

Abstract
Diabetic kidney disease (DKD) is the most common cause of ESKD in the United States and worldwide. Current treatment for DKD includes strict glycemic control and normalization of BP with renin-angiotensin-aldosterone system (RAAS) blockade. Although RAAS blockers slow progression of disease, they do not generally prevent ESKD and none of the studies with these agents in DKD included patients who were nonproteinuric, which make up an increasingly large percentage of patients with diabetes now seen in clinical practice. Recent studies with glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter-2 (SGLT2) inhibitors have shown beneficial renal effects, and the benefits of SGLT2 inhibitors likely extend to patients who are nonproteinuric. However, there remains a need to develop new therapies for DKD, particularly in those patients with advanced disease. A role of chronic low-grade inflammation in microvascular complications in patients with diabetes has now been widely accepted. Large clinical trials are being carried out with experimental agents such as bardoxolone and selonsertib that target inflammation and oxidative stress. The Food and Drug Administration–approved, nonspecific phosphodiesterase inhibitor pentoxifylline (PTX) has been shown to have anti-inflammatory effects in both animal and human studies by inhibiting the production of proinflammatory cytokines. Small randomized clinical trials and meta-analyses indicate that PTX may have therapeutic benefits in DKD, raising the possibility that a clinically available drug may be able to be repurposed to treat this disease. A large, multicenter, randomized clinical trial to determine whether this agent can decrease time to ESKD or death is currently being conducted, but results will not be available for several years. At this time, the combination of RAAS blockade plus SGLT2 inhibition is considered standard of care for DKD, but it may be reasonable for clinicians to consider addition of PTX in patients whose disease continues to progress despite optimization of current standard-of-care therapies.
Keywords: Diabetes and the Kidney, Anti-Inflammatory Agents, Diabetic Nephropathies, Inflammation, Pentoxifylline, Sodium-Glucose Transporter 2 Inhibitors, Standard of Care
Introduction
Diabetic kidney disease (DKD) is the most common cause of ESKD in the United States (1). The pathogenesis of DKD includes mesangial expansion, endothelial dysfunction, loss of glomerular podocytes, and interstitial fibrosis. The classic natural history of DKD is the development of albuminuria, with small amounts of albuminuria (microalbuminuria) progressing to overt albuminuria (macroalbuminuria) and nephrotic syndrome, eventually leading to ESKD. The characteristic renal pathologic findings are diffuse and nodular glomerulosclerosis (2). Proteinuria is an important predictor of outcome in CKD, including DKD (3,4). Risk factors for progression to ESKD include hyperglycemia, hypertension, severity of albuminuria, and presence of retinopathy (5). High salt intake and arteriosclerosis are implicated in the development of DKD, especially in patients with type 2 diabetes mellitus (DM) (6). Patients with DKD are at markedly increased risk for cardiovascular events and mortality (7,8).
Current treatment for DKD includes strict glycemic control and normalization of BP, with renin-angiotensin-aldosterone system (RAAS) blockade being the cornerstone of antihypertensive therapy (9). Although RAAS blockers such as angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are effective in slowing progression of disease, they do not generally prevent progression to ESKD (10,11). Combination RAAS blockade has not been proven to be more effective than monotherapy and is associated with increased adverse events (12). Recent studies with glucagon-like peptide-1 receptor agonists and, in particular, sodium-glucose cotransporter-2 (SGLT2) inhibitors have shown beneficial renal effects (13,14). In the CREDENCE study, the first study since those with RAAS blockers to show a reduction in hard renal end points, there was an impressive 34% reduction in ESKD and also a reduction in cardiovascular mortality with the SGLT2 inhibitor canagliflozin (14).
Albuminuric versus Nonalbuminuric DKD
In recent years, possibly due to better treatment of diabetes and hypertension and the use of RAAS blockers, the prevalence of nonalbuminuric versus albuminuric DKD has increased, especially in type 2 DM. In a cross-sectional analysis of United States adults with diabetes from the National Health and Nutrition Examination Survey (NHANES) III (1988–1994), 35% of subjects with an eGFR of <60 ml/min per 1.73 m2 were normoalbuminuric, and albuminuria and retinopathy were both absent in 30% of subjects with reduced eGFR (15). In subsequent cross-sectional analyses of NHANES data, higher adjusted prevalence rates (approximately 50%) for the nonalbuminuric phenotype among individuals with reduced eGFR were observed (8). Similar findings have been observed in cohorts of patients with type 2 DM outside the United States and in those enrolled in multicenter, multinational, interventional studies (16).
Currently there are no large trials that have been performed in nonalbuminuric DKD. It is not known whether RAAS blockers have similar benefits in these patients. Concern has been raised that RAAS blockers, by preventing constriction of the efferent arteriole, may actually increase susceptibility to AKI in patients who are nonalbuminuric (16). With respect to SGLT2 inhibitors, in a post hoc analysis of data from the CANVAS program, canagliflozin slowed the annual loss of kidney function across albuminuria subgroups, suggesting that SGLT2 inhibitors may also be beneficial in patients who are nonalbuminuric, although there was a greater absolute benefit in participants with severely increased albuminuria (17). The concern about AKI that can occur with RAAS blockers does not appear to extend to SGLT2 inhibitors (18). The beneficial effect of SGLT2 inhibitors might attenuate with declining kidney function and there is currently no clear evidence for benefit in those with eGFR of <30 ml/min per 1.73 m2, although such studies are being conducted (19). The increasing prevalence of nonalbuminuric or minimally albuminuric DKD underscores the need to develop new therapies for nonalbuminuric DKD, particularly in those patients with advanced CKD.
Nonalbuminuric DKD is thought to be predominantly due to vascular and tubulointerstitial lesions, and decline in renal function in such patients may be at least partly due to ongoing inflammation not entirely remediated by current therapies (16). Therefore, there is much interest in the development of anti-inflammatory agents for the treatment of DKD.
Inflammation in DKD
DKD has traditionally been considered to be caused by the adverse effects of hyperglycemia (metabolic theory) and hemodynamic alterations that increase systemic and intraglomerular pressure (hemodynamic theory) in patients who are genetically predisposed. Nearly three decades ago, Hasegawa et al. (20) initially suggested, based on studies in diabetic animals, that proinflammatory cytokines might be involved in the pathogenesis of DKD. The source of cytokine production by the kidneys in DM is from both infiltrating macrophages and resident kidney cells. Production of reactive oxygen species, proinflammatory factors, and certain growth factors (such as TGF-β) can induce renal damage, and macrophage-depletion studies in rodent models have shown a causal role for macrophages in the progression of DKD (21). In a human biopsy study, Nguyen et al. (22) reported that accumulation of macrophages was more prevalent in the interstitium than in the glomeruli and that interstitial macrophages correlated strongly with proteinuria, decline in renal function, and extent of interstitial fibrosis. Various types of renal cells (endothelial, mesangial, epithelial, and tubular cells) are capable of synthesizing proinflammatory cytokines such as TNF-α, IL-1, and IL-6. These cytokines, acting in a paracrine or autocrine manner, contribute to the pathophysiology of DKD (23). Plasma concentrations of proinflammatory cytokines are elevated in patients with type 2 DM (24,25) and increase as nephropathy progresses (26,27). Inflammation and oxidative stress are associated with both micro- and macrovascular diabetic complications (28,29).
