

Abstract
An epidemiological study of rotavirus infection was conducted on specimens collected from patients with gastroenteritis and domiciled in the rural Upper Eastern Region of Ghana during 1998. Fifty isolates, randomly selected from 165 human group A rotavirus-positive samples, were G and P characterized by a reverse transcription (RT)-PCR assay using a seminested multiplex method. Rotaviruses of the G3 genotype were found to be the predominant strain (78%), followed by G2 (14%) and G1 (2%). Mixed infections, as shown by combinations of G3 and G2 (4%) and G3 and G1 (2%), were also observed. P typing showed P[4] (72.34%) to be the prevalent strain, followed by P[6] (21.3%), P[8] (2.13%), and a combination of P[4] and P[6] (4.3%).
Rotavirus diarrhea is a public health problem throughout the world. Group A human rotaviruses are a major cause of acute gastroenteritis in young children in both developing and developed countries (16). More than 870,000 children under 5 years old are estimated to die annually from rotavirus infections in developing countries. Earlier studies in Ghana have also shown rotaviruses to be important pathogens in diarrhea in children (2). These studies, which were all conducted in southern Ghana, showed that group A human rotavirus was responsible for more than 20% of diarrheas in children aged 18 months or less, was seasonal, and was detectable in 10 of the 12 months, with peaks in September and February.
Rotaviruses are at present the subject of intense vaccine research and trials worldwide (7, 19). However, studies of the immunogenicity of natural infection have shown that initial infection is predominantly associated with a homotypic response which broadens after subsequent infections (13), leading to protective immunity to all antigenic types. The implication is that a vaccine must induce protective immunity against antigenic types circulating in the community before the first exposure (21). Present formulation of a rhesus rotavirus tetravalent vaccine which was licensed by the U.S. Food and Drug Administration (the vaccine was suspended because of suspected association with intussusception) protected against the four rotavirus serotypes, G1, G2, G3, and G4, that predominate globally (11). However, recent studies in Brazil, Malawi, and India (6, 18, 20) have identified serotypes other than those known globally, and possible implications for rotavirus vaccines are now being studied.
The outer capsid of the rotavirus is made up of two structural proteins, VP7 and VP4, which elicit neutralizing antibodies. These proteins, encoded by genes 9 (7 or 8, depending on strain) and 4 of the rotavirus genome, can segregate independently by the mechanism of reassortment (6) and form the basis of the dual classification system of rotaviruses. VP7, which is a glycoprotein and hence designated G, is the major neutralization antigen of the virion and defines its G serotype. To date, more than 14 VP7 serotypes have been identified in humans and animals (serotypes G1, G2, G3, and G4 occur commonly in humans). The VP4 gene exhibits antigenic polymorphism and is important for virulence and cellular attachment. Ten VP4 proteins, including eight in humans, have been identified by neutralization assays. The most commonly found P types in children with gastroenteritis are P[8] and P[4]. VP4, designated P, is a protease-sensitive protein, and infectivity is activated by the cleavage of this protein. Both G and P form the basis of rotavirus classification and description (8). Knowledge of the diversity and distribution of G and P types circulating in a community is crucial to the formulation of an adequate vaccine as well as the evaluation of protection after vaccination.
In this study, we report on results of VP7 and VP4 characterization by reverse transcription (RT)-PCR. Out of 165 samples positive for rotavirus enzyme-linked immunosorbent assay (ELISA), 66 had sufficient RNA by polyacrylamide gel electrophoresis (PAGE) analysis, out of which 50 were randomly selected for further analysis. The rotavirus strains were isolated from children under 2 years of age with gastroenteritis in northern Ghana during the rotavirus season of 1998.
The Kasena Nankana district of the Upper East region of Ghana lies within the Guinea savannah woodland area and has a population of 140,000. The population is rural except for those living in the town of Navrongo, the district administrative center, which has a population of about 20,000. It has two main seasons, a short wet season from June to September and a long dry season for the rest of the year. The average annual rainfall is 950 mm, mean monthly temperatures range from 20 to 40°C, and settlements are dispersed. Data from the only district hospital indicate that diarrheal diseases are among the main health problems in the district. It is the second most common cause of admission (after malaria), accounting for 19.7% (608 of 3,085) of all admissions (annual district report, 1996, Navrongo Health Research Centre, Navrongo, Ghana). In 1996, 10.6% of all outpatients in attendance at the district hospital were diagnosed as having diarrhea, with most of them being children less than 5 years of age.
