

Abstract
Purpose
To examine the clinical value of multiband (MB) sensitivity encoding (SENSE)–accelerated diffusion-weighted imaging (DWI) for breast imaging by performing quantitative and qualitative comparisons with conventional diffusion-weighted echo-planar imaging, or conventional DWI (cDWI).
Materials and Methods
In this prospective study (ClinicalTrials.gov identifier NCT03607552), women with breast cancer were recruited from July 2018 to July 2019 to undergo additional MB SENSE DWI during clinical 3-T breast MRI examinations. The cDWI and MB SENSE DWI acquisitions were assessed both quantitatively and qualitatively. Regions of interest were defined for tumorous and normal tissue, and the tumor apparent diffusion coefficient (ADC), contrast-to-noise ratio (CNR), and signal index (SI) were calculated for both DWI methods. Three readers independently reviewed the two acquisitions side by side and provided relative image quality scores. Tumor ADC, CNR, and SI measures were compared between cDWI and MB SENSE DWI acquisitions by using a paired t test, and reader preferences were evaluated by using the sign test.
Results
The study included 38 women (median age, 48 years; range, 28–83 years). Overall agreement was good between cDWI and MB SENSE DWI tumor ADC measures (intraclass correlation coefficient, 0.87 [95% CI: 0.75, 0.94]), and no differences were evident in the ADC (median, 0.93 × 10–3 mm2/sec vs 0.87 ×10−3 mm2/sec; P = .50), CNR (2.2 vs 2.3; P = .17), or SI (9.2 vs 9.2; P = .23) measurements. The image quality of cDWI and MB SENSE DWI acquisitions were considered equal for 51% of images (58 of 114), whereas MB SENSE DWI was preferred more often than cDWI (37% [42 of 114] vs 12% [14 of 114]; P < .001). The preference for MB SENSE DWI was most often attributed to better fat suppression.
Conclusion
MB SENSE can be used to accelerate breast DWI acquisition times without compromising the image quality or the fidelity of quantitative ADC measurements.
Keywords: MR-Diffusion-weighted Imaging, Breast, Comparative Studies, Technology Assessment
Clinical trial registration no. NCT03607552
© RSNA, 2022
Keywords: MR-Diffusion-weighted Imaging, Breast, Comparative Studies, Technology Assessment
Summary
Multiband sensitivity encoding expedites breast diffusion-weighted imaging (DWI) without compromising the image quality or the fidelity of apparent diffusion coefficient measurements; by shortening the imaging duration, this technique increases the clinical feasibility of performing advanced DWI examinations.
Key Points
■ Multiband (MB) sensitivity encoding (SENSE) acceleration can be used to shorten breast diffusion-weighted imaging (DWI) time, facilitating the collection of more b values, more gradient directions, greater coverage, and/or thinner slices within a clinical setting.
■ There was good overall agreement between breast tumor apparent diffusion coefficient measurements obtained by using conventional DWI (cDWI) and those obtained by using MB SENSE DWI (intraclass correlation coefficient, 0.87 [95% CI: 0.75, 0.94]).
■ Through qualitative assessment, it was found that the use of MB SENSE DWI resulted in image quality that was equal to or higher than that obtained by using cDWI in 88% (100 of 114) of reader comparisons.
Introduction
Diffusion-weighted imaging (DWI) is an emerging technique that shows potential as both a supplemental and a stand-alone technique for breast cancer imaging (1). Through the generation of signal contrast based on differences in Brownian motion, DWI enables the acquisition of information reflecting the molecular function and microarchitecture of the human body. This provides a distinct mechanism for differentiating malignant from benign tissues without the use of contrast agents. Quantitative apparent diffusion coefficient (ADC) measures obtained by using DWI have demonstrated value for improving the diagnostic performance of and reducing unnecessary biopsies associated with conventional dynamic contrast-enhanced breast MRI (2). Furthermore, the high costs associated with dynamic contrast-enhanced MRI and concerns about long-term health effects of gadolinium-based contrast material administration (3) have fueled a recent interest in DWI as a non–contrast-enhanced alternative to dynamic contrast-enhanced imaging for breast cancer screening.
Free-breathing, single-shot echo-planar imaging (EPI) is the predominant acquisition sequence for breast DWI in clinical practice. In single-shot EPI, all the k-space spatial encoding data for a single slice are obtained after each slice is individually excited. Because of an increasing desire for higher spatial resolution with full coverage, especially when DWI is being used as a stand-alone screening tool, DWI acquisition times are lengthened accordingly. A longer acquisition time makes DWI more sensitive to patient motion and hinders the clinical applicability of performing more advanced DWI techniques (eg, intravoxel incoherent motion modeling and diffusion-tensor imaging) in a clinical setting (1,4). Therefore, it is important to expedite the acquisition time of breast DWI while preserving the image and diagnostic quality and, hence, the quantification accuracy of the ADC and other diffusion metrics.
