

Abstract
Objective:
To compare the magnitude of external apical root resorption (EARR) of incisors in patients undergoing the initial phase of orthodontic treatment with two sets of brackets.
Materials and Methods:
According to the results of the power analysis for sample size calculation, 19 Angle Class I patients (anterior crowding: 3 to 5 mm; mean age: 20.6 years) were included in the study and randomly divided into two groups: group I (n = 11, self-ligating brackets) and group II (n = 8, conventional preadjusted brackets). The degree of EARR was detected in 152 upper and lower incisors by using cone-beam computed tomography (CBCT) scans and a three-dimensional program (Dolphin 11.5, Dolphin Imaging & Management Solutions, Chatsworth, Calif) with 25% level of sensitivity. The CBCT scans were obtained before (T1) and 6 months after initiation of treatment (T2). Differences between and within groups were analyzed by nonpaired and paired t-test, respectively, with 5% significance level.
Results:
Significant differences were found for both groups between T1 and T2. However, no differences in the degree of EARR were detected between the groups studied.
Conclusions:
Although EARR has occurred in all teeth evaluated, the bracket design (self-ligating or conventional) did not demonstrate any influence on the results observed.
Keywords: Self-ligating brackets, Root resorption, Cone beam computed tomography
INTRODUCTION
The search for improved efficiency in orthodontic treatment has afforded new designs of brackets.1 One such evolution occurred with the use of self-ligating brackets, which were introduced in the early 1930s but have been gaining popularity only in recent years.2 Self-ligating brackets can be divided into two main categories, active and passive, according to their mechanisms of closure. Active self-ligating brackets have a spring clip that stores energy to press against the archwire, and passive self-ligating brackets usually have a slide that can be closed which does not encroach on the slot lumen, thus exerting no active force on the archwire.1 These brackets are referred to as having less friction, a higher rate of dental movement, and shorter period of treatment.3 Other claimed advantages of this system are fewer appointments, improved oral hygiene, better acceptance by patients, and better treatment results.3
Although considered to have clinical advantages, the self-ligating brackets seem to present significant benefits only with regard to chair time when compared to the conventional brackets.1,4 In terms of treatment duration, number of appointments, and efficiency in correcting malocclusions, no significant differences were found between both types of brackets.1,4 The duration of orthodontic treatment is susceptible to the professional's ability and experience and depends on the objectives of the orthodontic treatment, in addition to the severity of the patient's initial malocclusion.4 Thus, professionals must decide whether such an advantage is worth paying the higher cost of self-ligating brackets.4
Since efficiency of orthodontic treatment with the system of self-ligating brackets has been widely discussed, a hypothesis has been raised as to what may occur to tooth roots during dental movement. In fact, a faster correction of the malocclusion could lead to undesirable side effects, such as root resorption, which is a great concern for orthodontists.5
External apical root resorption (EARR) presents with a multifactorial etiology, individual predisposition being one of the factors.6–8 Since the greatest cause of root resorption in the population refers to orthodontic movement, a correlation exists between severity of the malocclusion and the degree of consequent root resorption.7–9 This occurs as a result of the mechanical resources demanded and is due to long-lasting treatment.7 In addition, characteristics that are inherent to orthodontic treatment, such as type of brackets, the mechanics used, and the type and magnitude of the forces applied,7,8,10 are also relevant.
The influence of genetic factors in EARR in patients submitted to orthodontic treatment has been cited6,8–11 since root resorption is a common side effect of treatment, though it is also present in patients who were not orthodontically treated.9 The degree of root resorption associated with orthodontic treatment is influenced by a number of individual and general factors.6,8–10 Genetic factors are responsible for at least 50% of EARR variations.9
Orthodontic patients with detectable root resorption during the first 6 months of active treatment are reported to be more susceptible to root resorption after this period.10,12 Therefore, patients who are under the risk of root resorption should be identified early, and this is why radiographic examinations 6 months after corrective treatment are advisable.10,12
A radiographic examination is essential for the diagnosis of root resorption. Recently, two-dimensional radiographs (2D) have still been used for this diagnosis, including periapical, panoramic,13–15 and occlusal radiographs, or a combination thereof.13 Computed tomography scans have been regarded as the most precise tool in detecting root resorption.5,13,15–18 Therefore, cone-beam computed tomography (CBCT) images showing root resorption may influence orthodontists in either continuing or modifying the treatment plan as needed.15
The purpose of this prospective study was to compare the magnitude of EARR incisors in patients undergoing the initial phase of orthodontic treatment, with self-ligating and conventional brackets.
