

Abstract
Background:
The effects of adductor muscle injury on performance in soccer athletes are unknown.
Purpose:
To (1) determine the rate and time to return to play (RTP) after adductor muscle injury, (2) investigate the rate of reinjury after RTP, and (3) investigate any long-term effects of injury on elite soccer player performance.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Using publicly available records, athletes sustaining adductor muscle injury were identified across the 5 major European soccer leagues (English Premier League, Bundesliga, La Liga, Ligue 1, and Serie A) between 2000 and 2015. Injured athletes were matched to controls by demographic characteristics and performance metrics from 1 season before the index timepoint. Investigations included the rate of RTP, reinjuries, player characteristics associated with RTP within 2 seasons, player availability, field time, and performance metrics during the 4 seasons after injury.
Results:
A total of 671 players with adductor muscle injury were included. Based on time to RTP, 86% of injuries were mild to moderate (4-28 days missed), and 4% required surgical intervention. Players with adductor muscle injury were absent for a median of 22 days (range, 1-700 days) and 4 games (range, 1-76 games). A total of 521 (78%) players returned at the same level, with no demographic or clinical characteristics associated with RTP on the multivariable regression. Of those returning to play, 143 (21%) experienced adductor reinjury. After RTP, defenders demonstrated decreased field time compared with controls (P < .05). As compared with controls, defenders and midfielders scored more points and goals per game during the season of the injury (P < .01), while attackers recorded more goals and assists per game the season after injury (P < .05).
Conclusion:
Only 3 in 4 players (78%) returned to participate in an official match, and the reinjury rate was high (21%). After RTP, defenders demonstrated decreased field time versus controls. On the other hand, defenders and midfielders recorded more points and goals per game, while attackers recorded more goals and assists per game versus controls. Although the multivariable analysis results did not identify player characteristics associated with RTP, there was a position-dependent association on player performance after RTP.
Keywords: football (soccer), general sports trauma, epidemiology, performance outcomes, adductor muscle injury, case-control
Hip and groin injuries are among the most common injuries in soccer athletes, 10 a population that is estimated at 265 million people worldwide in 2006. 10 Adductor-related injuries are specifically the most common hip and groin injuries in professional soccer players, with an estimated incidence rate of 0.6 per 1000 exposure hours. 3 Adductor muscle injuries account for up to 63% of hip/groin injuries and up to 23% of all muscle injuries. 3,10,25 Functional movements in soccer that have been proposed as risk factors for adductor muscle injuries include repetitive kicking motions, fast changes in the direction of body momentum, reaching/stretching movements, and sprints. 25 Preventable risk factors for adductor muscle injury include previous groin injury, reduced adductor strength, and reduced abductor strength. 6,25,28
Adductor muscle injuries in soccer players can account for significant time missed from practices and matches, which in turn can affect player performance and career longevity. Ekstrand et al 4 found that professional soccer players suffering from adductor muscle injuries missed a mean of 14 days of sports. In a cohort of 34 soccer players with adductor injuries, Tak et al 28 found that 82% returned to preinjury levels within 2 weeks after undergoing manual therapy. Unfortunately, up to 18% of soccer players have been reported to suffer reinjury after acute or chronic adductor muscle injuries. 4 Although there is a great deal of literature on the epidemiology and kinesiology of adductor muscle injuries in soccer players, there is a lack of data that demonstrate how these injuries affect game performance and player durability after RTP.
We conducted a case-control investigation of European elite-level soccer athletes with the purpose of (1) determining the rate and time to return to play (RTP) after adductor muscle injury, (2) investigating the rate of reinjury after RTP, and (3) comparing the effect adductor muscle injury may have on player performance for up to 4 seasons after initial injury. We hypothesized that the majority of players sustaining adductor muscle injury will RTP, a minority will experience adductor reinjury, and injured players will return to prior levels of performance after RTP.
