

Abstract
Background
The oral, selective Janus kinase 1/2 inhibitor baricitinib has shown efficacy in studies of hospitalised adults with COVID-19. COV-BARRIER (NCT04421027) was a multinational, phase 3, randomised, double-blind, placebo-controlled trial of baricitinib in patients with confirmed SARS-CoV-2 infection. We aimed to evaluate the efficacy and safety of baricitinib plus standard of care in critically ill hospitalised adults with COVID-19 requiring invasive mechanical ventilation or extracorporeal membrane oxygenation.
Methods
This exploratory trial followed the study design of COV-BARRIER in a critically ill cohort not included in the main phase 3 trial. The study was conducted across 18 hospitals in Argentina, Brazil, Mexico, and the USA. Participants (aged ≥18 years) hospitalised with laboratory-confirmed SARS-CoV-2 infection on baseline invasive mechanical ventilation or extracorporeal membrane oxygenation were randomly assigned (1:1) to baricitinib (4 mg) or placebo once daily for up to 14 days in combination with standard of care. Participants, study staff, and investigators were masked to study group assignment. Prespecified endpoints included all-cause mortality through days 28 and 60, number of ventilator-free days, duration of hospitalisation, and time to recovery through day 28. The efficacy analysis was done in the intention-to-treat population and the safety analysis was done in the safety population. This trial is registered with ClinicalTrials.gov, NCT04421027.
Findings
Between Dec 23, 2020, and April 10, 2021, 101 participants were enrolled into the exploratory trial and assigned to baricitinib (n=51) or placebo (n=50) plus standard of care. Standard of care included baseline systemic corticosteroid use in 87 (86%) participants. Treatment with baricitinib significantly reduced 28-day all-cause mortality compared with placebo (20 [39%] of 51 participants died in the baricitinib group vs 29 [58%] of 50 in the placebo group; hazard ratio [HR] 0·54 [95% CI 0·31–0·96]; p=0·030; 46% relative reduction; absolute risk reduction 19%). A significant reduction in 60-day mortality was also observed in the baricitinib group compared with the placebo group (23 [45%] events vs 31 [62%]; HR 0·56 [95% CI 0·33–0·97]; p=0·027; 44% relative reduction; absolute risk reduction 17%). In every six baricitinib-treated participants, one additional death was prevented compared with placebo at days 28 and 60. The number of ventilator-free days did not differ significantly between treatment groups (mean 8·1 days [SD 10·2] in the baricitinib group vs 5·5 days [8·4] in the placebo group; p=0·21). The mean duration of hospitalisation in baricitinib-treated participants was not significantly shorter than in placebo-treated participants (23·7 days [SD 7·1] vs 26·1 days [3·9]; p=0·050). The rates of infections, blood clots, and adverse cardiovascular events were similar between treatment groups.
Interpretation
In critically ill hospitalised patients with COVID-19 who were receiving invasive mechanical ventilation or extracorporeal membrane oxygenation, treatment with baricitinib compared with placebo (in combination with standard of care, including corticosteroids) reduced mortality, which is consistent with the mortality reduction observed in less severely ill patients in the hospitalised primary COV-BARRIER study population. However, this was an exploratory trial with a relatively small sample size; therefore, further phase 3 trials are needed to confirm these findings.
Funding
Eli Lilly and Company.
Introduction
Patients who require hospitalisation due to infection with SARS-CoV-2 will often experience an intense hyperinflammatory state that can lead to multiple organ dysfunction, including acute respiratory distress syndrome, septic shock, and death.1, 2, 3, 4 There have been many treatment advances in therapeutics for patients hospitalised with COVID-19, such as remdesivir, dexamethasone, tocilizumab, and baricitinib.5, 6, 7, 8, 9, 10 Globally, however, there remains a crucial and urgent need to evaluate new treatment options to reduce mortality in hospitalised patients with COVID-19, because of the persisting high occurrence of deaths despite these improvements in standard of care. For example, WHO reports that there have been more than 5 535 000 COVID-19 deaths reported globally since the beginning of the SARS-CoV-2 pandemic in 2020.11 Mortality remains particularly high among critically ill patients who require invasive mechanical ventilation (IMV) or extracorporeal membrane oxygenation (ECMO), which are the primary means of treatment in patients with severe COVID-19, with an estimated case fatality rate of 45% in this population.12 In the platform RECOVERY trial,7 mortality was 29·3% in patients on IMV at baseline randomly assigned to dexamethasone versus 41·4% in those assigned to usual care (rate ratio [RR] 0·64 [95% CI 0·51−0·81], corresponding to a 36% relative reduction in mortality). Similarly, mortality was 49% in participants on IMV at baseline who were randomly assigned to tocilizumab versus 51% in those assigned to usual care (RR 0·93 [95% CI 0·74−1·18]; not significant, corresponding to a 7% relative reduction in mortality).8 Notably, in the tocilizumab study, benefits in mortality across the whole study population were only seen in those who had concomitant use of corticosteroids. Thus, interventions to reduce mortality in critically ill patients with COVID-19 remain a crucial unmet medical need.
Research in context.
Evidence before this study
To evaluate studies assessing the efficacy and safety of interventions in patients with COVID-19 requiring invasive mechanical ventilation (IMV), we searched PubMed using the terms “COVID-19”, “SARS-CoV-2”, “treatment”, “critical illness”, “invasive mechanical ventilation”, “baricitinib”, and “JAK inhibitor” for articles in English, published from Feb 1, 2020, to Dec 1, 2020, regardless of article type. We also reviewed the National Institutes of Health and Infectious Diseases Society of America COVID-19 guidelines and reviewed similar terms on ClinicalTrials.gov. At the time of implementation of this exploratory trial in a critically ill population following the COV-BARRIER study design, there had been only one open-label study of dexamethasone that showed mortality benefit in hospitalised patients with COVID-19 requiring IMV. Small studies of interleukin (IL)-6 inhibitors had shown no effect and larger trials were ongoing. Guidelines recommended use of dexamethasone with or without remdesivir and recommended against the use of IL-6 inhibitors, except in clinical trials. There were no reported double-blind, placebo-controlled, phase 3 trials that included corticosteroids as part of standard of care investigating the efficacy and safety of novel treatments in the National Institute of Allergy and Infectious Disease (NIAID) ordinal scale score 7 population (NIAID-OS 7; hospitalised and on IMV or extracorporeal membrane oxygenation [ECMO]).
Baricitinib's mechanism of action as a Janus kinase 1/2 inhibitor was identified as a potential intervention for the treatment of COVID-19, given its known anticytokine properties and potential antiviral mechanism of targeting host proteins that mediate viral endocytosis.
