

Abstract
Fracture non‐union represents a common complication, seen in 5%–10% of all acute fractures. Despite the enhancement in scientific understanding and treatment methods, rates of fracture non‐union remain largely unchanged over the years. This systematic review investigates the biological, molecular and genetic profiles of both (i) non‐union tissue and (ii) non–union‐related tissues, and the genetic predisposition to fracture non‐union. This is crucially important as it could facilitate earlier identification and targeted treatment of high‐risk patients, along with improving our understanding on pathophysiology of fracture non‐union. Since this is an update on our previous systematic review, we searched the literature indexed in PubMed Medline; Ovid Medline; Embase; Scopus; Google Scholar; and the Cochrane Library using Medical Subject Heading (MeSH) or Title/Abstract words (non‐union(s), non‐union(s), human, tissue, bone morphogenic protein(s) (BMPs) and MSCs) from August 2014 (date of our previous publication) to 2 October 2021 for non‐union tissue studies, whereas no date restrictions imposed on non–union‐related tissue studies. Inclusion criteria of this systematic review are human studies investigating the characteristics and properties of non‐union tissue and non–union‐related tissues, available in full‐text English language. Limitations of this systematic review are exclusion of animal studies, the heterogeneity in the definition of non‐union and timing of tissue harvest seen in the included studies, and the search term MSC which may result in the exclusion of studies using historical terms such as ‘osteoprogenitors’ and ‘skeletal stem cells’. A total of 24 studies (non‐union tissue: n = 10; non–union‐related tissues: n = 14) met the inclusion criteria. Soft tissue interposition, bony sclerosis of fracture ends and complete obliteration of medullary canal are commonest macroscopic appearances of non‐unions. Non‐union tissue colour and surrounding fluid are two important characteristics that could be used clinically to distinguish between septic and aseptic non‐unions. Atrophic non‐unions had a predominance of endochondral bone formation and lower cellular density, when compared against hypertrophic non‐unions. Vascular tissues were present in both atrophic and hypertrophic non‐unions, with no difference in vessel density between the two. Studies have found non‐union tissue to contain biologically active MSCs with potential for osteoblastic, chondrogenic and adipogenic differentiation. Proliferative capacity of non‐union tissue MSCs was comparable to that of bone marrow MSCs. Rates of cell senescence of non‐union tissue remain inconclusive and require further investigation. There was a lower BMP expression in non‐union site and absent in the extracellular matrix, with no difference observed between atrophic and hypertrophic non‐unions. The reduced BMP‐7 gene expression and elevated levels of its inhibitors (Chordin, Noggin and Gremlin) could potentially explain impaired bone healing observed in non‐union MSCs. Expression of Dkk‐1 in osteogenic medium was higher in non‐union MSCs. Numerous genetic polymorphisms associated with fracture non‐union have been identified, with some involving the BMP and MMP pathways. Further research is required on determining the sensitivity and specificity of molecular and genetic profiling of relevant tissues as a potential screening biomarker for fracture non‐unions.
Keywords: non‐union(s), nonunion(s), fracture, human tissue, mesenchymal stem cell(s), mesenchymal stromal cell(s)
1. INTRODUCTION
Bone healing is a complex biological process aiming at restoring the affected area to its pre‐injury levels. This is achieved through repair and regeneration of the cellular and extracellular components, regaining its former biochemical and biomechanical properties. 1 , 2 Successful bone healing requires the orchestrated interaction between the biological (cellular, signalling molecules and extracellular matrix) and mechanical environments. 3 Moreover, according to the ‘Diamond Concept’, other parameters that are considered essential for a successful healing include the local vascularity and the patient's biological fitness and comorbidities. 4
The definition of non‐union has been inconsistent in the literature. The FDA (Food and Drug Administration), however, defines non‐union as incomplete fracture healing within 9 months following injury, coupled by the lack of progression in radiological signs of healing over the course of three consecutive months. 5 Despite the advancement in both the understanding of fracture healing and some of the pathways that regulate it, the rates of fracture non‐union remain largely unchanged over the years. To date, fracture non‐union remains common, occurring in 5%–10% of the 850,000 fractures seen yearly in the UK. 6 This poses a significant direct and indirect socioeconomic burden through prolonged medical treatments and productivity losses. 6 Further understanding of the biological processes and underlying mechanisms, along with their interactions, leading to fracture non‐union need to be elucidated in order to reduce this risk.
We have previously published a systematic review outlining the biological and molecular profile of ‘non‐union tissue’. 1 Nevertheless, one critically relevant and important aspect not previously considered because of the scarce evidence at the time was the relevance of tissues harvested from sites away from the non‐union site, such as peripheral blood and bone marrow products. Moreover, the accelerated improvement in laboratory techniques over the last decade also meant the biological and molecular understanding of the multiple pathways involved in bone healing is everchanging. Consequently, the herein study provides an up‐to‐date review on the knowledge that has been acquired in this important clinical condition. We aim to summarize the current evidence on (i) macroscopic and microscopic characteristics; (ii) cellular characteristics and function (cell surface protein expression, morphology, viability, proliferation, senescence, mineralization and alkaline phosphatase [ALP] activity); (iii) molecular characteristics (protein, mRNA, miRNA and gene expression) of non‐union tissue and relevant tissues; (iv) differences between atrophic and hypertrophic non‐unions; (v) effect of intervention(s) on non‐union tissue and relevant tissues; and (vi) genetic predispositions to fracture non‐union.
2. MATERIALS AND METHODS
This systematic review was conducted according to the PRISMA guidelines. 7 Our protocol was similar to that of our previous publication, with the only difference being the addition of other types of tissues not harvested from the non‐union site (‘relevant tissue’) in our inclusion criteria. 1 We define ‘relevant tissue’, as bone marrow or peripheral blood derived products, investigated to identify associations with progression to non‐union. The reason for including studies assessing relevant tissue was due to the growing body of evidence demonstrating the correlation of these tissues with the occurrence of non‐union, which we feel could be helpful to guide clinicians in their practice.
2.1. Eligibility criteria
The inclusion criteria were as follows: (i) tissue obtained from the non‐union site and processed for defining its characteristics and properties, OR studies assessing tissue relevant to non‐union as defined above (‘relevant tissue’); (ii) only tissue acquired from human subjects was included; (iii) articles were published in English language; (iv) the full text of each article was available; and (vi) for non‐union tissue, articles published between August 2014 (date of our previous publication) and 2 October 2021; for relevant tissue, no publication date restrictions were imposed. Studies that did not fulfil the eligibility criteria were excluded from further analysis.
2.2. Search strategy and information sources
Adhering to our previously published protocol, the following databases were used during literature search: PubMed Medline; Ovid Medline; Embase; Scopus; Google Scholar; and the Cochrane Library. The full search strategy is as detailed in Table 1. Briefly, the search terms included non‐union(s), nonunion(s), human, tissue, bone morphogenic protein(s) (BMPs) and MSCs. Bibliographies of all identified articles were collected in Endnote X9, manually reviewed and searched for any potentially eligible studies.
TABLE 1.
PubMed search strategy (searched 2 October 2021)
| 1. | (("non‐union"[All Fields] OR ("nonunion"[All Fields] OR "nonunions"[All Fields])) |
| 2. |
("mesenchymal stem cells"[MeSH Terms] OR ("mesenchymal"[All Fields] AND "stem"[All Fields] AND "cells"[All Fields]) OR "mesenchymal stem cells"[All Fields] OR ("mesenchymal"[All Fields] AND "stem"[All Fields] AND "cell"[All Fields]) OR "mesenchymal stem cell"[All Fields] |
| 3 | "MSC"[All Fields] |
| 4. |
("mesenchymal stem cells"[MeSH Terms] OR ("mesenchymal"[All Fields] AND "stem"[All Fields] AND "cells"[All Fields]) OR "mesenchymal stem cells"[All Fields] OR ("mesenchymal"[All Fields] AND "stromal"[All Fields] AND "cell"[All Fields]) OR "mesenchymal stromal cell"[All Fields]) |
| 5. | "bone morphogenetic proteins"[MeSH Terms] OR ("bone"[All Fields] AND "morphogenetic"[All Fields] AND "proteins"[All Fields]) OR "bone morphogenetic proteins"[All Fields] OR ("bone"[All Fields] AND "morphogenetic"[All Fields] AND "protein"[All Fields]) OR "bone morphogenetic protein"[All Fields] |
| 6. | ("tissue s"[All Fields] OR "tissues"[MeSH Terms] OR "tissues"[All Fields] OR "tissue"[All Fields]))) |
| 7. | (humans[Filter]) |
| 8. | (english[Filter])) |
| 9. | 2 OR 3 OR 4 OR 5 OR 6 |
| 10. | 1 AND 9 |
| 11. | 10 AND 7 AND 8 |
2.3. Study selection
Two of the authors (MP and JV) performed the eligibility assessment independently, in an unblinded, standardized manner. Title and abstract sift were conducted first, followed by review of full text by MP and JV. Only studies fulfilling the eligibility criteria were included. Data of each eligible study were independently extracted by MP and JV, with results checked by the third author (IP). Any disagreement between reviewers was resolved by consensus, and if necessary, the senior researcher (PVG) was consulted.
2.4. Extraction of data
Information on author, year of publication, patient demographics, non‐union site, the duration and type of non‐union, characteristics of non‐union tissue (macroscopic/microscopic), cellular characteristics and functions (cell surface protein expression, morphology, viability, proliferation and cellular senescence), molecular characteristics (gene expression, protein expression) and effect of additional interventions were all carefully extracted.
2.5. Data analysis
Outcomes of interest as mentioned in ‘Extraction of data’ section were inserted in an electronic database. Wherever possible, each characteristic of tissue samples was compared across different studies. We also evaluated the effect of any interventions documented in these studies. Qualitative results were summarized and presented in tables, whereas quantitative results are presented with p values if stated by the study. Statistical comparison was not made between studies, due to the heterogeneity in terms of study methodologies observed in each of these in vitro studies.
