

Abstract
Background
Research studies have described the morbidity associated with inherited bleeding disorders such as hemophilia and von Willebrand disease in women, but their effect on daily living has long been underrecognized. This systematic review sought to document the lived experience of women with a bleeding disorder by assessing research findings on quality of health care, socioeconomic factors, and mental health.
Methods
A systematic search was carried out in Web of Science, the Cumulative Index to Nursing and Allied Health Literature, and PubMed on July 31, 2020. References were hand searched. Abstracts of the 2019 and 2020 congresses on bleeding disorders were hand searched. Key journals were screened for relevant studies published after the search date until the analysis was completed on December 7, 2020.
Results
Of 635 potentially eligible publications, 27 published since 1998 were selected for review. Most studies were of moderate to high quality but meta‐analysis of quantitative studies was not possible due to difference in outcomes and assessment.
Women with a bleeding disorder experience obstacles to accessing care, difficulties living with their disorder, interference with schooling and work, and poor mental health. Diagnostic delay and lack of recognition of symptoms mean treatment and support may not be available. Where comparisons with controls were made, women’s negative experiences were greater than those of men.
Conclusions
Women with bleeding disorders experience major negative impacts of their disorders on daily life and mental well‐being. Many of the challenges identified in earlier research are evident in more recent studies.
Keywords: access and evaluation, health care quality, hemophilia, mental health, socioeconomic factors, systematic review, women
Essentials.
We do not know enough about the experience of women who live with a bleeding disorder.
This systematic review includes research published between 1998 and 2020.
Women with a bleeding disorder report delayed diagnosis, stigma, reduced access to health care, and poor mental health.
These findings have changed little over time.
1. INTRODUCTION
Hemophilia is probably the bleeding disorder most familiar to nonspecialists. It is less common than von Willebrand disease (VWD), but it is associated with a higher prevalence of the severe phenotype. 1 , 2 , 3 Conversely, it is much more common than other factor deficiencies and platelet function disorders that may also cause severe bleeding. 4 It has for many years been perceived as a disorder that causes excessive bleeding in boys and men and is passed between generations by women, who are clinically unaffected. This perception of hemophilia as “the archetypal bleeding disorder, affecting only males” has cast “a long shadow over the evaluation of women with bleeding disorders.” 5
Women with bleeding disorders face multiple challenges from their experience of excessive bleeding. 6 , 7 , 8 , 9 Many have heavy menstrual bleeding every month when, by contrast, a man with hemophilia managed by prophylaxis with factor replacement might have an average annual bleed rate of 3. 10 , 11 , 12 They also have an increased risk of bleeding associated with trauma, childbirth, and surgery, and in addition to coping with their personal health, some also face the demands of caring for a family in which one or more children are affected. 13
It has long been known that bleeding disorders adversely affect health‐related quality of life in women, 6 , 14 but little has been reported about their socioeconomic impact. A recent Canadian qualitative study involving 15 women with a bleeding disorder found they lived with “multiple uncertainties around their diagnosis, challenges with diagnostic labels, as well as misdiagnoses and diagnostic delay,” experiencing stigma and interference with hobbies, schooling, and work. 15 This study also showed that women with bleeding disorders may define their identity by their bleeding disorder, and many obtain a sense of community with their peers that mitigates feelings of loneliness, shame, and fear.
The impact of bleeding disorders on women is therefore profound, but little has been reported about their impact on daily life. In 2019, Haemnet began the Cinderella project to explore the lived experience of women who bleed due to a diagnosed bleeding disorder or low clotting factor levels. The project aims to improve understanding of the unmet need among women who bleed by reviewing access to support and care, describing the social and financial burden, and identifying strategies to support commissioners and health care providers to improve the quality of health care. This systematic review was carried out to provide evidence for the Cinderella project by assessing research findings on the impact of living with a bleeding disorder on women’s experience of access to care, socioeconomic status, and mental health.
2. MATERIALS AND METHODS
2.1. Inclusion criteria
Included studies were those published in English of any design that included qualitative or quantitative outcomes for women with a bleeding disorder for three end points: access to care, socioeconomic impact (eg, income, education, employment, period poverty), or productivity (eg, level of employment, presenteeism/absenteeism, workdays lost, loss of income, disability), and mental health challenges. Studies published in gray literature and unpublished studies were also eligible. Women labeled as carriers were considered to be women with a bleeding disorder. Studies reporting outcomes for women who did not have a bleeding disorder but who were mothers or carers of people with a bleeding disorder, and studies not reporting outcomes for women separately, were excluded. No distinction was made between inherited and acquired bleeding disorders.
2.2. Search strategy
A systematic search was carried out in Web of Science, the Cumulative Index to Nursing and Allied Health Literature, and PubMed on July 31, 2020. The strategy was defined to maximize search sensitivity; search terms and protocol are listed in Appendix S1. In addition, an online alert strategy was implemented to identify relevant new publications during the review process. The references cited by the selected publications were hand searched. Abstracts of the 2019 and 2020 congresses of the World Federation of Hemophilia, the European Association of Haemophilia and Allied Disorders, and the ISTH were hand searched; these years were selected on the basis that older abstracts would probably have been published by 2020. Key journals (Haemophilia, Journal of Thrombosis and Haemostasis, Research and Practice in Thrombosis and Haemostasis) were screened for relevant studies published after the search date until the analysis was completed on December 7, 2020.
2.3. Study selection
After excluding duplicates, all eligible studies were imported to the Rayyan platform (https://rayyan.qcri.org). 16 All articles were screened using inclusion and exclusion criteria applied first at the title and abstract level, and then at the full article level by two independent reviewers (AS, SC). The reviewers independently scanned the abstract, title, or both, of every record retrieved to determine which studies to assess further. All articles deemed potentially relevant at this stage were reviewed in full text using a blinded protocol. Any discrepancies were resolved through consensus by the two reviewers.
