

Introduction
Argentina is the third most populated country in South America with an estimated population of 44,494,502. Despite having an area of 2,780,400 km2 (eighth largest in the world), 90% of the population resides in urban areas, with the majority concentrated in and around Buenos Aires. Life expectancy is 79.7 years in women and 73.6 years in men, with cardiovascular disease as the leading cause of mortality. Argentina spends approximately 10% of its gross domestic product on health care (1). There are 3.94 physicians and 4.5 hospital beds per 1000 inhabitants in Argentina (2). The physician-patient ratio is similar to that of Australia, Italy, Spain, and Switzerland, and is double than Brazil and almost four times than Chile and Peru.
Argentina has a multitiered, decentralized health care system that is plagued by fragmented management and financing. There are national, provincial, and municipal government–sponsored health care insurances, which together with union-sponsored insurances, provide health care coverage to nearly 22 million people. An additional approximately 10% of the population has private health insurance, leaving nearly 36% of the population without health care coverage or the financial means to pay for private insurance. These individuals are cared for at cost-free public hospitals and community facilities (1,2).
The first hemodialysis (HD) treatment in Argentina dates back to 1955. Five years later in 1960, the Argentine Society of Nephrology was founded (3).
Epidemiology
The incidence and prevalence of CKD and ESKD have been growing steadily, most likely because of increasing rates of diabetes and obesity as well as an aging population. Indeed, CKD is now the seventh leading cause of mortality in Argentina, and CKD-related deaths have increased by 15% between 2007 and 2017 (4).
The National Transplantation Institute (INCUCAI) supports a National Dialysis and Transplant Registry (5,6). Patient reporting is obligatory; therefore, national data are valid and representative. Reporting is the responsibility of the dialysis center director, and it is provided online. Patient identity is preserved by data security systems.
The annual incidence of ESKD is 160 patients per million population, with diabetes and hypertension as the most common etiologies (Table 1). At the end of 2018, there were 29,929 patients with ESKD on chronic dialysis, representing a prevalence rate of 673 patients per million population (Figure 1) (5,6). Of these, approximately 93.5% are on in-center HD, 6.5% on peritoneal dialysis (PD), and none are on home HD. Of the patients on HD, 70% receive dialysis via an arteriovenous fistula, 15% receive dialysis via an arteriovenous graft, and 15% receive dialysis via central venous catheters. First year and annual mortality rates on dialysis are 18% and 16.4%, respectively (Table 1), with cardiovascular cause being the most common (6). Annual mortality rate has been above 16% for the last 4 years (Figure 2). RRT in Argentina has incidence and prevalence rates above the mean for Latin America, most likely because dialysis and transplant are readily available in the country (Table 2). Nevertheless, PD is relatively less used compared with the rest of Latin America (7–9).
Table 1.
Characteristics of patients on dialysis in Argentina
| Characteristic | Value |
| Country population | 44,494,502 |
| Patients on hemodialysis | 29,929 |
| Patients on peritoneal dialysis | 1945 |
| Patients with functioning kidney transplant | 11,486 |
| Prevalence of hepatitis B, % | 0.2 |
| Prevalence of hepatitis C, % | 1 |
| Prevalence of HIV, % | 0.8 |
| Prevalence of diabetes, % | 28 |
| Membrane dialyzer (reuse), synthetic/substituted cellulose/cellulose, % | 83/14/4 |
| Type of vascular access, native AVF/prosthetic AVF/catheter | 70/15/15 |
| Prevalence of patients with ESA, % | 87 |
| No. of hemodialysis centers | 597 |
| Hospital-based dialysis units, % | 25 |
| Nonprofit dialysis units, % | 11 |
| No. of peritoneal dialysis centers | 79 |
| Dialysis covered by insurance, % | 100 |
| Out-of-pocket expenses, % | 0 |
| Dialysis unit staffing, nurses/technicians, % | 95/5 |
| Payment per hemodialysis session, USD | 55 |
| Patient-nurse ratio in hemodialysis units, adult/pediatric | 4–5/2–3 |
| Average length of dialysis session, h | 4 |
| Minimum patient evaluation by physician per mo | 4 |
| No. of transplant centers | 55 |
| Adjusted annual mortality dialysis rate, % | 16.48 |
| Etiology of ESKD, % | |
| Diabetes | 36.5 |
| Nephroangiosclerosis | 20 |
| Unknown cause | 17 |
| GN | 9 |
| Myeloma and amyloidosis | 1 |
| Obstructive uropathy | 6 |
| Polycystic kidney disease, adult type | 5 |
| Epidemic uremic hemolytic syndrome | 0.5 |
| Other | 5 |
| Cause of death, % | |
| Cardiovascular | 50 |
| Infection | 25 |
| Neoplasia | 6 |
| Other | 19 |
Figure 1.