3. RESULTS
3.1. Literature search
The electronic literature search retrieved 342 citations, of which 24 met the inclusion criteria for the final analysis (Figure 1). 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 Overall, 10 studies 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 assessed non‐union tissue (Table 2), whereas 14 studies 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 investigated relevant tissue (Table 3).
FIGURE 1.
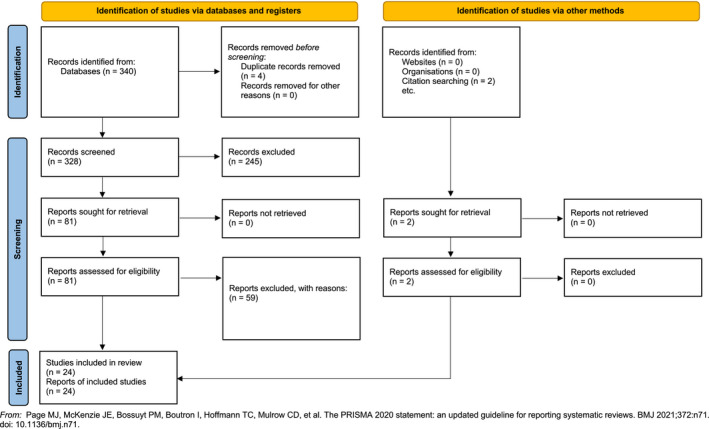
PRISMA 2020 flow diagram—study selection
TABLE 2.
Non‐union tissue: patient demographics
| Author | Year | Time frame | Number of specimens | Site of non‐union | Patients’ age (mean ± SD) | Amount of tissue |
|---|---|---|---|---|---|---|
| Cuthbert 8 | 2020 | Not mentioned | Atrophic non‐union: 20 (11 males); critical size defects requiring induced membrane/Masquelet procedure: 15 (10 males); BMA: 8 (3 males) | Not mentioned | Atrophic non‐union: median age 53, range 23–81; critical size defects requiring induced membrane/Masquelet procedure: median age 61, range 19–80; BMA: median age 38, range 19–52 | Atrophic non‐union: not mentioned; induced periosteum: 1 cm of membrane tissue from centre of bone defect area; BMA: not mentioned |
| Wei 9 | 2020 | Not mentioned | Atrophic non‐union: n = 3; controls (healed fractures): n = 3 | Not mentioned | Not mentioned | Not mentioned |
| Wang 10 | 2018 | Not mentioned | 8 non‐unions compared to 8 with uneventful healing | Not mentioned | Not mentioned | Not mentioned |
| Vallim 11 | 2018 | Not mentioned | 15 (9 male) | Tibia: 3; femur: 4; humerus: 7; ulna: 1 | 46.4 ± 12.5 | Approximately 1 cm3 |
| Takahara 12 | 2016 | Not mentioned | 4 (2 male) | Femur: 1; humerus: 2; clavicle: 1 | 65.3 ± 5.4 | "Small amount" |
| Schira 13 | 2015 | Not mentioned | 80 (77 male) | Scaphoid | 24.6 years (range, 18–71 years) | Not mentioned |
| Han 14 | 2015 | 2009 to 2010 | 11 | Not mentioned | 40 years (range 27–81 years) | Not mentioned |
| Wang 15 | 2014 | October 2010 to March 2014 | Hypertrophic non‐union: 20 (15 male); atrophic non‐union: 20 (14 male) |
Hypertrophic non‐unions: femur 8; femoral neck 1; tibia: 2; humerus: 9. Atrophic non‐unions: femur 5; tibia: 8; humerus: 7. |
Hypertrophic non‐unions: 39.35 ± 11.67 years Atrophic non‐unions: 33.75 ± 8.37 years |
Not mentioned |
| Schwabe 16 | 2014 | Not mentioned | Atrophic non‐union: 44 (22 male) (Histology: 25; GF‐quantification: 19); healed fracture: 13 (7 male) (Histology: 5; GF‐quantification: 8) |
Non‐union: Femur: 16; tibia; 12; clavicle: 9; ulna: 4; humerus: 3. Control group: tibia: 4; ulna: 4; femur: 2; radius: 1; metacarpus: 1 |
49 years (range 20–74 years) | Not mentioned |
| Ismail 17 | 2013 | Not mentioned | 5 (5 male) | Tibia: 1; femur: 3; humerus: 1 | 27.40 years ± 7.64 (range, 18–17 years) | 10 mls of BMA |
Abbreviation: BMA, bone marrow aspirate.
TABLE 3.
Relevant tissue: Patient Demographics.
| Author | Year | Time frame | Number of specimens | Site of non‐union | Patients’ age (mean ± SD) | Amount of tissue |
|---|---|---|---|---|---|---|
| Burska 18 | 2020 | Not mentioned | 15 (study group ‐ 10 union; 5 non‐union); 18 (healthy controls) | Femur, tibia | 15 (study group ‐ 10 union; 5 non‐union; range 18–70 years); 18 (healthy controls; range 26–64 years) | Not mentioned |
| El‐Jawhari 19 | 2019 | Not mentioned | 71 (46 male) | Femur, tibia, humerus | Non‐union group: 49 years (range: 18–76); union group: 44 years (range: 20–75); healthy controls: 42 years (range: 23–60) | BMA: 15mls from ASIS; peripheral venous blood: 12mls; serum from healthy controls: not stated |
| Ouyang 20 | 2019 | Not mentioned | Not mentioned | Not mentioned | Not mentioned | BMA: 2 ml |
| McCoy 21 | 2019 | Biobank (Not mentioned) | 131 (47 male) compared to 1627 (588 male) with uneventful healing | Upper or lower extremity fractures | Control group: 64.3 ± 15.0; non‐union group: 66.8 ± 12.7 | Not applicable |
| Zhang 22 | 2018 | May 2012–April 2015 | 24 (11 male) compared to 24 (11 male) with uneventful healing | Fibular head fracture | Control group: 41.5 ± 11.6; non‐union group: 40.4 ± 11.1 | Not mentioned |
| Huang 23 | 2018 | 2012–2016 | 1229 (346 non‐unions of which 199 males; 883 unions of which 505 males) |
Tibial diaphysis: 113/315; femur diaphysis: 98/233; humeral shaft: 82/188; ulnar shaft: 39/117; femur neck: 14/30 (Non‐union/Union) |
Non‐union: 46.1 ± 8.1; Union: 44.7 ± 8.3 |
Not applicable |
| Granchi 24 | 2017 | Not mentioned | 26 (15 male) | Tibia: 11; femur: 11; humerus: 3; not reported: 1 | 39.6 ± 14 | Not applicable |
| Sathyendra 25 | 2014 | 2005–2010 | Atrophic non‐union: 33 (14 male); normal healing: 29 (18 male) |
Non‐union: femur: 13; tibia; 18; ulna: 2. Normal healing: femur: 10; tibia; 15; humerus: 4. |
Atrophic non‐union: 48.6 years; normal healing: 47.3 years | Not applicable |
| Zeckey 27 | 2011 | 2000–2008 | 50 compared to 44 patients with uneventful healing | Femur: 21; tibia: 29 | 37.5 ± 2.0 | Not applicable |
| Dimitriou 28 | 2011 | 2005–2007 | 62 (45 male) compared to 47 (33 male) with uneventful healing | Tibia: 41; femur: 18; humerus: 2; ulna: 1 | 43.9 years (range, 19–65 years) | Not applicable |
| Marchelli 26 | 2009 | Not mentioned | Atrophic non‐union: 16 (16 male); healed ‐ 6 months: 18 (18 males); healing ‐ 1 month: 14 (14 males) |
Atrophic non‐unions: Tibia: 7; radius: 1; radius + ulna: 3; humerus: 2; femur: 3. Healed: Tibia: 9; radius: 2; radius + ulna: 4; humerus: 1; femur: 2. Healing: Tibia: 8; radius + ulna: 2; humerus: 2; femur: 2. |
Atrophic non‐union: 28.1 ± 5.9 years; healed: 32.2 ± 5.7 years; healing: 31.4 ± 7.1 years | Not mentioned |
| Xiong 29 | 2009 | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Seebach 30 | 2007 | Not mentioned | Not mentioned | Male: 41 ± 15; female: 42 ± 13 | Not mentioned | Not mentioned |
| Henle 31 | 2005 | Jan 2002–Jan 2004 | 15 (12 males) from non‐unions and matched group with uncomplicated unions | Tibia: 11; femur: 2; humerus: 1; forearm: 1 | 47 years (range, 20–75 years) | Not applicable |
Abbreviations: ASIS, anterior superior iliac spine; BMA, bone marrow aspirate.
3.2. Studies characteristics
The study characteristics of the non‐union tissue and relevant tissue are outlined in Table 4. 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 Non‐union was defined based upon radiographic and clinical examination, with minor variations between studies. Samples of non‐union tissue and relevant tissue were mostly obtained during the surgical treatment of non‐unions.
TABLE 4.