2.4. Data processing
The selected studies were imported to the Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (SUMARI; https://www.jbisumari.org) platform for data extraction, appraisal, assessment of risk of bias, and systematic analysis. Due to heterogeneity of study design, it was not possible to extract quantitative outcomes in a uniform way, and systematic analysis was not feasible. All end points of interest were therefore extracted and summarized. For the systematic review, qualitative studies were assessed according to SUMARI criteria to determine the appropriateness of the study methods to answer the proposed study question and aims, quality of reporting, and validity of findings. Qualitative studies were analyzed separately by identifying common themes (“categories”) that could be synthesized under broader headings and linked to the four outcomes of interest in a meta‐aggregative flowchart.
3. RESULTS
A total of 635 potentially eligible publications were identified, of which 36 were congress abstracts from 2019 and 2020, and one identified from a key journal after the literature search. After review of the titles and abstracts, 35 of these were duplicates or ineligible and 28 publications were selected for analysis (Figure 1). Fifteen were conducted in Europe, 11 in North America, and the remainder in India and Brazil. Potentially relevant studies were excluded largely due to absence of data specifically about women; several recent studies were available only in abstract form and lacked information about methodology and participant characteristics. One study was identified by screening publications in key journals after the date of the systematic review. Four were qualitative studies, five were case‐control studies, 17 were cross‐sectional studies, one was a prospective cohort study, and one was a retrospective review of patient records (Table 1).
FIGURE 1.
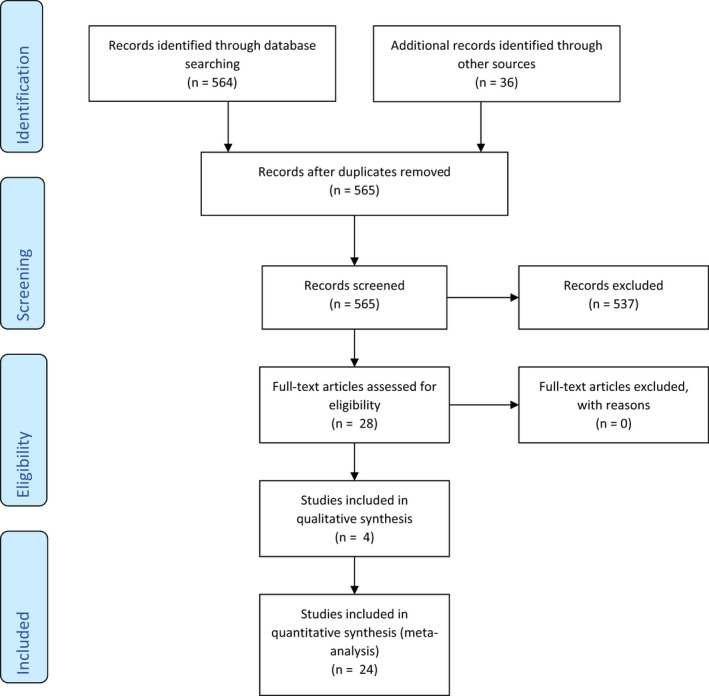
Preferred Reporting Items for Systematic Reviews and Meta‐Analyses flow diagram of search results
TABLE 1.
Studies included in the analysis
| Reference | Design | Study population | Location | N (no. women) | Comparators | End points |
|---|---|---|---|---|---|---|
| [5] | Cross‐sectional | Women with a bleeding disorder attending a treatment center or a member of a patient representative organization | Europe | 709 | … | Impact of bleeding disorder on social life, activities, reproductive choices (locally designed questionnaire) |
| [11] | Cross‐sectional | Adults with moderate or severe von Willebrand disease registered at treatment center | Netherlands | 509 (317F) | General population | Quality of life (SF‐36) |
| [14] | Cross‐sectional | People with von Willebrand disease registered with the national hemophilia registry | Canada | 417 | General population | Quality of life (Health Utility Index), education, menorrhagia, iron status |
| [15] | Qualitative | Women receiving treatment for a bleeding disorder | Canada | 15 | … | Diagnosis, associated symptoms and complications, impact of a bleeding disorder on life, type of care, challenges to the care experience |
| [17] | Qualitative | Members of the Association of Hemophilia Clinic Directors of Canada, the Canadian Association of Nurses in Hemophilia, and the Canadian Physiotherapists in Hemophilia Care | Canada | 157 | … | Access to care, quality of life |
| [18] | Cross‐sectional | Participants in two national clinical trials with autosomal inherited bleeding disorders | Netherlands | 1030 (625 F) | … | Bleeding phenotype, diagnostic delay, treatment |
| [19] | Cross‐sectional | Women diagnosed as hemophilia carriers | India | 47 | … | Stress, anxiety, coping strategies |
| [20] | Cross‐sectional | Patients registered with a bleeding disorder ≥13 years | Canada | 28 (18 F) | … | Quality of life (Health Utilities Index) |
| [21] | Cross‐sectional | Participants in cross‐sectional study with congenital platelet disorder | Netherlands | 156 (126 F) | General population | Quality of life (SF‐36), cognitive and emotional representation of illness (Brief Illness Perception Questionnaire), phenotype |
| [22] | Prospective cohort | People with von Willebrand disease and their families | France | 355 (227 F) | … | Quality of life |
| [23] | Cross‐sectional | Participants in B‐HERO‐S study aged ≥18 y (<18 y represented by caregivers) | United States | 299 (86 F) | – | International Physical Activity Questionnaire, Haemophilia Activities List, Patient Health Questionnaire, Generalized Anxiety Disorder 7‐Item Scale |
| [24] | Cross‐sectional | Participants in B‐HERO‐S study aged ≥18 y (<18 y represented by caregivers) | United States | 299 (86F) | – | Quality of life (EQ‐5D‐5L), Brief Pain Inventory, Haemophilia Activities List, Patient Health Questionnaire, Generalized Anxiety Disorder 7‐Item Scale |
| [25] | Retrospective records review | Adolescents aged 12‐19 y with inherited bleeding disorders registered at a treatment center and attending multidisciplinary hemophilia and gynecology clinic for management of menorrhagia | United Kingdom | 42 | … | Quality of life (locally designed questionnaire) |
| [26] | Cross‐sectional | Women aged 18‐50 y registered with von Willebrand disease | Sweden | 30 | … | Quality of life (SF‐36), bleeding score |
