

Abstract
Background
Current treatments for amblyopia, typically patching or pharmacological blurring, have limited success. Less than two‐thirds of children achieve good acuity of 0.20 logMAR in the amblyopic eye, with limited improvement of stereopsis, and poor adherence to treatment. A new approach, based on presentation of movies or computer games separately to each eye, may yield better results and improve adherence. These treatments aim to balance the input of visual information from each eye to the brain.
Objectives
To determine whether binocular treatments in children, aged three to eight years, with unilateral amblyopia result in better visual outcomes than conventional patching or pharmacological blurring treatment.
Search methods
We searched CENTRAL (which contains the Cochrane Eyes and Vision Trials Register), MEDLINE, Embase, ISRCTN, ClinicalTrials.gov, and the WHO ICTRP to 19 November 2020, with no language restrictions.
Selection criteria
Two review authors independently screened the results of the search for relevant studies. We included randomised controlled trials (RCTs) that enrolled children between the ages of three and eight years old with unilateral amblyopia. Amblyopia was classed as present when the best‐corrected visual acuity (BCVA) was worse than 0.200 logMAR in the amblyopic eye, with BCVA 0.200 logMAR or better in the fellow eye, in the presence of an amblyogenic risk factor, such as anisometropia, strabismus, or both. To be eligible, children needed to have undergone cycloplegic refraction and ophthalmic examination, including fundal examination and optical treatment, if indicated, with stable BCVA in the amblyopic eye despite good adherence with wearing glasses. We included any type of binocular viewing intervention, on any device (e.g. computer monitors viewed with liquid‐crystal display shutter glasses; hand‐held screens, including mobile phones with lenticular prism overlay; or virtual reality displays). Control groups received standard amblyopia treatment, which could include patching or pharmacological blurring of the better‐seeing eye. We included full‐time (all waking hours) and part‐time (between 1 and 12 hours a day) patching regimens.
We excluded children who had received any treatment other than optical treatment; and studies with less than 8‐week follow‐up.
Data collection and analysis
We used standard methodological procedures expected by Cochrane. The primary outcome of the review was the change from baseline of distance BCVA in the amblyopic eye after 16 (± 2) weeks of treatment, measured in logMAR units on an age‐appropriate acuity test.
Main results
We identified one eligible RCT of conventional patching treatment versus novel binocular treatment, and analysed a subset of 68 children who fulfilled the age criterion of this review. We obtained data for the mean change in amblyopic eye visual acuity, adverse events (diplopia), and adherence to prescribed treatment at 8‐ and 16‐week follow‐up intervals, though no data were available for change in BCVA after 52 weeks. Risk of bias for the included study was considered to be low.
The certainty of evidence for the visual acuity outcomes at 8 and 16 weeks of treatment and adherence to the study intervention was rated moderate using the GRADE criteria, downgrading by one level due to imprecision. The certainty of evidence was downgraded by two levels and rated low for the proportion of participants reporting adverse events due to the sample size.
Acuity improved in the amblyopic eye in both the binocular and patching groups following 16 weeks of treatment (improvement of ‐0.21 logMAR in the binocular group and ‐0.24 logMAR in the patching group), mean difference (MD) 0.03 logMAR (95% confidence interval (CI) ‐0.10 to 0.04; 63 children). This difference was non‐significant and the improvements in both the binocular and patching groups are also considered clinically similar.
Following 8 weeks of treatment, acuity improved in both the binocular and patching groups (improvement of ‐0.18 logMAR in the patching group compared to ‐0.16 logMAR improvement in the binocular‐treatment group) (MD 0.02, 95% CI ‐0.04 to 0.08). Again this difference was statistically non‐significant, and the differences observed between the patching and binocular groups are also clinically non‐significant. No adverse event of permanent diplopia was reported.
Adherence was higher in the patching group (47% of participants in the iPad group achieved over 75% compliance compared with 90% of the patching group).
Data were not available for changes in stereopsis nor for contrast sensitivity following treatment.
Authors' conclusions
Currently, there is only one RCT that offers evidence of the safety and effectiveness of binocular treatment.
The authors are moderately confident that after 16 weeks of treatment, the gain in amblyopic eye acuity with binocular treatment is likely comparable to that of conventional patching treatment. However, due to the limited sample size and lack of long term (52 week) follow‐up data, it is not yet possible to draw robust conclusions regarding the overall safety and sustained effectiveness of binocular treatment.
Further research, using acknowledged methods of visual acuity and stereoacuity assessment with known reproducibility, is required to inform decisions about the implementation of binocular treatments for amblyopia in clinical practice, and should incorporate longer term follow‐up to establish the effectiveness of binocular treatment. Randomised controlled trials should also include outcomes reported by users, adherence to prescribed treatment, and recurrence of amblyopia after cessation of treatment.
Plain language summary
Treatments to stimulate eye co‐operation versus standard patching or blurring treatment for amblyopia (lazy eye) in children aged three to eight years
Review question Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years.
Background At present, amblyopia (lazy eye) in children is treated with glasses, followed by either patching or blurring of the better‐seeing eye with atropine eyedrops. These treatments are not popular with children, and the amount of patching or eye drops that parents and carers can apply is often less than what was prescribed. Less than two‐thirds of children develop normal vision in the lazy eye, and three‐dimensional vision may remain limited in some cases. A new type of binocular treatment (with both eyes open) that matches the visual information shown to the better eye to the level of vision in the lazy eye may yield better results. Children may find this approach easier to tolerate, as during treatment they play computer games or watch movies through special lenses or on modified computers.
What did we want to find out? We wanted to find out if binocular treatments were better than conventional patching or pharmacological blurring treatment in getting better visual outcomes in children, aged three to eight years, with unilateral amblyopia.
What did we do? We searched for studies that examined this new treatment, compared with standard patching or eye‐drop blurring treatment, in children aged three to eight years with lazy eye. We searched all standard sources of information. Two review authors independently reviewed the results of this search. We planned to include only studies reporting results from randomised controlled trials (RCTs) ‐ studies comparing the new treatment with a standard treatment, and where children were assigned treatment groups at random (like flipping a coin).
What did we find? We identified one RCT that met these criteria. The study recruited 385 children of which a subset were analysed; 36 were randomised to a binocular iPad game and 32 children were randomised to conventional patching treatment. The study found, on average that vision improves with both patching and the new computer treatment after 16 weeks, with little‐to‐no difference in the amount of improvement with either approach, though there were some limitations with the study.
We conclude that more research is needed to allow decisions about the new treatment. We recommend that future research be done in the form of RCTs, and that researchers use acknowledged tests of visual acuity (fine detail) and three‐dimensional vision to report the results. It will also be important to publish observations reported by children and families, how much the treatment was used, and if and when the vision in the lazy eye got worse after the treatment was stopped.
How up to date is this evidence? This review updates our previous review. The evidence is up to date to November 2020.
Summary of findings
Summary of findings 1. Binocular iPad treatment compared with occlusion therapy for amblyopia.
| Binocular iPad treatment compared with occlusion therapy for amblyopia | ||||||
|
Patient or population: 5‐ to 8‐year‐old children with amblyopia Settings: clinical Intervention: binocular iPad treatment Comparison: occlusion therapy | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk with occlusion therapy | Corresponding risk with binocular iPad treatment | |||||
|
Change in BCVA amblyopic eye after 16 weeks logMAR (lower logMAR values indicate better visual acuity) |
Mean change in acuity for the occlusion group was an improvement of 0.24 logMAR | Mean change in acuity for the binocular iPad groups was 0.03 logMAR higher (worse)(‐0.04 to 0.10) | 63 (1 study) | ⊕⊕⊕⊝
moderatea |
||
|
Change in BCVA amblyopic eye after 8 weeks logMAR (lower logMAR values indicate better visual acuity) |
Mean change in acuity for the occlusion group was an improvement of 0.18 logMAR | Mean change in acuity for the binocular iPad groups was 0.02 logMAR higher (worse)(‐0.04 to 0.08) |
62 (1 study) | ⊕⊕⊕⊝ moderatea | ||
|
Change in distance BCVA in the amblyopic eye 12 months after cessation of treatment |
– | – | – | – | – | No data recorded for this outcome |
|
Adherence to intervention Proportion of adherence to prescribed intervention across predefined categories |
Subjective recording of adherence to treatment: 90.3% of participants achieved over 75% compliance. | Subjective recording of treatment adherence: 46.9% of participants achieved over 75% compliance. | N/A | 63 (1 study) |
⊕⊕⊕⊝
moderatea |
|
|
Proportion of participants experiencing an adverse event of permanent diplopia (double vision) Reports of diplopia across all measured time points |
No reports of permanent diplopia. |
63 (1 study) | ⊕⊕⊝⊝
lowb |
|||
|
Change in the interocular difference in contrast sensitivity Any validated test, from baseline to 16 (± 2) weeks |
– | – | – | – | – | No data recorded for this outcome |
|
Measurable change in stereopsis after 8 (± 2) weeks and 16 (± 2) weeks of intervention 'Real change' in stereopsis is defined as a change in stereoacuity of two or more octaves. |
– | – | – | – | – | No data recorded for this outcome |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BCVA: best‐corrected visual acuity;CI: Confidence interval; RR: Risk Ratio | ||||||
| GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate‐certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low‐certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect Very low‐certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded one level due to imprecision bDowngraded two levels due to sample size
Background
Description of the condition
Unilateral amblyopia is a developmental disorder of vision. With 2% to 5% prevalence, it is the most common cause of reduced vision in one eye in children in the UK (Carlton 2008; daCunha 1961; McNeil 1955; Powell 2009; Rahi 2006), and the second most common cause of functional low vision for children in low‐income countries (Gilbert 2008). The most common risk factors for the development of amblyopia are anisometropia (a difference in refraction or glasses prescription between the two eyes) and strabismus (misalignment of the visual axes (Barrett 2004; McKee 2003)); rarely, congenital or early childhood cataracts, or other opacities of the ocular media can give rise to amblyopia by deprivation.
The imbalance of input to the brain from the two eyes results in a range of amblyopic deficits in vision and gaze stability. This includes the definitive reduction in acuity or resolution, as well as abnormal binocular function (Levi 1985; McKee 2003), with suppression of information from the amblyopic eye and poor stereopsis (three‐dimensional vision (Birch 2013; Greenwood 2012; Hess 2014; McKee 2003)). This reduction in stereopsis can be associated with reduced motor skills, both in children and adults (Grant 2007; Grant 2011; Hrisos 2006; Niechwiej‐Szwedo 2011; O'Connor 2010; Webber 2008a). The precise cause of amblyopia further influences the pattern of visual deficits; anisometropic amblyopia produces additional reductions in contrast sensitivity (McKee 2003), while strabismic amblyopia yields a range of spatial disruptions, including vulnerability to crowding (the disruptive influence of clutter on recognition) in the central visual field (Greenwood 2012; Levi 1985; Levi 2008; Song 2014), perceptual distortions (Barrett 2003; Mirabella 2011), and deficits in positional acuity (the ability to localise the relative position of an object in space (Levi 1986; Neri 2006)). Higher‐order deficits in global‐motion processing (Husk 2012; Simmers 2003), and spatial attention (the ability to direct visual attention to certain locations in the visual field) have also been reported (Ho 2006; Sharma 2000).
If amblyopia persists into adulthood, affected individuals may be unable to take up professions that require depth perception, such as piloting aeroplanes. Accidents affecting the better‐seeing eye can lead to a severe loss of quality of life and independence (Rahi 2002). Children treated for amblyopia have lower social acceptance scores than their peers (Birch 2019; Webber 2008b). Low self esteem and negative self image as a result of amblyopia and its treatment are common, as are feelings of depression, frustration, and embarrassment (Dixon‐Woods 2006; Sinha 2008).
The distinct pattern of deficits in anisometropic and strabismic amblyopia are likely to be associated with specific alterations to the visual system (Birch 2000; Levi 1982; Levi 1985). Anisometropia causes blurred vision in one eye, and defocused input to the visual cortex, leading to selective loss of neurons tuned to high spatial frequencies (i.e. high resolution input (Kiorpes 1998; Kiorpes 1999)). On the other hand, in strabismus, the focus of retinal images is clear, but misalignment of the visual axes disrupts the input to binocular cortical neurons, leading to fixation preference for one eye, and subsequent visual deficits in the other eye (Birch 2013; Kiorpes 1998; Kiorpes 1999).
The cortical changes associated with amblyopia are not fully understood, however. Best characterised are the disruptions of neural activity in the primary visual cortex (V1) in the occipital lobe (Sengpiel 2006; Victor 1994; Vorobyov 2013; Wiesel 1963). The imbalance of visual inputs appears to induce a reallocation of V1 neurons; those receiving input from the amblyopic eye shift their responsiveness to the better‐seeing eye (Kiorpes 1998; Kiorpes 1999; Li 2007; Sengpiel 2011; Vorobyov 2013; Wiesel 1963). In strabismus, although V1 neurons receive input from both eyes, the number of V1 neurons responding to stimuli from both eyes is reduced, as binocular neurons in V1 only mature when receiving matching input from both eyes (Mitchell 2009). However, these disruptions to V1 function are probably insufficient to account for the extent of visual deficits in amblyopia (Kiorpes 1999). Indeed, processing in extrastriate areas is also altered (Barnes 2001; Clavagnier 2015; Conner 2007; Zhang 2011), which may account for the deficits in crowding (Anderson 2012), positional acuity (Maus 2010), and spatial attention (Corbetta 1995). Both ventral (object recognition) and dorsal (motion processing and action) pathways may be affected (Goodale 1992), perhaps differentially for early‐ versus late‐onset amblyopia (Davis 2006).
The development of the functional architecture, or maps of the visual cortex, occurs in stages (Espinosa 2012; White 2007). The phase of maturation of the functional maps of the visual cortex is called the 'critical period', because imbalance or disruption in the form of visual deprivation causes dramatic changes to the strength and organisation of the functional maps (Espinosa 2012). Different aspects of visual processing have slightly different critical periods, though they may overlap (Daw 1998; Harwerth 1986; White 2007). Thus, for area V1, the selective characteristics of these neurons are thought to be refined and matched to the input from both eyes at an earlier stage than those of extrastriate areas. Nonetheless, imbalance of visual input could affect the maturation of the functional maps in a range of cortical areas.
