

Abstract
Introduction
Breast cancer patients with germline pathogenic variants may benefit from risk-reducing surgeries, intensive screening, and targeted cancer therapies. There is a paucity of data regarding prevalence and distribution of germline pathogenic variants in the Brazilian population. Our primary endpoint was the description of prevalence and distribution of germline pathogenic variants among breast cancer patients who underwent next-generation sequencing (NGS) panel testing. Secondary endpoint was the assessment of predictive factors of a positive test.
Methods
We analyzed NGS results, personal, and family history data from a prospectively collected cohort of breast cancer patients from August 2013 to May 2019. Exact logistic regression was used to perform multivariable analysis.
Results
Of 370 breast cancer patients, we found 59 pathogenic variants in 57 (15%) patients. Pathogenic variants were identified in BRCA1 (24%), ATM (14%), BRCA2 (10%), TP53 (8%), PALB2 (8%), CHEK2 (7%), CDH1 (3%), RAD51C (3%), MITF (2%), PMS2 (2%), RAD51D (2%), and TERT (2%). Monoallelic MUTYH pathogenic variants were found in 15%. After multivariable analysis, age of diagnosis (OR 0.89, 95% CI: 0.81–0.95, for each year increase), triple-negative subtype (OR 17.2, 95% CI: 3.74–114.72), and number of breast cancers in the family (OR 2.46, 95% CI 1.57–4.03, for each additional case) were associated with BRCA1 pathogenic variants. In the present study, a quarter of triple-negative breast cancer patients harbored a germline pathogenic variant and two-thirds of those were BRCA1 carriers.
Conclusions
Prevalence and distribution of germline pathogenic variants in this Brazilian sample of breast cancer patients are mostly similar to other populations. However, there is a trend to an overrepresentation of TP53 pathogenic variants that merits confirmation in further studies. Early-onset breast cancer patients should be offered genetic counseling, particularly those with triple-negative subtype.
Keywords: breast neoplasms, high-throughput nucleotide sequencing, Brazil, genetic predictive testing, genetic predisposition to breast cancer
Introduction
Breast cancer affects approximately 66,000 women and accounts for more than 17,000 deaths annually in Brazil (1). Approximately 10% of breast cancer patients carry a germline pathogenic variant that may indicate screening strategies or preventive recommendations (2). Targeted therapy options may be indicated as further treatment.
After the identification of the BRCA1 gene in 1994 by Dr. Mary-Claire King (3), DNA sequencing techniques and bioinformatics have evolved significantly (4) and rendered germline testing accessible to an increasingly wider population. Since then, other high penetrance genes such as TP53 and PALB2 have also been described as breast cancer susceptibility genes, as well as moderate penetrance genes such as ATM and CHEK2 (5). Recommendations for BRCA1 and BRCA2 range from risk-reducing mastectomies (6) to intensive screening with breast magnetic resonance imaging (MRI) (7) and specific therapies such as platinum agents (8) and PARP inhibitors (9, 10). There is an ongoing effort to understand the magnitude and the modifying factors of risk conferred by each gene and to which extent we could generalize what we learned from high penetrance genes to moderate penetrance counterparts (11).
As there is a paucity of data describing the germline landscape of breast cancer patients in the Brazilian population, we aimed to describe the prevalence and distribution of germline pathogenic variants among breast cancer patients in a tertiary oncology hospital in Brazil.
Methods
This is a cross-sectional study from a prospectively collected database from the Oncogenetics Unit at Hospital Sírio-Libanês, a tertiary oncology hospital based in São Paulo and Brasília, Brazil. From August 2013 to May 2019, 2,116 subjects were included in the registry, and 867 had a personal history of breast cancer. Among these, 386 had non-NGS testing, and 97 did not have a sample collected. Eligible subjects were breast cancer patients who received genetic counseling in this time frame and to whom next-generation-sequencing (NGS) cancer panel was performed (Invitae™ 83 or 84 Multi-Cancer Panel) (12). Patients were referred based on their physician’s assessment of risk factors for hereditary cancer. The indication of germline testing followed NCCN criteria, but 10% of our sample were offered testing without a formal criterion, mainly because of second malignancies or the presence of multiple breast cancer cases above age 50 in the family. Tests were paid out-of-pocket and reimbursed by insurance companies, whenever applicable. Exclusion criteria were inability to retrieve data and absence of family history records.