Stool and rectal swab samples were obtained from children less than 2 years of age who sought medical attention at the only district hospital and two other selected health centers with high outpatient attendance. This was during the period from August to December 1998. Stool and swab samples were kept at −20°C and transported weekly on ice by airplane to the Noguchi Memorial Institute for Medical Research in Accra, where they were stored at −20°C until tested.
As stated above, all 165 samples were positive for human rotavirus obtained from the study by using a commercial rotavirus ELISA kit (Dako Diagnostics Ltd., Ely, Cambridgeshire, United Kingdom). The 50 samples subjected to genotyping were randomly selected from 66 samples that were positive by PAGE analysis. Rotavirus diagnosis was confirmed by ELISA. Briefly, 10% of stool samples were made in phosphate buffered saline (PBS; pH 7.2) and tested for group A rotaviruses with the IDEIA Rotavirus Kit (Dako Diagnostics Ltd.) following the manufacturer's instructions. All swabs were immersed in 1 ml of PBS and allowed to soak for 30 min, and suspensions were expressed from the cotton swab. This was repeated and the two washings were pooled. The tests were read both visually and spectroscopically at a wavelength of 450 nm. Each plate included a negative and positive control, and all tests were performed in duplicate.
The subgrouping of rotaviruses was performed on the 50 randomly selected rotavirus PAGE-positive samples using 96-well microtiter plates coated with rabbit polyclonal antirotavirus antibodies (provided by Dako) with minor modifications to published procedures (3). Monoclonal antibodies 255/60 and 631/9, specific for subgroup I and II, respectively, were used for subgrouping ELISA responses. A commercial horseradish peroxidase-conjugated goat anti-mouse immunoglobulin G and tetramethylbenzidine-H2O2 (Sigma) were used as the chromogen and substrate. Absorbance (optical density [OD]) was measured at 450 nm (OD450). The cutoff value was calculated as the mean OD450 plus three standard deviations of the rotavirus-negative fecal sample controls. A sample was considered positive if the OD450 was above the cutoff value and if the ratio of the highest OD450 value obtained versus the OD450 of that sample reacting against monoclonal antibodies to the other subgroup was equal to or greater than 2. When the value of this ratio was between 1.5 and 2, the result was considered equivocal.
Further analysis of the 165 ELISA-positive samples by PAGE allowed us to select samples with intact virus particles that had genomic RNA for further characterization by RT-PCR. Our experience and that of others (15) has shown that samples that are positive by both ELISA and PAGE have a better chance of being able to be typed by molecular methods. Furthermore, the PAGE analysis on the ELISA-positive samples also made it possible to study the electropherotypes. Control samples were rotavirus strain SA11 and ELISA-negative stool samples. RNA was extracted by the method described by Gallimore et al. (9). Briefly, 500 μl of a 10% fecal extract was added to 1 ml of L6 (consisting of guanidine thiocyanate and Triton X-100) extraction buffer and 10 μl of size-fractionated silica and vortexed for 10 s. The pellet was washed with L2 buffer (consisting of guanidine thiocyanate), dehydrated in 70% ethanol and acetone, and finally dried at 56°C in a dry heating block for 15 min (with the microcentrifuge tube lid open). The nucleic acids were then eluted from the silica by adding 50 μl of RNase-free double-distilled water and incubating at 56°C for 15 min. Approximately 20 μl of sample was loaded onto a 10% acrylamide gel using the discontinuous buffer system (17) and run overnight at a constant voltage of 40 A. A 5% stacking gel was employed to enhance resolution of the RNA bands. The gels were stained using a silver staining technique (14).
RNA was extracted from 100 μl of 10% fecal suspensions in PBS according to the method described by Boom et al. (4) and eluted in 26 μl of RNase-free sterile distilled water containing 40 U of ribonuclease inhibitor (RNasin; Promega, Madison, Wis.). The extracted RNA was used for RT-PCR after random priming with hexamers (15). Briefly, 1 μl of random primer (20 mU; PdN6; Pharmacia Biotech) was added to 20 μl of the extracted RNA, heated at 97°C for 5 min to denature the double-stranded RNA, and chilled on ice for 2 min, followed by annealing of the primers for 5 min at room temperature. Fourteen microliters of the RT reaction mixture was added, yielding a total volume of 35 μl, consisting of 20 mM Tris-HCl (pH 8.4), 50 mM KCl, 5 mM MgCl2, a 50 μM concentration of each deoxynucleoside triphosphate (Life Technologies, Gaithersburg, Md.), and 200 U of Moloney murine leukemia virus reverse transcriptase (Life Technologies). The RT-PCR was carried out by incubation at 37°C for 1 h, and the reaction was terminated by heating at 95°C for 5 min followed by chilling on ice for 2 min.