For a long time, it was held that the critical period for amblyopia treatment was identical to that of visual development, and that after the end of the critical period, amblyopia could not be induced, nor could established amblyopia be reversed (Assaf 1982; Wiesel 1963). However, newer observations have challenged the concept of a complete loss of plasticity in the visual processing areas of the brain, even in adulthood, though the quality of plasticity in adulthood may differ from that in childhood (Sato 2008). Reports indicate that suppression can be reversed, and vision successfully improved, even after the end of the conventional critical period (Evans 2011; Levi 2005; Levi 2009), though early intervention may still deliver better visual outcomes (Eibschitz‐Tsimhoni 2000; Holmes 2011).
Description of the intervention
In the UK, amblyopia is treated by first correcting any refractive error with glasses (optical treatment, refractive adaptation). Improvement in vision is typically greatest in the first few weeks of wearing glasses, but can continue for up to four months and beyond (Cotter 2006; Cotter 2007; Stewart 2004b; Taylor 2014; Wallace 2006). If amblyopia persists, current treatment consists of patching the better‐seeing eye for two or six hours a day, depending on the severity of the amblyopia (Awan 2005; Holmes 2003; Loudon 2006; Repka 2003; Stewart 2004a; Stewart 2004b; Stewart 2005; Taylor 2014). Successful patching treatment is associated with an improvement of visual acuity and stereopsis, both statistically, and in clinical terms (Stewart 2013; Wallace 2011). Pharmacological blurring of the better‐seeing eye, using atropine eye drops, appears to be equivalent to patching treatment in improving visual acuity (Li 2009; PEDIG 2002; Repka 2009; Scheiman 2008). Although the sequential approach to amblyopia treatment (optical treatment followed by patching) is a clinical standard, it is yet to be supported by empirical evidence. A recent clinical trial has examined whether the sequential approach can improve the number of successfully treated children with amblyopia, though published data is not yet available (ISRCTN51712593).
The main drawbacks of patching and pharmacological blurring are poor adherence to treatment, and suboptimal treatment outcomes. Lack of adherence to patching treatment is common. Patching the better‐seeing eye functionally incapacitates the child, and children often attempt to remove the patch. Figures reported for adherence range from 41% to 57% (Awan 2005; Loudon 2006), with adherence decreasing with both an increase in severity of amblyopia, and an increase in the prescribed daily dose of patching (Awan 2005; Loudon 2006; Moseley 1995; Stewart 2002). A questionnaire tool has been developed to measure the burden of treatment to the child and the family (Felius 2010; Holmes 2008). Whether poor parent knowledge of the condition contributes to poor adherence to treatment is controversial, though educational interventions may be beneficial (Dixon‐Woods 2006; Loudon 2006).
Even with the best current treatment, only a fraction of children achieve near‐normal visual acuity in the amblyopic eye. Using best‐corrected visual acuity (BCVA) after optical treatment as the baseline, around 25% of eyes with severe amblyopia and 58% of eyes with moderate amblyopia improve to a level of 0.20 logMAR or better with patching treatment (Holmes 2003; Repka 2003). After treatment is discontinued, visual acuity typically regresses (Hertle 2007; Holmes 2004), and a low‐dose maintenance treatment is often used to wean children off treatment. Nevertheless, two years after stopping treatment, BCVA in the amblyopic eye can still be 2 lines worse than in the better‐seeing eye (Repka 2005). Regression to pre‐treatment BCVA may occur in 30% of cases (Malik 1975). This leaves a significant proportion of children at risk of severe functional impairment and loss of quality of life, should they lose vision in the better‐seeing eye at any stage during their life. In addition, stereoacuity (three‐dimensional vision) improves in less than half of children (Stewart 2013).
In order to develop treatments that, at the same time, appeal more to children and improve not only visual acuity in the amblyopic eye but also promote binocularity (where both eyes work together as a pair), several groups have designed methods of simultaneous binocular visual stimulation, i.e. binocular treatment for amblyopia. To date, four systems have been developed.
1. Anti‐suppression therapy
Anti‐suppression therapy presents the visual scene with reduced contrast to the better‐seeing eye and normal contrast to the amblyopic eye (Hess 2010a; Hess 2010b; Hess 2011; Hess 2012; Hess 2013). This approach aims to balance the input to visual cortex, in order to overcome interocular suppression. The difference in input to the two eyes (dichoptic presentation) can be achieved with a mirror haploscope (Hess 2010a; Hess 2010b), a head‐mounted video display (Knox 2012), lenticular prism overlays on tablet computers or screens of other hand‐held devices (To 2011), or red/green anaglyph glasses (Birch 2020; Gao 2018; Li 2014). The observer then has to carry out a task that requires the combination of the information from the two eyes. With improving performance, the contrast of the visual scene shown to the better‐seeing eye is gradually increased, until contrast is equal for both eyes. A popular task is the Tetris game, in which a series of falling blocks have to be combined to form complete lines (Black 2011); other games include DigRush, where children manipulate miners digging for gold (Kelly 2016). In each case, game elements are divided between the two eyes. The training dose for these treatments may be up to two hours a day. Improvement of visual acuity and binocular vision can occur within weeks of training in adults (Hess 2010a; Hess 2012; To 2011), and children (Kelly 2016; Knox 2012).
2. Balanced binocular viewing
Balanced binocular viewing (BBV) uses dichoptically presented movies, such that each eye receives an altered version of the same image, with the goal to balance input to the visual cortex (Bossi 2014; Bossi 2017). Children watch movies at home for an hour on a desktop computer, while wearing LCD shutter glasses. Visibility of the content across the two eyes is balanced by applying Gaussian blur to the image seen by the better‐seeing eye, with the amount of blur set to reduce its resolution to that of the amblyopic eye. A simple game, interspersed with the movies, allows both compliance and the level of interocular suppression to be monitored throughout the treatment period. BBV has been further developed into a handheld device that uses a parallax barrier to separate the input to each eye without the need for shutter glasses. A phase 2a feasibility randomised controlled trial (RCT) evaluating this handheld system is currently in progress (NCT03754153).
3. I‐BiT™
The I‐BiT™ system presents different parts of a two‐dimensional visual scene to each eye via shutter glasses, combined with a task that requires the combination of the two images (Eastgate 2006; Foss 2013; Herbison 2013; Waddingham 2006). Images are viewed with both eyes, but parts of the image can only be seen with the amblyopic eye. As with the other binocular therapies, presentation of the visual scene is dichoptic rather than stereoscopic: the shutter glasses present a distinct, but visually related image to both eyes (Foss 2013). The material viewed consists of videos and interactive games aimed at children aged eight years and younger. While initially designed for hospital‐based use, the I‐BiT™ system has recently been designed for home use, achieved using a desktop computer (Brown 2019). Shutter glasses have typically been used to separate the images for each eye, though red/green anaglyph glasses have also been used with this approach (Rajavi 2019).
4. Dichoptic action video‐games
Rather than split the presented image between the two eyes, an alternative approach presents the same image to each eye at different luminance levels. This technique was initially applied to action video‐games, presented via mirror haploscope to adults (Vedamurthy 2015a; Vedamurthy 2015b). A Gabor orientation discrimination task is interspersed with gameplay to give continuous measures of resolution and interocular suppression. Binocular fusion is encouraged with nonius fixation lines (where elements of the fixation target are presented to each eye). The approach has recently been adapted with more child‐friendly video‐games, similarly presented via mirror haploscope and with intermittent resolution/suppression measurements (Gambacorta 2018).
How the intervention might work
Binocular treatments have been developed against a background of studies on the effect of perceptual learning on amblyopia (Levi 2005). A range of studies have shown that targeted practice of a specific task, such as Vernier acuity, can improve performance on that task. Although this often does not transfer to other tasks or stimulus configurations (Levi 1986), in some cases, training on one task does improve performance on others. For instance, training on tasks for contrast detection (Polat 2004), crowding (Hussain 2012), and stereopsis (Xi 2014), have all been found to produce improvements in the acuity of those with amblyopia. This pattern of transfer is somewhat complex; while training on a contrast task can transfer to acuity, acuity training does not transfer to contrast detection (Astle 2011). It is possible that by identifying and targeting the fundamental deficit in amblyopia, a range of amblyopic deficits could be improved at once.
Binocular treatments, as considered in this review, are those based on dichoptic stimulus presentation to balance the input to the visual cortex from the right and left eyes, either by reducing the contrast (anti‐suppression therapy) or luminance (dichoptic action video‐games) of the visual scene viewed with the better‐seeing eye, or by blurring it to match the perception with the amblyopic eye (balanced binocular viewing). The I‐BiT™ approach does not modify contrast or sharpness, but presents different parts of the visual scene to the amblyopic and to the better‐seeing eye, and requires the user to combine the information provided to successfully play a computer game. In other words, these systems, based on dichoptic presentation of images, specifically target binocular combination. It is known that balancing visibility in both the amblyopic and better‐seeing eye can allow both binocular summation and binocular interactions in tasks, such as motion coherence and orientation discrimination (Baker 2007; Baker 2008; Mansouri 2008). Given that the binocular imbalance is a fundamental component of amblyopia, it is possible that the specific targeting of this deficit will lead to improved outcomes for a range of amblyopic visual deficits.
The role of interocular suppression in these treatments is more controversial. Some have argued that binocular therapies (and anti‐suppression therapy in particular) operate by breaking interocular suppression, which in turn allows vision to improve (Hess 2014). Were this to be the case, any gains in acuity should follow reductions in suppression. However, though one study observed both an improvement in acuity and a reduction in suppression following dichoptic action video‐game treatment, the two were not correlated (Vedamurthy 2015a). Balanced binocular viewing has further been found to produce improvements in acuity without a measurable change in suppression (Bossi 2017). Therefore, although suppression may play a causal role in the development of amblyopic deficits, it seems that the mechanism underlying these deficits in acuity and stereovision can be altered by binocular therapies without changes in suppression (Li 2011). Instead, improvements in binocular combination could be driven by increases in the number of neurons driven by the amblyopic eye (Kiorpes 1998), a decrease in the positional disorganisation of their receptive fields (Hess 1994), alterations of their spatial properties, or a combination (Clavagnier 2015).
Why it is important to do this review
Binocular treatments aim to address the causal mechanisms underlying amblyopia, and may deliver better outcomes than current standard treatments. In addition, these new treatment modalities are more child‐friendly than conventional treatment. With home‐based treatments becoming available, these treatments may soon enter regular clinical use. A robust framework is required to facilitate the evaluation of RCT results and provide evidence on the benefits and harms of these treatments.
Objectives
To determine whether binocular treatments in children, aged three to eight years, with unilateral amblyopia result in better visual outcomes than conventional patching or pharmacological blurring treatment.
Methods
Criteria for considering studies for this review
Types of studies
We only included randomised controlled trials (RCT) in this review. To ensure that these RCTs had allowed for sufficient time to adequately identify the change in best‐corrected visual acuity (BCVA) in either treatment arm, we only included RCTs with a minimum of 8 (± 2)‐week follow‐up intervals.
Types of participants
We included participants between the ages of three and eight years old with unilateral amblyopia, defined as BCVA worse than 0.200 logMAR in the amblyopic eye, and BCVA 0.200 logMAR or better in the fellow eye, in the presence of an amblyogenic risk factor, such as anisometropia, strabismus, or both. In practice, an interocular difference in visual acuity of 0.200 logMAR or greater is usually required for a diagnosis of amblyopia.
Prior to enrolment, participants would have undergone a cycloplegic refraction and comprehensive ophthalmic examination, including fundal examination. In addition, participants would have completed a period of optical treatment, and BCVA in the amblyopic eye would have been considered stable, despite reportedly good adherence with wearing glasses. To avoid any potential confounding factors due to the inclusion of pretreated amblyopes (e.g. improvement of BCVA to their previous best‐corrected level, rather than new improvement following binocular treatment), participants included in this review would not have received any treatment other than optical treatment prior to enrolment.
Types of interventions
We included any type of binocular viewing intervention; these could have been delivered on different devices, including computer monitors viewed with LCD shutter glasses; hand‐held screens, including mobile phone screens with lenticular prism overlay; or virtual reality displays.
Control groups received standard amblyopia treatment; this could have included patching or pharmacological blurring of the better‐seeing eye. We planned to include full‐time (all waking hours) and part‐time (between 1 and 12 hours a day) patching regimens.
Types of outcome measures
Primary outcomes
Change in distance best‐corrected visual acuity (BCVA) in the amblyopic eye from baseline to 16 (± 2) weeks of treatment, measured in logMAR units on an age‐appropriate acuity test. Lower logMAR values indicate better visual acuity, but as we examined change in BCVA, a higher logMAR difference indicates higher levels of improvement in BCVA following treatment (either conventional or binocular).
Secondary outcomes
Main secondary outcome: change in BCVA in the amblyopic eye from baseline to 8 (± 2) weeks of treatment, measured in logMAR units on an age‐appropriate acuity test.
Change in stereopsis from baseline to 8 (± 2) and 16 (± 2) weeks of intervention. 'Real change' in stereopsis was defined as a change in stereoacuity of two or more octaves (Adams 2009).
Change in distance BCVA in the amblyopic eye, measured 12 months after cessation of treatment.
Adherence to interventions, measured by usage time as a proportion of prescribed time, following 8 (± 2) and 16 (± 2) weeks of treatment.
Change in the interocular difference in contrast sensitivity from baseline to 16 (± 2) weeks, using any validated test.
Proportion of participants experiencing adverse events, such as permanent diplopia (double vision), at any time point.
Search methods for identification of studies
Electronic searches
The Cochrane Eyes and Vision Information Specialist conducted systematic searches in the following databases for randomised controlled trials and controlled clinical trials. There were no restrictions to language or year of publication.
Cochrane Central Register of Controlled Trials, which contains the Cochrane Eyes and Vision Trials Register (CENTRAL; 2020, Issue 11) in the Cochrane Library (searched 19 November 2020; Appendix 1);
MEDLINE Ovid (1946 to 19 November 2020; Appendix 2);
Embase Ovid (1980 to 19 November 2020; Appendix 3);
International Standard Randomised Controlled Trial Number (ISRCTN) registry (www.isrctn.com/editAdvancedSearch; searched 19 November 2020; Appendix 4);
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 19 November 2020; Appendix 5);
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP; www.who.int/ictrp; searched 19 November 2020; Appendix 6).
