

Abstract
This study examines SARS-CoV-2 infections detected in close contacts of confirmed cases within the Olympic Village at the 2021 Tokyo Olympic and Paralympic Games.
The Tokyo 2020 Olympic and Paralympic Games were held in the summer of 2021, despite concerns about SARS-CoV-2 transmission.1,2 We assessed SARS-CoV-2 infections detected in close contacts of confirmed cases within the Olympic and Paralympic Village.
Methods
All participants (such as athletes, coaches, medical staff, physical therapists, and Paralympic companions) were required to test negative for SARS-CoV-2 prior to departure from their country of origin. COVID-19 vaccination was recommended but not mandatory. All individuals were tested with a SARS-CoV-2 saliva antigen test on airport arrival in Japan and were moved to the Village immediately if results were negative.
Several public health measures were implemented to control SARS-CoV-2 transmission in the Village, including behavioral interventions such as mask wearing.3 Almost all participants were required to stay in the Village except during training and competitions. All participants had laboratory-based saliva antigen screening every morning. Those with a positive screening result had a confirmatory nasopharyngeal polymerase chain reaction (PCR) test. Individuals with positive PCR test results were moved to isolation hotels outside of the Village, with no contact with others allowed.
Data on close contacts of participants whose test results were positive were collected in the area for testing of close contacts in the Village (hereafter referred to as the Area) from July 13, 2021, to August 11, 2021, for the Olympic Games and from August 17, 2021, to September 8, 2021, for the Paralympic Games. Close contacts were identified according to the guidance of the Ministry of Health, Labour and Welfare, Japan (within 6 ft for 15 consecutive minutes, which is the same as the World Health Organization guidance4) by public health center staff working with the Tokyo 2020 Organising Committee, following the same procedures used across Japan. Close contacts were required to stay in designated accommodations in the Village, and nasopharyngeal swabs were collected daily for SARS-CoV-2 PCR testing for 14 days. We describe the incidence of testing and positive cases among close contacts. Neither institutional review board approval nor informed consent was necessary in accordance with the Act on the Prevention of Infectious Diseases and Medical Care for Patients With Infectious Diseases (the Infectious Diseases Control Law) in Japan.
Results
At the airport, 54 250 SARS-CoV-2 tests were conducted for arriving participants, with 55 individuals with positive test results confirmed by nasopharyngeal SARS-CoV-2 PCR testing (0.10%) who were moved to quarantine isolation facilities.5 Among 1 014 170 screening tests conducted during the Olympics and Paralympics, 299 were confirmed to have positive results (0.03%).5
Approximately 11 000 participants stayed in the Village during the Olympics and 4400 during the Paralympics; 3426 SARS-CoV-2 PCR tests for close contacts were conducted in the Area (0.34% of all screening tests conducted) and 15 results were confirmed positive (0.44%; 7 of 1508 tests during the Olympics [0.46%] and 8 of 1918 tests during the Paralympics [0.42%]; Figure). The number of SARS-CoV-2 PCR tests for close contacts increased after the opening of both the Olympics and Paralympics. For the Olympics, the number of SARS-CoV-2 PCR tests increased from 70 on opening day (day 1), reached a peak of 142 on day 5, and then decreased. For the Paralympics, the number of SARS-CoV-2 PCR tests increased from 122 on day 1 to a peak of 166 on day 5, decreasing to 33 on the final day. The 15 positive cases were distributed across the duration of the Olympics and Paralympics, with no major clusters.
Figure. Daily SARS-CoV-2 Tests for Close Contacts in Dedicated Testing Area in the Olympic and Paralympic Village in Tokyo.