MATERIALS AND METHODS
For this prospective study, 19 patients (mean age 20.6 years, minimum 11, maximum 30) were randomly divided into two groups: group I (n = 11; 5 female and 6 male subjects using passive self-ligating brackets with a 0.022- × 0.027-inch slot (EasyClip, Aditek, Cravinhos, SP, Brazil) and group II (n = 8; 6 female and 2 male subjects using conventional preadjusted brackets with a 0.022- × 0.030-inch slot (3M Unitek, Monrovia, Calif).
All of the patients presented Angle Class I malocclusion, with anterior crowding ranging from 3 to 5 mm. Only patients with complete permanent dentition, except third molars, were accepted for the study. Patients who submitted to previous orthodontic treatment or with signs of EARR observed at the first examination were excluded. Extraction of premolars and dental stripping were not included in the treatment proposed.
Informed consent was signed by all parents or guardians of the patients after they received detailed information about the planned clinical trial and their children's future orthodontic treatment. This trial was approved by the ethical committee of the University of North Paraná.
The patients were orthodontically treated during the initial leveling and alignment for the 6-month period beginning with the same sequence of 0.013-, 0.014-, and 0.016-inch nickel-titanium archwires. According to the protocol chosen, each archwire remained for 2 months, and it was replaced in the previously mentioned sequence. The archwires for group II were attached to the brackets by using a metallic ligature.
CBCT scans were obtained from all patients in two time intervals, prior to the beginning of the orthodontic treatment and 6 months after it. All CBCT scans were carried out by a single experienced radiologist using the same tomographer (i-Cat Imaging Sciences International, Hatfield, Pa). The specifications are the following: 22 ×16 cm FOV, 40 seconds, 120 kVp, 36 mA. This tomographer has high-resolution sensors and affords 0.4 mm voxel images.
The CBCT scans were assessed by the same researcher in order to evaluate the root resorption of upper and lower incisors, requested both at the beginning and after 6 months of the initiation of the orthodontic treatment, by using the Dolphin 3D program (Version 11.5, Dolphin Imaging & Management Solutions, Chatsworth, Calif) with a level of sensitivity fixed at 25%.
Sagittal cuts of lower and upper incisors were selected and a sectional cut was made in the center of the long axis thereof, which coincided with the incisal border and the root apex (Figure 1). The EARR was calculated by assessing the difference in the total tooth length, which was measured from the incisal border to the root apex, between T1 and T2 (T2–T1), in millimeters. Thus, 152 incisors were blindly evaluated regarding root resorption.
Figure 1.
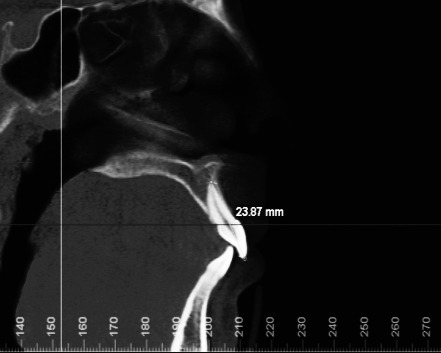
Sectional cut in the center of the long axis, coinciding with the incisal border and the root apex of the tooth.
Statistical Analysis
Power analysis showed that a sample size of at least 19 patients would give an 80% probability of detecting a real difference of 0.4 mm between groups at a statistically significant level of 5%.
Thirty days after the first evaluation, 50% of the CBCT scans were randomly selected, and the respective measurements were repeated in order to determine intraexaminer errors by means of paired t-test (systematic errors) and Dahlberg formula (casual errors).19
The data were tested regarding the normal distribution by applying the Kolmogorov-Smirnov test. Because the distributions were normal, parametric tests could be used. The results were described by parameters of mean and standard deviation of T1 and T2 measurements for both groups. A paired t-test was employed to compare the degree of root resorption in each group between T1 and T2 periods, and a nonpaired t-test was used for comparison between both groups. In all statistical tests, the significance level was set at 5%.
Statistical calculations were made with Statistica software (version 7.0, StatSoft Inc, Tulsa, Okla).
RESULTS
Intraexaminer agreement was excellent (P = .656 and Dahlberg = 0.27). Coefficients showed high rates of agreement for the measures with CBCT.
A statistically significant difference occurred in all teeth in the comparison between T1 and T2 for patients of group I, as shown in Table 1.
