

Abstract
BACKGROUND:
Previous studies have reported that medical students show high rates of depression, anxiety, and stress levels, but mixed findings were found regarding possible differences between gender and different years of medical training. This study evaluated depression, anxiety, and stress levels and psychiatric drug use in students in an Italian medical school and investigated the differences between gender and year of study.
MATERIALS AND METHODS:
This cross-sectional study included 694 medical students in their 1st (n = 286), 4th (n = 209), and 6th (n = 199) year of study. The questionnaire included demographic information, self-report questionnaires regarding depression, anxiety, and stress, and questions about psychiatric drug use. Data analysis was performed using SPSS/Ver 22 through descriptive and analytic statistics, including Mann–Whitney U-test, Fisher's exact test, and GLM two-way ANOVA.
RESULTS:
Depression, anxiety, and stress symptoms were reported by 365 (52.6%), 428 (61.7%), and 545 (78.5%) medical students, respectively. Female students in their 4th year of study reported higher depression levels than males of the same year (P = 0.004), whereas levels of anxiety were higher in 6th-year female students compared with those in their 1st and 4th years (P = 0.001; P = 0.025). Stress levels were consistently higher in females than in males for all 3 years (1st year: P = 0.041; 4th year: P < 0.001; 6th year: P = 0.004). No gender differences were found in the use of psychiatric and stimulant drugs.
CONCLUSION:
This study provides preliminary evidence suggesting the importance of planning interventions aimed at reducing emotional distress among medical students that should be targeted on gender and year of the study.
Keywords: Anxiety, depression, medical students, mental health, psychological stress, sex
Introduction
Medical schools are considered among those placing the greatest academic and emotional load upon their students.[1] Numerous studies have highlighted the presence of psychological distress among medical students in various parts of the world, including the United States and Canada,[2] Europe and the English-speaking world outside North America,[3] the Arab world,[4] and China,[5,6] and other contexts around the globe.[1,7,8,9] According to recent meta-analyses, medical students show a high rate of mental health problems, with a prevalence of 6.0%–66.5% for depression, 7.7%–65.5% for anxiety, and 12.2%–96.7% for psychological distress.[1,3,7] The presence of depressive and anxiety symptoms appears to be associated with poor academic performance,[10] financial burden, unhealthy lifestyles, substance use, and suicidal ideation.[6,10,11]
Medical students are also more prone to stress than the general university student population.[10] The various sources of stress include examination pressure, long hours of study, a high workload, financial difficulties, and an imbalance between the study efforts and results obtained. Furthermore, stress appears to be correlated with decreased sleep duration and quality, and related daytime dysfunction, with important consequences on students’ performance.[12,13]
Emotional distress can lead to, or be related to, the use of psychiatric drugs (i.e., hypnotic and sedative medications) and stimulants, reportedly used by approximately 10% and 7.7% of medical students, respectively.[14] A connection between substance use and academic stress has been hypothesized,[15] as medical students reported that they used stimulants to maintain concentration when preparing for examinations.[16]
Mixed findings have been reported in the literature with regard to trends in depression, anxiety, and stress over the years of medical training. While some studies report a reduction in the levels of emotional distress between the first and the last years of medical training,[17,18,19] other studies show an increase.[11,15] Two recent meta-analyses investigating the prevalence of depression and anxiety in medical students across different countries found evidence that both symptoms were relatively constant across all years of study.[1,8]
As regards gender differences related to emotional distress levels, once again, different studies have reported different findings. Several studies found that female students tend to experience more stress,[3,19,20] depressive,[3,5,10,19,21] and anxiety symptoms[3,10,21,22] than males, which are also related to higher burnout scores.[9,20,23] These differences have not been associated with a single factor, but with different bio-socio-cultural factors, such as social stigma, gender inequality, personality traits, role conflict, and the academic environment.[21,24] Conversely, a recent systematic review of depression and anxiety in medical students in China reported greater levels of depression, but not anxiety, in males than in females.[5] This difference was more prevalent in studies conducted in more recent years, whereas older studies reported the opposite trend. Furthermore, other meta-analyses that included studies conducted in different countries reported gender differences neither for depression[6,7,8] nor for anxiety.[1,6] The use of substances, mainly cannabis and alcohol, was reported to be more common among male than female medical students, although this was not the case in relation to psychiatric drugs.[14,25]
In Italy, the literature concerning emotional distress in medical students is still in its infancy. Few studies have been conducted so far to investigate the prevalence and associated characteristics of depression, anxiety, and stress levels and the use of psychiatric drugs and stimulants among medical students.[26,27,28,29] To date, research has reported high rates of depression, anxiety, and stress levels among medical students, but mixed findings exist with regard to the possible differences associated with gender and between different years of medical training. Therefore, these aspects need to be investigated further in various contexts, including that of Italy. The aim of the present study was to describe the levels of depression, anxiety, and perceived stress and the use of psychiatric drugs among male and female medical students in the 1st, 4th, and 6th years of an Italian medical school.