Data from the NIAID-funded ACTT-2 trial showed that baricitinib, when added to remdesivir, improved time to recovery and other outcomes, including mortality compared with placebo plus remdesivir. In participants requiring IMV (NIAID-OS 7) at baseline, there was no significant difference in the proportion of participants who had improvement in NIAID-OS at day 15 after receiving baricitinib plus remdesivir compared with those who received placebo plus remdesivir (odds ratio 1·7 [95% CI 0·8–3·4]). We designed COV-BARRIER, a phase 3, multinational, double-blind, randomised, placebo-controlled trial, to evaluate the efficacy and safety of baricitinib in combination with standard of care (including corticosteroids) for the treatment of hospitalised adults with COVID-19 who did not require mechanical ventilation (ie, NIAID-OS 4–6). There was a significant reduction in the prespecified secondary endpoint of mortality by day 28 in the baricitinib group compared with the placebo group (HR 0·57 [95% CI 0·41–0·78], corresponding to a 43% relative reduction; p=0·0018); one additional death was prevented per 20 baricitinib-treated participants. In the more severely ill NIAID-OS 6 subgroup, one additional death was prevented per nine baricitinib-treated participants (HR 0·52 [95% CI 0·33–0·80], corresponding to a 48% relative reduction; p=0·0065). We therefore implemented an exploratory study, which followed the COV-BARRIER trial design, to evaluate baricitinib in the critically ill NIAID-OS 7 population.
Added value of this study
This exploratory trial, though in a small sample, was the first randomised controlled trial to our knowledge to evaluate baricitinib in addition to the current standard of care, including antivirals, anticoagulants, and corticosteroids, in patients who were receiving IMV or ECMO at enrolment. This was a multinational, randomised, double-blind, placebo-controlled trial in regions with high COVID-19 hospitalisation rates. Treatment with baricitinib reduced 28-day all-cause mortality compared with placebo (HR 0·54 [95% CI 0·31–0·96]; p=0·030), corresponding to a 46% relative reduction and absolute reduction of 19%, and reduced 60-day all-cause mortality (0·56 [0·33–0·97]; p=0·027), corresponding to a 44% relative reduction and absolute reduction of 17%; overall, one additional death was prevented per six baricitinib-treated participants. No significant differences between groups were observed for number of ventilator-free days, duration of hospitalisation, and time to recovery. The frequencies of serious adverse events, serious infections, and venous thromboembolic events were similar between baricitinib and placebo groups, respectively.
The COV-BARRIER primary trial results plus these exploratory trial data in a smaller group of patients on mechanical ventilation or ECMO provide important information in the context of other large, phase 3, randomised trials in patients on invasive mechanical ventilation at baseline. The RECOVERY study reported mortality of 29·3% following treatment with dexamethasone compared with 41·4% for usual care (rate ratio of 0·64, corresponding to a 36% relative reduction) and 49% mortality in participants who received tocilizumab compared with 51% for usual care (0·93, corresponding to a 7% relative reduction). The ACTT-2 study reported 28-day mortality of 23·1% in the baricitinib plus remdesivir group and 22·6% in the placebo plus remdesivir group in this critically ill patient population; however, the primary outcome of ACTT-2 was time to recovery, and the study was not powered to detect a change in mortality.
Implications of all the available evidence
In this exploratory trial, baricitinib in addition to standard of care (which predominantly included corticosteroids) had a significant effect on all-cause mortality reduction at 28 days in critically ill hospitalised patients with COVID-19; an effect which was maintained at 60 days. These data were similar to those seen in the COV-BARRIER primary study population of hospitalised patients, which excluded patients who required IMV or ECMO at enrolment. These findings suggest that baricitinib has additional benefits when given in combination with other standard-of-care treatment modalities, including remdesivir and dexamethasone. On the basis of the available evidence, baricitinib might present a novel treatment option to decrease all-cause mortality in hospitalised, critically ill patients with COVID-19, even when started late in the disease process (ie, after steroids, mechanical ventilation, and ECMO have already been implemented). However, further phase 3 studies in this population are required to confirm these findings.
In February, 2020, baricitinib (a selective Janus kinase [JAK]1/JAK2 inhibitor)13, 14 was identified as a potential intervention for the treatment of COVID-19 by the artificial intelligence platform Benevolent AI, given its known anti-inflammatory profile in patients with autoimmune diseases15 and potential for targeting host proteins for its antiviral mechanism.16, 17 Several observational studies, in small cohorts of hospitalised patients with COVID-19 (including older patients), have provided evidence of clinical improvement associated with baricitinib treatment.18, 19, 20, 21, 22 Other medications of the JAK inhibitor class have also shown clinical benefit in treating COVID-19 when combined with standard of care in phase 2 and phase 3 studies.23, 24, 25
ACTT-2,6 a National Institute of Allergy and Infectious Disease (NIAID)-funded, multinational, double-blind, randomised, placebo-controlled, phase 3 trial in hospitalised adults with COVID-19, found that baricitinib plus remdesivir was superior to remdesivir in reducing time to recovery (RR for recovery 1·16 [95% CI 1·01–1·32]; p=0·03). 28-day mortality was 5·1% in participants treated with baricitinib plus remdesivir versus 7·8% in those who received placebo plus remdesivir (hazard ratio [HR] 0·65 [95% CI 0·39–1·09]); an endpoint for which the study was not powered. There were fewer serious adverse events in the participants who received baricitinib plus remdesivir than in those who received placebo plus remdesivir. In 111 participants enrolled with baseline use of IMV or ECMO, there were no significant differences in time to recovery, 28-day mortality, or other secondary outcomes between treatment groups.
COV-BARRIER10 was a phase 3, multinational, double-blind, randomised, placebo-controlled trial designed to evaluate the efficacy and safety of baricitinib in combination with standard of care, which could include corticosteroids, for the treatment of hospitalised adults with COVID-19 who did not require mechanical ventilation (ie, NIAID ordinal scale [NIAID-OS] score 4–6). Although there was no difference between groups in the primary endpoint of reduction of disease progression, a significant reduction in 28-day all-cause mortality was found between the baricitinib and placebo groups (HR 0·57 [95% CI 0·41–0·78]; p=0·0018), corresponding to a 43% relative reduction in the baricitinib group.10 In the more severely ill subgroup who required high-flow oxygen or non-invasive ventilation (NIAID-OS 6), the difference in 28-day all-cause mortality between baricitinib and placebo groups resulted in a HR of 0·52 (95% CI 0·33–0·80; p=0·0065), corresponding to a 48% relative reduction in the baricitinib group. The number needed to treat to prevent one additional death was nine patients in this more severely ill subgroup (NIAID-OS 6), compared with one death prevented per 20 baricitinib-treated participants in the overall primary COV-BARRIER study population (NIAID-OS 4–6).
The US Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the use of baricitinib to treat COVID-19 in hospitalised adults and paediatric patients aged 2 years or older requiring supplemental oxygen, non-invasive mechanical ventilation or IMV, or ECMO.26 The EUA was first issued in November, 2020, on the basis of ACTT-2 results and later updated in July, 2021, based on COV-BARRIER NIAID-OS 4–6 results. In October, 2020, the FDA requested further evaluation of baricitinib for the treatment of critically ill adult patients with COVID-19 requiring IMV or ECMO. We aimed to evaluate the efficacy and safety of baricitinib in combination with standard of care for the treatment of critically ill hospitalised adults with COVID-19 requiring IMV or ECMO.