All medical charts were electronically reviewed, and the following data were collected: NGS panel results, age of personal breast cancer diagnosis, gender, Ashkenazi ethnicity, personal history of bilateral breast cancer, histology, and immunohistochemistry (IHC) subtype. Family history was collected up to third-degree relatives including personal history, and comprehended number of breast cancer cases (bilateral cases count as 2 and personal history was excluded), number of male breast cancer, cancer of the ovary, pancreas, prostate, melanoma, sarcoma, adrenocortical, central nervous system (CNS), leukemia, gastric, colon, endometrium, thyroid, and kidney.
New assessment of variants segregation within families was not possible. However, we already had information on the segregation of 20 pathogenic variants. In the absence of segregation information, either maternal or paternal family history was collected based on the following criteria, in order of priority: number of additional breast cancer cases, youngest additional breast cancer case, degree of relationship to proband, and the presence of ovarian, pancreatic, sarcoma, or central nervous system cancers. There were no ties beyond this point.
Primary endpoint was the description of prevalence and distribution of germline pathogenic variants among breast cancer patients that had NGS testing. Secondary endpoint was the assessment of predictive clinical factors of a positive test. Likely Pathogenic Variants were regarded as Pathogenic and Variants of Unknown Significance as Not Pathogenic.
Continuous data were not normally distributed and are presented as median and interquartile range. Since most of family history data had a median of zero, data are presented as categorical (at least 1 case of each cancer) in order to better disclose clinical significance, but they were treated as continuous variables for the purpose of statistical inference. Categorical data are presented as percentiles. Univariate analysis was performed with Mann–Whitney’s or Fisher’s exact test for continuous and categorical data, respectively. For the purpose of multivariable analysis, exact logistic regression was performed for each gene in a forward selection manner from the most significant one, until there was no significant covariate left behind. Since there were 13 models, Bonferroni correction was applied to account for multiple testing. Therefore, a significant p-value was set at 0.0038. There was less than 8% of missing data in histology and breast cancer subtype only. Missingness was not related to any other variable. Hence, it was assumed to be missing completely at random and dealt with the worst-case scenario. All analyses were performed using the software Stata 17.
Patients prospectively signed an informed consent form to have their data and family history collected and used for research purposes. Institutional Review Board approved data collection as no new medical intervention would be pursued and confidentiality would be preserved. Data were de-identified for the purpose of statistical analysis and protected from re-identification.
Results
In total, 384 charts were electronically reviewed. One subject was excluded for not having an NGS panel test, five for not having a personal history of breast cancer and eight for substantial missing data. Among the remaining 370 subjects, 59 pathogenic variants were identified in 57 (15%) subjects. Two subjects had 2 pathogenic variants concomitantly, one being the combination of TP53 and ATM pathogenic variants and the other TP53 and monoallelic MUTYH. In the span of six years, 62 variants were reclassified, most of them from unknown significance to benign, but there was one CHEK2 intronic variant that was reclassified as likely pathogenic. As of January 2020, there were 178 (48%) variants of unknown significance identified. The distribution of pathogenic variants can be found in Figure 1 .
Figure 1.
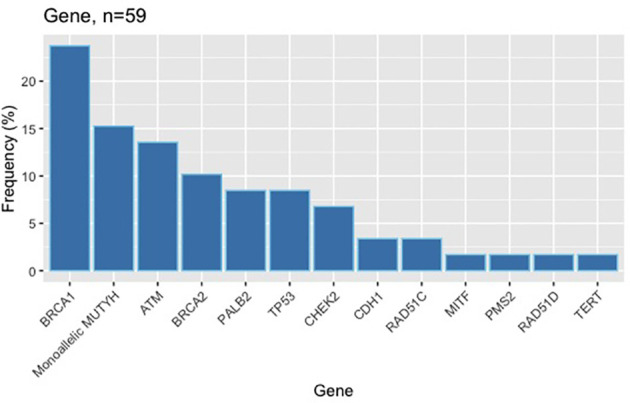
Distribution of germline pathogenic variants.