Study characteristics of non‐union tissue and relevant tissue
| Author | Duration of non‐union (months) | Classification | Definition of non‐union | Isolation of tissue | Cells/material isolation |
|---|---|---|---|---|---|
| Cuthbert*, 8 | Not mentioned | Atrophic | Not mentioned | Non‐union: Fibrotic tissue lying directly between the fractured bone fragments was excised and collected; induced periosteum from centre of bone defect area; and bone marrow | Colony forming unit fibroblast (CFU‐F) assay; trilineage differentiation; histological analysis of vessel number, size and area; immunohistochemistry (CD45, SDF1, VEGF, BMP‐2); flow cytometry; qPCR; matrigel‐based angiotube formation assay |
| Wei*, 9 | Not mentioned | Atrophic | Not mentioned | Tissue samples were collected intra‐operatively from (i) non‐union tissues of atrophic bone; and (ii) healing callus around internal fixation plates in normal controls. Collected tissues were cut into “small” pieces | RNA isolation, miRNA microarray, bioinformatics of target genes, qPCR, Western blot, luciferase reporter assay |
| Burska**, 18 | Not mentioned | Not mentioned | Failure of the fracture to progress to healing radiographically with the presence of bridging callous on at least 3 cortices by a period of 9 months | Peripheral blood | ELISA |
| El‐Jawhari**, 19 | Not mentioned | Atrophic | Absence of radiological features of fracture healing (lack of callus formation in at least 3 cortices) either on plane radiographs or computed tomography scans after 9 months from fracture fixation and with ongoing pain at the NU site during ambulation | BMA; peripheral venous blood | FACS cell sorting; flow cytometry surface cytokine receptor measurement; flow cytometry—immunosuppression assay: levels of IDO, PGE2 and TGF‐β transcripts; osteogenic differentiation; RNA extraction; RT‐qPCR; proliferation (XTT colorimetric assay); ELISA |
| Ouyang**, 20 | Not mentioned | Not mentioned | Not mentioned | BMA | circRNA microarray, RNA FISH, Osteogenic differentiation assay (ALP and Alizarin red staining), cck‐8 assay, RNA pull‐down assay, double luciferase reporter assay, qPCR, RNA immunoprecipitation, Western Blot |
| McCoy**, 21 | Not mentioned | Not mentioned | Not mentioned | Peripheral blood | DNA was extracted from blood samples |
| Zhang**, 22 | Not mentioned | Not mentioned | Not mentioned | Peripheral blood | DNA was extracted from blood samples |
| Wang*, 10 | Not mentioned | Not mentioned | Not mentioned | Not applicable | Cell viability; mineralization assay; gene expression |
| Vallim*, 11 | 34 months (range 9–120 months) | Not mentioned | Lack of bone healing after 9 months of the fracture | Fibrous tissue interposed between the bone ends was excised, along with adjacent osseous fragments | Histology; population doubling; cell senescence; flow cytometry; osteogenic / adipogenic differentiation |
| Huang**, 23 | >9 months | Not mentioned | The cessation of all healing processes and failure to achieve union within 9 months without radiographic signs of progression of the fracture callus | Peripheral blood | DNA was extracted from blood samples |
| Granchi**, 24 | >3 months | Not mentioned | Not mentioned | BMA, peripheral blood | Immunoenzymatic assays |
| Takahara*, 12 | 14.8 months (range 4–26 months) | Pseudoarthrosis | (1) gross motion at the fracture site on physical examination; (2) bridging bone on 0 of 4 cortices on anteroposterior and lateral radiographs; (3) CT showing no purpose‐ ful cross‐sectional area of healing; and (4) evidence showing the existence of pseudocapsule and fluid collection between the fracture gap at the surgery | A small amount of pseudoarthrosis tissue (pseudocapsule) was obtained during the surgical treatment |
Alizarin Red S staining, ALP activity assay, and RT‐PCR after osteogenic induction. Chondrogenic differentiation capacity was assessed via Safranin O staining and RT‐PCR after chondrogenic induction. Histological analysis and cell cultures |
| Schira*, 13 | 18.3 months (range, 3–100 months) | Not mentioned | Non‐unified fractures >3 months with a resorption zone wider than 1 mm (as determined by a mandatory CT scan) with no apparent potential to heal without surgical intervention | Non‐union tissue (excluding the cortex) and cancellous bone from the ipsilateral radius has been obtained at the time of operative repair | Histology, immunohistochemistry, gene expression |
| Han*, 14 | 11 months (range, 6–30 months) | Not mentioned | Failure of the fracture to heal 6 months or more after surgery or non‐surgical treatment | Fracture and scar tissue during surgery, which was divided into bone stump tissue, marrow cavity contents, and sticking bone scars according to the sites | Histology, immunohistochemistry, gene expression |
| Wang*, 15 |
Hypertrophic non‐unions: 19.88 ± 17.88 months. Atrophic non‐unions: 14.20 ± 7.42 months |
Not mentioned | Failure of the fracture to heal 9 months or more after the injury | Intra‐operative biopsy samples | Immunohistochemistry |
| Schwabe*, 16 | Not mentioned | Not mentioned | Time span from the initial operation until the revision surgery of a least 6 months | Intra‐operative biopsy samples for the treatment of the non‐union or removal of metalwork for the control (normal healing) | Histology, immunohistochemistry, ELISA |
| Sathyendra**, 25 | Not applicable | Not applicable | Minimal callus formation 6 months after injury requiring additional surgery to achieve union | Buccal mucosal cell harvesting | SNP genotype |
| Ismail*, 17 |
37.2 ± 24.0 (range, 12–72) |
Not mentioned | Not mentioned | Intra‐operative BM from the site adjacent to the non‐union, compared to BM from iliac crest. | Not mentioned |
| Marchelli**, 26 | Atrophic non‐union: 6 to 11 months; healed: 8.5 ± 3.5 months; healing: 0.5 ± 0.5 months | Not mentioned | Not mentioned | Blood samples | ELISAs |
| Zeckey**, 27 | >9 months | Aseptic tibial and femoral shaft non‐unions | Clinically and radiologically confirmed unhealed shaft fractures >9 months following the injury and osteosynthesis treatment | Peripheral venous blood sample | DNA was extracted from blood samples |
| Dimitriou**, 28 | Required further intervention to achieve union | Atrophic | Cessation of all healing processes and failure to achieve union after the expected period of time, as seen clinically and radiologically | Peripheral venous blood sample | DNA was extracted from blood samples |
| Xiong**, 29 | Not mentioned | Not mentioned | Fracture that does not heal 6 months after injury | Normal and non‐union callous bone samples examined | Gene expression |
| Seebach**, 30 | Not mentioned | Atrophic | Not mentioned | BM cells were obtained from the iliac crest aspirate | CFU‐F; flow cytometry; osteogenic differentiation |
| Henle**, 31 | >4 months | Atrophic | No bony consolidation of the fracture in conventional X‐ray films and the patient continued to report exercise induced pain 4 months after trauma + no bone healing on CT scan | Venous blood | Immunosorbent assays |
Abbreviations: BM, bone marrow; BMA, bone marrow aspirate.
Non‐union tissue.
Relevant tissue.
3.3. Macroscopic characteristics of non‐union tissue
The macroscopic structure of non‐union tissue was only assessed by Han et al.’s study, whereby tough scars surrounding the site of fracture non‐union were identified. 14 The same team also described bony sclerosis of the fracture ends and complete obliteration of the medullary canal, with fibrous connections found between the fracture fragments. 14
3.4. Microscopic characteristics of non‐union tissue and relevant tissue
3.4.1. Histology
Histological findings of non‐union tissue are summarized in Table 5. 8 , 10 , 11 , 12 , 13 , 14 , 16 Direct comparison of histological findings between atrophic and hypertrophic union is presented in Table 6. 8 , 11 , 13 , 15 , 16 , 32 , 33 , 34 , 36 , 45 , 46 , 49
TABLE 5.
Histological findings of non‐union tissue
| Author | Classification | Histology |
|---|---|---|
| Cuthbert 8 | Atrophic | H&E stain of non‐union tissue: small fragments of dead bone, lack of viable osteocytes, suggesting inadequate clearance by osteoclasts. Lack of viable osteoclasts and greater percentage of pericytes, CD31+ and reduced number of lymphocytes compared to induced membrane tissue. |
| Vallim 11 | Atrophic | Connective tissue with a dense collagenous extracellular matrix, populated by fibroblast‐like cells, and areas of vascularization. |
| Takahara 12 | Pseudoarthrosis | Mainly fibrous tissue with variable amount of fibroblastic cells. Small vessels were sparsely populated. No ossicles or hyaline cartilage were seen in any of the sections examined. |
| Schira 13 | Not mentioned | Pentachrome staining revealed a heterogeneous mix of different tissues, with a domination of connective tissue and fibroblasts in non‐unions, whilst osteoid was the dominant tissue in cancellous bone. Representative TRAP staining of control cancellous bone and scaphoid non‐unions revealed enhanced osteoclasts activity in non‐unions. |
| Han 14 | Not mentioned | Delayed union and non‐union areas comprised a mix of different types of tissues: fracture fragments and surrounding tissues were mainly subject to fibrosis, in which the formation of new blood vessels could be seen, and a small amount of woven bone could be seen nearby. In these woven bones, Gergen Bauer's cells grew along the osteoid as cubes, suggesting active bone formations. A large number of cartilage cells existed in the intramedullary tissues, and there was no new bone and neovascularization. Bone marrow occlusion was observed, and in the fibrous tissue of adjacent bone and the gap of bone fractures, there were internal cartilage ossifications and fibrous ossifications. Scattered lamellar bone fragments were observed in some samples; these fractures were surrounded by osteoclasts, and there was a lack of osteoblasts. |
| Wang 10 | Not mentioned | There were no significant differences in the morphology of atrophic / hypertrophic non‐union tissues. They included MSCs, fibrocartilage cells and hyaline chondrocytes. Some sections showed very few bone islands. BMP‐2‐positive cells were present in both hypertrophic and atrophic non‐union tissue. |
| Schwabe 16 | Not mentioned | The tissue was a very heterogeneous mixture of fragments of lamellar bone, immature and hypertrophic cartilage, unorganized fibrous tissue and newly formed woven bone. Independent of the group, bone apposition and resorption were seen in the tissue samples. Differences between the groups were not obvious. |
TABLE 6.