| [27] | Cross‐sectional | Women aged ≥18 y attending a menorrhagia clinic, 10 with von Willebrand disease, 25 with platelet function disorders, 1 with Bernard‐Soulier syndrome | Turkey | 90 | … | Quality of life (Likert scale) |
| [28] | Case‐control | Women with von Willebrand disease, factor XI deficiency, or diagnosed as hemophilia carriers registered at a treatment center | United Kingdom | 99 | Female staff at the same hospital aged 15‐50 y | Health, activities of daily living, dysmenorrhea, quality of life during menstruation (locally designed questionnaire) |
| [29] | Cross‐sectional | Women diagnosed as obligate or potential hemophilia carriers registered at a treatment center | United Kingdom | 197 | … | Experience of pregnancy, attitudes toward reproductive choices |
| [30] | Cross‐sectional | Teenage girls attending a treatment center and women diagnosed as carriers attending an educational meeting | United Kingdom | 47 | … | Impact of having a bleeding disorder socially, psychologically, and on activities; information needs |
| [31] | Case‐control | Women with von Willebrand disease registered at treatment centers | United States | 102 | Friends nominated by participants | Impact of bleeding disorder on activities, social life, depression (Center for Epidemiological Studies Depression Scale) |
| [32] | Case‐control | Women with von Willebrand disease registered at a treatment center | United States | 81 | Volunteers who were menstruating | Quality of life during menstruation (locally designed questionnaire) |
| [33] | Case‐control | Women with factor VII deficiency registered at a treatment center | United Kingdom | 14 | Female hospital staff aged 13‐53 y | Health, activities, dysmenorrhea, quality of life (locally designed scale) |
| [34] | Cross‐sectional | Adolescents and young adults with hemophilia or von Willebrand disease (aged 13‐25 y) recruited through educational meetings, treatment centers, and social media | United States | 108 (18 F) | … | Treatment adherence, pain, quality of life (SF‐36) |
| [35] | Cross‐sectional | People aged 8‐77 y with a bleeding disorder, registered at a treatment center; patients with deep vein thrombosis treated with anticoagulation | Germany | 236 (140 F) | Healthy blood donors | Quality of life (revised KINDer Lebensqualitaetsfragebogen Scale) |
| [36] | Case‐control | Women diagnosed as carriers of bleeding disorder registered at treatment centers | Sweden | 124 | Nominated friends, general population | Quality of life (SF‐36), bleeding |
| [37] | Cross‐sectional | Women diagnosed as hemophilia carriers | Brazil | 74 | … | Phenotype, quality of life, laboratory parameters |
| [38] | Qualitative | Women diagnosed as hemophilia carriers attending treatment centers or educational meeting (mothers represented two children) | Canada | 9 | … | Medical experiences, emotional and behavioral responses |
| [39] | Qualitative | Women diagnosed as carriers who had a son with hemophilia | Norway | 16 | … | Psychosocial aspects of hemophilia carrier status |
| [40] | Cross‐sectional | Adults with von Willebrand disease attending a treatment center | Canada | 105 (80F) | General population | Quality of life (SF‐36), bleeding, laboratory data, iron status |
Abbreviations: B‐HERO‐S, Bridging Hemophilia B Experiences, Results and Opportunities into Solutions; SF‐36, Short Form‐36.
The results of the SUMARI quality appraisal process for the included studies are provided in Table S1. Some recent publications, including the only cohort study included, did not contain sufficient information to meet some criteria because they were abstracts of conference proceedings. 18 , 19 , 22 , 37 The proportion of criteria met by cross‐sectional studies was otherwise moderate or high. Most publications did not document a strategy for managing potential confounding, and some did not use a validated instrument to assess end points or did not make this clear. In case‐control studies, control populations were sometimes selected from hospital staff or patient acquaintances or not matched. The proportion of criteria met by these studies was moderate. The qualitative studies did not include statements locating the researcher culturally or theoretically or, in two studies, stating the influence of the researcher. Overall, the proportion of criteria met by these studies was high.
3.1. Qualitative studies
Three qualitative studies met the inclusion criteria. 15 , 38 , 39 These reported data collected in two countries from 2011 to 2020 (two in Canada and one in Norway) with a total of 42 participants (range, 11‐16). Two studies included only women diagnosed as hemophilia A carriers; the other reported data from women diagnosed with a wide variety of bleeding disorders, including hemophilia B carrier, VWD types 1 and 2, disorders of platelet dysfunction, Glanzmann thrombasthenia, Hermansky‐Pudlak syndrome, and congenital dysfibrinogenemia. The thematic analyses are presented as flow diagrams in Figure 2.
FIGURE 2.
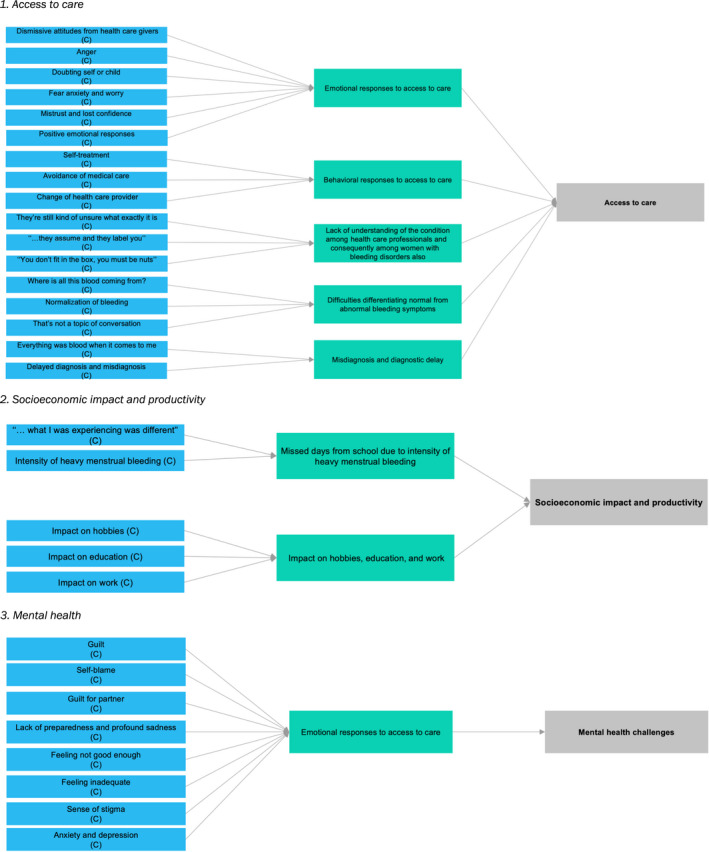
Thematic analysis of qualitative studies. (C denotes “category” in the SUMARI analysis –that is, the first step in thematic analysis)
The review question is addressed by three key themes: (i) access to care, (ii) socioeconomic impact and productivity, and (iii) mental health.
