

Abstract
Educational attainment is widely accepted as a cognitive reserve variable. However, few studies have demonstrated that education statistically moderates the effects of pathology on cognition. Here, we explored this issue in a sample of 441 Alzheimer’s disease (AD) and mild cognitive impairment (MCI) participants from the Alzheimer’s Disease Neuroimaging Initiative (ADNI2) cohort who had AD markers (Aβ42, tau, structural brain volumes) at baseline and underwent cognitive testing at baseline and at 6-month, 12-month, and 24-month timepoints. An AD-related atrophy/pathology composite at baseline was developed using stepwise backward linear regression. Potential moderation effects of education on the relationship between pathology and memory and executive function were explored using linear mixed models. Education was positively correlated with cognition, and pathology was negatively correlated with cognition, across domains and diagnostic groups. However, education generally did not moderate the effects of pathology on baseline or longitudinal cognition. Our results do not support the hypothesis that education protects cognitive function from brain pathology in the ADNI 2 cohort, questioning its accepted status as a reserve variable.
Keywords: Education, Cognitive Reserve, Alzheimer’s Disease, Cognition, Biomarkers
1. Introduction
Educational attainment and its correlates have positive effects on cognitive performance across the lifespan (Brewster et al., 2014; Salthouse, 1991a, 1991b). Such findings have raised the possibility that education may promote cognitive reserve (CR)(Stern, 2002). A number of studies have provided apparent support for education as a CR variable, reporting more severe AD pathology in those with higher versus lower education (Garibotto et al., 2008; Kemppainen et al., 2008). However, new consensus guidelines concerning CR research (Stern et al., 2018) suggest that conclusions concerning CR variables should be based on statistical moderation between pathology and clinical/cognitive status variables. That is, cognitive performance should be predicted by the interaction between a purported CR variable and brain status.
