

Guatemala is an upper-middle-income country of 16.4 million people located in Central America (1). The gross domestic product in Guatemala is 76 billion USD. In 2014, health financing (public and private) represented 6% of gross domestic product, and the proportion of government expenditure on health was only around 35% of the total health expenditure. In 2019, approximately 19 million USD per year was destined for kidney care in the public health sector. The Guatemalan Ministry of Health (MoH) is financed through general government revenues (taxes) (2). Around 50% of the Guatemalan population are indigenous Maya people who live in rural communities, where access to healthcare, including kidney care and dialysis, is limited (3,4). The Pan American Health Organization estimated that mortality due to chronic kidney failure in Guatemala in 2008 was 13.6 per 100,000 people, one of the highest rates in the Americas (5).
In 1964, the first Guatemalan nephrologist, Dr. César Augusto Vargas Monterroso, returned after completing his training at Walter Reed National Military Medical Center in the United States. It was not until 1975 that the first hemodialysis (HD) service was created in the Instituto Guatemalteco de Seguridad Social (IGSS; Guatemalan Institute of Social Security). However, the true rise and development of the HD technique were promoted when IGSS introduced freestanding dialysis centers in 1996. This program was first launched and led by Dr. José Vicente Sánchez Polo (6). IGSS serves the Guatemalan patients who have social security, which represents approximately 40% of all individuals with the diagnosis of with CKD or ESKD (7).
In 1997, the Guatemalan MoH created the Unidad Nacional de Atención al Enfermo Renal Crónico (UNAERC; National Center for Chronic Renal Disease), which is the only freestanding dialysis provider for those who are uninsured and without social security (2). As of 2018, approximately 60% of patients with access to RRT were being dialyzed by UNAERC (7). The Guatemalan Fundación para el Niño Enfermo Renal (FUNDANIER; Foundation for Children with Kidney Diseases) was founded in 2003; this foundation provides kidney care to the pediatric and adolescent population with CKD or ESKD in Guatemala (8).
Due to fragmented CKD care in Guatemala, it has been challenging to understand the epidemiology of ESKD and dialysis care in Guatemala. Recently, the Guatemalan Nephrology Association and MoH launched the Guatemalan Registry of Dialysis and Transplantation (9). In this perspective, we provide an update on the state of delivery of dialysis in Guatemala.
Dialysis in Guatemala
Specific data on vascular access, cost of dialysis, nurse/patient ratio, and dialysis duration were collected by contacting the medical directors of the dialysis centers. Every effort was carried out to verify the data presented here, and this report is not an official document of the Guatemalan MoH. Instead, it reflects the knowledge and opinions of its authors.
Incidence and Prevalence of RRT
As of 2019, the incidence of dialysis in Guatemala was 174 per million population (pmp), and the prevalence of patients on dialysis was 564 pmp (Table 1). The incidence and prevalence have been markedly increasing in the past 5 years. In 2013, the incidence was 125 pmp and the prevalence of patients on dialysis was 379 pmp. However, the prevalence of RRT in Guatemala is still of the lowest in the Americas (10), and dialysis prevalence is markedly lower in rural highland areas with predominantly Maya indigenous populations. This could represent lack of access to a higher level of care due to geographic, economic, linguistic, and institutional barriers (Figure 1) (4).
Table 1.