3.2. Theme 1: Access to care
The experiences surrounding access to care varied between studies. Many experiences discussed by participants were negative, the majority highlighting dismissive caregiver attitudes, which resulted in a variety of emotional and behavioral responses. 38 It was highlighted that women experienced four times more negative responses than positive; anger was among the emotional responses women expressed.
I was just so angry. I was angry with myself, I was angry with them because despite my trying to follow up, people just kept saying this is normal. [38, p. 240]
Women described a range of responses, from self‐advocacy and taking their own precautions, to partial or complete avoidance of health care systems. Negative experiences were amplified by the collective experience of the family and hemophilia community. The proposed explanations for these experiences were most often associated with a lack of information and knowledge among health care providers about symptoms related to bleeding. Others included a tendency to downplay symptoms, reluctance to discuss gynecological or obstetrical bleeding, insufficiencies in management policies and protocols, and trivialization of “women’s issues” by some physicians.
Uncertainties surrounding diagnosis are also potential barriers to access to care. Irrespective of their underlying diagnosis, women described challenges associated with distinguishing between normal and abnormal bleeding, especially vaginal bleeding. 15 Women have also experienced difficulty with diagnostic labels, misdiagnoses, and diagnostic delay.
It was even after [my geneticist appointment] that I was given the referral to go to [the specialist center]. So, I could probably, it was easily, say, a year before I even saw someone. [15, p. 5]
Women felt that use of labels such as “carrier” was dismissive, representing an attitude that did not fully acknowledge their bleeding experiences. Similarly, some felt they struggled because their symptoms did not readily fit into a diagnostic category, leading to underrecognition and undertreatment. Often, women stated that they were diagnosed only after a bleeding disorder was identified in a male relative; because female family members had normalized excessive bleeding, it was difficult for them to understand their own symptoms.
3.3. Theme 2: Socioeconomic impact and productivity
Women reported excessive bleeding ranging from mild to severe or life threatening. Many described an inability to engage with recreational activities, school, or work due to the intensity of menstrual bleeding. Some reported a loss of days at school or work, but this was not a uniform finding.
It was hard to be in school. It was hard to concentrate. I used to collapse a lot. I would just be walking down the street, and I would just collapse because I had low iron. [15, p. 7]
One participant highlighted not being able to work and having financial difficulties.
I lost my job, I lost my apartment. I’m still struggling financially… [15, p. 8]
3.4. Theme 3: Mental health
Women said that their feelings of guilt and self‐blame had been evident in generations of women beforehand. Some described significant emotional distress, including anxiety and depression, and feelings of confusion and a sense of failure arising from their reproductive decisions; they also felt sad for their partners.
I had such a guilty conscience because my boyfriend ended up with me who gave him a son with an illness. It was my fault. [39, p. 1327]
Feelings of sadness and shock were also relived by women diagnosed as hemophilia carriers when their children were diagnosed with hemophilia. Some felt different and alienated by their bleeding disorder, and this sense of stigma was highlighted by the way they were treated.
When I was younger, I actually got bullied a lot because they would say, “Don’t touch [her] or she’ll bruise” or “We don’t want you on our team because you’re just going to get injured.” [15, p. 8]
The mental health challenges experienced by women, from minimal to severe, were evident at varying points throughout their lives. They felt isolated and alone but found support and understanding through affiliation with a community of other women with bleeding disorders and their families, leading to “positive feelings” such as “a sense of empowerment, understanding, and acceptance” and feeling closer to family members. 15
3.5. Quantitative studies
3.5.1. Theme 1: Access to care
Aspects of access to care for women were addressed in three studies. 17 , 18 , 24 , 29
In a survey of people with bleeding disorders (mainly VWD) in the Netherlands, women were more often referred for bleeding than men (46.1% vs 34.3%; (P < .001). 17 Mean age at referral was not different (9.1 ± 13.0 years for men vs 10.8 ± 11.1 years for women; P = .23) but mean age at diagnosis was much lower in men (18.0 ± 19.5 years vs 25.4 ± 19.3 years (P < .001). This meant that women encountered substantially longer diagnostic delay (14.0 ± 16.6 years vs 8.1 ± 17.0 years; P < .001). In this study, the bleeding score was lower in women (9.7 ± 6.9 vs 11.6 ± 7.3; P < .001) but “after deduction of sex‐specific bleeding,” the score was numerically higher in men (9.7 ± 6.9 vs 8.8 ± 6.1; P = .05). This distinction between bleeding and “sex‐specific bleeding” raises the possibility that menstrual bleeding may be underrecognized when assessing the impact of bleeding disorders on women.
Questionnaire responses from health care professionals showed that 42% believed women with inherited bleeding disorders experience less access to care as compared to men, without qualifying what “less” meant. 17 Thirty‐four percent stated this not to be the case, and 24% were unsure. A large survey of women (n = 625) and men (n = 405) with VWD or a rare bleeding disorder found that a greater proportion of women were referred for bleeding (46% vs 34%; P < .001); however, although the mean age at referral was similar (10.8 vs 9.1 years), mean age at diagnosis was lower for men (18.0 vs 25.4 years; P < .001). 18 Mean diagnostic delay was therefore shorter in men (8.1 vs 14.0 years; P < .001) even though their mean bleeding score was lower (9.7 vs 11.6; P < .001).