Only a few studies with large sample sizes have reported such statistical moderation (Bennett et al., 2005, 2003; Stern et al., 1995, 1992). Further, these findings are counterbalanced by several null results (Koepsell et al., 2008; Roe et al., 2007; Stern et al., 1999). Potential discrepancies between previous results could include the clinical status of participants, the cognitive domain tested and the use of cross-sectional versus longitudinal designs. Here, we comprehensively explored these possibilities by examining if education moderates the effects of pathology on either baseline or longitudinal memory and/or executive function in MCI and/or AD clinical groups.
2. Materials and Methods
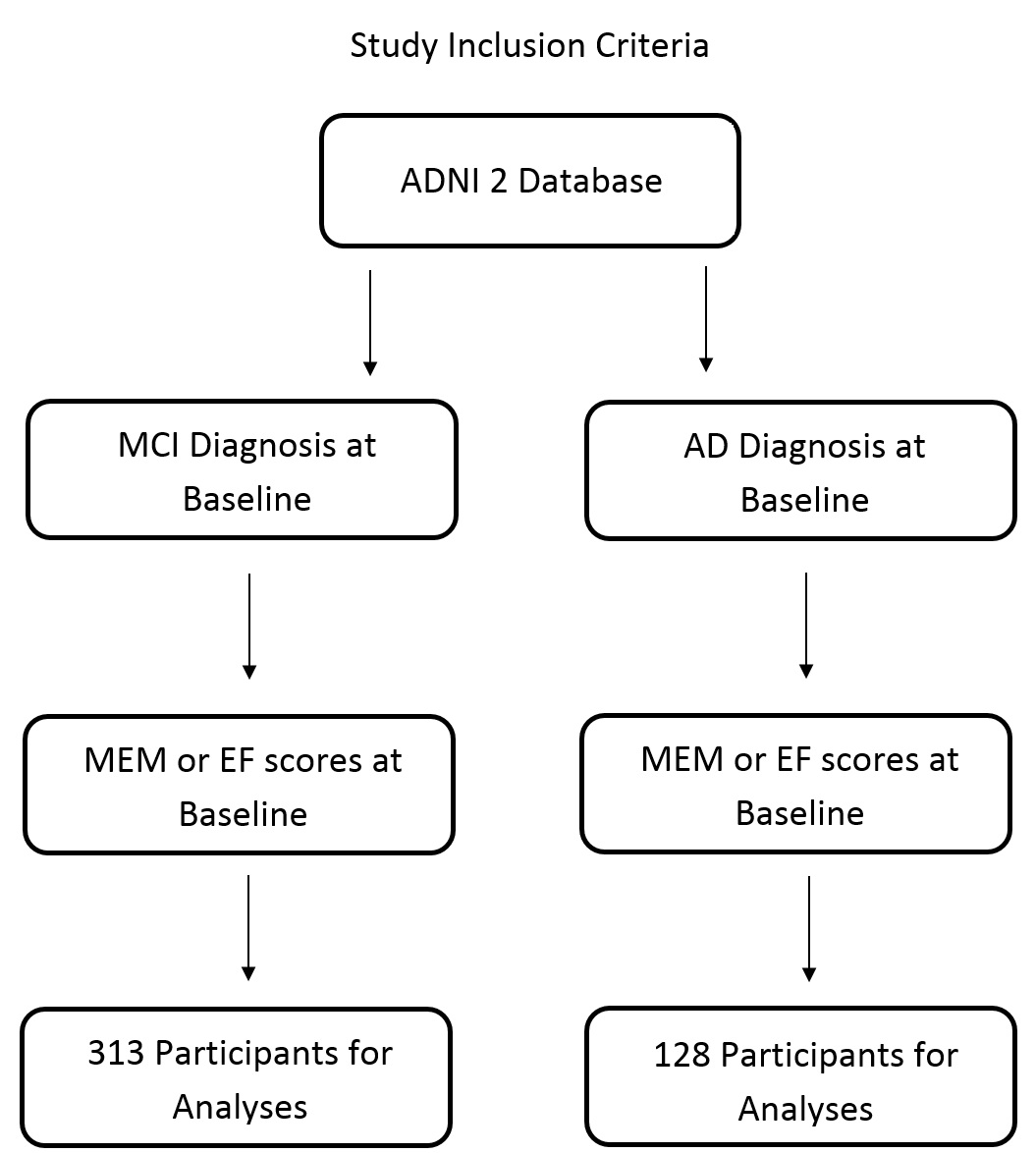
We accessed data from 441 participants with MCI or AD from Alzheimer’s Disease Neuroimaging Initiative 2 (ADNI2) that had summary measures of MRI regional volumes, CSF AD pathology (n=426), composite scores of memory (Crane et al., 2012) and EF (Gibbons et al., 2012), and basic demographic information (Table 1) at baseline (Figure S1). Composite measures of baseline atrophy/pathology were derived empirically based on their association with scores per cognitive domain. Baseline composite measures of atrophy/pathology here included both structural volumes and concentration ratio of tau/Aβ42 in the CSF (Bakkour et al., 2009; Fagan et al., 2007; Shaw et al., 2009). Individual structures were ICV-normalized, and both structural volumes and tau/Aβ42 ratio were z-scored relative to the group mean before they were entered into the composites. Backward elimination was used to remove the least significant predictor one at a time until only z-scored predictors with p < 0.05 were remaining which were averaged to form the cognitive domain specific composites.
Table 1.
Participant Demographics at Baseline
| Characteristic | Total (N=441) | MCI (N=313) | AD (N=128) | p-value |
|---|---|---|---|---|
| Age (Years) | 72.5 (7.7) | 71.7 (7.3) | 74.4 (8.4) | 0.001 |
| Female (n, %) | 191 (43.3) | 140 (44.7) | 51 (39.8) | 0.347 |
| Education (Years) | 16.2 (2.6) | 16.4 (2.6) | 15.8 (2.6) | 0.021 |
| Tau/Aβ42 ratio* | 0.73 (0.55) | 0.60 (0.47) | 1.05 (0.60) | <0.001 |
| MEM Cognitive Composite | −0.073 (0.82) | 0.25 (0.70) | −0.88 (0.49) | <0.001 |
| EF Cognitive Composite | −0.028 (1.07) | 0.32 (0.92) | −0.87 (0.96) | <0.001 |
| MEM Pathology Composite | 0 (0.34) | −0.12(0.30) | 0.27(0.27) | <0.001 |
| EF Pathology Composite | 0 (0.45) | −0.14(0.40) | 0.34(0.36) | <0.001 |
Demographic, pathology, and performance information is displayed for all participants. Reported values are mean with standard deviation, beside gender. Those with AD were significantly older, had greater AD pathology burden, were less educated, and performed worse on neurocognitive testing than those with MCI.