Characteristics of dialysis treatment in Guatemala, as of 2019
| Characteristics | Response |
|---|---|
| Number of prevalent patients on dialysis | N=9245; 564 pmp; 0.56/1000 people |
| Patients on home dialysis (%) | |
| Total | 45 |
| CAPD | 100 |
| Are all dialysis sessions covered by insurance, or do some patients have out-of-pocket expenses? (%) | |
| UNAERC | 63 |
| IGSS | 34 |
| FUNDANIER | 2 |
| Othera | <1 |
| Are the dialysis units hospital based or freestanding? | Freestanding |
| Are the dialysis units for profit or nonprofit? | UNAERC and IGSS are both for profit (a company is hired to provide dialysis services) |
| What is the reimbursement per dialysis session in USD? | |
| HD | $14,000/yr per patient |
| CAPD | $5000–6500/yr per patient |
| Transplant | $3250/yr per patient |
| Are all of the staff who deliver dialysis nurses, or do you also use patient-care technicians? | Only dialysis technicians |
| What is the typical patient/technician ratio in the dialysis units? | |
| UNAERC | 5:1 technician |
| IGSS | 3:1 technician |
| What is the average length of a dialysis session? (min) | 180 |
| How many times per month are patients seen by a nephrologist during dialysis sessions? | |
| UNAERC | Once every 2 mo |
| IGSS | Once every month |
| What is the proportion of prevalent patients on HD in Guatemala using an AVF, AVG, and CVC? (%) | |
| AVF | |
| UNAERC | 25 |
| IGSS | 64 |
| AVG | 0 |
| CVC | |
| UNAERC | <10 |
| IGSS | 10 |
| Temporary catheter | |
| UNAERC | 75 |
| IGSS | 26 |
| Total number of kidney transplants performed in Guatemala since 1982 (n) | |
| IGSS | |
| DDKT | 101 |
| LDKT | 699 |
| Hospital San Juan de Dios | |
| DDKT | 111 |
| LDKT | 569 |
| UNAERC | |
| DDKT | 0 |
| LDKT | 308 |
| FUNDANIER | |
| DDKT | 13 |
| LDKT | 97 |
pmp, per million people; CAPD, continuous ambulatory peritoneal dialysis; UNAERC, Unidad Nacional de Atención al Enfermo Renal Crónico (National Center for Chronic Renal Disease); IGSS, Instituto Guatemalteco de Seguridad Social (Guatemalan Institute of Social Security); FUNDANIER, Fundación para el Niño Enfermo Renal (Foundation for Children with Kidney Disease); HD, hemodialysis; AVF, arteriovenous fistula; AVG, arteriovenous graft; CVC, central venous catheter; DDKT, deceased-donor kidney transplant; LDKT, living-donor kidney transplant.
Army hospital.
Figure 1.

Geographic variation in the prevalence of dialysis treatment (per million population) by department (state) in Guatemala in 2019, and the location of dialysis centers. Most patients with ESKD are located near Guatemala City. The prevalence is markedly lower in rural highland areas with predominantly indigenous populations. FUNDANIER, Fundación para el Niño Enfermo Renal (Guatemalan Foundation for Children with Kidney Diseases); IGSS, Instituto Guatemalteco de Seguridad Social (Guatemalan Institute of Social Security); pmp, per million population; UNAERC, Unidad Nacional de Atención al Enfermo Renal Crónico (National Center for Chronic Renal Disease).
The prevalence of patients on continuous ambulatory peritoneal dialysis (CAPD) in Guatemala (45% of patients on dialysis) is one of the highest when compared with most other Latin American countries. The MoH dialysis center UNAERC (Table 2) mainly provides CAPD (60% of patients on dialysis at UNAERC), whereas IGSS provides mainly HD (83% of patients on dialysis at IGSS).
Table 2.
Dialysis modality by provider in Guatemala
| Dialysis Modality | UNAERC, N (%)a | IGSS, N (%)b | FUNDANIER, N (%)b |
|---|---|---|---|
| Conventional HD | 2010 (40) | 2917 (83) | 30 (21) |
| CAPD | 3004 (60) | 587 (17) | 110 (79) |
| Total | 5014 (100) | 3504 (100) | 140 (100) |
UNAERC, Unidad Nacional de Atención al Enfermo Renal Crónico (National Center for Chronic Renal Disease); IGSS, Instituto Guatemalteco de Seguridad Social (Guatemalan Institute of Social Security); FUNDANIER, Fundación para el Niño Enfermo Renal (Foundation for Children with Kidney Disease); HD, hemodialysis; CAPD, continuous ambulatory peritoneal dialysis.
Data until June 30, 2019.
Data until June 30, 2020.
Costs
Despite private entities in Guatemala providing 8% of general medical care (2), most Guatemalans are unable to cover the costs of dialysis in the private sector because the minimum wage is around 390 USD per month. Therefore, most patients use the MoH services or IGSS. Around 34% of dialysis care is provided by IGSS, and around 65% is provided by the MoH via the adult unit UNAERC or the pediatric unit FUNDANIER. Care received at UNAERC and FUNDANIER is free of charge, with CAPD supplies delivered to rural homes throughout the country (3). The cost of CAPD is less than half the cost of HD per person per year. Private entities provide all of the dialysis services; thus, the MoH and IGSS sublease the dialysis service to private companies.