Methods
Player Identification
This study was a retrospective review of male soccer players playing in any of the 5 major European soccer leagues (English Premier League, Bundesliga, Serie A, La Liga, and Ligue 1) within the Union of European Football Associations (UEFA) between the seasons of 1999-2000 and 2015-2016. Players sustaining adductor muscle injuries and matched controls were identified using publicly available injury data via previously established methods. 8,9,11 –17,31 Sources for injury reports included official team websites, injury reports, official team press releases, personal websites, and professional statistical websites. Injury reports from public media platforms were manually cross-referenced with official league reports by 2 authors (O.L.-G. and S.P.). Player performance data were compiled from www.transfermarkt.com, one of the largest and most frequently visited sports media platforms reporting scores, transfers, and player values.
Inclusion Criteria
Criteria for inclusion in either the injured or control cohort included the following: the player was drafted or signed to be on the roster during a season; the team was ranked within 1 of the 5 major European soccer leagues; the player played in at least 1 game before the index timepoint; and the player had a minimum of 1-year follow-up after the index timepoint. Players were excluded if they did not play for a team during a season, or the team participated in the major leagues. Players were included in the injured cohort if they were reported to sustain a “tear of the adductor muscle,” “groin surgery,” or “avulsion of the adductors.”
Data Collection
Individual player demographic data consisted of age, height, playing position, and number of seasons played before the index timepoint. Injury and RTP data consisted of date of injury, days missed, games missed, date of RTP, and subsequent adductor muscle injury up to 4 years after initial injury. Seasonal performance metrics collected included total games played, minutes played, goals scored, assists, clean sheets, conceded goals, and average minutes played per game.
Injury Severity
As the available data did not include information on injury grade, days missed served as a proxy for injury severity, utilizing the same classification as in prior epidemiological studies utilizing the UEFA data. 4,12 Time to RTP is a reasonable proxy variable, as it has been associated with adductor muscle injury grade. 24 –26 Injuries were classified as minimal (0-3 day of absence), mild (4-7 days), moderate (8-28 days), and severe (>28 days). 12
Case-Control
A matched cohort analysis was used to investigate the association of adductor muscle injury and changes in player performance metrics. Players were matched by playing position, height, age (within 2 years), season of play (within 1 year), number of seasons played within the league before the index timepoint (within 1 year), total games played, total time played, goals scored, and assists recorded the season before the index timepoint. Season of play was included to minimize the influence of improvements in conservative treatment options, potential changes in league playing schedules, and technological innovations over time. Number of seasons played before the index timepoint were included to minimize the likelihood of observing inflated differences in metrics because of the natural progression and regression of playing skills over the span of a soccer career.
The elite nature of ranking within 1 of the 5 major European soccer leagues led to a limited cohort of players for inclusion in the study. Manual selection of control cohorts and propensity score matching predispose to selection bias. 17,23 Thus, an optimized matching algorithm was utilized to identify the 2 nearest neighbor players without lower extremity injury for every 1 player with adductor muscle injury. 7,8,15,18,20,21
Statistical Analysis
Each player’s performance metrics during the 4 playing seasons after the index timepoint were compared with their individual metrics of the playing season preceding the index timepoint. This baseline was chosen to minimize the potential confounders of deflated metrics of a rookie season 2 or 3 seasons preceding the index timepoint. Because of the dynamic nature of player participation throughout the follow-up period, players were included in the analyses of all follow-up seasons during which they recorded metrics; conversely, they were excluded from timepoints during which they did not record any metrics. Subgroup analyses of performance metrics by position were conducted to account for differences in player roles on the field. Statistical analyses consisted of independent-samples t tests and Wilcoxon rank-sum tests where appropriate for continuous data, and chi-square tests of independence for categorical data. Analyses were performed using R Studio software Version 3.6.2 (R Foundation for Statistical Computing), and statistical significance was set at P < .05.
Results
Characteristics
A total of 671 players who sustained an adductor muscle injury between 2000 and 2015 were included. The case-control match was satisfactory, with no significant differences in player characteristics (position, height, age, season of play, and total years played) or baseline performance (games, total time played, goals, and assists 1 season before the index timepoint) between cohorts (Table 1). Within the injured cohort, the mean age of attackers was 26.04 ± 3.79 years, that of midfielders 26.89 ± 3.86 years, and that of defenders 26.45 ± 3.79 years. Goalkeepers were significantly older, with a mean age of 29 ± 3.27 (P < .001). Within the control cohort, the mean age of attackers was 26.95 ± 5.03 years, that of midfielders 27.38 ± 5.48 years, and that of defenders 27.30 ± 4.95 years. Goalkeepers were significantly older, with a mean age of 31.03 ± 6.26 (P < .001).
