. The survey year and the number of reproductive-age women in each country are presented in the tables. The weighted number of reproductive-age women and the weighted percentage of women for each sociodemographic variable are presented in table 2. Model comparison is presented in table 3. The results of the multivariable generalised mixed-effect model are presented to see the effect size of the association between the outcome and the independent variables.
Table 2.
Socioeconomic and demographic characteristics of reproductive-age women in Sub-Saharan Africa
| Variable | Category | Weighted frequency | % |
| Region | Southern Africa | 30 140 | 6.02 |
| Central Africa | 88 207 | 17.63 | |
| Eastern Africa | 193 949 | 38.76 | |
| Western Africa | 188 143 | 37.60 | |
| Residence | Rural | 313 428 | 62.63 |
| Urban | 187 011 | 37.37 | |
| Age group | 15–24 | 198 907 | 39.75 |
| 25–34 | 157 282 | 31.43 | |
| 35–49 | 144 250 | 28.82 | |
| Marital status | Single | 136 519 | 27.28 |
| Married | 363 920 | 72.72 | |
| Literacy level | Cannot read and write | 212 244 | 42.41 |
| Can read and write | 288 195 | 57.59 | |
| Maternal education | No education | 158 532 | 31.68 |
| Primary education | 163 734 | 32.72 | |
| Secondary education and above | 178 173 | 35.60 | |
| Husband’s education (n=332 753) | No education | 124 184 | 37.32 |
| Primary education | 90 831 | 27.30 | |
| Secondary education and above | 117 738 | 35.38 | |
| Maternal occupation | No | 155 707 | 31.11 |
| Yes | 344 732 | 68.89 | |
| Wealth index | Poor | 195 653 | 39.10 |
| Middle | 95 039 | 18.99 | |
| Rich | 209 747 | 41.91 | |
| Media exposed | Yes | 350 348 | 70.02 |
| No | 150 023 | 29.98 | |
| Birth order (n=492 403) | 1 | 70 740 | 14.37 |
| 2–4 | 170 095 | 34.54 | |
| 5+ | 251 568 | 51.09 | |
| Wanted pregnancy (n=255 685) | No | 17 434 | 6.82 |
| Yes | 238 251 | 93.18 |
Table 3.
Model comparison and random-effect results for the final model
| Parameter | Standard logistic regression | Mixed-effect logistic regression analysis (GLMM) |
| LLR | −144 966 | −144 223 |
| Deviance | 289 932 | 288 466 |
| ICC | 12.09 (11.17, 13.08) | |
| LR test | LR test vs logistic model: chibar2(01)=1486.67 Prob>=chibar2=<0.001 | |
| MOR | 1.44 (1.40, 1.49) | |
| Cluster variance | 0.1526 (0.1289, 0.1806) |
GLMM, generalised linear mixed effect model; ICC, intraclass correlation coefficient; LLR, log-likelihood ratio; LR test, likelihood ratio test; MOR, median OR.
STATA V.14 software was used for analysis. First, each country was given a code and then appended together to create a single data set that represents the SSA countries. There are individual-level and community-level variables in the data set. The nature of the DHS data set is hierarchical and needs advanced statistical techniques to account for variability. The generalised linear mixed-effect model was fitted. Both fixed and random estimates were reported. For fixed-effect estimates, adjusted OR (AOR) and its 95% CI were reported to see the effect size of the association between healthcare access problem and the independent variables (table 4). For random-effect estimates, intraclass correlation and median OR were reported (table 3). First, in the bivariable analysis, variables with a p value less than 0.2 were taken as a candidate variable for the final model. Variables in the final model with a p value less than 0.005 were declared as determinants significantly associated with accessing healthcare in SSA.
Table 4.