In a cross‐sectional US study in which respondents noted difficulties accessing factor for replacement therapy in the preceding 5 years due to availability and/or affordability, the problem was more prevalent among women than men (72% vs 44%) (n=299 adults with hemophilia B). 24 Health professionals stated the main barriers to accessing care were lack of awareness about what constitutes abnormal bleeding among women (90% of respondents) and among health professionals (73%). 17 Others were lower likelihood of referral to a hematologist (47%), stigma associated with vaginal bleeding (29%), and women’s focus on male family members with hemophilia rather than themselves (20%).
This study also found that distance from a bleeding disorders clinic or hematology department was a barrier to accessing care, a finding echoed in a survey of women considering reproductive choices. 29 This survey of 197 women labeled as hemophilia carriers found that living close to a hemophilia center that offered counseling and prenatal diagnostic tests was a factor in the decision to have children in 14% of first pregnancies and 10% of subsequent pregnancies.
3.6. Theme 2: Socioeconomic factors and productivity
3.6.1. Productivity
Five studies described the impact of a bleeding disorder on an aspect of productivity. 24 , 26 , 31 , 32 , 33
Menstruation has been consistently associated with work impairment among women with a bleeding disorder. In women with VWD, one study (n = 30) found that 46% reported a negative impact of menstruation on ability to work, and 36% reported a negative impact on their ability to carry out housework. 26 A second (n = 102) reported that 37% of women (vs 10% of controls; P = .004) said their menstrual period limited routine work and social activities and had a negative effect on life. 31 In a third study (n = 81), women with VWD rated their ability to attend work or school worse than controls (mean 3.1 ± 3.3 vs 0.1 ± 0.4 on a 5‐point Likert scale where higher score indicates worse impact; P = .0001). 32 Forty‐six percent said they had lost time from work or school in the preceding 12 months due to menorrhagia (median, 4 days; range, 1‐24).
In 14 women with factor VII deficiency, 86% reported they had reduced time spent on work during their menstrual period, and 71% said they had accomplished less than they would like and were limited in the kind of work or other activities they could do. 33 Ten women (71%) reported difficulty carrying out work or other activities during their period. Dysmenorrhea (P = .02) and the interference with daily work (P = .001) were more frequent than among controls. Half of the women with factor VII deficiency reported severe or very severe dysmenorrhea; 43% felt that pain interfered “quite a bit” or “extremely” with their normal work.
There are few data on income among women with a bleeding disorder. The Bridging Hemophilia B Experiences, Results and Opportunities into Solutions (B‐HERO‐S) study reported that there was little difference between men and women with hemophilia B in the United States in the proportion with a household income of ≥$100 000 (29% vs 33%) but the proportion was higher for girls than boys (60% vs 41%). 24 The proportion receiving disability benefits was higher for both women (57% vs 40%) and girls (45% vs 18%). The statistical significance of these differences was not reported.
3.7. Socioeconomic factors
Ten studies assessed the socioeconomic impact of bleeding disorders on women. 5 , 14 , 23 , 25 , 26 , 27 , 28 , 30 , 32 , 33
Not all papers identified a specific cause of socioeconomic impairment; of those that did, heavy menstrual bleeding was the most frequently reported. 25 , 26 , 28 , 31 , 33 In part, this was because menstruation was a focus of the study. Heavy menstrual bleeding affected all aspects of life. In adolescent girls, it limited the activities they could carry out, the time spent doing them, and their accomplishments. 25 They also reported missing school, but most reported no activity impairment after treatment for the bleeding disorder. About half to three‐quarters of women with VWD reported that menstruation impaired family life, holidays, leisure, sex life, social relations and daily activities; 32% stated they were confined to bed for at least half a day during menstruation. 26
Another survey found that half of 14 women with congenital factor VII deficiency felt menstruation limited vigorous activities (running, lifting heavy objects, and walking more than a mile) “a lot,” though only one reported being limited a lot during menstruation. 33 The median total health and daily activity score was not different from controls overall (P = .05), but fewer women with factor VII deficiency reported no interference with health and daily activity (1 vs 15; P = .0002) and no interference of dysmenorrhea with work (2 vs 11; P = .001). This study group had earlier reported a larger survey (n = 99 women with a bleeding disorder and 69 controls), which found that 25% of affected women and 10% of controls described limitation of all activities during menstruation (P = .004) and a slightly higher proportion were limited a lot in vigorous activities (27% vs 22%; statistical significance not reported). 29 In this study, severe (16% vs 4.4%) and very severe dysmenorrhea (8.3% vs 0%) were more prevalent among women with a bleeding disorder than controls (P = .001 for overall impact of dysmenorrhea in women with a bleeding disorder vs controls), and this corresponded with interference with daily work “quite a bit” (21% vs 5.8%) and “extremely” (5.3% vs 0%) (P = .001 for overall impact).
In a US survey, “excessive bleeding symptoms” were reported by 74% of 102 women with VWD and by 6% of controls (P < .01), 31 and they reported significantly greater limitation of social activities and lifestyle, including routine work and social activities limited by menstruation (37% vs 10%; P = .004). Even those who reported no activity limitation said menstruation had a negative impact on life (32% vs 16%; statistical significance not reported). In this survey, more women with VWD experienced heavy menstrual bleeding (44% vs 17% of controls; P = .01). Women with type 1 VWD (n = 81) self‐rated the impact of menses on quality of life significantly worse than controls for the domains of general activity, ability to attend work or school, family activities, ability to enjoy life, sleep, and mood. 32 Among women with bleeding disorders (n = 315), menorrhagia was associated with lower scores for cognition (P < .001), and impairment of daily activities was significantly more prevalent than it was among women not reporting menorrhagia (78% vs 43%; P < .001). 14
By contrast, the B‐HERO‐S study (including 86 women with hemophilia B) reported no differences between men and women in either overall or composite Haemophilia Activities List scores. 23 In a comparison of women with VWD with women with other bleeding disorders, absence from work or school was higher in women with VWD, but the difference was not statistically significant (54% vs 37%; P = .123). 27
Even when not specifically singled out as a contributory factor, heavy menstrual bleeding was common. Of 45 girls and young women with a bleeding disorder, 80% said they experienced heavy and prolonged periods. 30 In a subgroup of 27 respondents, 80% reported limitation of sports participation, 48% getting tattooed or pierced, and 30% traveling abroad, with 1 to 4 respondents noting limitations on socializing and relationships. Pain during menstruation was specifically identified. Severe pain was described more frequently in women with VWD than other women with menorrhagia, some of whom had a platelet function disorder (data not reported; P = .002). 27 Among 24 girls and young women with a bleeding disorder, aged 12 to 19 years, moderate to severe pain during menstruation was reported by 88% before treatment and by 17% after treatment (statistical significance not reported). 25 Moderate to severe pain during menstruation was more prevalent among women with a bleeding disorder who reported menorrhagia than among those who did not (64% vs 46%; P = .02). 14
A survey of 709 women with a bleeding disorder in 32 European countries found significantly greater impact on physical life (P < .01), social and romantic life (P < .01), and active life (P < .01) among women with no known family history compared with those with a family history of a bleeding disorder. 5 Precise figures are not available in the published report because the findings are described graphically. There were no consistent differences between women diagnosed as a hemophilia carrier with low or high factor VIII activity (<40% vs >40%). More women with bleeding disorders other than hemophilia reported an impact on these aspects of life, with small differences in the severity of impact. However, most women reported that their condition had an impact on their decision to have children or prevented them from doing so, with the prevalence of severe impact ranging from 19% of women diagnosed as a hemophilia carrier with level <40% IU/dL to 38% of those with other factor deficiencies or combined deficiencies.