Table 1.
Characteristics and Baseline Metrics Between Injured and Control Cohorts a
| Injured Players (n = 671) | Controls (n = 692) | P Value | |
|---|---|---|---|
| Case-control match | |||
| Player position | .08 | ||
| Attacker | 195 | 166 | |
| Midfielder | 218 | 200 | |
| Defender | 237 | 295 | |
| Goalkeeper | 21 | 31 | |
| Season of play | 2011 ± 3.42 | 2012 ± 5.23 | ≥.999 |
| Years played before index timepoint | 6.99 ± 4.39 | 5.27 ± 3.67 | ≥.999 |
| Height, m | 1.82 ± 0.06 | 1.82 ± 0.06 | .215 |
| Age during season, y | 25.97 ± 3.74 | 25.68 ± 4.06 | ≥.999 |
| Baseline metrics b | |||
| Games played | 22.8 ± 9.85 | 20.57 ± 10.55 | ≥.999 |
| Total time played, min | 1697.44 ± 912.41 | 1494.43 ± 957.67 | ≥.999 |
| Goals scored | 4.66 ± 4.68 | 3.03 ± 3.18 | ≥.999 |
| Assists recorded | 3.63 ± 2.92 | 2.36 ± 1.88 | ≥.999 |
| Total career length, y | 15.02 ± 4.59 | 14.25 ± 3.81 | ≥.999 |
a Values are reported as mean ± SD unless otherwise indicated.
b Metrics 1 season before the index timepoint.
Within the injured cohort, the majority of players sustained mild (46%) to moderate (40%) injuries, and a minority of players required surgical intervention (4%) (Table 2).
Table 2.
Injury Characteristics (N = 671 players) a
| Characteristic | Value |
|---|---|
| Injury severity | |
| Minimal | 70 (10) |
| Mild | 311 (46) |
| Moderate | 271 (40) |
| Severe | 19 (3) |
| Surgical intervention | 25 (4) |
| Primary injury | |
| Days missed | 39.85 ± 57.47 |
| Games missed | 5.91 ± 7.39 |
| Return to play | |
| At any timepoint | 521 (78) |
| Same season as injury | 477 (71) |
| 1 season postinjury | 506 (75) |
| 2 seasons postinjury | 517 (77) |
| 3 seasons postinjury | 521 (78) |
| Secondary injury | |
| Number of reinjuries | 143 (21) |
| Time to reinjury, y | 2.76 ± 2.14 |
| Days missed b | 36.87 ± 57.45 |
| Games missed c | 5.53 ± 7.72 |
a Values are reported as mean ± SD or n (%).
b Not significantly different compared with primary injury (P = .574).
c Not significantly different compared with primary injury (P = .599).
Return to Play
A total of 521 (78%) players with adductor muscle injury returned to play at the same level. Of these, 477 (71%) returned within 1 season of injury. Players missed a median of 22 days (range, 1-700) and 4 games (range, 1-76). Of those returning to play, 143 (21%) experienced subsequent adductor muscle injury, with a median time to reinjury of 2 years (range, 1-11 years) (Table 2). There were no significant differences in days or games missed between initial and repeat adductor muscle injuries.
On the multivariable regression, there were no player characteristics associated with rate of RTP (Table 3). Factors in the multivariable regression included demographic characteristics (age, player experience in the league, and position of play) and performance metrics 1 season before injury (games played, time played, goals per 90 minutes of play, and assists per 90 minutes of play).
Table 3.
