

This cohort study identifies baseline predictors of COVID-19 pandemic experiences, as defined by both child and parent report, using data from the Adolescent Brain and Cognitive Development cohort.
Key Points
Question
What baseline pre–COVID-19 pandemic household factors are associated with COVID-19 experiences as reported by approximately 10 000 children and their parents?
Findings
In this study of 9267 youth-parent dyads, of more than 17 000 variables, social determinants of inequity, including household income and family structure, emerged as the primary correlates of negative COVID-19 experiences, including increased difficulties with school among children and concerns over racism associated with the COVID-19 pandemic among parents.
Meaning
Community-level, transgenerational intervention strategies may be needed to combat the disproportionate burden of pandemics on minoritized and marginalized racial and ethnic populations.
Abstract
Importance
The experienced consequences of the COVID-19 pandemic have diverged across individuals, families, and communities, resulting in inequity within a host of factors. There is a gap of quantitative evidence about the transgenerational impacts of these experiences and factors.
Objective
To identify baseline predictors of COVID-19 experiences, as defined by child and parent report, using a multivariate pattern-learning framework from the Adolescent Brain and Cognitive Development (ABCD) cohort.
Design, Setting, and Participants
ABCD is an ongoing prospective longitudinal study of child and adolescent development in the United States including 11 875 youths, enrolled at age 9 to 10 years. Using nationally collected longitudinal profiling data from 9267 families, a multivariate pattern-learning strategy was developed to identify factor combinations associated with transgenerational costs of the ongoing COVID-19 pandemic. ABCD data (release 3.0) collected from 2016 to 2020 and released between 2019 and 2021 were analyzed in combination with ABCD COVID-19 rapid response data from the first 3 collection points (May-August 2020).
Exposures
Social distancing and other response measures imposed by COVID-19, including school closures and shutdown of many childhood recreational activities.
Main Outcomes and Measures
Mid–COVID-19 experiences as defined by the ABCD’s parent and child COVID-19 assessments.
Results
Deep profiles from 9267 youth (5681 female [47.8%]; mean [SD] age, 119.0 [7.5] months) and their caregivers were quantitatively examined. Enabled by a pattern-learning analysis, social determinants of inequity, including family structure, socioeconomic status, and the experience of racism, were found to be primarily associated with transgenerational impacts of COVID-19, above and beyond other candidate predictors such as preexisting medical or psychiatric conditions. Pooling information across more than 17 000 baseline pre–COVID-19 family indicators and more than 280 measures of day-to-day COVID-19 experiences, non-White (ie, families who reported being Asian, Black, Hispanic, other, or a combination of those choices) and/or Spanish-speaking families were found to have decreased resources (mode 1, canonical vector weight [CVW] = 0.19; rank 5 of 281), escalated likelihoods of financial worry (mode 1, CVW = −0.20; rank 4), and food insecurity (mode 1, CVW = 0.21; rank 2), yet were more likely to have parent-child discussions regarding COVID-19–associated health and prevention issues, such as handwashing (mode 1, CVW = 0.14; rank 9), conserving food or other items (mode 1, CVW = 0.21; rank 1), protecting elderly individuals (mode 1, CVW = 0.11; rank 21), and isolating from others (mode 1, CVW = 0.11; rank 23). In contrast, White families (mode 1, CVW = −0.07; rank 3), those with higher pre–COVID-19 income (mode 1, CVW = −0.07; rank 5), and presence of a parent with a postgraduate degree (mode 1, CVW = −0.06; rank 14) experienced reduced COVID-19–associated impact. In turn, children from families experiencing reduced COVID-19 impacts reported longer nighttime sleep durations (mode 1, CVW = 0.13; rank 14), less difficulties with remote learning (mode 2, CVW = 0.14; rank 7), and decreased worry about the impact of COVID-19 on their family’s financial stability (mode 1, CVW = 0.134; rank 13).
Conclusions and Relevance
The findings of this study indicate that community-level, transgenerational intervention strategies may be needed to combat the disproportionate burden of pandemics on minoritized and marginalized racial and ethnic populations.
Introduction
COVID-19 and associated response measures to mitigate spread of the virus will have considerable mental health and psychosocial consequences for years to come that will have significant public health impact.1,2 In youth, important sequelae of the COVID-19 pandemic, direct and indirect, will include profound developmental, educational, and social impacts.3 Critically, these developmental events will likely vary as a function of individual (child), familial (parental, transgenerational), and region-level (community, state) factors. While multiple studies have assessed specific COVID-19 impacts on adults and youth,4,5,6 separately, very little is known about the transgenerational effects of this ongoing public health crisis. In addition, while COVID-19 is acknowledged to have widened health disparities,7,8 little is known about baseline predictors of such inequities, particularly at the level of family systems.
Here, we use data from the ongoing Adolescent Brain and Cognitive Development (ABCD) cohort,9 a data collection initiative of unprecedented size and scope, to characterize transgenerational features of COVID-19 pandemic experiences, as defined by child and parent report. We use a multivariate pattern learning approach to identify links across clusters of pre–COVID-19 child and parent demographic and clinical features, as assessed using approximately 6000 deep-profiling assessments, corresponding with more than 17 000 individual items at baseline, and clusters of COVID-19–associated child and parent experiences. This strategy is entirely data driven and offers a comprehensive set of transgenerational social, demographic, health, and community factors, enabling identification of complex multifaceted contributors of day-to-day COVID-19 experiences. Our approach also enables direct comparison between traditional items (eg, stress, engagement with social services) and less traditional items (eg, pet ownership, social media use), with simultaneous assessment of factors that characterize COVID-19 pandemic experiences at the levels of the individual, family, and community.
Methods
Participants and Study Design
Data were collected as part of the ongoing ABCD cohort initiative. This data aggregation collaboration from across the US is funded by the US National Institutes of Health and is anticipated to revolutionize our understanding of neurodevelopmental trajectories.10 However, children in this cohort are now facing a developmental challenge unique to their generation because they are entering adolescence during a time of heightened nationwide mental and psychosocial stress and uncertainty due to the COVID-19 pandemic. The availability of baseline, pre–COVID-19 data from this cohort therefore provides an unprecedented opportunity to quantify transgenerational predictors of COVID-19 experiences.