Ninety percent of our population had at least 1 criterion according to the National Comprehensive Cancer Network (NCCN) guidelines, version 1.2020. There were only 2 male subjects, and only 4 with Ashkenazi ethnicity. None of them carried a germline pathogenic variant. Median age at breast cancer diagnosis was 46 in patients with no pathogenic variants. Median age was 5 years younger in the pathogenic group and 10 years younger in BRCA1 carriers. Bilateral cancers were twice more frequent in the pathogenic group ( Table 1 ).
Table 1.
Personal characteristics of the study population.
| Total (%) n = 370 (100%) | Not Pathogenic (%) n = 313 (85%) | Pathogenic (%) n = 57 (15%) | Univariate Analysis p-value | |
|---|---|---|---|---|
| Female | 368 (99) | 311 (99) | 57 (100) | ns |
| Ashkenazi Ethnicity | 4 (01) | 4 (01) | 0 (00) | ns |
| Median age at diagnosis (IQR) | 45 (39–52) | 46 (40–53) | 41 (35–48) | 0.0038 |
| Bilateral Cancers | (07) | 18 (06) | 8 (14) | 0.042 |
| At least 1 NCCN criterion | 332 (90) | 277 (88) | 55 (96) | ns |
| Ductal Carcinoma In Situ | 42 (11) | 37 (12) | 5 (09) | ns |
| Ductal Carcinoma | 253 (68) | 211 (67) | 42 (74) | ns |
| Lobular Carcinoma | 36 (10) | 31 (10) | 5 (09) | ns |
| Histology Others | 22 (06) | 20 (06) | 2 (04) | ns |
| Histology Missing Data | 17 (05) | 14 (04) | 3 (05) | ns |
| HR positive Her2 negative | 236 (64) | 203 (65) | 33 (58) | ns |
| HR positive Her2 positive | 27 (07) | 23 (07) | 04 (07) | ns |
| HR negative Her2 positive | 30 (08) | 27 (09) | 3 (05) | ns |
| HR negative Her2 negative | 63 (17) | 46 (15) | 17 (30) | 0.011 |
| Subtype Missing Data* | 27 (07) | 23 (07) | 4 (07) | ns |
IQR, interquartile range; HR, Hormone Receptors; Her2, Human Epidermal growth factor Receptor 2; ns, not significant; NCCN, National Comprehensive Cancer Network.
*Data do not sum up to 100% due to bilateral cancers.
Groups were similar according to histology and subtype, except for the triple-negative subtype, which was doubled in prevalence in the pathogenic group. A quarter of triple-negative patients harbored a germline pathogenic variant, and two-thirds of those were BRCA1 carriers. Eighty percent of BRCA1 carriers had a triple-negative cancer ( Tables 1 and 4 ).
Table 4.
Description of germline pathogenic variants.
| Patient | Germline Pathogenic Variant | Age at Diagnosis | Bilateral Cancer | Triple Negative | Cancer Family History up to Third Degree (Age) | Second Malignancies of Proband (Age) |
|---|---|---|---|---|---|---|
| 01 | ATM c.1339C>T (p.Arg447Ter) | 39 | No | No | Breast (40) and Colon (58). | |
| 02 | ATM c.2999del (p.Asn1000Thrfs*2) | 35 | No | No | Breast (65) and Breast (72). | |
| 03 | ATM c.3802delG (p.Val1268*) | 41 | No | No | Breast (54) and Breast (56). | |
| 04 | ATM c.3802delG (p.Val1268*) | 33 | No | No | None. | |
| 05 | ATM c.4741dupA (p.Ile1581Asnfs*5) | 48, 67 | Yes | Yes | Breast (64), Breast (80), Leukemia (80), and Kidney (81). | |
| 06 | ATM c.4906C>T (p.Gln1636Ter) | 42, 46 | Yes | No | Breast (40), Gastric, Colon (73), and Kidney. | |