Comparison of histological findings between atrophic—hypertrophic non‐unions
| Atrophic | Hypertrophic | |
|---|---|---|
| Type of tissue | ||
| Fibrocartilaginous tissue | 33, 34 | 34, 46 |
| Fibrous tissue | 16, 32, 34 | 34, 36 |
| Cartilaginous tissue | 16 | 32, 34, 45 |
| Collagenous extracellular matrix/connective tissue | 11, 13, 32, 33 | 32, 33, 45 |
| Bone tissue |
No ossicles 32 ; occasional bony islands 15 , 33 , 34 ; lack of viable osteoclasts and greater percentage of pericytes, CD31+ and reduced number of lymphocytes compared to induced membrane tissue 8 Mixture of lamellar and woven bone 16 |
No ossicles 32 , 36 ; bony islands 15 , 34 , 45 , 46 |
| Necrotic bone | More prevalent 34 | ‐ |
| Bone production | Predominantly via the endochondral route 34 | Bone formation by both endochondral and intramembranous ossification 34 |
| Cells | ||
| Vascularization | Well vascularized 34 | |
As only reporting on studies published after our original review 1 would provide an incomplete picture of the differences between atrophic and hypertrophic non‐unions, we include all relevant data regardless of publication date.
References highlighted bold: new references published after our original review. 1
3.4.2. Immunohistochemistry
The immunohistochemical findings of non‐union tissue and relevant tissue are summarized in Table 7. 8 , 13 , 14 , 15 , 16 , 18 , 19 BMPs were present in non‐union tissue. 8 , 14 Interestingly, Han et al. found BMP to be locally generated by non‐union tissue. 14 Additionally, BMP antagonists were also found to be present in both normal and non‐union tissue alike. 16 ALP and SMAD2/3 were both found to be increased in scaphoid non‐union tissue. 13 Cuthbert et al. also confirmed the presence of SDF‐1 and VEGF in non‐union tissue. 8
TABLE 7.
Immunohistochemistry findings
| Author | Classification | Immunohistochemistry |
|---|---|---|
| Cuthbert 8 | Atrophic | Presence of SDF‐1, VEGF and BMP‐2 in NU tissue. CD 45 staining: greater in induced membrane than in non‐union. Non‐union tissue contains significantly greater percentage of cells expressing (i) pericyte (13.8% vs. 4.9%), (ii) CD31+ endothelial cells (18.2% vs. 5.5%) phenotypic markers. Non‐union tissue had significantly reduced numbers of lymphocytes (6.8% vs. 22.2%) |
| Burska 18 | Not mentioned |
PIGF was higher in non‐union patients, reaching significance at Days 1 and 3 (p < 0.05); but less marked at Day 5 (p = 0.09). PIGF displayed initial massive surge followed by rapid decline in non‐union patients. TGF‐beta 2 appeared higher in union group (not statistically significant). Levels of MCP‐1 and IL8 showed no clear difference between non‐union and union groups. |
| El‐Jawhari 19 | Atrophic | IFN‐γ, TNF‐α and IL‐1 levels similar between non‐union, union and control arms. However, lower levels of IL‐17 detected at later stages of fracture healing (vs. union and control arms) |
| Schira 13 | Atrophic | ALP reached higher levels in scaphoid non‐unions as opposed to cancellous bone. Likewise, immunofluorescence for phosphorylated SMAD2/3 revealed increased activity in scaphoid non‐unions. |
| Han 14 | Not mentioned |
The depth of BMP‐2 staining in the cytoplasm increased with increasing proximity to the new bone formation region, and there was some staining of the Golgi apparatus, showing that BMP‐2 was locally generated. A wide variety of cells, including epithelial cells, smooth muscle cells around the small blood vessels, fusiform fibroblast‐like cells and chondrocyte cells, showed positive staining in the fibrous tissues, indicating osteogenesis. There was no difference in the immunostaining of fibrous tissue between the samples with and without new bone. There was no positive BMP staining in the extracellular matrix or the fibrous tissue space. Sub‐parts of view, fracture fragments were mainly fibrotic tissues and BMP‐2 staining was negative. In the surrounding tissues, especially in the sticking scars and posted plate scars, neovascular and woven bone filled in a lot of the fibrous tissues, and in the vicinity, there were stained cells, indicating BMP‐2 expression. There was a small amount of cartilage with positive staining in the cytoplasm, without expression in fibrous tissues of the closed medullary cavity. DCN expression was extensive in the interstitial fracture fragments. There was no positive staining of cartilage cells in the medullary cavity. DCN expression in the sticking scars was close to perivascular. The rate of expression of BMP‐2 was highest in the posted bone scar group, and was low in the bone ends and canal content group (p < 0.05). There was no significant difference between the other two groups. The fracture fragment group had the highest DCN expression, with significant differences from the other two groups; the least significant difference analysis showed that between the fracture fragment group and the other two groups, p < 0.05; between the other two groups, p > 0.05 |
| Wang 15 | Atrophic/hypertrophic | The mean optical density of BMP‐2 was 0.154 ± 0.041 in hypertrophic non‐union tissue, 0.137 ± 0.037 in atrophic non‐union tissue, there was no significant difference between the 2 groups (p > 0.05). The mean optical density of BMP‐2 was 0.148 ± 0.040 in the 20‐ to 35‐year‐old group, 0.142 ± 0.040 in the 35‐ to 50‐year‐old group, 0.146 ± 0.056 in the more than 50‐year‐old group, there was no significant difference among the three groups (p > 0.05). The mean optical density of BMP‐2 was 0.145 ± 0.037 in the 9–12 months group, 0.147 ± 0.0400 in the 13–24 months group, 0.145 ± 0.054 in the more than 24 months group, there was no significant difference among the 3 groups (p > 0.05). |
| Schwabe 16 | Atrophic | Bone morphogenic antagonists were demonstrated in non‐union and control tissue. |
In terms of relevant tissue, peripheral PIGF levels were found to be higher in non‐union patients, with an initial surge followed by a rapid decline. Both TGF‐ß2 20 and IL‐17 19 on the contrary were reported to be lower in non‐union patients.
3.4.3. Analysis of vessel calibre, area and density
Blood vessels were present in cases of hypertrophic non‐unions, with a varying density (Table 8). 8 , 13 , 16 Only one study assessed vessel density in atrophic non‐unions, reporting a 2.4‐fold increase when compared against that of induced periosteal membrane (control group). 8 However, both vessel calibre and median area were smaller in non‐union tissue in this study. 8 All these reaffirms histological findings whereby vascular tissue was found to be present in both atrophic and hypertrophic non‐unions. 11 , 12 , 14 , 16
TABLE 8.
Analysis of vessel density
| Author | Analysis of vessel density |
|---|---|
| Cuthbert 8 | 2.4‐fold increase in non‐union tissue when compared against induced membrane tissue. Both calibre and median internal vessel area of bloods vessels in NU tissue were smaller compared to induced membrane. |
| Schira 13 | Angiogenesis in scaphoid non‐unions is similar to cancellous bone. Blood vessels and endothelial cells were detected by immunohistochemical staining of PECAM‐1 in non‐unions and controls revealing similar levels of angiogenesis in both tissues. |
| Schwabe 16 |
Histology: Vessels were present in all investigated samples without a difference between the tissue from non‐union and control patients. Immunohistochemistry: well vascularized but also unvascularized areas with no difference between the non‐union and the control tissue. |
3.5. Cellular characteristics and functions
3.5.1. Cell surface protein expression
Altogether, four studies evaluated the expression of cell surface protein using flow cytometry (Table 9). 11 , 12 , 17 , 19 Non‐union tissue was found to be positive for MSC‐related markers CD73, 11 , 17 CD90 11 , 17 and CD105, 11 , 12 , 17 but negative for haematopoietic markers CD14, 17 CD34, 17 CD45 12 , 17 and HLA‐DR. 17 El‐Jawhari et al. demonstrated in relevant tissue in the form of BM‐MSC harvested from the iliac crest of non‐union patients to express lower levels of IL‐1R1 compared to controls. 19
TABLE 9.
Cell surface protein expression
| Author | Cell surface protein expression (flow Cytometry) |
|---|---|
| El‐Jawhari 19 |
|
| Vallim 11 |
Compared to BM MSC and osteoblasts, non‐union MSCS:
|
| Takahara 12 | Consistently positive for MSC‐related markers such as CD29, CD44, CD105 and CD166. The cells were negative for haematopoietic‐lineage markers such as CD31, CD34, CD45 and CD133. |
| Ismail 17 | There was positive expression of CD105, CD73 and CD90 for at least 95%, negative expression of CD45, CD34, CD14 or CD11b, CD79a or CD19, and HLA‐DR. |
Abbreviations: BMSC, bone marrow stromal cells; MSC, mesenchymal stem cells; NUSC, non‐union stromal cells.
3.6. Morphology, viability, proliferation and cellular senescence
The (i) cell morphology, viability and proliferation of non‐union tissue; and (ii) the effect of non‐union serum on proliferation of BM‐MSCs are outlined in Table 10. 8 , 10 , 11 , 12 , 17 , 19 Overall, non‐union MSCs were found to have comparable proliferative capacities and viability to that of BM‐MSCs. 8 , 10 , 11 , 12 , 17 On the contrary, non‐union serum was found to have a negative effect on MSC proliferation. 19 Comparing the cell senescence rates of non‐union MSCs and those of bone marrow MSCs, Vallim et al. found no difference between the two groups. 11
TABLE 10.