All protocols for ABCD are approved by either a central or site-specific institutional review board committee.11 Caregivers have provided written, informed consent and children provide verbal assent to all research protocols.12 Additional details on the ABCD study are in the eMethods in the Supplement. Data were downloaded in March 2021 under National Institute of Mental Health Data Archive use agreement #785. Full ABCD baseline data, collected between 2016 and 2018, was downloaded via the RDS 3.0 file (#1042). Methods follow Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) reporting guidelines for prognostic studies.
Baseline Characteristics of the Family System: Pre–COVID-19 Assessments
The ABCD study’s baseline assessment includes comprehensive measures across child and parent domains including self-report measures of race and ethnicity, demographic, and socioeconomic measures; measures of child physical and mental health; family psychiatric histories; trait measures; neurocognitive performance; and child culture and environment measures. These and other indicators were captured at baseline using more than 6000 deep-profiling assessments (corresponding with more than 17 000 individual items).
Mid–COVID-19 Characteristics of the Family System: COVID-19 Assessments
In rapid response to the evolving pandemic, the ABCD consortium developed COVID-19 questionnaires (eTables 2 and 3 in the Supplement). This battery includes both youth self-report and parent report forms, comprising a total of 281 items. Questions for parents were available in English or Spanish, whereas youth assessments are only available in English. COVID-19 assessments covered multiple dimensions: school attendance and activities, family stressors, access to needs, social distancing, attitudes, change in routine, sleep, physical activity, screen time, mental health, and physical health symptoms, including self-report of COVID-19 infection. Data from COVID-19 assessments collected between May and August 2020 were recently released and are available for 9268 family dyads, corresponding with approximately 84% of the baseline sample (approximate n = 11 000). Comparisons of children from families with (n = 9267) and without (n = 2608) COVID-19 data indicated no significant differences in age (months) or sex. More comprehensive demographic details are provided in eTable 1 in the Supplement.
Multivariate Pattern Analysis Workflow
Data cleaning steps and the primary Python programming code for all analysis is provided in the eMethods in the Supplement. Our analysis aimed to identify dominant modes of population variation that provide insight into how baseline questionnaire items can explain COVID-19 questionnaire items. A first variable set X was constructed from the clean baseline items (9267 × 6402 matrix), and a second variable set Y was constructed from the COVID-19 items (9267 × 281 matrix). We elected canonical correlation analysis (CCA) as a multivariate pattern learning approach that is ideally suited to delineate cross-associations between 2 high-dimensional variable sets.13,14 CCA involves finding the canonical vectors u and v that maximize the symmetric association between a linear combination of X (deep profiling of each family at baseline) and a linear combination of Y (child and parent impact assessments during COVID-19). The ensuing set of k orthogonal modes of variation were uncorrelated with each other and naturally ordered from the most to least important baseline COVID-19 projections. Therefore, the first and strongest mode explained the largest fraction of covariance between baseline profiling and COVID-19 impact assessment. Each particular mode captured a fraction of COVID-19 pandemic variation that was not explained by one of the k − 1 other modes. In this way, CCA thus identified the 2 projections Xu and Yv that yield maximal linear cross-associations between multidimensional facets of the family system at the outset and measures of coping during the public health crisis.
Each identified CCA mode was entered into statistical significance tests of robustness as determined by hypothesis testing in a nonparametric permutation, consistent with prior work.15,16,17 Relying on minimal modeling assumptions, a valid null distribution was derived for the achieved association between canonical variates distilled from CCA analysis. In 1000 permutation iterations, the COVID-19 assessment matrix was held constant, while the baseline profiling matrix was subject to participantwise random shuffling. The constructed surrogate matrices preserved the statistical structure idiosyncratic to the data yet permitted selectively removing the signal property associated with the CCA test statistic to be evaluated for robustness.18 Thus, the generated empirical distribution reflected the null hypothesis of random association between baseline profiling and COVID-19 impact across families. In each iteration, we record the Pearson correlations r between the perturbed canonical vectors. P values were obtained from the number of correlations r from the null CCA model that yielded k = 9 highly significant CCA modes, where explicit correction for multiple comparisons was carried out searching through all estimated CCA modes (P < .010, familywise-error corrected).
Predictive Annotation of Baseline COVID-19 Modes: Out-of-Sample Validated Prediction
Next, as an additional validation and further annotation of the identified CCA modes, we brought to bear predictive models and validated their accuracy in unseen (ie, not previously included in the model) children and caregivers. These algorithmic tools used the information from the family-specific mode expressions (ie, how explanatory is a particular population mode for a particular family?) to predict key COVID-19 experiences. To evaluate the predictive accuracy of our CCA modes in unseen families, we used a rigorous model validation pipeline. In each of 100 iterations, a random participant selection of 9268 participants was pulled (with replacement) to obtain an alternative, perturbed version of the original data set (ie, bootstrapping). Thus, for these random selections, a given participant could occur (1) not at all, (2) once, or (3) several times. Each random selection also excluded data from roughly one-third of the families, such that data from these unseen individuals could be used for evaluation of model accuracy in new individuals (ie, whose data were not used for model building) in each iteration. A linear predictive model (generalized linear regression) was fitted on the k significant modes’ canonical variates (eg, loadings for mode 1) as input variables and the outcome of interest (eg, state vaccination rates). The mean prediction accuracy across the 100 repetitions yielded the out-of-sample estimation for the predictive model performance that we would expect to obtain in families that are new or recruited in the future. Two-sided P values were significant at less than .01.