| 07 | ATM c.67C>T (p.Arg23*) | 45 | No | No | Breast (54), Breast, Colon (80), Kidney (40), and Kidney (71). | |
| 08 | ATM Partial Deletion (Exon 27-29) | 66 | No | No | Breast (30), Pancreas, Prostate (85), Sarcoma, and Thyroid (15). | |
| 09 | BRCA1 c.1071dup (p.Leu358Thrfs*8) | 34 | No | Yes | Breast (34), Bilateral Breast (35, 35), and Breast (36). | |
| 10 | BRCA1 c.1687C>T (p.Gln563*) | 35, 35 | Yes | Yes | Ovary (58). | |
| 11 | BRCA1 c.188T>A (p.Leu63Ter) | 46 | No | Yes | Pancreas (64) and Gastric (72). | |
| 12 | BRCA1 c.2176_2177delCT (p.Leu726Serfs) | 39 | No | No | Breast (42), Breast (69), Prostate (68), and Prostate (75). | |
| 13 | BRCA1 c.3770_3771delAG (p.Glu1257Glyfs*9) | 41, 43 | Yes | Yes | Breast (50), Breast (80), and Melanoma (43). | |
| 14 | BRCA1 c.4165_4166delAG (p.Ser1389*) | 32 | No | Yes | Breast (55). | |
| 15 | BRCA1 c.441+2T>A (Splice donor) | 42 | No | Yes | Breast (38), Breast (38), Breast (60), and Ovary (48). | |
| 16 | BRCA1 c.5074+2T>C (Splice donor). | 29, 39 | Yes | Yes | Breast (45), Breast (48), and Breast (55). | |
| 17 | BRCA1 c.5266dupC (p.Gln1756Profs) | 28 | No | – | Breast (36), Breast, Breast, and Pancreas (70). | Colon (70). |
| 18 | BRCA1 c.5266dupC (p.Gln1756Profs) | 62 | No | No | Breast (28), Breast, Prostate, and Prostate. | Lymphoma (62). |
| 19 | BRCA1 c.5266dupC (p.Gln1756Profs) | 48, 55 | Yes | Yes | Breast (40), Bilateral Breast (43, 54), Breast (64), Ovary (80), Pancreas (42), and Prostate (67). | Ovary (52). |
| 20 | BRCA1 c.5266dupC (p.Gln1756Profs) | 32 | No | Yes | Breast (70). | |
| 21 | BRCA1 c.5554_5555delAC (p.Thr1852Leufs*27) | 32 | No | Yes | Breast (40) and Colon (55). | |
| 22 | BRCA1 c.798_799del (p.Ser267Lysfs*19) | 32 | No | Yes | Bilateral Breast (38, 40), Breast (45), Ovary (40), and Ovary (50). | |
| 23 | BRCA2 c.1138del (p.Ser380Valfs*19) | 28 | No | No | Breast (47) and Breast (70). | |
| 24 | BRCA2 c.6034del (p.Ser2012Profs*28) | 32 | No | No | Breast (78), Colon (70), and Thyroid (60). | |
| 25 | BRCA2 c.7007G>A (p.Arg2336His) | 41 | No | No | Breast (60) and Breast (65). | |
| 26 | BRCA2 c.8009C>T (p.Ser2670Leu) | 57 | No | No | Gastric (59). | |
| 27 | BRCA2 c.8878C>T (p.Gln2960Ter) | 29 | No | No | Ovary (35), Pancreas (73), Melanoma (58), and Melanoma (63). | |
| 28 | BRCA2 c.9097dupA (p.Thr3033Asnfs*11) | 53 | No | No | Breast (20), Breast (44), Breast (58), and Breast (70). | |
| 29 | CDH1 c.1763_1764del p.Val588Glufs*2 | 47 | No | – | Breast (48) and Colon (70). | Melanoma (41). |
| 30 | CDH1 c.471dup (p.Ile158Tyrfs*10) | 47 | No | No | Bilateral Breast (32, 47), Colon (63), Colon (64), and Colon (69). | |
| 31 | CHEK2 c.1100del C (p.T367Mfs*15) | 48 | No | No | Prostate (43). | |
| 32 | CHEK2 c.1459C>T (p.Gln487*) | 41 | No | No | Prostate (70), Thyroid (42), Thyroid (55), and Thyroid (60). | |
| 33 | CHEK2 c.846+1G>C (Splice donor) | 42 | No | No | Breast, Breast, Breast, Pancreas, and Kidney (75). | Parotid (49) and Kidney (62). |
