

An intraluminal variant of endoscopic vacuum therapy (EVT) 1 2 was used in a case of acute spontaneous perforation of the esophagus. To enable simultaneous enteral nutrition, a double-lumen vacuum drainage with intestinal feeding tube was constructed.
A 31-year-old woman with the human immunodeficiency virus presented with thoracic pain and dysphagia after vomiting caused by a bolus of dry fish. Computed tomography revealed a perforation of the thoracic esophagus with discharge of air ( Fig. 1 ). Endoscopy found an acute transmural perforation from 26 cm to 31 cm ( Fig. 2 ). Intraluminal EVT 1 2 was started within 24 hours after the perforation event.
Fig. 1.

Thoracic computed tomography showing perforation (P) of the esophagus with extraluminal air next to the esophagus.
Fig. 2.

Endoscopy revealed a long perforation in the esophagus (arrows).
A triluminal tube (Freka Trelumina, CH/Fr 16/9, 150 cm; Fresenius Kabi AG, Bad Homburg, Germany) was used to construct a double-lumen vacuum drainage device ( Fig. 3 ). First, the ventilation channel of the tube was blocked with a clamp, as it was not required for the procedure. Then the tube was inserted nasally and guided out orally. All openings of the drainage channel were wrapped in a 15-cm length of open-pore polyurethane foam (Suprasorb CNP; Wundschaum, Lohmann & Rauscher GmbH & Co. KG, Neuwied, Germany), and secured with a suture. The double-lumen drainage device was then inserted endoscopically and the intestinal feeding channel was placed in the stomach. The open-pore polyurethane foam section of the tube covered the perforation region completely. After application of negative pressure with an electronic device (KCI V.A.C. Freedom; KCI USA Inc., San Antonio, Texas, USA; setting – 125 mmHg, continuous, intensity 10), the esophageal lumen collapsed around the foam.
Fig. 3.