Cell culture characteristics and functions
| Author | Classification | Intervention | Cell morphology | Cell viability (MTT‐Test) | Cell proliferation |
|---|---|---|---|---|---|
| Cuthbert 8 | Atrophic | Not applicable | Not applicable | Not applicable | Cells isolated from non‐union tissue behave similarly to that of BMA, readily forming colonies. CFU‐F from non‐union tissue were comparable to that of induced membrane tissue, indicating no difference in MSC content between the two tissues. |
| El‐Jawhari 19 | Atrophic | MSC cultured in non‐union serum vs. union serum | Not applicable | Not applicable | Non‐union serum has negative effect on MSC proliferation (p = 0.031). |
| Wang 10 | Not mentioned | Chordin, Noggin and Gremlin expression knockdown | Not applicable | The cell viability of MSCs remained unchanged with PSI. By contrast, the cell viability of PEI25 kDa‐treated MSCs dramatically dropped to 20% of the original value when the polymer concentration reached 15 μg/ml. | Not applicable |
| Vallim 11 | Not mentioned | Non‐union MSCs, BM MSCs and osteoblasts were transplanted into the subcutaneous tissue of immunodeficient mice | Not applicable | Not applicable | Non‐union MSCs had proliferative and rates comparable to BM MSCs and osteoblasts. The percentage of cells staining positive for b‐galactosidase activity in non‐union MSCs cultures was comparable to those observed in BM MSCs and osteoblasts. |
| Takahara 12 | Pseudoarthrosis | Not applicable | Fibroblast‐like spindle shape | Not applicable | Could be cultured through at least 10 passages, with minimal decline in their proliferative capacity |
| Ismail 17 | Not mentioned | Not applicable | Not applicable |
Non‐union: viability of 87.1% (81.7%–90.8%); iliac crest: 89.8% (84.7%–94.5%). No differences were found between the two sources of MSCs (p = 0.175). |
Not applicable |
Abbreviations: BMA, bone marrow aspirate; BMP, bone morphogenic protein.
3.6.1. Mineralization and Alkaline phosphatase (ALP) activity assay
The outcomes of mineralization assay for non‐union tissue are outlined in Table 11. 10 , 11 , 12 , 13 , 24 , 26 The findings of the four studies which evaluated ALP activity and its mRNA expression are outlined in Table 12. 12 , 13 , 24 , 26
TABLE 11.
Osteocalcin expression and mineralization assay
| Author | Classification | Intervention | Osteocalcin | Mineralization Assay |
|---|---|---|---|---|
| Wang*, 10 | Not mentioned | Chordin, Noggin and Gremlin expression knockdown | Promoted by Chordin knockdown, more strongly than Gremlin. Decreased by Noggin knockdown | The osteogenic differentiation of MSCs isolated from non‐unions was lower than those isolated for patients with uncomplicated healing |
| Vallim*, 11 | Not mentioned | Non‐union MSCs, BM MSCs and osteoblasts were transplanted into the subcutaneous tissue of immunodeficient mice | Not applicable | Non‐union MSCs deposited mineralized matrix positive for Von Kossa, similarly as BM MSCs and osteoblasts |
| Granchi**, 24 | Not mentioned | Regenerative approach consisted in a minimally invasive administration of autologous bone marrow cells expanded in good manufacturing practice (GMP) facilities |
After regenerative treatment:
Intact osteocalcin and N‐terminal/midregion osteocalcin levels were significantly decreased at 6 weeks in patients healed after 24 weeks, to increase afterwards, with changes not significantly different from baseline values. |
Not applicable |
| Takahara*, 12 | Pseudoarthrosis | Not applicable | Its expression under osteogenic conditions was upregulated compared with those under control conditions, and had a similar pattern to that shown by BMSCs. | Formed a mineralized matrix as observed on Alizarin Red S staining, contrasting with the absence of a mineralized matrix under control conditions after the same duration |
| Schira*, 13 | Not mentioned | Not applicable | Similar expression pattern in non‐union tissue and controls. | Not applicable |
| Marchelli**, 26 | Not mentioned | Not applicable | Serum osteocalcin levels in non‐unions were similar to healed and healing fractures (p > 0.05) | Not applicable |
Non‐union tissue.
Relevant tissue.
TABLE 12.
ALP activity and ALP related mRNA expression
| Author | Classification | Intervention | ALP activity assay | ALP mRNA |
|---|---|---|---|---|
| Granchi**, 24 | Not mentioned | Regenerative approach consisted in a minimally invasive administration of autologous bone marrow cells expanded in good manufacturing practice (GMP) facilities |
After regenerative treatment:
Bone‐specific ALP correlated to the imaging results collected at 12 and 24 weeks. Its variation along the healing course differed in patients who had an early consolidation (at 12 weeks). A remarkable decrease in ALP was observed at all time points in a single patient who experienced a treatment failure. |
Not applicable |
| Takahara*, 12 | Pseudoarthrosis | Not applicable | ALP activity increased with time and declined on Day 28. By contrast, under control conditions, ALP activity in culture remained low between days 7 and 28. ALP activity under osteogenic conditions was significantly higher than that under control conditions on days 14 and 21 (p = 0.0179 and 0.0489 respectively). | Its expression under osteogenic conditions was upregulated compared with those under control conditions, and had a similar pattern to that shown by BMSCs. |
| Schira*, 13 | Not mentioned | Not applicable | Not applicable | ALP was significantly upregulated across all non‐unions. |
| Marchelli**, 26 | Not mentioned | Not applicable | Serum ALP levels in non‐unions were similar to healed and healing fractures (p > 0.05) | Not applicable |
Abbreviations: BMP, bone morphogenic protein; ALP, alkaline phosphatase; mRNA, messenger RNA; CFU, colony forming units
Non‐union tissue.
Relevant tissue.
3.7. Molecular characteristics
3.7.1. Protein and micro RNA levels
Wang et al. utilized Western blot assay to evaluate the expression of p‐SMAD1/5/8 protein in non‐union tissue and that of ‘normal’ fracture healing. 10 The same team also reported decreased expression of p‐SMAD1/5/8 in MSCs isolated from patients with non‐union. 10 Interestingly, chordin knockdown was found to rescue the osteogenic capacity of MSCs of non‐union patients. 10 Wei et al. identified the four micro RNAs (miRNAs) significantly upregulated in atrophic non‐unions (hsa‐miR‐149∗, hsa‐miR‐221, has‐miR‐628‐3p and hsa‐miR‐654‐5p); and upon transfection of BM‐MSCs with the same four miRNAS, significantly decreased its expression of ALPL, PDGFA and BMP2. 9 Marchelli et al. found that serum osteocalcin levels in non‐unions were similar to healed and healing fractures (p > 0.05). 26 Interestingly, Granchi et al. demonstrated that osteocalcin and N‐terminal/midregion osteocalcin levels to be significantly decreased at 6 weeks, followed by a return to levels similar to baseline values. 24
3.7.2. Gene expression and genetic predisposition
Several authors have examined the expression of different genes in the non‐union tissue 8 , 10 , 12 , 13 , 14 and relevant tissue. 19 , 21 , 22 , 23 , 25 , 27 , 28 , 29 Summaries of their results are outlined in Tables 12, 12 , 13 , 24 , 26 and 13. 8 , 10 , 12 , 13 , 14 , 19 , 21 , 22 , 23 , 25 , 27 , 28 , 29
TABLE 13.
Gene expression/genetic predisposition
| Author | Gene expression/genetic predisposition |
|---|---|
| Non‐union tissue | |
| Cuthbert 8 |
|
| Wang 10 |
|
| Takahara 12 |
|
| Schira 13 |
|
| Han 14 |
|
| Relevant tissue | |
| El‐Jawhari 19 |
|
| McCoy 21 |
|
| Zhang 22 |
|
| Huang 23 |
|
| Sathyendra 25 |
|
| Zeckey 27 |
|
| Dimitriou 28 |
|
| Xiong 29 |
|
Takahara et al. discovered that non‐union tissues behaved in a similar fashion to that of BM‐MSCS, whereby osterix and bone sialoprotein expression were both upregulated in non‐union tissue cultured under osteogenic conditions, when compared against control conditions. 12 Even more interestingly, under osteogenic conditions, Takahara et al. found that the expression of bone sialoprotein had a similar pattern to that shown by BM‐MSCs. 12 Schira et al. reported similar patterns of Dickkopf‐1 expression in both scaphoid non‐union tissue and controls (cancellous bone adjacent to non‐union site). 13 In terms of osteocalcin expression of non‐union MSCs, both Takahara and Schira et al. found this to be similar to that of BM‐MSCs (control). 12 , 13
Studies on relevant tissue have also investigated genetic predisposition to fracture non‐union and identified numerous polymorphisms and genotypes associated with the increased risk of developing non‐union (Table 13). 21 , 22 , 23 , 25 , 27 , 28 , 29
3.7.3. Comparison between atrophic and hypertrophic non‐unions
Table 14, 8 , 13 , 15 , 16 , 19 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 provides a summarized comparison between tissues (non‐union tissue and relevant tissue) obtained from patients with atrophic and hypertrophic non‐unions.
TABLE 14.