Multiband (MB) sensitivity encoding (SENSE) imaging has been introduced as an acquisition acceleration technique by simultaneously exciting multiple imaging slices (a type of technique also known as simultaneous multislice acquisition). MB composite radiofrequency pulses are applied to excite multiple slices simultaneously, followed by the separation of imaging slices using the spatial sensitivity profile of the phased-array coil. The fast acquisition speed of MB SENSE results from the shortened repetition time (TR), which is proportionally related to the MB factor (ie, the number of imaging slices that are excited concurrently). Although conceptually similar to parallel imaging, there is no undersampling signal-to-noise ratio (SNR) penalty with MB SENSE imaging; only the g-factor imposed by the coil geometry creates any penalty (5). In addition, the controlled aliasing method—controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) (6)—was developed to further reduce the noise amplification during disentangling of the simultaneously excited slices by shifting the aliased slices relative to each other. In EPI, such a shift is achieved by adding gradient blips along the slice gradient direction. DWI has greatly benefited from simultaneous multislice techniques as used to study disorders in the head and cerebral tissues (7–12) and the abdomen (13–18). The implementation of the reconstruction technique varies across vendors. For the MB SENSE implementation (with Philips Healthcare MRI systems), SENSE-based unfolding in the image domain is used. Simultaneous multislice techniques provided by other vendors use the generalized autocalibrating partially parallel acquisition (ie, GRAPPA) type of parallel reconstruction, in which unfolding is applied in the k-space domain. There have been a number of recent publications evaluating the use of simultaneous multislice techniques for breast imaging, but no studies to date, to our knowledge, have specifically reported on the performance of the MB SENSE technique for breast DWI (19–23). Moreover, MB SENSE is currently only available as a research sequence and requires further validation before clinical implementation in breast DWI.
We hypothesized that MB SENSE could shorten acquisition times for breast DWI but may detrimentally affect image quality. The purpose of this work was therefore to examine the clinical value of MB SENSE–accelerated, single-shot echo-planar DWI for breast imaging by comparing the image quality and accuracy of ADC measurements with those obtained by using conventional SENSE-accelerated, single-shot echo-planar DWI.
Materials and Methods
Participant Sample
The protocol for this prospective study was approved by our institutional review board and was compliant with the Health Insurance Portability and Accountability Act. The study sample was enrolled during the technical optimization phase of a larger trial (ClinicalTrials.gov identifier: NCT03607552). Data generated or analyzed during the study are available from the corresponding author by request. Participants with known breast cancer planning to undergo MRI to enable evaluation of the extent of disease were consecutively recruited at and provided consent at our institution between July 2018 and July 2019. The race and ethnicity of the participants were collected from their electronic health records and reported to the funding agency (National Institutes of Health). An additional MB SENSE–accelerated DWI examination was performed during their regular clinical examination. A subset of participants in our study (n = 30) were previously described in another study testing the impact of DWI b values (both acquired and synthesized) on lesion conspicuity (24). In this study, the value of the MB SENSE acceleration technique was evaluated and compared with that of conventional DWI (cDWI).
MR Image Acquisition
All of the MR images were acquired with a 3-T clinical imager (3-T Achieva system; Philips Healthcare) using a dedicated 16-channel breast coil. The MB SENSE acceleration capability was provided for use in the study through in-kind research support from Philips Healthcare; Philips employees did not have access to the study data.
Phantom study.—Initial experiments to test the viability of using MB SENSE for axial bilateral breast DWI were performed using a custom bilateral breast DWI phantom (CaliberMRI, formerly High Precision Devices). Phantom DWI examinations were first run without MB SENSE, using the following parameters: TR, 5725 msec; echo time (TE), 75 msec; echo train length, 67; field of view, 360 mm × 360 mm; voxel size, 1.8 mm × 1.8 mm × 4 mm; in-plane SENSE factor, three; spectral attenuated inversion recovery (SPAIR) with gradient reversal fat suppression; b values of 0, 100, 800, 1500, and 2500 sec/mm2; number of signal averages, two (for b = 0 and 100 sec/mm2 acquisitions), four (for b = 800 sec/mm2 acquisitions), and six (for b = 1500, 2500 sec/mm2 acquisitions); 30 slices; and acquisition time, 5 minutes 26 seconds. Next, DWI was run with MB SENSE acceleration, keeping the above prescription constant except for the following: MB SENSE factor, two; CAIPIRINHA shift, 1/2 field of view (6); TR, 3500 msec; TE, 80 msec; and an acquisition time of 3 minutes 20 seconds.
Clinical study.—To evaluate the effect of MB SENSE on image quality in breast DWI, otherwise matched bilateral axial DWI acquisitions were obtained with and without MB SENSE for comparison. The standard echo-planar cDWI sequence used for clinical breast MRI examinations at our institution that was performed as a reference had the following parameters: TR, 5043 msec; TE, 60 msec; excitation bandwidth, 814 Hz; echo train length, 67; field of view, 360 mm × 360 mm; voxel size, 1.8 mm × 1.8 mm × 4 mm; in-plane SENSE factor, three; SPAIR with gradient reversal fat suppression; b values of 0, 100, 600, 800, and 1000 sec/mm2; 30 slices; and an acquisition time of 4 minutes 33 seconds. The MB SENSE DWI sequence was performed with the same parameters as cDWI except for the following: TR, 3500 msec; TE, 80 msec; excitation bandwidth, 407 Hz; b values of 0, 100, 800, 1500, and 2500 sec/mm2; MB SENSE factor, 2; CAIPIRINHA shift, 1/2 field of view; and an acquisition time of 3 minutes 20 seconds. In vivo clinical DWI parameters are shown in Table 1.