Table 1.
Comparison of the Degree of Root Resorption (mm) Between T1 and T2 for the Patients in Group I (Self-ligating Brackets)

The same occurred for Group II, in which all of the teeth had statistically significant root resorption, as can be seen in Table 2.
Table 2.
Comparison of the Degree of Root Resorption (mm) Between T1 and T2 for the Patients in Group II (Conventional Preadjusted Brackets)

No statistically significant difference was found in the comparison of the degree of root resorption between the two groups, as can be seen in Table 3.
Table 3.
Comparison of the Difference in Root Resorption Between Group I (Self-ligating Brackets) and Group II (Conventional Preadjusted Brackets)

DISCUSSION
Apical root resorption is a frequent undesirable side effect in orthodontic treatment. However, innovations in techniques and orthodontic materials have been developed to reduce this problem.20 Its multifactorial etiology includes individual predisposition,6–8,14 characteristics associated to orthodontic treatment, and root morphology.7,8 Nevertheless, the groups in this study were not selected according to these criteria. Yet, various root types were randomly distributed in the groups. In order to define the sample, the presence of some variables plays an important role in the result of EARR measurements during orthodontic treatment. It becomes difficult to obtain groups treated by a single operator when taking into account the sample size and the type of study, whether prospective or retrospective. However, even samples of varied sources do not seem to interfere in the results.21
In this sample, different operators treated the patients, but in order to obtain more reliable results, measurements were made by a single previously calibrated examiner. Even with previous training, it is advisable to investigate intraexaminer errors, which was carried out by using paired t-test for systematic errors; to calculate casual errors, the formula proposed by Dahlberg was used.19 The method for measuring root resorption with CBCT scans was deemed reliable due to high rates of agreement for all teeth examined, as previously cited in the literature.5,13,18 Despite the changes in teeth position due to orthodontic treatment,8,18 CBCT scans produce a high level of reproducibility, which reasserts its use in orthodontics.5,17,18
In order to evaluate root length, an in vitro CBCT precision study was performed. Measurement differences ranged from 0.07 to 0.26 mm and occurred because anatomic differences were not considered clinically significant.18 A disadvantage of this method is a greater dose of radiation compared with conventional radiographies (periapical and panoramic). However, CBCT is an invaluable tool in orthodontic research.18
The presence of EARR is detectable by means of radiographic examinations, which must be carried out 6 months after the beginning of the treatment for a proper diagnosis.6,10,12,22 When EARR is detected previously to orthodontic treatment it may influence its magnitude during and after treatment due to patients susceptibility.9 Thus, in this study the presence of previous root resorption was regarded as an exclusion criterion.
The definition of the time evaluated in this research has a scientific basis, since 6 months of treatment is sufficient to detect some degree of root resorption, thus characterizing patient individual predisposition. These patients will be more susceptible to resorption in the period following the 6 months than those who did not have this kind of problem.10,12
The power analysis showed that 19 patients were needed to achieve 80% power to detect meaningful differences of 0.4 mm between the groups at a statistically significant level of 5%. Based on that, the sample size of this research was adequate to demonstrate differences in the degree of EARR between the groups studied. Despite the fact that the age ranged from 11 to 30 years, the scientific evidence shows no relationship between patient's age and the amount of root resorption.14
In this research, only the incisors (n = 152 teeth) were analyzed, which are the most moved and reabsorbed teeth during orthodontic treatment.7,14,20 Upper incisors have been mentioned in the literature as having the greatest root resorption.10,12,20 The results of this study showed a tendency of these teeth to suffer the lowest external root resorption, with an average of 0.34 mm. The average found in studies with fixed orthodontic therapy, but using periapical radiographies, was 0.53 mm22 and 0.76 mm.10 This difference may occur due to the method used, since the time of treatment was similar, 22 to 26 weeks, as compared to 24 weeks in this study. Yet, for root analysis most studies use periapical radiographies with parallelism technique, although some teeth may have their image lengthened, suggesting amplification and processing errors.5 Incisor angular positioning may change with orthodontic movement, and so may affect tooth length in the radiography.12 Consequently, technological innovations made it possible to evaluate the degree of root resorption in a three-dimensional way, due to its precision in measuring root shortening.17 Another factor that could also explain the smaller resorption in this study would be the use of only nickel-titanium archwires, which offer less force in relation to stainless steel archwires, thus affecting the magnitude of the EARR.24
Regarding the amount of root resorption in all incisors, an average of 0.35 mm was found—a value close to that in the literature of 0.25 mm in the leveling and alignment phase.25 Although it occurred in all teeth, this degree of EARR is small and clinically irrelevant.25–27
The comparison of the degree of EARR between patients treated with different models of brackets was based on the possible advantages attributed to self-ligating brackets.3 It was suggested that patients submitted to a supposedly faster dental movement may have a greater level of root resorption, since orthodontic mechanics could be regarded as an etiologic factor of root shortening after treatment.7,20,28
In a relevant study comparing conventional and self-ligating brackets, no difference was found in the amount of root resorption.29 These data are in accordance with the results of this research (Table 3) in which no statistically significant differences were detected between the two groups. Other studies reported the same findings.28,30
Based on the results of this study, self-ligating brackets were not able to induce greater apical root shortening measured in CBCT scans, regarding upper and lower incisors. However, further long-term clinical studies are necessary to confirm the results observed in this research.
