

Abstract
Objective:
College campuses closed in March 2020 because of the COVID-19 pandemic, disrupting the lives of students. The goal of the present study was to examine whether cannabis use changed from before campus departures prompted by COVID-19 to after campus departures and after the semester ended—and if living situation explained observed changes. We also examined changes in specific formulations of cannabis and self-reported reasons for perceived changes in use frequency.
Method:
A sample of 223 college student cannabis users (61% female) from three universities completed two online surveys (one in May 2020 assessing cannabis use pre-campus closure [pre-closure] and since campus closed [post-closure-1], and another in September 2020 assessing cannabis use since remote classes ended [post-closure-2]).
Results:
Any use of cannabis and use of each specific formulation (leaf, edibles, concentrates) declined from pre-closure to post-closure-1, whereas the frequency of use did not change. Any cannabis use declined for those who stayed living dependently or moved to dependent living. Leaf use declined for all groups, concentrate use declined only for those who moved from independent to dependent living, and edible use declined only for those who stayed living dependently or moved to dependent living. Cannabis use did not change between post-closure-1 and post-closure-2, regardless of living situation stability or transition.
Conclusions:
Overall, among a sample of cannabis-using college students, the prevalence of any cannabis use, but not frequency of use, was reduced during the pandemic. Living with parents appears to be protective against frequent cannabis use.
In March 2020, many college campuses closed because of the COVID-19 pandemic. Although an increasing body of work has explored COVID-19–related changes in alcohol use in college students, research on COVID-19–related changes in cannabis use among college students has been limited. We examined changes in cannabis use from before campus departures to post-campus departures and after the end of the semester—as well as possible explanations for any changes.
There is mixed evidence regarding COVID-19–related changes in cannabis use. Across various populations, some studies have documented average decreases in prevalence (Dumas et al., 2020; Starks et al., 2020) or quantity and/or frequency of use (Bartel et al., 2020), or reductions in expected escalation of adolescent cannabis use prevalence (Leatherdale et al., 2021). Others showed increases in frequency/perceived frequency (Bonar et al., 2021; Cousijn et al., 2021; Dumas et al., 2020; Palamar et al., 2021) or increased frequency but not quantity (Benschop et al., 2021). Still others suggested no change (Graupensperger et al., 2021; Vanderbruggen et al., 2020). Research also suggests that there are subgroups of individuals who perceive their cannabis use has increased, decreased, or remained the same (Benschop et al., 2021; Leatherdale et al., 2021; Manthey et al., 2021). Thus far, research on COVID-19–related changes in cannabis use among college students has been conducted primarily outside the United States and is limited by the use of single time point surveys (Gritsenko et al., 2020; Yehudai et al., 2020). Importantly, evidence that cannabis use increased for some individuals and decreased for others (Manthey et al., 2021) raises the possibility that moderators of change in cannabis use are at play.
Living situation
A disruptive change that occurred for college students during the pandemic was related to living situation. There is strong evidence that living situation affects substance use (Stone et al., 2012). Whereas White et al. (2006) found both moving away from home and going to college were significantly related to increased alcohol use, neither was related to increased frequency of cannabis use. However, using national data, Gfroerer et al. (1997) found past-month cannabis use rates were highest among college students not living with parents. It is plausible that students’ cannabis use declines when they are forced to move from independent (alone or with peers) to dependent living situations (e.g., with parents) because of campus closures.
Other potential reasons for changes in cannabis use behavior
Motivational models (Cooper et al., 2016) suggest that substance use behavior is driven by desires to alleviate negative affect (coping), enhance positive affect, facilitate social interaction, and avoid social sanctions. Some of these reasons may also apply to why individuals changed their substance use during the pandemic. With respect to coping, given known impacts of the pandemic on stress and mental health (Elmer et al., 2020), students experiencing emotional distress may increase their use of cannabis to cope. Bartel et al. (2020) found youths who “always” used cannabis to cope with depression during the pandemic (relative to those who “never” did) had 31% higher cannabis use (i.e., product of self-reports of past-30-day cannabis use frequency [1–15 times/day] and typical quantity per single sitting [in grams]). Moreover, young adults who perceived an increase in their cannabis smoking (although not vaping or dabbing) were also more likely to report increased depression, anxiety, and stress (Bonar et al., 2021).
Other changes in context and accessibility of cannabis during the pandemic may also explain changes in cannabis use. Among college students, cannabis use typically occurs at parties and in small groups of friends (Beck et al., 2009; Buckner et al., 2012). Accordingly, cannabis use may have declined following campus closure in response to reduced social interaction. Yet, Bartel et al. (2020) found that youths who engaged in social isolation versus those who did not reported 20% more cannabis consumption. In the context of stay-at-home orders, students may also have had fewer sources for obtaining cannabis. Moreover, students who lost on- or off-campus jobs because of the pandemic may have had financial restraints on their ability to purchase cannabis. Additionally, reasons related to upbringing (e.g., family disapproval) (Epler et al., 2009) may have resulted in declines in cannabis use, particularly for students moving home with parents. Alternatively, a combination of remote coursework and suspension of extracurricular activities may have led to increased free time and boredom, resulting in increased use.
A handful of studies have focused on cannabis use motives during the pandemic. In a sample of U.S. young adults, Graupensperger et al. (2021) examined changes in cannabis use motives between January and April/May 2020. Boredom motives increased over time, whereas celebration motives decreased. In a sample of adolescents reporting past-year cannabis use, 27% endorsed using cannabis to cope with COVID-19–related changes (Leatherdale et al., 2021). In a large sample of mostly adolescents and young adults in the Netherlands (Benschop et al., 2021), the most strongly endorsed reason for current use among both those who increased and decreased cannabis use was “because I find it pleasant/fun/mind expanding,” but those who increased use more strongly endorsed reasons related to coping (e.g., “to feel less worried/afraid/angry/stressed”) relative to those who decreased. Note that motives for current use (and the way they change over time) may be distinct from more explicit reasons for changing (increasing or decreasing) use. In the only study thus far on reasons for COVID-19–related changes in cannabis use, self-reported reductions in use in adolescents were attributed to fewer opportunities for social interaction and decreased availability, and self-reported increases were attributed to more time, fewer responsibilities, and boredom (Chu et al., 2020). Whether similar reasons are cited among college students is yet unknown.