Comparison between atrophic/hypertrophic non‐union tissue
| Type of analysis | Atrophic | Hypertrophic |
|---|---|---|
| Histology | Table 6 | |
| Immunohistochemistry |
SMAD2/3 revealed increased activity in non‐unions 13 Close vicinity to immature osteoid trabeculae 35 SDF‐1, VEGF, BMP‐2 present in non‐unions 8 IL‐17 levels lower at later stages of fracture healing in non‐union BM‐MSC. IFN‐γ, TNF‐α, and IL‐1 levels in non‐union group similar to union and control group 19 |
‐ |
| Vessel density |
No difference in the median vessel count between atrophic/hypertrophic non‐unions 34 2.4‐fold increase in non‐union tissue when compared against induced membrane tissue 8 |
No difference in the median vessel count between atrophic/hypertrophic non‐unions 34 |
| Cell surface antigen profile |
Less than 1% of NUSC and BMSC were positive for CD34 and CD45, whilst 78% ± 14% of NUSC and 92% ± 7% of BMSC were positive for CD105 33 Lesser IL‐1R1 surface protein and transcripts in uncultured non‐union BMMSC; whilst no significant difference in IFNGR1, TNFRS1A AND IL‐17RA when compared to union group 19 |
Positive for MSC‐related markers CD13, CD29, CD44, CD90, CD105, and CD166, but negative for hematopoietic markers CD14, CD34, CD45, and CD133 36 |
| Cell morphology | Cells formed a uniform monolayer of elongated cells that had few cellular extensions 32 | Also consisted of elongated cells, but the cells were more cuboidal, having cellular extensions in a multilayer 32 |
| Cell Proliferation |
Cells differentiate along each mesenchymal lineage 33 Cells isolated from non‐union tissue behave similarly to that of BMA, readily forming colonies 8 |
Significantly inferior to that of fracture haematoma cells 36 |
| ALP Activity |
No differences between atrophic/hypertrophic non‐unions 32 Higher levels in scaphoid non‐unions as opposed to cancellous bone 13 Markedly lower than that for BMSC cultures 33 |
No differences between atrophic/hypertrophic non‐unions 32 No difference with controls 37 |
| Osteocalcin | Very low levels 32 |
Very low levels 32 ; higher than in human dermal fibroblasts 36 The expression of osteocalcin under osteogenic conditions was higher than under undifferentiated conditions in the control group 36 |
| BMPs |
No significant difference in BMP‐2 levels between atrophic/hypertrophic non‐unions 15 BMPs antagonists present in non‐union tissue and controls 16 |
No significant difference in BMP‐2 levels between atrophic/hypertrophic non‐unions 15 BMP‐2: present in the fibrous tissue of the non‐union 39 BMP‐7: absent 39 |
| MMP | ‐ | MMP‐7 and MMP‐12 were present 38 |
| Mineralization Assay | Significant reduction in the MSCs capacity to differentiate along an osteoblastic lineage compared to BMSC 33 |
Higher than haematoma cells 36 Very low mineralization potential and significantly lower than ‘normal’ human osteoblasts 37 Under osteogenic conditions, mineralization was significantly higher than that of fracture haematoma cells, in contrast to undifferentiated conditions 36 |
As only reporting on studies published after our original review 1 would provide an incomplete picture of the differences between atrophic and hypertrophic non‐unions, we include all relevant data regardless of publication date.
References highlighted bold: new references published after our original review. 1
3.7.4. Effect of interventions on non‐union tissue and relevant tissue
Table 15, 10 , 19 outlines the effects of interventions on the non‐union tissue, 10 and BM‐MSC cultured in serum taken from non‐union patients (relevant tissue). 19
TABLE 15.
Effect of interventions
| Author | Wang 10 | El‐Jawhari 19 |
|---|---|---|
| Type of Intervention | Chordin, Noggin and Gremlin expression knockdown |
BM‐MSC cultured in:
|
| Cell Proliferation | Not applicable | Non‐union serum has negative effect on BM‐MSC proliferation (p = 0.031). |
| Transforming Growth Factor‐β1 | Not applicable | Lower levels in cytokine treated (IFN‐γ, TNF‐α, IL‐1 and IL‐17) NU BM‐MSC |
| Osterix | Promoted by Chordin knockdown, more strongly than Gremlin. Decreased by Noggin knockdown | Not applicable |
| Osteocalcin | Promoted by Chordin knockdown, more strongly than Gremlin. Decreased by Noggin knockdown | Not applicable |
| Mineralization Assay | Chordin knockdown rescued the osteogenic ability of hBMSCs isolated from patients with non‐union | Not applicable |
| Col1a1 | Promoted by Chordin knockdown, more strongly than Gremlin. Decreased by Noggin knockdown | Not applicable |
4. DISCUSSION
Fracture non‐union represents a significant public health problem with detrimental socioeconomic costs. In addition to productivity losses, the direct treatment cost of established non‐union in the UK has been estimated to be in the regions of £7,000 and £79,000 per person, dependent on its complexity. 40 With multiple pathophysiological factors influencing its progression, fracture non‐union remains a challenging condition to treat. 41 The improved understanding of its pathophysiology has seen the evolution with the treatment of non‐unions, from prolonged immobilization in the 1950s 42 to the modern techniques of biological stimulation and polytherapy. 43
The commonest macroscopic appearance of non‐unions is soft tissue interposition between fracture fragments. 14 , 42 , 44 Han et al.’s study furthered this description, reporting bony sclerosis of fracture ends and complete obliteration of medullary canal. 14 Additionally, non‐union tissue colour and its surrounding fluid are also important characteristics used to differentiate between septic and aseptic non‐unions (white tissue and clear surrounding fluid: aseptic; yellowish tissue and murky surrounding fluid: septic). Taken altogether, macroscopic appearances of the fracture site immediately visible to the treating surgeon in the operating theatre could serve as a powerful visual marker, aiding the confirmation/suspicion of a septic non‐union. More importantly, it could support surgeons with prompt surgical decision and the swift treatment of septic non‐unions. 1
In terms of histological analysis, several similarities exist between atrophic and hypertrophic non‐unions. Firstly, fibrous, cartilaginous and connective tissues were historically reported to be the tissue types common to both atrophic and hypertrophic non‐unions. 32 , 33 , 34 , 36 , 45 , 46 Studies included in this systematic review 11 , 13 , 16 confirm these findings. Secondly, bony islands were not always present in both atrophic 15 , 32 , 33 , 34 and hypertrophic non‐unions. 15 , 32 , 34 , 36 , 45 , 46 Thirdly, whilst fibroblast‐like cells account for the majority of the population in both atrophic and hypertrophic non‐unions, 11 , 13 , 33 , 36 MSCs were still present in both tissues. 15 However, several differences also exist. Atrophic non‐unions contain a mixture of lamellar and woven bone, 16 with a prevalence of necrotic bone, 8 , 34 lack of viable osteocytes and osteoclasts, 8 and a predominance of endochondral bone formation. 34 In contrast, bone formation in hypertrophic non‐unions were reported to occur equally through both endochondral and intramembranous ossification. 34 Furthermore, cellular density was lower in atrophic non‐unions, with some areas being completely acellular. 32 , 33 Collectively speaking, these differences in both the cellularity and local environment may account for the higher failure rate observed following revision surgery in atrophic non‐union cases. 47
Contrary to common historical belief that atrophic non‐unions are relatively avascular and inert, 34 , 48 several authors have confirmed the presence of vascular tissue, evidenced by histological analysis of atrophic 11 , 32 , 33 , 34 , 49 and hypertrophic 34 non‐union tissues, with no major differences between the two. 34 Similar to the study by Reed et al., 34 vessel density of non‐union tissue in new studies was largely found to be at similar levels in non‐unions and cancellous 13 or healing bone. 16 Interestingly, Cuthbert et al. reported a 2.4‐fold increase in the vessel density of atrophic non‐union tissue, although the calibre and median internal vessel area were found to be smaller when compared against controls. 8 These findings are promising as it highlights a research area which has the potential to restore and enrich local angiogenesis, and ultimately successful fracture healing.
Bajada et al. first reported in 2009 the presence of cells positive for MSCs‐related markers and negative for haematopoetic markers in non‐union tissue. 33 This was later confirmed by other authors, whereby non‐union tissue was found to contain biologically active cells with the potential to differentiate into osteoblastic, chondrogenic and adipogenic lineages. 11 , 12 , 17 , 36 , 50
With regard to culture characteristics of the non‐union tissue, only a few of the current list of studies assessed cell morphology, viability and proliferation. Both studies by Cuthbert et al. and Vallim et al. found the proliferative capacity of MSCs isolated from non‐union tissue to be comparable to that of BM‐MSCs. 8 , 11 Furthermore, the proliferative capacity of non‐union MSCs was found to have minimal decline following multiple passages. 12 However, when compared against studies published in our previous review, 1 we found an inconsistency in the reported findings on culture characteristics. This could be explained by the variability in the type of non‐union tissue examined, the geographical location of non‐union tissue and sample size.
Cell senescence have been found to impair the regenerative and therefore healing potential of MSCs and differentiated cells in non‐union tissue. 51 There is, however, variation in terms of rates of senescence of non‐union tissues found in the literature—Vallim et al. reported senescence rate to be no different, 11 whereas Bajada et al. reported increased proportion of senescent non‐union MSC when compared against BM‐MSC. 33 Further work is therefore warranted since the influence of contributory factors (such as repeated cellular replication and stress) and pathways leading to the genomic damage in senescent non‐union MSCs remains unknown.
Bone morphogenic protein (BMP) plays a key role as a signalling molecule in promoting the MSC osteoblastic and chondrogenic differentiation and has therefore been extensively studied given its important role in the field of bone regeneration. 52 , 53 Interestingly, studies have reported evidence of BMP signalling and generation in non‐union MSCs, 8 , 14 , 49 with no difference in BMP expression between atrophic and hypertrophic non‐unions. 15 Noteworthy, BMP expression was found to be low in the bone ends and canal contents of the non‐union site, and absent in the extracellular matrix. 14 The effects of BMP on non‐union cell cultures in vitro have also been assessed, with improved osteogenic differentiation and increased ALP levels of osteocalcin expression and mineralization potential observed following addition of BMP. 54 , 55
Studies by Wang et al. and Fajardo et al. have further shed light on the important topic of homeostasis between gene expression of BMP and its inhibitors (Chordin, Noggin and Gremlin). 10 , 39 Both studies identified reduced BMP‐7 gene expression and elevated levels of Chordin, Gremlin and Noggin. 10 , 39 Wang et al. went on to investigate the effects of Chordin, Gremlin and Noggin knockdown—reporting increased expression of osterix, osteocalcin and collagen following Chordin and Gremlin knockdown. 10 Furthermore, they also demonstrated Chordin knockdown to rescue the osteogenic ability of non‐union cells. 10 Taken altogether, these findings support the idea of imbalance expression between BMP and its inhibitors driving the pathophysiology of impaired bone healing observed in non‐union MSCs. 16 , 39 , 56
Matrix metalloproteinases (MMP) are important key player, which modulate bone remodelling and repair. Disruption to either MMP or their inhibitors could result in disorders of fracture healing. 38 In vitro studies on hypertrophic non‐union tissues have found MMP to bind directly and degrade BMP‐2, known to be an osteoinductive molecule. 38 Furthermore, non‐union tissues were found to have an upregulation of MMP‐7, MMP‐9 and MMP‐17 genes. 13 , 38 All these findings highlight the potential role of MMP as one of the key players in the pathogenesis of fracture non‐union.