Given the nature of the present analytical approach, statistical significance testing was carried out at the level of the population modes of baseline COVID-19 covariation. The whole population mode, with all its corresponding single-variable associations, was certified as either statistically robust or not, based on permutation-based null hypothesis testing (additional details earlier in Methods). For each such population mode exceeding the significance threshold, we then considered its single-variable associations (ie, canonical weight vector) and the relative importance of each such association (ie, rank indicating relevance relative to all other items in that canonical weight vector).17
Results
Canonical vector weights for all top-performing variables are provided in eTables 4 to 21 in the Supplement.
Multivariate Pattern Analysis
We identified 9 statistically significant signatures (modes) of how pre–COVID-19 family measures systematically covary with COVID-19 experiences. Of these, the dominant population mode 1 accounted for an explained variance, as indexed by Pearson r (also known as canonical correlation in the context of CCA) for canonical correlations, of r = 0.80 (P = .002; only 2 of 1000 permutation iterations exceeded the empirical null distribution) and the second strongest mode 2 accounted for an explained variance of r = 0.62 (P = .009; only 9 of 1000 permutation iterations exceeded the empirical null distribution) (complete CCA output and details on other modes are available19). The remaining 7 modes accounted for a much lower amount of variance (details in eTables 8-21 in the Supplement). Of the more than 17 000 diverse individual baseline items, including a myriad of measurements for child and parental mental and physical health, these first 2 cardinal modes of variation were overwhelmingly associated with social determinants of inequity including socioeconomic status, basic family structure (eg, family size, marital status), and demographic (eg, parental education) features. Post hoc analyses accounting for site effects indicated a similar pattern of results (ie, highly similar explained variances for the 9 statistically significant modes).
Mode 1: Social Determinants of Inequity Foreshadow Pandemic Experiences
Figure 1 summarizes pre–/post–COVID-19 associations revealed by mode 1. Complete data, including canonical vector weights, for top variables for mode 1 are shown in eTables 4 and 5 in the Supplement. This primary explanatory mode revealed that social determinants of inequity emerged as the primary correlates of negative COVID-19 experiences across families. At baseline, variables with the highest loading for mode 1 were associated with race and ethnicity and social determinants of inequity, such as parental education, marital status, and household income. During the COVID-19 pandemic, this mode was preferentially associated with financial insecurity, caregiver support, and parent-child interactions associated with COVID-19. The negative end of this continuum included increased likelihoods of financial worry and food insecurity among families whose parents did not endorse their race as White (ie, families who reported being Asian, Black, Hispanic, other, or a combination of those choices) and who chose to take assessments in Spanish. White families, those with higher pre–COVID-19 income, and the presence of a parent with a postgraduate degree experienced reduced COVID-19–associated impact, as indicated by factors including decreased food insecurity and financial worry. This end of the continuum was also anchored in a host of supportive factors such as parental reports of a continued ability to enjoy day-to-day activities and the presence of multiple adult caregivers. In turn, familial variation on this mode was directly linked to within-family COVID-19 pandemic perceptions and behaviors: those with vulnerabilities in the social determinants (eg, those with lower household incomes) were more likely to have parent-child discussions regarding COVID-19–associated health and prevention issues, including handwashing, conserving food or other items, protecting elderly individuals, and maintaining social distancing.