Searching other resources
We manually searched the reference lists of the included trials for additional trials. We also used the Science Citation Index to identify reports that had cited the studies included in this review. With both of these strategies, we aimed to identify any relevant reports or trials that we had not identified by the electronic searches. We did not specifically handsearch journals or conference proceedings for this review.
Data collection and analysis
We planned to follow the guidelines in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions for data analysis (Deeks 2017). We planned to meta‐analyse the primary outcome, mean distance BCVA in the amblyopic eye after 16 (± 2) weeks of treatment. LogMAR acuities are normally distributed, and provided we did not detect heterogeneity, we planned to meta‐analyse data using the random‐effects model, with the mean difference as our treatment effect measure. With fewer than three studies, we planned to use a fixed‐effect model.
Selection of studies
Two review authors (VT and SL) independently screened the results of the search (titles and abstracts) to identify studies that loosely met the inclusion criteria of the review (Figure 1). Review authors were not masked to study authors, institution, or journal. We divided studies into 'definitely include', 'definitely exclude', and 'possibly include'. We made final judgements on inclusion or exclusion by obtaining the full‐text copy of those studies in the 'definitely include' and 'possibly include' category. We had abstracts, and where necessary, full‐text articles translated into English before making a final decision regarding inclusion or exclusion. We took care to identify multiple reports of the same study, and when identified, we planned to link them. The review authors independently examined full‐text reports for compliance with inclusion criteria. We resolved any disagreements by discussion with the third review author (ADN). We listed studies that we excluded after obtaining the full‐text in Characteristics of excluded studies, giving a reason for exclusion.
1.
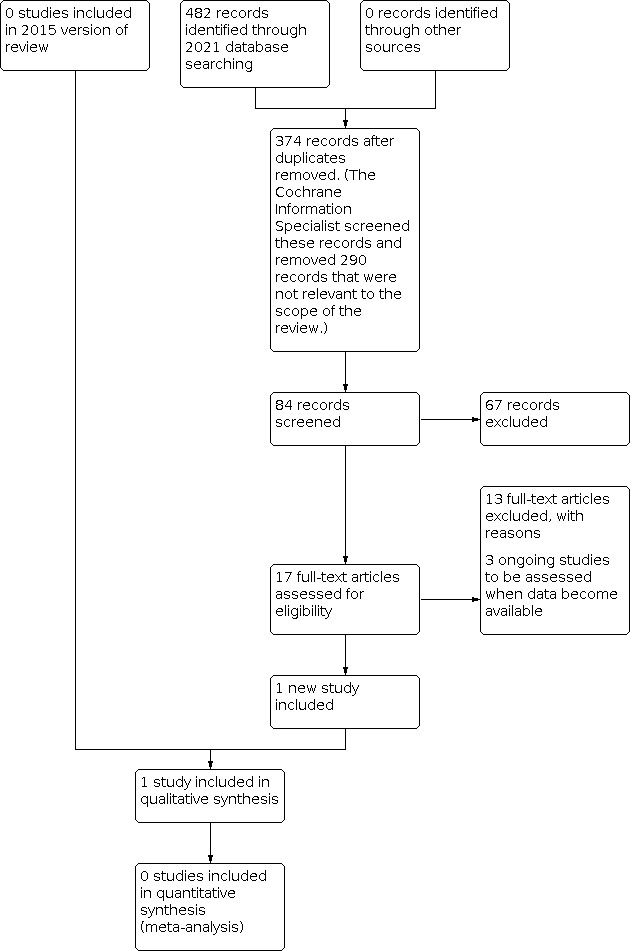
PRISMA flowchart for study selection (2015 and 2021 literature searches)
Data extraction and management
Two review authors (VT and SL) independently extracted data, using a data extraction form developed in conjunction with Cochrane Eyes and Vision, using guidance from Chapter 7 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011; Table 2). When data were missing or unclear, one review author (SL) attempted to contact the trial authors for unpublished data, or for clarification. We made initial contact via email, sending a second email if there was no response. We planned to enter data into Review Manager 5 (Review Manager 2020); one review author (SL) entered the data, after which a second review author (VT) checked for any errors.
1. Data extraction form.
| Review author | ||||||
| Trial registration ID | ||||||
| Dates when study was conducted | If not available, comment "dates not available" | |||||
| Funding source(s) | ||||||
| Declarations of interest by researchers | ||||||
| Methods | Study design (RCT) Interventions; mean dose prescribed and mean dose received |
|||||
| Participants | Total number, number in each group (sample size) Comparability Setting |
|||||
| Risk of bias | Assessed using risk of bias tool (see Handbook) | |||||
| Outcomes (as defined in study) Please specify which |
Primary outcome Change in distance BCVA in the amblyopic eye following 16(±2) weeks of intervention, as measured in logMAR units on an age‐appropriate acuity test. Secondary outcomes
|
|||||
| Interventions compared | Intervention 1 = standard care (occlusion or pharmacological blurring) Intervention 2 = binocular treatment |
|||||
|
PRIMARY OUTCOME Change in distance BCVA in the amblyopic eye following 16 (± 2) weeks of intervention, as measured in logMAR units on an age‐appropriate acuity test |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| Baseline (note method used to measure BCVA) | ||||||
| BCVA at 16 (± 2) | ||||||
| Or: improvement of BCVA from baseline | ||||||
|
SECONDARY OUTCOME Main secondary outcome: change in BCVA in the amblyopic eye from baseline to 8 (± 2) weeks, as measured in logMAR units on an age‐appropriate acuity test |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| Baseline (note method used to measure BCVA) | ||||||
| BCVA at 8 (± 2) | ||||||
| Or: improvement of BCVA from baseline | ||||||
|
SECONDARY OUTCOME Change in stereoacuity after 16 (± 2) weeks of intervention, measured in octaves |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| Baseline stereopsis | ||||||
| Change in stereopsis after 16 (± 2) | ||||||
| Change in stereoacuity after 8 (± 2) weeks of intervention, measured in octaves | ||||||
| Time point | ||||||
| Baseline stereopsis | ||||||
| Change in stereopsis after 8 (± 2) | ||||||
|
SECONDARY OUTCOME Adherence to intervention determined by a ratio of usage/prescribed treatment dosage |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| End of intervention (specify time from start of treatment) | ||||||
|
SECONDARY OUTCOME Change in contrast sensitivity interocular difference from baseline to 16 (± 2) weeks measured using any validated test |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| End of intervention (specify test) | ||||||
|
SECONDARY OUTCOME Adverse events (Proportion of participants experiencing an adverse event of permanent diplopia (double vision) at any time point during intervention.) |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Number of affected participants | Total number of participants | Number of affected participants | ||
| Permanent diplopia | ||||||
| Time point | ||||||
| Other (specify) | ||||||
|
SECONDARY OUTCOME Change in distance BCVA in the amblyopic eye 12 months after cessation of treatment |
Intervention 1 | Intervention 2 | ||||
| Time point | Total number of participants | Mean | Standard deviation* | Total number of participants | Mean | Standard deviation* |
| Baseline (note method used to measure BCVA) | ||||||
| 12 months after cessation of treatment | ||||||
| Or: improvement of BCVA from baseline to 12 months post‐treatment | ||||||
ATI: Amblyopia Treatment Index BCVA: best‐corrected visual acuity CAT‐QoL: Child Amblyopia Treatment Questionnaire QoL: quality of life RCT: randomised controlled trial
At a minimum, we planned to extract the following data, which we presented in the 'Characteristics of included studies' table.
Trial registration ID
Methodology: study design, interventions, intervention arms, duration of treatment
Participants: number in each group, age, gender, comparability at baseline
Outcomes: primary and secondary outcomes collected and reported; for each outcome, we recorded the unit of measurement, or if a scale was used, the upper and lower limits of the scale of measurement, and whether a high or low score was good
Results: sample size, missing participants, summary data
Miscellaneous: dates (when study was conducted), funding source, declarations of interest, whether correspondence was required, miscellaneous comments by the review authors
Assessment of risk of bias in included studies
Studies that were identified as meeting the inclusion criteria were independently reviewed by two authors (VT and SL), who assessed for risk of bias, using RoB 1, according to Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). We considered the following domains: generation of the random sequence, allocation concealment, masking (blinding) of examiners, completeness of outcome data, selective reporting, and other biases (such as any conflicts of interest or financial interests).
We graded each domain as low, high, or unclear risk of bias.
Examples of low risk of bias:
randomisation using computer‐generated sequences or random number table;
central allocation;
masking of examiners;
no missing data or missing data are balanced in numbers across intervention groups and similar reasons given across groups;
study protocol is available, with clearly specified primary and secondary outcomes.
Examples of high risk of bias:
randomisation is determined by date of visit or name (an example of quasi‐randomisation, which would make study ineligible for inclusion);
alternate allocation used (as above);
examiners are aware of the treatment allocation prior to assessing outcomes;
missing data are excluded and appear to be more common in one treatment arm than the other;
none of the study's prespecified primary outcomes are reported.
Examples of unclear risk of bias:
insufficient information in publications to allow us to make a judgement.
Measures of treatment effect
Our primary outcome was the change in BCVA in the amblyopic eye in logMAR 16 (± 2) weeks after commencing treatment. LogMAR acuities tend to be normally distributed, and we aimed to use the mean difference with 95% confidence intervals as our measure of treatment effect. However, we planned to note whether authors assessed symmetry of their data, and which logMAR test they used, as different charts may yield different values.
Our main secondary outcome was a change in BCVA in the amblyopic eye in logMAR after 8 (± 2) weeks of treatment. This is also typically normally distributed, and we aimed to use the mean difference with 95% confidence intervals.
Unit of analysis issues
Each child would have one amblyopic eye, so there would be a single observation per child. Therefore, the unit of analysis was the child.
Dealing with missing data
We planned to carry out intention‐to‐treat analysis for each outcome. One review author (SL) was to retrieve any missing data by contacting the authors of the relevant papers. If we failed to obtain this, but the review authors (SL and VT) examined reasons for loss to follow‐up adequately, and found that losses were similar between treatment groups, we may have used available case analysis. We planned to document whether the original studies stated that they compared the characteristics of participants with complete data to those without, and whether they provided any information about possible effects of missing data.
Assessment of heterogeneity
We planned to examine studies for sources of methodological and clinical heterogeneity. We intended to then assess statistical heterogeneity by:
examining the characteristics of the included studies;
looking for poor overlap of the confidence intervals on the forest plot;
carrying out a Chi² test and calculation of I² with confidence intervals. We planned to interpret values of I² as advised by Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2017). We did not plan to adopt strict thresholds for I², but would typically be concerned with values of 50% or more.
Assessment of reporting biases
If we had a sufficient number of trials (10 or more), we planned to generate a funnel plot to assess evidence of publication bias, although we acknowledge that asymmetry in such a plot does not always indicate publication bias.
Data synthesis
We planned to collate all data that were relevant to our primary and secondary outcomes.
We intended to meta‐analyse outcomes where appropriate.
We planned to use a random‐effects model, unless there was a very small number of studies (less than three), in which case we planned to use a fixed‐effect model. Had we detected substantial heterogeneity (either by methodological review of studies or by values of I² > 50%), as advised by Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2017), we planned not to conduct a meta‐analysis, unless effect estimates were in the same direction.
Subgroup analysis and investigation of heterogeneity
As we expected visual outcomes to be similar across studies, at both 8 (± 2) and 16 (± 2) week time points, we did not plan to carry out subgroup analysis or investigations of heterogeneity.
Sensitivity analysis
We planned sensitivity analysis to assess how robust our review results were, and to study the effects of:
missing data: we planned to consider whether or not data were likely to be missing completely at random, or whether there was a possibility that missingness was related to the treatment, which might bias our results;
excluding studies at high risk of bias, i.e. any study that scored high risk in any domain;
the funding source as an indicator of potential conflict of interest, such as studies that are commercially, as opposed to charity‐ or research‐council funded.
Summary of findings and assessment of the certainty of the evidence
We prepared a summary of findings table, presenting relative and absolute risks. Two review authors (VT and SL) independently graded the overall certainty of the evidence for each outcome, using the GRADE factors (study limitations, indirectness of evidence, inconsistency of results, imprecision, and publication bias) and GRADEpro GDT software (GRADEpro GDT). We included the following outcomes in the summary of findings table:
Change in distance best‐corrected visual acuity (BCVA) in the amblyopic eye from baseline to 16 (± 2) weeks of treatment
Change in BCVA in the amblyopic eye from baseline to 8 (± 2) weeks of treatment
Change in distance BCVA in the amblyopic eye, measured 12 months after cessation of treatment
Change in stereoacuity after 16 (± 2) and 8 (± 2) weeks of treatment
Adherence to interventions, measured by usage time as a proportion of prescribed time, following 8 (± 2) and 16 (± 2) weeks of treatment
Change in the interocular difference in contrast sensitivity from baseline to 16 (± 2) weeks
Proportion of participants experiencing adverse events, such as permanent diplopia (double vision), at any time point
Results
Description of studies
Results of the search
Our initial (2015) electronic search yielded a total of 541 references. The Cochrane Eyes and Vision Information Specialist (CIS) removed 105 duplicate records, screened the remaining 436 records, and removed 357 references that were not relevant to the scope of this review. We screened the remaining 79 references and discarded 70 reports as not relevant. We reviewed eight full‐text reports of seven studies for possible inclusion in the review. After this assessment, we excluded eight reports of seven studies (see Characteristics of excluded studies for details). That is, no studies met the inclusion criteria in 2015.
Updated searches run in November 2020 yielded a total of 482 records (Figure 1). After 108 duplicates were removed, the CIS screened the remaining 374 records, and removed 290 references that were not relevant to the scope of the review. We screened the remaining 84 references and obtained 17 full‐text reports for further assessment. We included one new study in the review (Holmes 2016), and excluded 13 studies (see Characteristics of excluded studies).
Included studies
Holmes 2016 recruited 385 children aged 5 to 13 years old, 187 of whom were female. Sixty‐eight children were aged between three and eight years; we requested, received and analysed their data. Thirty‐six children were randomised to a binocular iPad game (implementing anti‐suppression therapy) and 32 children were randomised to conventional patching treatment. Please see Characteristics of included studies for further details.