CONCLUSION
Based on the similarity of the amount of root shortening in the studied groups during the first 6 months of orthodontic treatment, the design of the brackets (passive self-ligating or conventional preadjusted) did not seem to influence the degree of EARR.
REFERENCES
- 1.Chen S. S. H, Greenlee G. M, Kim J, Smith C. L, Huang G. J. Systematic review of self-ligating brackets. Am J Orthod Dentofacial Orthop. 2010;137:726.e1–726.e18. doi: 10.1016/j.ajodo.2009.11.009. [DOI] [PubMed] [Google Scholar]
- 2.Stolzenberg J. The Russell attachment and its improved advantages. Int J Orthod Dent Child. 1935;21:837–840. [Google Scholar]
- 3.Berger J, Byloff F. K. The clinical efficiency of self-ligated brackets. J Clin Orthod. 2001;35:304–308. [PubMed] [Google Scholar]
- 4.Fleming S. P, Dibiase A. T, Lee R. T. Randomized clinical trial of orthodontic treatment efficiency with self-ligating and conventional fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2010;137:738–742. doi: 10.1016/j.ajodo.2009.06.023. [DOI] [PubMed] [Google Scholar]
- 5.Sherrard J. F. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137:S100–108. doi: 10.1016/j.ajodo.2009.03.040. [DOI] [PubMed] [Google Scholar]
- 6.Weltman B. Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462–476. doi: 10.1016/j.ajodo.2009.06.021. [DOI] [PubMed] [Google Scholar]
- 7.Levander E, Malmgren O. Evaluation of the risks of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988;10:30–38. doi: 10.1093/ejo/10.1.30. [DOI] [PubMed] [Google Scholar]
- 8.Mirabella D, Ärtun J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108:48–55. doi: 10.1016/s0889-5406(95)70065-x. [DOI] [PubMed] [Google Scholar]
- 9.Hartsfield J. K, Jr, Everett E. T, Al-Qawasmi R. A. Genetic factors in external apical root resorption and orthodontic treatment. Crit Rev Oral Biol Med. 2004;15:115–122. doi: 10.1177/154411130401500205. [DOI] [PubMed] [Google Scholar]
- 10.Ärtun J, Smale I, Behbehani F, Doppel D, Van′t Hof M, Kuijpers-Jagtman A. M. Apical root resorption six and 12 months after initiation of fixed orthodontic appliance therapy. Angle Orthod. 2005;29:919–926. doi: 10.1043/0003-3219(2005)75[919:ARRSAM]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Al-Qawasmi R. A, Hartsfield J. K, Everett E. T, Weaver M. R, Foroud T. M, Faust D. M. Root resorption associated with orthodontic force in inbred mice: genetic contributions. Eur J Orthod. 2006;28:13–19. doi: 10.1093/ejo/cji090. [DOI] [PubMed] [Google Scholar]
- 12.Apajalahti S, Peltona J. S. Apical root resorption after orthodontic treatment—a retrospective study. Eur J Orthod. 2007;29:408–412. doi: 10.1093/ejo/cjm016. [DOI] [PubMed] [Google Scholar]
- 13.Alqerban A, Jacobs R, Souza P. C, Willems G. In-vitro comparison of 2 cone-beam computed tomography systems and panoramic imaging for detecting simulated canine impaction-induced external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2009;136:764.e1–764.e11. doi: 10.1016/j.ajodo.2009.03.036. [DOI] [PubMed] [Google Scholar]
- 14.Jiang R, McDonald J. P, Fu M. Root resorption before and after orthodontic treatment: a clinical study of contributory factors. Eur J Orthod. 2010;32:693–697. doi: 10.1093/ejo/cjp165. [DOI] [PubMed] [Google Scholar]
- 15.Dudic, Giannopoulou C, Leuzinger M, Kiliaridis S. Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofacial Orthop. 2009;135:434–437. doi: 10.1016/j.ajodo.2008.10.014. [DOI] [PubMed] [Google Scholar]