| 34 | CHEK2 c.846+4_846+7del (Intronic) | 40 | No | No | Leukemia (35). | |
| 35 | MITF c.952G>A (p.Glu318Lys) | 57 | No | No | Prostate (49), Prostate (70), and Colon (78). | |
| 36 | Monoallelic MUTYH c.1147delC (p.Ala385Profs) | 41 | No | No | Sarcoma (70). | |
| 37 | Monoallelic MUTYH c.1187G>A (p.Gly396Asp) | 35 | No | No | Breast (60), Ovary (64), Prostate (72), Prostate (75), Melanoma (56), Central Nervous System (70), and Colon (48). | |
| 38 | Monoallelic MUTYH c.1187G>A (p.Gly396Asp) | 53 | No | No | Breast, Breast, Ovary (50), and Melanoma. | |
| 39 | Monoallelic MUTYH c.1187G>A (p.Gly396Asp) | 53 | No | No | Pancreas (73), Prostate (65), and Prostate (80). | Thyroid (32). |
| 40 | Monoallelic MUTYH c.1187G>A (p.Gly396Asp) | 40 | No | No | Breast and Pancreas. | |
| 41 | Monoallelic MUTYH c.1187G>A (p.Gly396Asp) | 47 | No | Yes | Breast (73) and Endometrium (67). | |
| 42 | Monoallelic MUTYH c.1437_1439delGGA (p.Glu480del) | 34 | No | No | Breast (42). | |
| 43 | Monoallelic MUTYH c.536A>G (p.Tyr179Cys) | 40 | No | No | Breast (47), Ovary, and Colon. | |
| 44 | Monoallelic MUTYH Deletion (Exons 4-16) | 58 | No | No | Breast (50), Breast (70), Ovary (89), and Sarcoma (06). | |
| 45 | PALB2 c.1240C>T (p.Arg414*) | 54, 67 | Yes | Yes | Breast and Breast. | Thyroid (54). |
| 46 | PALB2 c.1671_1674delTATT (p.Ile558Lysfs) | 50 | No | – | Breast and Breast. | |
| 47 | PALB2 c.1671_1674delTATT (p.Ile558Lysfs) | 38 | No | No | Breast (67) and Colon (65). | |
| 48 | PALB2 c.355delC (p.Gln119Lysfs) | 38 | No | No | Breast (50). | Thyroid (36). |
| 49 | PALB2 Deletion (Exons 7-10) | 41 | No | No | Breast (41), Breast (60), and Prostate (75). | |
| 50 | PMS2 c.903G>T (p.Lys301Asn) | 60 | No | No | Colon (63) and Endometrium (69). | |
| 51 | RAD51C c.709C>T (p.Arg237*) | 51, 51 | Yes | Yes | Prostate (87). | |
| 52 | RAD51C Deletion (Exons 6-9) | 43 | No | Yes | Melanoma (65) and Central Nervous System (70). | Gastrointestinal Stromal Tumor (45). |
| 53 | RAD51D c.694C>T (p.Arg232*) | 34 | No | No | Breast (45), Pancreas (69), and Colon (60). | |
| 54 | TERT c.336dupC (p.Glu113Argfs) | 38 | No | Yes | ||
| 06 | TP53 c.1010G>A (p.Arg337His) | 42, 46 | Yes | No | Breast (40), Gastric, Colon (73), and Kidney. | |
| 37 | TP53 c.1010G>A (p.Arg337His) | 35 | No | No | Breast (60), Ovary (64), Prostate (72), Prostate (75), Melanoma (56), Central Nervous System (70), and Colon (48). | |
| 55 | TP53 c.1010G>A (p.Arg337His) | 38 | No | No | Breast (41), Breast (55), Prostate (75), Central Nervous System (15), and Colon (55). | Sarcoma (29). |
| 56 | TP53 c.1010G>A (p.Arg337His) | 47 | No | – | Breast (50), Breast (60), Central Nervous System (01), and Central Nervous System (56). | Lung (56). |
| 57 | TP53 c.1010G>A (p.Arg337His) | 44 | No | No | Breast (66) and Sarcoma (12). |
Median number of breast cancer cases in the family was similar between groups, but there was 1.5 extra case in BRCA1 carriers. Prevalence of ovarian and pancreatic cancers was doubled in the pathogenic group ( Table 2 ).