G typing was performed using a seminested PCR and adapted from the method of Gouvea et al. (12). The first-round PCR amplified the whole length of the VP7 gene using primers Beg 9 and End 9. The second-round typing PCR was a multiplex PCR and incorporated the primer End 9 and the G-type-specific primers aBT1 (G1 specific), aCT2 (G2 specific), aET3 (G3 specific), aDT4 (G4 specific), aAT8 (G8 specific), and aFT9 (G9 specific). The PCR mixture for the first round consisted of 18 mM Tris-HCl (pH 8.4), 45 mM KCl, 2 mM MgCl2, 50 μM concentrations of each deoxynucleoside triphosphate, 1 U of Taq polymerase (Life Technologies), and 2 μM concentrations of each primer. The first-round PCR was performed by adding 5 μl of the random-primed cDNA to 45 μl of the PCR mix. After denaturation at 94°C for 5 min, 30 PCR cycles each consisting of 94°C for 1 min, 42°C for 2 min, and 72°C for 1 min were performed, followed by an extension at 72°C for 7 min. The second-round PCR was performed using the same protocol but with 1 μl of the first-round reaction product as the template in a final reaction volume of 50 μl and reducing the number of cycles to 15. All amplified products were examined by gel electrophoresis in 2% agarose gels (Seakem; Flowgen) containing 4 μg of ethidium bromide/ml under standard conditions.
P typing was performed using a seminested PCR adapted from the method of Gentsch et al. (10). The first-round PCR amplified an 876-bp fragment of gene 4 of group A rotaviruses by using the consensus primers Con2 and Con3. The second-round PCR incorporated Con3 and the P-type-specific primers 1T-1 (P[8] specific), 2T-1 (P[4] specific), 3T-1 (P[6] specific), 4T-1 (P[9] specific), and 5T-1 (P[10] specific). The PCR mix for the first and second rounds of amplification was the same as that for the G typing, except for the primer concentrations (1 μM Con2 and Con3 for the first-round PCR and 2 μM concentrations of each typing primer for the second round). Forty PCR cycles were performed, with annealing at 50°C for 1 min. The second-round PCR was reduced to 25 cycles. PCR products were examined as described above.
Of 165 ELISA-positive samples analyzed for genomic RNA by PAGE, 66 were positive and exhibited the typical rotavirus electrophoretic pattern. These samples were collected from children less than 2 years old with diarrhea who sought medical assistance at health facilities in the Upper East region of Ghana. All the samples were collected during the months of August to December 1998. However, 50 samples for which there was enough genomic RNA available were randomly selected for further study. The electrophoretic patterns of the selected samples were all of the short electropherotype, as shown in Fig. 1, and did not exhibit any unusual patterns. Two distinct rotavirus RNA profiles were observed, with the dominant being pattern b (69%).
FIG. 1.