Cannabis formulations
Although use of cannabis flower or leaf remains most prevalent (Russell et al., 2018), use of other cannabis formulations is rapidly increasing (Goodman et al., 2020; Spindle et al., 2019). These include concentrates (e.g., oil, dabs) and edibles (e.g., cannabis-infused candies) (Daniulaityte et al., 2017; Knapp et al., 2019; Schauer et al., 2016; Steigerwald et al., 2018). Concentrates are associated with negative consequences, cannabis use disorder symptomology, and anxiety (Bidwell et al., 2018; Meier, 2017; Mokrysz et al., 2021). Additionally, edibles can produce unpredictable and extreme subjective effects (Barrus et al., 2016; Hudak et al., 2015; Vandrey et al., 2015).
Beyond COVID-19–related changes in any cannabis use, changes in the use of specific formulations are possible. Moving from independent living to home with parents may result in the selection of formulations such as edibles or concentrates that are easier to conceal and do not smell as strong (Morean et al., 2017). To date, research on whether and how use of specific cannabis formulations may have changed during COVID-19 has been limited. A single study was conducted among emerging adults enrolled in a randomized clinical trial targeting cannabis use and compared perceptions of past-30-day behavior (during the pandemic) to before the pandemic (Bonar et al., 2021). Smoking cannabis was perceived to have increased among 49% and decreased among 18% of respondents, vaporizing was perceived to have increased among 44% and decreased among 24%, dabbing was perceived to have increased among 37% and decreased among 28%, and eating cannabis was perceived to have increased among 36% and decreased among 20%. Whether similar findings emerge more specifically for college students during the transition off campus is unknown.
Present study
The current study extends our prior work on changes in alcohol consumption following COVID-related campus closures (Jackson et al., 2021; White et al., 2020) by examining changes in cannabis use from before being required to depart campus in the spring semester of 2020 (pre-closure) to following COVID-19–related departures from campus in the spring semester (post-closure-1) and during the summer months, beyond the end of remote classes (post-closure-2). We extended the growing literature on COVID-19 and substance use, being the first to examine the role of pandemic-related living situation changes on college student cannabis use and the second study to test effects of the pandemic on the use of specific cannabis formulations (Bonar et al., 2021), and by further examining reasons for perceived changes in use. In addition, in contrast to most previous studies that were cross-sectional, we collected longitudinal data post-closure over a 3-month period.
We hypothesized that, on average, students would decrease cannabis use from pre-closure to post-closure-1. We expected the change would be most pronounced for those who transitioned from living independently to dependently. Although we did not have hypotheses regarding the change between post-closure-1 and post-closure-2, we sought to explore the extent to which any initial changes in cannabis use were maintained or continued to change. We also explored changes in specific formulations and characterized self-reported reasons for perceived increases and decreases in cannabis use frequency to further contextualize changes in cannabis use.
Method
Design and sample
Participants were recruited from a study of simultaneous alcohol and cannabis use among college students. The larger study enrolled 1,390 18- to 24-year-old full-time students from three state universities who had used alcohol and cannabis in the past year and completed two online surveys in October 2017 and January 2018 (for details, see White et al., 2019). At the study's end, students were asked if they would like to be contacted for future studies. Those who agreed were invited in May 2020 to participate in a supplemental study about COVID-19 impacts. A total of 312 individuals (66% of those invited; 71% of the 439 with valid email addresses) completed the first of two surveys administered as a part of this study.1 This first survey (May 2020) asked to retrospectively report on the time before being required to depart campus because of COVID-19 in the spring semester 2020 (“pre-closure”) and following COVID-19–related departures from campus in the spring semester (“post-closure-1”). Of these 312 participants, 285 (91.3%) completed the second survey in September 2020. The second survey focused on the time since the end of remote classes (“post-closure-2”). Procedures were approved by the Brown University Institutional Review Board. Participants received a $25 gift card for each survey.
The current sample consisted of 223 participants (Table 1) who endorsed cannabis use during at least one of the three time points.2 The sample was 61% female, and the mean age was 21.26 years (SD = 0.83). The majority were either seniors (48%) or juniors (40%); 10% were no longer in school.3 The majority were White (63%), with 14% Asian, 5% Black, 8% another race, and 9% bi- or multiracial; 12% were Hispanic/Latinx.
Table 1.
Descriptives across pre-closure, post-closure-1, and post-closure-2 (N = 223)

| Variable | Pre-closure n (%)or M (SD) | Post-closure-1 n (%) or M (SD) | Post-closure-2 n (%) or M (SD) | ICCa |
|---|---|---|---|---|
| Any cannabis use | 193 (87%) | 170 (76%) | 170 (78%) | .34 |
| Leaf | 171 (77%) | 129 (58%) | 124 (57%) | .46 |
| Concentrates | 92 (41%) | 78 (35%) | 81 (36%) | .66 |
| Edibles | 106 (48%) | 75 (34%) | 79 (35%) | .40 |
| Cannabis days/week | 3.06 (2.88) | 3.12 (3.05) | 3.00 (2.96) | .71 |
| 0 | 61 (28%) | 78 (36%) | 77 (35%) | |
| 1-2 | 62 (28%) | 38 (17%) | 40(18%) | |
| 3 | 19 (9%) | 10 (5%) | 16(7%) | |
| 4-6 | 14 (6%) | 19 (9%) | 21 (10%) | |
| 7 | 66 (30%) | 73 (33%) | 64 (29%) | |
| Living independently School | 191 (86%) | 104 (47%) | 102 (46%) | |
| A | 62 (27.8%) | |||
| B | 63 (28.3%) | |||
| C | 57 (25.6%) | |||
| Other | 18(8.1%) | |||
| No longer in school | 23 (10.3%) | |||
| Recreational cannabis legal in state | 98 (44%) |
Notes: ICC = Intraclass correlation. Valid percentages of sample are shown in context of missing data.
ICCs represent the amount of between-person variance in each outcome. For example, 34% of the variability in any cannabis use occurs at the between-person level.
Measures
Cannabis use
Participants were asked whether they used cannabis in the time frame of interest (i.e., pre-closure: before campus closed; post-closure-1: since campus closed; post-closure-2: since remote classes ended) and marked each form of cannabis used, yielding four dichotomous variables (any vs. no use of any cannabis, leaf, concentrates, edibles) for each time point. They also completed an adapted version of the Daily Drinking Questionnaire (Collins et al., 1985) for cannabis use, allowing calculation of total days using cannabis during a typical week at each time point.4
Living situation
Participants were asked where they lived at each time point. Response options were recoded to represent living “independently” (dormitory/residence hall, fraternity/sorority house, apartment/house with friend(s)/roommate(s)/partner, apartment/house where I live alone) versus “dependently” (apartment/house with parent(s), apartment/house with friend's family). We created a set of dummy-coded variables to represent the transition in living situation (independent vs. dependent) across the three time points.5 Participants also self-reported their current state of residence post-closure-1, and when missing (n = 11) we used state from post-closure-2. Each state was coded for whether recreational cannabis was legal at the time of data collection (i.e., post-closure; 0 = not legal, 1 = legal).