Multivariable Regression of RTP Within 2 Seasons of Injury a
| OR (95% CI) | P Value | |
|---|---|---|
| Age, y | ||
| <21 | Reference | |
| 21-25 | 0.83 (0.59-1.19) | .29 |
| 26-30 | 0.76 (0.53-1.10) | .13 |
| >30 | 0.67 (0.42-1.06) | .09 |
| Time in league, y | ||
| <3 | Reference | |
| 3-5 | 1.07 (0.79-1.46) | .66 |
| 6-8 | 1.05 (0.75-1.48) | .78 |
| >8 | 1.15 (0.83-1.61) | .39 |
| Player position | ||
| Goalkeeper | Reference | |
| Attacker | 1.30 (0.73-2.51) | .40 |
| Midfielder | 1.31 (0.75-2.48) | .37 |
| Defender | 1.36 (0.79-2.54) | .30 |
| Surgery | 0.66 (0.36-1.11) | .15 |
| Games played b | ||
| <10 | Reference | |
| 10-19 | 1.02 (0.72-1.42) | .91 |
| 20-29 | 0.95 (0.57-1.59) | .85 |
| >30 | 1.01 (0.53-1.92) | .97 |
| Time played, min b | ||
| <1000 | Reference | |
| 1000-1999 | 1.20 (0.76-1.89) | .42 |
| 2000-2500 | 1.28 (0.74-2.19) | .38 |
| >2500 | 1.34 (0.71-2.55) | .36 |
| Goals b | ||
| <3 | Reference | |
| 3-6 | 0.94 (0.70-1.26) | .70 |
| 7-9 | 1.07 (0.68-1.65) | .76 |
| >9 | 0.94 (0.56-1.53) | .80 |
| Assists b | ||
| 0-3 | Reference | |
| >3 | 1 (0.75-1.32) | .98 |
a Refers to RTP at same league level. OR, odds ratio; RTP, return to play.
b Overall metrics for 1 season before the index timepoint.
Player Availability After RTP
Player retention was significantly higher for those sustaining adductor muscle injury compared with controls (P < .001) (Figure 1). Among those who retired during the study period, there was no significant difference between the injured and control cohorts in total career length (Table 1).
Figure 1.
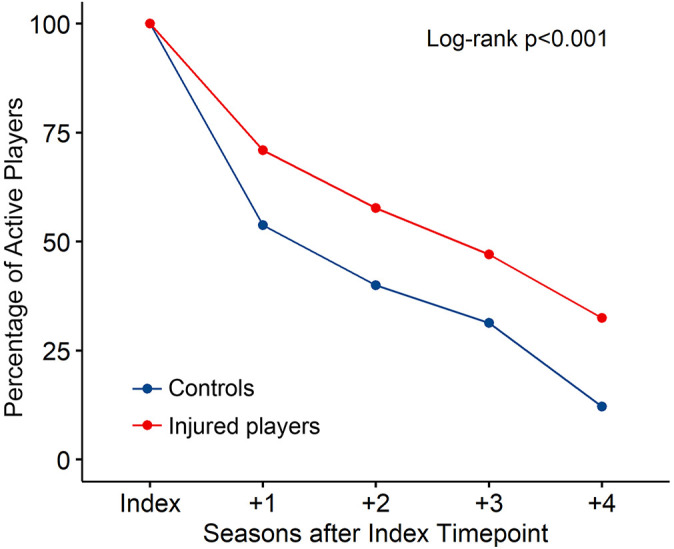
Player retention in the leagues by injury status during the study follow-up period.
Player Performance
Players sustaining an adductor muscle injury played approximately 218 less total minutes and 2 less games as compared with controls 1 season after injury (Figure 1). Furthermore, injured players played consistently fewer minutes per game than controls up to 4 seasons after injury (range, 4-7 fewer minutes; P < .05) (Figure 2). On the other hand, players sustaining an adductor muscle injury scored more points per game as compared with controls up to 3 seasons after injury (range, 0.13-0.19 more points per game; P < .05). Injured players also recorded more goals per 90 minutes of play as compared with controls up to 2 seasons after injury (range, 0.07-0.08 more goals; P < .05) and 0.06 more assists as compared with controls per 90 minutes of play 1 season after injury (P < .001) (Figure 2).
Figure 2.

Overall player performance and field time. *P < .05, **P < .01, ***P < .001, ****P < .0001.
Field Time by Position
On the subgroup analysis of field time, defenders sustaining adductor muscle injury played 2 fewer games (P < .05) and 199 fewer total minutes (P < .01) as compared with controls 1 season after injury, whereas attackers and midfielders demonstrated no statistically significant differences as compared with controls during the study period (Figure 3). Similarly, defenders demonstrated a declining trend in minutes played per game over the seasons, playing approximately 6 fewer minutes per game as compared with controls 3 seasons after injury (P < .01) (Figure 3). Attackers and midfielders demonstrated no significant differences in field time as compared with controls (Figure 3).