A total of 15 participants were missing data on this component of the pathology composite.
Using SPSS, linear mixed models were then used to determine if baseline pathology and education predict cognitive scores at baseline and longitudinally for both MCI and AD groups at p<0.05, with MEM or EF scores as the dependent variables. Models included all possible interactions excluding age and gender (pathology × time, education × time, pathology × education, and pathology × education × time).
3. Results
There was a main effect of education on both cognitive domains in the AD and MCI groups (Tables 2, 3). There were no significant education x time interactions in either cognitive domain, for either group (Tables 2, 3).
Table 2:
AD
| Memory | EF | |||||
|---|---|---|---|---|---|---|
| Category | Beta | F-value | p-value | Beta | F-value | p-value |
| Age | −0.001 | 0.019 | 0.889 | 0.003 | 0.116 | 0.734 |
| Gender | −0.155 | 3.465 | 0.065 | −0.159 | 1.180 | 0.280 |
| Education | 0.063 | 5.006 | 0.027 | 0.154 | 6.586 | 0.012 |
| Pathology Composite | −0.837 | 39.523 | <0.001 | −1.216 | 41.90 | <0.001 |
| Time | −0.446 | 34.772 | <0.001 | −0.780 | 19.87 | <0.001 |
| Path Composite × Time | −0.034 | 5.257 | 0.003 | 0.191 | 2.135 | 0.103 |
| Education × Path | −0.140 | 1.712 | 0.193 | −0.198 | 0.490 | 0.486 |
| Education × Time | 0.141 | 2.374 | 0.078 | 0.174 | 1.419 | 0.245 |
| Education x Path x Time | −0.313 | 1.118 | 0.348 | −0.003 | 0.916 | 0.438 |
Unstandardized beta, F and p values are reported for linear mixed models for both MEM and EF in those with AD. There were no education x pathology interactions either at baseline or longitudinally through 2 years.
Table 3:
MCI
| Memory | EF | |||||
|---|---|---|---|---|---|---|
| Category | Beta | F-value | p-value | Beta | F-value | p-value |