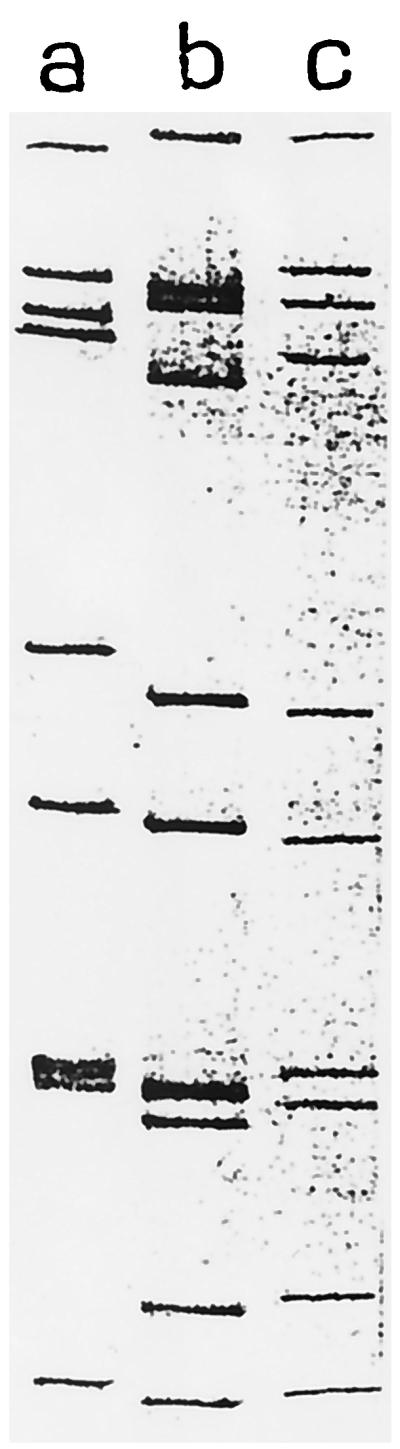
Electropherotypes of isolated strains. Lane a is the control rotavirus strain SA11.
All 50 samples that were positive by ELISA and had sufficient genomic RNA by PAGE were subjected to both VP4 and VP7 genotyping by using RT-PCR. All of the samples could be assigned both G and P genotypes, except for three (6%) which could only be assigned a G genotype. Three G types, namely G1, G2, and G3, were observed during the study period. The predominant G type observed was G3 (80%), followed by G2 (12%) and G1 (2%). The interesting observation was that all G2 strains were of the subgroup 1 subtype and had short electrophoretic profiles. There were no rotavirus strains with the VP7 G4 genotype detected in the study area. The mixed infections detected were of G1 plus G2 and G2 plus G3 genotype specificity.
The VP4 genotypes detected during the study were P[4], P[6], and P[8], as well as strains with the dual P types P[4] and P[6]. The predominant P type was P[4] (72.3%), followed by P[6] (21.3%) and P[8] (2.1%). The most common G-P combinations were G3P[4] (74%), G2P[6] (12%), and G3P[6] (7.0%). Isolates with the G2P[4], G3P[8], and G1P[6] G-P combinations were also detected. Three isolates (6%) were mixed infections of either G1 plus G3 or G2 plus G3. The genotype distributions are shown in Table 1.
TABLE 1.
Circulating G and P genotypes in Northern Ghana during 1998
| Genotype | G1 | G2 | G3 | G1+G3 | G2+G3 | Total |
|---|---|---|---|---|---|---|
| P[4] | 0 | 1 | 32 | 1 | 0 | 34 |
| P[6] | 1 | 5 | 3 | 0 | 1 | 10 |
| P[8] | 0 | 0 | 1 | 0 | 0 | 1 |
| P[4+6] | 0 | 0 | 1 | 0 | 1 | 2 |
| P[nt]a | 0 | 0 | 3 | 0 | 0 | 3 |
| Total | 1 | 6 | 40 | 1 | 2 | 50 |
nt, nontypeable.
In this study of rotavirus G and P types in Ghana, strains with the genotype G3 were the predominant strain, followed closely by G2 and combinations of G1, G2, and G3. Genotype G4, one of the most common G types worldwide, was not detected in the samples examined. This is in contrast to what was observed in our earlier studies in southern Ghana (2). The inability to detect G4 strains may be associated with the relatively small number of samples tested, nonoccurrence in the study area, or a genetic shift, since it had been detected earlier in the south of the country. PAGE analysis showed that the RNA profiles of the isolated G1 and G3 strains were all of the short electropherotype. This phenomenon has also been observed in studies in the nearby countries of the Ivory Coast (V. Akran, C. Akoua-Koffi, H. Kette, and M. Dosso, Abstr. Afr. Health Sci. Congr., abstr. O-209, p. 149, 1997) and Burkina Faso (S. Sawodogo, personal communication). Adah et al. (1) also reported strains of the G3 genotype with the short RNA electropherotype in Nigeria.