Figure 1. Association of COVID-19 Pandemic Impact With Economic Disadvantage and Household Environment.
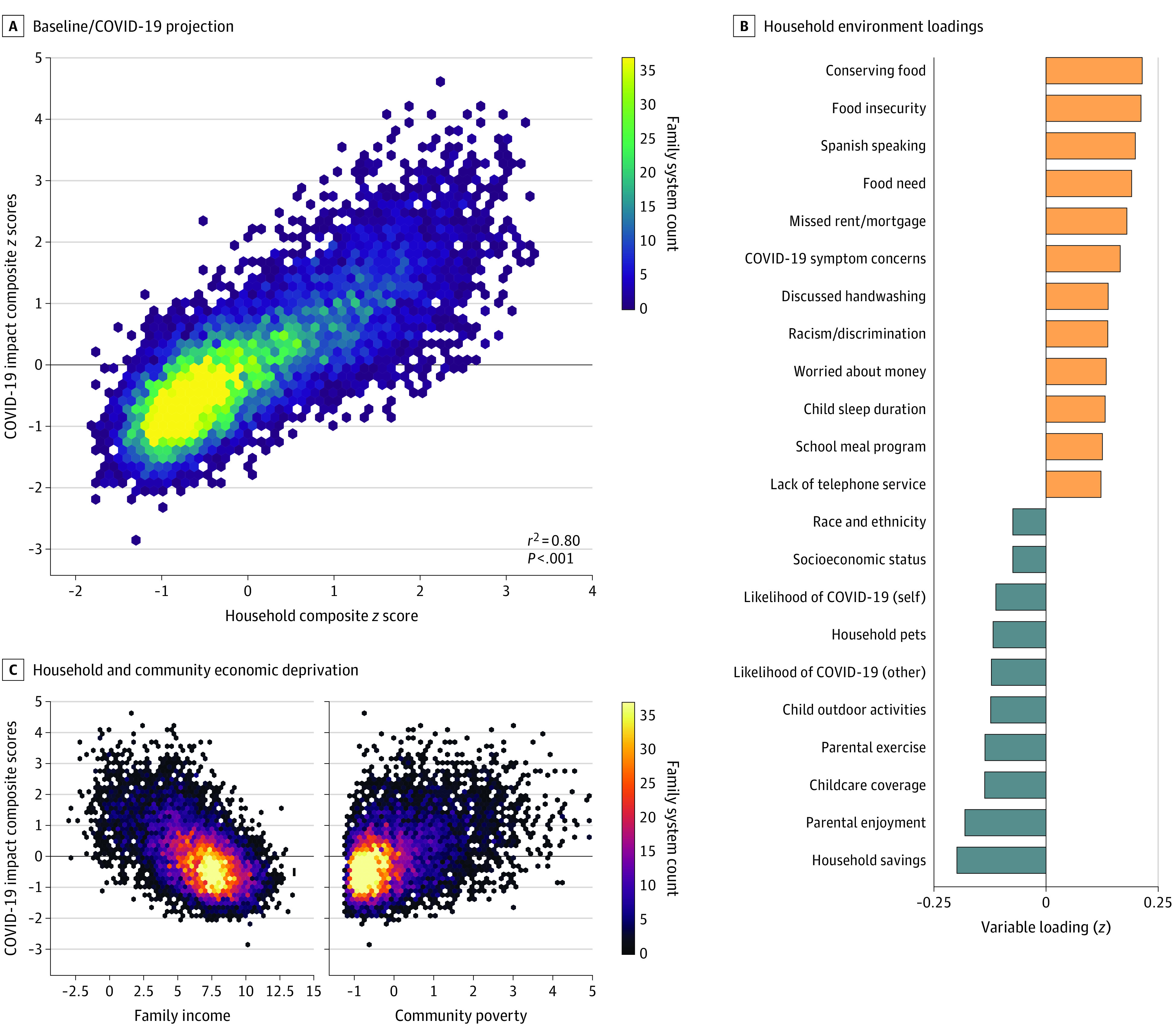
Our analysis identified cross-associations between an array of family characteristics at baseline (ie, household composite score) and subsequent COVID-19–associated experience during the pandemic (ie, COVID-19 impact scores). A, Across individual families, household environment was positively associated with COVID-19 impact composite scores of the primary mode. Modeling results are displayed in a hexagonal binning plot: scale bar reflects the number of families with the same baseline COVID-19 association. B, Household environment variable loadings from the main baseline COVID-19 association indicate a strong positive association with household economic disadvantage. The bar plot reflects the top-ranked household characteristics in families with high mode 1 expression (orange indicates positive associations; blue, negative associations). C, High COVID-19 impact is robustly linked to both lower family income (left) and increased neighborhood poverty (percentage of people below poverty level in a given community; right). For complete variable definitions, see eTables 2 and 3 in the Supplement.
This dominant mode of baseline COVID-19 covariation was further linked to experiences of racism during the COVID-19 pandemic and to worries about and experiences of financial difficulties in fulfilling food, rent, or other household expenses. In addition, this mode of population covariation was associated with several variables associated with child mental health, such that children from families without financial insecurity reported longer nighttime sleep durations and decreased worry about the impact of COVID-19 on their family. Cross-validated prediction analyses (Figure 2) further revealed that the constellation of mode 1 COVID-19 experiences within an individual family could be used to reliably predict their corresponding salary or work loss, ability to pay rent or mortgage, both parent and child concerns about becoming ill with COVID-19, tendency to socially isolate out of precaution, and their likelihood of expressing concerns of racism and racial discrimination (as indicated by positive endorsement of the statement: “I am worried that our family will experience racism or discrimination in relation to coronavirus”).
Figure 2. Economic Deprivation–Associated Household Characteristics Predict Struggle and Worry During COVID-19.
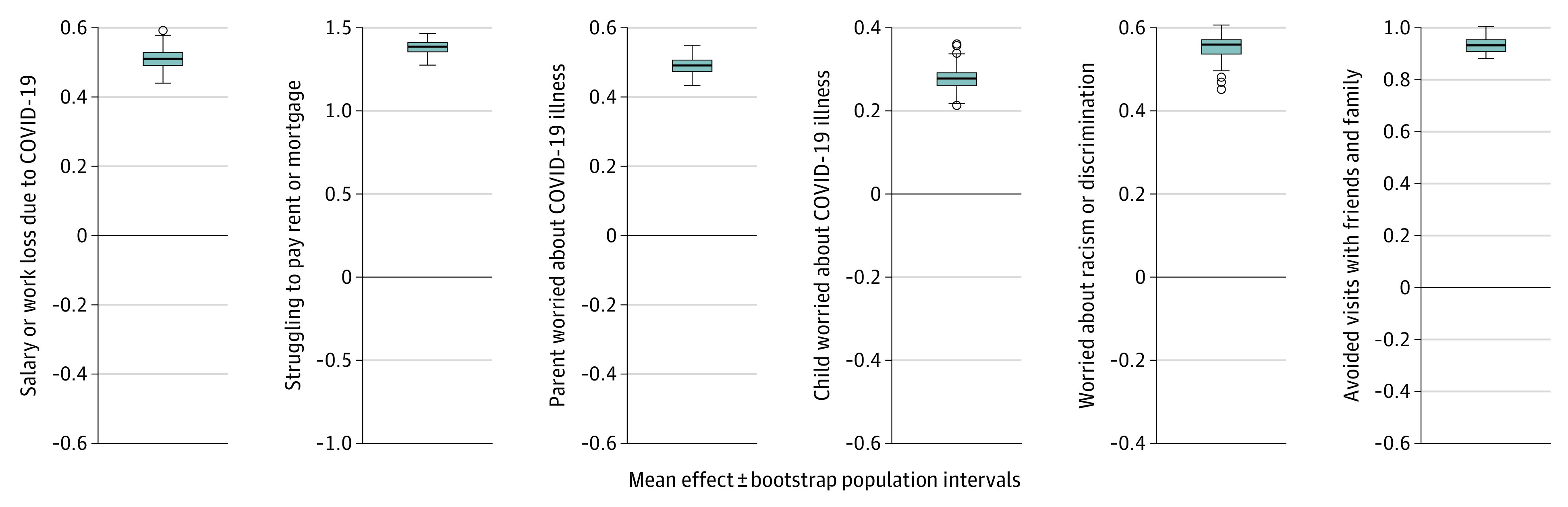
The constellation of mode 1 COVID-19 experiences within an individual family can be used to reliably predict their corresponding salary or work loss, ability to pay rent or mortgage, parent and child concerns about becoming ill with COVID-19, tendency to socially isolate out of precaution, and their tendency of expressing concerns of racism and racial discrimination. For each box plot, family data from approximately two-thirds of random family picks were used to train linear predictive models (details in Methods), which were then evaluated for prediction accuracy in approximately one-third of unseen holdout families (dispersion and whiskers). Box plots show the corresponding effect sizes, while the error bars show the robustness of the effect sizes. For complete variable definitions, see eTables 2 and 3 in the Supplement.