| Age | −0.008 | 3.222 | 0.074 | −0.027 | 15.372 | <0.001 |
| Gender | −0.215 | 12.227 | 0.001 | −0.104 | 1.341 | 0.248 |
| Education | 0.076 | 4.805 | 0.029 | 0.132 | 4.757 | 0.030 |
| Pathology Composite | −1.244 | 156.122 | <0.001 | −0.789 | 58.864 | <0.001 |
| Time | −0.107 | 18.210 | <0.001 | −0.072 | 1.918 | 0.127 |
| Path Composite × Time | −0.538 | 13.794 | <0.001 | −0.357 | 5.692 | 0.001 |
| Education × Path | 0.053 | 0.070 | 0.792 | −0.151 | 3.753 | 0.054 |
| Education × Time | 0.006 | 0.158 | 0.924 | −0.076 | 1.376 | 0.250 |
| Education x Path x Time | −0.122 | 1.236 | 0.297 | −0.176 | 0.960 | 0.412 |
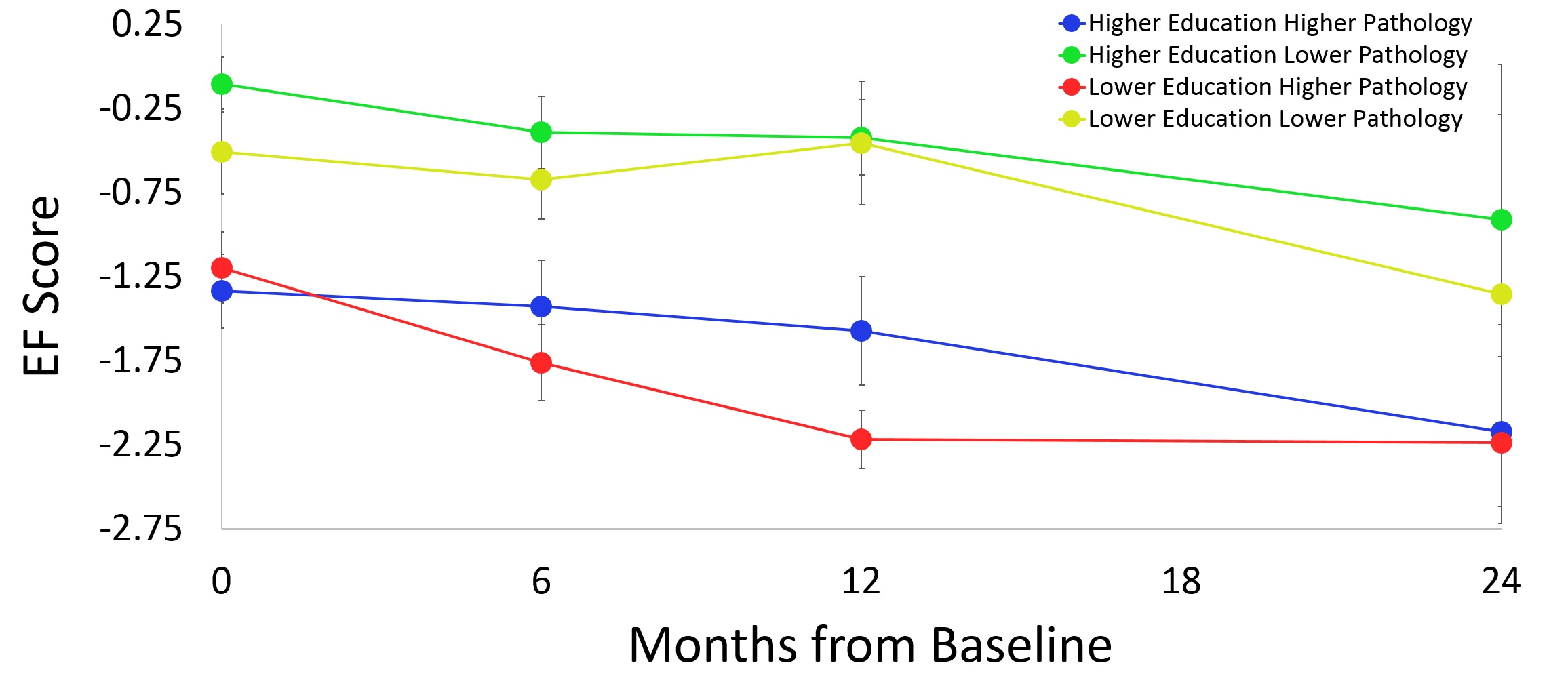
Unstandardized beta, F and p values are reported for linear mixed models for both MEM and EF in those with MCI. There were no education x pathology x time interactions through 2 years, although there was a trend for an education x pathology interaction at baseline for EF. However, in this interaction EF scores were not as negatively affected by pathology in lower education than those with higher education, which the opposite direction expected using cognitive reserve theory.
The specific pathology variables predictive of each cognitive composite variable are listed in Table S1. The MEM and EF pathology composite measures were highly significant predictors of their respective baseline cognitive domain scores as listed in Tables 2, 3 (all p values ≤ 0.001).
There were no significant education x pathology or education x pathology x time interactions in either cognitive domain for either diagnostic group (Tables 2, 3). Further investigation using an age median split yielded the same conclusion for memory (Tables S2, S3) with a mixed conclusion for EF (Tables S2, S3; Figure S2).