Materials and Methods
Study design and setting
This was a cross-sectional study of 1st-, 4th-, and 6th-year medical students from the University of Torino School of Medicine (Italy) during the academic year 2017–2018.
Study participants and sampling
Students were recruited by convenience sampling and invited to complete an anonymous survey that included questions on depression, anxiety, perceived stress, and the usage of psychiatric drugs and stimulants. Raosoft® (Raosoft Sample Size Online Calculator, http://www.raosoft.com/samplesize.html) software was used to calculate a minimum sample size of 292, based on a 5% margin of error, a 95% confidence level, 50% response distribution, and a population of 1211 (total number of 1st-, 4th-, and 6th-year medical students at the University of Turin during the academic year 2017–2018).
Data were collected between January and March 2018. Students in the 1st and 4th years were asked to complete a paper version of the survey during a lecture, while the link to the online version of the survey created with Qualtrics software (Qualtrics, Provo, UT) was sent with an e-mail to 6th-year students.
Data collection tool and technique
Demographic information (gender, age, and year of study) was collected. To assess different areas of emotional distress, the following psychological self-report questionnaires were administered:
Beck Depression Inventory-short form (BDI-sf):[30] It is a 13-item self-report questionnaire that assesses the presence and severity of depression symptoms. The overall total score may range from 0 to 39, with a score range of 5–7 for mild depression, 8–15 for moderate depression, and 16 or higher for severe depression
State-Trait Anxiety Inventory (STAI-Y):[31] It is a 40-item self-report measure that assesses for the presence and severity of current symptoms of anxiety (state anxiety; STAI-S) and a generalized propensity to be anxious (trait anxiety; STAI-T). The score range for each subtest is 20–80, with higher scores indicating greater levels of anxiety. A cutoff of 39–40 has been suggested to detect clinically significant symptoms for the state anxiety scale
Perceived Stress Scale (PSS):[32] It is a 10-item self-report questionnaire that measures the perception of stress. The overall total score may range from 0 to 40, with a higher score indicating higher perceived stress. Scores ranging from 0 to 13 are indicative of low stress, from 14 to 26 indicate moderate stress, and from 27 to 40 denote high perceived stress.
To investigate the use of psychiatric drugs and stimulants in medical students, two yes–no questions were administered: (1) “Have you ever taken psychiatric drugs during your university career?” (2) “Have you ever taken stimulants to improve your academic performance, e.g., examinations, traineeships?”
Data were processed and analyzed using the Statistical Package for the Social Sciences (SPSS version 22.0; Chicago, IL, USA). Differences between genders in the overall sample and in each year of study were calculated using the Mann–Whitney U-test for continuous measures and Fisher's exact test for categorical measures. To evaluate the effect of gender on depression, anxiety, and perceived stress levels among the students from the 3 years of study, a GLM two-way ANOVA was performed for each dependent variable (BDI-sf, STAI-S, STAT-T, and PSS) with year group and gender as independent variables. F-tests were calculated for the main effect of each independent variable, as well as for the interactions. Simple pairwise comparisons between groups and between genders were made and are reported as mean differences, with the Bonferroni correction and 95% confidence intervals applied for multiple comparisons.
Fisher's exact tests were used to evaluate the association between the use of drugs and stimulants and study year. All tests were two-sided. A P < 0.05 was considered statistically significant.
Ethical consideration
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. This study was approved by the University Bioethics Committee of the University of Torino, Italy (Protocol No. 190231 dated July 5, 2014). Written informed consent was obtained from all participants, by collecting their signatures on the paper version of the survey, or by asking respondents to click the appropriate button on the online version.
Results
A total of 777 medical students completed the questionnaires (response rate: 777/1211 = 64.2%; divided as follows: 1st year: 91.9%; 4th year: 47.4%; 6th year: 58.1%). This study focused on the participants’ responses that contained no missing data for all the variables of interest (694/1211 = 57.3%, divided as follows: 1st year: n = 286; 4th year: n = 209; 6th year: n = 199). Of these, 60.8% were female and 39.27% were male. The overall prevalence of depressive symptoms was 52.6%. Specifically, 20.6% reported mild depression levels, 26.7% moderate levels, and 5.3% severe symptoms. Symptoms of anxiety were found in 61.7% of the sample. Perceived stress was found in 78.5% of the students, with 59.8% and 18.7% reporting moderate and high levels of stress, respectively. The use of psychiatric drugs was admitted by 9.1% of medical students, whereas 3.5% declared to have used psychostimulants.