In summary, population mode 1 revealed that social determinants of inequity—rather than preexisting medical or psychiatric conditions—were the primary predictors of multigenerational lived COVID-19 experiences, as indexed based on the COVID-19 assessments. It further indicated that families experiencing fewer COVID-19 impacts were less likely to engage in conversations about basic public health measures with their children or to engage in/abide by social-distancing practices.
Mode 2: Family Demographics and Structure Foreshadow COVID-19 Experiences
Figure 3 summarizes pre–/post–COVID-19 associations revealed by mode 2. Complete data, including canonical vector weights, for top variables for mode 2 are shown in eTables 6 and 7 in the Supplement. This second mode of covariation highlighted pre–COVID-19 baseline factors preferentially associated with parent demographics and familial structure, including language preference, household size, marital status, and parental employment, and which further extended to encompass aspects of pre–COVID-19 child health and child screen time use. During the COVID-19 pandemic, this distinct mode was further associated with variables associated with specific consequences of COVID-19 including changes in family routines, impacts on child sleep, child health care access, child schoolwork, and child screen time, as well as childcare impacts on parental employment, household responsibilities, and parental perceptions of COVID-19 severity. Specifically, this mode indicated that parent-child dyads who were more likely to live in single-caregiver households and less likely to have a stay-at-home parent were more likely to report facing challenges balancing between childcare, work, and other responsibilities, while also expressing more worries about COVID-19 in general. In turn, children from these families were less likely to be rated by their parents as prepared for the next school year—spending more time and yet experiencing increased difficulties completing schoolwork remotely. Children from these families were also more likely to report asthma, poor sleep quality, and increased screen time use during the COVID-19 pandemic.
Figure 3. Association of Exacerbated COVID-19 Impact With Family Structure.
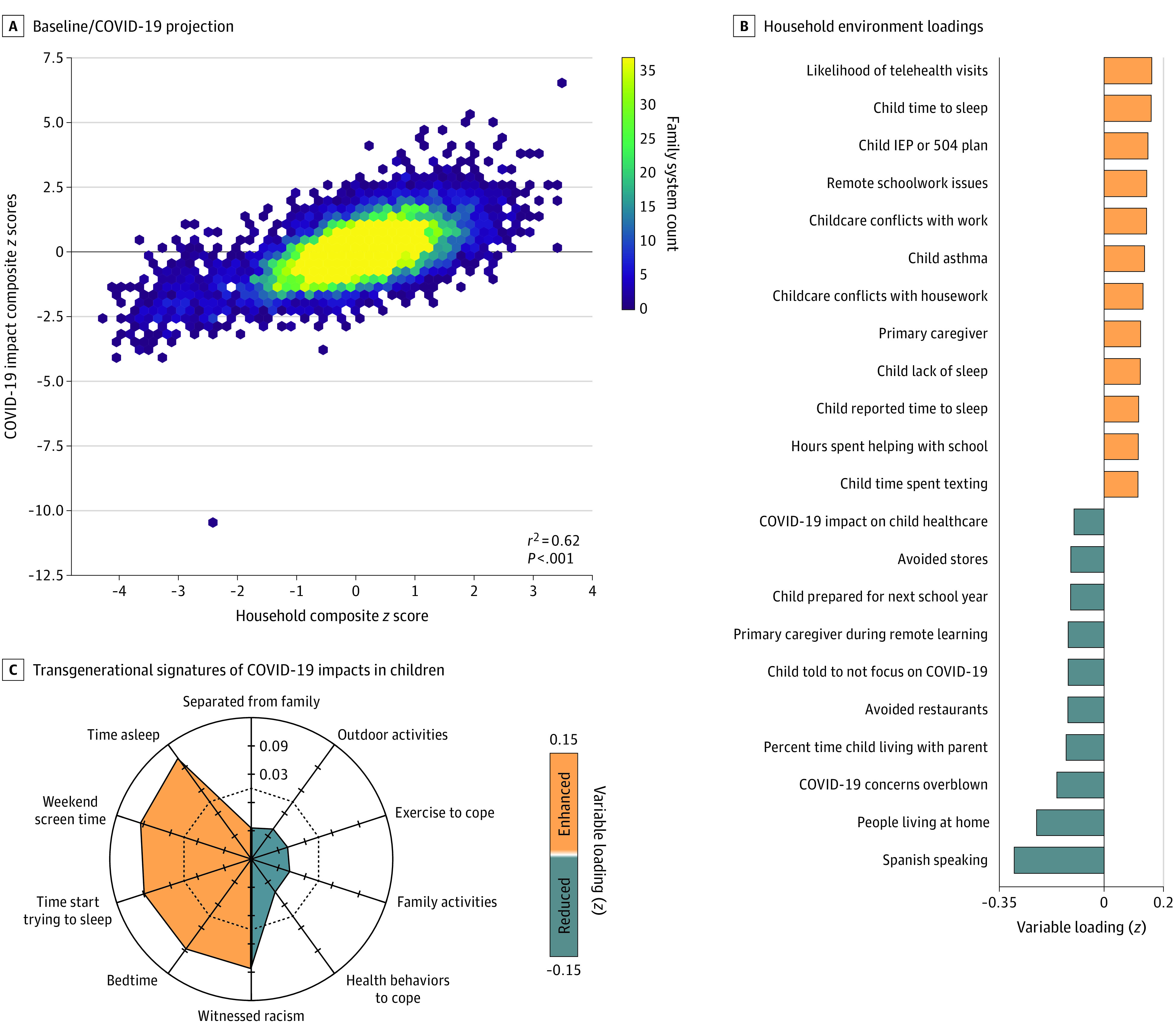
A, Across individual families, household environment was positively associated with COVID-19 impact composite scores of the secondary mode. Modeling results are displayed in a hexagonal binning plot: scale bar reflects the number of families with the same baseline COVID-19 association. B, The bar plot reflects household environment variable loadings from mode 2 indicating a strong positive association with family structure, childcare needs, and child medical and school support needs. The bar plot reflects the top-ranked household characteristics in families with high mode 2 expression (orange indicates positive associations; blue, negative associations). C, The radial plot summarizes experienced racism, sleep hygiene, and social media consumption associated with mode 2. For complete variable definitions, see eTables 2 and 3 in the Supplement. IEP indicates individualized education program.