- 16.Mah J. K, Yi L, Huang R. C, Choo H. Advanced applications of cone beam computed tomography in orthodontics. Semin Orthod. 2011;17:57–71. [Google Scholar]
- 17.Leuzinger M, Dudic A, Giannopoulou C, Kiliaridis S. Root-contact evaluation by panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofacial Orthop. 2010;137:389–392. doi: 10.1016/j.ajodo.2009.10.027. [DOI] [PubMed] [Google Scholar]
- 18.Lund H, Gröndahl K, Gröndahl H. Cone beam computed tomography for assessment of root length and marginal bone level during orthodontic treatment. Angle Orthod. 2010;80:466–473. doi: 10.2319/072909-427.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dalhlberg G. Statistical Methods for Medical and Biological Students. London, UK: George Allen and Unwin; 1940. [Google Scholar]
- 20.Janson G. R, Canto G. L, Martins D. R, Henriques J. F. C, Freitas M. R. A radiographic comparison of apical root resorption after orthodontic treatment with 3 different fixed appliance techniques. Am J Orthod Dentofacial Orthop. 1999;118:262–273. doi: 10.1067/mod.2000.99136. [DOI] [PubMed] [Google Scholar]
- 21.Remington D. N, Joondeph D. R, Ärtun J, Riedel R. A, Chapko M. K. Long-term evaluation of root resorption occurring during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1989;96:43–46. doi: 10.1016/0889-5406(89)90227-8. [DOI] [PubMed] [Google Scholar]
- 22.Alexander S. A. Levels of root resorption associated with continuous arch and sectional arch mechanics. Am J Orthod Dentofacial Orthop. 1996;110:321–324. doi: 10.1016/s0889-5406(96)80017-5. [DOI] [PubMed] [Google Scholar]
- 23.Weiland F. Constant versus dissipating forces in orthodontics: the effect on initial tooth movements and root resorption. Eur J Orthod. 2003;25:335–342. doi: 10.1093/ejo/25.4.335. [DOI] [PubMed] [Google Scholar]
- 24.Ramanathan C, Hofman Z. Root resorption during tooth movements. Eur J Orthod. 2009;31:578–583. doi: 10.1093/ejo/cjp058. [DOI] [PubMed] [Google Scholar]
- 25.Malmgren O, Goldson L, Hill C, Orwin A, Petrini L, Lundberg M. Root resorption after orthodontic treatment of traumatized teeth. Am J Orthod. 1982;82:487–491. doi: 10.1016/0002-9416(82)90317-7. [DOI] [PubMed] [Google Scholar]
- 26.Makedonas D, Lund H, Gröndahl K, Hansen K. Root resorption diagnosed with cone beam computed tomography after 6 months of orthodontic treatment with fixed appliance and the relation to risk factors. Angle Orthod. 2011;139:e73–81. doi: 10.2319/112810-691.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Smale I, Ärtun J, Behbehani F, Doppel D, Van′t Hof M, Kuijpers-Jagtman A. M. Apical root resorption 6 months after initiation of fixed orthodontic appliance therapy. Am J Orthod Dentofacial Orthop. 2005;128:57–67. doi: 10.1016/j.ajodo.2003.12.030. [DOI] [PubMed] [Google Scholar]
- 28.Scott P, Di Biase A. T, Sherriff M, Cobourne M. Alignment efficiency of Damon 3 self-ligating and conventional orthodontic bracket systems: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2008;134:470.e1–8. doi: 10.1016/j.ajodo.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 29.Blake M, Woodside D. J, Pharoah M. J. A radiographic comparison of apical root resorption after orthodontic treatment with the edgewise and speed appliances. Am J Orthod Dentofacial Orthop. 1995;108:76–84. doi: 10.1016/s0889-5406(95)70069-2. [DOI] [PubMed] [Google Scholar]
- 30.Pandis N. External apical root resorption in patients treated with conventional and self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008;134:646–651. doi: 10.1016/j.ajodo.2007.01.032. [DOI] [PubMed] [Google Scholar]