Reasons for perceived change in cannabis use frequency
Participants were asked whether their cannabis use frequency had decreased, remained the same, or increased since campus closed (pre-closure to post-closure-1). We assessed reasons for the change (check all that apply) upon reporting a decrease (context, access/opportunity, and upbringing) or increase (context, access/opportunity, and coping with distress). A checklist of reasons was developed by the authors (Jackson et al., 2021) with options based on literature on motives for substance use (Cooper et al., 2016), reasons for limiting or abstaining from drinking (Epler et al., 2009), and COVID-19 (Acuff et al., 2020).
Analytic plan
Primary outcomes were (a) any cannabis use at each time point (binomial) and (b) the number of cannabis use days per typical week (ordinal). Secondary outcomes included the use of specific cannabis formulations (binomial): leaf, concentrates, and edibles. Hierarchical linear models (HLMs) were run in the HLM 7.01 program for the binomial outcomes (Raudenbush et al., 2013) and in SAS PROC GLIMMIX (SAS Institute Inc., 2012) for the ordinal outcome. Missing data on Level 1 outcomes were minimal (n = 2 at pre-closure, n = 18 at post-closure-1, n = 5 at post-closure-2) and were handled in HLM with full maximum likelihood estimation and in SAS with Laplace approximation.
With data from three time points, we created two dummy-coded time components (change from pre-closure to post-closure-1, coded 0, 1, 1; change from post-closure-1 to post-closure-2, coded 0, 0, 1), entered into Level 1 of the model to construct a piecewise model of change. First, we examined the change in each of the five outcomes between time points, without entering predictors of the slopes. Next, we added Level-2 variables related to the change in living situation. Specifically, dummy-coded Level-2 variables representing each individual's change in living situation between pre-closure and post-closure-1 were entered as predictors of both the model intercept and the slope for pre-closure to post-closure-1 change. In addition, variables representing the change in living situation between post-closure-1 and post-closure-2 were entered as predictors of both the model intercept and the slope for post-closure-1 to post-closure-2 change. The referent group was changed systematically to test the effects of each living situation change; tables show “simple effects” for each group. In all models, Level-2 (person-level) covariates included age, sex, school pre-closure, and whether cannabis was legal in the participants’ post-closure state of residence.6
Results
Change in cannabis use over time
Controlling for sex, age, school, and state legalization, the likelihood of any cannabis use decreased between pre-closure and post-closure-1, as did the use of leaf, concentrates, and edibles (Table 2). Days using cannabis during a typical week did not significantly change on average. There were no changes in outcomes between post-closure-1 and post-closure-2.
Table 2.
Change in cannabis use behavior over time (N = 223)

| Variable | Change from pre-closure to post-closure-1 | Change from post-closure-1 to post-closure-2 | ||||||
|---|---|---|---|---|---|---|---|---|
| B | OR | [95% CI] | P | B | OR | [95% CI] | P | |
| Any use | −0.77 | 0.46 | [0.28, 0.74] | .001 | 0.07 | 1.08 | [0.74, 1.58] | .702 |
| Days using | −0.09 | 0.91 | [0.60, 1.38] | .658 | −0.14 | 0.87 | [0.57, 1.33] | .523 |
| Leaf | −1.06 | 0.35 | [0.24, 0.51] | <.001 | −0.11 | 0.90 | [0.64, 1.26] | .530 |
| Concentrates | −0.35 | 0.70 | [0.51, 0.98] | .036 | 0.10 | 1.11 | [0.78, 1.57] | .563 |
| Edibles | −0.68 | 0.51 | [0.37, 0.69] | <.001 | 0.11 | 1.11 | [0.76, 1.64] | .579 |
Notes: OR = odds ratio; CI = confidence interval. Results come from a separate model for each outcome, each of which included covariates for age, sex, school pre-closure, and whether cannabis was legal in participants’ post-closure-1 state of residence.
Living situation changes
Cannabis use and frequency
For those who lived dependently over time or moved from living independently to dependently, endorsement of any cannabis use significantly declined between pre-closure and post-closure-1 (Table 3). Prevalence of any cannabis use did not change between post-closure-1 and post-closure-2 regardless of living situation change. There was no effect of living situation change on cannabis frequency.
Table 3.
Hierarchical linear models predicting change in any cannabis use and number of days using cannabis from pre-closure to post-closure-1 and from post-closure-1 to post-closure-2 (N = 223)

| Variable | Change in any cannabis use | Change in cannabis use days | ||||||
|---|---|---|---|---|---|---|---|---|
| B | OR | [95% CI] | P | B | OR | [95% CI] | P | |
| Residential change from pre-closure to post-closure-1 | ||||||||
| Stayed dependent | −1.22 | 0.30 | [0.09,1.00] | .049 | 0.30 | 1.34 | [0.61, 2.94] | .459 |
| Stayed independent | −0.44 | 0.64 | [0.33, 1.27] | .200 | 0.36 | 1.44 | [0.81, 2.57] | .218 |
| Moved to dependent | −0.87 | 0.42 | [0.23, 0.78] | .006 | −0.41 | 0.66 | [0.37, 1.16] | .148 |
| Residential change from post-closure-1 to post-closure-2 | ||||||||
| Stayed dependent | 0.25 | 1.28 | [0.73, 2.26] | .385 | 0.12 | 1.13 | [0.60, 2.15] | .706 |
| Stayed independent | 0.12 | 1.13 | [0.67, 1.88] | .650 | 0.05 | 1.05 | [0.63, 1.75] | .844 |
| Moved to dependent | 0.15 | 1.17 | [0.66, 2.06] | .593 | −0.26 | 0.77 | [0.41, 1.45] | .416 |
| Moved to independent | 0.19 | 1.21 | [0.68, 2.15] | .514 | −0.09 | 0.92 | [0.49, 1.73] | .792 |
| Covariatesa | ||||||||
| Sex (ref. = male) | −0.19 | 0.83 | [0.51, 1.37] | .457 | −0.19 | 0.83 | [0.36, 1.93] | .664 |
| Age | −0.02 | 0.98 | [0.74, 1.29] | .882 | −0.20 | 0.82 | [0.49, 1.37] | .442 |
| School A (ref. = not in school) | −0.75 | 0.47 | [0.13, 1.78] | .268 | −1.09 | 0.34 | [0.04, 2.92] | .322 |
| School B (ref. = not in school) | 0.23 | 1.26 | [0.36, 4.43] | .713 | 1.37 | 3.93 | [0.54, 28.91] | .177 |
| School C (ref. = not in school) | −0.13 | 0.88 | [0.31, 2.52] | .806 | −0.75 | 0.47 | [0.10, 2.19] | .337 |
| Other school (ref. = not in school) | −0.58 | 0.56 | [0.16, 1.94] | .357 | −0.54 | 0.58 | [0.08, 4.51] | .601 |
| Cannabis legalization (ref. = no) | −0.18 | 0.83 | [0.37, 1.90] | .665 | −0.09 | 0.91 | [0.19, 4.37] | .907 |
Notes: Bolded effects represent p < .05. Results come from separate models in which the referent group was switched to obtain group-specific effects. OR = odds ratio; CI = confidence interval; ref. = referent group. Although not tabled for parsimony, models also included each Level 2 variable that was entered as a predictor of a Level 1 slope effect (i.e., dummy codes for change in living situation) as an additional predictor of the model intercept, to appropriately test the cross-level interactions.