Cross-validated prediction analyses further confirmed these findings, indicating that the constellation of mode 2 COVID-19 experiences within an individual family could be used to reliably predict corresponding factors including family conflict, engagement in social distancing, child loneliness, and food insecurity (Figure 4). In summary, population mode 2 provides strong evidence for the heightened cost of COVID-19–associated school and business closings on economically disadvantaged families, family units with increased child health care needs, and/or parents whose work conflicts with sudden and unexpected shifts in their caregiving duties.
Figure 4. Family Structure–Associated Household Characteristics Predict Behavior in Response to COVID-19.
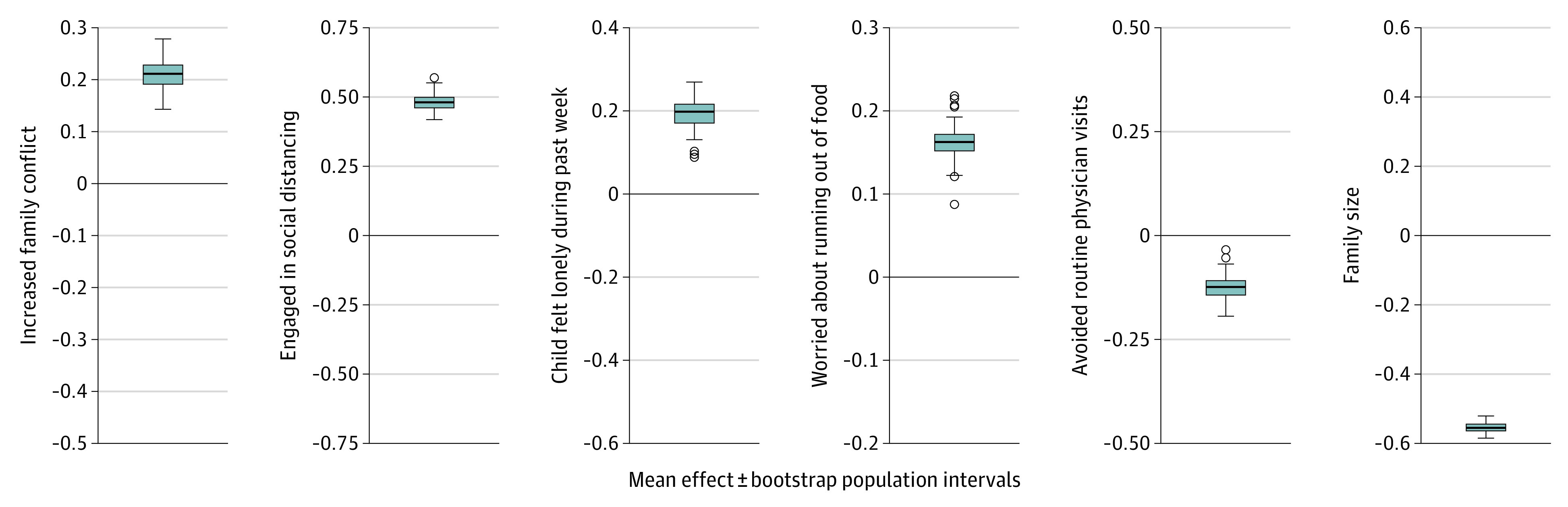
Mode 2 COVID-19 experiences within an individual family can be used to reliably predict corresponding factors including family conflict, engagement in social distancing, child loneliness, and sense of food insecurity. For each box plot, family data from approximately two-thirds of random family picks were used to train linear predictive models (details in Methods), which were then evaluated for prediction accuracy in approximately one-third of unseen holdout families (dispersion and whiskers). Box plots show the corresponding effect sizes, while the error bars show the robustness of the effect sizes. For complete variable definitions, see eTables 2 and 3 in the Supplement.
Out-of-Sample Pattern Prediction of Region-Level Political and Vaccination Variables
To seek deeper understanding of the association between the identified modes and external factors, we tested the ability of modes 1 and 2 to predict region-level differences in political affiliations and COVID-19 policies (Figure 5). These analyses indicated that the constellation of COVID-19 responses within individual families can be used to reliably predict the corresponding political affiliation and pace of vaccine rollout for a given geographic region. Specifically, families with higher mode 1 expressions were more likely to live in Republican states with slower vaccination rates, and families with higher mode 2 expressions were more likely to live in Democratic states with higher vaccination rates.
Figure 5. Out-of-Sample Pattern Prediction of Preferred News Media Outlet, Political Affiliation, and Vaccine Rollout During COVID-19.

Both modes 1 and 2 can be used to predict the political affiliation and pace of vaccine rollout for a given geographic region. Political affiliations were defined based on the results of the 2020 US presidential election. Vaccine rates are defined as the percentage of individuals having received at least 1 vaccine dose as of May 2021, based on US Centers for Disease Control and Prevention data (eMethods in the Supplement). For each box plot, family data from approximately two-thirds of random family picks were used to train linear predictive models (details in Methods), which were then evaluated for prediction accuracy in approximately one-third of unseen holdout families (dispersion and whiskers). Box plots show the corresponding effect sizes, while the error bars show the robustness of the effect sizes.