TNF-α is an important proinflammatory cytokine and has been much studied in DKD. In a study by Navarro et al. in patients with type 2 DM with mild proteinuria (<1 g/d), serum concentrations of high-sensitivity C-reactive protein and serum and urine concentrations of TNF-α correlated with albuminuria. Urinary TNF-α levels increased significantly as nephropathy progressed (30). In a recent meta-analysis, serum and urinary concentrations of TNF-α are elevated in patients with DKD and these concentrations increase concomitantly with the progression of CKD (31). This cytokine is cytotoxic to glomerular cells in vitro (32) and increases protein permeability in isolated glomeruli, independent of hemodynamic alterations or effects of recruited inflammatory cells (33). In diabetic animals, increased urinary as well as renal interstitial concentrations of TNF-α precede the rise in albuminuria (34). In a proof-of-concept study, Moriwaki et al. (35) found that diabetic rats treated with the chimeric anti–TNF-α antibody infliximab showed a reduction in albuminuria.
Proinflammatory ILs are also involved in the pathogenesis of DKD. In a biopsy study, IL-6 mRNA was expressed by glomerular resident cells and interstitial cells in patients with DKD (36). Most cells in the area of mesangial proliferation were strongly stained for IL-6 mRNA, and some positive cells were found in the Kimmelstiel–Wilson nodular lesions. In the interstitium, some tubules and infiltrating cells were also positively stained for IL-6 mRNA, and the interstitial expression of IL-6 mRNA correlated significantly with the degree of interstitial injury. In another biopsy study in type 2 DM, glomerular basement membrane width was directly correlated with IL-6 (37), and both IL-1 and IL-6 have been shown to be overproduced by interstitial and glomerular cells in diabetes (37–39). In streptozotocin diabetes in the rat, renal cortical mRNA expression for TNF-α, IL-1, and IL-6 was 2.4-, 1.2-, and 3.4-fold higher than in nondiabetic rats. Albuminuria was significantly associated with renal mRNA expression of TNF-α and IL-6 but not IL-1 (38). Another proinflammatory IL, IL-18, may also play an important role in DKD (40). Chronically increased levels of inflammation are associated with an increase in C-reactive protein, the latter of which is associated with many pathologic conditions in diabetes, including atherosclerosis and DKD (41).
Targeting Inflammation in DKD
A role of chronic low-grade inflammation in the microvascular complications in patients with diabetes has now been widely accepted (42,43). Several approaches have been proposed to treat inflammation in DKD, including lifestyle modifications (diet and exercise) and medications. Anti-inflammatory effects may explain some of the benefits of SGLT2 inhibitors and possibly also glucagon-like peptide-1 receptor agonists (21). In addition, three large randomized controlled trials specifically targeting inflammation in DKD have been or are currently being performed.
Bardoxolone
Bardoxolone targets oxidative stress and reduces inflammation by inhibiting proinflammatory cytokines and decreasing TGF-β and extracellular matrix proteins (44). The BEACON study using the NF erythroid 2-related factor 2 activator bardoxolone methyl was stopped prematurely due to an increase in adverse cardiovascular outcomes, and thus its role in ESKD prevention could not be assessed (45). However, in a subsequent post hoc analysis, patients treated with bardoxolone were significantly less likely to experience the composite renal end point (46). Bardoxolone is being studied again in Japan in a Phase 3 Study of Bardoxolone Methyl in Patients with DKD; AYAME Study (NCT03550443), with an estimated completion date of March 2022. Patients with an eGFR of 15–60 ml/min per 1.73 m2 will be studied. The primary outcome is time to onset of a ≥30% decrease in eGFR from baseline or ESKD.
Selonsertib
Glucose can activate the transcription factor NF-κB, resulting in increased inflammatory gene expression, in part through oxidative stress, advanced glycation end products (AGEs), protein kinase C, and mitogen-activated protein kinases. Apoptosis signal–regulating kinase 1 (ASK1) acts as an upstream regulator for the activation of p38 mitogen-activated protein kinases and c-Jun N-terminal kinase. Oxidative stress increases ASK1 activity, promoting inflammation, apoptosis, and fibrosis. In animal models of DKD, ASK1 inhibition reduces progressive kidney injury, inflammation, and fibrosis (47). Selonsertib is a highly selective, potent, small-molecule inhibitor of ASK1 being developed as a once-daily oral agent for the management of DKD. In a recent double-blind, placebo-controlled, phase 2 trial, selonsertib appeared safe with no dose-dependent adverse effects over 48 weeks. Effects on urinary albumin-to-creatinine ratio (UACR) did not differ between selonsertib and placebo, but exploratory post hoc analyses suggest that selonsertib may slow DKD progression (48). A phase 3 trial, Efficacy and Safety of Selonsertib in Participants with Moderate to Advanced DKD (MOSAIC; NCT04026165) is currently enrolling patients with type 2 DM and eGFR of 20–60 ml/min per 1.73 m2 with albuminuria and is estimated to be completed in December 2024. Clinical outcome measures are time to ≥40% decline in eGFR from baseline, ESKD, or death due to kidney disease.
Pentoxifylline
Phosphodiesterases (PDEs) are a class of enzymes that hydrolyze cAMP and cyclic guanosine monophosphate and are involved in many physiologic processes including cell proliferation and differentiation, cell-cycle regulation, gene expression, cellular metabolism, apoptosis, and inflammation. PDEs are composed of 11 different families and each family contains different subtypes. Pentoxifylline (PTX) is a methylxanthine derivative with pleomorphic effects including nonspecific inhibition of PDEs. PTX was approved by the US Food and Drug Administration for the treatment of intermittent claudication >30 years ago (49). Clinical experience has indicated that this agent has a favorable safety profile; therefore, if it can be shown to be efficacious, it could be an attractive agent to treat DKD (50).
PTX: Mechanism of Action.
PTX is known as a hemorheologic agent because it results in a reduction in blood viscosity, erythrocyte aggregation, erythrocyte rigidity, and platelet aggregation. The increase in red blood cell flexibility and deformability leads to improved blood flow (51). In addition, PTX has been shown to have immunomodulatory and anti-inflammatory effects (52). PDE inactivates the intracellular second messengers cAMP and cyclic guanosine monophosphate. PTX predominantly inhibits the PDE3 and PDE4 isoforms and thus primarily affects cAMP. The PTX-induced increase in cAMP will in turn increase protein kinase A activation, leading to a reduction in synthesis of the inflammatory cytokines IL-1, IL-6, and TNF-α (43,50).
PTX: Basic and Translational Studies.
PTX has an inhibitory effect on primary human renal fibroblasts in a time- and dose-dependent fashion (53). In animal studies in both diabetic and nondiabetic models, PTX exhibited a marked antiproteinuric effect while attenuating interstitial inflammation and progression of renal injury (34,38,54–57). In the streptozotocin-diabetic rat, PTX treatment can lead to improvement in signs of inflammation, oxidative stress, and subsequent fibrosis by acting on cytokine signaling (28,58). Similarly, in an alloxan-induced diabetic rat model, PTX also exerted anti-inflammatory effects via decreasing the levels of TNF-α and IL-6 (59). PTX may also be able to decrease inflammation generated by formation of AGEs. AGEs cause a series of signaling cascade events that result in an increase in oxidative stress and production of proinflammatory cytokines (i.e., IL-6, IL-1, and TNF-α) (60). PTX has been shown to decrease oxidative stress in diabetic animal models (58).