Table 1:
Sequence Acquisition Parameters

A T2-weighted turbo spin-echo–based sequence (using either SPAIR or mDixon techniques for fat suppression) was performed during the examination and used as the reference standard for anatomic evaluations. Imaging parameters for the T2-weighted acquisitions were as follows: TR, 5000 msec; TE, 60 msec; SENSE, 3.1; field of view, 220–240 mm × 330–360 mm; matrix, 240 × 275–360; voxel size, 0.8 mm × 0.8 mm × 1.3 mm; and acquisition time, 2 minutes (mDixon) or 2 minutes 45 seconds (SPAIR).
Image Analysis
Quantitative ADC measurements.—All DWI acquisitions were first registered to correct for eddy current and participant motion effects using a vendor-provided registration tool (25). Quantitative DWI analysis was performed offline by a research scientist (D.B., with more than 4 years of experience in quantitative breast MRI) using custom software developed in MATLAB (MathWorks) (24). ADC maps of cDWI and MB SENSE DWI were generated with b = 0, 100, and 800 sec/mm2 by using a voxelwise linear regression fit of the standard monoexponential decay function (26,27):
 |
In the phantom, regions of interest were segmented for the tumor (40% polyvinylpyrrolidone) and normal tissue (water) ADC mimic vials (28), with ADC values of 0.68 mm2/sec ± 0.01 and 2.03 mm2/sec, respectively, at 20°C (values according to the phantom manufacturer specifications). For the in vivo clinical imaging, the lesions were segmented on the b = 800 sec/mm2 images of the MB SENSE DWI and cDWI examinations separately by using a threshold-based, semiautomatic tool (24). The fibroglandular tissue region was segmented on the image for b = 0. The contrast-to-noise ratio (CNR) was defined as
 |
Where μl and μn represent the mean signal intensity of lesion and normal fibroglandular tissue, respectively, and σl and σn are the standard deviations of the lesion and fibroglandular tissue on b = 800 sec/mm2 images. With challenges related to noise and SNR measurement in the presence of parallel imaging reconstruction, the signal index (SI) was defined as a reflection of signal quality in the tumor by using
 |
Qualitative assessment.—Qualitative assessment of in vivo clinical DWI acquisitions was performed by three independent readers who were blinded to the type of acquisition. Two experienced radiologists (J.R.S. and H.R., each with more than 10 years of experience in breast imaging) and one MR physicist (S.C.P., with more than 20 years of experience in DWI) compared cDWI acquisitions with MB SENSE DWI acquisitions in terms of image quality and the presence of artifacts or other issues. Assessments were performed on a clinical workstation to best mimic the clinic environment. The b = 0 and 800 sec/mm2 images from cDWI and MB SENSE DWI were provided side by side. The order of cDWI and MB SENSE DWI acquisitions was randomized, and the images were provided without annotation indicating the technique. Readers either scored the two images as equal (score of 0) or preferred one over the other (score of +1). Readers were also asked to give a reason for choosing a nonequal score in terms of distortion, fat suppression, SNR, and artifacts present in the image, and they were free to choose multiple reasons for a single case.
Statistical Analysis
Overall agreement between the ADC measures obtained with cDWI and MB SENSE DWI was assessed by using the intraclass correlation coefficient. Bland-Altman methods were used to compare ADCs, CNRs, and SIs between cDWI acquisitions and MB SENSE DWI acquisitions. These comparisons were performed on the log scale to reduce skewness (29). The paired t test was used to test for an overall mean difference between the techniques. Qualitative assessments of the three readers for the preferred image quality between cDWI and MB SENSE DWI were compared by using a sign test. Comparisons were made by using all reads combined and for each reader separately. For the comparisons based on all reads combined, the sign test was clustered by participant to account for the repeated reads. Similarly, the nonparametric bootstrap was used to calculate 95% CIs, with resampling performed by participant to account for the repeated reads. All statistical calculations were conducted with the statistical computing language R (version 4.0.3; R Foundation for Statistical Computing). Two-sided tests were used, and statistical significance was defined as a P value less than .05 being achieved.