Those patients enrolled in CAPD at UNAERC have a peritoneal catheter placed at UNAERC, receive CAPD supplies delivered to their homes at no cost, and attend every 2-month outpatient consultation at UNAERC. The patients have to incur extra expenses related to ESKD care, including the trips to Guatemala City for their outpatient appointments, phosphate binders, calcitriol, erythropoietin-stimulating agents, and antihypertensive medications. From our previous experience running a CAPD program in rural Guatemala, we estimated these out-of-pocket costs to be around 1800 USD per patient per year for new CAPD starts, and approximately 500 USD per patient per year for ongoing patients. These costs do not include calcitriol or intravenous iron (3). Patients on dialysis face significant social and occupational limitations because of their time-consuming treatment. Patients who were once independent and able to support their families can no longer work and, therefore, feel like a burden to their families (11).
Human Resources and Quality of Care
In Guatemalan dialysis centers, there are no dialysis nurses; instead, there are dialysis technicians. The ratio of technician to patient varies by type of service (3:1 in IGSS and 5:1 in UNAERC). In our recent experience, we found that healthcare professionals working at UNAERC experience challenges in providing high-quality care due to resource limitations and, therefore, need to implement strategies to meet the rising demands for RRT. These strategies include decreasing the frequency and duration of HD treatments, and encouraging new patients to enroll in CAPD rather than HD (12). Due to this precarious situation, most patients at UNAERC receive HD weekly rather than three times per week. This differs from IGSS, where most patients receive HD three times per week. At IGSS, the 1-year mortality rate is lower among patients on CAPD (9%) than those on HD (14%). Unfortunately, we do not have data on mortality among those cared for at UNAERC. Because of high cost, we have observed that many patients never receive RRT, whereas others are forced to discontinue RRT after a short period of time. Therefore, we estimate the mortality rate to be higher at UNAERC than IGSS, but further research is needed.
Vascular Access
Most Guatemalans getting dialysis at UNAERC have a temporary dialysis catheter (75% of those on HD), whereas most of the patients on HD at IGSS have an arteriovenous fistula (64%).
Kidney Transplantation
The first successful kidney transplant occurred in 1982. This achievement was followed by the creation of the first kidney transplant program at IGSS in 1985 (6). Since 1985, there have been a total of 800 kidney transplants at IGSS; 680 at Hospital San Juan de Dios, a large referral hospital run by the MoH in Guatemala City; and 308 at UNAERC. FUNDANIER, the pediatric unit, has performed 110 kidney transplants since 2008. Most of the transplants (>85%) are living-donor kidney transplants.
Future Directions
Guatemala has one of the highest rates of child undernutrition worldwide (13). Early life exposures to malnutrition and obesity in Guatemala increase the adult risk for noncommunicable diseases, such as diabetes (14). Therefore, CKD in Guatemala is a complex public health problem due to increasing prevalence of traditional causes (such as diabetes, hypertension, and lower nephron mass) and nontraditional risk factors, such as Mesoamerican nephropathy (15,16). The solution to the CKD problem should be focused on a comprehensive approach that ranges from early CKD detection and prevention, improving the quality of therapies to replace kidney function, and increasing the rate of kidney transplants. For rational resource use and optimal results for patient-reported outcomes, implementing a palliative care program focused on ESKD and advanced comorbidities is also essential (Figure 2).
Figure 2.