Discussion
The ABCD study is a data collection initiative of unprecedented size and scope with the potential to transform understanding of development trajectories. To our knowledge, the present study is the first to demonstrate that social determinants of inequity worsened by the COVID-19 pandemic are associated with negative impacts on the functioning of children, regardless of pre–COVID-19 functionality. This is highlighted by the negative outcomes of families with lower socioeconomic status, single-parent households, and minoritized racial and ethnic backgrounds, despite increased adherence to handwashing and social distancing. Further, children in this cohort are now facing developmental challenges unique to their generation—entering adolescence during a time of escalated nationwide psychosocial stress and uncertainty due to COVID-19. However, the impact of these challenges is disproportionately confronted by children from households with poor social determinants, as well as reversible social, physical, and economic conditions that affect health. Notably, these social determinants of inequity—and not diverse measures of medical or psychiatric health, as included in the baseline ABCD battery—emerged from our purely data-driven analysis as the primary correlates of lived COVID-19 pandemic experiences among US families.
Our results underscore that families most affected by inequity during COVID-1920 were more likely to abide by safe practices such as social distancing and handwashing, despite a popular narrative that individuals from these communities are less likely to engage in such behavior.21 These findings have potential implications for policy makers, stakeholders, and decision makers who seek to mitigate the inequity confronted by minoritized and marginalized populations.22 In particular, our investigation is consistent with the interpretation that individual behavior alone cannot singly affect or mitigate health outcomes. Rather, psychosocial factors such as built environment, access to education, racism, and parental and community support all play pivotal roles in promoting health equity.
While these observational results cannot, by definition, provide direct support for the potential efficacy of different intervention approaches to combat these associations, our findings nonetheless suggest several important areas for future work. In particular, these data raise the possibility that interventions aimed at the community level (eg, provision of childcare, increased access to school meals, universal basic income to cover fundamental needs, continued COVID-19 unemployment assistance)23 might be effective in either preventing or combatting negative COVID-19 experiences across multiple generations within a single family. Critically, the identified modes extended to reliably predict region-level factors including state political affiliation and current vaccination rates. These findings further suggest a reciprocal association between individual, family-level factors, and state-level policy factors.
Limitations
Our study has several limitations. First, it is important to acknowledge that we cannot rule out the possibility that associations with some individual-level survey items (eg, pet ownership) may in fact be due to the presence of unobserved confounding variables and/or be proxy measures of latent variables. Second, our analysis only focused on the first wave of ABCD’s COVID-19 battery assessments. These data nonetheless provide an important empirical baseline from which subsequent COVID-19 experiences may be tracked through later ABCD data releases. By sharing all of the code and output for our analyses, we hope that other groups will be able to assess associations between identified factors and later COVID-19 experiences. Third, while our analysis workflow incorporating validation of the CCA using nonparametric permutation testing is considered state of the art,24 we cannot entirely rule out the possibility that our multivariate analyses may have been subject to some overfitting. Again, by sharing our code, we hope that other groups may verify or falsify our findings in other data sets and in later data releases of ABCD. Fourth, our analysis approach only assessed linear (and not nonlinear) associations. Finally, it is critical to acknowledge that early 2020 was characterized by numerous non–COVID-19–associated events, such as the murder of George Floyd, that may have influenced study findings. While the COVID-19 assessments specifically asked about experiences of “racism or discrimination in relation to coronavirus,” it is nonetheless possible that this and other societal events may have influenced concerns and experiences of racism.
Conclusions
In this analysis, variations in day-to-day transgenerational COVID-19 experiences were associated with differences in social determinants of inequity. People from minoritized racial and ethnic populations experienced greater COVID-19 impacts associated with these inequities. Future work assessing the impact of community-level, transgenerational intervention strategies is urgently needed to combat the disproportionate burdens of the ongoing pandemic.
eMethods
eTable 1. Demographic characteristics of youth with and without COVID-19 assessment data
eTable 2. ABCD Child COVID-19 Assessments
eTable 3. ABCD Parent COVID-19 Assessments
eTable 4. Top 20 Loadings Mode 1 ABCD Baseline
eTable 5. Top 20 Loadings Mode 1 COVID Baseline
eTable 6. Top 20 Loadings Mode 2 ABCD Baseline
eTable 7. Top 20 Loadings Mode 2 COVID Baseline
eTable 8. Top 10 Loadings Mode 3 ABCD Baseline
eTable 9. Top 10 Loadings Mode 3 COVID Baseline
eTable 10. Top 10 Loadings Mode 4 ABCD Baseline
eTable 11. Top 10 Loadings Mode 4 COVID Baseline
eTable 12. Top 10 Loadings Mode 5 ABCD Baseline
eTable 13. Top 10 Loadings Mode 5 COVID Baseline
eTable 14. Top 10 Loadings Mode 6 ABCD Baseline
eTable 15. Top 10 Loadings Mode 6 COVID Baseline
eTable 16. Top 10 Loadings Mode 7 ABCD Baseline
eTable 17. Top 10 Loadings Mode 7 COVID Baseline
eTable 18. Top 10 Loadings Mode 8 ABCD Baseline
eTable 19. Top 10 Loadings Mode 8 COVID Baseline
eTable 20. Top 10 Loadings Mode 9 ABCD Baseline
eTable 21. Top 10 Loadings Mode 9 COVID Baseline
eReferences
References