Another possible anti-inflammatory effect of PTX may be stimulation of Klotho, a type I single-pass transmembrane protein predominantly expressed in the kidneys (61). Reduced renal Klotho expression has been observed in biopsies from patients with early stages of DKD (62), and decreased plasma soluble Klotho may be an early biomarker for predicting DKD progression in patients with type 2 DM (63). The proinflammatory cytokines TNF-α and TNF-like weak inducer of apoptosis decrease renal Klotho expression mediated by NF-κB (64–66). In a recent post hoc analysis of the PREDIAN trial by Navarro-González et al. (67), administration of PTX to patients with type 2 DM with CKD stages 3 and 4 resulted in some reduction of serum and urinary TNF-α and increased serum and urinary Klotho concentrations. The mechanisms by which PTX is thought to inhibit inflammation are depicted in Figure 1.
Figure 1.
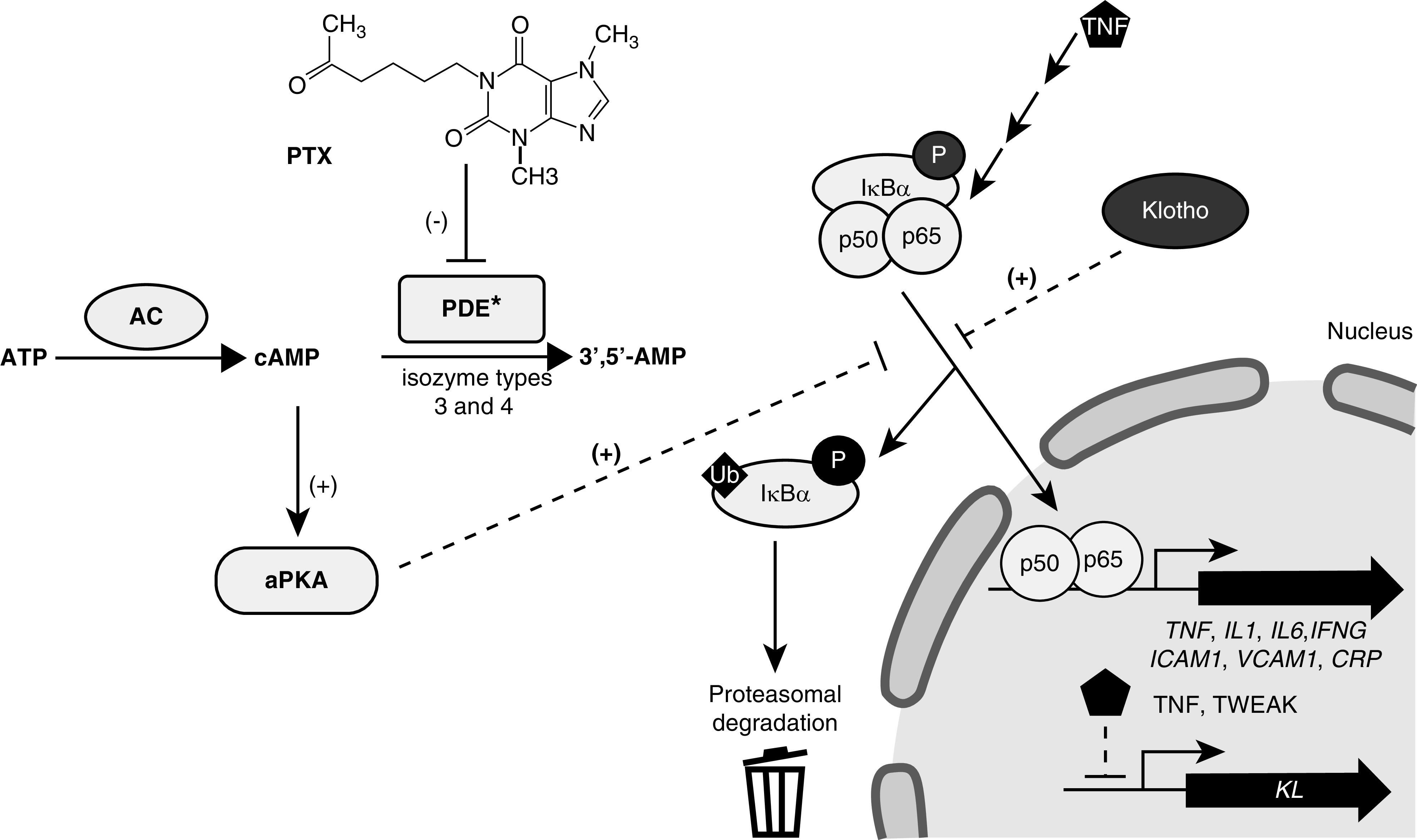
Pentoxifylline inhibits phosphodiesterase activity, increasing cAMP levels that activate protein kinase A. Active protein kinase A (aPKA) would inhibit ubiquitination that drives inhibitor of κ B α (IκBα) to 26S proteasome degradation and p50/p65 activation of the expression of cytokines and other genes. Decreased levels of TNF-α (TNF) and TNF-related weak inducer of apoptosis (TWEAK) increases Klotho (KL) expression, whereas KL inhibits the production of proinflammatory cytokines and TNF-induced adhesion molecules. AC, adenylate cyclase; CRP, C-reactive protein; ICAM1, intercellular adhesion molecule 1; IFNG, IFN-γ; P, phosphorylation; p50, NF-κB p50 subunit (NF-κ-light-chain-enhancer of activated B cells 1); p65, NF-κB p65 subunit (RelA; v-rel avian reticuloendotheliosis viral oncogene homolog A); PTX, pentoxifylline; VCAM1, vascular cell adhesion molecule 1. Reprinted from reference 43 (Donate-Correa J, Tagua VG, Ferri C, Martín-Núñz E, Hernández- Carballo C, Ureña-Torres P, Ruiz-Ortega M, Ortiz A, Mora-Fernández C, Navarro-González JF: Pentoxifylline for renal protection in diabetic kidney disease. A model of old drugs for new horizons. J Clin Med 8: E287, 2019), which is available under the terms of the Creative Commons Attribution License.
PTX: Clinical Trials.
Clinical data supporting a role for PTX in DKD have been accumulating for the past two decades. Most of these trials have used a small number of subjects and were of short duration, and all used surrogate end points such as reduction in proteinuria and changes in eGFR and not hard end points such as ESKD and death (Table 1) (68–82). Some, but not all, of these studies were placebo controlled, and none used intention-to-treat analysis or reported blinding of data assessors. Only the PREDIAN trial (73) provided details about the process of allocation concealment. In this study, the renoprotective effects of 2 years of PTX therapy in addition to RAAS blockade was evaluated in 169 white patients with type 2 DM and stage 3 or 4 CKD and urinary albumin excretion of >30 mg/24 h. Treatment with PTX (1200 mg/d) decreased proteinuria and urinary concentration of TNF-α and slowed decline in eGFR. At study end, eGFR had decreased by 2.1 ml/min per 1.73 m2 in the PTX group versus 6.5 ml/min per 1.73 m2 (between-group difference of 4.3 ml/min per 1.73 m2, P=0.001). The difference in reduction of eGFR was evident at 6 months and reached statistical significance at 1 year. There were no serious adverse events, and the only adverse events that occurred more commonly than with placebo were digestive symptoms (abdominal discomfort, flatus, dyspepsia, nausea, and vomiting), which were about twice as common in the treated group. Only one patient needed to have PTX withdrawn because of side effects. The favorable safety profile is supported by clinical experience in using this agent in treatment of peripheral vascular disease for decades with minimal side effects. Although these results are very intriguing, there are some limitations to the PREDIAN trial. First, the study enrolled only white patients. Second, it was a single-center study, which may limit its generalizability. Third, the study was open label and not placebo controlled. Finally, and most importantly, the study was not powered to detect differences in hard outcomes such as ESKD and mortality.