First, comparisons were made to analyze for differences between genders. Table 1 presents the demographic characteristics and clinical features of the student population, both overall and stratified by gender and year of study. There was no significant difference between females and males in relation to median age. In the group of 1st-year students, a significant difference was revealed between male and female with regard to perceived stress levels. In the 4th-year students, male students showed lower depressive, anxiety, and stress levels than females. In the 6th-year students, females showed greater state anxiety levels compared with males.
Table 1.
Differences between gender in demographic and clinical data of medical students
| Overall (n=694) | P | 1st year (n=286) | P | 4th year (n=209) | P | 6th year (n=199) | P | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||||||
| Female (n=422) | Male (n=272) | Female (n=167) | Male (n=119) | Female (n=132) | Male (n=77) | Female (n=123) | Male (n=76) | |||||
| Age (years)* | 22 (4) | 22 (4) | 0.272 | 19 (1) | 19 (1) | 0.925 | 23 (1) | 23 (1) | 0.328 | 25 (1) | 24 (1) | 0.270 |
| BDI-sf* | 5 (8) | 4 (6) | 0.046 | 4 (5) | 4 (5) | 0.704 | 7 (6.75) | 4 (5) | 0.004 | 7 (8) | 5 (8.50) | 0.450 |
| BDI-sf§ | ||||||||||||
| None | 189 (44.8) | 140 (51.5) | 0.329 | 100 (59.9) | 67 (56.3) | 0.906 | 40 (30.3) | 41 (53.2) | 0.009 | 49 (39.8) | 32 (42.1) | 0.228 |
| Mild | 88 (20.9) | 55 (20.2) | 33 (19.8) | 25 (21.0) | 36 (27.3) | 13 (16.9) | 19 (15.4) | 17 (22.4) | ||||
| Moderate | 121 (28.7) | 64 (23.5) | 32 (19.2) | 26 (21.8) | 46 (34.8) | 21 (27.3) | 43 (35.0) | 17 (22.4) | ||||
| Severe | 24 (5.7) | 13 (4.8) | 2 (1.2) | 1 (0.8) | 10 (7.6) | 2 (2.6) | 12 (9.8) | 10 (13.2) | ||||
| STAI-S* | 45 (20) | 40 (17) | <0.001 | 44 (18) | 41 (18) | 0.178 | 45 (19.75) | 38 (18.50) | 0.003 | 48 (22) | 41.5 (17.75) | 0.002 |
| STAI-S§ | ||||||||||||
| Above cutoff | 284 (67.3) | 144 (52.9) | <0.001 | 105 (62.9) | 70 (58.8) | 0.539 | 84 (63.6) | 32 (41.6) | 0.002 | 95 (77.2) | 42 (55.3) | 0.002 |
| STAI-T* | 47 (17) | 42.5 (19) | 0.001 | 46 (15) | 44 (18) | 0.362 | 49 (16.75) | 41 (16) | 0.001 | 47 (20) | 43.5 (24) | 0.068 |
| PSS* | 21 (11) | 17 (10) | <0.001 | 20 (10) | 18 (11) | 0.041 | 23 (9) | 17 (8.50) | <0.001 | 21 (10) | 17 (10) | 0.004 |
| PSS§ | ||||||||||||
| Low | 71 (16.8) | 78 (28.7) | <0.001 | 36 (21.6) | 37 (31.1) | 0.202 | 17 (12.9) | 19 (24.7) | <0.001 | 18 (14.6) | 22 (28.9) | 0.046 |
| Moderate | 256 (60.7) | 159 (58.5) | 107 (64.1) | 67 (56.3) | 69 (52.3) | 49 (63.6) | 80 (65.0) | 43 (56.6) | ||||
| High | 95 (22.5) | 35 (12.9) | 24 (14.4) | 15 (12.6) | 46 (34.8) | 9 (11.7) | 25 (20.3) | 11 (14.5) | ||||
| Psychiatric drugs§ | ||||||||||||
| Yes | 38 (9.0) | 25 (9.2) | 1.000 | 3 (1.8) | 2 (1.7) | 1.000 | 8 (6.1) | 2 (2.6) | 0.327 | 27 (22.0) | 21 (27.6) | 0.396 |
| No | 384 (91.0) | 247 (90.8) | 164 (98.2) | 117 (98.3) | 124 (93.9) | 75 (97.4) | 96 (78.0) | 55 (72.4) | ||||
| Stimulants§ | ||||||||||||
| Yes | 17 (4.0) | 7 (2.6) | 0.396 | 12 (7.2) | 4 (3.4) | 0.199 | 1 (0.8) | 1 (1.3) | 1.000 | 4 (3.3) | 2 (2.6) | 1.000 |
| No | 405 (96.0) | 265 (97.4) | 155 (92.8) | 115 (96.6) | 131 (99.2) | 76 (98.7) | 119 (96.7) | 74 (97.4) | ||||
*Data are reported as median (IQR), §Data are reported as n (%). BDI-sf=Beck depression inventory-short form, STAI-T=State-trait anxiety inventory-trait, STAI-S=State-trait anxiety inventory-state, PSS=Perceived stress scale, IQR=Interquartile range
To examine the role of gender and year of study as predictors of depression, anxiety, and stress levels, two-way ANOVAs were conducted for each dependent variable. As regards the BDI-sf, ANOVA yielded a significant effect of both gender (F (1, 688) = 4.181, P = 0.041; η2 p = 0.006) and year of study (F (2, 688) = 20.951, P < 0.001; η2 p = 0.057). The interaction between year group and gender was not statistically significant (F (2, 688) = 2.477, P = 0.085; η2 p = 0.007). Planned post hoc analyses of simple main effects showed that, in both male and female students, depression levels were significantly higher in those in their 6th year compared with those in their 1st year of study. With regard to depression levels in the 4th-year students, only the scores relating to female students were significantly higher in comparison with 1st-year students of the same sex [Table 2 and Figure 1].