Excluded studies
In our 2015 review, we excluded eight full‐text reports of seven studies; none of the studies met the inclusion criteria. For the 2022 update, we excluded six full‐text reports of six studies, this in total is 13 excluded studies. We have listed the reasons for exclusion in the Characteristics of excluded studies table. Discussion of the results of these studies are included in the Description of the intervention section.
Ongoing studies
We identified three ongoing studies (ChiCTR1900022490; NCT03754153; NCT03767985). Because NCT03767985 should have completed recruitment, we contacted the study lead, who informed us that recruitment had finished, but they were awaiting the collection of follow‐up data. As data collection is ongoing, we did not include this study in this review; however, we shall assess these data once they become available. NCT03754153 and ChiCTR1900022490 may be included in the next edition of this review, as recruitment is still ongoing.
Risk of bias in included studies
We evaluated the risk of bias according to prespecified criteria in RoB 1 (Figure 2). Overall, we judged Holmes 2016 to have a low risk of bias, however, some elements were unclear from the available reports (Figure 3).
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
Allocation
Holmes 2016 used a computer generated permuted block design randomisation, with 1:1 allocation, stratified by age and site. This was considered an appropriate allocation method, and as such we determined that there was low risk of selection bias. Allocation concealment was also deemed adequate as the examiner was masked.
Blinding
The primary outcome of Holmes 2016 was the change in visual acuity following treatment with either a binocular iPad game (implementing anti‐suppression therapy) or patching. Visual acuity and stereoacuity assessment were completed by an examiner masked to the participant's treatment allocation. Investigators unmasked to the participants' treatment allocation carried out the remaining examinations, such as ocular alignment and completion of questionnaires. As the primary outcome was performed by masked observers, detection bias for the primary outcome could be considered low risk. However, having some investigations completed by team members unmasked to treatment allocation could introduce some bias on any other outcomes reported. Therefore, we judged the overall risk of bias to be unclear. Allocation was not blinded to the participants as they undertook two different tasks. It is not possible to undertake a placebo comparison with two different treatment arms.
Incomplete outcome data
Holmes 2016 data had an attrition rate of 4% in the patching group and 1% in the binocular group at 16 weeks. As mentioned above, the primary study outcome was change in visual acuity after 16 weeks of treatment. One hundred and ninety participants were recruited to each treatment arm; 182 participants in the patching group and 188 in the binocular group completed the 16 week follow‐up visit. Therefore, the overall risk of attrition bias was considered to be low.
Selective reporting
We had insufficient evidence to judge reporting bias in Holmes 2016. For example, it was not possible to interpret the stereoacuity data because the dataset was supplied in rank change format (i.e. the change from baseline per participant was not supplied). Data have now been offered and will be incorporated in the next update of this review. The analysis window for the 16‐week follow‐up visit was 98 to 140 days; from the supplementary information, seven participants completed the 16‐week visit outside of the analysis window (at 147 to 196 days), though these participants were retained in the analysis. While the number completing the primary outcome visit outside the analysis window was small (7/370), the inclusion of participants outside the analysis window led to our assessment of an unclear risk of bias.
Other potential sources of bias
There were no risk of bias in relation to financial interests and no obvious conflict of interest identified.
Effects of interventions
See: Table 1
We included one trial in this review (Holmes 2016). As detailed in the Included studies section and the Table 1, 68 children from this study satisfied the inclusion criteria, and we therefore included their data in this review. Data were obtained for our primary outcome and the following secondary outcomes:
Primary outcome
Change in distance best‐corrected visual acuity (BCVA) in the amblyopic eye from baseline to 16 (± 2) weeks of treatment
At 16 weeks of treatment, mean amblyopic eye BCVA in the patching group improved by 0.24 logMAR from baseline. Mean improvement for the iPad (binocular group) was 0.21 logMAR. Improvements for the patching group were 0.03 logMAR better (95% CI ‐0.04 worse to 0.10‐ better) than those of the binocular group, although the overlap of the CI with zero indicates a non‐significant difference. Therefore, we cannot exclude the possibility that they are clinically comparable. The certainty of evidence for the visual acuity at 16 weeks of treatment was rated moderate using the GRADE criteria, downgrading by one level due to imprecision.
Secondary outcomes
Change in BCVA in the amblyopic eye from baseline to 8 (± 2) weeks of treatment
Improvement in amblyopic eye acuity was observed in both the patching and binocular groups at the 8‐week follow‐up interval. Improvement with patching was found to be 0.02 logMAR better (95% CI ‐0.04 worse to 0.08 better) than the binocular treatment. Again, this difference in improvement between the patching and binocular group is non‐significant, suggesting that the tests are clinically comparable. The certainty of evidence for the visual acuity at 8 weeks of treatment was rated moderate using the GRADE criteria, downgrading by one level due to imprecision.
Change in distance BCVA in the amblyopic eye, 12 months after cessation of treatment
The included study did not measure this outcome.
Change in stereoacuity from baseline to 8 (± 2) and 16 (± 2) weeks of treatment
The included study did not measure this outcome.
Adherence to interventions following 8 (± 2) and 16 (± 2) weeks of treatment
Compliance was reported to be high in the patching group (90.3% reported adherence of 75% or more) compared to the iPad group (46.9% reported adherence of 75% or more). The certainty of evidence for the adherence to the interventions at 16 and 8 weeks of treatment was rated moderate using the GRADE criteria, downgrading by one level due to imprecision.
Change in the interocular difference in contrast sensitivity from baseline to 16 (± 2) weeks of treatment
The included study did not measure this outcome.
Proportion of participants experiencing adverse events, such as permanent diplopia (double vision), at any time point
In this small subgroup analysis, no participant was reported to have experienced permanent diplopia. However, it was noted that one participant self‐reported episodes of diplopia up to 10 times a day at the 16‐week follow‐up. As this analysis included a relatively small sample size, the authors cannot be certain that there was adequate power to detect any true risk of permanent diplopia in this study. The certainty of evidence was downgraded by two levels and rated low for the proportion of participants reporting adverse events due to the sample size.
Discussion
Summary of main results
We identified one RCT examining anti‐suppression therapy that met our inclusion criteria (Holmes 2016). This study compared a new anti‐suppression therapy against the standard patching treatment. We analysed a subset of data that fit our criteria. In this, our findings were that the subset of data, both treatments successfully improved acuity, though the difference between them was non‐significant, and the data was limited by the small sample size and imprecision in the primary and secondary outcomes.
Overall completeness and applicability of evidence
Holmes 2016 examined the efficacy of a binocular treatment (anti‐suppression therapy) compared to conventional treatment (patching) in children with amblyopia. The study included children aged 5 to 12 years, making the full published dataset outside the age range of this review. The full published dataset also included children who had previously undergone amblyopia treatment. A subset of participants did fit the remit of this review and following a request, Holmes 2016 kindly obliged by providing the data for the eligible subset in order to complete this update.
We obtained data relating to children aged five to eight years who did not have any prior patching treatment. Participants were randomised to either binocular treatment or conventional patching. Data were available for 16‐week and 8‐week follow‐up visits (Table 1). We obtained data for the mean amblyopic eye visual acuity, adverse events (diplopia), and adherence to prescribed treatment at each follow‐up point. We were unable to analyse the provided stereoacuity values because the results were presented in a rank format. Contrast sensitivity was not evaluated in this study, so we did not seek the data. Final follow‐up in this study was 16 weeks; therefore, change in distance BCVA in the amblyopic eye 12 months after cessation of treatment was not available.
Despite all the relevant studies being identified in this review, the review remains limited by the number of studies available for inclusion. Many studies were excluded as the participant group included children who had had prior amblyopia treatment. Regression of visual acuity over time is possible following conventional amblyopia treatment; therefore, including previously treated amblyopes can confound data, as it is not possible to differentiate between visual acuity gain from the study treatment arms or previous amblyopia treatment. In order to identify real change achieved with binocular amblyopia treatments, it is important to maintain exclusion of previously treated amblyopia.
Quality of the evidence
Only one RCT met the criteria for inclusion (Holmes 2016), from which only a small subset of the data were applicable to this review. The overall certainty of the included methodology was good. The study was limited in that the protocol included previously treated amblyopic children, though however the subset analysis that we undertook dealt with this issue. There was no inconsistency of results noted, but we do note that the data provided for the 16‐week and 8‐week timepoints was low. We therefore downgraded its rating due to the resulting imprecision. We graded the certainty of evidence for the proportion of participants experiencing adverse events to low and downgraded this two levels due to the small sample size. There was no notable publication bias. Overall, the available evidence does not therefore allow us to draw robust conclusions regarding the efficacy of binocular amblyopia treatments compared to conventional patching or blurring eye drops.
Potential biases in the review process
Although all relevant studies were identified in this review, the review is obviously limited by the number of studies suitable for inclusion. Given our adherence to the protocol set out in our plan, the review presents the best‐possible characterisation of the current evidence on the efficacy of these treatments.
Agreements and disagreements with other studies or reviews
The rather muted conclusions of this review differ somewhat from the optimism of reviews discussing exploratory studies on binocular treatments for amblyopia (Hess 2014; Hess 2015; Levi 2015; Piano 2019; Tailor 2016; Tailor 2017). A range of these exploratory studies have investigated the effectiveness of binocular treatments on individuals with amblyopia (Black 2012; Bossi 2017; Cleary 2009; Eastgate 2006; Foss 2013; Gambacorta 2018; Gao 2018; Herbison 2013; Herbison 2016; Hess 2010a; Hess 2010b; Hess 2012; Kelly 2016; Knox 2012; Li 2014; Rajavi 2019; Repka 2014; Sauvan 2019; Spiegel 2013a; Spiegel 2013b; To 2011; Vedamurthy 2015b; Waddingham 2006), a summary of which is included in Table 3 and Table 4. While these do give us insight into possible effectiveness of the binocular treatment approach, the results of these published cohort studies are limited by various methodological factors, such as the lack of a control group, the use of different testing protocols for visual acuity, stereoacuity and other psychophysical assessments, and the enrolment of participants from different age groups, different subtypes of amblyopia, and those with and without prior treatment. A further systematic review encompassing studies outside the remit of this review may be useful in this regard. However, the variability in treatment outcomes amongst these studies does suggest that their success will depend on the precise nature of the binocular treatment approach, including details such as the treatment duration, daily dose duration, and viewing content. Therefore, it is important that these approaches are examined in further RCTs.
2. Summary of methodologies in published studies of binocular treatment for amblyopia.
| Treatment | N | Age range (mean) | Control group | Type of amblyopia | Previous treatment other than glasses | Treatment duration | Daily dose received | Total dose received | |
| Hess 2010a; Hess 2010b | Anti‐suppression: dichoptic coherent motion, via lenticular overlay, red‐green glasses or head‐mounted display | 9 | 24 to 49 (39.6) | No | Strabismic, combined mechanism | 5/9 occlusion | Around 60 trials/block (0.5 to 3.7 per week, i.e. 1 to 3 hours in 2 to 3 days for 2 to 6 weeks) | ‐ | 8.2 blocks per week (SD 6.3) |
| Hess 2012 | Anti‐suppression: Tetris game with modulation of contrast on iPod | 10 | 17 to 51 (33.8) | No | All | 4/10 occlusion | 0.5 to 2 hours per day for 1 to 9 weeks | 45 min to 1 hour | 15 sessions (SD 4) |
| Knox 2012 | Anti‐suppression: Tetris game using head‐mounted display goggles | 14 | 5 to 14 (8.5) | No | All | All occlusion (at least 6 months) | 1 hour for 5 days in 1 week | 1 hour | 5 hours |
| To 2011 | Anti‐suppression: Tetris game, interleaved breaks, via lenticular layer | 9 | 18 to 51 (35.5) | No | All | Not specified | 10 to 19 sessions | Not specified | 15.75 hours (0.88 to 27.42 hours per week) |
| Li 2014 | Anti‐suppression: binocular games through anaglyph glasses (contrast increment in fellow eye) | 45/50 binocular group; 24/25 sham group | 4 to 12 | Yes (sham game and +/‐ occlusion) | All | 77% occlusion or atropine for around 1.9 years (n = 58) | 4 hours/week for 4 weeks (+ 4 weeks in 60% binocular, but no gain) | ‐ | ≥ 1 hour per week, 4 weeks (i.e. 25% prescribed dose) |
| Kelly 2016 | Anti‐suppression: binocular iPad adventure game: red/green anaglyphic glasses worn to separate game elements; high contrast elements seen by amblyopic eye with altered contrast to fellow eye relative to visual acuity level | 28 | 4 to 10 (6.78) | Yes | All | None | 10 hours total (1 hour a day for 5 days over 2 weeks) | 1 hour per day | 10 hours |
| Gao 2018 | Anti‐suppression: falling blocks game on iPod with dichoptic offset of contrast | 115 (11 7 to 8 years of age) | > 7 years (age range not specified) | Yes (placebo) | All | No | 1 to 2 hours daily for six weeks | – | >10.5hrs (i.e. 25% of prescribed dose) |
| Sauvan 2019 | Anti‐suppression: dichoptic movie design: parts of image seen by one eye and complementary parts by the other with unequal contrast to amblyopic and non amblyopic eye | 17 | 9 to 67 years (34.47) |
Yes (sham ‐ treatment and patch for 2 hours prior to treatment) | All | 7/17 previous occlusion treatment | 6 x 1.5 hour dichoptic movie sessions for both groups; patched group augmented with 2 hours of patching prior to session | – | 16/17 participants ‐ 9 hours 1/17 participant – 7.5 hours |
| Birch 2020 | Anti‐suppression: binocular iPad adventure game: red/green anaglyphic glasses worn to separate game elements; high contrast elements seen by amblyopic eye with altered contrast to fellow eye relative to visual acuity level | 47 | 4.3 to 10.8 (6.8) |
Yes | All | 58% previous patching, atropine or both | 10 x 1 hour session over 2 weeks | 1 hour 5 days a week | 10 hours |
| Vedamurthy 2015a | Dichoptic action video‐games | 38 | 39.18 years | Yes (sham ‐ watching movies monocularly with patch on) | All | 25/38 previous occlusion treatment | Total treatment time 40 hours | – | 1.5 to 2 hours for 2 to 5 times per week |
| Vedamurthy 2015b | Dichoptic action video‐games | 23 | 39.57 (15.74) | No | All | Not stated | Total treatment 40 hours | Not stated | Not stated |
| Waddingham 2006 | I‐BiT™: videos and modified video games (imbalanced visual scene to favour amblyopic eye) | 6 | 5.42 to 7.75 (6.25) | No | All | 3 occlusion; 3 neither occlusion nor atropine | 7 to 15 sessions of 20 minutes each | 1 to 2 sessions of 20 minutes twice a week | mean 4.4 hours |
| Herbison 2013 | I‐BiT™: videos and modified video games (imbalanced visual scene to favour amblyopic eye) | 10 | 4 to 8 (5.4) | No | All | All, occlusion or atropine | 6 weeks, 0 to 10 games + 15 to 30 videos | 0 to 10 to 15 to 30 min per day | 159.3 min |
| Herbison 2016 | I‐BiT™: videos and modified video games (imbalanced visual scene to favour amblyopic eye) | 75 | 4 to 8 (separate means per group) | No | All | All, occlusion or atropine | 30 minutes a week for six weeks | – | 3 hours |
| Bossi 2017 | Balanced binocular viewing: watching modified movies wearing 3D glasses | 22 | 3.5 to 11.3 (6.6) | No | All | None | Anisometropia – 56 hours Strabismus – 168 hours |