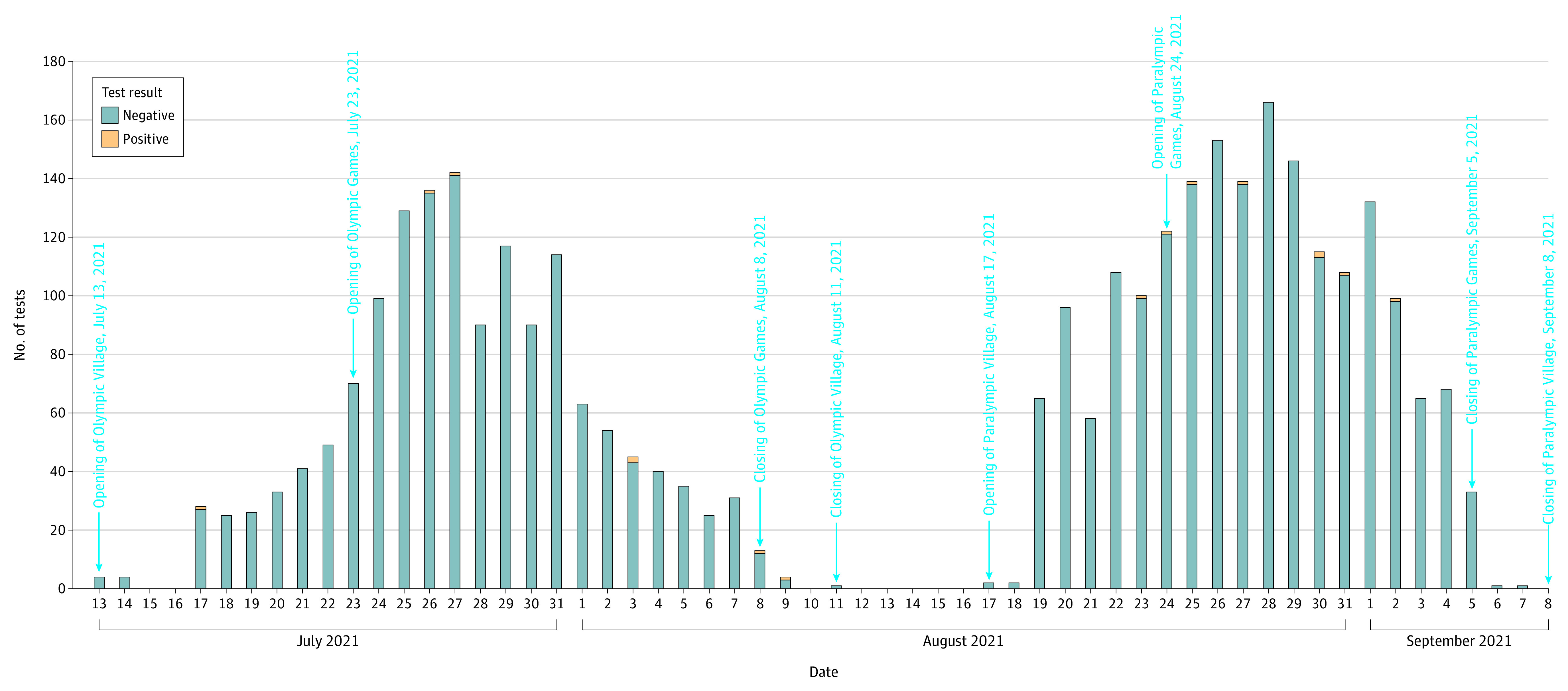
Close contacts who tested positive were retested by nasopharyngeal polymerase chain reaction (PCR) testing. Those with negative PCR results could reenter the Village. If they tested positive again by daily saliva antigen screening, they had to take another nasopharyngeal PCR test.
Discussion
The number of close contacts of participants with SARS-CoV-2 after the opening of the Olympics and Paralympics increased, but few positive cases were identified. The increasing numbers of SARS-CoV-2 PCR tests of close contacts likely were a consequence of new overseas arrivals to the Village who were identified as close contacts of a positive case on an inbound flight and some close contacts of positive cases returning to the Village from various training camps across Japan. More close contacts were tested during the Paralympics because the participants had to move together in close groups.
A limitation of the study is not including participants staying outside the Village, although the numbers were very small. The public health control measures at the Tokyo Olympics and Paralympics worked well to prevent COVID-19 clusters inside the Village, despite a surge in new COVID-19 cases recorded in Tokyo during that time.
Section Editors: Jody W. Zylke, MD, Deputy Editor; Kristin Walter, MD, Associate Editor.
References
- 1.Shimizu K, Sridhar D, Taniguchi K, Shibuya K. Reconsider this summer’s Olympic and Paralympic games. BMJ. 2021;373(n962):n962. doi: 10.1136/bmj.n962 [DOI] [PubMed] [Google Scholar]
- 2.Sparrow AK, Brosseau LM, Harrison RJ, Osterholm MT. Protecting Olympic participants from COVID-19: the urgent need for a risk-management approach. N Engl J Med. 2021;385(1):e2. doi: 10.1056/NEJMp2108567 [DOI] [PubMed] [Google Scholar]
- 3.The Playbook: Athletes and Officials. International Olympic Committee and International Paralympic Committee; 2021. [Google Scholar]
- 4.World Health Organization . Global surveillance for COVID-19: interim guidance. Published December 16, 2020. Accessed January 28, 2021. https://www.who.int/publications/i/item/who-2019-nCoV-surveillanceguidance-2020.7
- 5.Tokyo 2020 Organising Committee . Review of Tokyo 2020. Published December 22, 2021. Accessed January 14, 2022. https://www.tokyo2020.jp/ja/%E6%9D%B1%E4%BA%AC2020%E5%A4%A7%E4%BC%9A%E3%81%AE%E6%8C%AF%E3%82%8A%E8%BF%94%E3%82%8A%E3%81%AB%E3%81%A4%E3%81%84%E3%81%A6.pdf