Table 1.
Renal effects of pentoxifylline in clinical trials
| Study | Duration | Entry Criteria | Groups | N | Intervention | Placebo Controlled | Outcome |
| Aminorroaya et al. (68) | 2 mo | Type 2 DM; UPE >300 mg/24 h | PTX versus captopril | 39 | PTX 1200 mg/d | No | Decrease in UPE in both groups (PTX, 29% reduction, P<0.05; captopril, 38% reduction, P<0.01) |
| Ghorbani et al. (69) | 6 mo | Type 2 DM; persistent UPE >150 mg/24 h despite RAAS blockers | PTX+losartan and enalapril versus losartan and enalapril | 100 | PTX 400 mg/d | No | Decrease in UPE (PTX, 69% reduction, P<0.001; control, 16% reduction, P=NS); increase in creatinine clearance (PTX, 6% increase; control, 0.7% decrease, P=0.04) |
| Guerrero-Romero et al. (70) | 4 mo | Type 1 and type 2 DM with overt proteinuria | PTX versus placebo | 86 | PTX 1200 mg/d | Yes | Decrease in UPE (type 1: PTX, 86% reduction, P<0.01; placebo, 7% reduction, P=NS; type 2: PTX, 93% reduction, P<0.001; placebo, 6% increase, P=NS) |
| Han et al. (71) | 6 mo | Type 2 DM; UACR >30 mg/g | PTX versus placebo | 174 | PTX 1200 mg/d | Yes | Decrease in UACR (PTX, 23% reduction; placebo, 4% reduction; P=0.012) |
| Harmankaya et al. (72) | 9 mo | Type 2 DM; persistent microalbuminuria | PTX+lisinopril versus lisinopril | 50 | PTX 600 mg/d | No | Decrease in UAE (PTX, 42% reduction, P<0.05; control, 35% reduction, P<0.05) |
| Navarro-González et al. (73) | 24 mo | Type 2 DM; stage 3–4 CKD; UAE >30 mg/24 h | PTX and ACEi or ARB versus ACEi or ARB | 169 | PTX 1200 mg/d | No | Decrease in UAE (PTX, 15% reduction; control, 6% increase; P=0.001); decrease in eGFR decline (PTX, 2.1 ml/min per 1.73 m2; control, 6.5 ml/min per 1.73/m2; P<0.001) |
| Navarro et al. (74) | 6 mo | DM (type not stated) with creatinine clearance <35 ml/min | PTX versus standard Rx | 24 | PTX 400 mg/d | No | Decrease in UPE (PTX, 59% reduction, P<0.05; control, P=NS) |
| Navarro et al. (75) | 4 mo | Type 2 DM with proteinuria (<3 g/d) | PTX and ACEi or ARB versus ACEi or ARB | 45 | PTX 1200 mg/d | No | Decrease in UPE (PTX, 15% reduction, P<0.001; control, 0.5% reduction, P=NS) |
| Navarro et al. (76) | 4 mo | Type 2 DM; UAE >300 mg/24 h, normal renal function | PTX and ARB versus ARB | 61 | PTX 1200 mg/d | No | Decrease in UAE (PTX, 17% reduction; control, 6% reduction, P<0.001) |
| Oliaei et al. (77) | 3 mo | Type 2 DM; proteinuria >500 mg/d | PTX+ACEi or ARB versus ACEi or ARB | 56 | PTX 1200 mg/d | Yes | Decrease in proteinuria (PTX, 61% reduction; placebo, 20% reduction, P<0.001) |
| Rodríguez-Morán et al. (78) | 6 mo | Type 2 DM; UAE 20–200 mcg/min; no RAAS blockers | PTX versus captopril | 130 | PTX 1200 mg/d | No | Equivalent decrease in UAE (PTX, 77% reduction; captopril, 76% reduction; P=NS) |
| Rodriguez-Morán et al. (79) | 16 wk | Type 2 DM; UAE 200–200 mcg/min; no RAAS blockers | PTX versus placebo | 40 | PTX 1200 mg/d | Yes | Decreased UAE (PTX, 74% reduction, P=0.02; placebo, 7% reduction, P=NS) |
| Roozbeh et al. (80) | 6 mo | Type 2 DM; UPE >500 mg/d | PTX+captopril versus captopril | 70 | PTX 1200 mg/d | No | Decrease in UPE (PTX, 56% reduction; placebo, 28% reduction; P=0.007) |
| Shahidi et al. (81) | 6 mo | Type 2 DM with microalbuminuria; eGFR >60 ml/min per 1.73 m2 | PTX versus placebo | 40 | PTX 1200 mg/d | Yes | No difference in UACR, BP, or eGFR (PTX, 2% reduction in UACR; placebo, 1% increase in UACR; P=NS) |
| Solerte et al. (82) | 12 mo | Type 1 DM; UPE >500 mg/d | PTX versus conventional Rx | 21 | PTX 1200 mg/d | No | Decrease in UPE (PTX, 47% reduction, P<0.01; conventional, 42% reduction, P<0.01); increase in creatinine clearance (PTX, 20% increase, P<0.01; conventional, 14% increase, P<0.01) |
DM, diabetes mellitus; UPE, urine protein excretion; PTX, pentoxifylline; RAAS, renin-angiotensin-aldosterone system; UACR, urinary albumin-to-creatinine ratio; UAE, urine albumin excretion; ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; Rx, prescription.
The Veterans Affairs Cooperative study Pentoxifylline in DKD (PTXRx; NCT03625648) is comparing PTX to placebo in patients with type 2 DM and eGFR of 15–60 ml/min per 1.73 m2, targeting high-risk patients according to the “heat map” of the Kidney Disease Improving Global Outcomes (83). Patients will need to have an eGFR of 15 to <30 ml/min per 1.73 m2, or an eGFR of 30 to <45 ml/min per 1.73 m2 with UACR >30 mg/g, or eGFR 45 to <60 ml/min per 1.73 m2 with UACR >300 mg/g. The primary outcome is time to ESKD or all-cause mortality. The study plans to randomize 2510 patients, began enrolling in November 2019, and is predicted to be completed by 2030.
PTX: Meta-Analyses.