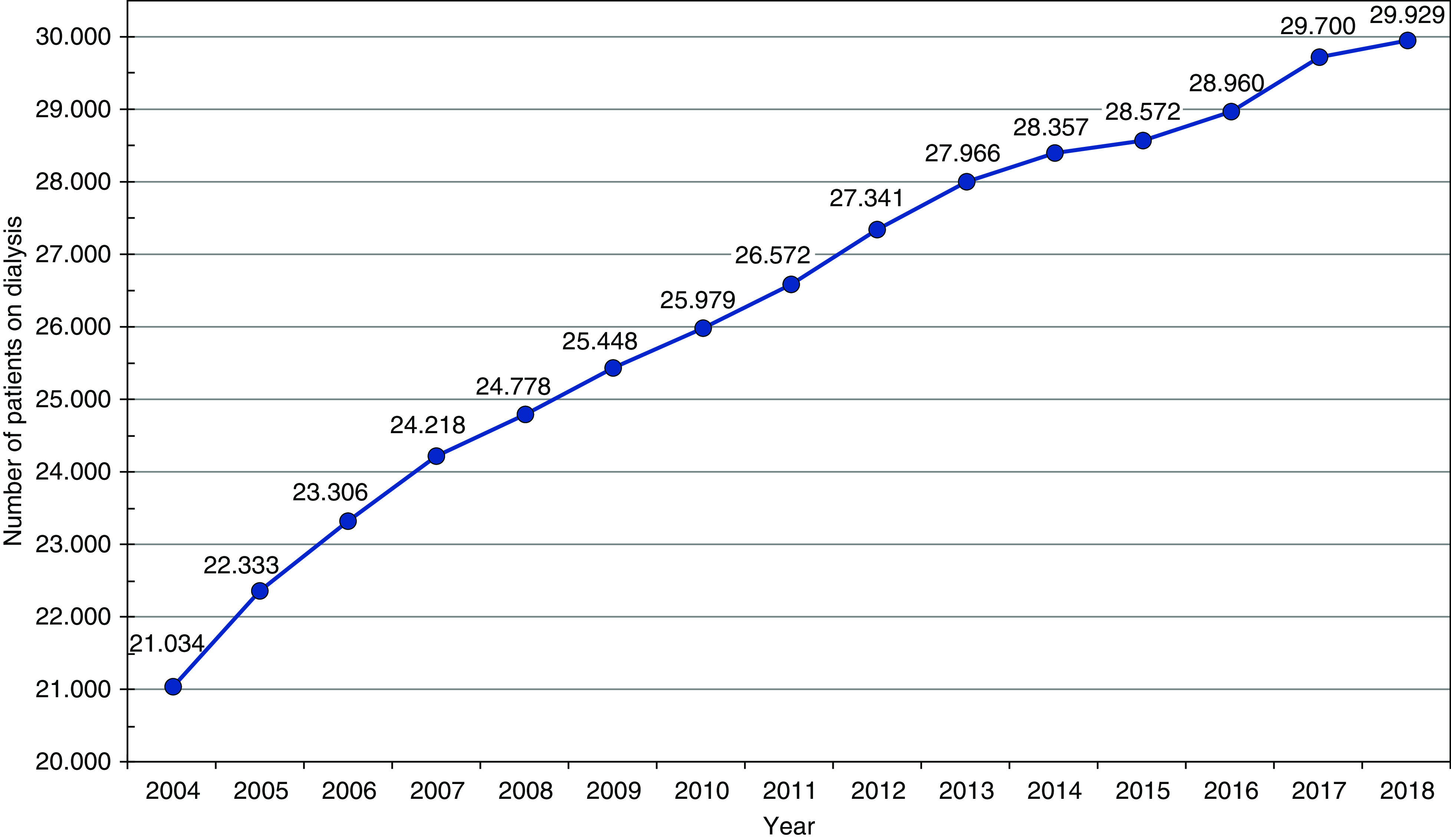
Figure 2.