Effects of covariates are presented from the model in which Stayed Dependent was the referent group, but remained nonsignificant across all models.
Cannabis formulations
Endorsement of leaf declined between pre-closure and post-closure-1, regardless of living situation stability or change (Table 4). Concentrate use significantly declined only among those who moved from independent to dependent living. Finally, endorsement of edibles significantly declined between pre-closure and post-closure-1 for those living dependently across time or those who moved from independent to dependent living and marginally decreased among those living independently across time.
Table 4.
Hierarchical linear models predicting change in use of each cannabis formulation (N = 223)

| Variable | Change in leaf | Change in concentrates | Change in edibles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | OR | [95% CI] | P | B | OR | [95% CI] | P | B | OR | [95% CI] | P | |
| Residential change from pre-closure to post-closure-1 | ||||||||||||
| Stayed dependent | −1.22 | 0.30 | [0.15, 0.59] | <.001 | −0.17 | 0.85 | [0.47, 1.54] | .585 | −0.94 | 0.40 | [0.21, 0.76] | .004 |
| Stayed independent | −0.79 | 0.46 | [0.28, 0.75] | .002 | −0.25 | 0.78 | [0.50, 1.22] | .275 | −0.39 | 0.67 | [0.45, 1.00] | .052 |
| Moved to dependent | −1.35 | 0.26 | [0.15, 0.45] | <.001 | −0.66 | 0.52 | [0.32, 0.83] | .007 | −0.81 | 0.44 | [0.28, 0.70] | <.001 |
| Residential change from post-closure-1 to post-closure-2 | ||||||||||||
| Stayed dependent | 0.34 | 1.40 | [0.87, 2.26] | .164 | 0.23 | 1.26 | [0.75, 2.12] | .384 | 0.45 | 1.56 | [0.85, 2.88] | .154 |
| Stayed independent | −0.05 | 0.95 | [0.62, 1.46] | .806 | 0.16 | 1.18 | [0.74, 1.88] | .497 | 0.25 | 1.29 | [0.80, 2.13] | .323 |
| Moved to dependent | 0.03 | 1.03 | [0.61, 1.74] | .924 | 0.36 | 1.43 | [0.77, 2.64] | .255 | 0.29 | 1.33 | [0.71, 2.51] | .374 |
| Moved to independent | 0.14 | 1.15 | [0.68, 1.97] | .602 | 0.35 | 1.42 | [0.84, 2.39] | .189 | 0.50 | 1.66 | [0.89, 3.09] | .113 |
| Covariatesa | ||||||||||||
| Sex (ref. = male) | −0.16 | 0.85 | [0.50, 1.44] | .547 | 0.15 | 1.17 | [0.67, 2.05] | .589 | 0.13 | 1.10 | [0.69, 1.73] | .585 |
| Age | −0.25 | 0.78 | [0.56, 1.10] | .152 | 0.00 | 1.00 | [0.71, 1.43] | .987 | 0.19 | 1.20 | [0.92, 1.57] | .153 |
| School A (ref. = not in school) | −0.02 | 0.984 | [0.32, 3.06] | .978 | −0.91 | 0.40 | [0.09, 1.79] | .230 | −1.26 | 0.28 | [0.09, 0.87] | .028 |
| School B (ref. = not in school) | 0.95 | 2.58 | [0.89, 7.53] | .081 | −0.15 | 0.86 | [0.21, 3.58] | .839 | −0.28 | 0.76 | [0.27, 2.15] | .602 |
| School C (ref. = not in school) | 0.06 | 1.06 | [0.41, 2.75] | .909 | −0.20 | 0.82 | [0.26, 2.61] | .737 | −0.41 | 0.66 | [0.30, 1.47] | .308 |
| Other (ref. = not in school) | −0.16 | 0.85 | [0.26, 2.81] | .788 | −0.49 | 0.61 | [0.15, 2.53] | .494 | −0.66 | 0.52 | [0.16, 1.65] | .264 |
| Cannabis legalization (ref. = no) | −0.29 | 0.75 | [0.34, 1.66] | .474 | −0.18 | 0.83 | [0.29, 2.39] | .734 | −0.03 | 0.97 | [0.00, 16.17] | .940 |
Notes: Bolded effects represent p < .05. OR = odds ratio; CI = confidence interval; ref. = referent group. Although not tabled for parsimony, models also included each Level 2 variable that was entered as a predictor of Level 1 slope effects (i.e., dummy codes for change in living situation) as an additional predictor of the model intercept, to appropriately test the cross-level interactions.
Effects of covariates are presented from the model in which Stayed Dependent was the referent group, but remained non-significant across all models.