An early meta-analysis published in 2008 suggested that decreased production of proinflammatory cytokines was the most likely explanation for the antiproteinuric action of PTX in patients with DKD (84). In a Cochrane meta-analysis of the renoprotective effect of PTX when used in combination with RAAS inhibitors (angiotensin-converting enzyme inhibitors/angiotensin receptor blockers) published in 2012 (85), PTX reduced albuminuria and proteinuria, with no obvious serious adverse effects in patients with DKD. However, most included studies were poorly reported, small, and methodologically flawed. Since the Cochrane analysis there have been several other meta-analyses published. Tian et al. (86) reported eight studies with a total of 587 patients (all diabetic), in which PTX was combined with RAAS blockers. Addition of PTX resulted in further reductions in albuminuria, proteinuria, and urinary TNF-α, but did not result in significant changes in glycated hemoglobin (hemoglobin A1c), serum creatinine, creatinine clearance, systolic BP, or diastolic BP. Jiang et al. (87) reported 12 trials with 613 participants (most included only patients with diabetes). PTX significantly decreased proteinuria compared with the placebo or no-treatment groups and led to a lesser decline of eGFR. There were no significant differences in BP or adverse events. Most of the included studies were small and of short duration, with the exception of the PREDIAN trial. Meta-analyses by Leporini et al. (88) and Liu et al. (89) also concluded that there is evidence for some renoprotective effects of PTX but no conclusive data proving the usefulness of this agent for improving renal outcomes in CKD. Moreover, meta-analyses of small trials are insufficient to guide therapy because they tend to overestimate treatment effects compared to large trials, partly due to publication bias.
Conclusions
Although there is much evidence that inflammation is important in the progression of DKD, there are no large clinical trials showing benefit of anti-inflammatory therapies. The current literature suggests that PTX may have therapeutic benefits in addition to RAAS blockade in DKD. PTX could be beneficial in patients unable to tolerate RAAS blockade or in those with very advanced CKD in whom RAAS blockade may carry increased risk. The available evidence thus suggests the possibility of the use of PTX as a valuable repurposing of an old drug in the treatment of DKD. However, a large-scale, multicenter, randomized clinical trial is needed to determine whether this agent can reduce hard end points such as ESKD and death. Such a trial is currently being conducted (PTXRx; www.clinicaltrials.gov, NCT03625648), but the results will not be available for several years. At this time, the combination of RAAS blockade plus SGLT2 inhibition is considered standard of care for patients with type 2 DM and CKD (eGFR 30 to ≤60 ml/min per 1.73 m2 or UACR >30 mg/g, particularly >300 mg/g) to prevent progression of CKD and adverse cardiovascular outcomes (90). It may be reasonable for clinicians to consider addition of PTX in patients with type 2 DM whose CKD continues to progress despite optimization of current standard-of-care therapies.
Disclosures
D. Leehey has nothing to disclose.
Funding
None.
Acknowledgments
The author would like to thank Holly J. Kramer for her review of the manuscript.
Author Contributions
D. Leehey wrote the original draft of the manuscript, reviewed and edited the manuscript, and was responsible for conceptualization, project administration, resources, and software.
References
- 1.Gregg EW, Li Y, Wang J, Burrows NR, Ali MK, Rolka D, Williams DE, Geiss L: Changes in diabetes-related complications in the United States, 1990-2010. N Engl J Med 370: 1514–1523, 2014 [DOI] [PubMed] [Google Scholar]
- 2.Alsaad KO, Herzenberg AM: Distinguishing diabetic nephropathy from other causes of glomerulosclerosis: An update. J Clin Pathol 60: 18–26, 2007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gnudi L, Gentile G, Ruggenenti P: Oxford Textbook of Clinical Nephrology, Vol. 2, 4th Ed., Oxford, UK, Oxford University Press, 2016, pp 1199–1247 [Google Scholar]
- 4.Cravedi P, Remuzzi G: Pathophysiology of proteinuria and its value as an outcome measure in chronic kidney disease. Br J Clin Pharmacol 76: 516–523, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rossing K, Christensen PK, Hovind P, Tarnow L, Rossing P, Parving HH: Progression of nephropathy in type 2 diabetic patients. Kidney Int 66: 1596–1605, 2004 [DOI] [PubMed] [Google Scholar]
- 6.Kawabata N, Kawamura T, Utsunomiya K, Kusano E: High salt intake is associated with renal involvement in Japanese patients with type 2 diabetes mellitus. Intern Med 54: 311–317, 2015 [DOI] [PubMed] [Google Scholar]
- 7.Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M: Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 339: 229–234, 1998 [DOI] [PubMed] [Google Scholar]
- 8.Afkarian M, Sachs MC, Kestenbaum B, Hirsch IB, Tuttle KR, Himmelfarb J, de Boer IH: Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol 24: 302–308, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.American Diabetes Association : 11. Microvascular complications and foot care: Standards of medical care in diabetes-2019. Diabetes Care 42[Suppl 1]: S124–S138, 2019 [DOI] [PubMed] [Google Scholar]
- 10.Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S; RENAAL Study Investigators: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 [DOI] [PubMed] [Google Scholar]
- 11.Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I; Collaborative Study Group: Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860, 2001 [DOI] [PubMed] [Google Scholar]
- 12.Fried LF, Emanuele N, Zhang JH, Brophy M, Conner TA, Duckworth W, Leehey DJ, McCullough PA, O’Connor T, Palevsky PM, Reilly RF, Seliger SL, Warren SR, Watnick S, Peduzzi P, Guarino P; VA NEPHRON-D Investigators: Combined angiotensin inhibition for the treatment of diabetic nephropathy [published correction appears in N Engl J Med 158: A7255, 2014]. N Engl J Med 369: 1892–1903, 2013 [DOI] [PubMed] [Google Scholar]
- 13.Tuttle KR, Lakshmanan MC, Rayner B, Busch RS, Zimmermann AG, Woodward DB, Botros FT: Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol 6: 605–617, 2018 [DOI] [PubMed] [Google Scholar]
- 14.Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW; CREDENCE Trial Investigators: Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 380: 2295–2306, 2019 [DOI] [PubMed] [Google Scholar]