Multivariable mixed-effect logistic regression analysis of determinants of healthcare access in Sub-Saharan Africa
| Variable | Category | Accessing healthcare | COR (95% CI) | AOR (95% CI) | |
| Not a big problem | Big problem | ||||
| Region | Southern Africa | 14 875 | 15 265 | 1 | 1 |
| Central Africa | 34 844 | 53 365 | 0.66 (0.64 to 0.68) | 0.75 (0.71 to 0.80)* | |
| Eastern Africa | 91 888 | 102 061 | 0.84 (0.82 to 0.87) | 0.77 (0.73 to 0.81)* | |
| Western Africa | 75 409 | 112 734 | 0.64 (0.63 to 0.66) | 0.69 (0.65 to 0.73)* | |
| Residence | Rural | 117 457 | 195 971 | 1 | 1 |
| Urban | 99 559 | 87 452 | 1.93 (1.90 to 1.95) | 1.25 (1.22 to 1.28)* | |
| Age group | 15–24 | 88 177 | 110 730 | 1 | |
| 25–34 | 69 064 | 88 218 | 0.97 (0.96 to 0.98) | 1.01 (0.98 to 1.03) | |
| 35–49 | 59 775 | 84 475 | 0.86 (0.86 to 0.89) | 0.98 (0.95 to 1.02) | |
| Literacy level | Cannot read and write | 75 149 | 136 850 | 1 | 1 |
| Can read and write | 146 421 | 141 774 | 1.68 (1.66 to 1.70) | 1.15 (1.08 to 1.18)* | |
| Maternal education | No education | 55 647 | 102 858 | 1 | |
| Primary education | 67 016 | 96 858 | 1.22 (1.20 to 1.24) | 1.080 (1.07 to 1.10)* | |
| Secondary education and above | 94 326 | 83 847 | 1.96 (1.94 to 1.99) | 1.12 (1.10 to 1.14)* | |
| Husband’s education (n=332 753) | No education | 43 689 | 80 495 | 1 | 1 |
| Primary education | 33 628 | 57 203 | 1.06 (1.04 to 1.08) | 1.06 (1.04 to 1.08)* | |
| Secondary education and above | 58 147 | 59 591 | 1.76 (1.73 to 1.79) | 1.22 (1.18 to 1.27)* | |
| Maternal occupation | No | 66 261 | 89 446 | 1 | 1 |
| Yes | 150 755 | 193 977 | 0.99 (0.97 to 1.00) | 1.02 (0.99 to 1.03) | |
| Wealth index | Poor | 62 413 | 133 240 | 1 | |
| Middle | 39 054 | 55 985 | 1.46 (1.44 to 1.48) | 1.43 (1.40 to 1.47)* | |
| Rich | 115 549 | 94 198 | 2.60 (2.57 to 2.64) | 2.19 (2.13 to 2.24)* | |
| Media exposed | Yes | 52 457 | 97 566 | 1.59 (1.57 to 1.61) | 1.15 (1.13 to 1.17)* |
| No | 164 537 | 185 811 | 1 | 1 | |
| Birth order (n=492 403) | 1 | 32 718 | 38 023 | 1 | 1 |
| 2–4 | 74 434 | 95 660 | 0.89 (0.88 to 0.91) | 0.98 (0.97 to 1.02) | |
| 5+ | 105 803 | 145 765 | 0.83 (0.82 to 0.85) | 0.96 (0.94 to 1.01) | |
| Wanted pregnancy (n=255 685) | No | 52 457 | 97 566 | 1 | 1 |
| Yes | 164 537 | 185 811 | 1.23 (1.19 to 1.27) | 1.24 (1.19 to 1.29)* | |
*significant at alpha 0.05, **significant at alpha 0.01 and ***significant at alpha 0.001
AOR, adjusted odds ratio; COR, crude odds ratio.
Patient and public involvement
There is no direct public and patient involvement in the design and conduct of this research.
Results
A total of 500 439 reproductive-age women 5 years preceding the survey in SSA countries were included in this study. Of these, 193 949 (38.76%) respondents were from the eastern region of Africa and 30 140 (6.02%) respondents were from the southern region. A total of 313 428 (62.63%) respondents were rural residents. Among the respondents, 158 532 (31.68) women and 124 184 (37.32%) men had no formal education, and 195 653 (39.10%) respondents were of poor wealth status (table 2).
Pooled prevalence of healthcare access in SSA
The pooled prevalence of healthcare access in SSA was 42.56% (95% CI 42.43 to 42.69), with the highest rate of healthcare access in the southern region of Africa at 49% (95% CI 48 to 49) and the lowest rate of healthcare access in the central region at 37% (95% CI 37 to 37). Among the SSA countries, the highest rate of healthcare access was from Kenya at 77% (95% CI 76 to 77) and the lowest rate of healthcare access was from Gabon and Sao Tome at 17% for both countries (95% CI 16 to 18 and 95% CI 15 to 18, respectively; figure 2).
Figure 2.