Figure 3.

Field time by position. Asterisks indicate statistically significant differences between injured and control players. *P < .05, **P < .01, ***P < .001.
Player Performance by Position
There were no player position subgroups that demonstrated decreased performance as compared with controls after adductor muscle injury. Midfielders and defenders scored more points per game (0.14 and 0.15, respectively; P < .01) as well as more goals per 90 minutes of play (0.04 [P <.05] and 0.03 [P < .001], respectively) as compared with controls 1 season after injury (Figure 4). Additionally, defenders recorded 0.04 more assists per 90 minutes of play as compared with controls 1 season after injury (Figure 4). Attackers recorded 0.1 more goals per 90 minutes 1 season after injury (P < .01) and 0.18 more assists per 90 minutes of play 2 seasons after injury (P < .05) as compared with controls (Figure 4). Attackers sustaining adductor muscle injury did not have a significant difference in points per game as compared with controls for up to 4 seasons after injury (Figure 4).
Figure 4.

Performance metrics by position. Asterisks indicate significant differences between injured and control players. *P < .05, **P < .01, ***P < .001, ****P < .0001.
Discussion
Although there has been increased understanding of the epidemiology of adductor muscle injuries within soccer, the impact of these injuries on RTP and elite player performance remains unknown. In this retrospective study of modern elite soccer players sustaining adductor muscle injuries, an encouraging rate of RTP (78%) was observed with a reasonable period of absence at a median 22 days and 4 games missed. On the other hand, there was a high risk of reinjury (21%) within a relatively short period of time after RTP (mean, 2.76 years). Although defenders were affected by adductor muscle injury in terms of field time, all players demonstrated position-dependent improvements in performance metrics after RTP as compared with their uninjured teammates. In summary, these results suggest that despite the decreased field time and elevated risk of reinjury after adductor muscle injury in elite soccer players, career longevity and performance is not compromised. The fact that some players improved their performance metrics the season after injury is interesting. Whether this is secondary to the positive effects of adductor and core muscle rehabilitation on player performance is potentially a concept warranting further investigation.
Three in 4 (78%) players with an adductor muscle injury returned to play at prior levels. It is imperative to note that this rate reflects the proportion of players both cleared for full team training and selected for participation in an official match against an opposing team. There is an inherent difference between participating in a match as compared with participating in full team training, and thus participation in a match was included in the RTP criteria, as it more closely captured an athlete’s ability to truly return to prior levels of play. While a previous study reported that 93% of players with adductor injuries were able to RTP (ie, were capable of participating in full training and available for match selection), 24 results from the present cohort suggest that a much smaller proportion of athletes participate in both full team training and official matches after RTP.
As compared with the 4% rate of surgery in the present study, Kerbel et al 16 reported a 1.3% rate of surgical intervention in collegiate athletes from a variety of sports who suffered hip or groin injuries, including adductor/groin tears, hip flexor tears, iliopsoas/sartorius tears, and internal rotator/groin tears. The pursuit of surgical intervention may have an association with the athlete’s sport, as a reported 1.2% of football athletes undergo surgery as compared with 3.9% in wrestling athletes. 16 Furthermore, it is likely that professional athletes undergo surgical intervention at a higher rate than collegiate or amateur athletes, given the financial incentives to return to peak performance. Although there have been a number of studies focused on determining optimal nonoperative rehabilitation protocols after adductor strains in elite soccer players, rates of surgical intervention largely remain unknown. 13,14,19,27 Nonetheless, the clinical outcomes after surgical intervention for adductor muscle injury have drastically improved in the past decade, as evident in the RTP rate of 54% in 2010 versus 93% in 2020 after tenotomy. 1,11,26 Personalized rehabilitation targeting at-risk functional movements may drive ongoing improvements in future rates of RTP.