- 15.Kramer HJ, Nguyen QD, Curhan G, Hsu CY: Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. JAMA 289: 3273–3277, 2003 [DOI] [PubMed] [Google Scholar]
- 16.Pugliese G, Penno G, Natali A, Barutta F, Di Paolo S, Reboldi G, Gesualdo L, De Nicola L; Italian Diabetes Society and the Italian Society of Nephrology: Diabetic kidney disease: New clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on “The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function”. Nutr Metab Cardiovasc Dis 29: 1127–1150, 2019 [DOI] [PubMed] [Google Scholar]
- 17.Neuen BL, Ohkuma T, Neal B, Matthews DR, de Zeeuw D, Mahaffey KW, Fulcher G, Li Q, Jardine M, Oh R, Heerspink HL, Perkovic V: Effect of canagliflozin on renal and cardiovascular outcomes across different levels of albuminuria: Data from the CANVAS program. J Am Soc Nephrol 30: 2229–2242, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Menne J, Dumann E, Haller H, Schmidt BMW: Acute kidney injury and adverse renal events in patients receiving SGLT2-inhibitors: A systematic review and meta-analysis. PLoS Med 16: e1002983, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Neuen BL, Young T, Heerspink HJL, Neal B, Perkovic V, Billot L, Mahaffey KW, Charytan DM, Wheeler DC, Arnott C, Bompoint S, Levin A, Jardine MJ: SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: A systematic review and meta-analysis. Lancet Diabetes Endocrinol 7: 845–854, 2019 [DOI] [PubMed] [Google Scholar]
- 20.Hasegawa G, Nakano K, Sawada M, Uno K, Shibayama Y, Ienaga K, Kondo M: Possible role of tumor necrosis factor and interleukin-1 in the development of diabetic nephropathy. Kidney Int 40: 1007–1012, 1991 [DOI] [PubMed] [Google Scholar]
- 21.Matoba K, Takeda Y, Nagai Y, Kawanami D, Utsunomiya K, Nishimura R: Unraveling the Role of inflammation in the pathogenesis of diabetic kidney disease. Int J Mol Sci 20: E3393, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nguyen D, Ping F, Mu W, Hill P, Atkins RC, Chadban SJ: Macrophage accumulation in human progressive diabetic nephropathy. Nephrology (Carlton) 11: 226–231, 2006 [DOI] [PubMed] [Google Scholar]
- 23.Alexandraki K, Piperi C, Kalofoutis C, Singh J, Alaveras A, Kalofoutis A: Inflammatory process in type 2 diabetes: The role of cytokines. Ann N Y Acad Sci 1084: 89–117, 2006 [DOI] [PubMed] [Google Scholar]
- 24.Katsuki A, Sumida Y, Murashima S, Murata K, Takarada Y, Ito K, Fujii M, Tsuchihashi K, Goto H, Nakatani K, Yano Y: Serum levels of tumor necrosis factor-alpha are increased in obese patients with noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab 83: 859–862, 1998 [DOI] [PubMed] [Google Scholar]
- 25.Pickup JC, Chusney GD, Thomas SM, Burt D: Plasma interleukin-6, tumour necrosis factor alpha and blood cytokine production in type 2 diabetes. Life Sci 67: 291–300, 2000 [DOI] [PubMed] [Google Scholar]
- 26.Festa A, D’Agostino R, Howard G, Mykkänen L, Tracy RP, Haffner SM: Inflammation and microalbuminuria in nondiabetic and type 2 diabetic subjects: The Insulin Resistance Atherosclerosis Study. Kidney Int 58: 1703–1710, 2000 [DOI] [PubMed] [Google Scholar]
- 27.Bruno G, Merletti F, Biggeri A, Bargero G, Ferrero S, Pagano G, Cavallo Perin P; Casale Monferrato Study: Progression to overt nephropathy in type 2 diabetes: The casale monferrato study. Diabetes Care 26: 2150–2155, 2003 [DOI] [PubMed] [Google Scholar]
- 28.Elmarakby AA, Sullivan JC: Relationship between oxidative stress and inflammatory cytokines in diabetic nephropathy. Cardiovasc Ther 30: 49–59, 2012 [DOI] [PubMed] [Google Scholar]
- 29.Mora C, Navarro JF: Inflammation and diabetic nephropathy. Curr Diab Rep 6: 463–468, 2006 [DOI] [PubMed] [Google Scholar]
- 30.Navarro JF, Mora C, Maca M, Garca J: Inflammatory parameters are independently associated with urinary albumin in type 2 diabetes mellitus. Am J Kidney Dis 42: 53–61, 2003 [DOI] [PubMed] [Google Scholar]
- 31.Chen YL, Qiao YC, Xu Y, Ling W, Pan YH, Huang YC, Geng LJ, Zhao HL, Zhang XX: Serum TNF-α concentrations in type 2 diabetes mellitus patients and diabetic nephropathy patients: A systematic review and meta-analysis. Immunol Lett 186: 52–58, 2017 [DOI] [PubMed] [Google Scholar]
- 32.Ortiz A, Bustos C, Alonso J, Alcázar R, López-Armada MJ, Plaza JJ, González E, Egido J: Involvement of tumor necrosis factor-alpha in the pathogenesis of experimental and human glomerulonephritis. Adv Nephrol Necker Hosp 24: 53–77, 1995 [PubMed] [Google Scholar]
- 33.McCarthy ET, Sharma R, Sharma M, Li JZ, Ge XL, Dileepan KN, Savin VJ: TNF-alpha increases albumin permeability of isolated rat glomeruli through the generation of superoxide. J Am Soc Nephrol 9: 433–438, 1998 [DOI] [PubMed] [Google Scholar]
- 34.Kalantarinia K, Awad AS, Siragy HM: Urinary and renal interstitial concentrations of TNF-alpha increase prior to the rise in albuminuria in diabetic rats. Kidney Int 64: 1208–1213, 2003 [DOI] [PubMed] [Google Scholar]
- 35.Moriwaki Y, Inokuchi T, Yamamoto A, Ka T, Tsutsumi Z, Takahashi S, Yamamoto T: Effect of TNF-alpha inhibition on urinary albumin excretion in experimental diabetic rats. Acta Diabetol 44: 215–218, 2007 [DOI] [PubMed] [Google Scholar]
- 36.Suzuki D, Miyazaki M, Naka R, Koji T, Yagame M, Jinde K, Endoh M, Nomoto Y, Sakai H: In situ hybridization of interleukin 6 in diabetic nephropathy. Diabetes 44: 1233–1238, 1995 [DOI] [PubMed] [Google Scholar]
- 37.Dalla Vestra M, Mussap M, Gallina P, Bruseghin M, Cernigoi AM, Saller A, Plebani M, Fioretto P: Acute-phase markers of inflammation and glomerular structure in patients with type 2 diabetes. J Am Soc Nephrol 16[Suppl 1]: S78–S82, 2005 [DOI] [PubMed] [Google Scholar]
- 38.Navarro JF, Milena FJ, Mora C, León C, García J: Renal pro-inflammatory cytokine gene expression in diabetic nephropathy: Effect of angiotensin-converting enzyme inhibition and pentoxifylline administration. Am J Nephrol 26: 562–570, 2006 [DOI] [PubMed] [Google Scholar]
- 39.DiPetrillo K, Coutermarsh B, Gesek FA: Urinary tumor necrosis factor contributes to sodium retention and renal hypertrophy during diabetes. Am J Physiol Renal Physiol 284: F113–F121, 2003 [DOI] [PubMed] [Google Scholar]
- 40.Navarro-González JF, Mora-Fernández C: The role of inflammatory cytokines in diabetic nephropathy. J Am Soc Nephrol 19: 433–442, 2008 [DOI] [PubMed] [Google Scholar]
- 41.Hayaishi-Okano R, Yamasaki Y, Katakami N, Ohtoshi K, Gorogawa S, Kuroda A, Matsuhisa M, Kosugi K, Nishikawa N, Kajimoto Y, Hori M: Elevated C-reactive protein associates with early-stage carotid atherosclerosis in young subjects with type 1 diabetes. Diabetes Care 25: 1432–1438, 2002 [DOI] [PubMed] [Google Scholar]