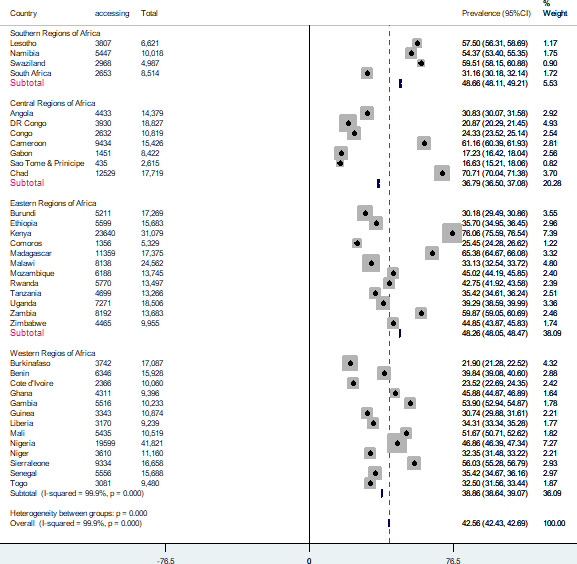
Forest plot of healthcare access among reproductive-age women in Sub-Saharan Africa. DR Congo, Democratic Republic of Congo.
Model comparison
Model comparison was done and a mixed-effect logistic regression model was chosen over ordinary logistic regression model due to low deviance. Furthermore, the intraclass correlation coefficient value was 12.09% (95% CI 11.17 to 13.08) and the median OR was 1.44, indicating that if we randomly select two women from different clusters, women from a cluster with better healthcare access increased by 44% as compared with women with low healthcare access. Besides, the likelihood ratio test was (likelihood ratio test vs logistic model: chibar2 (01)=1486.67 Prob>=chibar2=<0.001), which informed that the mixed-effect logistic regression model (generalised linear mixed effect model (GLMM)) is the better model over the basic logistic regression model (table 3).
Determinants of accessing healthcare
In the multivariable mixed-effect logistic regression model, region, residence, literacy level, maternal and husband educational status, media exposure, wealth status, and wanted pregnancy were statistically associated with accessing healthcare in SSA.
Women living in the central, eastern and western regions of Africa had decreased likelihood of accessing healthcare, at 25%, 23% and 31% (AOR=0.75, 95% CI 0.71 to 0.80; AOR=0.77, 95% CI 0.73 to 0.81; AOR=0.69, 95% CI 0.65 to 0.73), respectively, as compared with women living in the southern region. Women who reside in urban areas are 1.25 times more likely (AOR=1.25, 95% CI 1.22 to 1.28) to access healthcare than women living in rural areas. Women who can read and write are 1.15 times more likely (AOR=1.15, 95% CI 1.08 to 1.18) to access healthcare than women who cannot read and write. Women with primary and secondary and above education are 1.08 and 1.12 times more likely (AOR=1.08, 95% CI 1.07 to 1.12; AOR=1.22, 95% CI 1.10 to 1.14) to access healthcare than women who had no formal education, respectively. Women whose husbands had primary and secondary and above education are 1.06 and 1.22 times more likely (AOR=1.08, 95% CI 1.07 to 1.12; AOR=1.22, 95% CI 1.10 to 1.14) to access healthcare than women whose husband had no formal education. The odds of accessing healthcare among media-exposed women increased by 15% compared with women who were not exposed to mass media (AOR=1.08, 95% CI 1.07 to 1.12). Women below the middle and rich wealth status are 1.43 and 2.19 times more likely (AOR=1.43, 95% CI 1.40 to 1.47; AOR=2.19, 95% CI 2.13 to 2.24) to access healthcare than poor women, respectively. The odds of accessing healthcare among women who wanted pregnancy increased by 24% compared with women who did not want their pregnancy (table 4).
Discussion
This study attempted to assess the determinants of accessing healthcare among reproductive-age women in SSA. This study evidenced that the pooled prevalence of healthcare access in SSA was 42.56%. The determinants associated with accessing healthcare are place of residence, maternal education, husband’s education, wealth index and wanted pregnancy.
The pooled prevalence of healthcare access among reproductive-age women in SSA was 42.56% (95% CI 42.43% to 42.69%), which is consistent with Myanmar,18 South Africa26 and Tanzania.27
This study showed that literacy level is a determinant of healthcare access among reproductive-age women in SSA. Women who can read and write had higher odds of accessing healthcare compared with women who cannot read and write. This finding is consistent with studies conducted in other countries.14 The possible reason might be that women who can read and write can use the information they get from reading for health service utilisation.