Methods
Study design and participants
This exploratory trial followed the phase 3 COV-BARRIER study design in critically ill patients with baseline IMV or ECMO. In this multicentre, randomised, double-blind, placebo-controlled, parallel-group trial, participants were enrolled across 18 centres in four countries (Argentina, Brazil, Mexico, and the USA). A detailed description of the parent study design has been published previously.10
Eligible patients were those aged 18 years or older, who had been hospitalised with laboratory-confirmed SARS-CoV-2 infection, with use of IMV or ECMO at study entry and randomisation, evidence of pneumonia or clinical symptoms of COVID-19, and indicators of progression risk with at least one elevated inflammatory marker greater than the upper limit of normal range based on the local laboratory result (C-reactive protein, D-dimer, lactate dehydrogenase, or ferritin). Dexamethasone use was permitted as described in the RECOVERY trial,7 but patients were excluded if they were receiving high-dose corticosteroids (>20 mg per day [or prednisone equivalent] for ≥14 consecutive days in the month before study entry, unless indicated per standard of care for a concurrent condition, such as asthma, chronic obstructive pulmonary disease, or adrenal insufficiency), immunosuppressants, biologics, T-cell or B-cell-targeted therapies, interferon (IFN), or JAK inhibitors; had received convalescent plasma or intravenous immunoglobulin for COVID-19; or had suspected serious active bacterial, fungal, or other infection, or untreated tuberculosis infection.
COV-BARRIER was conducted in accordance with ethical principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The institutional review board or independent ethics committee at each study centre approved the study. All participants (or legally authorised representatives) provided written informed consent to participate.
Randomisation and masking
Participants who met all criteria for enrolment were randomly assigned (1:1) to receive baricitinib 4 mg or matched placebo, in combination with standard of care. Randomisation was facilitated by a computer-generated random sequence using an interactive web-response system and was performed by a study investigator or designee. Participants were stratified at randomisation according to geographical region (Europe, USA, or the rest of the world). Participants, study staff, and investigators were masked to the study group assignment. An independent, external data monitoring committee oversaw the study. An independent, masked, clinical event committee adjudicated potential venous thromboembolic events and deaths.
Procedures
Baricitinib 4 mg or matched placebo was crushed for nasogastric tube delivery (or given orally when feasible) and given once daily for up to 14 days or until discharge from hospital, whichever occurred first. Participants assigned to baricitinib with baseline estimated glomerular filtration rate (eGFR) of 30 to less than 60 mL/min per 1·73 m2 received baricitinib 2 mg or matched placebo. If eGFR decreased to 30 to less than 60 mL/min per 1·73 m2 after randomisation, patients received baricitinib 2 mg until eGFR returned to 60 mL/min per 1·73 m2 or greater.
All participants received standard of care in keeping with local clinical practice for COVID-19 management, which could include concomitant medications such as corticosteroids, antivirals, and other treatments, including vasopressors. Prophylaxis for venous thromboembolic events per local practice was required for all participants unless contraindicated. Use of renal replacement therapy was collected, as was National Early Warning Score (NEWS), a physiological score of illness severity in hospitalised patients.27 NEWS is determined from six parameters: respiration rate, oxygen saturation, temperature, systolic blood pressure, heart rate, and level of consciousness.
For efficacy and health outcomes, baseline measurements were defined as the last non-missing assessment recorded at or before the first study drug administration on day 1. Efficacy and safety were evaluated for all participants up to day 28; all-cause mortality was also evaluated up to day 60. Participants had a follow-up visit 28 days after receiving their last dose of study drug. Investigators evaluated and determined the intensity of the adverse event (mild, moderate, or severe) on the basis of their clinical assessment of the intensity of the event and criteria guidance as provided in the protocol.
Outcomes
The prespecified key endpoints for this exploratory trial were all-cause mortality at day 28 and day 60; number of ventilator-free days; overall improvement (assessed by odds of improvement in clinical status) on NIAID-OS, evaluated at days 4, 7, 10, 14, and 28; proportion of participants with at least 1-point improvement on the NIAID-OS or live discharge from hospital at days 4, 7, 10, 14, and 28; duration of hospitalisation; and time to recovery through day 28. As the cohort reported here was an addition to the parent trial study design, all endpoints are considered exploratory.
Statistical analysis
The sample size for this exploratory trial was approximately 50 participants per treatment group, which was selected to match the number of participants enrolled in the ACTT-2 study who required IMV or ECMO at baseline. This number was deemed a sufficient sample size to evaluate participants treated with baricitinib in addition to standard of care in a randomised controlled study in hospitalised adults receiving IMV or ECMO at baseline. No formal sample size calculation was done as this was an exploratory trial.
Efficacy was analysed in the intention-to-treat population, defined as all participants who were assigned to a treatment group. Participants who discontinued on the day of randomisation with no baseline or post-baseline NIAID-OS data were excluded. In participants who discontinued study participation due to transfer to another hospital, all available information was used to inform the mortality and safety analyses, including date of death when this was known to occur after transfer date. Log-rank test and HR from Cox proportional hazard model were used for time-to-event analyses. Logistic regression with the last-observation-carried-forward methodology was used for dichotomous endpoints, proportional odds model was used for ordinal endpoints, and analysis of variance model was used for continuous endpoints. These statistical models were adjusted for treatment group, baseline age group (<65 years vs ≥65 years), and geographical region (USA vs the rest of the world). Analysis of NIAID-OS outcomes at day 60 was performed using descriptive statistics on observed values. Safety analyses included all randomised participants who received at least one dose of study drug and who did not discontinue the study for the reason of lost to follow-up at the first post-baseline visit. Adverse events were inclusive of the 28-day treatment period. Statistical tests of treatment effects were performed at a two-sided significance level of 0·05, unless otherwise stated; p values were not adjusted for multiplicity. Statistical analyses were performed using SAS (version 9.4 or higher). This trial is registered with ClinicalTrials.gov, NCT04421027.
Role of the funding source
The funder of the study had a role in study design, data analysis, data interpretation, and writing of the report, but had no role in data collection.
Results
Between Dec 23, 2020, and April 10, 2021, 101 participants were enrolled into the exploratory trial and assigned to receive baricitinib (n=51) or placebo (n=50) plus standard of care. Two randomly assigned participants discontinued from the trial before dosing and 99 participants received at least one dose, of whom 46 (47%) completed the 28-day double-blind treatment period (figure 1 ). 52 (53%) of 99 participants discontinued during the treatment period; 46 (88%) of these 52 discontinuations were due to death. No randomly assigned participants were excluded from the intention-to-treat population, including the four participants who were discontinued from the trial after transfer to another hospital. The status of these participants was recorded during the follow-up visit at day 60 and included in the mortality and safety analyses.