Table 2.
Cancer family history.
| Total (%) n = 370 (100%) | Not Pathogenic (%) n = 313 (85%) | Pathogenic (%) n = 57 (15%) | Univariate Analysis p-value | |
|---|---|---|---|---|
| Median Number of Breast Cancer Cases in the Family up to Third Degree, excluding proband (IQR) | 1 (0–2) | 1 (0–2) | 1 (0–2) | 0.0402 |
| At least 1 Cancer in the Family up to Third Degree, including proband: | ||||
| Male Breast | 4 (01) | 4 (01) | 0 (00) | ns |
| Ovary | 35 (09) | 26 (08) | 9 (16) | ns |
| Pancreas | 34 (09) | 25 (08) | 9 (16) | ns |
| Prostate | 79 (21) | 67 (21) | 12 (21) | ns |
| Melanoma | 26 (07) | 20 (06) | 6 (11) | ns |
| Sarcoma | 12 (03) | 7 (02) | 5 (09) | 0.0105 |
| Adrenocortical | 0 (00) | 0 (00) | 0 (00) | NA |
| Central Nervous System | 28 (08) | 24 (08) | 4 (07) | ns |
| Leukemia | 29 (08) | 27 (09) | 2 (04) | ns |
| Gastric | 37 (10) | 34 (11) | 3 (05) | ns |
| Colon | 93 (25) | 78 (25) | 15 (26) | ns |
| Endometrium | 8 (02) | 6 (02) | 2 (04) | ns |
| Thyroid | 30 (08) | 24 (08) | 6 (11) | ns |
| Kidney | 14 (04) | 10 (03) | 4 (07) | ns |
IQR, interquartile range; ns, not significant; NA, not applicable.
Sarcoma was a rare event, but at least four times more frequent in the pathogenic group. Numerically, there were more cases of melanoma, endometrium, and kidney cancers, as well as less cases of leukemia and gastric cancers in the pathogenic group. Prostate, CNS, colon, and thyroid cancers were well balanced between groups ( Table 2 ).
Multivariable analysis was significant only for BRCA1 after correction for multiple testing. Younger age, triple-negative subtype, and number of breast cancer cases in the family were highly correlated with the presence of a BRCA1 pathogenic variant ( Table 3 ).
Table 3.
Multivariable analysis.
| Variable | BRCA1 (%) | Not BRCA1 (%) | Odds Ratio | p-value |
|---|---|---|---|---|
| Median Age at Diagnosis (IQR) | 34.5 (32–42) | 45 (39.5–52) | OR 0.89 (0.81–0.95) | 0.0005 |
| Triple-Negative Subtype | 11/14 (79) | 75/356 (21) | OR 17.20 (3.74–114.72) | <0.0001 |
| Median Number of Breast Cancer Cases in the Family up to Third Degree, excluding proband (IQR) | 2.5 (1–3) | 1 (0–2) | OR 2.46 (1.57–4.03) | 0.0001 |
IQR, interquartile range; OR, Odds Ratio.
Complete description of germline pathogenic variants and cases can be found in Table 4 .
Discussion
This is a highly selected convenience sample from a tertiary oncology hospital in Brazil. Median age at breast cancer diagnosis was 45, while previous studies have found it to be 54 in a Brazilian sample (13), and 62 in SEER registry (14). Notwithstanding this selection, having a BRCA1 pathogenic variant was significantly associated with age at diagnosis, further lowering median age to 34, with 75th percentile at 42.
Germline pathogenic variants prevalence at 15% is in accordance with previous studies. The true prevalence lies at approximately 10%, according to the largest series published to date (2), but that ranged from 6% in a study from the Mayo Clinic (15), to 34% from Stanford University (12). The higher prevalence from Stanford can be partially explained by the recruitment period in which testing criteria were more stringent, whereas the study from Mayo already included patients when NGS technology was commonly available.