56 min per day | Not reported |
3. Summary of outcomes in published studies of binocular treatment for amblyopia.
|
Treatment adherence % |
Visual acuity gain amblyopic eye in logMAR (SD) | Visual acuity % change in amblyopic eye * | Stereoacuity gain | Recurrence | |
| Hess 2010a; Hess 2010b | ‐ | 0.26 | Not specified | “significant” | Not specified |
| Hess 2012 | ‐ | 0.19 (0.17) | Not specified | 6/10 improved | Nil at 1 to 2 months (in 4/10) |
| Knox 2012 | All | 0.09 | 22% | 7/14 (small squint), 4/7 significant | Not specified |
| To 2011 | All | 0.16 (0.18) | Not specified (fellow eye acuity not available) | Trend of improvement | Not specified |
| Li 2014 | 34/45 (76%) | 0.08 (0.01) | Not specified (not individual acuities, also in supp. material) | 5/50, not significant | Nil at 3 months |
| Kelly 2016 | 82 to 100% | ||||
| Gao 2018 | 64% in treatment group | 0.06 (0.12) active group | Not specified | 0.23 (0.76) log seconds of arc in active group; no significant change | Not specified |
| Sauvan 2019 | 16/17 participants – 9 hours 1/17 participant – 7.5 hours |
0.08 in non‐patched group | Not specified | Trend of improvement in both groups; no statistically significant improvement | Not specified |
| Birch 2020 | 103% in binocular group | 0.15 | Not specified | No significant improvement reported | Not specified |
| Vedamurthy 2015a | All | 0.14 (0.01) in dichoptic game group | 28% (2%) | 0.18 (0.05) log arc second improvement | 0.12 (0.02) in dichoptic game group at 8 week follow‐up |
| Vedamurthy 2015b | Not stated | 0.14 | Not specified | ||
| Waddingham 2006 | – | 0.27 | 42% | – | Not specified |
| Herbison 2013 | 88.5% | 0.18 (0.143) | 32.3% | Not measured | 0.055 at 10 weeks (in 6/9) |
| Herbison 2016 | > 90% (specifics not given) | 0.06 to 0.10 (mean 0.08) | Not specified | No significant improvement | Not specified |
| Bossi 2017 | Anisometropia – 87% Strabismus – between 84% and 90% |
0.27 (0.22) | not reported | Anisometropia – 6/7, significant mean gain of 165 seconds of arc Strabismus – not reported |
Unclear, as participants went onto conventional treatments after BBV |
SD: standard deviation
* calculated as (AEs‐AEe)/(AEs‐FEe), where AEs and AEe are respectively visual acuity values in amblyopic eye at entry (best‐corrected visual acuity) and exit, FEe is the acuity in the fellow eye at entry (baseline)
Authors' conclusions
Implications for practice.
We only included a subset of data from one randomised controlled trial in this review and find the current evidence base is insufficient to recommend binocular treatment for clinical practice at this time. This was due to the downgrading two of the five GRADE domains for imprecision of the data and the small sample size. We are moderately confident in the results of the subset of data for this trial. It seems probable that following four months of treatment, improvement in amblyopic eye acuity obtained with binocular treatment is comparable to that obtained with patching. However, this study lacks longer term follow‐up data to indicate whether these gains can be maintained over time. Furthermore, it does not have a sufficient sample size to establish the risk of permanent diplopia following treatment.
Implications for research.
The current evidence base for binocular treatments in amblyopia is limited by methodology, in particular by the inclusion of previously treated children with amblyopia, or the reporting of non‐controlled cohort studies.
Future research should be conducted in the form of randomised controlled trials (RCT), using acknowledged methods of visual acuity and stereoacuity assessment with known reproducibility in order to reach firm conclusions regarding the applicability and efficacy of binocular treatments in amblyopia. Other important outcome measures include outcomes reported by users, treatment adherence levels, amblyopic eye acuity after prolonged periods (e.g. 12 months), and recurrence rates of amblyopia after cessation of treatment. There are currently a number of RCTs in progress, investigating binocular treatments in amblyopia, the results of which may provide further guidance in this area in the future.
What's new
| Date | Event | Description |
|---|---|---|
| 23 March 2022 | Amended | Following publication, further data have now been offered to the review team which will be incorporated in the next update of this review. We have added some text to clarify this in the review. We have also corrected some typological errors in the text. |
History
Protocol first published: Issue 11, 2014 Review first published: Issue 8, 2015
| Date | Event | Description |
|---|---|---|
| 18 February 2021 | New search has been performed | Searches updated; secondary outcomes updated; addition of a summary of findings table |
| 18 February 2021 | New citation required and conclusions have changed | One trial included (Holmes 2016); subset data analysed; conclusions updated |
Acknowledgements
2022 update Cochrane Eyes and Vision created and executed the electronic search strategies. We thank Eileen Birch and Dan Fortenbacher for their comments on the review and Jennifer Evans and Anupa Shah for her assistance in the review process.
We thank Ray Kraker, Director, PEDIG coordinating centre for providing the subset data from Holmes 2016 included in this review.
Appendices
Appendix 1. CENTRAL search strategy
#1 [mh amblyopia] #2 amblyop* #3 lazy near/3 eye* #4 [mh strabismus] #5 strabism* or squint* #6 astigmati* or meridonal #7 [mh anisometropia] #8 [mh "refractive errors"] #9 anisometropi* #10 ammetropi* #11#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 #12 [mh "computer systems"] #13 [mh software] #14 [mh "computer simulation"] #15 [mh "computer graphics"] #16 [mh "imaging, three‐dimensional"] #17 [mh "photic stimulation"] #18 [mh "therapy, computer‐assisted"] #19 [mh "play and playthings"] #20 [mh "video games"] #21 (computer) near/2 (game* or device* or application*) #22 handheld near/2 device* #23 (mobile) near/2 (phone* or app* or device*) #24 (perceptual) near/2 (learn* or train*) #25 anti‐suppression therap* #26 mirror haploscope* #27 head‐mounted video* #28 lenticular near/3 prism #29 Balanced Binocular Viewing #30 BBV #31 Interactive Binocular Treatment #32 i‐bit or I‐BiTTM #33 shutter near/3 (glasses or spectacles) #34 virtual reality #35 #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #33 or #34 #36 #11 and #35
Appendix 2. MEDLINE Ovid search strategy
1. randomized controlled trial.pt. 2. (randomized or randomised).ab,ti. 3. placebo.ab,ti. 4. dt.fs. 5. randomly.ab,ti. 6. trial.ab,ti. 7. groups.ab,ti. 8. or/1‐7 9. exp animals/ 10. exp humans/ 11. 9 not (9 and 10) 12. 8 not 11 13. exp amblyopia/ 14. amblyop$.tw. 15. (lazy adj3 eye$).tw. 16. exp strabismus/ 17. (strabism$ or squint$).tw. 18. (astigmati$ or meridonal).tw. 19. anisometropia/ 20. exp refractive errors/ 21. anisometropi$.tw. 22. ammetropi$.tw. 23. or/13‐22 24. exp computer systems/ 25. exp software/ 26. exp computer simulation/ 27. computer graphics/ 28. imaging, three‐dimensional/ 29. photic stimulation/ 30. therapy, computer‐assisted/ 31. "play and playthings"/ 32. video games/ 33. (computer adj2 (game$ or device$ or application$)).tw. 34. (handheld adj2 device$).tw. 35. (mobile adj2 (phone$ or app$ or device$)).tw. 36. (perceptual adj2 (learn$ or train$)).tw. 37. anti‐suppression therap$.tw. 38. mirror haploscope$.tw. 39. head‐mounted video$.tw. 40. (lenticular adj3 prism$).tw. 41. Balanced Binocular Viewing.tw. 42. BBV.tw. 43. Interactive Binocular Treatment.tw. 44. (i‐bit or I‐BiTTM).tw. 45. (shutter adj3 (glasses or spectacles)).tw. 46. virtual reality.tw. 47. or/24‐46 48. 23 and 47 49. 12 and 48
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville 2006.
Appendix 3. Embase Ovid search strategy
1. exp randomized controlled trial/ 2. exp randomization/ 3. exp double blind procedure/ 4. exp single blind procedure/ 5. random$.tw. 6. or/1‐5 7. (animal or animal experiment).sh. 8. human.sh. 9. 7 and 8 10. 7 not 9 11. 6 not 10 12. exp clinical trial/ 13. (clin$ adj3 trial$).tw. 14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 15. exp placebo/ 16. placebo$.tw. 17. random$.tw. 18. exp experimental design/ 19. exp crossover procedure/ 20. exp control group/ 21. exp latin square design/ 22. or/12‐21 23. 22 not 10 24. 23 not 11 25. exp comparative study/ 26. exp evaluation/ 27. exp prospective study/ 28. (control$ or prospectiv$ or volunteer$).tw. 29. or/25‐28 30. 29 not 10 31. 30 not (11 or 23) 32. 11 or 24 or 31 33. exp amblyopia/ 34. amblyop$.tw. 35. (lazy adj3 eye$).tw. 36. exp strabismus/ 37. (strabism$ or squint$).tw. 38. (astigmati$ or meridonal).tw. 39. anisometropia/ 40. exp refractive errors/ 41. anisometropi$.tw. 42. ammetropi$.tw. 43. or/33‐42 44. computer/ 45. computer system/ 46. computer simulation/ 47. computer graphics/ 48. photostimulation/ 49. computer assisted therapy/ 50. virtual reality/ 51. recreation/ 52. play/ 53. psychomotor performance/ 54. (computer adj2 (game$ or device$ or application$)).tw. 55. (handheld adj2 device$).tw. 56. (mobile adj2 (phone$ or app$ or device$)).tw. 57. (perceptual adj2 (learn$ or train$)).tw. 58. anti‐suppression therap$.tw. 59. mirror haploscope$.tw. 60. head‐mounted video$.tw. 61. (lenticular adj3 prism$).tw. 62. Balanced Binocular Viewing.tw. 63. BBV.tw. 64. Interactive Binocular Treatment.tw. 65. (i‐bit or I‐BiTTM).tw. 66. (shutter adj3 (glasses or spectacles)).tw. 67. virtual reality.tw. 68. or/44‐67 69. 43 and 68 70. 32 and 69
Appendix 4. ISRCTN search strategy
Amblyopia AND participant age range: child
Appendix 5. ClinicalTrials.gov search strategy
Condition = amblyopia AND study type = Interventional studies AND age = children
Appendix 6. WHO ICTRP search strategy
amblyopia = Condition limited to children
Data and analyses
Comparison 1. iPad versus patching.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Change in BCVA amblyopic eye at 16 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.2 Change in BCVA amblyopic eye at 8 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
1.1. Analysis.

Comparison 1: iPad versus patching, Outcome 1: Change in BCVA amblyopic eye at 16 weeks
1.2. Analysis.

Comparison 1: iPad versus patching, Outcome 2: Change in BCVA amblyopic eye at 8 weeks
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Holmes 2016.
| Study characteristics | ||
| Methods | Randomised controlled trial | |
| Participants | 385; subset 68 to be analysed | |
| Interventions | 36 for Binocular iPad game, 32 for conventional treatment | |
| Outcomes | Change in amblyopic‐eye VA from baseline to 16 weeks | |
| Notes | Additional information gathered from supplement 1 and 2, as not available and clear in the final published article. Funding source. This study was supported by the National Eye Institute, National Institutes of Health (NIH), Department of Health and Human Services grants EY011751, EY023198, and EY018810. Casey Eye Institute received support from NIH grant EY010572 to fund shared departmental resources for research purposes. Casey Eye Institute, Wilmer Institute,Mayo Clinic, Rainbow Babies and Children’s Hospital, and University of Minnesota received support from an unrestricted grant from Research to Prevent Blindness Inc. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Permutated block design stratified by age group (5 to < 7 years and 7 to < 13 years) and site |
| Allocation concealment (selection bias) | Low risk | Computer generated via the PEDIG website, determined by age group and site |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | A masked examiner performed distance visual acuity testing and stereo‐acuity testing. Researcher was not masked to randomisation of participant treatment group. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Main outcomes were performed by masked examiner. Other procedures were undertaken by researchers who were not masked to outcome of participant treatment group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The 16‐week primary outcome was completed by 182 children (95.8%) in the binocular group and 188 children (96.4%) in the patching group. |
| Selective reporting (reporting bias) | Unclear risk | CONSORT legend leads us to believe there is an unclear risk of reporting bias due to some participants performing outcome visits outside the specified time‐point window |
| Other bias | Low risk | There was no evidence demonstrating a conflict of evidence or funding source conflict for this study |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Astle 2011 | Perceptual learning to reduce stereo deficits. Adults; review article; no randomisation |
| Bau 2012 | Stimulation therapy: drifting sinus grating combined with computer games; better‐seeing eye occluded during treatment, so treatment not binocular |
| Birch 2020 | Insufficient follow‐up interval (too short) |
| Chen 2008 | Perceptual learning approach, grey‐level gratings, Gabor patch contrast detection task. Better‐seeing eye occluded during treatment, so treatment not binocular; no randomisation |
| Foss 2013 | None of the treatment groups received an occlusion or blurring treatment |
| Gambacorta 2018 | Insufficient follow‐up interval (too short) |
| Gao 2018 | None of the treatment groups received an occlusion or blurring treatment |
| Herbison 2016 | None of the treatment groups received an occlusion or blurring treatment |
| Ide 2013 | Treatment not for amblyopia |
| Kampf 2001 | Stimulation therapy: drifting sinus grating combined with foreground game. Better‐seeing eye occluded during treatment, so treatment not binocular |
| Kelly 2016 | Study time points not compatible with Cochrane protocol (8 or 16 weeks). |
| Lennerstrand 1983 | Stimulation therapy: grating; full‐time occlusion. Better‐seeing eye occluded during treatment, so treatment not binocular |
| Rajavi 2019 | Insufficient follow‐up interval (too short) |
Characteristics of ongoing studies [ordered by study ID]
ChiCTR1900022490.