Reasons for change
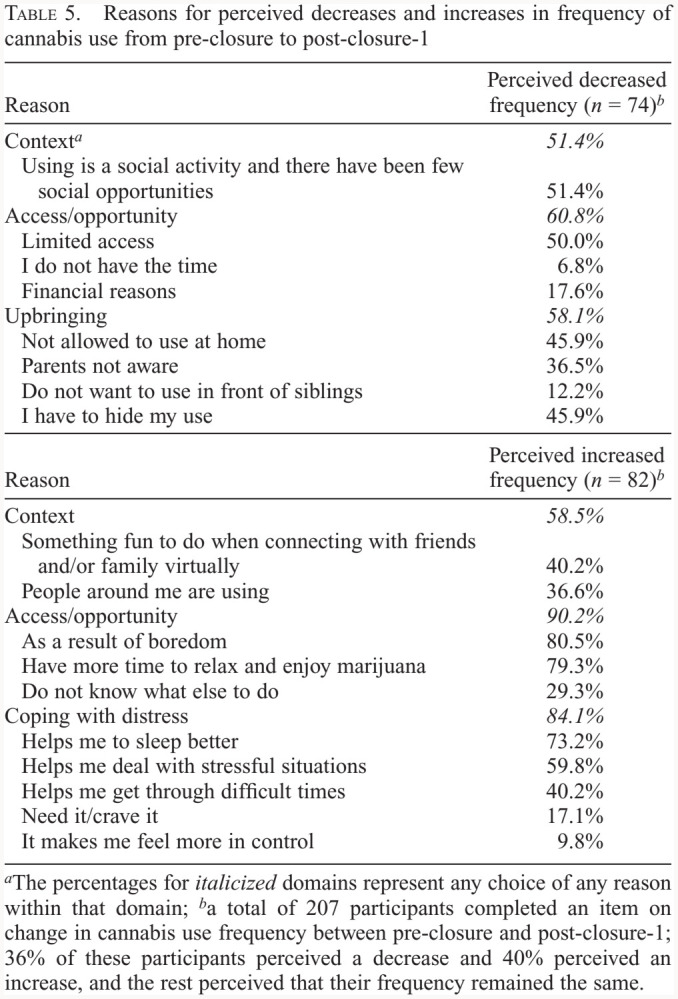
Among those who perceived a decrease in cannabis use frequency from pre-closure to post-closure-1, the most common self-reported reason was a lack of social opportunities (Table 5). Limited access was another prominent reason for a decrease. Within the category of upbringing, not being allowed to use at home or having to hide cannabis use were common reasons for self-reported declines in frequency.
Table 5.
Reasons for perceived decreases and increases in frequency of cannabis use from pre-closure to post-closure-1
| Reason | Perceived decreased frequency (n = 74)b |
|---|---|
| Contexta | 51.4% |
| Using is a social activity and there have been few social opportunities | 51.4% |
| Access/opportunity | 60.8% |
| Limited access | 50.0% |
| I do not have the time | 6.8% |
| Financial reasons | 17.6% |
| Upbringing | 58.1% |
| Not allowed to use at home | 45.9% |
| Parents not aware | 36.5% |
| Do not want to use in front of siblings | 12.2% |
| I have to hide my use | 45.9% |
| Reason | Perceived increased frequency (n = 82)b |
| Context | 58.5% |
| Something fun to do when connecting with friends and/or family virtually | 40.2% |
| People around me are using | 36.6% |
| Access/opportunity | 90.2% |
| As a result of boredom | 80.5% |
| Have more time to relax and enjoy marijuana | 79.3% |
| Do not know what else to do | 29.3% |
| Coping with distress | 84.1% |
| Helps me to sleep better | 73.2% |
| Helps me deal with stressful situations | 59.8% |
| Helps me get through difficult times | 40.2% |
| Need it/crave it | 17.1% |
| It makes me feel more in control | 9.8% |
The percentages for italicized domains represent any choice of any reason within that domain;
a total of 207 participants completed an item on change in cannabis use frequency between pre-closure and post-closure-1; 36% of these participants perceived a decrease and 40% perceived an increase, and the rest perceived that their frequency remained the same.
Among those who perceived an increase in their cannabis use frequency, greater access and opportunity were prevalent explanations (Table 5). Many also endorsed boredom and/or more time to relax and enjoy cannabis. The majority of the sample who reported increases in use endorsed at least one coping-related reason (e.g., deal with stress).
Discussion
This was among the first studies to examine the change in cannabis use behavior, including use of specific formulations, across key transitional time points for college students forced to move from on-campus to remote learning during COVID-19, and to identify factors explaining observed behavioral changes. On average, there were declines following campus closures in any use of cannabis (12% reduction) and formulation-specific use of leaf (25% reduction), edibles (29%), and concentrates (15%). However, frequency (days per week) did not change across time. Observed changes were only evident at the point of COVID-19–related campus closures and not following the end of remote classes. Importantly, findings were qualified by transitions in living situation. As hypothesized, among those moving from independent to dependent living following campus closure, we observed a decline in the use of any cannabis, as well as the use of each specific formulation of cannabis. As dependent living was typically characterized by living with parents, findings are consistent with prior work suggesting that continued parental involvement, including living with parents, may serve a protective role in substance use (e.g., Abar & Turrisi, 2008; White et al., 2006).
Yet, declines in cannabis use were evident following campus closures even among those who did not change living situation, with reductions in the use of any cannabis as well as the use of leaf and edibles among those who lived dependently at both time points. There was little reduction in use among those who lived independently at both time points other than for leaf specifically. The use of concentrates did not decline for either group who maintained their living situation, and displayed the overall lowest rate of reduction. One possibility is that leaf and edibles were previously used in more social settings, outside of one's own or parents’ home, and that these opportunities were no longer available. Alternatively, the use of concentrates may be easier to conceal (Morean et al., 2017), whether or not students are living with parents. Although edibles may also be concealable, they may have been more difficult to make and/or obtain, especially while living at home.
Our sample of cannabis users retained their degree of use in spite of the pandemic. That is, despite changes in endorsement of use of any cannabis, frequency did not change over time, regardless of living situation stability or change. This is in contrast to findings from a study of Canadian adolescents (ages 14–19 years) demonstrating increased frequency (Dumas et al., 2020). Most of the variance in frequency of use was attributable to how people differed from one another (between-person vs. within-person change), with about one third of our sample being daily users at each time point.