Figure 1.
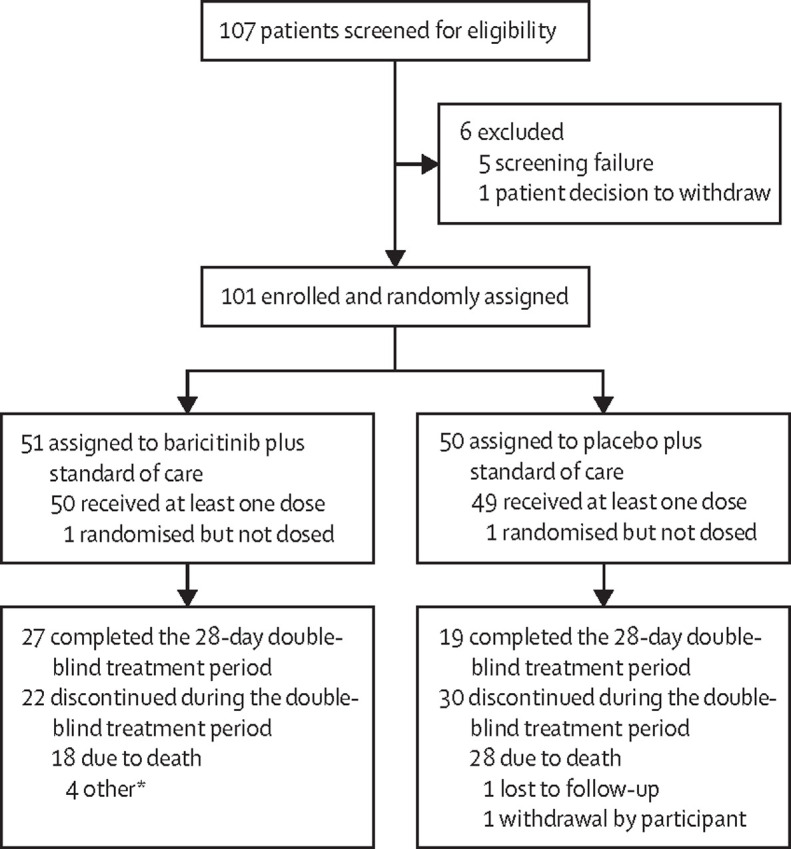
Trial profile
One participant in the baricitinib plus standard of care group did not have a recorded treatment period disposition form, so the treatment period disposition was missing. *Four participants discontinued from the trial after transfer to another hospital; they were included in the intention-to-treat population, with all available information used to inform the mortality and safety analyses. Specifically, three participants died after transfer and time of death was used in the mortality analysis. One participant was alive at follow-up and censored at the last available visit.
Baseline characteristics were balanced between treatment groups (table 1 ). The mean participant age was 58·6 years (SD 13·8); 55 (54%) of 101 participants were male and 46 (46%) were female. At baseline, 87 (86%) of 101 participants were receiving systemic corticosteroids and two (2%) were receiving remdesivir (table 1). All 101 (100%) participants had at least one pre-existing comorbidity of interest. Venous thromboembolic event prophylaxis was utilised as required; most participants (79 [78%] of 101) received enoxaparin. The median duration of treatment exposure was 12·0 days (IQR 5·0–14·0) in the placebo group and 11·0 days (7·0–14·0) in the baricitinib group. One (2%) of 50 participants in the placebo group and two (4%) of 51 in the baricitinib group were receiving ECMO at baseline. Any use of ECMO, including participants who received ECMO after baseline, was observed in two (4%) participants in the placebo group and three (6%) in the baricitinib group.
Table 1.
Baseline characteristics
| Baricitinib plus standard of care group (n=51) | Placebo plus standard of care group (n=50) | ||
|---|---|---|---|
| Age, years | 58·4 (12·4) | 58·8 (15·2) | |
| Sex | |||
| Male | 25 (49%) | 30 (60%) | |
| Female | 26 (51%) | 20 (40%) | |
| Race | |||
| American Indian or Alaska Native* | 15 (29%) | 17 (34%) | |
| Asian | 0 | 1 (2%) | |
| Black or African American | 1 (2%) | 1 (2%) | |
| Multiple | 2 (4%) | 0 | |
| White | 32 (63%) | 30 (60%) | |
| Missing | 1 (2%) | 1 (2%) | |
| Country | |||
| Argentina | 12 (24%) | 9 (18%) | |
| Brazil | 15 (29%) | 14 (28%) | |
| Mexico | 14 (27%) | 17 (34%) | |
| USA | 10 (20%) | 10 (20%) | |
| Body-mass index, kg/m2 | 34·3 (7·8) | 32·1 (6·3) | |
| Duration of symptoms before enrolment | |||
| <7 days | 2 (4%) | 4 (8%) | |
| ≥7 days | 49 (96%) | 44 (88%) | |
| Missing | 0 | 2 (4%) | |
| Duration of hospitalisation before randomisation, days | 4 (2–7) | 4 (2–7) | |
| Key concomitant medications at baseline | |||
| Remdesivir use | 0 | 2 (4%) | |
| Corticosteroid use | 43 (84%) | 44 (88%) | |
| Pre-existing comorbid conditions of interest† | |||
| Obesity | 28 (55%) | 29 (58%) | |
| Diabetes (type 1 and type 2) | 20 (39%) | 16 (32%) | |
| Chronic respiratory disease | 1 (2%) | 2 (4%) | |
| Hypertension | 31 (61%) | 24 (48%) | |
| Vasopressor use at baseline | 32 (63%) | 31 (62%) | |
| Renal replacement therapy use at baseline | 0 | 0 | |
| ECMO use at baseline | 2 (4%) | 1 (2%) | |
| NEWS‡ | 10·5 (2·0) | 10·6 (2·0) | |
| Inflammatory markers | |||
| C-reactive protein concentration, mg/L | 124·9 | 109·5 | |
| D-dimer concentration, mg/L | 1·6 | 1·6 | |
| Lactate dehydrogenase concentration, U/L | 499·5 | 543·6 | |
| Ferritin concentration, pmol/L | 2622·0 | 2836·9 | |
Data are mean (SD), median (IQR), median, or n (%). ECMO=extracorporeal membrane oxygenation. NEWS=National Early Warning Score.
Includes participants from Mexico and Latin America.
Patients with estimated glomerular filtration rate <30 mL/min per 1·73 m2 were excluded from study enrolment.
NEWS was used to detect and report changes in illness severity in participants with acute illness; participants on mechanical ventilation or ECMO were assigned a score of 3 for respiration rate regardless of the ventilator setting; participants on ECMO were assigned a score of 3 for heart rate because they were on cardiopulmonary bypass; the aggregate score is reflective of the participant's status, with higher scores representing higher level of acuity; a score of 7 or greater reflects high clinical risk for worsening acuity.