Results
Participant Characteristics
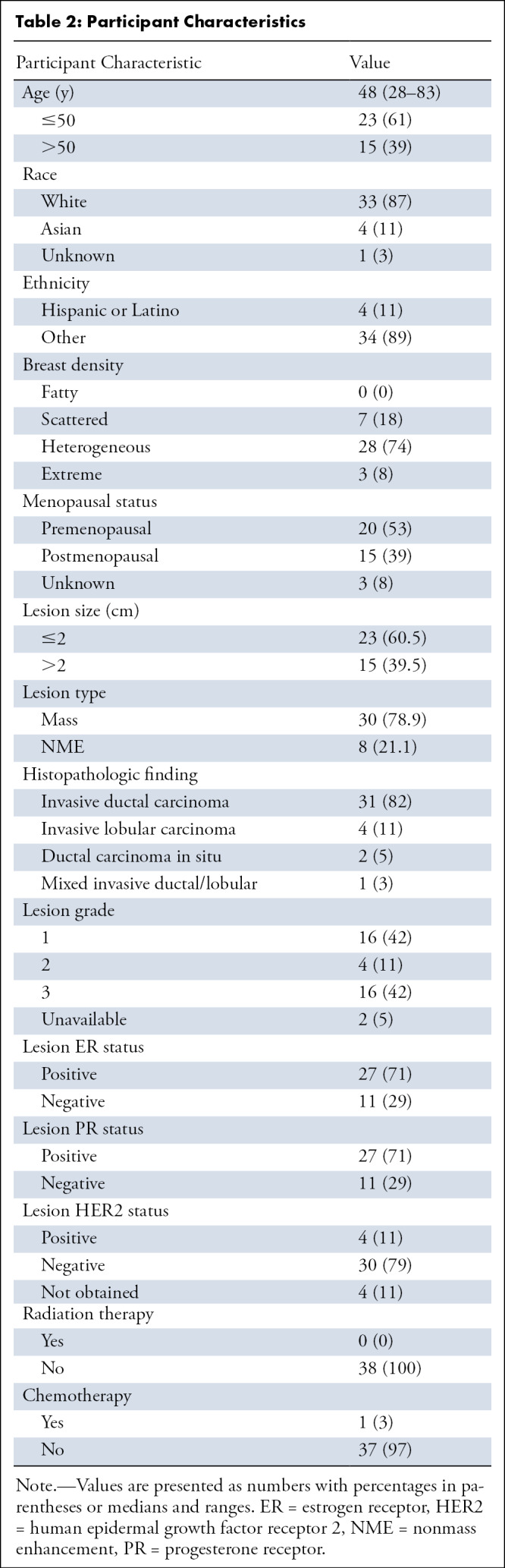
A total of 38 consecutive participants with breast cancer were enrolled and underwent both cDWI and MB SENSE DWI examinations for the study. Thirty-three of 38 participants (87%) were White, four (11%) were Asian, and four (11%) were Hispanic or Latino. Ages ranged from 28 to 83 years (median, 48 years); 31 had invasive ductal carcinoma, four had invasive lobular carcinoma, two had ductal carcinoma in situ, and one had a mixed invasive ductal and lobular carcinoma. Lesions ranged in size from 4 to 124 mm (median, 19 mm). Participant and lesion characteristics are provided in more detail in Table 2.
Table 2:
Participant Characteristics
Quantitative Assessment
Phantom study.—ADC maps were generated for the phantom DWI acquisitions with and without MB SENSE. ADC measurements were in close agreement for both the tumor mimic (0.66 × 10−3 mm2/sec for cDWI and 0.63 × 10−3 mm2/sec for MB SENSE DWI) and normal tissue mimic (2.20 × 10−3 mm2/sec for both acquisitions). Additionally, compared with MB SENSE DWI acquisitions, cDWI acquisitions had a higher CNR (4.5 vs 2.4) and SI (38.4 vs 27.9) on b = 800 sec/mm2 images (Fig 1).
Figure 1:

Images in a bilateral breast diffusion-weighted imaging (DWI) phantom. Shown are T1-weighted axial and coronal cross-section views (top) and representative images obtained at DWI (b = 0 and 800 sec/mm2) that depict the tumor mimic (arrow 1) and the normal tissue mimic (arrow 2) vials in the left breast used for quantitation of the ADC, contrast-to-noise ratio, and signal index. Corresponding regions of interest used for quantitation are shown for tumor tissue (dotted line) and normal tissue (solid line) mimics. ADC = apparent diffusion coefficient, MB = multiband, SENSE = sensitivity encoding.
In vivo study.—Quantitative analysis was performed in 32 of 38 participants; in six participants, lesions were not visible and could not be measured because of neoadjuvant chemotherapy (n = 2) and the presence of biopsy artifacts (n = 4). An example case is shown in Figure 2. Overall agreement between ADC measures obtained with MB SENSE DWI and cDWI was good, with an intraclass correlation coefficient of 0.87 (95% CI: 0.75, 0.94). There was no evidence of a difference between ADC values measured on cDWI acquisitions and those measured on MB SENSE DWI acquisitions (median, 0.93 [interquartile range, 0.81–1.05] × 10–3 mm2/sec vs 0.87 [95% CI: 0.80, 1.13] × 10–3 mm2/sec; P = .50) (Fig 3).
Figure 2:
![Images obtained at diffusion-weighted imaging (DWI) by using conventional (left) and MB SENSE–accelerated (right) acquisitions in a 36-year-old participant with a 43-mm grade 3 invasive ductal carcinoma (arrow, outline). Good image quality was observed (shown are b = 0 and b = 800 sec/mm2 images) on images obtained by using both sequences (with two of three readers rating them equal [0] and one preferring MB SENSE [+1]), and the resulting apparent diffusion coefficient (ADC) maps (bottom) were also very similar both qualitatively and quantitatively. The tumor mean ADC values (within the outlined regions of interest shown) were closely matched, with ADC = 0.82 and 0.86 × 10–3 mm2/sec for conventional DWI and MB SENSE DWI, respectively. MB = multiband, SENSE = sensitivity encoding.](https://www.ncbi.nlm.nih.gov/core/lw/2.0/html/tileshop_pmc/tileshop_pmc_inline.html?title=Click%20on%20image%20to%20zoom&p=PMC3&id=8830507_rycan.210063.fig2.jpg)
Images obtained at diffusion-weighted imaging (DWI) by using conventional (left) and MB SENSE–accelerated (right) acquisitions in a 36-year-old participant with a 43-mm grade 3 invasive ductal carcinoma (arrow, outline). Good image quality was observed (shown are b = 0 and b = 800 sec/mm2 images) on images obtained by using both sequences (with two of three readers rating them equal [0] and one preferring MB SENSE [+1]), and the resulting apparent diffusion coefficient (ADC) maps (bottom) were also very similar both qualitatively and quantitatively. The tumor mean ADC values (within the outlined regions of interest shown) were closely matched, with ADC = 0.82 and 0.86 × 10–3 mm2/sec for conventional DWI and MB SENSE DWI, respectively. MB = multiband, SENSE = sensitivity encoding.