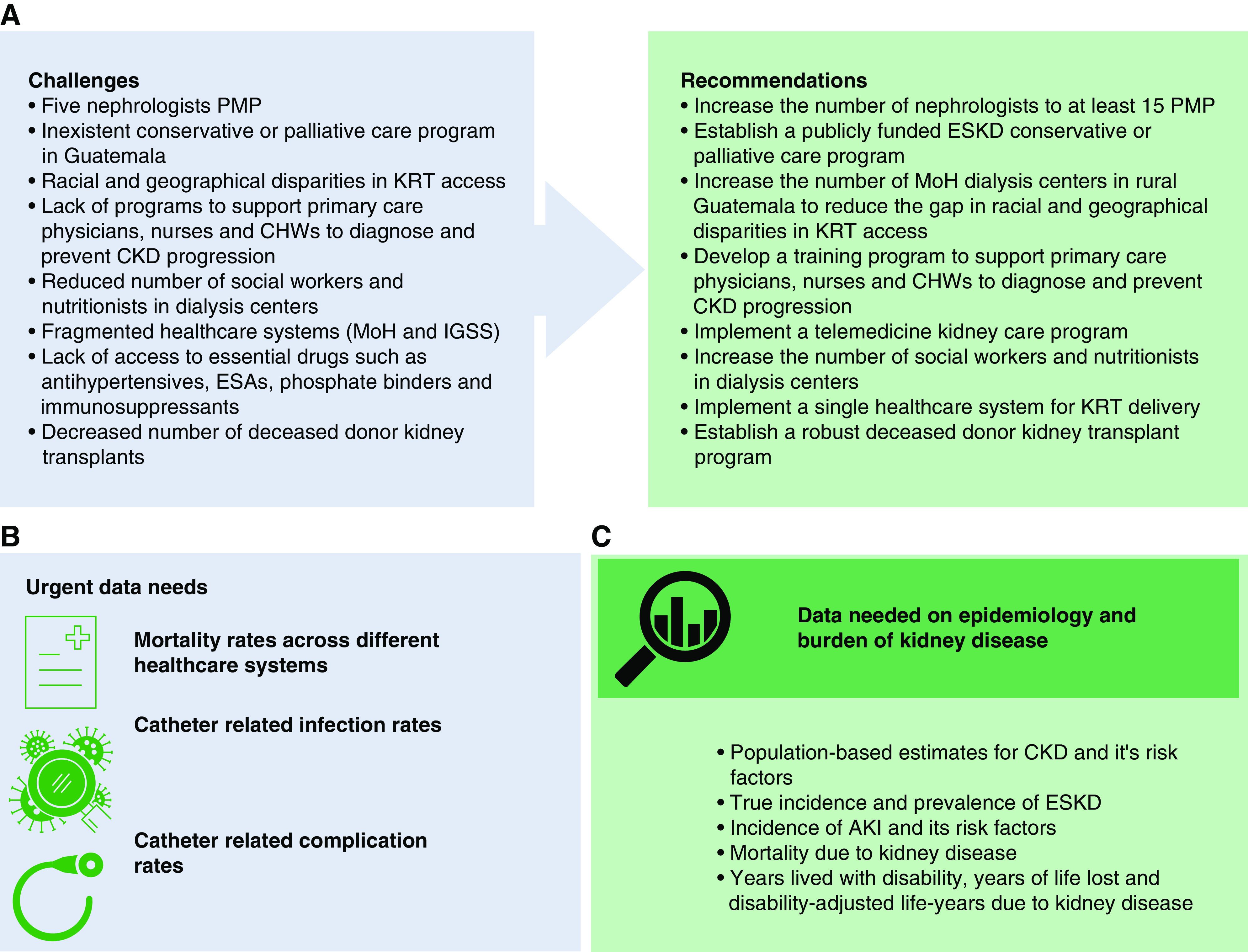
Challenges, recommendations, and epidemiological data to improve kidney care in Guatemala. (A) Challenges and recommendations to expand RRT access and improve ESKD care in Guatemala. (B) Urgent data needs. (C) Data needed on epidemiology and burden of kidney disease. CHW, community healthcare workers; ESA, erythropoietin-stimulating agent; KRT, kidney replacement therapy; MoH, Ministry of Health.
Here, we described several inequities in the system. The quality of care delivered at UNAERC is suboptimal and compromised due to high clinical demand with limited resources. IGSS has implemented a system to expand the accessibility of dialysis treatment beyond the borders of Guatemala City. It has expanded to 14 out of 22 departments in Guatemala, whereas the MoH has only three dialysis centers (Figure 1). To expand the number of people covered, reduce out-of-pocket payments, and thus reduce financial hardship, we recommend that the MoH should consider the implementation of a single healthcare system for RRT delivery, instead of a dual healthcare system (Figure 2).