4. Discussion
Our results indicate that higher educational attainment was associated with better cognitive functioning in MCI and AD, in both MEM and EF domains. However, education generally did not moderate the effects of atrophy/pathology, time or their interaction on cognitive function. Only in a subgroup of younger AD participants was a moderating effect of education observed and this effect was selective to EF. These results are consistent with other studies with large samples (Koepsell et al., 2008; Roe et al., 2007; Vemuri et al., 2011). Overall, our results are consistent with a view that education is an insufficient proxy for cognitive reserve. However, the selective CR effect we observed in a younger AD subgroup leaves open the possibility that education may protect EF against significant pathology prior to additional brain declines associated with advanced aging (See Supplementary Material for the complete version of this manuscript).
Supplementary Material
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
Funding
This work was supported by the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012) and the National Institutes of Health (R01 AG055449).
Abbreviations:
- ADNI
Alzheimer’s Disease Neuroimaging Initiative
- AD
Alzheimer’s Disease
- MCI
Mild Cognitive Impairment
- CR
Cognitive Reserve
- MRI
Magnetic Resonance Imaging
- MEM
Memory
- EF
Executive Function
- CSF
Cerebrospinal Fluid
- Aβ42
Amyloid-Beta 42
- ICV
Intracranial Volume
- LMM
Linear Mixed Models
Footnotes
Disclosures:
Dr. Christopher Bauer reports no disclosures.
Dr. Christopher Brown reports no disclosures.
Dr. Brian Gold reports no disclosures.
References
- Bakkour A, Morris JC, Dickerson BC, 2009. The cortical signature of prodromal AD; Regional thinning predicts mild AD dementia. Neurology 72, 1048–1055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett DA, Schneider JA, Wilson RS, Bienias JL, Arnold SE, 2005. Education modifies the association of amyloid but not tangles wiht cognitive function. Neurology 65, 953–955. 10.1016/0006-3207(73)90069-4 [DOI] [PubMed] [Google Scholar]
- Bennett DA, Wilson RS, Schneider JA, Evans DA, Mendes de Leon CF, Arnold SE, Barnes LL, Bienias JL, 2003. Education modifies the relation of AD pathology to level of cognitive function in older persons. Neurology 60, 1909–1915. 10.1212/01.WNL.0000069923.64550.9F [DOI] [PubMed] [Google Scholar]
- Brewster P, Melrose R, Marquine M, Johnson J, Napoles A, MacKay-Brandt A, Farias S, Reed B, Mungas D, 2014. Life Experience and Demographic Influences on Cognitive Function in Older Adults. Neuropsychology 28, 846–858. 10.1037/neu0000098.Life [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crane PK, Carle A, Gibbons LE, Insel P, Mackin RS, Gross A, Jones RN, Mukherjee S, Curtis SMK, Harvey D, Weiner M, Mungas D, 2012. Development and assessment of a composite score for memory in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Brain Imaging Behav. 6, 502–516. 10.1007/s11682-012-9186-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagan AM, Roe CM, Xiong C, Mintun MA, Morris JC, Holtzman DM, 2007. Cerebrospinal Fluid tau/B-Amyloid 42 Ratio as a Prediction of Cognitive Decline in Nondemented Older Adults. Arch. Neurol 64, 343–349. [DOI] [PubMed] [Google Scholar]
- Garibotto V, Borroni B, Kalbe E, Herholz K, Salmon E, Holtoff V, Sorbi S, Cappa SF, Padovani A, Fazio F, Perani D, 2008. Education and occupation as proxies for reserve in aMCI converters and AD. Neurology 71, 1342–1349. [DOI] [PubMed] [Google Scholar]