| Study name | A randomized controlled study for a new binocular game in children with anisometropic amblyopia |
| Methods | Randomised controlled trial, patching treatment vs binocular game |
| Participants | 92 |
| Interventions | Binocular game |
| Outcomes | Ongoing |
| Starting date | 2019 |
| Contact information | dr_zhaochen@163.com |
| Notes | Recruitment end date March 2021 |
NCT03754153.
| Study name | Binocularly Balanced Viewing Study (BALANCE) |
| Methods | Randomised controlled trial, novel treatment vs conventional patching or pharmacological blurring |
| Participants | 66 |
| Interventions | Balanced binocular viewing (BBV) ‐ customised movies presented on Nintendo 3DSXL console |
| Outcomes | Ongoing |
| Starting date | September 2019 |
| Contact information | res-admin@moorfields.nhs.uk |
| Notes | Anticipated study conclusion June 2021 |
NCT03767985.
| Study name | A randomised clinical trial objectively comparing the effect of patching therapy with video gaming for amblyopia |
| Methods | Randomised controlled trial, standard patching therapy or the dichoptic video game therapy |
| Participants | 124 |
| Interventions | Dichoptic video game therapy |
| Outcomes | Ongoing |
| Starting date | December 2017 |
| Contact information | s.loudon@erasmusmc.nl |
| Notes | Anticipated study conclusion June 2021 |
Differences between protocol and review
2022 review update Following updated Cochrane guidance, we included methods for preparing a summary of findings table, including the use of the GRADE classification to grade the overall certainty of the evidence for each outcome, specified for inclusion in the summary of findings table.
The primary outcome of the previous review was the change in visual acuity 12 months following cessation of treatment. Unfortunately, there are no such trials investigating binocular treatment for amblyopia reporting this data. Many studies investigating binocular treatments report short‐term outcomes and it is unlikely at this stage that any trials will be in a position to report such data in the near future, given the early stages of these trials. There is also a paucity of data for this outcome in the conventional occlusion evidence base to facilitate comparison. In view of this, we amended the primary and secondary outcome time points in this review to 8 (± 2) and 16 (± 2) weeks. We undertook this amendment to ensure the maximum inclusion of available randomised controlled trials (RCT) to inform management decisions. While we amended the primary outcome, the outcome of change in amblyopic eye acuity 12 months after the cessation of treatment is still of utmost importance to accurately inform clinical practice. As such, this outcome remains an essential part of this review, and features as a secondary outcome. We have also clarified ambiguity in how the change in amblyopic eye best corrected visual acuity (BCVA) was reported – this is now reported as the change in BCVA of the amblyopic eye from baseline.
We have now simplified secondary outcomes to include the most salient outcomes, with amended secondary outcome time points such that where two timepoints are to be considered these consistently are 8 (± 2) and 16 (± 2) weeks. In order to ensure that any included RCTs provided adequate follow‐up time to identify real change in BCVA in both the conventional and binocular treatment arms, we decided to exclude studies where the follow‐up time was less than 8 (± 2) weeks. Currently in the UK, children undergoing amblyopia treatment attend between 4 and 10 follow‐up visits per annum (Royal College of Ophthalmologists). Therefore, 8 (± 2)‐week follow‐up was selected as the minimum time frame, to ensure the maximum inclusion of studies, whilst still ensuring that those included had allowed sufficient follow‐up time for treatment in the control and intervention arms to show treatment effect.
Different stereotests may be used across studies; as such, comparisons of any change in stereoacuity during treatment may be confounded by the type(s) of stereotest used. Therefore, we decided to amend how we reported the change in stereoacuity to ensure appropriate comparison. In this update, change in stereoacuity was reported in octaves, to ensure appropriate comparison across stereotests (Adams 2009).
Trial registration ID was added as a data collection item.
Where previously we had decided to collate rather than meta‐analyse data, we amended this in line with current guidance; in this protocol update, we decided to undertake meta‐analysis of outcomes where appropriate.
Contributions of authors
2022 update VT, SL, MB, JG, and ADN developed the background, objectives, and methods with CB's support in writing the methods section. VT and SL reviewed the results of the updated search. SL and VT drafted the results and discussion, and all review authors contributed critically to the final version.
Sources of support
Internal sources
-
National Institute for Health Research (NIHR) Biomedical Research Centre, UK
The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology.
The views expressed are those of the review author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
External sources
-
National Institute for Health Research (NIHR), UK
Up to March 2021, the NIHR supported this review update by funding the Cochrane Eyes and Vision editorial base.
The views expressed in this publication are those of the review authors and not necessarily those of the NIHR, NHS, or the Department of Health.
-
Public Health Agency, UK
As of April 2021, this review update was supported by the HSC Research and Development (R&D) Division of the Public Health Agency which funds the Cochrane Eyes and Vision editorial base at Queen's University Belfast.
-
Queen's University Belfast, UK
Gianni Virgili, Co‐ordinating Editor for Cochrane Eyes and Vision’s work, is funded by the Centre for Public Health, Queen’s University Belfast, Northern Ireland.
Declarations of interest
VT: No relevant interests were disclosed SL: No relevant interests were disclosed MB: No relevant interests were disclosed CB: No relevant interests were disclosed JG: No relevant interests were disclosed ADN: received payment from
Coopervistion inc. for speaking at an educational event;
Novartis for participation in a patient/family/eye care professional forum;
Santen and SightGlassVision for participating on their Advisory Board.
These activities are unrelated to the topic of this review.
Edited (no change to conclusions)
References
References to studies included in this review
Holmes 2016 {published and unpublished data}
- Holmes JM, Manh VM, Lazar EL, Beck RW, Birch EE, Kraker RT, et al.Effect of a binocular iPad game vs part-time patching in children aged 5 to 12 years with amblyopia. JAMA Ophthalmology 2016;134(12):1391-400. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Astle 2011 {published data only}
- Astle AT, McGraw PV, Webb BS.Can human amblyopia be treated in adulthood? Strabismus 2011;19(3):99-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bau 2012 {published data only}
- Bau V, Rose K, Pollack K, Spoerl E, Pillunat LE.Effectivity of an occlusion-supporting PC-based visual training programme by horizontal drifting sinus gratings in children with amblyopia. Klinische Monatsblatter fur Augenheilkunde 2012;229(10):979-86. [DOI] [PubMed] [Google Scholar]
Birch 2020 {published data only}NCT02365090
- Birch E, Jost RM, Kelly KR, Leffler JN, Dao L, Beauchamp CL.Baseline and clinical factors associated with response to binocular amblyopia treatment in a randomized clinical trial. Optometry and Vision Science 2020;97:316-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chen 2008 {published data only}
- Chen PL, Chen JT, Fu JJ, Chien KH, Lu DW.A pilot study of anisometropic amblyopia improved in adults and children by perceptual learning: an alternative treatment to patching. Ophthalmic and Physiological Optics 2008;28(5):422-8. [DOI] [PubMed] [Google Scholar]
Foss 2013 {published data only}
- Foss AJ, Gregson RM, MacKeith D, Herbison N, Ash IM, Cobb SV, et al.Evaluation and development of a novel binocular treatment (I-BiT) system using video clips and interactive games to improve vision in children with amblyopia ('lazy eye'): study protocol for a randomised controlled trial. Trials 2013;14:145. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gambacorta 2018 {published data only}
- Gambarcota C, Nahum M, Vedamurthy I, Bayliss J, Jordan J, Bavelier D, et al.An action video game for the treatment of amblyopia in children: a feasibility study. Vision Research 2018;148:1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gao 2018 {published data only (unpublished sought but not used)}
- Gao TY, Guo CX, Babu RJ, Black JM, Bobier WR, Chakraborty A, et al.Effectiveness of a binocular video game vs placebo video game for improving visual functions in older children, teenagers, and adults with amblyopia: a randomized clinical trial. JAMA Ophthalmology 2018;136(2):172-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Herbison 2016 {published data only}
- Herbison N, MacKeith D, Vivian A, Purdy J, Fakis A, Ash IM, et al.Randomised controlled trial of video clips and interactive games to improve vision in children with amblyopia using the I-BiT system. British Journal of Ophthalmology 2016;100(11):1511-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ide 2013 {published data only}
- Ide T, Ishikawa M, Tsubota K, Miyao M.The effect of 3D visual simulator on children's visual acuity – a pilot study comparing two different modalities. Open Ophthalmology Journal 2013;7:69-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kampf 2001 {published data only}
- Kampf U, Muchamedjarow F, Seiler T.Supportive amblyopia treatment by means of computer games with background stimulation; a placebo controlled pilot study of 10 days. Klinische Monatsblatter fur Augenheilkunde 2001;218(4):243-50. [DOI] [PubMed] [Google Scholar]
Kelly 2016 {published data only}
- Kelly KR, Reed JM, Dao L, Beauchamp CL, Leffler JM, Birch EE.Binocular iPad game vs patching for treatment of amblyopia in children. JAMA Ophthalmology 2016;134(12):1402-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lennerstrand 1983 {published data only}
- Lennerstrand G, Samuelsson B.Amblyopia in 4-year-old children treated with grating stimulation and full-time occlusion; a comparative study. British Journal of Ophthalmology 1983;67(3):181-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rajavi 2019 {published data only}NCT03940222
- Rajavi Z, Sabbaghi H, Sharifi A, Behradfar N, Kheiri B.Comparison between patching and interactive binocular treatment in amblyopia: a randomized clinical trial. Journal of Current Ophthalmology 2019;31:426-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to ongoing studies
ChiCTR1900022490 {published data only}
- ChiCTR1900022490.A randomized controlled study for a new binocular game in children with anisometropic amblyopia. www.chictr.org.cn/com/25/historyversionpuben.aspx?regno=ChiCTR1900022490 (last refreshed 13 April 2019).
NCT03754153 {published data only}
- NCT03754153.Binocularly Balanced Viewing Study (BALANCE). clinicaltrials.gov/ct2/show/NCT03754153 (first received 27 November 2018).
NCT03767985 {published data only}
- NCT03767985.Patching or gaming as amblyopia treatment. clinicaltrials.gov/ct2/show/NCT03767985 (first received 7 December 2018).