This study revealed that women who reside in rural settings are less likely to access healthcare compared with women who reside in urban settings. This finding is consistent with studies done in Saudi Arabia,28 Athens, Greece,29 USA,30 Washington,31 East Africa32 and Ethiopia.17 Accessing healthcare is influenced by different infrastructures, such as roads, distance to a health facility and transport service, as well as access to education, economic limitations and the influence of sociocultural behaviours where women ask permission from their husbands before seeking healthcare.33
The findings also showed that maternal and husband education is a significant determinant of healthcare access among reproductive-age women in SSA. Women and husbands with low-level education are less likely to access healthcare compared with women and husbands with higher-level education. This finding is consistent with studies done in Africa,34 South Africa,35 SSA,26 WHO global health survey,36 and South Asia and SSA.37 The possible reason might be that education is a basis for everything and that educated people have better sources of information and use the health education they get from health institutions. Women and men of higher educational level benefit economically compared with uneducated women and men.23
Wealth index is another determinant of healthcare access among reproductive-age women in SSA. Women of better wealth index status had higher odds of accessing healthcare compared with the poorest women. This finding is consistent with studies done in Namibia, Kenya, Nepal, India,38 Myanmar,18 East Africa,32 Kenya,39 Ethiopia17 and SSA.25 40 The possible reason might be that wealthy women can access healthcare because they can pay for their health services and have increased accessibility to healthcare. Meanwhile, it is a big problem for poor women as they are unable to pay for health services.
This study revealed that the odds of accessing healthcare among women who had wanted pregnancy increased by 24% compared with women who did not want their pregnancy. This finding is consistent with studies done in different countries, such as Tanzania,41 UK42 and Ghana.24 The possible reason might be that women with unwanted pregnancy have a negative attitude towards maternal health service utilisation, such as Antenatal (ANC) visits, delivery and Postnatal (PNC) services.
Living regions in Africa also had a significant effect on healthcare access among reproductive-age women in SSA. Women living in the central, eastern and western regions of Africa had decreased likelihood of accessing healthcare at 25%, 23% and 31%, respectively, compared with women living in the southern region. This is due to the fact that the southern region of Africa had better economic status and health infrastructure compared with other regions.43
Strengths and limitations of this study
The study included 36 SSA countries and each country’s DHS data set is representative of the country and is generalisable. The study used mixed-effect analysis which considers clustering effect in order to provide reliable estimates. Incorporating a large sample size with adequate power allows detection of the true effect of independent variables. This study has its own limitation, that is, the findings do not establish a cause and effect relationship due to the cross-sectional nature of the data/surveys.
Conclusion
Healthcare access in SSA was found at 42.56%, which is very low even if SDG 3.8 targeted universal health coverage for everyone so they can obtain the health services they need. The major determinants of healthcare access among reproductive-age women in SSA were urban residence, higher educational level, higher wealth index and wanted pregnancy. The findings of this study suggest and recommend strengthening and improving healthcare access for women who reside in the countryside, women with low level of education and women of low socioeconomic status.
Supplementary Material
Acknowledgments
We would like to thank the Measure DHS programme for providing the data set.
Footnotes
Contributors: Conceptualisation: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Data curation: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Investigation: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Methodology: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Software: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Validation: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Writing: ZTT, MGW, GAT, TSA, ABT, YY, AZA, HGA and AML. Writing - review: ZTT, YY, AML, GAT, TSA, MGW and ABT. Writing - editing: AZA, ZTT, MGW, GAT, TSA, ABT, YY, HGA and AML. All authors read and approved the manuscript. ZTT is responsible for the overall content as the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request. Data are available online and can be accessed from www.measuredhs.com.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