Although Dkk‐1 is well known as an antagonist of the Wnt signalling pathway inhibiting osteogenic differentiation, 33 , 57 Dkk‐1 expression by non‐union tissue has only been investigated by two studies, reporting similar expression when compared against BM‐MSC 33 and healthy cancellous bone. 13 However, release of Dkk‐1 by atrophic non‐union MSCS cultured in osteogenic conditions was higher than that of BM‐MSCs. 33 Whilst this study suggests the potential role of Dkk‐1 in the pathophysiology of non‐union, further research is still warranted to better understand the mechanism of action which Dkk‐1 plays in causing non‐union.
There has been emerging evidence over the recent years on the genetic predisposition of fracture non‐union. 19 , 21 , 22 , 23 , 25 , 27 , 28 , 29 Numerous genetic polymorphisms associated with fracture non‐union have been identified, with some involving the BMP 25 , 28 and MMP pathways. 25 , 27 However, most of these studies were significantly underpowered due to is small number of patients and single nucleotide polymorphism (SNP) investigated. Additionally, Wei et al. have identified four micro RNAs (miRNAs) significantly upregulated in atrophic non‐unions (hsa‐miR‐149∗, hsa‐miR‐221, has‐miR‐628‐3p and hsa‐miR‐654‐5p); and result in the significant decrease in the expression of ALPL, PDGFA and BMP2. 9 Comprehensive analysis on a wider genomic profile combined with bioinformatics may reveal genes, SNPs and miRNAs responsible for the acceleration or inhibition of fracture healing—serving as potential key targets of novel gene therapies.
This literature review is not without its limitations. Firstly, this review excludes animal studies and those which involve experimental animal models, since direct clinical translation is often difficult. Secondly, heterogeneity with the definition of non‐union, timing of tissue harvest and laboratory assays may all account for the different results reported in studies. Lastly, the abbreviation/term MSC is only more recently used in this field, which could be referred to as mesenchymal stem cells or mesenchymal stromal cells. 58 As such, historical studies using alternative terms such as ‘osteoprogenitors’ and ‘skeletal stem cells’ were excluded as authors felt it does not guarantee the accuracy of comparison made.
There are several strengths of this systematic review. This includes the systematic approach on both screening and analysis of the findings from current literature. Furthermore, this systematic review provides an up‐to‐date understanding on the biological profile of non‐union tissue and relevant tissue at a cellular and molecular level. Due to the huge heterogeneity in available evidence, we are unable to recommend any direct clinical application. The complex pathophysiology of non‐union requires the treating clinician to consider the interaction between biological, physiological and molecular components of the ‘diamond concept’ of bone healing. 59 Cellular therapies with osteogenic cells and osteoinductive molecules, osteoconductive scaffolds and tissue engineering are treatment strategies which holds great promise. 60 , 61 Although still in its early stages, further work on the molecular and genetic profiling of relevant tissue such as patient's serum could serve as an advantageous screening and predictive tool of fracture non‐union.
5. CONCLUSION
Fracture non‐union is a challenging condition to treat and poses significant health and socioeconomic burden. Both atrophic and hypertrophic non‐unions were found to possess some degree of vascularity, with resident populations of MSCs with osteogenic capacities. The imbalance in the homeostasis between BMP, chordin, noggin, gremlin and Wnt pathways were believed to be contribute towards non‐union. Increasing body of evidence has identified genetic predisposition in patients with non‐union. Further research is required on determining the sensitivity and specificity of molecular and genetic profiling of relevant tissues as a potential screening biomarker for fracture non‐unions. Other targets of future research include the isolation of specific genes involved in the process of non‐union and the effect of their up‐ or down‐regulation. This along with research around the reactivation of the resident MSCs could potentially revolutionize the management of non‐unions.
CONFLICTS OF INTEREST
All authors declare no conflict of interest.
AUTHOR CONTRIBUTION
Michalis Panteli: Conceptualization (lead); Data curation (lead); Formal analysis (lead); Investigation (lead); Methodology (lead); Project administration (lead); Resources (lead); Validation (lead); Visualization (lead); Writing – original draft (lead); Writing – review & editing (lead). James SH Vun: Data curation (supporting); Formal analysis (supporting); Visualization (supporting); Writing – original draft (supporting); Writing – review & editing (supporting). Ippokratis Pountos: Conceptualization (supporting); Methodology (supporting); Supervision (supporting); Visualization (supporting); Writing – original draft (supporting); Writing – review & editing (supporting). Anthony J Howard: Data curation (supporting); Formal analysis (supporting); Writing – original draft (supporting); Writing – review & editing (supporting). Elena Jones: Conceptualization (supporting); Methodology (supporting); Project administration (supporting); Supervision (supporting); Writing – review & editing (supporting). P. V. Giannoudis: Conceptualization (equal); Methodology (equal); Project administration (equal); Supervision (equal); Writing – original draft (supporting); Writing – review & editing (supporting).
ACKNOWLEDGEMENTS
MP and JV performed the research. MP and PVG designed the research study. MP, JV and PVG analysed the data. MP and JV wrote the paper. All authors contributed to the preparation of the manuscript.
Panteli M, Vun JSH, Pountos I, Howard AJ, Jones E, Giannoudis PV. Biological and molecular profile of fracture non‐union tissue: A systematic review and an update on current insights. J Cell Mol Med. 2022;26:601–623. doi: 10.1111/jcmm.17096
Funding information
No funding was received.
REFERENCES
- 1. Panteli M, Pountos I, Jones E, et al. Biological and molecular profile of fracture non‐union tissue: current insights. J Cell Mol Med. 2015;19(4):685‐713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Einhorn TA, Gerstenfeld LC. Fracture healing: mechanisms and interventions. Nat Rev Rheumatol. 2015;11(1):45‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: the diamond concept. Injury. 2007;38(Suppl 4):S3‐6. [DOI] [PubMed] [Google Scholar]
- 4. Calori GM, Giannoudis PV. Enhancement of fracture healing with the diamond concept: the role of the biological chamber. Injury. 2011;42(11):1191‐1193. [DOI] [PubMed] [Google Scholar]
- 5. Bishop JA, Palanca AA, Bellino MJ, et al. Assessment of compromised fracture healing. J Am Acad Orthop Surg. 2012;20(5):273‐282. [DOI] [PubMed] [Google Scholar]
- 6. Hak DJ, Fitzpatrick D, Bishop JA, et al. Delayed union and nonunions: epidemiology, clinical issues, and financial aspects. Injury. 2014;45(Suppl 2):S3‐7. [DOI] [PubMed] [Google Scholar]
- 7. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cuthbert R, Jones E, Sanjurjo‐Rodríguez C, et al. Regulation of angiogenesis discriminates tissue resident MSCs from effective and defective osteogenic environments. J Clin Med. 2020;9(6):1628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wei J, Chen H, Fu Y, et al. Experimental study of expression profile and specific role of human microRNAs in regulating atrophic bone nonunion. Medicine (Baltimore). 2020;99(36):e21653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wang C, Xiao F, Gan Y, et al. Improving bone regeneration using chordin siRNA delivered by pH‐responsive and non‐toxic polyspermine imidazole‐4,5‐imine. Cell Physiol Biochem. 2018;46(1):133‐147. [DOI] [PubMed] [Google Scholar]
- 11. Vallim FC, Guimarães JAM, Dias RB, et al. Atrophic nonunion stromal cells form bone and recreate the bone marrow environment in vivo. OTA International. 2018;1(3):e008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Takahara S, Niikura T, Lee SY, et al. Human pseudoarthrosis tissue contains cells with osteogenic potential. Injury. 2016;47(6):1184‐1190. [DOI] [PubMed] [Google Scholar]
- 13. Schira J, Schulte M, Dobele C, et al. Human scaphoid non‐unions exhibit increased osteoclast activity compared to adjacent cancellous bone. J Cell Mol Med. 2015;19(12):2842‐2850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Han XG, Wang DK, Gao F, et al. Bone morphogenetic protein 2 and decorin expression in old fracture fragments and surrounding tissues. Genet Mol Res. 2015;14(3):11063‐11072. [DOI] [PubMed] [Google Scholar]
- 15. Wang L, Liu T, Zhang X, et al. Expression of bone morphogenetic protein 2 in human nonunion tissue and the clinical significance. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2014;39(10):1023‐1028. [DOI] [PubMed] [Google Scholar]
- 16. Schwabe P, Simon P, Kronbach Z, et al. A pilot study investigating the histology and growth factor content of human non‐union tissue. Int Orthop. 2014;38(12):2623‐2629. [DOI] [PubMed] [Google Scholar]