Figure 3:

Agreement between lesion diffusion-weighted imaging (DWI) measures by using multiband (MB) sensitivity encoding (SENSE) and conventional DWI (cDWI) techniques. Shown are Bland-Altman plots for (A) apparent diffusion coefficient (ADC) measures, (B) contrast-to-noise ratio (CNR) measures, and (C) signal index (SI) values. Bland-Altman analysis demonstrates no apparent systematic bias in the ADC, CNR, or SI measurements between the techniques. The dashed line indicates the mean ratio (MB SENSE DWI vs cDWI), and the dotted lines indicate the 95% limits of agreement.
Comparing signal on b = 800 sec/mm2 images from cDWI with images from MB SENSE DWI, there was no evidence of a difference in the CNR (median, 2.2 [interquartile range, 1.6–2.6] vs 2.3 [interquartile range, 1.8–2.8]; P = .17) or SI (median 9.2 [interquartile range, 7.2–13.0] vs 9.2 [interquartile range, 6.4–12.0]; P = .23) between the two image types. The mean difference (MB SENSE DWI minus cDWI) in the CNR was 13.6% (95% CI: −5.5%, 36.6%), and the mean difference in the SI was −6.6% (95% CI: −16.6%, 4.6%) (Table 3).
Table 3:
Comparisons of Quantitative Measures

Qualitative Assessment
For qualitative assessment, three readers evaluated the overall image quality of MB SENSE DWI compared with cDWI. Reader preferences and scoring are summarized in Table 4. For the three readers combined (n = 114 total combined reads), the image quality from MB SENSE DWI was preferred more often than that from cDWI (37% [42 of 114] vs 12% [14 of 114]; P < .001), whereas images from cDWI and MB SENSE DWI were considered of equal quality for 51% (58 of 114). Overall, the image quality for MB SENSE DWI was scored as being equal to or better than that for cDWI in 100 of 114 (88% [95% CI: 82%, 93%]) cases. Results were similar when the analysis was restricted to the 32 participants (n = 96 total combined reads) who could be analyzed in the quantitative assessment, with the image quality of MB SENSE DWI being preferred more often than that of cDWI (39% [37 of 96] vs 12% [12 of 96]; P < .001) and scoring equal to or better than cDWI in 84 of 96 (88% [95% CI: 81%, 93%]).
Table 4:
Qualitative Assessment of MB SENSE and cDWI Techniques

Table 4 further summarizes scores and attributed factors for reads in which the image quality resulting from using one technique was preferred over another. Multiple factors could be selected for a particular case (making the total exceed 100%). As described, MB SENSE DWI was more often preferred over cDWI (n = 42 reads), with the most common factor being superior fat suppression on MB SENSE DWI acquisitions (57% [24 of 42], Fig 4), followed by a superior SNR (31% [13 of 42]) and fewer artifacts or distortions (31% [13 of 42]). In cases when cDWI was preferred over MB SENSE DWI (n = 14 reads), the most common factor was a higher SNR (79% [11 of 14], Figure 5).
Figure 4:

Example of differences in fat suppression observed on images obtained at MB SENSE diffusion-weighted imaging (DWI) compared with those obtained at conventional DWI. On the conventional DWI acquisition (left), unsuppressed fat signal is apparent in both anterior breasts, particularly at b = 800 sec/mm2 (arrows), which was not observed on the MB SENSE DWI acquisition (right), on which tissue contrast is higher. Two readers preferred the image quality of the MB SENSE DWI acquisition, whereas one reader rated them equally. MB = multiband, SENSE = sensitivity encoding.
Figure 5:

Example of differences in signal quality observed on images obtained by using MB SENSE compared with images obtained by using conventional diffusion-weighted imaging (DWI). Posterior fibroglandular tissue regions can be better evaluated on conventional DWI acquisition (left) than on the MB SENSE DWI acquisition (right) because of the reduced signal of the MB SENSE image, most apparent on b = 800 sec/mm2 (arrows). Reduced signal is also evident in the chest wall and sternum (arrowhead) for the MB SENSE acquisition compared with the conventional DWI acquisition. One reader preferred conventional DWI, whereas the other two rated the techniques as being equal. MB = multiband, SENSE = sensitivity encoding.
Discussion
Results from our study showed that MB SENSE enabled a substantial reduction in the TR and permitted the acquisition of breast DWI data in a shorter time without compromising image quality. Shorter acquisition times can increase DWI quality and potentially reduce artifacts by decreasing overall patient motion. The study also confirmed that use of MB SENSE to expedite breast DWI acquisitions does not compromise the fidelity of quantitative ADC measurements. ADC measurements showed good agreement between MB SENSE DWI and cDWI for both phantom and clinical acquisitions (with intraclass correlation coefficient = 0.87 for clinical acquisitions).