Each institution in Guatemala—including the private, public, and social security sectors—must consolidate efforts to bring CKD care to urban centers, rural indigenous communities, and the southern coast region, where individuals are primarily affected by Mesoamerican nephropathy. This effort will allow timely detection of those patients at risk for, or in the early stages of, CKD and the implementation of measures that slow down the progression of kidney disease (Figure 2).
Guatemala has one of the lowest rates of nephrologists pmp in Latin America. There are only three nephrology training programs (7). Two of these programs are part of the International Society of Nephrology Sister Renal Center Program, and those programs have built a robust educational collaboration with their respective sister program in the United States. Unfortunately, the existing training programs are not sufficient to diversify and increase the number of nephrologists. Therefore, a policy must be implemented by local universities to carry out more training programs, because it is essential to increase the number of nephrologists.
Another element that must be considered to increase access to kidney care is the capacity to reach patients through primary healthcare physicians. However, it is essential to train primary care physicians to be able to detect CKD in patients with risk factors in a timely manner, because the toolbox to prevent ESKD for one of the most common causes of progressive CKD—i.e., diabetes—is expanding with highly effective therapies (renin-angiotensin-aldosterone system inhibitors and sodium-glucose cotransporter-2 inhibitors). We must implement educational efforts such as webinars, online courses, and all other alternatives that education and technology offer today. Hence, it is essential that government authorities allocate a budget for a robust and sustainable educational program.
Furthermore, it is important to continue building on the already established dialysis and transplant registry, and to generate rational allocation of new resources on the basis of evaluations of healthcare outcomes and quality benchmarks. The estimated prevalence of CKD in Guatemala is still unknown. One of the aims established by our Guatemalan CKD research consortium is to join efforts to conduct population-based studies to better understand the CKD epidemiology in understudied rural and indigenous populations in Guatemala (7).
Disclosures
P. Garcia is supported by the American Kidney Fund Clinical Scientist in Nephrology Fellow Program, and the Leeds Scholar Endowment Fund. The remaining author has nothing to disclose.
Funding
None.
Acknowledgments
The authors thank Dr. Shuchi Anand, Dr. Randall Lou-Meda (FUNDANIER), and Dr. Julio Boj (UNAERC) for their input during the preparation of this manuscript.
The content of this article reflects the personal experience and views of the author(s) and should not be considered medical advice or recommendations. The content does not reflect the views or opinions of the American Society of Nephrology (ASN) or Kidney360. Responsibility for the information and views expressed herein lies entirely with the author(s).
Author Contributions
P. Garcia was responsible for visualization; P. Garcia and V. Sánchez-Polo conceptualized the study; were responsible for data curation, investigation, and methodology; wrote the original draft; and reviewed and edited the manuscript; and V. Sánchez-Polo provided supervision.