In addition, only 47.9% of Mayo’s sample had at least 1 NCCN criterion, and 29.9% of identified pathogenic variants came from subjects without any criterion. That led the authors to propose access to germline testing for all breast cancer patients diagnosed below age 65. In this study, having at least 1 NCCN criterion was not associated to the presence of a pathogenic variant. We cannot reach the same conclusion solely based on our sample, because the majority (90%) of our subjects had at least 1 criterion.
Distribution of variants was likewise in accordance with previous studies, being roughly a third to a half in BRCA1 and BRCA2, and the remaining among ATM, CHEK2, PALB2, and TP53.
We performed an unplanned exploratory analysis comparing our results to formerly published ones from different countries ( Table 5 ). In this study, the frequency of TP53 variants at 1.3% was 6.2 times higher than the pooled results from previous reports, p = 0.002, although we acknowledge our limited absolute number. While the prevalence of TP53 variants among all available data is 0.2%, the frequency in our sample and in Asian countries was approximately 1.0%. The largest series from the USA reports a TP53 prevalence of 0.17% (2), whereas in Asian countries it was 1.9% in China (17), 1.0% in South Korea (18), and 1.5% in Taiwan (21). This was not replicated in other Latin American countries other than Brazil. There were no reports of the TP53 R337H in breast cancer cohort studies from Argentina, Colombia, Guatemala, Mexico, or Peru (16, 22).
Table 5.
Prevalence and istribution of germline pathogenic variants in breast cancer patients from different populations.
| Brazil(%) | Latin-America† (16) (%) | China (17) (%) | South-Korea (18) (%) | USADana-Farber (19) (%) | USAMayo (15) (%) | USAMyriad (2) (%) | USAStanford† (12) (%) | Italy† (20) (%) | Taiwan (21) (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| N | 370 | 222 | 937 | 496 | 488 | 3907 | 35409 | 198 | 255 | 133 |
| Patdogenic | 57 (15) | 31 (14) | 215 (23) | 79 (16) | 52 (11) | 246 (06) | 3388 (10) | 68 (34) | 68 (27) | 28 (21) |
| APC | 0 (00) | 0 (00) | 0 (00) | 0 (00) | 0 (00) | – | 11 (00) | 0 (00) | 0 (00) | 0 (00) |
| ATM | 8 (02) | 1 (00) | 6 (01) | 0 (00) | 4 (01) | 43 (01) | 329 (01) | 2 (01) | 3 (01) | 1 (01) |
| BARD1 | 0 (00) | – | 5 (01) | 0 (00) | 0 (00) | – | 68 (00) | – | – | 0 (00) |
| BLM | 0 (00) | 0 (00) | – | 0 (00) | – | – | – | 1 (01) | 0 (00) | – |
| BRCA1 | 14 (04) | 10 (04) | 82 (09) | 31 (06) | 18 (04) | 51 (01) | 814 (02) | 35 (18) | 32 (13) | 9 (07) |
| BRCA2 | 6 (02) | 14 (06) | 81 (09) | 30 (06) | 12 (02) | 56 (01) | 828 (02) | 24 (12) | 26 (10) | 11 (08) |
| BRIP1 | 0 (00) | 0 (00) | 3 (00) | 1 (00) | 4 (01) | – | 110 (00) | 0 (00) | 2 (01) | 1 (01) |
| CDH1 | 2 (01) | 0 (00) | 2 (00) | 8 (02) | 0 (00) | 6 (00) | 23 (00) | 1 (01) | 0 (00) | 0 (00) |
| CDKN2A | 0 (00) | 1 (00) | 0 (00) | 0 (00) | 0 (00) | – | 32 (00) | 2 (01) | 0 (00) | – |
| CHEK2 | 3 (01) | 0 (00) | 6 (01) | 2 (00) | 10 (02) | 67 (02) | 397 (01) | – | 0 (00) | 0 (00) |
| EPCAM | 0 (00) | 0 (00) | – | 0 (00) | 0 (00) | – | 4 (00) | 0 (00) | 0 (00) | 0 (00) |