A growing number of studies have explored simultaneous multislice acceleration techniques for breast DWI, primarily implemented with other MRI vendor platforms (19–23). One of the first studies compared readout segmented images obtained at EPI acquired with and without simultaneous multislice in healthy women and found that the ADC values and the SNR in the normal parenchyma were similar (21). A more recent study in women with breast cancer showed similar ADC values in the tumor and better image quality on the simultaneous multislice–accelerated acquisitions compared with the standard readout–segmented EPI acquisitions (22). Similar to our study, Ohlmeyer et al (23) compared conventional single-shot breast echo-planar DWI acquisitions obtained with and without simultaneous multislice and did not find any statistically significant differences in the average lesion ADC values or diagnostic performance but found a substantial reduction in the acquisition time (from 3 minutes 27 seconds to 1 minute 53 seconds) by using simultaneous multislice. Another study by McKay et al (20) showed that simultaneous multislice made it possible to achieve higher spatial resolution for breast DWI by using a sagittal acquisition and axial reformatting approach, without degrading image quality. Our study expands on prior work to evaluate the clinical value of the MB SENSE with CAIPIRINHA technique, implemented on Philips MRI platforms, which, to our knowledge, has not been previously reported for breast DWI.
For MB SENSE DWI in our study, we combined an MB SENSE factor of 2 with a parallel imaging SENSE factor of 3 to optimize the acceleration both in-plane and along the slice direction. We also fixed the TR at 3500 msec. Although it is possible to increase the MB SENSE factor and/or reduce the TR even further to reduce acquisition time, it comes at the cost of signal quality, which was not desirable. Prior research in abdominal imaging (15) showed that even though the acquisition time can be reduced by at least 60% or more by increasing the MB factor to 3 or above, signal degradation and inaccurate ADC quantification would impede its usage in a clinical setting. Therefore, we determined the best compromise was to use an MB factor of 2. The minimum TR was selected to align with the European Society of Breast Imaging Breast DWI consensus recommendations to achieve an adequate SNR (30).
In general, readers rated images from MB SENSE DWI to be equal or better in quality than those from cDWI in 88% (100 of 114) of cases. It is useful to note that when the readers preferred MB SENSE DWI over cDWI (37% of comparisons), they most often attributed the preference to better fat suppression on MB SENSE DWI acquisitions compared with the corresponding cDWI acquisitions. In the few cases in which cDWI was preferred (14% of comparisons), most often the readers thought the signal quality (ie, the SNR) was better on cDWI acquisitions than on MB SENSE DWI acquisitions. A lower SNR on MB SENSE DWI acquisitions arising from the longer TE (80 vs 60 msec), leading to more T2 decay, and shorter TR (3500 vs 5043 msec), leading to decreased longitudinal relaxation and an overall reduced signal compared with cDWI acquisitions, is expected. The observation of improved fat suppression for MB SENSE DWI acquisitions was surprising but was also reported as an incidental finding in a prior simultaneous multislice breast DWI study by Ohlmeyer et al (23) and may be linked to the lower excitation bandwidth used at MB SENSE DWI. Specifically, to avoid exceeding specific absorption rate and peak amplitude limits, composite radiofrequency pulses used for MB excitation have longer pulse duration and therefore lower excitation bandwidth than those in cDWI (407 Hz for MB SENSE DWI, 814 Hz for cDWI). For a given slice thickness, lower bandwidth is thus associated with a weaker slice-selection gradient. A gradient reversal technique was used for improved fat suppression in this study, in which slice-selection gradients for the refocusing pulses are applied with opposite polarity. As reported by Nagy and Weiskopf (31), for slice-selection gradient reversal fat suppression, displacement of fat relative to water signal is inversely proportional to the gradient strength. Hence, a weaker gradient results in a greater relative extent of displacement, or shift, between fat and water signals (31), which could explain the superior fat suppression observed in MB SENSE DWI (Fig 4).
There were some limitations to the study. First, readers could have been biased by differences in both T1 and T2 weighting (for MB SENSE, the TR was 3500 msec and the TE was 80 msec; for cDWI, the TR was 5043 msec and TE was 60 msec), with associated stronger T1 and T2 weighting possibly also contributing to a greater preference for MB SENSE DWI. These additional technical factors, along with the observed improvement in fat suppression by using a lower excitation bandwidth with the gradient reversal technique (for the MB SENSE DWI examination) warrant further exploration for refining breast DWI sequences to improve image quality. Although the comparisons between cDWI and MB SENSE DWI sequences were performed using images and ADCs with the same diffusion weightings (b = 0 and 800 sec/mm2), the MB SENSE DWI acquisition incorporated a wider b value range (maximum b value of 2500 vs 1000 sec/mm2 for cDWI) to collect additional high b value data for other research questions, which further contributed to the differences in TE and other sequence parameters, such as acquisition time. If identical b values were acquired for both types of DWI acquisitions, MB SENSE would have resulted in an even greater amount of time saving (5 minutes 26 seconds vs 3 minutes 20 seconds, as shown in the phantom experiment). The study was performed for 3-T axial imaging only, and it is not clear if more dramatic effects would be observed at other field strengths or imaging orientations. Last, the sample size was not large, so although the average differences we observed between ADC, CNR, and SI measurements from cDWI acquisitions and MB SENSE DWI acquisitions were not significant, it is possible that there are true differences that were not statistically detected because of insufficient power. The limited sample size also precluded subanalysis by participant and lesion characteristics.
In conclusion, results from this study suggest that the MB SENSE implementation of simultaneous multislices can be used to expedite breast DWI without compromising the image quality and fidelity of quantitative ADC measurements. By shortening acquisition durations, MB SENSE and other simultaneous multislice acceleration techniques increase the clinical feasibility of performing advanced breast DWI examinations involving a larger number of slices so as to achieve a higher spatial resolution with thinner slices, and to facilitate advanced DWI modeling approaches requiring a greater number of b values and/or gradient directions.