Table 2.
Depression, anxiety, and stress differences between the years of study for female and male medical students
| Variable | Gender | I | J | Mean differences (J−I) | 95% CI for mean differences | P | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Inferior limit | Superior limit | ||||||
| BDI-sf | Female | 1st year | 4th year | 2.943* | 1.548 | 4.303 | <0.0001 |
| 6th year | 3.064* | 1.677 | 4.451 | <0.0001 | |||
| 4th year | 6th year | 0.120 | −1.343 | 1.583 | 1.000 | ||
| Male | 1st year | 4th year | 0.958 | −0.749 | 2.665 | 0.536 | |
| 6th year | 2.610* | 0.896 | 4.324 | 0.001 | |||
| 4th year | 6th year | 1.652 | −0.235 | 3.540 | 0.108 | ||
| STAI-S | Female | 1st year | 4th year | 0.161 | −3.360 | 3.681 | 1.000 |
| 6th year | 4.341* | 0.749 | 7.392 | 0.012 | |||
| 4th year | 6th year | 4.180* | 0.392 | 7.968 | 0.025 | ||
| Male | 1st year | 4th year | −3.486 | −7.907 | 0.935 | 0.177 | |
| 6th year | −0.006 | −4.444 | 4.433 | 1.000 | |||
| 4th year | 6th year | 3.480 | −1.480; | 8.368 | 0.264 | ||
| STAI-T | Female | 1st year | 4th year | 2.925 | −0.390 | 6.241 | 0.104 |
| 6th year | 2.498 | −0.884 | 5.881 | 0.230 | |||
| 4th year | 6th year | −0.427 | −3.995 | 3.140 | 1.000 | ||
| Male | 1st year | 4th year | −1.135 | −5.299 | 3.028 | 1.000 | |
| 6th year | 0.368 | −3.812 | 4.548 | 1.000 | |||
| 4th year | 6th year | 1.503 | −3.009 | 6.106 | 1.000 | ||
| PSS | Female | 1st year | 4th year | 3.727* | 1.779 | 5.674 | <0.0001 |
| 6th year | 1.258 | −0.729 | 3.245 | 0.388 | |||
| 4th year | 6th year | −2.469* | −4.564 | −0.373 | 0.015 | ||
| Male | 1st year | 4th year | 0.339 | −2.107 | 2.785 | 1.000 | |
| 6th year | 0.153 | −2.303 | 2.608 | 1.000 | |||
| 4th year | 6th year | −0.187 | −2.891 | 2.517 | 1.000 | ||
*Statistically significant. N female: 1st year=167, 4th year=132, 6th year=123, N male: 1st year=119, 4th year=77, 6th year=76. BDI-sf=Beck depression inventory-short form, STAI-T=State-trait anxiety inventory-trait, STAI-S=State-trait anxiety inventory-state, PSS=Perceived stress scale
Figure 1.
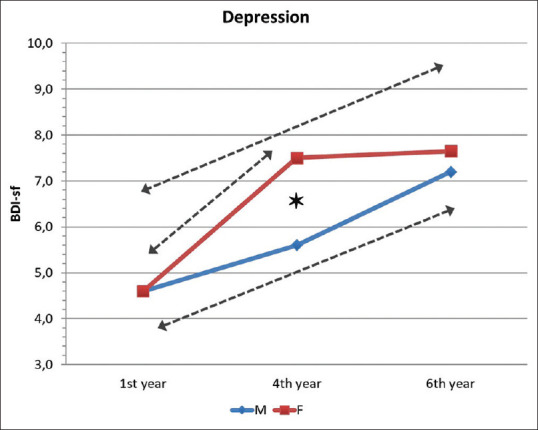
Gender and year group differences in depression. <–––>Statistically significant differences between year of study. *Statistically significant difference between genders
As regards STAI-S, ANOVA yielded a significant effect of gender (F (1, 688) = 19.944, P < 0.001; η2 p = 0.028) and year group (F (2, 688) = 4.444, P = 0.012; η2 p = 0.013). The interaction between group and gender was not statistically significant (F (2, 688) = 2.057, P = 0.129; η2 p = 0.006).