- 42.Navarro JF, Mora C: Role of inflammation in diabetic complications. Nephrol Dial Transplant 20: 2601–2604, 2005 [DOI] [PubMed] [Google Scholar]
- 43.Donate-Correa J, Tagua VG, Ferri C, Martín-Núñez E, Hernández-Carballo C, Ureña-Torres P, Ruiz-Ortega M, Ortiz A, Mora-Fernández C, Navarro-González JF: Pentoxifylline for renal protection in diabetic kidney disease. A model of old drugs for new horizons. J Clin Med 8: E287, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ruiz S, Pergola PE, Zager RA, Vaziri ND: Targeting the transcription factor Nrf2 to ameliorate oxidative stress and inflammation in chronic kidney disease. Kidney Int 83: 1029–1041, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.de Zeeuw D, Akizawa T, Audhya P, Bakris GL, Chin M, Christ-Schmidt H, Goldsberry A, Houser M, Krauth M, Lambers Heerspink HJ, McMurray JJ, Meyer CJ, Parving HH, Remuzzi G, Toto RD, Vaziri ND, Wanner C, Wittes J, Wrolstad D, Chertow GM; BEACON Trial Investigators: Bardoxolone methyl in type 2 diabetes and stage 4 chronic kidney disease. N Engl J Med 369: 2492–2503, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chin MP, Bakris GL, Block GA, Chertow GM, Goldsberry A, Inker LA, Heerspink HJL, O’Grady M, Pergola PE, Wanner C, Warnock DG, Meyer CJ: Bardoxolone methyl improves kidney function in patients with chronic kidney disease stage 4 and type 2 diabetes: Post-hoc analyses from bardoxolone methyl evaluation in patients with chronic kidney disease and type 2 diabetes study. Am J Nephrol 47: 40–47, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Tesch GH, Ma FY, Han Y, Liles JT, Breckenridge DG, Nikolic-Paterson DJ: ASK1 inhibitor halts progression of diabetic nephropathy in nos3-deficient mice. Diabetes 64: 3903–3913, 2015 [DOI] [PubMed] [Google Scholar]
- 48.Chertow GM, Pergola PE, Chen F, Kirby BJ, Sundy JS, Patel UD; GS-US-223-1015 Investigators: Effects of selonsertib in patients with diabetic kidney disease. J Am Soc Nephrol 30: 1980–1990, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.US Food and Drug Administration : Drugs@FDA: FDA-approved drugs, 2018. Available at: https://www.accessdata.fda.gov/scripts/cder/daf/. Accessed March 6, 2020
- 50.Bhanot S, Leehey DJ: Pentoxifylline for diabetic nephropathy: An important opportunity to re-purpose an old drug? Curr Hypertens Rep 18: 8, 2016 [DOI] [PubMed] [Google Scholar]
- 51.Aviado DM, Porter JM: Pentoxifylline: A new drug for the treatment of intermittent claudication. Mechanism of action, pharmacokinetics, clinical efficacy and adverse effects. Pharmacotherapy 4: 297–307, 1984 [DOI] [PubMed] [Google Scholar]
- 52.Rodríguez-Morán M, Guerrero-Romero F: Efficacy of pentoxifylline in the management of microalbuminuria in patients with diabetes. Curr Diabetes Rev 4: 55–62, 2008 [DOI] [PubMed] [Google Scholar]
- 53.Strutz F, Heeg M, Kochsiek T, Siemers G, Zeisberg M, Müller GA: Effects of pentoxifylline, pentifylline and gamma-interferon on proliferation, differentiation, and matrix synthesis of human renal fibroblasts. Nephrol Dial Transplant 15: 1535–1546, 2000 [DOI] [PubMed] [Google Scholar]
- 54.Han KH, Han SY, Kim HS, Kang YS, Cha DR: Prolonged administration enhances the renoprotective effect of pentoxifylline via anti-inflammatory activity in streptozotocin-induced diabetic nephropathy. Inflammation 33: 137–143, 2010 [DOI] [PubMed] [Google Scholar]
- 55.Sun HK, Lee YM, Han KH, Kim HS, Ahn SH, Han SY: Phosphodiesterase inhibitor improves renal tubulointerstitial hypoxia of the diabetic rat kidney. Korean J Intern Med (Korean Assoc Intern Med) 27: 163–170, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Badri S, Dashti-Khavidaki S, Lessan-Pezeshki M, Abdollahi M: A review of the potential benefits of pentoxifylline in diabetic and non-diabetic proteinuria. J Pharm Pharm Sci 14: 128–137, 2011 [DOI] [PubMed] [Google Scholar]
- 57.An ZM, Dong XG, Guo Y, Zhou JL, Qin T: Effects and clinical significance of pentoxifylline on the oxidative stress of rats with diabetic nephropathy. J Huazhong Univ Sci Technolog Med Sci 35: 356–361, 2015 [DOI] [PubMed] [Google Scholar]
- 58.Dávila-Esqueda ME, Martínez-Morales F: Pentoxifylline diminishes the oxidative damage to renal tissue induced by streptozotocin in the rat. Exp Diabesity Res 5: 245–251, 2004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Garcia FA, Rebouças JF, Balbino TQ, da Silva TG, de Carvalho-Júnior CH, Cerqueira GS, Brito GA, Viana GS: Pentoxifylline reduces the inflammatory process in diabetic rats: Relationship with decreases of pro-inflammatory cytokines and inducible nitric oxide synthase. J Inflamm (Lond) 12: 33, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Schmidt AM, Yan SD, Wautier JL, Stern D: Activation of receptor for advanced glycation end products: A mechanism for chronic vascular dysfunction in diabetic vasculopathy and atherosclerosis. Circ Res 84: 489–497, 1999 [DOI] [PubMed] [Google Scholar]
- 61.Matsumura Y, Aizawa H, Shiraki-Iida T, Nagai R, Kuro-o M, Nabeshima Y: Identification of the human klotho gene and its two transcripts encoding membrane and secreted klotho protein. Biochem Biophys Res Commun 242: 626–630, 1998 [DOI] [PubMed] [Google Scholar]
- 62.Asai O, Nakatani K, Tanaka T, Sakan H, Imura A, Yoshimoto S, Samejima K, Yamaguchi Y, Matsui M, Akai Y, Konishi N, Iwano M, Nabeshima Y, Saito Y: Decreased renal α-Klotho expression in early diabetic nephropathy in humans and mice and its possible role in urinary calcium excretion. Kidney Int 81: 539–547, 2012 [DOI] [PubMed] [Google Scholar]
- 63.Kim SS, Song SH, Kim IJ, Lee EY, Lee SM, Chung CH, Kwak IS, Lee EK, Kim YK: Decreased plasma α-Klotho predict progression of nephropathy with type 2 diabetic patients. J Diabetes Complications 30: 887–892, 2016 [DOI] [PubMed] [Google Scholar]
- 64.Moreno JA, Izquierdo MC, Sanchez-Niño MD, Suárez-Alvarez B, Lopez-Larrea C, Jakubowski A, Blanco J, Ramirez R, Selgas R, Ruiz-Ortega M, Egido J, Ortiz A, Sanz AB: The inflammatory cytokines TWEAK and TNFα reduce renal klotho expression through NFκB. J Am Soc Nephrol 22: 1315–1325, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Zhao Y, Banerjee S, Dey N, LeJeune WS, Sarkar PS, Brobey R, Rosenblatt KP, Tilton RG, Choudhary S: Klotho depletion contributes to increased inflammation in kidney of the db/db mouse model of diabetes via RelA (serine)536 phosphorylation. Diabetes 60: 1907–1916, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Maekawa Y, Ishikawa K, Yasuda O, Oguro R, Hanasaki H, Kida I, Takemura Y, Ohishi M, Katsuya T, Rakugi H: Klotho suppresses TNF-alpha-induced expression of adhesion molecules in the endothelium and attenuates NF-kappaB activation. Endocrine 35: 341–346, 2009 [DOI] [PubMed] [Google Scholar]