Supported by funding from the National Institutes of Health/National Cancer Institute grants R01CA207290 and U01CA225427, the Safeway Foundation, and by research support from Philips Healthcare.
Data Sharing. Data generated or analyzed during the study are available from the corresponding author by request.
Disclosures of conflicts of interest: D.B. Support for present work from National Institutes of Health (NIH) (payments through institution), Philips Healthcare (in-kind support through institution), and Safeway Foundation (payments through institution). D.S.H. Support for present work from NIH grants (R01 CA207290, P30 CA015704) to institution; institution has grants from GE Healthcare, Philips Healthcare, Canon Medical Systems USA, and Siemens Healthineers. Y.W. No relevant relationships. M.R.D. In-kind support for present work from Philips Healthcare (use of the sequence); currently employed by Philips Healthcare (employment began after work on the present manuscript had concluded). M.Z. Research grant from GE Healthcare. J.R.S. Grants from Radiological Society of North America Global Oncology-Fred Hutchinson Cancer Research center and GE Healthcare, unrelated to the current work; leadership or fiduciary role in RAD-AID and Breast Health Global Initiative. H.R. Current work supported by NIH grant (R01CA207290), author is co-investigator; institution has grant from GE Healthcare, author is co-investigator, funding not related to this study. S.C.P. Current work supported by NIH grant (R01CA207290), author is principal investigator; institution has grant from GE Healthcare, author is co-investigator, funding not related to this study.
Abbreviations:
- ADC
- apparent diffusion coefficient
- CAIPIRINHA
- controlled aliasing in parallel imaging results in higher acceleration
- cDWI
- conventional DWI
- CNR
- contrast-to-noise ratio
- DWI
- diffusion-weighted imaging
- EPI
- echo-planar imaging
- MB
- multiband
- SENSE
- sensitivity encoding
- SI
- signal index
- SNR
- signal-to-noise ratio
- SPAIR
- spectral attenuated inversion recovery
- TE
- echo time
- TR
- repetition time
References
- 1. Partridge SC , Nissan N , Rahbar H , Kitsch AE , Sigmund EE . Diffusion-weighted breast MRI: clinical applications and emerging techniques . J Magn Reson Imaging 2017. ; 45 ( 2 ): 337 – 355 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rahbar H , Zhang Z , Chenevert TL , et al . Utility of diffusion-weighted imaging to decrease unnecessary biopsies prompted by breast MRI: a trial of the ECOG-ACRIN cancer research group (A6702) . Clin Cancer Res 2019. ; 25 ( 6 ): 1756 – 1765 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Khawaja AZ , Cassidy DB , Al Shakarchi J , McGrogan DG , Inston NG , Jones RG . Revisiting the risks of MRI with gadolinium based contrast agents-review of literature and guidelines . Insights Imaging 2015. ; 6 ( 5 ): 553 – 558 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Whisenant JG , Romanoff J , Rahbar H , et al . Factors affecting image quality and lesion evaluability in breast diffusion-weighted MRI: observations from the ECOG-ACRIN cancer research group multisite trial (A6702) . J Breast Imaging 2020. ; 3 ( 1 ): 44 – 56 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Setsompop K , Gagoski BA , Polimeni JR , Witzel T , Wedeen VJ , Wald LL . Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty . Magn Reson Med 2012. ; 67 ( 5 ): 1210 – 1224 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Breuer FA , Blaimer M , Heidemann RM , Mueller MF , Griswold MA , Jakob PM . Controlled Aliasing in Parallel Imaging Results in Higher Acceleration (CAIPIRINHA) for multi-slice imaging . Magn Reson Med 2005. ; 53 ( 3 ): 684 – 691 . [DOI] [PubMed] [Google Scholar]
- 7. Wen Q , Kelley DA , Banerjee S , et al . Clinically feasible NODDI characterization of glioma using multiband EPI at 7 T . Neuroimage Clin 2015. ; 9 ( 291 ): 299 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Setsompop K , Kimmlingen R , Eberlein E , et al . Pushing the limits of in vivo diffusion MRI for the human connectome project . Neuroimage 2013. ; 80 ( 220 ): 233 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Chakhoyan A , Leu K , Pope WB , Cloughesy TF , Ellingson BM . Improved spatiotemporal resolution of dynamic susceptibility contrast perfusion MRI in brain tumors using simultaneous multi-slice echo-planar imaging . AJNR Am J Neuroradiol 2018. ; 39 ( 1 ): 43 – 45 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hsu YC , Chu YH , Tsai SY , Kuo WJ , Chang CY , Lin FH . Simultaneous multi-slice inverse imaging of the human brain . Sci Rep 2017. ; 7 ( 1 ): 17019 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Jiang JS , Zhu LN , Wu Q , et al . Feasibility study of using simultaneous multi-slice RESOLVE diffusion weighted imaging to assess parotid gland tumors: comparison with conventional RESOLVE diffusion weighted imaging . BMC Med Imaging 2020. ; 20 ( 1 ): 93 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Feinberg D , Setsompop K . Ultra-fast MRI of the human brain with simultaneous multi-slice imaging . J Magn Reson 2013. ; 229 ( 90 ): 100 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Zhang G , Sun H , Qian T , et al . Diffusion-weighted imaging of the kidney: comparison between simultaneous multi-slice and integrated slice-by-slice shimming echo planar sequence . Clin Radiol 2019. ; 74 ( 4 ): 325.e1 – 325.e8 . [DOI] [PubMed] [Google Scholar]