Planned post hoc analyses showed that there were no significant differences between the three year groups for the male respondents, whereas significant differences existed between 1st-and 6th-year female students and between 4th and 6th-year female students [Table 2 and Figure 2].
Figure 2.
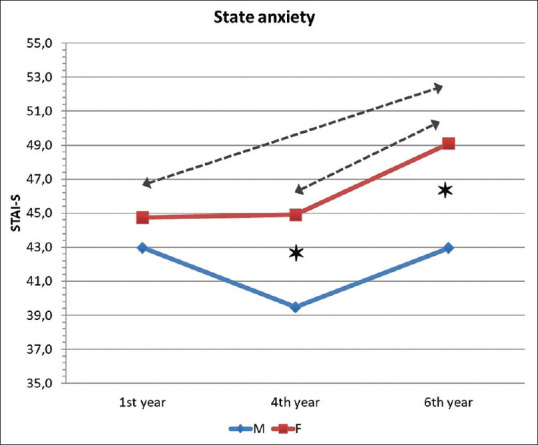
Gender and year group differences in state anxiety. <–––>Statistically significant differences between year of study. *Statistically significant differences between genders
As for STAI-T, ANOVA yielded a significant effect of gender (F (1, 688) = 11.140, P = 0.001; η2 p = 0.016), while the effect of year group (F (2, 688) = 0.867, P = 0.421; η2 p = 0.003) and the interaction between year group and gender were not statistically significant (F (2, 688) = 1.701, P = 0.183; η2 p = 0.005). Planned post hoc analyses of simple main effects showed that there were no significant differences among the three year groups for either females or males [Table 2 and Figure 3].
Figure 3.
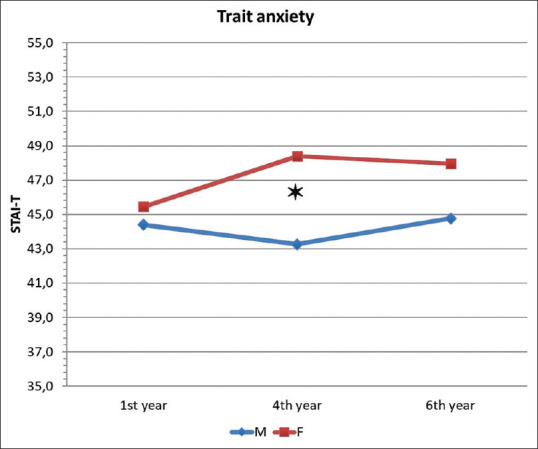
Gender differences in trait anxiety. *Statistically significant difference between genders
Regarding PSS, ANOVA yielded a significant effect of gender (F (1, 688) = 36.543, P < 0.001; η2 p = 0.050) and year group (F (2, 688) = 4.894, P = 0.008; η2 p = 0.014) and a significant interaction between year group and gender (F (2, 688) = 3.409, P = 0.034; η2 p = 0.010). Planned post hoc analyses of simple main effects showed no significant differences between the three year groups in males, whereas significant differences existed between the 1st- and the 4th-year female students and between the 4th- and the 6th-year female students [Table 2 and Figure 4].
Figure 4.
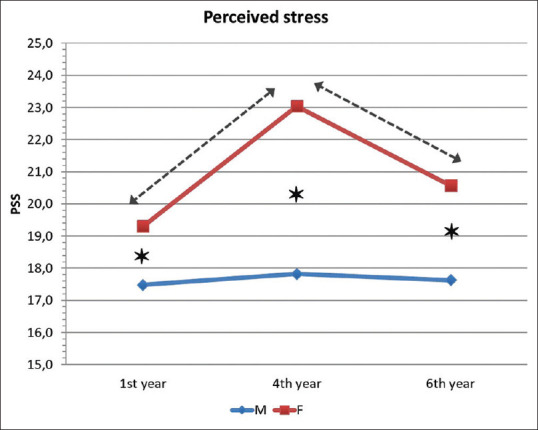
Gender and year groups’ differences in perceived stress. <–––>Statistically significant differences between year of study. *Statistically significant differences between genders
Finally, no statistically significant differences were found between gender with regard to the proportion of students reporting to have used psychiatric drugs or stimulants for all three year groups analyzed. However, the percentages of students reporting to have used psychiatric drugs or stimulants were statistically different for the 3 years of study, with different trends evident. While more 6th-year medical students reported to have used psychiatric drugs compared with 1st-year students, the use of stimulants was more common among 1st-year students compared those in their 4th year of study.