In this cohort of players with adductor injury, the median time to RTP was 22 days. Although this is higher than the previously reported mean of 14 days in soccer players, 4 it is similar to that reported in numerous other sports. 14,22,25 Previous soccer-specific investigations included a selection of players from the UEFA Champions League, a subset of the teams included in the current study. In addition to the compensation received for participation in the 5 major leagues included in the present study, teams participating in the UEFA Champions League games are awarded 2.7 million euros for every match won and 900,000 euros for every match they draw. 31 Thus, the teams included in prior investigations may have had a higher team budget and more allocated resources to expedite rehabilitation after adductor muscle injury. 4 Additionally, the financial incentivization of RTP during the high-profile UEFA Champions League competition is greater than during domestic league competitions, which may contribute to the expedited RTP of their athletes. Another factor contributing to the longer time to RTP observed in this series may revolve around the increasing awareness of adductor reinjury risk after RTP since the completion of the prior study in 2009. As knowledge of this risk evolved, RTP protocols may have lengthened across multiple leagues, leading to longer RTP in the current study, which included data up to 2015. 34
There has been increased focus on optimization of rehabilitation programs for adductor muscle injury, with promising results. Active therapy is associated with higher RTP than physiotherapy without active training. 14 Multimodal treatment consisting of heat, manual therapy, stretching, and a gradual return to running has been shown to be more effective than exercise therapy alone in athletes with adductor muscle pain. 32 Implementation of these multimodal methods into the care of elite athletes has been efficacious and may contribute to the high rate of RTP and success of nonoperative management in the current study. 33
In addition to recovery from primary injury, risk of subsequent injury is crucial to consider during management of adductor muscle injury. Rates of adductor retear in basketball players are similar to the rate of reinjury within the present investigation. 22 The most recent report of adductor reinjury rates in the UEFA was 18% in 2011, which is comparable to the 21% seen in the current study. 4 A promising preventative measure for both primary and secondary adductor muscle injury is deliberate strengthening of hip abductors and groin muscles. 13,29,30 Functional movement rehabilitation with biofeedback has been increasingly used both to address the primary injury and to modify functional movement patterns that may predispose the athlete to secondary injury or a different type of injury. 14,25,32,35 As a result, athletes may return to the field fully recovered from a moderate injury, with the additional benefits of corrected at-risk functional movement patterns, leading to tangible increases in performance metrics. 2
Of those sustaining adductor muscle injury, defenders and midfielders scored more points and goals while attackers recorded more goals and assists per game after RTP as compared with controls. Additionally, defenders recorded increased performance metrics in the context of significantly decreased field time. Although adductor muscle injury leads to player absence, the mean time missed was relatively short (approximately 30 days and 6 games), with likely minor repercussions on productivity and value. It is possible that the combination of functional rehabilitation and rest had a positive influence on their physical condition compared with their teammates who continued playing at a high level uninterrupted.
Limitations
This study was not without limitations. Publicly accessible data sources were utilized to generate the adductor muscle injury and control cohorts. As such, selection bias may have occurred because of underreporting of adductor muscle injury to the public as well as unintended exclusion of adductor muscle injuries reported by more broad descriptions (eg, adductor problems or groin pain). However, this limitation was likely minimal, as rates of injuries identified are consistent with those published as part of the UEFA Injury Study program. 4,12 Second, because of the nature of publicly sourced data, it was not possible to obtain each player’s specific treatment regimen, including specific surgical procedures and rehabilitation protocols, or injury grade diagnoses without access to official medical record documentation. However, the presently reported rate of 4% of players requiring surgical intervention is similar to rates reported in prior studies published, and the methods utilized for injury grade proxies were directly derived from the UEFA Injury Study program. 16 It is important to note that the UEFA Injury Study is directly funded and supervised by the Union of European Football Associations. 9 Publications with these data have been limited to epidemiologic investigations of incidence, RTP, and reinjury rates rather than changes in performance after injury. 3 –5,25,33 To our knowledge, there is no established infrastructure to process applications of study proposals utilizing these official data. In consideration of these realities, we firmly believe that despite the absence of official medical record documentation within this study’s publicly sourced data, this study garners strength in the objective presentation of results reporting on the previously unknown associations between injury and player performance after RTP.