3.8. Theme 3: Mental health
Thirteen studies reported mental health outcomes. 19 , 20 , 22 , 23 , 24 , 26 , 30 , 31 , 32 , 35 , 36 , 37 , 40
Several reported reductions in the mental health domain of the health‐related quality‐of‐life instrument Short Form‐36. Compared with normative data, women with VWD reported significant reductions (P < .05) in all domain components except “role emotional,” including vitality, mental health, and mental component summary; iron deficiency was one of the contributory factors. 40 The mental component score was also reduced compared with controls in women diagnosed as hemophilia carriers and in the subgroup with a bleeding tendency (P = .05 for both comparisons); however, there were no significant differences in the individual domains. 36 In 355 people with VWD recruited to a French study, the mental component summary score at baseline was lower among women than men (no statistical significance was reported). 22 This finding was also reported in a study in Brazil, though it is unclear what the comparator group was. 37
Although one US study found no excess of depression among women with VWD compared with controls, 31 most studies have reported that mood is adversely affected in women with a bleeding disorder. Women with type 1 VWD rated their ability to enjoy life, sleep, and mood worse than controls (P < .0001). 32 Menstruation was associated with mood changes in 91% of women with VWD and with anxiety in 63%. 26 In a survey in India (n = 47), 74% of women diagnosed as a hemophilia carrier reported a moderate level of stress and anxiety, and 15% reported major stress and anxiety. 19 The utility scores for emotion, pain, and cognition were identified as the major contributors to reduced quality‐of‐life scores in women compared with men in people with VWD (n = 28). 20
In the B‐HERO‐S study, women with hemophilia B more frequently reported anxiety (43% vs 15%) or depression (42% vs 14%) than men (statistical significance not reported). 24 Women had a higher median depression score (Patient Health Questionnaire) and more had mild (20% vs 16%) or moderate depression (60% vs 29%) than men; however, more men had moderately severe (6% vs 3%) or severe depression (1% vs 0%) (statistical significance not reported). 23
Two studies have assessed the impact of a bleeding disorder on mental health differently. A UK survey of girls and young women attending a treatment center clinic identified psychological trauma due to being bullied or stigmatized in 11% to 16%. 30 One girl expressed concern about taking a hormonal contraceptive as treatment for menorrhagia in case it was perceived as being prescribed “for sexual reasons.” Most participants did not know anyone outside their family who had a bleeding disorder, and half expressed a desire to meet others, suggesting some may experience isolation.
The second study compared 74 children and adolescents with a bleeding disorder plus 12 siblings and 35 peers; 82 adults with a bleeding disorder; 198 adults receiving treatment with an anticoagulant for deep vein thrombosis; and, as controls, 1011 healthy blood donors. 35 Outcomes were not reported by sex for children and young people. Friend‐related quality of life was reduced less among women with a bleeding disorder compared with those taking an anticoagulant (P = .04); it is unclear how generalizable this finding is to other comparisons.
4. DISCUSSION
This review has found consistent evidence that the lived experience of women with bleeding disorders is challenging. Although our review spanned >20 years, we found many of the problems identified in 1998 were still being reported in 2020. Women face obstacles with access to care, difficulties living with the socioeconomic impact of their disorder and its effects on work and schooling, and poor mental health. For example, Kadir et al 28 found in 1998 that health and daily activity was significantly worse in women with inherited bleeding disorders compared with controls and that this limited time spent on work and other activities; and Arya et al 15 in 2020 reported that women experienced embarrassment and reduced quality of life due to heavy menstrual bleeding. Diagnosis of bleeding disorders in women is delayed; treatment and support are not offered because their symptoms are unacknowledged. The practice of describing women with hemophilia as “carriers”—a term that both implies fault for passing the bleeding disorder on to children and diminishes the burden of excessive bleeding—is a persistent failing.
Heavy menstrual bleeding interferes with work and social life, and low mood and poor mental health are more common than among controls. Women with bleeding disorders experience stigma, and they feel guilt and sadness, even with a family history of excessive bleeding stretching back several generations. Some report experiences indicating that their importance is considered secondary to men and boys with a bleeding disorder. Where comparisons with controls are made, there is evidence that the negative experiences of women are often greater than those of men with bleeding disorders or samples from the general population.
We found only three qualitative studies with findings relevant to the defined outcomes. Common weaknesses included limited discussion of researcher positionality or reflexivity, limited detail on research methodology, and limited discussion of strengths and limitations or recommendations for future research or practice. However, the studies met most of the SUMARI quality appraisal criteria and therefore provide a valuable insight into women’s experience of living with a bleeding disorder, which supports the conclusion that their medical management is tainted by sexism. 41
Quantitative studies described a variety of methodologies and end points that could not be unified into a single outcome. The majority of included quantitative studies met the SUMARI quality criteria. The weakest areas were specifying strategies to deal with possible confounding (met by 26% of studies) and using objective and standard criteria to measure the outcome (58%). Almost all clearly defined their inclusion criteria, and 74% to 79% provided adequate information about participants, measures used for exposure and outcomes, and statistics. Case‐control studies identified controls from local populations (eg, a small number of hospital staff or friends of participants), but most did not report matching and may therefore be subject to bias by failing to account for potential confounders such as social and economic factors.