Although our analyses did not reveal average changes in cannabis use frequency, similar percentages of participants perceived an increase (40%) versus a decrease (36%) in their cannabis use frequency between pre-closure and post-closure-1. Potential moderators not examined here might explain why some students began to use more often while others used less often. Our exploration of self-identified reasons for perceived change in frequency also provides some insight into this notion. A lack of social opportunities was the most common perceived reason for decreases in frequency, and limited access was also a prominent reason. In line with our findings for the impact of moving home with parents, not being allowed to use at home or having to hide use following campus closure were common reasons for perceived declines in frequency. Among those who perceived an increase in frequency, boredom and/or having more time to relax and enjoy cannabis were common explanations. Additionally, coping-related reasons (e.g., as a sleep aid, to deal with stress) were prevalent. Of note, we were unable to assess reasons for decreased or increased frequency among all participants who displayed a change in their quantitatively assessed days of use because reasons were only assessed when a change was perceived by the respondent. Future research that explores reasons for increased versus decreased use in response to major lifestyle changes, such as those provoked by the pandemic, is warranted.
Limitations
Our findings should be interpreted in the context of study limitations. Our sample included present or former college students from three state universities who were previously enrolled in a substance use study and agreed to be re-contacted; thus we cannot generalize to all young adults. In addition, all participants in the parent study from which our sample was recruited were required to report past-year cannabis use at recruitment. Although a subset of the present study sample (28%) did not use cannabis during the pre-closure timeframe, the extent to which individuals who had no prior cannabis use experience began to use during COVID-19 cannot be determined with our data. Data for pre-closure and post-closure-1 were both assessed in the May 2020 survey (i.e., cross-sectionally) to capture the effects of the pandemic on substance use behavior while also gathering information about their behavior before the pandemic as a comparator. As such, we relied on recall of cannabis use behavior before campus-related departures and can only provide insight into very specific points in time during the pandemic. Finally, pre-COVID cannabis use was not framed within a specific time; rather, participants were asked whether they used cannabis “at all” before campus closure. As such, declines in any cannabis use between pre-closure and post-closure-1 may be biased to appear larger than if a more specific timeframe had been used.
Conclusions
Overall, findings document declines in the prevalence of cannabis use of all formulations among college students who were required to leave campus during COVID-19. We also found evidence that changes in living situation were, in part, responsible for these declines; moving away from living independently to living with parents served as a protective factor. Although the changes prompted by COVID-19 were disruptive for students, declines in cannabis use prevalence represent a positive byproduct of the pandemic on health behavior at a time when health (and lack thereof) was on the minds of many. That college students should live at home while in college to protect against risky substance use behaviors may not be feasible; however, findings suggest an important role of living situation in understanding the reasons for change in cannabis use over time, likely even outside of the context of a pandemic.
Footnotes
The writing of this article was supported by National Institute on Drug Abuse Grant R01 DA040880 (multiple principal investigators: Kristina M. Jackson and Helene R. White) and training support for Angela K. Stevens (Grant T32 DA016184, principal investigator: Damaris J. Rohsenow). Points of view in this document are those of the authors and do not necessarily represent the official position or policies of the National Institutes of Health.
The funding sources had no role in the analysis or interpretation of the data, the preparation of this manuscript, or the decision to submit the manuscript for publication.
Angela K. Stevens died August 1, 2021.
Only Wave 1 first- and second-year students (n = 634) were invited because, assuming they matriculated as expected, they would still be in college (as juniors and seniors) in spring 2020; 473 of 634 (75%) students agreed to be re-contacted and were invited to participate in the COVID study. The 312 who agreed to participate did not differ significantly from the 161 who were invited but did not respond in terms of demographic characteristics (i.e., sex, age, year in school, race, ethnicity, school attended, and free lunch while growing up) or past-3-month alcohol or cannabis use frequency collected at Wave 1 of the original study.
Of the original 285 who completed both COVID surveys, 50 were excluded because they did not endorse use of cannabis at any of the three time points examined (pre-closure, post-closure-1, post-closure-2), 9 were excluded because they did not have data on key variables needed for analysis (i.e., change in living situation or state), and 3 were dropped because of a small group size (change between living dependently to independently between pre-closure and post-closure-1).
Although 10% of the participants were no longer in college, we treat the sample as a college sample given that they all had been enrolled full-time at the time of the parent study.
This measure was not normally distributed and was recoded into a 5-point categorical variable for substantive analyses (0 days = 0, 1–2 days = 1, 3 days = 2, 4–6 days = 3, and 7 days = 4). We considered alternative ordinal coding schemes for this variable. We analyzed data with a four-category variable (0 days = 0, 1–2 days = 1, 3–6 days = 2, and 7 days = 3) and with a three-category variable (0 days = 0, 1–6 days = 1, and 7 days = 2). Findings were robust and changed minimally with respect to directions of effect and statistical significance. Thus, we proceeded with the five-category variable to maximize the variance in the outcome.
Regarding transitions between pre-closure and post-closure-1, 87 participants (39%) went from living independently to dependently; 3 who went from living dependently to independently between these time points were dropped because of the small size of this group. Regarding transitions between post-closure-1 and post-closure-2, 30 participants (14%) went from independent to dependent, whereas 28 (13%) went from dependent to independent.
We also considered the state response to COVID-19 as a potential covariate, but all participants lived in states that responded early to the pandemic (i.e., before April 1, 2020).