Discussion
Overall, students reported a high prevalence of depression, anxiety, and perceived stress levels, similar to those reported by previous studies[1,3] and higher than the Italian general population.[33,34] Differences between gender and between year of study were found for depression, state anxiety, and perceived stress levels, similarly to previous studies.[3,5,19]
In general, women are more likely to develop depression than men.[35] Our results are in line with previous studies that have found higher levels of depression in female than in male students.[3,10,19,21] The higher rate of depressive symptoms found among students more advanced in their year of study could be linked to employment pressure, as 6th-year students are also approaching a period of transition and thus uncertainty about the future.
As expected, trait anxiety levels were found to be similar across the 3 years of study and without any difference between the two genders. Trait anxiety is a rather stable personality trait, and previous studies reported no gender differences in trait anxiety,[22] but it could correlate with how susceptible a student is toward depression as well as its persistence during medical training.[18] On the contrary, state anxiety levels were found to be different between male and female medical students and significantly greater in 6th-year female students compared with those in their 1st and 4th years. This result may reflect anxiety related to the final exam, the conclusion of the course of study and uncertainty about the future.
As regards perceived stress, female medical students reported higher stress levels than males in all the 3 years of study considered. Moreover, slightly higher stress levels were noted in the female students in their 4th year of study compared with 1st and 6th years. However, it is important to note that while these differences were statistically significant, they were not clinically meaningful since perceived stress scores remained within the “moderate” range in both genders.
No gender differences were found in the use of psychiatric drugs and stimulants. The rate of psychotropic medication use was found to be similar to that reported by other studies,[29,36] whereas the use of cognitive enhancers was less frequent.[28,29] The most frequent use of psychiatric drugs in the 6th year of study may be interpreted as a use of self-medication for higher levels of depression and anxiety or related to less stigmatization toward mental health problems and their medications by this year group.[37]
In summary, our findings provide evidence that levels of emotional stress in medical students increase as they progress through their medical training. The trend was steeper in female students with respect to depression and only present in females in relation to anxiety. Perceived stress levels showed an increase in the first 4 years, followed by a drop at the end of medical training in female students only, whereas male students presented similar levels across all the years analyzed.
The findings of this study suggest that the relationship between gender, year of study, and emotional distress among medical students should be investigated further. In fact, the inconsistencies between our findings and those reported by previous studies, who did not report any differences between gender or year of study with regard to emotional distress in medical students, could be due to different cultural and social environments and/or dissimilar medical education curricula.
As shown by previous studies, not only is emotional distress in medical students associated with poor academic performance and quality of life,[2] but also with a lack of empathy[20] and burnout symptoms,[38] which, as a result, affect the quality of doctor–patient relationships. Other studies have provided preliminary evidence of gender differences in empathy and burnout in medical students.[20,39] Future studies should continue to investigate the effect of gender on these outcomes. Furthermore, gender differences could be considered when planning interventions aimed at preventing or improving emotional distress in this population.
Limitation and recommendation
This study has several limitations. As this study has a cross-sectional design, it is only possible to describe associations between the variables studied. Moreover, variations between the years of study could be related to intrinsic differences between the groups of students and not to an actual increase/decrease in symptoms over time. As this study was conducted at a single university, the results cannot be generalized to the overall Italian medical student population. Future multicenter longitudinal cohort studies with multiple assessment points would be needed to investigate the trajectories of emotional distress along the medical training path better. Another limitation is characterized by the different methods of questionnaire administration (i.e., paper and pencil vs. online administration), which could have affected response rates and the self-selection of respondents. Further, the questions regarding psychiatric drug and stimulants were too limited to investigate this issue properly. Future studies should specifically evaluate possible gender differences in the use and abuse of such substances and their association with psychological distress. Finally, the lack of a control group prevents comparisons with other groups of students to understand whether distress symptoms affect only medical students or are common to university students, in general.
This study has also some strength. This study represents the first attempt in Italy to simultaneously evaluate different components of emotional distress (i.e., depression, anxiety, and perceived stress) across three different groups of medical students, also considering gender differences.
Conclusion
This study reports high prevalence rates of depression, anxiety, and stress among medical students and provides preliminary evidence of gender differences in depression, anxiety, and stress levels among Italian medical students during their first, middle, and last year of study. Future studies should investigate further the role of gender on emotional distress trajectories in students during their medical training, identify the possible differences in risk factors, and offer some effective interventions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank the students for their participation in the study. They also wish to thank Luca Cominu for his contribution and Stephanie Parsley for the proofreading of the manuscript.