The review therefore confirms that the findings of individual studies have been consistent over time. However, it could not provide a quantitative estimate of the impact on the outcomes of interest (access to care, socioeconomic impact, mental health) in a form suitable for comparison with other groups of resource users or for estimating health economic parameters.
4.1. Limitations
The review was limited to studies published in the English language and included in three biomedical databases or accepted for participation in major hematology conferences. We restricted our search of conference abstracts to those published after 2019, assuming that earlier studies would have been published within 2 years, though this may not always have been the case. We did not seek further data from authors when the published report lacked information. We found only three qualitative studies with our defined outcomes, only one of which included socioeconomic data. The conclusions should therefore be interpreted cautiously.
5. CONCLUSION
This review provides a clear picture that the lived experience of women with bleeding disorders is negatively affected by lack of support from health providers, underplaying the impact of their disorder, interference with daily life, and emotional suffering. The evidence base is consistent but is not suitable for meta‐analysis. There is a need for further studies to confirm these findings.
RELATIONSHIP DISCLOSURE
MH, KK, and DP are employees of the Haemnet Foundation.
AUTHOR CONTRIBUTIONS
AS and SC conducted the review and drafted the manuscript. All authors contributed to the critical review of the manuscript.
Supporting information
Table S1
Supplementary Material
ACKNOWLEDGMENTS
This review is part of the Cinderella study, which was funded by CSL Behring.
Sanigorska A, Chaplin S, Holland M, Khair K, Pollard D. The lived experience of women with a bleeding disorder: A systematic review. Res Pract Thromb Haemost. 2022;6:e12652. doi: 10.1002/rth2.12652
Handling Editor: Dr Suzanne Cannegieter
Contributor Information
Anna Sanigorska, Email: anna.sanigorska@nhs.net.
Mike Holland, @mikeholland360.
Kate Khair, @katekhair.
Debra Pollard, @Debra_PollardRN.
REFERENCES
- 1. UK Haemophilia Centres Doctors Organisation . UKHCDO Annual Report 2019. October 2019.
- 2. Leebeek FW, Eikenboom JC. Von Willebrand's disease. N Engl J Med. 2016;375(21):2067‐2080. [DOI] [PubMed] [Google Scholar]
- 3. Bowman M, Hopman WM, Rapson D, Lillicrap D, James P. The prevalence of symptomatic von Willebrand disease in primary care practice. J Thromb Haemost. 2010;8(1):213‐216. [DOI] [PubMed] [Google Scholar]
- 4. Bolton‐Maggs PH, Perry DJ, Chalmers EA, et al. The rare coagulation disorders–review with guidelines for management from the United Kingdom Haemophilia Centre Doctors’ Organisation. Haemophilia. 2004;10:593‐628. [DOI] [PubMed] [Google Scholar]
- 5. Noone D, Skouw‐Rasmussen N, Lavin M, et al. Barriers and challenges faced by women with congenital bleeding disorders in Europe: results of a patient survey conducted by the European Haemophilia Consortium. Haemophilia. 2019;25:468‐474. [DOI] [PubMed] [Google Scholar]
- 6. Von Mackensen S. Quality of life in women with bleeding disorders. Haemophilia. 2011;17(suppl 1):33‐37. [DOI] [PubMed] [Google Scholar]
- 7. Plug I, Mauser‐Bunschoten EP, Bröcker‐Vriends AH, et al. Bleeding in carriers of hemophilia. Blood. 2006;108(1):52‐56. [DOI] [PubMed] [Google Scholar]
- 8. Peyvandi F, Garagiola I, Menegatti M. Gynecological and obstetrical manifestations of inherited bleeding disorders in women. J Thromb Haemost. 2011;9(suppl 1):236‐245. [DOI] [PubMed] [Google Scholar]
- 9. Wolf S, Sardo Infirri S, Batty P, Sahar B, Beski S, Bowles L. Postpartum bleeding in women with inherited bleeding disorders: a matched cohort study. Blood Coagul Fibrinolysis. 2020;31(7):452‐458. [DOI] [PubMed] [Google Scholar]
- 10. Kadir RA, Economides DL, Sabin CA, Pollard D, Lee CA. Assessment of menstrual blood loss and gynaecological problems in patients with inherited bleeding disorders. Haemophilia. 1999;5(1):40‐48. [DOI] [PubMed] [Google Scholar]
- 11. de Wee E, Knol H, Mauser‐Bunschoten E, et al. Gynaecological and obstetric bleeding in moderate and severe von Willebrand disease. Thromb Haemost. 2011;106(11):885‐892. [DOI] [PubMed] [Google Scholar]
- 12. Ay C, Perschy L, Rejtö J, Kaider A, Pabinger I. Treatment patterns and bleeding outcomes in persons with severe hemophilia A and B in a real‐world setting. Ann Hematol. 2020;99(12):2763‐2771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. von Mackensen S, Myrin Westesson L, Kavakli K, et al. The impact of psychosocial determinants on caregivers’ burden of children with haemophilia (results of the BBC study). Haemophilia. 2019;25:424‐432. [DOI] [PubMed] [Google Scholar]
- 14. Rae C, Furlong W, Horsman J, et al. Bleeding disorders, menorrhagia and iron deficiency: impacts on health‐related quality of life. Haemophilia. 2013;19(3):385‐391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Arya S, Wilton P, Page D, et al. “Everything was blood when it comes to me”: understanding the lived experiences of women with inherited bleeding disorders. J Thromb Haemost. 2020;18(12):3211‐3221. doi: 10.1111/jth.15102 [DOI] [PubMed] [Google Scholar]
- 16. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan — a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi: 10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Arya S, Wilton P, Page D, et al. Healthcare provider perspectives on inequities in access to care for patients with inherited bleeding disorders. PLoS One. 2020;15(2):e0229099. doi: 10.1371/journal.pone.0229099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Atiq F, Saes JL, Meijer K, et al. Important sex differences in patients with autosomal inherited bleeding disorders. ISTH 2020 Congress. Abstract Number: PB1202 https://abstracts.isth.org/abstract/important‐sex‐differences‐in‐patients‐with‐autosomal‐inherited‐bleeding‐disorders/
- 19. Badagabettu S, Kurien A, Noronha A, et al. Psycho‐social status and coping strategies among women carrier for hemophilia ‐ A Descriptive Study from India. International Society on Thrombosis and Haemostasis Congress. Melbourne, July 2019. Oral abstracts. NUR 01.2.