References
- Abar C., Turrisi R. How important are parents during the college years? A longitudinal perspective of indirect influences parents yield on their college teens’ alcohol use. Addictive Behaviors. 2008;33:1360–1368. doi: 10.1016/j.addbeh.2008.06.010. doi:10.1016/j.addbeh.2008.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Acuff S. F., Tucker J. A., Murphy J. G. Behavioral economics of substance use: Understanding and reducing harmful use during the COVID-19 pandemic. Experimental and Clinical Psychopharmacology. Advance online publication. 2020 doi: 10.1037/pha0000431. doi:10.1037/pha0000431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrus D. G., Capogrossi K. L., Cates S. C., Gourdet C. K., Peiper N. C., Novak S. P., Wiley J. L. RTI Press Publication No. OP-0035-1611; Research Triangle Park, NC: RTI Press; 2016. Tasty THC: Promises and challenges of cannabis edibles. doi:10.3768/rtipress.2016.op.0035.1611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartel S. J., Sherry S. B., Stewart S. H. Self-isolation: A significant contributor to cannabis use during the COVID-19 pandemic. Substance Abuse. 2020;41:409–412. doi: 10.1080/08897077.2020.1823550. doi:10.1080/08897077.2020.1823550. [DOI] [PubMed] [Google Scholar]
- Beck K. H., Caldeira K. M., Vincent K. B., O’Grady K. E., Wish E. D., Arria A. M. The social context of cannabis use: Relationship to cannabis use disorders and depressive symptoms among college students. Addictive Behaviors. 2009;34:764–768. doi: 10.1016/j.addbeh.2009.05.001. doi:10.1016/j.addbeh.2009.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benschop A., van Bakkum F., Noijen J. Changing patterns of substance use during the coronavirus pandemic: Self-reported use of tobacco, alcohol, cannabis, and other drugs. Frontiers in Psychiatry. 2021;12:633551. doi: 10.3389/fpsyt.2021.633551. doi:10.3389/fpsyt.2021.633551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bidwell L. C., YorkWilliams S. L., Mueller R. L., Bryan A. D., Hutchison K. E. Exploring cannabis concentrates on the legal market: User profiles, product strength, and health-related outcomes. Addictive Behaviors Reports. 2018;8:102–106. doi: 10.1016/j.abrep.2018.08.004. doi:10.1016/j.abrep.2018.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonar E. E., Chapman L., McAfee J., Goldstick J. E., Bauermeister J. A., Carter P. M., Walton M. A. Perceived impacts of the COVID-19 pandemic on cannabis-using emerging adults. Translational Behavioral Medicine. 2021;11:1299–1309. doi: 10.1093/tbm/ibab025. doi:10.1093/tbm/ibab025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckner J. D., Crosby R. D., Silgado J., Wonderlich S. A., Schmidt N. B. Immediate antecedents of marijuana use: An analysis from ecological momentary assessment. Journal of Behavior Therapy and Experimental Psychiatry. 2012;43:647–655. doi: 10.1016/j.jbtep.2011.09.010. doi:10.1016/j.jbtep.2011.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chu L.-H., Wallace E. C., Jaffe A. E., Ramirez J. J. Changes in late adolescent marijuana use during the covid-19 outbreak vary as a function of typical use. Poster presented at the Research Society on Marijuana 4th Annual Meeting (Virtual) 2020 July 24; [Google Scholar]
- Collins R. L., Parks G. A., Marlatt G. A. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53:189–200. doi: 10.1037//0022-006x.53.2.189. doi:10.1037/0022-006X.53.2.189. [DOI] [PubMed] [Google Scholar]
- Cooper M. L., Kuntsche E., Levitt A., Barber L. L., Wolf S.2016Motivational models of substance use: A review of theory and research on motives for using alcohol, marijuana, and tobacco In The Oxford handbook of substance use and substance use disorders1pp. 375–421.New York, NY: Oxford University Press [Google Scholar]
- Cousijn J., Kuhns L., Larsen H., Kroon E. For better or for worse? A pre-post exploration of the impact of the COVID-19 lockdown on cannabis users. Addiction. 2021;116:2104–2115. doi: 10.1111/add.15387. doi:10.1111/add.15387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniulaityte R., Lamy F. R., Barratt M., Nahhas R. W., Martins S. S., Boyer E. W., Carlson R. G. Characterizing marijuana concentrate users: A web-based survey. Drug and Alcohol Dependence. 2017;178:399–407. doi: 10.1016/j.drugalcdep.2017.05.034. doi:10.1016/j.drugalcdep.2017.05.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dumas T. M., Ellis W., Litt D. M. What does adolescent substance use look like during the Covid-19 pandemic? Examining changes in frequency, social contexts, and pandemic-related predictors. Journal of Adolescent Health. 2020;67:354–361. doi: 10.1016/j.jadohealth.2020.06.018. doi:10.1016/j.jadohealth.2020.06.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elmer T., Mepham K., Stadtfeld C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS One. 2020;15:e0236337. doi: 10.1371/journal.pone.0236337. doi:10.1371/journal.pone.0236337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epler A. J., Sher K. J., Piasecki T. M. Reasons for abstaining or limiting drinking: A developmental perspective. Psychology of Addictive Behaviors. 2009;23:428–442. doi: 10.1037/a0015879. doi:10.1037/a0015879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gfroerer J. C., Greenblatt J. C., Wright D. A. Substance use in the US college-age population: Differences according to educational status and living arrangement. American Journal of Public Health. 1997;87:62–65. doi: 10.2105/ajph.87.1.62. doi:10.2105/AJPH.87.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman S., Wadsworth E., Leos-Toro C., Hammond D., & the International Cannabis Policy Study Team 2020Prevalence and forms of cannabis use in legal vs. illegal recreational cannabis markets International Journal on Drug Policy 76102658.doi:10.1016/j.drugpo.2019.102658 [DOI] [PubMed] [Google Scholar]
- Graupensperger S., Fleming C. B., Jaffe A. E., Rhew I. C., Patrick M. E., Lee C. M. Changes in young adults’ alcohol and marijuana use, norms, and motives from before to during the COVID-19 pandemic. Journal of Adolescent Health. 2021;68:658–665. doi: 10.1016/j.jadohealth.2021.01.008. doi:10.1016/j.jadohealth.2021.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gritsenko V., Skugarevsky O., Konstantinov V., Khamenka N., Marinova T., Reznik A., Isralowitz R.COVID 19 Fear, stress, anxiety, and substance use among Russian and Belarusian university students. International Journal of Mental Health and Addiction. Advance online publication. 2020. May 21, doi:10.1007/s11469-020-00330-z. [DOI] [PMC free article] [PubMed]
- Hudak M., Severn D., Nordstrom K. Edible cannabis–induced psychosis: Intoxication and beyond. American Journal of Psychiatry. 2015;172:911–912. doi: 10.1176/appi.ajp.2015.15030358. doi:10.1176/appi.ajp.2015.15030358. [DOI] [PubMed] [Google Scholar]