- Gibbons LE, Carle AC, Mackin RS, Harvey D, Mukherjee S, Insel P, Curtis SMK, Mungas D, Crane PK, 2012. A composite score for executive functioning, validated in Alzheimer’s Disease Neuroimaging Initiative (ADNI) participants with baseline mild cognitive impairment. Brain Imaging Behav. 6, 517–527. 10.1007/s11682-012-9176-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kemppainen NM, Aalto S, Karrasch M, Någren K, Savisto N, Oikonen V, Viitanen M, Parkkola R, Rinne JO, 2008. Cognitive reserve hypothesis: Pittsburgh compound B and fluorodeoxyglucose positron emission tomography in relation to education in mild Alzheimer’s disease. Ann. Neurol. 63, 112–118. 10.1002/ana.21212 [DOI] [PubMed] [Google Scholar]
- Koepsell TD, Kurland BF, Harel O, Johnson EA, Zhou XH, Kukull WA, 2008. Education, cognitive function, and severity of neuropathology in Alzheimer disease. Neurology 70, 1732–1739. [DOI] [PubMed] [Google Scholar]
- Roe CM, Xiong C, Miller JP, Morris JC, 2007. Education and Alzheimer disease without dementia; Support for the cognitive reserve hypothesis. Neurology 68, 223–228. [DOI] [PubMed] [Google Scholar]
- Salthouse TA, 1991a. Cognitive facets of aging well. Gener. J. Am. Soc. Aging 35, 35–38. [Google Scholar]
- Salthouse TA, 1991b. Mediation of Adult Age Differences in Cognition by Reductions in Working Memory and Speed of Processing. Psychol. Sci 2, 179–183. [Google Scholar]
- Shaw LM, Vanderstichele H, Knapik-Czajka M, Clark CM, Aisen PS, Petersen RC, Blennow K, Soares H, Simon A, Lewczuk P, Dean R, Siemers E, Potter W, Lee VMY, Trojanowski JQ, 2009. Cerebrospinal fluid biomarker signature in Alzheimer’s disease neuroimaging initiative subjects. Ann. Neurol 65, 403–413. 10.1002/ana.21610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern Y, 2002. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc 8, 448–460. [PubMed] [Google Scholar]
- Stern Y, Albert S, Tang M, Tsai W, 1999. Rate of memory decline in AD is related to education and occupation. Neurology 53, 1942–1947. [DOI] [PubMed] [Google Scholar]
- Stern Y, Alexander GE, Prohovnik I, Mayeux R, 1992. Inverse relationship between education and parietotemporal perfusion deficit in Alzheimer’s disease. Ann. Neurol 32, 371–375. 10.1002/ana.410320311 [DOI] [PubMed] [Google Scholar]
- Stern Y, Arenaza-Urquijo EM, Bartrés-Faz D, Belleville S, Cantilon M, Chetelat G, Ewers M, Franzmeier N, Kempermann G, Kremen WS, Okonkwo O, Scarmeas N, Soldan A, Udeh-Momoh C, Valenzuela M, Vemuri P, Vuoksimaa E, Arenaza Urquiljo EM, Bartrés-Faz D, Belleville S, Cantillon M, Chetelat G, Clouston SAP, Estanga A, Ewers M, Franzmeier N, Gold B, Habeck C, Jones R, Kempermann G, Kochhann R, Kremen W, Lim YY, Martínez-Lage P, Morbelli S, Okonkwo O, Ossenkoppele R, Pettigrew C, Rosen AC, Scarmeas N, Soldan A, Song X, Udeh-Momoh C, Stern Y, Valenzuela M, Van Loenhoud AC, Vemuri P, Vuoksimaa E, 2018. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dement. 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern Y, Tang HMX, Denaro J, Mayeux R, 1995. Increased Risk of Mortality in Alzheimer’s Disease Patients with More Advanced Educational and Occupational Attainment. Ann. Neurol 37, 590–595. [DOI] [PubMed] [Google Scholar]
- Vemuri P, Weigand S, Przybelski S, Knopman D, Smith G, Trojanowski J, Shaw L, Decarli C, Carmichael O, Bernstein M, Aisen P, Weiner M, Peterson R, Jack C Jr, 2011. Cognitive reserve and Alzheimer’s disease biomarkers are independent determinants of cognition. Brain 134, 1479–1492. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.