Annual dialysis mortality rate. Rate is expressed in deaths per 100 patients at risk with 95% confidence interval bars. Source: Argentinean Registry of Dialysis and Transplantation (5,6).
Table 2.
Comparison of RRT between Argentina and Latin America
| Argentina | Latin America | |
| Prevalence of patients with ESKD under RRT (dialysis and transplant)a | 976 | 805 |
| Dialysis incidence ratea | 160 | 154 |
| Kidney transplant ratea | 30 | 21 |
| Patients on peritoneal dialysis, % | 6.5 | 11.5 |
| Nephrologista | 30 | 18 |
Rates are expressed per million population. Source: Latin American Registry of Dialysis and Transplantation (7).
Structural Organization and Logistics of Dialysis
Argentina has dialysis units in both hospital and private settings. There are a total number of 597 dialysis centers in the country. Eleven percent (68 centers) of these centers are government owned, 377 (63%) are independent dialysis centers, and the rest (152 centers; 26%) are owned by foreign dialysis companies. One hundred eighty-seven dialysis units are in the province of Buenos Aires, and the rest are located throughout the rest of the country. Dialysis is covered by patients’ union health system or health insurance; ultimately, the government pays if the patient does not have insurance. Government coverage is universal if a patient does not have union or health insurance. This includes illegal immigrants, noncitizens, and refugees.
Payment for HD and PD is capitated at approximately United States $700 per month or United States $55 per HD session. Physicians across the country are paid by monthly salaries, and some also have private practice. PD solutions are not manufactured in the country and are, therefore, imported. Bundle HD and PD payment includes vascular access, erythropoietin, appropriate vaccination, and transfer to and from the dialysis unit. Monthly reimbursement is irrespective of procedure number.
Average HD sessions last for 240 minutes, with 95% of patients receiving three or more dialysis sessions per week (5,6). Online hemodiafiltration has been recorded since 2015. Approximately 20% of HD centers have this technology.
Although 70% of patients on incident dialysis start with a temporary catheter as their vascular access, at 6 months into treatment most have permanent vascular access. Seventy percent of prevalent patients have an arteriovenous fistula. Nephrologists insert all temporary catheter access. Permanent HD catheters are placed by nephrologists also but mostly by vascular surgeons. Arteriovenous fistulas are 100% done by vascular surgery. Interventional nephrologists do not perform arteriovenous fistulas. Almost 87% of the patients are on erythropoietin or similar agents, and synthetic HD membranes are most commonly used. (Table 1) (5,6).
The advent of technologic advancement, biosecurity implementation, and specific treatment has decreased the prevalence of hepatitis B, hepatitis C, and HIV in the dialysis population (0.2%, 1%, and 0.8%, respectively). Isolation of patients with hepatitis B is mandatory.
No formal end-of-life care support programs are available in Argentina.
Staffing of Dialysis Units
Argentina is third among Latin American countries considering nephrology physicians per million inhabitants (Table 2) (7,8). There is one nephrologist for every 40 patients, and a nephrologist must be present in the dialysis unit at all times. There are approximately 80 renal fellows in training per year. Most patients are seen daily or at least four times a month. In continuous ambulatory peritoneal dialysis, they are seen once a month. Historically, non-nurse technicians accounted for the majority of dialysis personnel, but this has progressively decreased to approximately 5%. Nurses now provide the lion’s share of dialysis care. The main driving force for this change occurred 10 years ago when regulations were changed to increase the number of dialysis nurses taking care of these patients. The nurse to patient ratio is four to five adult patients per nurse in HD units and two to three children per nurse in pediatric units. In PD, the ratio is 20 adult and 15 pediatric patients per nurse (5,6). No formal dialysis nurse certification is in place in the country.