Conclusion
The majority of adductor muscle injuries in elite soccer players were treated nonoperatively. Only 3 in 4 players (78%) returned to participate in an official match, with a high reinjury rate (21%). Defenders demonstrated decreased field time as compared with controls after RTP. On the other hand, defenders and midfielders recorded more points and goals per game, while attackers recorded more goals and assists per game after RTP as compared with controls. Although multivariable analysis results did not identify player characteristics associated with RTP, there was a position-dependent association on player performance after RTP.
Footnotes
Final revision submitted February 12, 2021; accepted February 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.R.C. has received hospitality payments from Medical Device Business Services. B.U.N. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; and hospitality payments from Stryker, Wright Medical, and Zimmer Biomet. B.F. has received research support from Arthrex, Stryker, and Smith & Nephew; and consulting fees from Stryker; education payments from Medwest; and has stock/stock options in Jace Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
- 1. Atkinson HD, Johal P, Falworth MS, et al. Adductor tenotomy: its role in the management of sports-related chronic groin pain. Arch Orthop Trauma Surg. 2010;130(8):965–970. [DOI] [PubMed] [Google Scholar]
- 2. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: the use of fundamental movements as an assessment of function-part 2. Int J Sports Phys Ther. 2014;9(4):549–563. [PMC free article] [PubMed] [Google Scholar]
- 3. Ekstrand J, Hagglund M, Walden M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–558. [DOI] [PubMed] [Google Scholar]
- 4. Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226–1232. [DOI] [PubMed] [Google Scholar]
- 5. Ekstrand J, Krutsch W, Spreco A, et al. Time before return to play for the most common injuries in professional football: a 16-year follow-up of the UEFA Elite Club Injury Study. Br J Sports Med. 2020;54(7):421–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. Am J Sports Med. 2010;38(10):2051–2057. [DOI] [PubMed] [Google Scholar]
- 7. Erickson BJ, Gupta AK, Harris JD, et al. Rate of return to pitching and performance after Tommy John surgery in Major League Baseball pitchers. Am J Sports Med. 2014;42(3):536–543. [DOI] [PubMed] [Google Scholar]
- 8. Erickson BJ, Harris JD, Heninger JR, et al. Performance and return-to-sport after ACL reconstruction in NFL quarterbacks. Orthopedics. 2014;37(8):e728–e734. [DOI] [PubMed] [Google Scholar]
- 9. Faulkner JA, Davis CS, Mendias CL, Brooks SV. The aging of elite male athletes: age-related changes in performance and skeletal muscle structure and function. Clin J Sport Med. 2008;18(6):501–507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Fédération Internationale de Football Association. FIFA Big Count 2006: 270 million people active in football. Accessed March 28, 2020. https://www.fifa.com/mm/document/fifafacts/bcoffsurv/bigcount.statspackage_7024.pdf
- 11. Gill TJ, Wall AJ, Gwathmey FW, et al. Surgical release of the adductor longus with or without sports hernia repair is a useful treatment for recalcitrant groin strains in the elite athlete. Orthop J Sports Med. 2020;8(1):2325967119896104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hagglund M, Walden M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med. 2005;39(6):340–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Haroy J, Clarsen B, Wiger EG, et al. The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med. 2019;53(3):150–157. [DOI] [PubMed] [Google Scholar]
- 14. Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. Lancet. 1999;353(9151):439–443. [DOI] [PubMed] [Google Scholar]
- 15. Keller RA Steffes MJ, Zhuo D Bey MJ Moutzouros V. The effects of medial ulnar collateral ligament reconstruction on Major League pitching performance. J Shoulder Elbow Surg. 2014;23(11):1591–1598. [DOI] [PubMed] [Google Scholar]
- 16. Kerbel YE, Smith CM, Prodromo JP, Nzeogu MI, Mulcahey MK. Epidemiology of hip and groin injuries in collegiate athletes in the United States. Orthop J Sports Med. 2018;6(5):2325967118771676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. King G, Nielsen R. Why propensity scores should not be used for matching. Political Analysis. 2018;27(4):435–454. [Google Scholar]