References
- 1.Quek TT, Tam WW, Tran BX, Zhang M, Zhang Z, Ho CS, et al. The global prevalence of anxiety among medical students: A meta-analysis. Int J Environ Res Public Health. 2019;16:2735. doi: 10.3390/ijerph16152735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81:354–73. doi: 10.1097/00001888-200604000-00009. [DOI] [PubMed] [Google Scholar]
- 3.Hope V, Henderson M. Medical student depression, anxiety and distress outside North America: A systematic review. Med Educ. 2014;48:963–79. doi: 10.1111/medu.12512. [DOI] [PubMed] [Google Scholar]
- 4.Elzubeir MA, Elzubeir KE, Magzoub ME. Stress and coping strategies among Arab medical students: Towards a research agenda. Educ Health (Abingdon) 2010;23:355. [PubMed] [Google Scholar]
- 5.Mao Y, Zhang N, Liu J, Zhu B, He R, Wang X. A systematic review of depression and anxiety in medical students in China. BMC Med Educ. 2019;19:327. doi: 10.1186/s12909-019-1744-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zeng W, Chen R, Wang X, Zhang Q, Deng W. Prevalence of mental health problems among medical students in China: A meta-analysis. Medicine (Baltimore) 2019;98:e15337. doi: 10.1097/MD.0000000000015337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Puthran R, Zhang MW, Tam WW, Ho RC. Prevalence of depression amongst medical students: A meta-analysis. Med Educ. 2016;50:456–68. doi: 10.1111/medu.12962. [DOI] [PubMed] [Google Scholar]
- 8.Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: A systematic review and meta-analysis. JAMA. 2016;316:2214–36. doi: 10.1001/jama.2016.17324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pacheco JP, Giacomin HT, Tam WW, Ribeiro TB, Arab C, Bezerra IM, et al. Mental health problems among medical students in Brazil: A systematic review and meta-analysis. Braz J Psychiatry. 2017;39:369–78. doi: 10.1590/1516-4446-2017-2223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mahroon ZA, Borgan SM, Kamel C, Maddison W, Royston M, Donnellan C. Factors associated with depression and anxiety symptoms among medical students in Bahrain. Acad Psychiatry. 2018;42:31–40. doi: 10.1007/s40596-017-0733-1. [DOI] [PubMed] [Google Scholar]
- 11.Pham T, Bui L, Nguyen A, Nguyen B, Tran P, Vu P, et al. The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PLoS One. 2019;14:e0221432. doi: 10.1371/journal.pone.0221432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Damiano RF, de Oliveira IN, Ezequiel OD, Lucchetti AL, Lucchetti G. The root of the problem: Identifying major sources of stress in Brazilian medical students and developing the Medical Student Stress Factor Scale. Braz J Psychiatry. 2020;43:35–42. doi: 10.1590/1516-4446-2019-0824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Manjareeka M, Yadav S. Predictors of high achievers in Indian medical undergraduates: Association with emotional intelligence and perceived stress. J Educ Health Promot. 2020;9:202. doi: 10.4103/jehp.jehp_263_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Roncero C, Egido A, Rodríguez-Cintas L, Pérez-Pazos J, Collazos F, Casas M. Substance use among medical students: A literature review 1988- 2013. Actas Esp Psiquiatr. 2015;43:109–21. [PubMed] [Google Scholar]
- 15.MacLean L, Booza J, Balon R. The impact of medical school on student mental health. Acad Psychiatry. 2016;40:89–91. doi: 10.1007/s40596-015-0301-5. [DOI] [PubMed] [Google Scholar]
- 16.Alebachew W, Semahegn A, Ali T, Mekonnen H. Prevalence, associated factors and consequences of substance use among health and medical science students of Haramaya University, eastern Ethiopia, 2018: A cross-sectional study. BMC Psychiatry. 2019;19:343. doi: 10.1186/s12888-019-2340-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jafari N, Loghmani A, Montazeri A. mental health of medical students in different levels of training. Int J Prev Med. 2012;3:S107–12. [PMC free article] [PubMed] [Google Scholar]
- 18.Silva V, Costa P, Pereira I, Faria R, Salgueira AP, Costa MJ, et al. Depression in medical students: Insights from a longitudinal study. BMC Med Educ. 2017;17:184. doi: 10.1186/s12909-017-1006-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Steiner-Hofbauer V, Holzinger A. How to cope with the challenges of medical education.Stress, depression, and coping in undergraduate medical students? Acad Psychiatry. 2020;44:380–7. doi: 10.1007/s40596-020-01193-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Worly B, Verbeck N, Walker C, Clinchot DM. Burnout, perceived stress, and empathic concern: Differences in female and male Millennial medical students. Psychol Health Med. 2019;24:429–38. doi: 10.1080/13548506.2018.1529329. [DOI] [PubMed] [Google Scholar]