- 67.Navarro-González JF, Sánchez-Niño MD, Donate-Correa J, Martín-Núñez E, Ferri C, Pérez-Delgado N, Górriz JL, Martínez-Castelao A, Ortiz A, Mora-Fernández C: Effects of pentoxifylline on soluble klotho concentrations and renal tubular cell expression in diabetic kidney disease. Diabetes Care 41: 1817–1820, 2018 [DOI] [PubMed] [Google Scholar]
- 68.Aminorroaya A, Janghorbani M, Rezvanian H, Aminian T, Gharavi M, Amini M: Comparison of the effect of pentoxifylline and captopril on proteinuria in patients with type 2 diabetes mellitus. Nephron Clin Pract 99: c73–c77, 2005 [DOI] [PubMed] [Google Scholar]
- 69.Ghorbani A, Omidvar B, Beladi-Mousavi SS, Lak E, Vaziri S: The effect of pentoxifylline on reduction of proteinuria among patients with type 2 diabetes under blockade of angiotensin system: A double blind and randomized clinical trial. Nefrologia 32: 790–796, 2012 [DOI] [PubMed] [Google Scholar]
- 70.Guerrero-Romero F, Rodríguez-Morán M, Paniagua-Sierra JR, García-Bulnes G, Salas-Ramírez M, Amato D: Pentoxifylline reduces proteinuria in insulin-dependent and non insulin-dependent diabetic patients. Clin Nephrol 43: 116–121, 1995 [PubMed] [Google Scholar]
- 71.Han SJ, Kim HJ, Kim DJ, Sheen SS, Chung CH, Ahn CW, Kim SH, Cho YW, Park SW, Kim SK, Kim CS, Kim KW, Lee KW: Effects of pentoxifylline on proteinuria and glucose control in patients with type 2 diabetes: A prospective randomized double-blind multicenter study. Diabetol Metab Syndr 7: 64, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Harmankaya O, Seber S, Yilmaz M: Combination of pentoxifylline with angiotensin converting enzyme inhibitors produces an additional reduction in microalbuminuria in hypertensive type 2 diabetic patients. Ren Fail 25: 465–470, 2003 [DOI] [PubMed] [Google Scholar]
- 73.Navarro-González JF, Mora-Fernández C, Muros de Fuentes M, Chahin J, Méndez ML, Gallego E, Macía M, del Castillo N, Rivero A, Getino MA, García P, Jarque A, García J: Effect of pentoxifylline on renal function and urinary albumin excretion in patients with diabetic kidney disease: The PREDIAN trial. J Am Soc Nephrol 26: 220–229, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Navarro JF, Mora C: Antiproteinuric effect of pentoxifylline in patients with diabetic nephropathy. Diabetes Care 22: 1006–1008, 1999 [DOI] [PubMed] [Google Scholar]
- 75.Navarro JF, Mora C, Muros M, Maca M, Garca J: Effects of pentoxifylline administration on urinary N-acetyl-beta-glucosaminidase excretion in type 2 diabetic patients: A short-term, prospective, randomized study. Am J Kidney Dis 42: 264–270, 2003 [DOI] [PubMed] [Google Scholar]
- 76.Navarro JF, Mora C, Muros M, García J: Additive antiproteinuric effect of pentoxifylline in patients with type 2 diabetes under angiotensin II receptor blockade: A short-term, randomized, controlled trial. J Am Soc Nephrol 16: 2119–2126, 2005 [DOI] [PubMed] [Google Scholar]
- 77.Oliaei F, Hushmand S, Khafri S, Baradaran M: Efficacy of pentoxifylline for reduction of proteinuria in type II diabetic patients. Caspian J Intern Med 2: 309–313, 2011 [PMC free article] [PubMed] [Google Scholar]
- 78.Rodríguez-Morán M, Guerrero-Romero F: Pentoxifylline is as effective as captopril in the reduction of microalbuminuria in non-hypertensive type 2 diabetic patients--a randomized, equivalent trial. Clin Nephrol 64: 91–97, 2005 [DOI] [PubMed] [Google Scholar]
- 79.Rodriguez-Morán M, González-González G, Bermúdez-Barba MV, Medina de la Garza CE, Tamez-Pérez HE, Martínez-Martínez FJ, Guerrero-Romero F: Effects of pentoxifylline on the urinary protein excretion profile of type 2 diabetic patients with microproteinuria: A double-blind, placebo-controlled randomized trial. Clin Nephrol 66: 3–10, 2006 [DOI] [PubMed] [Google Scholar]
- 80.Roozbeh J, Banihashemi MA, Ghezlou M, Afshariani R, Salari S, Moini M, Sagheb MM: Captopril and combination therapy of captopril and pentoxifylline in reducing proteinuria in diabetic nephropathy. Ren Fail 32: 172–178, 2010 [DOI] [PubMed] [Google Scholar]
- 81.Shahidi S, Hoseinbalam M, Iraj B, Akbari M: Effect of pentoxifylline on microalbuminuria in diabetic patients: A randomized controlled trial. Int J Nephrol 2015: 259592, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Solerte SB, Fioravanti M, Patti AL, Schifino N, Zanoletti MG, Inglese V, Ferrari E: Pentoxifylline, total urinary protein excretion rate and arterial blood pressure in long-term insulin-dependent diabetic patients with overt nephropathy. Acta Diabetol Lat 24: 229–239, 1987 [DOI] [PubMed] [Google Scholar]
- 83.Levey AS, de Jong PE, Coresh J, El Nahas M, Astor BC, Matsushita K, Gansevoort RT, Kasiske BL, Eckardt KU: The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int 80: 17–28, 2011 [DOI] [PubMed] [Google Scholar]
- 84.McCormick BB, Sydor A, Akbari A, Fergusson D, Doucette S, Knoll G: The effect of pentoxifylline on proteinuria in diabetic kidney disease: A meta-analysis. Am J Kidney Dis 52: 454–463, 2008 [DOI] [PubMed] [Google Scholar]
- 85.Shan D, Wu HM, Yuan QY, Li J, Zhou RL, Liu GJ: Pentoxifylline for diabetic kidney disease. Cochrane Database Syst Rev 2: CD006800, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Tian ML, Shen Y, Sun ZL, Zha Y: Efficacy and safety of combining pentoxifylline with angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker in diabetic nephropathy: A meta-analysis. Int Urol Nephrol 47: 815–822, 2015 [DOI] [PubMed] [Google Scholar]
- 87.Jiang X, Zhou S, Yao J, Kong X, Cui M: Effect of pentoxifylline in proteinuric chronic kidney disease: A systematic review and meta-analysis. J Nephrol 29: 653–662, 2016 [DOI] [PubMed] [Google Scholar]
- 88.Leporini C, Pisano A, Russo E, D Arrigo G, de Sarro G, Coppolino G, Bolignano D: Effect of pentoxifylline on renal outcomes in chronic kidney disease patients: A systematic review and meta-analysis. Pharmacol Res 107: 315–332, 2016 [DOI] [PubMed] [Google Scholar]
- 89.Liu D, Wang LN, Li HX, Huang P, Qu LB, Chen FY: Pentoxifylline plus ACEIs/ARBs for proteinuria and kidney function in chronic kidney disease: A meta-analysis. J Int Med Res 45: 383–398, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, D’Alessio DA, Davies MJ: 2019 update to: Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 43: 487–493, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]