- 20. Barr RD, Sek J, Horsman J, et al. Health status and health‐related quality of life associated with von Willebrand disease. Am J Hematol. 2003;73:108‐114. [DOI] [PubMed] [Google Scholar]
- 21. Blaauwgeers MW, Kruip MJHA, Beckers EAM, et al.; TiN study group . Congenital platelet disorders and health status‐related quality of life. Res Pract Thromb Haemost. 2019;4:100‐105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Borel Derlon A, Goudemand J, Deprez D, et al. WISH‐QoL Study: assessment of health‐related quality of life and health‐economic aspects in patients with von Willebrand disease in France: results from the 2nd interim analysis on the 355 enrolled patients ISTH virtual congress 2020. Abstract PB1553
- 23. Buckner TW, Witkop M, Guelcher C, et al. Impact of hemophilia B on quality of life in affected men, women, and caregivers—assessment of patient‐reported outcomes in the B‐HERO‐S study. Eur J Haematol. 2018;100:592‐602. [DOI] [PubMed] [Google Scholar]
- 24. Buckner TW, Witkop M, Guelcher C, et al. Management of US men, women, and children with hemophilia and methods and demographics of the Bridging Hemophilia B Experiences, Results and Opportunities into Solutions (B‐HERO‐S) study. Eur J Haematol. 2017;98(suppl 86):5‐17. [DOI] [PubMed] [Google Scholar]
- 25. Chi C, Pollard D, Tuddenham EG, et al. Menorrhagia in adolescents with inherited bleeding disorders. J Pediatr Adolesc Gynecol. 2010;23:215‐222. [DOI] [PubMed] [Google Scholar]
- 26. Govorov I, Ekelund L, Chaireti R, et al. Heavy menstrual bleeding and health‐associated quality of life in women with von Willebrand’s disease. Exp Ther Med. 2016;11:1923‐1929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Hacioglu S, Karabulut A, Sari I, et al. Haemostatic disorders in reproductive age women with menorrhagia and effects on quality of life. J Obstet Gynaecol. 2016;36:1041‐1045. [DOI] [PubMed] [Google Scholar]
- 28. Kadir RA, Sabin CA, Pollard D, et al. Quality of life during menstruation in patients with inherited bleeding disorders. Haemophilia. 1998;4:836‐841. [DOI] [PubMed] [Google Scholar]
- 29. Kadir RA, Sabin CA, Goldman E, Pollard D, Economides DL, Lee CA. Reproductive choices of women in families with haemophilia. Haemophilia. 2000;6:33‐40. [DOI] [PubMed] [Google Scholar]
- 30. Khair K, Holland M, Pollard D. The experience of girls and young women with inherited bleeding disorders. Haemophilia. 2013;19:e276‐e281. [DOI] [PubMed] [Google Scholar]
- 31. Kirtava A, Drews C, Lally C, et al. Medical, reproductive and psychosocial experiences of women diagnosed with von Willebrand’s disease receiving care in haemophilia treatment centres: a case‐control study. Haemophilia. 2003;9:292‐297. [DOI] [PubMed] [Google Scholar]
- 32. Kouides PA, Phatak PD, Burkart P, et al. Gynaecological and obstetrical morbidity in women with type I von Willebrand disease: results of a patient survey. Haemophilia. 2000;6:643‐648. [DOI] [PubMed] [Google Scholar]
- 33. Kulkarni A, Lee CA, Griffeon A, et al. Disorders of menstruation and their effect on the quality of life in women with congenital factor VII deficiency. Haemophilia. 2006;12:248‐252. [DOI] [PubMed] [Google Scholar]
- 34. McLaughlin JM, Munn JE, Anderson TL, et al. Predictors of quality of life among adolescents and young adults with a bleeding disorder. Health Qual Life Outcomes. 2017;15:67. doi: 10.1186/s12955-017-0643-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Nowak‐Göttl U, Clausnizer H, Kowalski D, et al. Health‐related quality of life in children, adolescents and adults with hereditary and acquired bleeding disorders. Blood Cells Mol Dis. 2017;67:96‐101. [DOI] [PubMed] [Google Scholar]
- 36. Olsson A, Hellgren M, Berntorp E, et al. Association between bleeding tendency and health‐related quality of life in carriers of moderate and severe haemophilia. Haemophilia. 2015;21:742‐746. [DOI] [PubMed] [Google Scholar]
- 37. Pastori MS, Stefanelli A, Siqueira LH, et al. Clinical and laboratory evaluation of female carriers of hemophilia. ISTH 2019 poster abstracts. PB0695.
- 38. Renault NK, Howell RE, Robinson KS, et al. Qualitative assessment of the emotional and behavioural responses of haemophilia A carriers to negative experiences in their medical care. Haemophilia. 2011;17:237‐245. [DOI] [PubMed] [Google Scholar]
- 39. von der Lippe C, Frich JC, Harris A, et al. “It was a lot tougher than I thought it would be.” A qualitative study on the changing nature of being a hemophilia carrier. J Genet Couns. 2017;26:1324‐1332. [DOI] [PubMed] [Google Scholar]
- 40. Xu Y, Deforest M, Grabell J, et al. Relative contributions of bleeding scores and iron status on health‐related quality of life in von Willebrand disease: a cross‐sectional study. Haemophilia. 2017;23:115‐121. [DOI] [PubMed] [Google Scholar]
- 41. Weyland AC, James PD. Sexism in the management of bleeding disorders. Res Pract Thromb Haemost. 2021;5(1):51‐54. doi: 10.1002/rth2.12468 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1
Supplementary Material