Additional references
Adams 2009
- Adams WE, Leske DA, Hatt SR, Holmes JM.Defining real change in measures of stereoacuity. Ophthalmology 2009;116(2):281-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Anderson 2012
- Anderson EJ, Dakin SC, Schwarzkopf DS, Rees G, Greenwood JA.The neural correlates of crowding-induced changes in appearance. Current Biology 2012;22(13):1199-206. [DOI] [PMC free article] [PubMed] [Google Scholar]
Assaf 1982
- Assaf AA.The sensitive period: transfer of fixation after occlusion for strabismic amblyopia. British Journal of Ophthalmology 1982;66(1):64-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Astle 2011
- Astle, AT, Webb, BS, & McGraw, PV.The pattern of learned visual improvements in adult amblyopia. Investigative Ophthalmology & Visual Science. 2011;52(10):7195-7204. [DOI] [PMC free article] [PubMed] [Google Scholar]
Awan 2005
- Awan M, Proudlock FA, Gottlob I.A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Investigative Ophthalmology & Visual Science 2005;46(4):1435-9. [DOI] [PubMed] [Google Scholar]
Baker 2007
- Baker DH, Meese TS, Mansouri B, Hess RF.Binocular summation of contrast remains intact in strabismic amblyopia. Investigative Ophthalmology & Visual Science 2007;48(11):5332-8. [DOI] [PubMed] [Google Scholar]
Baker 2008
- Baker DH, Meese TS, Hess RF.Contrast masking in strabismic amblyopia: attenuation, noise, interocular suppression and binocular summation. Vision Research 2008;48(15):1625-40. [DOI] [PubMed] [Google Scholar]
Barnes 2001
- Barnes GR, Hess RF, Dumoulin SO, Achtman RL, Pike GB.The cortical deficit in humans with strabismic amblyopia. Journal of Physiology 2001;533(Pt 1):281-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Barrett 2003
- Barrett BT, Pacey IE, Bradley A, Thibos LN, Morrill P.Nonveridical visual perception in human amblyopia. Investigative Ophthalmology & Visual Science 2003;44(4):1555-67. [DOI] [PubMed] [Google Scholar]
Barrett 2004
- Barrett BT, Bradley A, McGraw PV.Understanding the neural basis of amblyopia. Neuroscientist 2004;10(2):106-17. [DOI] [PubMed] [Google Scholar]
Birch 2000
- Birch EE, Swanson WH.Hyperacuity deficits in anisometropic and strabismic amblyopes with known ages of onset. Vision Research 2000;40(9):1035-40. [DOI] [PubMed] [Google Scholar]
Birch 2013
- Birch EE.Amblyopia and binocular vision. Progress in Retinal and Eye Research 2013;33:67-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Birch 2019
- Birch EE, Castañeda YS, Cheng-Patel CS, Morale SE, Kelly KR, Beauchamp CL, et al.Self-perception in children aged 3 to 7 years with amblyopia and its association with deficits in vision and fine motor skills. JAMA Ophthalmology 2019;137(5):499-506. [DOI] [PMC free article] [PubMed] [Google Scholar]
Black 2011
- Black JM, Thompson B, Maehara G, Hess RF.A compact clinical instrument for quantifying suppression. Optometry and Vision Science 2011;88(2):E334-43. [DOI] [PubMed] [Google Scholar]
Black 2012
- Black JM, Hess RF, Cooperstock JR, To L, Thompson B.The measurement and treatment of suppression in amblyopia. Journal of Visualized Experiments 2012;70:e3927. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bossi 2014
- Bossi M, Anderson EJ, Tailor V, Bex PJ, Greenwood JA, Dahlmann-Noor A, et al.An exploratory study of a novel home-based binocular therapy for childhood amblyopia. Investigative Ophthalmology & Visual Science 2014;55(5):ARVO E-abstract 5981. [DOI] [PubMed] [Google Scholar]
Bossi 2017
- Bossi M, Tailor VK, Anderson EJ, Bex P, Greenwood JA, Dahlmann-Noor AH, et al.Binocular therapy for childhood amblyopia improves vision without breaking interocular suppression. Investigative Ophthalmology & Visual Science 2017;58(7):3031-43. [DOI] [PubMed] [Google Scholar]
Brown 2019
- Brown R, Blanchfied P, Fakis A, McGraw P, Foss AJ, I-Bit Study Group.Clinical investigation plan for the use of interactive binocular treatment (I-BiT) for the management of anisometropic, strabismic and mixed amblyopia in children aged 3.5-12 years: a randomised controlled trial. Trials 2019;20(1):437. [DOI: 10.1186/s13063-019-3523-0] [DOI] [PMC free article] [PubMed] [Google Scholar]
Carlton 2008
- Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4-5 years: a systematic review and economic evaluation. Health Technology Assessment 2008;12(25):iii, xi-194. [DOI] [PubMed] [Google Scholar]
Clavagnier 2015
- Clavagnier S, Dumoulin SO, Hess RF.Is the cortical deficit in amblyopia due to reduced cortical magnification, loss of neural resolution, or neural disorganization? Journal of Neuroscience 2015;35(44):14740-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cleary 2009
- Cleary M, Moody AD, Buchanan A, Stewart H, Dutton GN.Assessment of a computer-based treatment for older amblyopes: the Glasgow Pilot Study. Eye 2009;23(1):124-31. [DOI] [PubMed] [Google Scholar]
Conner 2007
- Conner IP, Odom JV, Schwartz TL, Mendola JD.Monocular activation of V1 and V2 in amblyopic adults measured with functional magnetic resonance imaging. Journal of AAPOS 2007;11(4):341-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Corbetta 1995
- Corbetta M, Shulman GL, Miezin FM, Petersen SE.Superior parietal cortex activation during spatial attention shifts and visual feature conjunction. Science 1995;270(5237):802-5. [DOI] [PubMed] [Google Scholar]
Cotter 2006
- Cotter SA, Edwards AR, Wallace DK, Beck RW, Arnold RW, Astle WF, et al.Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology 2006;113(6):895-903. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cotter 2007
- Cotter SA, Edwards AR, Arnold RW, Astle WF, Barnhardt CN, Beck RW, et al.Treatment of strabismic amblyopia with refractive correction. American Journal of Ophthalmology 2007;143(6):1060-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
daCunha 1961
- daCunha D, Jenkins EM.Amblyopia in three year olds. Medical Officer 1961;106:146-8. [Google Scholar]
Davis 2006
- Davis AR, Sloper JJ, Neveu MM, Hogg CR, Morgan MJ, Holder GE.Differential changes of magnocellular and parvocellular visual function in early- and late-onset strabismic amblyopia. Investigative Ophthalmology & Visual Science 2006;47(11):4836-41. [DOI] [PubMed] [Google Scholar]
Daw 1998
- Daw NW.Critical periods and amblyopia. Archives of Ophthalmology 1998;116(4):502-5. [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JPT, Altman DG, editor(s), on behalf of the Cochrane Statistical Methods Group.Chapter 9: Analysing data and undertaking meta-analyses. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017). Cochrane, 2017. Available from training.cochrane.org/handbook/archive/v5.2.
Dixon‐Woods 2006
- Dixon-Woods M, Awan M, Gottlob I.A qualitative study. Archives of Disease in Childhood 2006;91(6):491-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Eastgate 2006
- Eastgate RM, Griffiths GD, Waddingham PE, Moody AD, Butler TK, Cobb SV, et al.Modified virtual reality technology for treatment of amblyopia. Eye 2006;20(3):370-4. [DOI] [PubMed] [Google Scholar]
Eibschitz‐Tsimhoni 2000
- Eibschitz-Tsimhoni M, Friedman T, Naor J, Eibschitz N, Friedman Z.Early screening for amblyogenic risk factors lowers the prevalence and severity of amblyopia. Journal of AAPOS 2000;4(4):194-9. [DOI] [PubMed] [Google Scholar]
Espinosa 2012
- Espinosa JS, Stryker MP.Development and plasticity of the primary visual cortex. Neuron 2012;75(2):230-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
Evans 2011
- Evans BJ, Yu CS, Massa E, Mathews JE.Randomised controlled trial of intermittent photic stimulation for treating amblyopia in older children and adults. Ophthalmic and Physiological Optics 2011;31(1):56-68. [DOI] [PubMed] [Google Scholar]
Felius 2010
- Felius J, Chandler DL, Holmes JM, Chu RH, Cole SR, Hill M, et al.Evaluating the burden of amblyopia treatment from the parent and child's perspective. Journal of AAPOS 2010;14(5):389-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gilbert 2008
- Gilbert CE, Ellwein LB.Prevalence and causes of functional low vision in school-age children: results from standardized population surveys in Asia, Africa, and Latin America. Investigative Ophthalmology & Visual Science 2008;49(3):877-81. [DOI] [PubMed] [Google Scholar]
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso-Stefinovic J.How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130-6. [PMC free article] [PubMed] [Google Scholar]
Goodale 1992
- Goodale MA, Milner AD.Separate visual pathways for perception and action. Trends in Neurosciences 1992;15(1):20-5. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime) GRADEpro GDT .Hamilton (ON): McMaster University (developed by Evidence Prime), accessed 18 March 2021. Available at gradepro.org.
Grant 2007
- Grant S, Melmoth DR, Morgan MJ, Finlay AL.Prehension deficits in amblyopia. Investigative Ophthalmology & Visual Science 2007;48(3):1139-48. [DOI] [PubMed] [Google Scholar]
Grant 2011
- Grant S, Moseley MJ.Amblyopia and real-world visuomotor tasks. Strabismus 2011;19(3):119-28. [DOI] [PubMed] [Google Scholar]
Greenwood 2012
- Greenwood JA, Tailor VK, Sloper JJ, Simmers AJ, Bex PJ, Dakin SC.Visual acuity, crowding, and stereo-vision are linked in children with and without amblyopia. Investigative Ophthalmology & Visual Science 2012;53(12):7655-65. [DOI] [PubMed] [Google Scholar]
Harwerth 1986
- Harwerth RS, Smith EL 3rd, Duncan GC, Crawford ML, Noorden GK.Multiple sensitive periods in the development of the primate visual system. Science 1986;232(4747):235-8. [DOI] [PubMed] [Google Scholar]
Herbison 2013
- Herbison N, Cobb S, Gregson R, Ash I, Eastgate R, Purdy J, et al.Interactive binocular treatment (I-BiT) for amblyopia: results of a pilot study of 3D shutter glasses system. Eye 2013;27(9):1077-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hertle 2007
- Hertle RW, Scheiman MM, Beck RW, Chandler DL, Bacal DA, Birch E, et al.Stability of visual acuity improvement following discontinuation of amblyopia treatment in children aged 7 to 12 years. Archives of Ophthalmology 2007;125(5):655-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hess 1994
- Hess RF, Field DJ.Is the spatial deficit in strabismic amblyopia due to loss of cells or an uncalibrated disarray of cells? Vision Research 1994;34(24):3397-406. [DOI] [PubMed] [Google Scholar]
Hess 2010a
- Hess RF, Mansouri B, Thompson B.A new binocular approach to the treatment of amblyopia in adults well beyond the critical period of visual development. Restorative Neurology and Neuroscience 2010;28(6):793-802. [DOI] [PubMed] [Google Scholar]
Hess 2010b
- Hess RF, Mansouri B, Thompson B.A binocular approach to treating amblyopia: antisuppression therapy. Optometry and Vision Science 2010;87(9):697-704. [DOI] [PubMed] [Google Scholar]
Hess 2011
- Hess RF, Mansouri B, Thompson B.Restoration of binocular vision in amblyopia. Strabismus 2011;19(3):110-8. [DOI] [PubMed] [Google Scholar]
Hess 2012
- Hess RF, Thompson B, Black JM, Machara G, Zhang P, Bobier WR, et al.An iPod treatment of amblyopia: an updated binocular approach. Optometry 2012;83(2):87-94. [PubMed] [Google Scholar]
Hess 2013
- Hess RF, Thompson B.New insights into amblyopia: binocular therapy and noninvasive brain stimulation. Journal of AAPOS 2013;17(1):89-93. [DOI] [PubMed] [Google Scholar]
Hess 2014
- Hess RF, Thompson B, Baker DH.Binocular vision in amblyopia: structure, suppression and plasticity. Ophthalmic & Physiological Optics 2014;34(2):146-62. [DOI] [PubMed] [Google Scholar]
Hess 2015
- Hess RF, Thompson B.Amblyopia and the binocular approach to its therapy. Vision Research 2015;114:4-16. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Deeks JJ, editor(s).Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S, editor(s), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Higgins 2017
- Higgins JPT, Altman DG, Sterne JAC, editor(s).Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017). Cochrane, 2017. Available from training.cochrane.org/handbook/archive/v5.2.
Ho 2006
- Ho CS, Paul PS, Asirvatham A, Cavanagh P, Cline R, Giaschi DE.Abnormal spatial selection and tracking in children with amblyopia. Vision Research 2006;46(19):3274-83. [DOI] [PubMed] [Google Scholar]
Holmes 2003
- Holmes JM, Kraker RT, Beck RW, Birch EE, Cotter SA, Everett DF, et al.A randomized trial of prescribed patching regimens for treatment of severe amblyopia in children. Ophthalmology 2003;110(11):2075-87. [DOI] [PubMed] [Google Scholar]
Holmes 2004
- Holmes JM, Beck RW, Kraker RT, Astle WF, Birch EE, Cole SR, et al.Risk of amblyopia recurrence after cessation of treatment. Journal of AAPOS 2004;8(5):420-8. [DOI] [PubMed] [Google Scholar]
Holmes 2008
- Holmes J, Strauber S, Quinn G, Cole S, Felius J, Kulp M, et al.Further validation of the Amblyopia Treatment Index parental questionnaire. Journal of AAPOS 2008;12(6):581-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Holmes 2011
- Holmes JM, Lazar EL, Melia BM, Astle WF, Dagi LR, Donahue SP, et al.Effect of age on response to amblyopia treatment in children. Archives of Ophthalmology 2011;129(11):1451-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hrisos 2006
- Hrisos S, Clarke MP, Kelly T, Henderson J, Wright CM.Unilateral visual impairment and neurodevelopmental performance in preschool children. British Journal of Ophthalmology 2006;90(7):836-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Husk 2012
- Husk JS, Farivar R, Hess RF.Amblyopic deficits in processing structure-from-motion. Journal of Vision 2012;12(4):1-12. [DOI] [PubMed] [Google Scholar]
Hussain 2012
- Hussain Z, Webb BS, Astle AT, McGraw PV.Perceptual learning reduces crowding in amblyopia and in the normal periphery. Journal of Neuroscience 2012;32(2):474-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
ISRCTN51712593
- EuPatch (European Paediatric Amblyopia Treatment Study for Children): the role of glasses wearing in amblyopia treatment. https://www.isrctn.com/search?q=51712593. [ISCRCTN: 51712593]
Kiorpes 1998
- Kiorpes L, Kiper DC, O'Keefe LP, Cavanaugh JR, Movshon JA.Neuronal correlates of amblyopia in the visual cortex of macaque monkeys with experimental strabismus and anisometropia. Journal of Neuroscience 1998;18(16):6411-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kiorpes 1999
- Kiorpes L, McKee SP.Neural mechanisms underlying amblyopia. Current Opinion in Neurobiology 1999;9(4):480-6. [DOI] [PubMed] [Google Scholar]
Knox 2012
- Knox PJ, Simmers AJ, Gray LS, Cleary M.An exploratory study: prolonged periods of binocular stimulation can provide an effective treatment for childhood amblyopia. Investigative Ophthalmology & Visual Science 2012;53(2):817-24. [DOI] [PubMed] [Google Scholar]
Levi 1982
- Levi DM, Klein S.Differences in vernier discrimination for grating between strabismic and anisometropic amblyopes. Investigative Ophthalmology & Visual Science 1982;23(3):398-407. [PubMed] [Google Scholar]
Levi 1985
- Levi DM, Klein SA.Vernier acuity, crowding and amblyopia. Vision Research 1985;25(7):979-91. [DOI] [PubMed] [Google Scholar]
Levi 1986
- Levi DM, Klein SA.Sampling in spatial vision. Nature 1986;320(6060):360-2. [DOI] [PubMed] [Google Scholar]