Permission to get access to the data was obtained from the Measure DHS programme through an online request at https://dhsprogram.com/ and the data used were publicly available with no personal identifier. Data were obtained from the Measure DHS programme through an online request and the data used were publicly available with no personal identifier (The Demographic Health Survey Program. Guide to DHS statistics. Available: https://dhsprogram.com/data/dataset_admin/index.cfm)
References
- 1.WHO WB . Half the world lacks access to essential health services, 100 million still pushed into extreme poverty because of health expenses, 2017. [Google Scholar]
- 2.Global Agenda . How Africa and Asia are joining forces on universal healthcare [Internet]. Available: https://www.weforum.org/agenda/2019/04/universal-health-coverage-uhc-asia-africa-kenya-thailand-japan-egypt/
- 3.WHO . The 13 biggest threats to global health according to WHO, 2020. [Google Scholar]
- 4.Gulliford M, Figueroa-Munoz J, Morgan M, et al. What does 'access to health care' mean? J Health Serv Res Policy 2002;7:186–8. 10.1258/135581902760082517 [DOI] [PubMed] [Google Scholar]
- 5.Pega F, Veale JF. The case for the world Health organization's Commission on social determinants of health to address gender identity. Am J Public Health 2015;105:e58–62. 10.2105/AJPH.2014.302373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sen G, Östlin P. Gender inequity in health: why it exists and how we can change it. Taylor & Francis, 2008. [DOI] [PubMed] [Google Scholar]
- 7.Shannon G, Jansen M, Williams K, et al. Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet 2019;393:560–9. 10.1016/S0140-6736(18)33135-0 [DOI] [PubMed] [Google Scholar]
- 8.Myatra SN, Tripathy S, Einav S. Global health inequality and women - beyond maternal health. Anaesthesia 2021;76 Suppl 4:6–9. 10.1111/anae.15431 [DOI] [PubMed] [Google Scholar]
- 9.WHO . Maternal health, 2016. Available: http://www.who.int/maternal_child_adolescent/topics/maternal/en/
- 10.WHO . How many people lack access to health care? (hint: more than who and the world bank report), 2019. Available: https://oneill.law.georgetown.edu/how-many-people-lack-access-to-health-care-hint-more-than-who-and-the-world-bank-report/
- 11.Pandey KR, Yang F, Cagney KA, et al. The impact of marital status on health care utilization among Medicare beneficiaries. Medicine 2019;98:e14871. 10.1097/MD.0000000000014871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yang Y-T, Iqbal U, Ko H-L, et al. The relationship between accessibility of healthcare facilities and medical care utilization among the middle-aged and elderly population in Taiwan. Int J Qual Heal Care 2015;27:222–31. 10.1093/intqhc/mzv024 [DOI] [PubMed] [Google Scholar]
- 13.National Academies of Sciences, Engineering and M . Health-Care utilization as a proxy in disability determination. health-care utilization as a proxy in disability determination, 2018. [PubMed] [Google Scholar]
- 14.Cho . HHS public access. Physiol Behav 2016;176:100–6. [Google Scholar]
- 15.Minyihun A, Tessema ZT. Determinants of access to health care among women in East African countries: a multilevel analysis of recent demographic and health surveys from 2008 to 2017. Risk Manag Healthc Policy 2020;13:1803–13. 10.2147/RMHP.S263132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pruckner GJ, Schneeweis N, Schober T, et al. Birth order, parental health investment, and health in childhood. SSRN J 2019. 10.2139/ssrn.3488201 [DOI] [PubMed] [Google Scholar]
- 17.Tamirat KS, Tessema ZT, Kebede FB. Factors associated with the perceived barriers of health care access among reproductive-age women in Ethiopia: a secondary data analysis of 2016 Ethiopian demographic and health survey. BMC Health Serv Res 2020;20:1–8. 10.1186/s12913-020-05485-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Htun NMM, Hnin ZL, Khaing W. Empowerment and health care access barriers among currently married women in Myanmar. BMC Public Health 2021;21:1–9. 10.1186/s12889-021-10181-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tessema ZT, Teshale AB, Tesema GA, et al. Determinants of completing recommended antenatal care utilization in sub-Saharan from 2006 to 2018: evidence from 36 countries using demographic and health surveys. BMC Pregnancy Childbirth 2021;21:1–12. 10.1186/s12884-021-03669-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tessema ZT, Yazachew L, Tesema GA, et al. Determinants of postnatal care utilization in sub-Saharan Africa: a meta and multilevel analysis of data from 36 sub-Saharan countries. Ital J Pediatr 2020;46:1–11. 10.1186/s13052-020-00944-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tessema ZT, Tamirat KS, Teshale AB, et al. Prevalence of low birth weight and its associated factor at birth in sub-Saharan Africa: a generalized linear mixed model. PLoS One 2021;16:1–13. 10.1371/journal.pone.0248417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Demographic T, Program HS . Guide to DHS statistics. Available: https://dhsprogram.com/data/dataset_admin/index.cfm