- 14. Haraikawa M , Suzuki M , Inoue K , Kozawa E , Tanaka J , Niitsu M . Simultaneous multi-slice MR imaging of the hip at 3 T to reduce acquisition times and maintain image quality . BMC Musculoskelet Disord 2018. ; 19 ( 1 ): 440 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Boss A , Barth B , Filli L , et al . Simultaneous multi-slice echo planar diffusion weighted imaging of the liver and the pancreas: optimization of signal-to-noise ratio and acquisition time and application to intravoxel incoherent motion analysis . Eur J Radiol 2016. ; 85 ( 11 ): 1948 – 1955 . [DOI] [PubMed] [Google Scholar]
- 16. Park JH , Seo N , Lim JS , Hahm J , Kim MJ . Feasibility of simultaneous multislice acceleration technique in diffusion-weighted magnetic resonance imaging of the rectum . Korean J Radiol 2020. ; 21 ( 1 ): 77 – 87 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Tabari A , Machado-Rivas F , Kirsch JE , Nimkin K , Gee MS . Performance of simultaneous multi-slice accelerated diffusion-weighted imaging for assessing focal renal lesions in pediatric patients with tuberous sclerosis complex . Pediatr Radiol 2021. ; 51 ( 1 ): 77 – 85 . [DOI] [PubMed] [Google Scholar]
- 18. Xu J , Cheng YJ , Wang ST , et al . Simultaneous multi-slice accelerated diffusion-weighted imaging with higher spatial resolution for patients with liver metastases from neuroendocrine tumours . Clin Radiol 2021. ; 76 ( 1 ): 81.e11 – 81.e19 . [DOI] [PubMed] [Google Scholar]
- 19. Sanderink WBG , Teuwen J , Appelman L , et al . Comparison of simultaneous multi-slice single-shot DWI to readout-segmented DWI for evaluation of breast lesions at 3T MRI . Eur J Radiol 2021. ; 138 109626 . [DOI] [PubMed] [Google Scholar]
- 20. McKay JA , Church AL , Rubin N , et al . A comparison of methods for high-spatial-resolution diffusion-weighted imaging in breast MRI . Radiology 2020. ; 297 ( 2 ): 304 – 312 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Filli L , Ghafoor S , Kenkel D , et al . Simultaneous multi-slice readout-segmented echo planar imaging for accelerated diffusion-weighted imaging of the breast . Eur J Radiol 2016. ; 85 ( 1 ): 274 – 278 . [DOI] [PubMed] [Google Scholar]
- 22. Song SE , Woo OH , Cho KR , et al . Simultaneous multislice readout-segmented echo planar imaging for diffusion-weighted MRI in patients with invasive breast cancers . J Magn Reson Imaging 2021. ; 53 ( 4 ): 1108 – 1115 . [DOI] [PubMed] [Google Scholar]
- 23. Ohlmeyer S , Laun FB , Palm T , et al . Simultaneous multislice echo planar imaging for accelerated diffusion-weighted imaging of malignant and benign breast lesions . Invest Radiol 2019. ; 54 ( 8 ): 524 – 530 . [DOI] [PubMed] [Google Scholar]
- 24. DelPriore MR , Biswas D , Hippe DS , et al . Breast cancer conspicuity on computed versus acquired high b-value diffusion-weighted MRI . Acad Radiol 2021. ; 28 ( 8 ): 1108 – 1117 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Arlinghaus LR , Welch EB , Chakravarthy AB , et al . Motion correction in diffusion-weighted MRI of the breast at 3T . J Magn Reson Imaging 2011. ; 33 ( 5 ): 1063 – 1070 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Le Bihan D , Breton E , Lallemand D , Grenier P , Cabanis E , Laval-Jeantet M . MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders . Radiology 1986. ; 161 ( 2 ): 401 – 407 . [DOI] [PubMed] [Google Scholar]
- 27. Stejskal EO , Tanner JE . spin diffusion measurements: spin echoes in the presence of a time‐dependent field gradient . J Chem Phys 1965. ; 42 ( 1 ): 288 – 292 . [Google Scholar]
- 28. Keenan KE , Ainslie M , Barker AJ , et al . Quantitative magnetic resonance imaging phantoms: a review and the need for a system phantom . Magn Reson Med 2018. ; 79 ( 1 ): 48 – 61 . [DOI] [PubMed] [Google Scholar]
- 29. Bland JM , Altman DG . Measuring agreement in method comparison studies . Stat Methods Med Res 1999. ; 8 ( 2 ): 135 – 160 . [DOI] [PubMed] [Google Scholar]
- 30. Baltzer P , Mann RM , Iima M , et al . Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI international breast diffusion-weighted imaging working group . Eur Radiol 2020. ; 30 ( 3 ): 1436 – 1450 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Nagy Z , Weiskopf N . Efficient fat suppression by slice-selection gradient reversal in twice-refocused diffusion encoding . Magn Reson Med 2008. ; 60 ( 5 ): 1256 – 1260 . [DOI] [PMC free article] [PubMed] [Google Scholar]