Treatment with baricitinib significantly reduced all-cause mortality by day 28 compared with placebo (20 [39%] of 51 participants died in the baricitinib group vs 29 [58%] of 50 in the placebo group; HR 0·54 [95% CI 0·31–0·96]; p=0·030), corresponding to a 46% relative reduction. There was an absolute risk reduction of 19% in the baricitinib group compared with placebo and, overall, one additional death was prevented per six baricitinib-treated participants (table 2 , figure 2A ). Between day 28 and day 60, five additional deaths occurred in the overall population, with a similar number of deaths in the baricitinib (n=3) and placebo (n=2) groups. All-cause mortality at day 60 remained significantly lower in the baricitinib group than in the placebo group (23 [45%] of 51 participants died in the baricitinib group vs 31 [62%] of 50 in the placebo group; HR 0·56 [95% CI 0·33–0·97]; p=0·027), corresponding to a 44% relative reduction and an absolute risk reduction of 17% (figure 2B).
Table 2.
Efficacy outcomes in the intention-to-treat population by day 28
| Baricitinib plus standard of care group (n=51) | Placebo plus standard of care group (n=50) | Baricitinib group compared with placebo (95% CI) | p value | ||
|---|---|---|---|---|---|
| All-cause mortality | |||||
| Deaths* | 20 (39%) | 29 (58%) | 0·54 (0·31 to 0·96) | 0·030 | |
| Kaplan-Meier estimates (95% CI) | 40·6% (25·8 to 59·7) | 59·0% (41·1 to 77·7) | .. | .. | |
| Time to mortality, days | NA (24·0 to NA) | 17·0 (11·0 to NA) | .. | .. | |
| Ventilator-free days, days† | 8·1 (10·2) | 5·5 (8·4) | 2·36 (−1·38 to 6·09) | 0·21 | |
| Likelihood of overall improvement on the NIAID-OS‡ | |||||
| Day 4 | .. | .. | 14·37 (1·79 to 115·65) | 0·012 | |
| Day 7 | .. | .. | 2·87 (1·12 to 7·36) | 0·028 | |
| Day 10 | .. | .. | 2·08 (0·96 to 4·49) | 0·062 | |
| Day 14 | .. | .. | 1·97 (0·95 to 4·09) | 0·068 | |
| Day 21 | .. | .. | 2·16 (1·04 to 4·49) | 0·040 | |
| Day 28 | .. | .. | 1·82 (0·87 to 3·81) | 0·11 | |
| ≥1-point improvement on NIAID-OS or live discharge from hospital‡ | |||||
| Day 4 | 6 (12%) | 1 (2%) | 6·89 (0·79 to 60·38) | 0·082 | |
| Day 7 | 8 (16%) | 5 (10%) | 1·85 (0·55 to 6·23) | 0·32 | |
| Day 10 | 13 (26%) | 8 (16%) | 1·80 (0·67 to 4·86) | 0·24 | |
| Day 14 | 16 (31%) | 13 (26%) | 1·27 (0·53 to 3·04) | 0·59 | |
| Day 21 | 19 (37%) | 15 (30%) | 1·29 (0·55 to 3·00) | 0·56 | |
| Day 28 | 23 (45%) | 15 (30%) | 1·80 (0·78 to 4·14) | 0·17 | |
| Duration of hospitalisation, days† | 23·7 (7·1) | 26·1 (3·9) | −2·30 (−4·59 to 0·00) | 0·050 | |
| Recovery§¶ | |||||
| Participants recovered | 19 (37%) | 13 (26%) | 1·57 (0·77 to 3·19) | 0·16 | |
| Kaplan-Meier estimates (95% CI) | 38·7% (18·8 to 52·6) | 27·0% (15·0 to 45·5) | .. | .. | |
| Time to recovery, days | NA (28·0 to NA) | NA (NA to NA) | .. | .. | |
Data are n (%), mean (SD), or median (95% CI) unless otherwise stated. Data were assessed from days 1 to 28, unless otherwise indicated. For dichotomous endpoints, a logistic regression model was used. For ordinal efficacy endpoints, a proportional odds model was used. For continuous endpoints, an analysis of variance was used. All of these analyses had age, geographical region, and treatment group in the model. For time-to-event endpoints, the p value was calculated using an unstratified log-rank test. Hazard ratios were calculated using a Cox proportional hazards model. p values are for comparisons of between the baricitinib group and the placebo group. All endpoints are exploratory due to the nature of the study. NA=not available. NIAID-OS=National Institute of Allergy and Infectious Disease ordinal scale.
Comparison is hazard ratio.
Comparisons are least square mean difference.
Comparisons are odds ratio.
Recovery was defined as clinical status of 1, 2, or 3 in the 8-point NIAID-OS (ie, not hospitalised or no longer requiring medical care).
Comparison is rate ratio.
Figure 2.

Kaplan-Meier estimates of all-cause mortality by day 28 and by day 60
(A) 28-day all-cause mortality. (B) 60-day all-cause mortality. All-cause mortality includes deaths potentially related with COVID-19 and deaths attributed to adverse events. The numbers at risk at days 27 and 59 represent the numbers of participants with available data at days 28 and 60, respectively. The data in parentheses below the curve represent the numbers of deaths that occurred during the interval until the next timepoint. HRs and 95% CIs were calculated using a Cox proportional hazard regression model adjusted for treatment group, age (<65 years vs ≥65 years), and geographical region (USA vs the rest of the world); unstratified. p values were calculated from an unstratified log-rank test. HR=hazard ratio.
There were no significant differences between groups in most of the other key endpoints examined in this exploratory trial, including number of ventilator-free days (mean 8·1 days [SD 10·2] in the baricitinib group vs 5·5 days [8·4] in the placebo group; p=0·21); overall improvement in NIAID-OS (likelihood of improvement at day 28 odds ratio 1·82 [95% CI 0·87–3·81]; p=0·11); proportion of participants who had at least a 1-point improvement on NIAID-OS or hospital discharge by day 28 (23 [45%] of 51 patients in the baricitinib group vs 15 [30%] of 50 in the placebo group; p=0·17); and duration of hospitalisation (mean 23·7 days [SD 7·1] in the baricitinib group vs 26·1 days [3·9] in the placebo group; p=0·050; table 2). More patients recovered (reached NIAID-OS 1, 2, or 3) by day 28 in the baricitinib group than in the placebo group (19 [37%] of 51 patients vs 13 [26%] of 50). There was no significant difference in the proportion of participants who had recovered at day 60 in the baricitinib group compared with the placebo group (24 [47%] vs 16 [32%]; appendix p 14). Analyses of outcomes by subgroup (baseline corticosteroid use, baseline remdesivir use, and country) at day 28 and day 60 are shown in the appendix (pp 5–14).