Construction of the double-lumen vacuum drainage device. PU, polyurethane foam; S, suture; lP, lateral perforations of the gastric channel; IC, intestinal feeding channel of the tube.
Placement of the drainage device (and its removal after treatment) was performed using a standard gastroscope and carbon dioxide insufflation with the patient under general anesthesia. The patient was transferred to a normal ward immediately after drainage placement.
After EVT for 5 days, the drainage device was removed by pulling the tube. The foam had been sucked onto the perforation wound ( Fig. 4 ), which was closed and covered with an erosive pattern ( Fig. 5 ). No fistula could be observed. Three days after the end of therapy, a small ulceration could be seen at the site of the former perforation, and after 18 days, complete healing of the perforation region was achieved. In addition, an intramural esophageal pseudodiverticulosis ( Fig. 6 ) was detected as a possible explanation for the perforation.
Fig. 4.
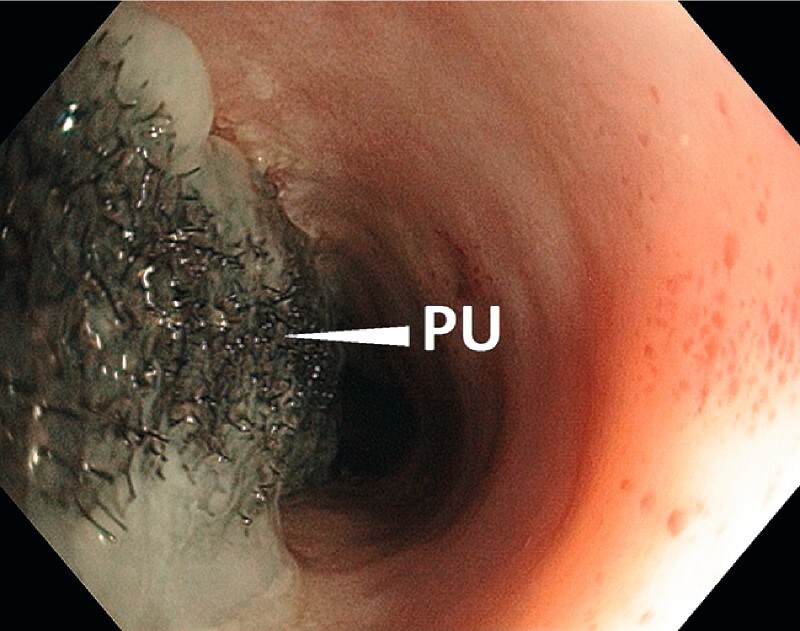
Day 5 of endoscopic vacuum therapy. The polyurethane foam (PU) had been sucked onto the perforation wound.
Fig. 5.
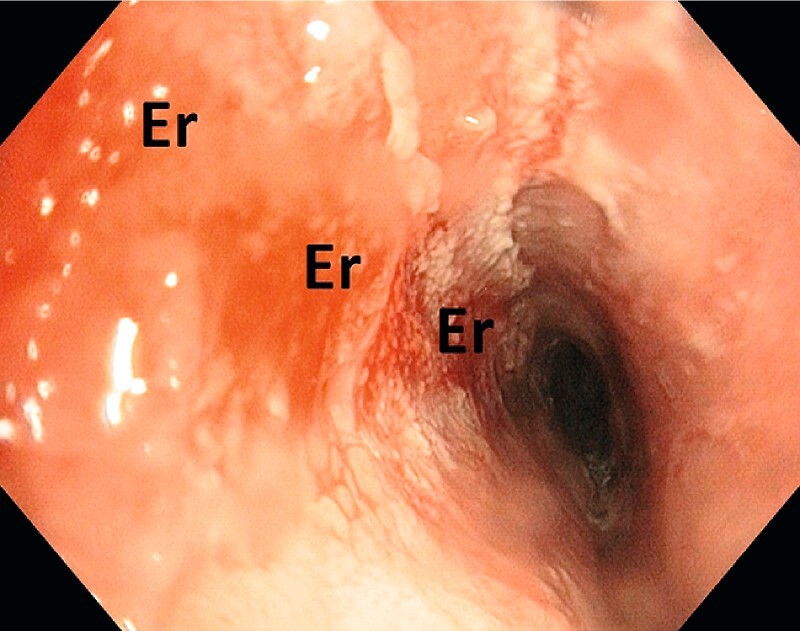
Day 5 of endoscopic vacuum therapy. Vacuum drainage was removed, revealing the former perforation site, which showed an erosion pattern (Er).
Fig. 6.

At follow-up endoscopy 18 days after treatment, complete healing was achieved and an esophageal pseudodiverticulosis was found.
Double-lumen vacuum drainage with intestinal feeding tube enabled full enteral nutrition from the beginning of esophageal intraluminal EVT ( Video 1 ).
Video 1: Endoscopic vacuum therapy for perforation of esophageal pseudodiverticulosis.
Endoscopy_UCTN_Code_TTT_1AO_2AI
Acknowledgment
We thank the nursing staff of the interdisciplinary endoscopic unit of Marienkrankenhaus Hamburg gGmbH for their excellent technical assistance. We thank the colleagues of Department of Anesthesiology, Intensive Care Medicine and Pain Therapy for their sedation. We thank the Institute of Diagnostic and Interventional Radiology of Marienkrankenhaus Hamburg gGmbH for providing the radiologic images.
Footnotes
Competing interests: G. Loske is a consultant for Lohmann & Rauscher GmbH & Co. KG.
References
- 1.Loske G, Schorsch T, Muller C. Intraluminal and intracavitary vacuum therapy for esophageal leakage: a new endoscopic minimally invasive approach. Endoscopy. 2011;43:540–544. doi: 10.1055/s-0030-1256345. [DOI] [PubMed] [Google Scholar]
- 2.Loske G, Schorsch T, Dahm C et al. Iatrogenic perforation of esophagus successfully treated with endoscopic vacuum therapy (EVT) Endosc Int Open. 2015;03:E547–E551. doi: 10.1055/s-0034-1392566. [DOI] [PMC free article] [PubMed] [Google Scholar]