This study in Ghana has brought to light some important observations that may have implications for rotavirus vaccine design and formulation. Firstly, the strains G1P[8], G3P[8], G4P[8], and G2P[4] are the most common strains globally associated with symptomatic disease. However, these strains seem to be underrepresented in our samples. Secondly, we report here the isolation of G3 strains with P[4] specificity for the first time in West Africa. The only other reported isolation of G3P[4] genotypes in Africa is the study of Cunliffe et al. (6) in Malawi. While in the Malawian study G3P[4] strains constituted only 1% of isolates, it was the most predominant (62%) strain in our studies. The next most predominant G type was G2. However, it is interesting that 83% of all of the isolated G2 strains exhibited the P[6] genotype, a genotype thought to be associated with asymptomatic infections in neonates. The P[6] genotype has also been implicated in diarrhea in children in Nigeria, Kenya, Brazil, Malawi, and India (1, 5, 6, 20). These results further emphasize the need to examine the role of P[6] genotypes in asymptomatic infections as well as its consideration for inclusion in future rotavirus vaccines. Thirdly, the detection of unusual G-P types such as G2P[6] (9.4%), G3P[6] (6.4%), and G1P[6] (2.13%) may be due to possible reassortment during natural infections. Studies involving rotavirus assays on porcine and bovine diarrheic samples collected from our study area are ongoing. The results from the molecular characterization of these strains will help us in discussing further the issue of possible reassortment. This is especially so because, in an area such as ours where domestic animals and humans live very closely together and in most cases share the same source of water, mixed infections are quite common. It must be further reiterated that the majority of the isolates in the study area belonged to uncommonly described G-P types. Fourthly, we observed that both the G1 and G3 strains, which are strains known to possess long RNA patterns, possessed short electrophoretic patterns. In some instances, the samples which could not be P typed using conventional primer sets could be an indication of an unknown strain(s) or of the emergence of a new VP4 type in West Africa.
This study has demonstrated the existence of rotavirus strains with unusual G and P combinations. The existence of multiple G and P types increases the possibility of natural reassortment and the creation of novel strains, with serious implications for vaccine design and development. There is, therefore, a need to reinforce continuous surveillance of rotavirus types in communities to identify circulating strains as well as to detect the emergence of new rotavirus strains. It is hoped that results from this genetic characterization will help address some of the issues raised.
Acknowledgments
We are extremely grateful to the Department of Foreign and International Development of the United Kingdom, the Noguchi Memorial Institute for Medical Research (NMIMR), University of Ghana, and The Ministry of Health, Ghana, for financial assistance in the form of research grants and salaries.
We thank the field staff of the Navrongo Health Research Centre and the technical staffs of the Electron Microscope Unit of NMIMR and the Central Public Health Laboratory, London, United Kingdom, for their assistance.
REFERENCES
- 1.Adah M I, Rohwedder A, Olaleyly O D, Werchau H. Nigerian rotavirus serotype G8 could not be typed by PCR due to nucleotide mutation at the 3′ end of the primer binding site. Arch Virol. 1997;142:1881–1887. doi: 10.1007/s007050050206. [DOI] [PubMed] [Google Scholar]
- 2.Armah G E, Hori H, Ayanful A, Mingle J A A, Commey J O O, Kamiya H, Nkrumah F K. Human rotavirus subgroups/subtypes and severity of associated diarrhoea in Ghana. Afr J Health Sci. 1995;2:388–391. [PubMed] [Google Scholar]
- 3.Beads G M. Serotyping of rotavirus by NADP-enhanced enzyme immunoassay. J Virol Methods. 1987;18:77–85. doi: 10.1016/0166-0934(87)90113-3. [DOI] [PubMed] [Google Scholar]