There were 44 (88%) of 50 participants in the baricitinib group and 47 (96%) of 49 in the placebo group with at least one treatment-emergent adverse event; 25 (50%) and 35 (71%) had at least one serious adverse event (table 3 ). The number of participants who discontinued study treatment due to adverse events (14 [28%] participants in the baricitinib group vs 17 [35%] in the placebo group) and the number of deaths due to adverse events (five [10%] vs three [6%]) were similar in both groups. The number of participants with treatment-emergent infections was similar between treatment groups (35 [70%] participants vs 35 [71%]). Serious infections were reported in 22 (44%) participants who received baricitinib and 26 (53%) who received placebo. There was a similar distribution of positively adjudicated venous thromboembolic events in both groups (three [6%] in the baricitinib group vs three [6%] in the placebo group; table 3, appendix p 15).
Table 3.
Adverse events in the safety population by day 28
| Baricitinib plus standard of care group (n=50) | Placebo plus standard of care group (n=49) | ||
|---|---|---|---|
| Treatment-emergent adverse event* | 44 (88%) | 47 (96%) | |
| Mild | 3 (6%) | 3 (6%) | |
| Moderate | 17 (34%) | 11 (22%) | |
| Severe | 24 (48%) | 33 (67%) | |
| Death due to adverse event† | 5 (10%) | 3 (6%) | |
| Serious adverse event | 25 (50%) | 35 (71%) | |
| Discontinuation from study treatment due to adverse event (including death) | 14 (28%) | 17 (35%) | |
| Treatment-emergent infection | 35 (70%) | 35 (71%) | |
| Serious infections | 22 (44%) | 26 (53%) | |
| Herpes simplex virus | 1 (2%) | 0 | |
| Opportunistic infections‡ | 0 | 2 (4%) | |
| Venous thromboembolic event§ | 3 (6%) | 3 (6%) | |
| Deep vein thrombosis | 1 (2%) | 2 (4%) | |
| Pulmonary embolism | 2 (4%) | 0 | |
| Other peripheral venous thrombosis | 1 (2%) | 1 (2%) | |
| Major adverse cardiovascular events¶ | |||
| Cardiovascular death | 1 (2%) | 0 | |
| Stroke | 1 (2%) | 0 | |
Data are n (%); n is number of participants. Data were assessed from days 1 to 28.
Patients with multiple occurrences of the same event are counted under the highest severity.
Included in the overall mortality together with deaths due to disease progression.
Includes Aspergillus infection (n=1) and fungal pneumonia (n=1).
Includes patients with at least one positively adjudicated treatment-emergent venous thromboembolic event.
Cardiovascular death event was classified as cardiogenic shock; stroke event was classified as cerebral haemorrhage; no myocardial infarction events were recorded in either treatment group.
Discussion
This exploratory study that followed the COV-BARRIER trial design evaluated the efficacy and safety of baricitinib in critically ill hospitalised patients with COVID-19 who were receiving IMV or ECMO at enrolment and was, to our knowledge, the first study of its kind to evaluate treatment specifically in this patient population with corticosteroids as part of the standard of care. Treatment with baricitinib plus standard of care (including corticosteroids) resulted in an absolute risk reduction of 17% in mortality at 60 days compared with placebo (HR 0·56 [95% CI 0·33–0·97]; p=0·027), which corresponds to a 44% relative reduction in mortality; overall, one additional death was prevented for every six baricitinib-treated participants at day 28 and day 60. These results in this exploratory study population are consistent with the reduction in mortality observed in the less severely ill hospitalised patients in the primary COV-BARRIER study population (NIAID-OS 4,5, or 6), in whom the HR was 0·57 (95% CI 0·41–0·78; p=0·018), corresponding to a 43% relative reduction in mortality at day 28 and an absolute risk reduction of 5% with baricitinib versus placebo. Compared with placebo, there was no evidence of an increased risk of infections, serious infections, venous thromboembolic events, or adverse cardiovascular events in participants treated with baricitinib.
Patients with severe COVID-19 can develop dysregulation of inflammatory mediators, such as cytokines IL-6, IL-10, tumour necrosis factor α, and IFN-γ and chemokines CXCL10 and monocyte chemoattract protein 3.3, 28, 29 Baricitinib has been shown to downregulate these inflammatory mediators implicated in COVID-19 pathophysiology in patients within 2 days after the start of treatment, through anti-inflammatory action caused by the selective inhibition of JAK1 and JAK2.30, 31, 32 A macaque study of SARS-CoV-2 infection also found that baricitinib treatment decreased cytokine and chemokine production, reduced the infiltration of inflammatory cells to the lungs, and reduced lung pathology in baricitinib-treated animals, without reducing innate antiviral type 1 IFN responses.33
The combination of baricitinib with corticosteroids, in particular dexamethasone, might have additive or indeed synergistic effects on these inflammatory molecules for the treatment of patients with COVID-19, as seen by the greater improvement in outcomes when baricitinib and other JAK inhibitors have been studied in combination with standard of care including corticosteroids.34 In the guidelines for the therapeutic management of hospitalised adults with COVID-19 published by the US National Institutes of Health (NIH; as of Aug 25, 2021), baricitinib is recommended in combination with dexamethasone for the treatment of patients who are hospitalised and have systemic inflammation and rapidly increasing oxygen requirements.35 Despite the advances in knowledge of potential treatments for COVID-19, few interventions are included in these guidelines, and options remain scarce for patients who require IMV or ECMO. In a meta-analysis of four trials, JAK inhibitors (baricitinib, ruxolitinib, tofacitinib, and nezulcitinib) were reported to reduce mortality risk in patients with COVID-19 by 43% and to reduce risk of requiring IMV or ECMO by 36%;36 this analysis did not include data from COV-BARRIER, which, to our knowledge, is the first randomised placebo-controlled trial of an immunomodulatory agent to report a reduction in COVID-19 mortality.37 The different mortality effect seen in critically ill patients (NIAID-OS 7) from COV-BARRIER reported here compared with those in ACTT-26 might be driven by the low use of corticosteroids in ACTT-2, whereas in this trial the majority of participants received baricitinib in combination with corticosteroids.
Although mortality was significantly reduced following treatment with baricitinib, the overall 28-day all-cause mortality for those on IMV or ECMO at baseline was 39% in participants who received baricitinib and 58% in those who received placebo. Published literature describes similar rates of mortality in this critically ill patient population; in one large meta-analysis, the case fatality rate of 45% was reported for the subgroup of patients with COVID-19 requiring IMV, with higher mortality rates in older patients (59% in those aged 51–60 years, which was similar to the population reported here who had a mean age of 58·6 years [SD 13·8]) and in early epicentres of COVID-19.12 RECOVERY, the open-label study that examined the efficacy of the anti-IL-6 antibody tocilizumab for the treatment of patients with COVID-19, reported 28-day mortality of 49% in participants who received tocilizumab while on IMV versus 51% in those who received standard of care.8 Some variability in the mortality rates might arise from differences in resource availability due to locations of study sites (the RECOVERY trial was conducted exclusively in the UK).