- 23.Becker G, Newsom E. Socioeconomic status and dissatisfaction with health care among chronically ill African Americans. Am J Public Health 2003;93:742–8. 10.2105/AJPH.93.5.742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sakeah E, Okawa S, Rexford Oduro A, et al. Determinants of attending antenatal care at least four times in rural Ghana: analysis of a cross-sectional survey. Glob Health Action 2017;10:1291879. 10.1080/16549716.2017.1291879 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pons-Duran C, Lucas A, Narayan A, et al. Inequalities in sub-Saharan African women's and girls' health opportunities and outcomes: evidence from the demographic and health surveys. J Glob Health 2019;9:010410. 10.7189/jogh.09.010410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Seidu A-A. Mixed effects analysis of factors associated with barriers to accessing healthcare among women in sub-Saharan Africa: insights from demographic and health surveys. PLoS One 2020;15:1–16. 10.1371/journal.pone.0241409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nisingizwe MP, Tuyisenge G, Hategeka C, et al. Are perceived barriers to accessing health care associated with inadequate antenatal care visits among women of reproductive age in Rwanda? BMC Pregnancy Childbirth 2020;20:88. 10.1186/s12884-020-2775-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Almalki M, FitzGerald G, Clark M. The nursing profession in Saudi Arabia: an overview. Int Nurs Rev 2011;58:304–11. 10.1111/j.1466-7657.2011.00890.x [DOI] [PubMed] [Google Scholar]
- 29.Pappa E, Niakas D. Assessment of health care needs and utilization in a mixed public-private system: the case of the Athens area. BMC Health Serv Res 2006;6:1–11. 10.1186/1472-6963-6-146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bhatt J, Bathija P. Ensuring access to quality health care in vulnerable communities. Acad Med 2018;93:1271–5. 10.1097/ACM.0000000000002254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.National Academies of Sciences E, Medicine . Health-care utilization as a proxy in disability determination, 2018. [PubMed] [Google Scholar]
- 32.Tessema ZT, Minyihun A. Utilization and determinants of antenatal care visits in East African countries: a multicountry analysis of demographic and health surveys. Adv Public Heal 2021;2021:1–9. 10.1155/2021/6623009 [DOI] [Google Scholar]
- 33.Munguambe K, Boene H, Vidler M, et al. Barriers and facilitators to health care seeking behaviours in pregnancy in rural communities of southern Mozambique. Reprod Health 2016;13:83–97. 10.1186/s12978-016-0141-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tsala Dimbuene Z, Amo-Adjei J, Amugsi D, et al. Women's education and utilization of maternal health services in Africa: a multi-COUNTRY and socioeconomic status analysis. J Biosoc Sci 2018;50:725–48. 10.1017/S0021932017000505 [DOI] [PubMed] [Google Scholar]
- 35.Tsawe M, Susuman AS. Determinants of access to and use of maternal health care services in the Eastern Cape, South Africa: a quantitative and qualitative investigation. BMC Res Notes 2014;7:1–10. 10.1186/1756-0500-7-723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Karlsen S, Say L, Souza J-P, et al. The relationship between maternal education and mortality among women giving birth in health care institutions: analysis of the cross sectional WHO global survey on maternal and perinatal health. BMC Public Health 2011;11:1–10. 10.1186/1471-2458-11-606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Tey N-P, Lai S-li. Correlates of and barriers to the utilization of health services for delivery in South Asia and sub-Saharan Africa. Scientific World J 2013;2013:1–11. 10.1155/2013/423403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Namasivayam A, Osuorah DC, Syed R, et al. The role of gender inequities in women's access to reproductive health care: a population-level study of Namibia, Kenya, Nepal, and India. Int J Womens Health 2012;4:351–64. 10.2147/IJWH.S32569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Otieno PO, Wambiya EOA, Mohamed SM, et al. Access to primary healthcare services and associated factors in urban slums in Nairobi-Kenya. BMC Public Health 2020;20:1–9. 10.1186/s12889-020-09106-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Annan J, Donald A, Goldstein M, et al. Taking power: women’s empowerment and household well-being in Sub-Saharan Africa. World Dev 2021;140:105292. 10.1016/j.worlddev.2020.105292 [DOI] [Google Scholar]
- 41.Gupta S, Yamada G, Mpembeni R, et al. Factors associated with four or more antenatal care visits and its decline among pregnant women in Tanzania between 1999 and 2010. PLoS One 2014;9:e101893. 10.1371/journal.pone.0101893 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Haddrill R, Jones GL, Mitchell CA, et al. Understanding delayed access to antenatal care: a qualitative interview study. BMC Pregnancy Childbirth 2014;14:1–14. 10.1186/1471-2393-14-207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cigna . A guide to healthcare in South Africa, 2019. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-054397supp001.pdf (43.1KB, pdf)
Data Availability Statement
Data are available upon reasonable request. Data are available online and can be accessed from www.measuredhs.com.