- 4.Boom R, Sol C J A, Salismans M M M, Jansen C L, Wertheim-van Dillen P M E, Van Den Noordaa J. Rapid and simple method for the purification of nucleic acids. J Clin Microbiol. 1990;28:495–503. doi: 10.1128/jcm.28.3.495-503.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Carmo M, Timenetsky S T, Santos N, Gouvea V. Survey of rotavirus G and P type associated with human gastroenteritis in Sao Paulo, Brazil, from 1986 to 1992. J Clin Microbiol. 1994;32:2622–2624. doi: 10.1128/jcm.32.10.2622-2624.1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cunliffe N A, Gondwe J S, Broadhead R L, Molyneux M E, Woods P A, Bresee J S, Glass R I, Gentsch J R, Hart A. Rotavirus G and P types in children with acute diarrhoea in Blantyre, Malawi, from 1997 to 1998: predominance of novel P(6)G8 strains. J Med Virol. 1999;57:308–312. [PubMed] [Google Scholar]
- 7.Estes M K. Advances in molecular biology: impact on rotavirus vaccine development. J Infect Dis. 1996;174(Suppl. 1):S37–S46. doi: 10.1093/infdis/174.supplement_1.s37. [DOI] [PubMed] [Google Scholar]
- 8.Estes M K. Rotaviruses and their replication. In: Fields B N, et al., editors. Fields virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven Press; 1996. pp. 1625–1655. [Google Scholar]
- 9.Gallimore C I, Appleton H, Lewis D, Green J, Brown D W G. Detection and characterization of bisegmented double-stranded RNA viruses (picobinaviruses) in human faecal specimens. J Med Virol. 1995;45:135–140. doi: 10.1002/jmv.1890450204. [DOI] [PubMed] [Google Scholar]
- 10.Gentsch J R, Glass R I, Woods P A, Gouvea V, Gorziglia M, Flores J, Das B K, Bhan M K. Identification of group A rotavirus gene 4 types by polymerase chain reaction. J Clin Microbiol. 1992;30:1365–1373. doi: 10.1128/jcm.30.6.1365-1373.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gentsch J R, Woods P A, Ramanhandran M, Das B K, Alfieri A, Kumar R, Bhan M K, Glass R I. Review of G and P typing results from a global collection of rotavirus strains: implications for vaccine development. J Infect Dis. 1996;174(Suppl. 1):S30–S36. doi: 10.1093/infdis/174.supplement_1.s30. [DOI] [PubMed] [Google Scholar]
- 12.Gouvea V, Glass R I, Woods P A, Taniguchi K, Clark H F, Forrester B, Fang Z-Y. Polymerase chain reaction amplification for typing of rotavirus nucleic acid from stool specimens. J Clin Microbiol. 1990;28:276–282. doi: 10.1128/jcm.28.2.276-282.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Green K, Taniguchi K, Mackow E, Kapikan A Z. Homotypic and heterotypic epitope-specific antibody responses in adults and infants vaccinees: implications for vaccine development. J Infect Dis. 1990;161:667–679. doi: 10.1093/infdis/161.4.667. [DOI] [PubMed] [Google Scholar]
- 14.Herring A J, Inglis N F, Ojeh C K, Snodgrass D R. Rapid diagnosis of rotavirus infection by direct detection of viral nucleic acid in silver-stained polyacrylamide gels. J Clin Microbiol. 1982;16:473–477. doi: 10.1128/jcm.16.3.473-477.1982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Iturriza-Gómara M, Green J, Brown D W G, Desselberger U, Gray J J. Comparison of specific and random priming in the reverse transcriptase polymerase chain reaction for genotyping group A rotaviruses. J Virol Methods. 1999;78:93–103. doi: 10.1016/s0166-0934(98)00168-2. [DOI] [PubMed] [Google Scholar]
- 16.Kapikian A Z. Overview of viral gastroenteritis. Arch Virol Suppl. 1996;12:7–19. doi: 10.1007/978-3-7091-6553-9_2. [DOI] [PubMed] [Google Scholar]
- 17.Laemmli U K. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature (London) 1970;227:680–685. doi: 10.1038/227680a0. [DOI] [PubMed] [Google Scholar]
- 18.Leite J P G, Alfieri A A, Woods P A, Glass R I, Gentsch J R. Rotavirus G and P types circulating in Brazil: characterization by RT-PCR, probe hybridization and sequence analysis. Arch Virol. 1996;141:2365–2374. doi: 10.1007/BF01718637. [DOI] [PubMed] [Google Scholar]
- 19.Parashar U D, Bresee J S, Gentsch J R, Glass R I. Rotavirus. Emerg Infect Dis. 1998;4:5611–5670. doi: 10.3201/eid0404.980406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ramachandran M, Das B K, Vij A, Kumar R, Bhambal S S, Kesari N, Rawat H, Bhal L, Thakur S, Woods P A, Glass R I, Bhan M K, Gentsch J R. Unusual diversity of human rotavirus G and P types in India. J Clin Microbiol. 1996;34:436–439. doi: 10.1128/jcm.34.2.436-439.1996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Smith J C, Haddix A C, Teutsch S M, Glass R I. Cost-effectiveness analysis of a rotavirus immunization program for the United States. Pediatrics. 1995;96:6609–6615. [PubMed] [Google Scholar]