Although many of the key endpoints showed no significant difference between the study groups in this small exploratory trial, the point estimates appeared to favour baricitinib over placebo for number of ventilator-free days, time to recovery, improvement in NIAID-OS of at least 1 point or discharge from hospital, and duration of hospital stay. A larger trial is needed to understand if there is a treatment effect of baricitinib on these endpoints. A similar reduction in the hospital duration of stay was seen in the RECOVERY adaptive platform trial where median time to discharge was 12 days in the dexamethasone group versus 13 days in the usual care group, and 19 days in the tocilizumab group versus greater than 28 days in the usual care group.7, 8
Despite the large effect size seen here, this exploratory trial has some limitations, such as the small sample size (which precludes definitive conclusions regarding other clinical outcomes, such as resource utilisation or duration of hospital stay). In addition, the intensity of these participants' hyperinflammatory state might warrant longer durations of immunomodulation that were not part of our study design. The authors recognise expected heterogeneity in the management of the critically ill patient population and potential variability in access to care (including variability in the availability of ECMO and IMV) in regions where the pandemic was peaking. Although participants with baseline NIAID-OS 7 were evaluated in this exploratory trial following a phase 3 study design, the authors acknowledge that the sample size was similar to other phase 2 trials.
A further limitation is that the baseline measures typically collected in critical care studies were not collected in this exploratory study, which would have strengthened the evaluation and interpretation of data in this critically ill patient population. These measures include ventilator settings (including fractional concentration of oxygen in inspired air) and other data necessary to calculate critical illness severity scores, which are typical in trials designed for critically ill persons, which were not included due to the constraints of conducting the trial during the pandemic and due to following the trial design of the parent study for the hospitalised COVID-19 population. However, further available information to understand the baseline disease severity is provided. Clinical status, NEWS, inflammatory biomarkers, use of renal replacement therapy, and use of vasopressors at baseline were collected and are shown. These characteristics were similar between treatment groups at baseline.
In conclusion, treatment with baricitinib plus standard of care (including use of corticosteroids) in critically ill patients with COVID-19 who were receiving IMV or ECMO at enrolment resulted in reduction in all-cause mortality at 28 days and 60 days compared with placebo plus standard of care in this exploratory trial. These results are consistent with the reduction in mortality observed in the less severely ill hospitalised patients in the primary COV-BARRIER study population and further support the use of baricitinib in hospitalised adults with COVID-19. Baricitinib, when used to treat critically ill patients with COVID-19, might represent a novel option to reduce mortality, even if the disease process has progressed to the point of already receiving corticosteroids, IMV, and ECMO. However, further well-designed, phase 3 trials are necessary to provide additional data to support routine use of baricitinib in the studied population.
This online publication has been corrected. The corrected version first appeared at thelancet.com/respiratory on February 11, 2022
Data sharing
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymisation, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the USA and EU or after the trial is completed, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents (including the study protocol, statistical analysis plan, clinical study report, and blank or annotated case report forms) will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at https://www.vivli.org.
Declaration of interests
EWE reports research grants from the US Centers for Disease Control and Prevention (CDC), NIH, and Veterans Affairs; and has served as an unpaid consultant for Eli Lilly and Company. AVR reports research grants from Eli Lilly and Company; and has served as a speaker or consultant for AbbVie, Eli Lilly and Company, Novartis, Pfizer, Roche, Sobi, and Union Chimique Belge. CEK, SdB, RL, MLBP, and SC are employees and shareholders of Eli Lilly and Company. JDG reports research support from Eli Lilly and Company, Regeneron Pharmaceuticals, and Gilead Sciences; grants from NIH, Biomedical Advanced Research and Development Authority (administered by Merck), and Eurofins Viracor; and has served as a speaker or consultant for Eli Lilly and Company, Gilead Sciences, and Mylan Pharmaceuticals. JFKS reports research grants from Eli Lilly and Company; and has served as a speaker or consultant for Eli Lilly and Company, Amgen, Novartis, Janssen, and NovoNordisk. VCM reports research grants from the CDC, Gilead Sciences, NIH, Veterans Affairs, and ViiV Healthcare; honoraria from Eli Lilly and Company; has served as an advisory board member for Eli Lilly and Company and Novartis; and has participated as a study section chair for the NIH.
Acknowledgments
Acknowledgments
This study was funded by Eli Lilly and Company, under license from Incyte Corporation. We would like to thank the study participants, investigators, and staff, including the COV-BARRIER Study Group who participated in the study. We also thank Anabela Cardoso, David H Adams, and Brenda Crowe (Eli Lilly and Company, Indianopolis, IN, USA) for scientific input; and Catherine Lynch (Eli Lilly and Company, Cork, Ireland) for medical writing and process support. VCM would like to thank his colleagues Christina Gavegnano, Raymond F Schinazi, and Boghuma Titanji (Emory University School of Medicine, Atlanta, GA, USA) for their expertise and support.