- 21.Brenneisen Mayer F, Souza Santos I, Silveira PS, Itaqui Lopes MH, de Souza AR, Campos EP, et al. Factors associated to depression and anxiety in medical students: A multicenter study. BMC Med Educ. 2016;16:282. doi: 10.1186/s12909-016-0791-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cipra C, Müller-Hilke B. Testing anxiety in undergraduate medical students and its correlation with different learning approaches. PLoS One. 2019;14:e0210130. doi: 10.1371/journal.pone.0210130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shokrpour N, Bazrafcan L, Ardani AR, Nasiraei S. The factors affecting academic burnout in medical students of Mashahd University of Medical Sciences in 2013-2015. J Educ Health Promot. 2020;9:232. doi: 10.4103/jehp.jehp_83_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Karimi N, Saadat-Gharin S, Tol A, Sadeghi R, Yaseri M, Mohebbi B. A problem-based learning health literacy intervention program on improving health-promoting behaviors among girl students. J Educ Health Promot. 2019;8:251. doi: 10.4103/jehp.jehp_476_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Papazisis G, Siafis S, Tsakiridis I, Koulas I, Dagklis T, Kouvelas D. Prevalence of cannabis use among medical students: A systematic review and meta-analysis. Subst Abuse. 2018;12:1178221818805977. doi: 10.1177/1178221818805977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bert F, Lo Moro G, Corradi A, Acampora A, Agodi A, Brunelli L, et al. Prevalence of depressive symptoms among Italian medical students: The multicentre cross-sectional “PRIMES” study. PLoS One. 2020;15:e0231845. doi: 10.1371/journal.pone.0231845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Messina G, Quercioli C, Troiano G, Russo C, Barbini3 E, Nisticò F, et al. Italian medical students quality of life: Years 2005-2015. Ann Ig. 2016;28:245–51. doi: 10.7416/ai.2016.2103. [DOI] [PubMed] [Google Scholar]
- 28.Pighi M, Pontoni G, Sinisi A, Ferrari S, Mattei G, Pingani L, et al. Use and propensity to use substances as cognitive enhancers in Italian medical students. Brain Sci. 2018;8:197. doi: 10.3390/brainsci8110197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Volpe U, Ventriglio A, Bellomo A, Kadhum M, Lewis T, Molodynski A, et al. Mental health and wellbeing among Italian medical students: A descriptive study. Int Rev Psychiatry. 2019;31:569–73. doi: 10.1080/09540261.2019.1654718. [DOI] [PubMed] [Google Scholar]
- 30.Beck AT, Beck RW. Screening depressed patients in family practice. A rapid technic. Postgrad Med. 1972;52:81–5. doi: 10.1080/00325481.1972.11713319. [DOI] [PubMed] [Google Scholar]
- 31.Spielberger C. Manual for the State-Trait Anxiety Inventory (STAI) (Form Y: Self-Evaluation Questionnaire) Redwood City, CA: Mind Garden; 1983. [Google Scholar]
- 32.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–96. [PubMed] [Google Scholar]
- 33.Binkin N, Gigantesco A, Ferrante G, Baldissera S. Depressive symptoms among adults 18-69 years in Italy: Results from the Italian behavioural risk factor surveillance system, 2007. Int J Public Health. 2010;55:479–88. doi: 10.1007/s00038-009-0106-y. [DOI] [PubMed] [Google Scholar]
- 34.Istat. Mental Health at Various Stages of Life. 2018. [Last accessed on 2020 May 24]. Available from: https://www.istat.it/en/archivio/219812 .
- 35.Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry. 2017;4:146–58. doi: 10.1016/S2215-0366(16)30263-2. [DOI] [PubMed] [Google Scholar]
- 36.Ribeiro AG, Cruz LP, Marchi KC, Tirapelli CR, Miasso AI. Antidepressants: Use, adherence and awareness among medical students. Cien Saude Colet. 2014;19:1825–33. doi: 10.1590/1413-81232014196.06332013. [DOI] [PubMed] [Google Scholar]
- 37.Nalçakan AD, Şahin EA, Yalcinkaya OK, Ak S. Antidepressant awareness and stigmatizing attitudes toward depression and antidepressants, a comparison between first and sixth-year medical students. Int J Soc Psychiatry 2021. 2021 Jan 5;:20764020985545. doi: 10.1177/0020764020985545. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 38.Altannir Y, Alnajjar W, Ahmad SO, Altannir M, Yousuf F, Obeidat A, et al. Assessment of burnout in medical undergraduate students in Riyadh, Saudi Arabia. BMC Med Educ. 2019;19:34. doi: 10.1186/s12909-019-1468-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Leombruni P, Di Lillo M, Miniotti M, Picardi A, Alessandri G, Sica C, et al. Measurement properties and confirmatory factor analysis of the Jefferson Scale of Empathy in Italian medical students. Perspect Med Educ. 2014;3:419–30. doi: 10.1007/s40037-014-0137-9. [DOI] [PMC free article] [PubMed] [Google Scholar]