- 18. Lu Y, Okoroha KR, Patel BH, et al. Return to play and performance after shoulder instability in National Basketball Association athletes. J Shoulder Elbow Surg. 2020;29(1):50–57. [DOI] [PubMed] [Google Scholar]
- 19. Lynch SA, Renström PA. Groin injuries in sport: treatment strategies. Sports Med. 1999;28(2):137–144. [DOI] [PubMed] [Google Scholar]
- 20. Okoroha KR, Kadri O, Keller RA, et al. Return to play after revision anterior cruciate ligament reconstruction in National Football League players. Orthop J Sports Med. 2017;5(4):2325967117698788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Okoroha KR, Taylor KA, Marshall NE, et al. Return to play after shoulder instability in National Football League athletes. J Shoulder Elbow Surg. 2018;27(1):17–22. [DOI] [PubMed] [Google Scholar]
- 22. Patel BH, Okoroha KR, Jildeh TR, et al. Adductor injuries in the National Basketball Association: an analysis of return to play and player performance from 2010 to 2019. Phys Sportsmed. 2020;48(4):450–457. [DOI] [PubMed] [Google Scholar]
- 23. Rohrer JM. Thinking clearly about correlations and causation: graphical causal models for observational data. Advances in Methods and Practices in Psychological Science. 2018;1(1):27–42. [Google Scholar]
- 24. Serner A, Weir A, Tol JL, et al. Return to sport after criteria-based rehabilitation of acute adductor injuries in male athletes: a prospective cohort study. Orthop J Sports Med. 2020;8(1):2325967119897247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Serner A, Weir A, Tol JL, et al. Characteristics of acute groin injuries in the adductor muscles: A detailed MRI study in athletes. Scand J Med Sci Sports. 2018;28(2):667–676. [DOI] [PubMed] [Google Scholar]
- 26. Serner A, Weir A, Tol JL, et al. Associations between initial clinical examination and imaging findings and return-to-sport in male athletes with acute adductor injuries: a prospective cohort study. Am J Sports Med. 2020;48(5):1151–1159. [DOI] [PubMed] [Google Scholar]
- 27. Svensson K, Eckerman M, Alricsson M, Magounakis T, Werner S. Muscle injuries of the dominant or non-dominant leg in male football players at elite level. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):933–937. [DOI] [PubMed] [Google Scholar]
- 28. Tak I, PhD M, Langhout RMP, Bertrand BM, et al. Manual therapy and early return to sport in football players with adductor-related groin pain: A prospective case series. Physiother Theory Pract. 2020;36(9):1009–1018. [DOI] [PubMed] [Google Scholar]
- 29. Tyler TF, Nicholas SJ, Campbell RJ, McHugh MP. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med. 2001;29(2):124–128. [DOI] [PubMed] [Google Scholar]
- 30. Tyler TF, Silvers HJ, Gerhardt MB, Nicholas SJ. Groin injuries in sports medicine. Sports Health. 2010;2(3):231–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. UEFA Champions League. How clubs' 2018/19 UEFA Champions League revenue will be shared. Updated June 12, 2018. Accessed June 1, 2020. https://www.uefa.com/uefachampionsleague/news/0252-0cda3874747b-58f3718c48c2-1000--how-clubs-2018-19-uefa-champions-league-revenue-will-be-shared/ [Google Scholar]
- 32. Weir A, Jansen JA, van de Port IG, Van de Sande HB, Tol JL, Backx FJ. Manual or exercise therapy for long-standing adductor-related groin pain: a randomised controlled clinical trial. Man Ther. 2011;16(2):148–154. [DOI] [PubMed] [Google Scholar]
- 33. Werner J, Hagglund M, Ekstrand J, Walden M. Hip and groin time-loss injuries decreased slightly but injury burden remained constant in men's professional football: the 15-year prospective UEFA Elite Club Injury Study. Br J Sports Med. 2019;53(9):539–546. [DOI] [PubMed] [Google Scholar]
- 34. Yousefzadeh A, Shadmehr A, Olyaei GR, Naseri N, Khazaeipour Z. Effect of Holmich protocol exercise therapy on long-standing adductor-related groin pain in athletes: an objective evaluation. BMJ Open Sport Exerc Med. 2018;4(1):e000343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Zalai D, Panics G, Bobak P, Csáki I, Hamar P. Quality of functional movement patterns and injury examination in elite-level male professional football players. Acta Physiol Hung. 2015;102(1):34–42. [DOI] [PubMed] [Google Scholar]