Transplantation in Argentina
The International Registry of Organ Donation and Transplantation reports that in 2019 there were approximately 1674 kidney transplants (1325 from deceased donors and 349 from living donors) in Argentina. There were 69 simultaneous kidney-pancreas transplants, 19 kidney-liver transplants, and 5 kidney-heart transplants. More men (62%) were transplanted than women. The availability of kidney transplants differs regionally around Argentina, with approximately 6546 patients with ESKD currently on the transplant list waiting for a new kidney. Average waiting time on the transplant list is over 4 years. Swap living kidney transplants have occurred, but there are very few cases (5). Transplantation is regulated by the INCUCAI (5,6). Since 2004, the INCUCAI has supported a National Dialysis and Transplant Registry. Patient reporting is obligatory, and therefore, national data are valid and representative. The INCUCAI in conjunction with the Argentine Society of Nephrology analyzes and reports the data of the National Dialysis and Transplant Registry (5,6). The INCUCAI, the Argentine Society of Nephrology, and the Argentine Transplant Society promote organ donation campaigns regularly. A recent law has declared the general population as presumed donors, and this has increased donation by 20%–25%. There are barriers to donation, but none are due to social or cultural barriers. Some of these barriers include logistics of organ harvesting and transportation in a large country, insufficient organ harvesting teams in some regions, etc.
Future Directions and Challenges
RRTs are accessible and available in Argentina, and utilization rates are acceptable compared with other countries in the region. It will be challenging to improve what is currently available with limited economic resources. An advanced kidney care program is not available nationwide and needs to be designed and implemented to guarantee early and programmed dialysis initiation and preemptive transplant when possible. PD is underused in Argentina for many reasons: peritoneal solutions are not manufactured in the country and are expensive, and most nephrologists have not been trained in PD because HD has been the predominant form of dialysis historically. Because many patients still begin dialysis without previous planification, the preferred dialysis modality used in urgent situations is HD through temporary catheter access. Training and economic incentives will help develop PD further. Home HD will most likely be set aside for some time. This technology is not available yet, and no reimbursement plans are underway for this dialysis modality.
Disclosures
G.J. Rosa Diez is employed by Fressenius. The remaining author has nothing to disclose.
Funding
None.
Author Contributions
M. Orias was responsible for validation; M. Orias and G.J. Rosa Diez provided supervision; G.J. Rosa Diez wrote the original draft; and M. Orias and G.J. Rosa Diez reviewed and edited the manuscript.
References
- 1.Rubinstein A, Zerbino MC, Cejas C, López A: Making universal health care effective in Argentina: A blueprint for reform. Health Syst Reform 4: 203–213, 2018 [DOI] [PubMed] [Google Scholar]
- 2.Arce H: Organización y financiamiento del sistema de salud en la Argentina. Medicina (Buenos Aires) 72: 414–418, 2012 [PubMed] [Google Scholar]
- 3.Argentinean Society of Nephrology : The history of nephrology in Argentina. Available at: http://www.san.org.ar/2015/institucional-historia.php. Accessed March 9, 2020
- 4.Institute for Health Metrics and Evaluation: Argentina, 2012. Available at: http://www.healthdata.org/argentina. Accessed September 20, 2019
- 5.Instituto Nacional Central Unico Coordinador de Ablación e Implante (INCUCAI), Sistema Nacional de Información de Procuración y Trasplante de la República Argentina (SINTRA), Insuficiencia Renal Crónica Terminal: National Registry of Terminal Chronic Renal Failure. Available at: https://irct.incucai.gov.ar/public/Modulo1.do. Accessed March 20, 2020
- 6.Marinovich S, Bisigniano L, Hansen Krogh D, Celia E, Tagliafichi V, Rosa Diez G, Fayad A: Registro Argentino de Diálisis Crónica SAN-INCUCAI 2018, Buenos Aires, Argentina, Sociedad Argentina de Nefrología e Instituto Nacional Central Único Coordinador de Ablación e Implante, 2019 [Google Scholar]
- 7.Rosa-Diez G, Gonzalez-Bedat M, Ferreiro A, García-García G, Fernandez-Cean J, Douthat W: Burden of end-stage renal disease (ESRD) in Latin America. Clin Nephrol 86[Suppl 1]: 29–33, 2016 [DOI] [PubMed] [Google Scholar]
- 8.Cusumano AM, Rosa-Diez GJ, Gonzalez-Bedat MC: Latin American Dialysis and Transplant Registry: Experience and contributions to end-stage renal disease epidemiology. World J Nephrol 5: 389–397, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Luxardo R, Kramer A, González-Bedat MC, Massy ZA, Jager KJ, Rosa-Diez G, Noordzij M; collaborators : The epidemiology of renal replacement therapy in two different parts of the world: The Latin American Dialysis and Transplant Registry versus the European Renal Association-European Dialysis and Transplant Association Registry. Rev Panam Salud Publica 42: e87, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]