- 1.Lee FS, Heimer H, Giedd JN, et al. Mental health. Adolescent mental health--opportunity and obligation. Science. 2014;346(6209):547-549. doi: 10.1126/science.1260497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912-920. doi: 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Teach SJ, St Geme JW III. The indirect effects of COVID-19 on pediatric research. Pediatr Res. 2021;90(2):246-247. doi: 10.1038/s41390-021-01563-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Firew T, Sano ED, Lee JW, et al. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open. 2020;10(10):e042752. doi: 10.1136/bmjopen-2020-042752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gloster AT, Lamnisos D, Lubenko J, et al. Impact of COVID-19 pandemic on mental health: an international study. PLoS One. 2020;15(12):e0244809. doi: 10.1371/journal.pone.0244809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Woolford SJ, Sidell M, Li X, et al. Changes in body mass index among children and adolescents during the COVID-19 pandemic. JAMA. 2021;326(14):1434-1436. doi: 10.1001/jama.2021.15036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abrams EM, Szefler SJ. COVID-19 and the impact of social determinants of health. Lancet Respir Med. 2020;8(7):659-661. doi: 10.1016/S2213-2600(20)30234-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lopez L III, Hart LH III, Katz MH. Racial and ethnic health disparities related to COVID-19. JAMA. 2021;325(8):719-720. doi: 10.1001/jama.2020.26443 [DOI] [PubMed] [Google Scholar]
- 9.Garavan H, Bartsch H, Conway K, et al. Recruiting the ABCD sample: design considerations and procedures. Dev Cogn Neurosci. 2018;32:16-22. doi: 10.1016/j.dcn.2018.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Volkow ND, Koob GF, Croyle RT, et al. The conception of the ABCD study: From substance use to a broad NIH collaboration. Dev Cogn Neurosci. 2018;32:4-7. doi: 10.1016/j.dcn.2017.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Auchter AM, Hernandez Mejia M, Heyser CJ, et al. A description of the ABCD organizational structure and communication framework. Dev Cogn Neurosci. 2018;32:8-15. doi: 10.1016/j.dcn.2018.04.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Paul SE, Hatoum AS, Fine JD, et al. Associations between prenatal cannabis exposure and childhood outcomes: results from the ABCD study. JAMA Psychiatry. 2021;78(1):64-76. doi: 10.1001/jamapsychiatry.2020.2902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Witten DM, Tibshirani R, Hastie T. A penalized matrix decomposition, with applications to sparse principal components and canonical correlation analysis. Biostatistics. 2009;10(3):515-534. doi: 10.1093/biostatistics/kxp008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Modabbernia A, Janiri D, Doucet GE, Reichenberg A, Frangou S. Multivariate patterns of brain-behavior-environment associations in the Adolescent Brain and Cognitive Development study. Biol Psychiatry. 2021;89(5):510-520. doi: 10.1016/j.biopsych.2020.08.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kernbach JM, Yeo BTT, Smallwood J, et al. Subspecialization within default mode nodes characterized in 10,000 UK Biobank participants. Proc Natl Acad Sci U S A. 2018;115(48):12295-12300. doi: 10.1073/pnas.1804876115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Miller KL, Alfaro-Almagro F, Bangerter NK, et al. Multimodal population brain imaging in the UK Biobank prospective epidemiological study. Nat Neurosci. 2016;19(11):1523-1536. doi: 10.1038/nn.4393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang HT, Smallwood J, Mourao-Miranda J, et al. Finding the needle in a high-dimensional haystack: canonical correlation analysis for neuroscientists. Neuroimage. 2020;216:116745. doi: 10.1016/j.neuroimage.2020.116745 [DOI] [PubMed] [Google Scholar]
- 18.Efron B. Large-scale Inference: Empirical Bayes Methods for Estimation, Testing, and Prediction. Cambridge University Press; 2012. [Google Scholar]
- 19.GitHub. dblabs-mcgill-mila/ABCD_covid19_popul_modes. Accessed January 5, 2022. https://github.com/dblabs-mcgill-mila/ABCD_covid19_popul_modes
- 20.Dyer O. Covid-19: Black people and other minorities are hardest hit in US. BMJ. 2020;369:m1483. doi: 10.1136/bmj.m1483 [DOI] [PubMed] [Google Scholar]
- 21.Gibbons J. Distancing the socially distanced: Racial/ethnic composition’s association with physical distancing in response to COVID-19 in the U.S. PLoS One. 2021;16(5):e0251960. doi: 10.1371/journal.pone.0251960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gray DM II, Anyane-Yeboa A, Balzora S, Issaka RB, May FP. COVID-19 and the other pandemic: populations made vulnerable by systemic inequity. Nat Rev Gastroenterol Hepatol. 2020;17(9):520-522. doi: 10.1038/s41575-020-0330-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Castrucci BC, Auerbach J. Meeting individual social needs falls short of addressing social determinants of health. Health Affairs Blog. Published January 16, 2019. Accessed January 5, 2022. https://www.healthaffairs.org/do/10.1377/forefront.20190115.234942/abs/
- 24.Bzdok D, Nichols TE, Smith SM. Towards algorithmic analytics for large-scale datasets. Nat Mach Intell. 2019;1(7):296-306. doi: 10.1038/s42256-019-0069-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods
eTable 1. Demographic characteristics of youth with and without COVID-19 assessment data
eTable 2. ABCD Child COVID-19 Assessments
eTable 3. ABCD Parent COVID-19 Assessments
eTable 4. Top 20 Loadings Mode 1 ABCD Baseline
eTable 5. Top 20 Loadings Mode 1 COVID Baseline
eTable 6. Top 20 Loadings Mode 2 ABCD Baseline
eTable 7. Top 20 Loadings Mode 2 COVID Baseline
eTable 8. Top 10 Loadings Mode 3 ABCD Baseline
eTable 9. Top 10 Loadings Mode 3 COVID Baseline
eTable 10. Top 10 Loadings Mode 4 ABCD Baseline
eTable 11. Top 10 Loadings Mode 4 COVID Baseline
eTable 12. Top 10 Loadings Mode 5 ABCD Baseline
eTable 13. Top 10 Loadings Mode 5 COVID Baseline
eTable 14. Top 10 Loadings Mode 6 ABCD Baseline
eTable 15. Top 10 Loadings Mode 6 COVID Baseline
eTable 16. Top 10 Loadings Mode 7 ABCD Baseline
eTable 17. Top 10 Loadings Mode 7 COVID Baseline
eTable 18. Top 10 Loadings Mode 8 ABCD Baseline
eTable 19. Top 10 Loadings Mode 8 COVID Baseline
eTable 20. Top 10 Loadings Mode 9 ABCD Baseline
eTable 21. Top 10 Loadings Mode 9 COVID Baseline
eReferences