- Jackson K. M., Merrill J. E., Stevens A. K., Hayes K. L., White H. R. Changes in alcohol use and drinking context due to the COVID-19 pandemic: A multimethod study of college students. Alcoholism: Clinical and Experimental Research. 2021;45:752–764. doi: 10.1111/acer.14574. doi:10.1111/acer.14574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knapp A. A., Lee D. C., Borodovsky J. T., Auty S. G., Gabrielli J., Budney A. J. Emerging trends in cannabis administration among adolescent cannabis users. Journal of Adolescent Health. 2019;64:487–493. doi: 10.1016/j.jadohealth.2018.07.012. doi:10.1016/j.jadohealth.2018.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leatherdale S. T., Bélanger R. E., Gansaonré R. J., Patte K. A., deGroh M., Jiang Y., Haddad S. Examining the impact of the early stages of the COVID-19 pandemic period on youth cannabis use: Adjusted annual changes between the pre-COVID and initial COVID-lockdown waves of the COMPASS study. BMC Public Health. 2021;21:1181. doi: 10.1186/s12889-021-11241-6. doi:10.1186/s12889-021-11241-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manthey J., Kilian C., Carr S., Bartak M., Bloomfield K., Braddick F., Rehm J. Use of alcohol, tobacco, cannabis, and other substances during the first wave of the SARS-CoV-2 pandemic in Europe: A survey on 36,000 European substance users. Substance Abuse Treatment, Prevention, and Policy. 2021;16:36. doi: 10.1186/s13011-021-00373-y. doi:10.1186/s13011-021-00373-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meier M. H. Associations between butane hash oil use and cannabis-related problems. Drug and Alcohol Dependence. 2017;179:25–31. doi: 10.1016/j.drugalcdep.2017.06.015. doi:10.1016/j.drugalcdep.2017.06.015. [DOI] [PubMed] [Google Scholar]
- Mokrysz C., Shaban N. D. C., Freeman T. P., Lawn W., Pope R. A., Hindocha C., Curran H. V. Acute effects of cannabis on speech illusions and psychotic-like symptoms: Two studies testing the moderating effects of cannabidiol and adolescence. Psychological Medicine. 2021;51:2134–2142. doi: 10.1017/S0033291720001038. doi:10.1017/S0033291720001038. [DOI] [PubMed] [Google Scholar]
- Morean M. E., Lipshie N., Josephson M., Foster D. Predictors of adult e-cigarette users vaporizing cannabis using e-cigarettes and vape-pens. Substance Use & Misuse. 2017;52:974–981. doi: 10.1080/10826084.2016.1268162. doi:10.1080/1082 6084.2016.1268162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palamar J. J., Le A., Acosta P. Shifts in drug use behavior among electronic dance music partygoers in New York during COVID-19 social distancing. Substance Use & Misuse. 2021;56:238–244. doi: 10.1080/10826084.2020.1857408. doi: 10.1080/10826084.2020.1857408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raudenbush S. W., Bryk A. S., Congdon R. Skokie, IL: Scientific Software International, Inc; 2013. HLM 7.01 for Windows [Computer software] [Google Scholar]
- Russell C., Rueda S., Room R., Tyndall M., Fischer B. Routes of administration for cannabis use – basic prevalence and related health outcomes: A scoping review and synthesis. International Journal on Drug Policy. 2018;52:87–96. doi: 10.1016/j.drugpo.2017.11.008. doi:10.1016/j.drugpo.2017.11.008. [DOI] [PubMed] [Google Scholar]
- Schauer G. L., King B. A., Bunnell R. E., Promoff G., McAfee T. A. Toking, vaping, and eating for health or fun: Marijuana use patterns in adults, US, 2014. American Journal of Preventive Medicine. 2016;50:1–8. doi: 10.1016/j.amepre.2015.05.027. doi:10.1016/j.amepre.2015.05.027. [DOI] [PubMed] [Google Scholar]
- Spindle T. R., Bonn-Miller M. O., Vandrey R. Changing landscape of cannabis: Novel products, formulations, and methods of administration. Current Opinion in Psychology. 2019;30:98–102. doi: 10.1016/j.copsyc.2019.04.002. doi:10.1016/j.copsyc.2019.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Starks T. J., Jones S. S., Sauermilch D., Benedict M., Adebayo T., Cain D., Simpson K. N. Evaluating the impact of COVID-19: A cohort comparison study of drug use and risky sexual behavior among sexual minority men in the U.S.A. Drug and Alcohol Dependence. 2020;216:108260. doi: 10.1016/j.drugalcdep.2020.108260. doi:10.1016/j.drugalcdep.2020.108260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steigerwald S., Wong P. O., Khorasani A., Keyhani S. The form and content of cannabis products in the United States. Journal of General Internal Medicine. 2018;33:1426–1428. doi: 10.1007/s11606-018-4480-0. doi:10.1007/s11606-018-4480-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone A. L., Becker L. G., Huber A. M., Catalano R. F. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addictive Behaviors. 2012;37:747–775. doi: 10.1016/j.addbeh.2012.02.014. doi:10.1016/j.addbeh.2012.02.014. [DOI] [PubMed] [Google Scholar]
- Vanderbruggen N., Matthys F., van Laere S., Zeeuws D., Santermans L., Van den Ameele S., Crunelle C. L. Self-reported alcohol, tobacco, and cannabis use during Covid-19 lockdown measures: Results from a web-based survey. European Addiction Research. 2020;26:309–315. doi: 10.1159/000510822. doi:10.1159/000510822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vandrey R., Raber J. C., Raber M. E., Douglass B., Miller C., BonnMiller M. O. Cannabinoid dose and label accuracy in edible medical cannabis products. JAMA. 2015;313:2491–2493. doi: 10.1001/jama.2015.6613. doi:10.1001/jama.2015.6613. [DOI] [PubMed] [Google Scholar]
- White H. R., Kilmer J. R., Fossos-Wong N., Hayes K., Sokolovsky A. W., Jackson K. M. Simultaneous alcohol and marijuana use among college students: Patterns, correlates, norms, and consequences. Alcoholism: Clinical and Experimental Research. 2019;43:1545–1555. doi: 10.1111/acer.14072. doi:10.1111/acer.14072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White H. R., McMorris B. J., Catalano R. F., Fleming C. B., Haggerty K. P., Abbott R. D. Increases in alcohol and marijuana use during the transition out of high school into emerging adulthood: The effects of leaving home, going to college, and high school protective factors. Journal of Studies on Alcohol. 2006;67:810–822. doi: 10.15288/jsa.2006.67.810. doi:10.15288/jsa.2006.67.810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White H. R., Stevens A. K., Hayes K., Jackson K. M. Changes in alcohol consumption among college students due to COVID-19: Effects of campus closure and residential change. Journal of Studies on Alcohol and Drugs. 2020;81:725–730. doi: 10.15288/jsad.2020.81.725. doi:10.15288/jsad.2020.81.725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yehudai M., Bender S., Gritsenko V., Konstantinov V., Reznik A., Isralowitz R. COVID-19 fear, mental health, and substance misuse conditions among university social work students in Israel and Russia. International Journal of Mental Health and Addiction. 2020 doi: 10.1007/s11469-020-00360-7. Advance online publication. doi:10.1007/s11469-020-00360-7. [DOI] [PMC free article] [PubMed] [Google Scholar]