References
- 1.Instituto Nacional de Estadistica Guatemala: Características generales de la población, 2019. Available at: https://www.censopoblacion.gt/censo2018/poblacion.php. Accessed July 20, 2020
- 2.Pan American Health Association: Health in the Americas+, 2017 edition. Summary: Regional outlook and country profiles. Washington, D.C., Pan American Health Organization, 2017 [Google Scholar]
- 3.Flood DC, Chary AN, Austad K, Garcia P, Rohloff PJ: A patient navigation system to minimize barriers for peritoneal dialysis in rural, low-resource settings: Case study from Guatemala. Kidney Int Rep 2: 762–765, 2017. 10.1016/j.ekir.2017.02.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chary A, Flood D, Austad K, Colom M, Hawkins J, Cnop K, Martinez B, Lopez W, Rohloff P: Accompanying indigenous Maya patients with complex medical needs: A patient navigation system in rural Guatemala. Healthc (Amst) 6: 144–149, 2018. 10.1016/j.hjdsi.2017.08.006 [DOI] [PubMed] [Google Scholar]
- 5.Pan American Health Organization (PAHO) : Chronic kidney diseases (N18) & Renal failure (N17-N19) mortality, countries of the Americas, 2014. Available at: http://ais.paho.org/phip/viz/nmh_renalfailure_ckd_visualization.asp. Accessed May 18, 2020
- 6.Lou-Meda R: La Nefrología en Guatemala Una Historia Vivida. Otra tesis. Guatemala City, Guatemala, Universidad de San Carlos de Guatemala, 2011
- 7.Garcia P, Mendoza C, Barnoya J, Monzon J, Miller AC, Aguilar-González A, Boj J, Cifuentes A, Dávila P, Flood D, Guzmán-Quilo C, Hernandez A, Lou-Meda R, Palacios E, Sánchez-Polo V, Sosa R, Rohloff P: CKD care and research in Guatemala: Overview and meeting report. Kidney Int Rep 5: 1567–1575, 2020. 10.1016/j.ekir.2020.06.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lou-Meda R: ESRD in Guatemala and a model for preventive strategies: Outlook of the Guatemalan foundation for children with kidney diseases. Ren Fail 28: 689–691, 2006. 10.1080/08860220600938258 [DOI] [PubMed] [Google Scholar]
- 9.Ministerio de Salud Pública y Asistencia Social (MSPAS): MSPAS presenta Registro Único Guatemalteco de Diálisis y Trasplante Renal. Available at: https://www.mspas.gob.gt/index.php/noticias/noticias-mspas/item/574-mspas-presenta-registro-unico-guatemalteco-de-dialisis-y-trasplante-renal. Accessed June 28, 2020
- 10.Rosa-Diez G, Gonzalez-Bedat M, Pecoits-Filho R, Marinovich S, Fernandez S, Lugon J, Poblete-Badal H, Elgueta-Miranda S, Gomez R, Cerdas-Calderon M, Almaguer-Lopez M, Freire N, Leiva-Merino R, Rodriguez G, Luna-Guerra J, Bochicchio T, Garcia-Garcia G, Cano N, Iron N, Cuero C, Cuevas D, Tapia C, Cangiano J, Rodriguez S, Gonzalez H, Duro-Garcia V: Renal replacement therapy in Latin American end-stage renal disease. Clin Kidney J 7: 431–436, 2014. 10.1093/ckj/sfu039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moore J, Garcia P, Rohloff P, Flood D: Treatment of end-stage renal disease with continuous ambulatory peritoneal dialysis in rural Guatemala. BMJ Case Reports 2018: bcr2017223641, 2018. 10.1136/bcr-2017-223641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Flood D, Wilcox K, Ferro AA, Mendoza Montano C, Barnoya J, Garcia P, Lou-Meda R, Rohloff P, Chary A: Challenges in the provision of kidney care at the largest public nephrology center in Guatemala: A qualitative study with health professionals. BMC Nephrol 21: 71, 2020. 10.1186/s12882-020-01732-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Flores-Quispe MDP, Restrepo-Méndez MC, Maia MFS, Ferreira LZ, Wehrmeister FC: Trends in socioeconomic inequalities in stunting prevalence in Latin America and the Caribbean countries: Differences between quintiles and deciles. Int J Equity Health 18: 156, 2019. 10.1186/s12939-019-1046-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ford ND, Behrman JR, Hoddinott JF, Maluccio JA, Martorell R, Ramirez-Zea M, Stein AD: Exposure to improved nutrition from conception to age 2 years and adult cardiometabolic disease risk: A modelling study. Lancet Glob Health 6: e875–e884, 2018. 10.1016/S2214-109X(18)30231-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Laux TS, Barnoya J, Cipriano E, Herrera E, Lopez N, Polo VS, Rothstein M: Prevalence of chronic kidney disease of non-traditional causes in patients on hemodialysis in southwest Guatemala. Rev Panam Salud Publica 39: 186–193, 2016 [PubMed] [Google Scholar]
- 16.Butler-Dawson J, Krisher L, Asensio C, Cruz A, Tenney L, Weitzenkamp D, Dally M, Asturias EJ, Newman LS: Risk factors for declines in kidney function in sugarcane workers in Guatemala. J Occup Environ Med 60: 548–558, 2018. 10.1097/JOM.0000000000001284 [DOI] [PMC free article] [PubMed] [Google Scholar]