Contributors
All authors contributed to the concept and design of the trial, data analysis and interpretation, and critical revision of the manuscript, and are accountable for the accuracy and integrity of the Article. CEK, RL, and SC accessed and verified the underlying data. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Contributor Information
COV-BARRIER Study Group:
Jorge Alatorre-Alexander, Javier David Altclas, Marcelo Casas, Valeria CevoliRecio, Todd Ellerin, Kleber Giovanni Luz, Jason D. Goldman, Maria Patelli Juliani Souza Lima, Akram Khan, Priscila Paulin, Ana Carolina Procopio Carvalho, Gustavo Rojas Velasco, Jose Francisco Kerr Saraiva, Imad Shawa, Jesus Simon Campos, Brian Tiffany, and Adilson Westheimer Cavalcante
Supplementary Material
References
- 1.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. doi: 10.1016/S0140-6736(20)30566-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Su Y, Chen D, Yuan D, et al. Multi-omics resolves a sharp disease-state shift between mild and moderate COVID-19. Cell. 2020;183:1479–1495. doi: 10.1016/j.cell.2020.10.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tan LY, Komarasamy TV, Rmt Balasubramaniam V. Hyperinflammatory immune response and COVID-19: a double edged sword. Front Immunol. 2021;12 doi: 10.3389/fimmu.2021.742941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of COVID-19—final report. N Engl J Med. 2020;383:1813–1826. doi: 10.1056/NEJMoa2007764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kalil AC, Patterson TF, Mehta AK, et al. Baricitinib plus remdesivir for hospitalized adults with COVID-19. N Engl J Med. 2021;384:795–807. doi: 10.1056/NEJMoa2031994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Horby P, Lim WS, Emberson JR, et al. Dexamethasone in hospitalized patients with COVID-19. N Engl J Med. 2021;384:693–704. doi: 10.1056/NEJMoa2021436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.RECOVERY Collaborative Group Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. 2021;397:1637–1645. doi: 10.1016/S0140-6736(21)00676-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goletti D, Cantini F. Baricitinib therapy in COVID-19 pneumonia—an unmet need fulfilled. N Engl J Med. 2021;384:867–869. doi: 10.1056/NEJMe2034982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marconi VC, Ramanan AV, de Bono S, et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir Med. 2021;9:1407–1418. doi: 10.1016/S2213-2600(21)00331-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.WHO WHO Coronavirus (COVID-19) dashboard. 2021. https://covid19.who.int/table
- 12.Lim ZJ, Subramaniam A, Ponnapa Reddy M, et al. Case fatality rates for patients with COVID-19 requiring invasive mechanical ventilation. A meta-analysis. Am J Respir Crit Care Med. 2021;203:54–66. doi: 10.1164/rccm.202006-2405OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Shi JG, Chen X, Lee F, et al. The pharmacokinetics, pharmacodynamics, and safety of baricitinib, an oral JAK 1/2 inhibitor, in healthy volunteers. J Clin Pharmacol. 2014;54:1354–1361. doi: 10.1002/jcph.354. [DOI] [PubMed] [Google Scholar]
- 14.McInnes IB, Byers NL, Higgs RE, et al. Comparison of baricitinib, upadacitinib, and tofacitinib mediated regulation of cytokine signaling in human leukocyte subpopulations. Arthritis Res Ther. 2019;21:183. doi: 10.1186/s13075-019-1964-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dörner T, Tanaka Y, Petri MA, et al. Baricitinib-associated changes in global gene expression during a 24-week phase II clinical systemic lupus erythematosus trial implicates a mechanism of action through multiple immune-related pathways. Lupus Sci Med. 2020;7 doi: 10.1136/lupus-2020-000424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Richardson P, Griffin I, Tucker C, et al. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet. 2020;395:e30–e31. doi: 10.1016/S0140-6736(20)30304-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stebbing J, Phelan A, Griffin I, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20:400–402. doi: 10.1016/S1473-3099(20)30132-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Titanji BK, Farley MM, Mehta A, et al. Use of baricitinib in patients with moderate to severe coronavirus disease 2019. Clin Infect Dis. 2021;72:1247–1250. doi: 10.1093/cid/ciaa879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cantini F, Niccoli L, Matarrese D, Nicastri E, Stobbione P, Goletti D. Baricitinib therapy in COVID-19: a pilot study on safety and clinical impact. J Infect. 2020;81:318–356. doi: 10.1016/j.jinf.2020.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cantini F, Niccoli L, Nannini C, et al. Beneficial impact of baricitinib in COVID-19 moderate pneumonia; multicentre study. J Infect. 2020;81:647–679. doi: 10.1016/j.jinf.2020.06.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stebbing J, Sánchez Nievas G, Falcone M, et al. JAK inhibition reduces SARS-CoV-2 liver infectivity and modulates inflammatory responses to reduce morbidity and mortality. Sci Adv. 2021;7 doi: 10.1126/sciadv.abe4724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Abizanda P, Calbo Mayo JM, Mas Romero M, et al. Baricitinib reduces 30-day mortality in older adults with moderate-to-severe COVID-19 pneumonia. J Am Geriatr Soc. 2021;69:2752–2758. doi: 10.1111/jgs.17357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cao Y, Wei J, Zou L, et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): a multicenter, single-blind, randomized controlled trial. J Allergy Clin Immunol. 2020;146:137–146. doi: 10.1016/j.jaci.2020.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Guimarães PO, Quirk D, Furtado RH, et al. Tofacitinib in patients hospitalized with COVID-19 pneumonia. N Engl J Med. 2021;385:406–415. doi: 10.1056/NEJMoa2101643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Singh D, Bogus M, Moskalenko V, et al. A phase 2 multiple ascending dose study of the inhaled pan-JAK inhibitor nezulcitinib (TD-0903) in severe COVID-19. Eur Respir J. 2021;58 doi: 10.1183/13993003.00673-2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.US Food and Drug Administration Letter of authorization: EUA for baricitinib (Olumiant) for treatment of coronavirus disease 2019 (COVID-19) 2020. https://www.fda.gov/media/143822/download
- 27.Royal College of Physicians . Royal College of Physicians; London: 2012. National Early Warning Score (NEWS): standardising the assessment of acute-illness severity in the NHS. Report of a working party. [Google Scholar]
- 28.Karki R, Sharma BR, Tuladhar S, et al. Synergism of TNF-α and IFN-γ triggers inflammatory cell death, tissue damage, and mortality in SARS-CoV-2 infection and cytokine shock syndromes. Cell. 2021;184:149–168. doi: 10.1016/j.cell.2020.11.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yang Y, Shen C, Li J, et al. Plasma IP-10 and MCP-3 levels are highly associated with disease severity and predict the progression of COVID-19. J Allergy Clin Immunol. 2020;146:119–127. doi: 10.1016/j.jaci.2020.04.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bronte V, Ugel S, Tinazzi E, et al. Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J Clin Invest. 2020;130:6409–6416. doi: 10.1172/JCI141772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Petrone L, Petruccioli E, Alonzi T, et al. In-vitro evaluation of the immunomodulatory effects of baricitinib: implication for COVID-19 therapy. J Infect. 2021;82:58–66. doi: 10.1016/j.jinf.2021.02.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sims JT, Krishnan V, Chang CY, et al. Characterization of the cytokine storm reflects hyperinflammatory endothelial dysfunction in COVID-19. J Allergy Clin Immunol. 2021;147:107–111. doi: 10.1016/j.jaci.2020.08.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hoang TN, Pino M, Boddapati AK, et al. Baricitinib treatment resolves lower-airway macrophage inflammation and neutrophil recruitment in SARS-CoV-2-infected rhesus macaques. Cell. 2021;184:460–475. doi: 10.1016/j.cell.2020.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Stebbing J, Lauschke VM. JAK inhibitors—more than just glucocorticoids. N Engl J Med. 2021;385:463–465. doi: 10.1056/NEJMe2108667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.COVID-19 treatment guidelines panel . National Institutes of Health; 2021. Coronavirus disease 2019 (COVID-19) treatment guidelines.https://www.covid19treatmentguidelines.nih.gov/ [PubMed] [Google Scholar]
- 36.Patoulias D, Doumas M, Papadopoulos C, Karagiannis A. Janus kinase inhibitors and major COVID-19 outcomes: time to forget the two faces of Janus! A meta-analysis of randomized controlled trials. Clin Rheumatol. 2021;40:4671–4674. doi: 10.1007/s10067-021-05884-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kalil AC, Stebbing J. Baricitinib: the first immunomodulatory treatment to reduce COVID-19 mortality in a placebo-controlled trial. Lancet Respir Med. 2021;9:1349–1351. doi: 10.1016/S2213-2600(21)00358-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymisation, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the USA and EU or after the trial is completed, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents (including the study protocol, statistical analysis plan, clinical study report, and blank or annotated case report forms) will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at https://www.vivli.org.