Levi 2005
- Levi DM.Perceptual learning in adults with amblyopia: a reevaluation of critical periods in human vision. Developmental Psychobiology 2005;46(3):222-32. [DOI] [PubMed] [Google Scholar]
Levi 2008
- Levi DM.Crowding – an essential bottleneck for object recognition: a mini-review. Vision Research 2008;48(5):635-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Levi 2009
- Levi DM, Li RW.Improving the performance of the amblyopic visual system. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences 2009;364(1515):399-407. [DOI] [PMC free article] [PubMed] [Google Scholar]
Levi 2015
- Levi DM, Knill DC, Bavelier D.Stereopsis and amblyopia: a mini-review. Vision Research 2015;114:17-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2007
- Li X, Dumoulin SO, Mansouri B, Hess RF.The fidelity of the cortical retinotopic map in human amblyopia. European Journal of Neuroscience 2007;25(5):1265-77. [DOI] [PubMed] [Google Scholar]
Li 2009
- Li T, Shotton K.Conventional occlusion versus pharmacologic penalization for amblyopia. Cochrane Database of Systematic Reviews 2009, Issue 4. Art. No: CD006460. [DOI: 10.1002/14651858.CD006460.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2011
- Li J, Thompson B, Lam CS, Deng D, Chan LY, Maehara G, et al.The role of suppression in amblyopia. Investigative Ophthalmology & Visual Science 2011;52(7):4169-76. [DOI] [PubMed] [Google Scholar]
Li 2014
- Li SL, Jost RM, Morale SE, Stager DR, Dao L, Stager D, et al.A binocular iPad treatment for amblyopic children. Eye 2014;28(10):1246-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Loudon 2006
- Loudon SE, Fronius M, Looman CW, Awan M, Simonsz B, Maas PJ, et al.Predictors and a remedy for noncompliance with amblyopia therapy in children measured with the occlusion dose monitor. Investigative Ophthalmology & Visual Science 2006;47(10):4393-400. [DOI] [PubMed] [Google Scholar]
Malik 1975
- Malik SR, Virdi PS, Goel BK.Follow-up results of occlusion and pleoptic treatment. Acta Ophthalmologica 1975;53(4):620-6. [DOI] [PubMed] [Google Scholar]
Mansouri 2008
- Mansouri B, Thompson B, Hess RF.Measurement of suprathreshold binocular interactions in amblyopia. Vision Research 2008;48(28):2775-84. [DOI] [PubMed] [Google Scholar]
Maus 2010
- Maus GW, Weigelt S, Nijhawan R, Muckli L.Does area V3A predict positions of moving objects? Frontiers in Psychology 2010;1:186. [DOI] [PMC free article] [PubMed] [Google Scholar]
McKee 2003
- McKee SP, Levi DM, Movshon JA.The pattern of visual deficits in amblyopia. Journal of Vision 2003;3(5):380-405. [DOI] [PubMed] [Google Scholar]
McNeil 1955
- McNeil J.Patterns of visual deficits in children. British Medical Journal 1955;39:820–5. [Google Scholar]
Mirabella 2011
- Mirabella G, Hay S, Wong AM.Deficits in perception of images of real-world scenes in patients with a history of amblyopia. Archives of Ophthalmology 2011;129(2):176-83. [DOI] [PubMed] [Google Scholar]
Mitchell 2009
- Mitchell DE, Sengpiel F.Neural mechanisms of recovery following early visual deprivation. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences 2009;364(1515):383-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moseley 1995
- Moseley M, Fielder A.Measurement of compliances with occlusion therapy. Journal of Pediatric Ophthalmology and Strabismus 1995;32(6):399-400. [DOI] [PubMed] [Google Scholar]
Neri 2006
- Neri P, Levi DM.Spatial resolution for feature binding is impaired in peripheral and amblyopic vision. Journal of Neurophysiology 2006;96(1):142-53. [DOI] [PubMed] [Google Scholar]
Niechwiej‐Szwedo 2011
- Niechwiej-Szwedo E, Goltz HC, Chandrakumar M, Hirji Z, Wong AM.Effects of anisometropic amblyopia on visuomotor behavior, III: Temporal eye-hand coordination during reaching. Investigative Ophthalmology & Visual Science 2011;52(8):5853-61. [DOI] [PubMed] [Google Scholar]
O'Connor 2010
- O'Connor AR, Birch EE, Anderson S, Draper H.The functional significance of stereopsis. Investigative Ophthalmology & Visual Science 2010;51(4):2019-23. [DOI] [PubMed] [Google Scholar]
PEDIG 2002
- Pediatric Eye Disease Investigator Group.A randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Archives of Ophthalmology 2002;120(3):268-78. [DOI] [PubMed] [Google Scholar]
Piano 2019
- Piano ME, Simmers AJ.‘It’s too late’. Is it really? Considerations for amblyopia treatment in older children. Therapeutic Advances in Ophthalmology 2019;11:1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Polat 2004
- Polat U, Ma-Naim T, Belkin M, Sagi D.Improving vision in adult amblyopia by perceptual learning. Proceedings of the National Academy of Sciences of the United States of America 2004;101(17):6692-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Powell 2009
- Powell C, Hatt SR.Vision screening for amblyopia in childhood. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No: CD005020. [DOI: 10.1002/14651858.CD005020.pub3] [DOI] [PubMed] [Google Scholar]
Rahi 2002
- Rahi J, Logan S, Timms C, Russell-Eggitt I, Taylor D.Risk, causes, and outcomes of visual impairment after loss of vision in the non-amblyopic eye: a population-based study. Lancet 2002;360(9333):597-602. [DOI] [PubMed] [Google Scholar]
Rahi 2006
- Rahi JS, Cumberland PM, Peckham CS.Does amblyopia affect educational, health, and social outcomes? Findings from the 1958 British birth cohort. BMJ 2006;332(7545):820-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Repka 2003
- Repka MX, Beck RW, Holmes JM, Birch EE, Chandler DL, Cotter SA, et al.A randomized trial of patching regimens for treatment of moderate amblyopia in children. Archives of Ophthalmology 2003;121(5):603-11. [DOI] [PubMed] [Google Scholar]
Repka 2005
- Repka MX, Wallace DK, Beck RW, Kraker RT, Birch EE, Cotter SA, et al.Two-year follow-up of a 6-month randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Archives of Ophthalmology 2005;132(2):149-57. [DOI] [PubMed] [Google Scholar]
Repka 2009
- Repka MX, Kraker RT, Beck RW, Birch E, Cotter SA, Holmes JM, et al.Treatment of severe amblyopia with weekend atropine: results from 2 randomized clinical trials. Journal of AAPOS 2009;13(3):258-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Repka 2014
- Repka MX, Kraker RT, Holmes JM, Summers AI, Glaser SR, Barnhardt CN, et al.Atropine vs patching for treatment of moderate amblyopia: follow-up at 15 years of age of a randomized clinical trial. JAMA Ophthalmology 2014;132(7):799-805. [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2020 [Computer program]
- The Cochrane Collaboration Review Manager 5 (RevMan 5).Version 5.4. The Cochrane Collaboration, 2020.
Royal College of Ophthalmologists
- Guidelines for the Management of Strabismus in Childhood. The Royal College of Ophthalmologists March 2012;https://www.rcophth.ac.uk/wp-content/uploads/2014/12/2012-SCI-250-Guidelines-for-Management-of-Strabismus-in-Childhood-2012.pdf.
Sato 2008
- Sato M, Stryker MP.Distinctive features of adult ocular dominance plasticity. Journal of Neuroscience 2008;28(41):10278-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sauvan 2019
- Sauvan L, Stolowy N, Denis D, Matonti F, Chavane F, Hess RF, et al.Contribution of short-time occlusion of the amblyopic eye to a passive dichoptic video treatment for amblyopia beyond the critical period. Neural Plasticity 2019;2019:6208414. [DOI: 10.1155/2019/6208414] [DOI] [PMC free article] [PubMed] [Google Scholar]
Scheiman 2008
- Scheiman MM, Hertle RW, Kraker RT, Beck RW, Birch EE, Felius J, et al.Patching vs atropine to treat amblyopia in children aged 7 to 12 years: a randomized trial. Archives of Ophthalmology 2008;126(12):1634-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sengpiel 2006
- Sengpiel F, Jirmann KU, Vorobyov V, Eysel UT.Strabismic suppression is mediated by inhibitory interactions in the primary visual cortex. Cerebral Cortex 2006;16(12):1750-8. [DOI] [PubMed] [Google Scholar]
Sengpiel 2011
- Sengpiel F.Experimental models of amblyopia: insights for prevention and treatment. Strabismus 2011;19(3):87-90. [DOI] [PubMed] [Google Scholar]
Sharma 2000
- Sharma V, Levi DM, Klein SA.Undercounting features and missing features: evidence for a high-level deficit in strabismic amblyopia. Nature Neuroscience 2000;3(5):496-501. [DOI] [PubMed] [Google Scholar]
Simmers 2003
- Simmers AJ, Ledgeway T, Hess RF, McGraw PV.Deficits to global motion processing in human amblyopia. Vision Research 2003;43(6):729-38. [DOI] [PubMed] [Google Scholar]
Sinha 2008
- Sinha I, Jones L, Smyth RL, Williamson PR.A systematic review of studies that aim to determine which outcomes to measure in clinical trials in children. PLoS Medicine 2008;5(4):e96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Song 2014
- Song S, Levi DM, Pelli DG.A double dissociation of the acuity and crowding limits to letter identification, and the promise of improved visual screening. Journal of Vision 2014;14(5):3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Spiegel 2013a
- Spiegel DP, Byblow WD, Hess RF, Thompson B.Anodal transcranial direct current stimulation transiently improves contrast sensitivity and normalizes visual cortex activation in individuals with amblyopia. Neurorehabilitation and Neural Repair 2013;27(8):760-9. [DOI] [PubMed] [Google Scholar]
Spiegel 2013b
- Spiegel DP, Li J, Hess RF, Byblow WD, Deng D, Yu M, et al.Transcranial direct current stimulation enhances recovery of stereopsis in adults with amblyopia. Neurotherapeutics 2013;10(4):831-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stewart 2002
- Stewart CE, Fielder AR, Stephens DA, Moseley MJ.Design of the Monitored Occlusion Treatment of Amblyopia Study (MOTAS). British Journal of Ophthalmology 2002;86(8):915-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stewart 2004a
- Stewart CE, Moseley MJ, Stephens DA, Fielder AR.Treatment dose-response in amblyopia therapy: the Monitored Occlusion Treatment of Amblyopia Study (MOTAS). Investigative Ophthalmology & Visual Science 2004;45(9):3048-54. [DOI] [PubMed] [Google Scholar]
Stewart 2004b
- Stewart CE, Moseley MJ, Fielder AR, Stephens DA.Refractive adaptation in amblyopia: quantification of effect and implications for practice. British Journal of Ophthalmology 2004;88(12):1552-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stewart 2005
- Stewart CE, Fielder AR, Stephens DA, Moseley MJ.Treatment of unilateral amblyopia: factors influencing visual outcome. Investigative Ophthalmology & Visual Science 2005;46(9):3152-60. [DOI] [PubMed] [Google Scholar]
Stewart 2013
- Stewart CE, Wallace MP, Stephens DA, Fielder AR, Moseley MJ, MOTAS Cooperative.The effect of amblyopia treatment on stereoacuity. Journal of AAPOS 2013;17(2):166-73. [DOI] [PubMed] [Google Scholar]
Tailor 2016
- Tailor V, Bossi M, Greenwood JA, Dahlmann-Noor A.Childhood amblyopia: current management and new trends. British Medical Bulletin 2016;119(1):75-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tailor 2017
- Tailor VK, Schwarzkopf DS, Dahlmann-Noor AH.Neuroplasticity and amblyopia: vision at the balance point. Current Opinion in Neurology 2017;30(1):74-83. [DOI] [PubMed] [Google Scholar]
Taylor 2014
- Taylor K, Elliott S.Interventions for strabismic amblyopia. Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No: CD006461. [DOI: 10.1002/14651858.CD006461.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
To 2011
- To L, Thompson B, Blum JR, Maehara G, Hess RF, Cooperstock JR.A game platform for treatment of amblyopia. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2011;19(3):280-9. [DOI] [PubMed] [Google Scholar]
Vedamurthy 2015a
- Vedamurthy I, Nahum M, Bavelier D, Levi DM.Mechanisms of recovery of visual function in adult amblyopia through a tailored action video game. Scientific Reports 2015;5:8482. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vedamurthy 2015b
- Vedamurthy I, Nahum M, Huang SJ, Zheng F, Bayliss J, Bavelier D, et al.A dichoptic custom-made action video game as a treatment for adult amblyopia. Vision Research 2015;114:173-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
Victor 1994
- Victor JD, Purpura K, Katz E, Mao B.Population encoding of spatial frequency, orientation, and color in macaque V1. Journal of Neurophysiology 1994;72(5):2151-66. [DOI] [PubMed] [Google Scholar]
Vorobyov 2013
- Vorobyov V, Kwok JC, Fawcett JW, Sengpiel F.Effects of digesting chondroitin sulfate proteoglycans on plasticity in cat primary visual cortex. Journal of Neuroscience 2013;33(1):234-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Waddingham 2006
- Waddingham PE, Butler TK, Cobb SV, Moody AD, Comaish IF, Haworth SM, et al.Preliminary results from the use of the novel Interactive binocular treatment (I-BiT) system, in the treatment of strabismic and anisometropic amblyopia. Eye 2006;20(3):375-8. [DOI] [PubMed] [Google Scholar]
Wallace 2006
- Wallace DK, Edwards AR, Cotter SA, Beck RW, Arnold RW, Astle WF, et al.A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology 2006;113(6):904-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wallace 2011
- Wallace DK, Lazar EL, Melia M, Birch EE, Holmes JM, Hopkins KB, et al.Stereoacuity in children with anisometropic amblyopia. Journal of AAPOS 2011;15(5):455-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Webber 2008a
- Webber AL, Wood JM, Gole GA, Brown B.The effect of amblyopia on fine motor skills in children. Investigative Ophthalmology & Visual Science 2008;49(2):594-603. [DOI] [PubMed] [Google Scholar]
Webber 2008b
- Webber AL, Wood JM, Gole GA, Brown B.Effect of amblyopia on self-esteem in children. Optometry and Vision Science 2008;85(11):1074-81. [DOI] [PubMed] [Google Scholar]
White 2007
- White LE, Fitzpatrick D.Vision and cortical map development. Neuron 2007;56(2):327-38. [DOI] [PubMed] [Google Scholar]
Wiesel 1963
- Wiesel TN, Hubel DH.Single-cell responses in striate cortex of kittens deprived of vision in one eye. Journal of Neurophysiology 1963;26:1003-17. [DOI] [PubMed] [Google Scholar]
Xi 2014
- Xi J, Jia WL, Feng LX, Lu ZL, Huang CB.Perceptual learning improves stereoacuity in amblyopia. Investigative Ophthalmology & Visual Science 2014;55(4):2384-91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhang 2011
- Zhang B, Tao X, Wensveen JM, Harwerth RS, Smith EL 3rd, Chino YM.Effects of brief daily periods of unrestricted vision during early monocular form deprivation on development of visual area 2. Investigative Ophthalmology & Visual Science 2011;52(10):7222-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Tailor 2014
- Tailor V, Bossi M, Bunce C, Greenwood JA, Dahlmann-Noor A.Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years. Cochrane Database of Systematic Reviews 2014, Issue 11. Art. No: CD011347. [DOI: 10.1002/14651858.CD011347] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tailor 2015
- Tailor V, Ludden S, Bossi M, Bunce C, Greenwood JA, Dahlmann-Noor A.Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years. Cochrane Database of Systematic Reviews 2015, Issue 8. Art. No: CD011347. [DOI: 10.1002/14651858.CD011347.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]