- 17. Ismail HD, Phedy P, Kholinne E, et al. Existence of mesenchymal stem cellsin sites of atrophic nonunion. Bone Joint Res. 2013;2(6):112‐115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Burska AN, Giannoudis PV, Tan BH, et al. Dynamics of early signalling events during fracture healing and potential serum biomarkers of fracture non‐union in humans. J Clin Med. 2020;9(2):492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. El‐Jawhari JJ, Kleftouris G, El‐Sherbiny Y, et al. Defective proliferation and osteogenic potential with altered immunoregulatory phenotype of native bone marrow‐multipotential stromal cells in atrophic fracture non‐union. Sci Rep. 2019;9(1):17340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Ouyang Z, Tan T, Zhang X, et al. CircRNA hsa_circ_0074834 promotes the osteogenesis‐angiogenesis coupling process in bone mesenchymal stem cells (BMSCs) by acting as a ceRNA for miR‐942‐5p. Cell Death Dis. 2019;10(12):932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. McCoy TH Jr, Fragomen AT, Hart KL, et al. Genomewide association study of fracture nonunion using electronic health records. JBMR plus. 2019;3(1):23‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Zhang W, Duan N, Zhang Q, et al. The intracellular NADH level regulates atrophic nonunion pathogenesis through the CtBP2‐p300‐Runx2 transcriptional complex. Int J Biol Sci. 2018;14(14):2023‐2036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Huang W, Zhang K, Zhu Y, et al. Genetic polymorphisms of NOS2 and predisposition to fracture non‐union: A case control study based on Han Chinese population. PLoS One. 2018;13(3):e0193673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Granchi D, Gomez‐Barrena E, Rojewski M, et al. Changes of bone turnover markers in long bone nonunions treated with a regenerative approach. Stem Cells Int. 2017;2017:3674045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Sathyendra V, Donahue HJ, Vrana KE, et al. Single nucleotide polymorphisms in osteogenic genes in atrophic delayed fracture‐healing: a preliminary investigation. J Bone Joint Surg Am. 2014;96(15):1242‐1248. [DOI] [PubMed] [Google Scholar]
- 26. Marchelli D, Piodi LP, Corradini C, et al. Increased serum OPG in atrophic nonunion shaft fractures. J Orthop Traumatol. 2009;10(2):55‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Zeckey C, Hildebrand F, Glaubitz LM, et al. Are polymorphisms of molecules involved in bone healing correlated to aseptic femoral and tibial shaft non‐unions? J Orthop Res. 2011;29(11):1724‐1731. [DOI] [PubMed] [Google Scholar]
- 28. Dimitriou R, Carr IM, West RM, et al. Genetic predisposition to fracture non‐union: a case control study of a preliminary single nucleotide polymorphisms analysis of the BMP pathway. BMC Musculoskelet Disord. 2011;12:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Xiong DH, Liu XG, Guo YF, et al. Genome‐wide association and follow‐up replication studies identified ADAMTS18 and TGFBR3 as bone mass candidate genes in different ethnic groups. Am J Hum Genet. 2009;84(3):388‐398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Seebach C, Henrich D, Tewksbury R, et al. Number and proliferative capacity of human mesenchymal stem cells are modulated positively in multiple trauma patients and negatively in atrophic nonunions. Calcif Tissue Int. 2007;80(4):294‐300. [DOI] [PubMed] [Google Scholar]
- 31. Henle P, Zimmermann G, Weiss S. Matrix metalloproteinases and failed fracture healing. Bone. 2005;37(6):791‐798. [DOI] [PubMed] [Google Scholar]
- 32. Guerkov HH, Lohmann CH, Liu Y, et al. Pulsed electromagnetic fields increase growth factor release by nonunion cells. Clin Orthop Relat Res. 2001;384:265‐279. [DOI] [PubMed] [Google Scholar]
- 33. Bajada S, Marshall MJ, Wright KT, et al. Decreased osteogenesis, increased cell senescence and elevated Dickkopf‐1 secretion in human fracture non union stromal cells. Bone. 2009;45(4):726‐735. [DOI] [PubMed] [Google Scholar]
- 34. Reed AA, Joyner CJ, Brownlow HC, et al. Human atrophic fracture non‐unions are not avascular. J Orthop Res. 2002;20(3):593‐599. [DOI] [PubMed] [Google Scholar]
- 35. Kilian O, Dahse R, Alt V, et al. Expression of EDA+ and EDB+ fibronectin splice variants in bone. Bone. 2004;35(6):1334‐1345. [DOI] [PubMed] [Google Scholar]
- 36. Iwakura T, Miwa M, Sakai Y, et al. Human hypertrophic nonunion tissue contains mesenchymal progenitor cells with multilineage capacity in vitro. J Orthop Res. 2009;27(2):208‐215. [DOI] [PubMed] [Google Scholar]
- 37. Hofmann A, Ritz U, Hessmann MH, et al. Cell viability, osteoblast differentiation, and gene expression are altered in human osteoblasts from hypertrophic fracture non‐unions. Bone. 2008;42(5):894‐906. [DOI] [PubMed] [Google Scholar]
- 38. Fajardo M, Liu CJ, Ilalov K, et al. Matrix metalloproteinases that associate with and cleave bone morphogenetic protein‐2 in vitro are elevated in hypertrophic fracture nonunion tissue. J Orthop Trauma. 2010;24(9):557‐563. [DOI] [PubMed] [Google Scholar]
- 39. Fajardo M, Liu CJ, Egol K. Levels of expression for BMP‐7 and several BMP antagonists may play an integral role in a fracture nonunion: a pilot study. Clin Orthop Relat Res. 2009;467(12):3071‐3078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Mills LA, Simpson AH. The relative incidence of fracture non‐union in the Scottish population (5.17 million): a 5‐year epidemiological study. BMJ Open. 2013;3(2):e002276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Fernandez‐Bances I, Perez‐Basterrechea M, Perez‐Lopez S, et al. Repair of long‐bone pseudoarthrosis with autologous bone marrow mononuclear cells combined with allogenic bone graft. Cytotherapy. 2013;15(5):571‐577. [DOI] [PubMed] [Google Scholar]
- 42. Urist MR, Mazet R Jr, Mc LF. The pathogenesis and treatment of delayed union and non‐union; a survey of eighty‐five ununited fractures of the shaft of the tibia and one hundred control cases with similar injuries. J Bone Joint Surg Am. 1954;36‐A(5):931‐980; passim. [PubMed] [Google Scholar]
- 43. Calori GM, Colombo M, Mazza E, et al. Monotherapy vs. polytherapy in the treatment of forearm non‐unions and bone defects. Injury. 2013;44(Suppl 1):S63‐S69. [DOI] [PubMed] [Google Scholar]
- 44. Milgram JW. Nonunion and pseudarthrosis of fracture healing. A histopathologic study of 95 human specimens. Clin Orthop Relat Res. 1991;268:203‐213. [PubMed] [Google Scholar]
- 45. Quacci D, Dell'Orbo C, Salvi M, et al. Ultrastructural aspects of human nonunion. Histol Histopathol. 1991;6(1):87‐93. [PubMed] [Google Scholar]
- 46. Bajada S, Harrison PE, Ashton BA, et al. Successful treatment of refractory tibial nonunion using calcium sulphate and bone marrow stromal cell implantation. J Bone Joint Surg Br. 2007;89(10):1382‐1386. [DOI] [PubMed] [Google Scholar]
- 47. Pneumaticos SG, Panteli M, Triantafyllopoulos GK, et al. Management and outcome of diaphyseal aseptic non‐unions of the lower limb: A systematic review. Surgeon. 2013;12(3):166‐175. [DOI] [PubMed] [Google Scholar]
- 48. Paley D, Catagni MA, Argnani F, et al. Ilizarov treatment of tibial nonunions with bone loss. Clin Orthop Relat Res. 1989;241:146‐165. [PubMed] [Google Scholar]
- 49. Kloen P, Doty SB, Gordon E, et al. Expression and activation of the BMP‐signaling components in human fracture nonunions. J Bone Joint Surg Am. 2002;84‐A(11):1909‐1918. [DOI] [PubMed] [Google Scholar]
- 50. Koga T, Lee SY, Niikura T, et al. Effect of low‐intensity pulsed ultrasound on bone morphogenetic protein 7‐induced osteogenic differentiation of human nonunion tissue‐derived cells in vitro. J Ultrasound Med. 2013;32(6):915‐922. [DOI] [PubMed] [Google Scholar]
- 51. Behrens A, van Deursen JM, Rudolph KL, et al. Impact of genomic damage and ageing on stem cell function. Nat Cell Biol. 2014;16(3):201‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Einhorn TA. The science of fracture healing. J Orthop Trauma. 2005;19(10 Suppl):S4‐6. [DOI] [PubMed] [Google Scholar]
- 53. Phillips AM. Overview of the fracture healing cascade. Injury. 2005;36(Suppl 3):S5‐7. [DOI] [PubMed] [Google Scholar]
- 54. Boyan BD, Schwartz Z, Swain LD, et al. Initial effects of partially purified bone morphogenetic protein on the expression of glycosaminoglycan, collagen, and alkaline phosphatase in nonunion cell cultures. Clin Orthop Relat Res. 1992;278:286‐304. [PubMed] [Google Scholar]
- 55. Qu G, von Schroeder HP. The osteogenic potential of pseudoarthrosis tissue and bone from human scaphoid non‐unions. J Hand Surg Eur. 2008;33(4):449‐456. [DOI] [PubMed] [Google Scholar]
- 56. Kwong FN, Hoyland JA, Freemont AJ, et al. Altered relative expression of BMPs and BMP inhibitors in cartilaginous areas of human fractures progressing towards nonunion. J Orthop Res. 2009;27(6):752‐757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Chen Y, Whetstone HC, Lin AC, et al. Beta‐catenin signaling plays a disparate role in different phases of fracture repair: implications for therapy to improve bone healing. PLoS Med. 2007;4(7):e249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Viswanathan S, Shi Y, Galipeau J, et al. Mesenchymal stem versus stromal cells: International Society for Cell & Gene Therapy (ISCT(R)) Mesenchymal Stromal Cell committee position statement on nomenclature. Cytotherapy. 2019;21(10):1019‐1024. [DOI] [PubMed] [Google Scholar]
- 59. Giannoudis PV, Panteli M, Calori GM. Bone Healing: The Diamond Concept. In: Bentley G, ed. European Instructional Lectures (Vol. 14, pp. 3‐16): Springer Berlin Heidelberg; 2014. [Google Scholar]
- 60. Pountos I, Georgouli T, Kontakis G, et al. Efficacy of minimally invasive techniques for enhancement of fracture healing: evidence today. Int Orthop. 2010;34(1):3‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Vun J, Panteli M, Jones E, et al. The in vitro effects of platelet products on the biophysiological functions of human bone marrow mesenchymal stromal cells: a systematic review. Eur Cell Mater. 2021;41:269‐315. [DOI] [PubMed] [Google Scholar]