| MITF | 1 (00) | – | – | – | – | – | – | – | 0 (00) | – |
| MLH1 | 0 (00) | 0 (00) | 1 (00) | 2 (00) | 0 (00) | – | 22 (00) | 1 (01) | 0 (00) | 0 (00) |
| MSH2 | 0 (00) | 1 (00) | 3 (00) | 1 (00) | 0 (00) | – | 37 (00) | 0 (00) | 0 (00) | 1 (01) |
| MSH6 | 0 (00) | 1 (00) | 0 (00) | 0 (00) | 1 (00) | – | 73 (00) | 0 (00) | 1 (00) | 0 (00) |
| Monoallelic MUTYH | 9 (02) | 3 (01) | 8 (01) | 1 (00) | 9 (02) | – | – | 5 (03) | – | 1 (01) |
| Biallelic MUTYH | 0 (00) | 0 (00) | 0 (00) | 0 (00) | 0 (00) | – | 7 (00) | 0 (00) | – | 0 (00) |
| NBN | 0 (00) | 0 (00) | 0 (00) | 3 (01) | 1 (00) | – | 59 (00) | 2 (01) | 0 (00) | 0 (00) |
| NF1 | 0 (00) | 0 (00) | 0 (00) | 0 (00) | – | 1 (00) | – | – | 0 (00) | – |
| PALB2 | 5 (01) | 2 (01) | 11 (01) | 0 (00) | 1 (00) | 15 (00) | 316 (01) | 0 (00) | 6 (02) | – |
| PMS2 | 1 (00) | 0 (00) | 2 (00) | 0 (00) | 1 (00) | – | 101 (00) | 0 (00) | 0 (00) | 0 (00) |
| PTEN | 0 (00) | 0 (00) | 0 (00) | 0 (00) | 1 (00) | 1 (00) | 17 (00) | 0 (00) | 0 (00) | 0 (00) |
| RAD50 | 0 (00) | – | 2 (00) | 0 (00) | – | – | – | – | – | 2 (01) |
| RAD51C | 2 (01) | 0 (00) | 0 (00) | 0 (00) | 1 (00) | – | 53 (00) | 0 (00) | 0 (00) | 1 (01) |
| RAD51D | 1 (00) | 0 (00) | 0 (00) | 0 (00) | 1 (00) | – | 19 (00) | – | 1 (00) | 0 (00) |
| RECQL4 | 0 (00) | 0 (00) | – | – | – | – | – | – | 1 (00) | – |
| SMAD4 | 0 (00) | 0 (00) | – | 0 (00) | 0 (00) | – | 3 (00) | 0 (00) | 0 (00) | 0 (00) |
| STK11 | 0 (00) | 0 (00) | 0 (00) | 0 (00) | 0 (00) | – | 4 (00) | 0 (00) | 0 (00) | 0 (00) |
| TERT | 1 (00) | – | 0 (00) | – | – | – | – | – | 0 (00) | – |
| TP53 | 5 (01)* | 0 (00) | 18 (02) | 5 (01) | 0 (00) | 6 (00) | 61 (00) | 0 (00) | 0 (00) | 2 (01) |
| TSC2 | 0 (00) | 0 (00) | – | – | – | – | – | – | 1 (00) | – |
| WRN | 0 (00) | 1 (00) | 0 (00) | – | – | – | – | – | 0 | – |
*p = 0.002. †Sample also included subjects with Hereditary Breast and Ovarian Cancer Syndrome without a Breast Cancer Diagnosis.
Of note, all TP53 variants identified in this study were the R337H, described by Achatz et al. (23) as associated to Li-Fraumeni syndrome, albeit with a later onset of disease. Even though we did not find any adrenocortical tumor in our sample, this variant has been linked to this cancer in the pediatric population of Brazil (24). In addition, this variant was identified at a surprisingly high rate (0.21%) among 35,000 newborns from an unselected population in the Southeast region of Brazil (25).
The frequency of triple-negative cancers at 17% is also in accordance with previous studies (13, 14). BRCA1 carriers had 80% of triple-negative cancers, an association long recognized in the literature (26). Triple-negative subtype was an important positive predictive factor, as a quarter of triple-negative cancers was linked to a pathogenic variant, and two-thirds of these variants were in BRCA1, an important finding that has clinical implications in the therapeutic and prophylactic settings.
As the assessment of variants segregation within families was not possible, family history was collected based on the criteria described in the Methods section. One limitation of this study is that tumors collected in family history could be sporadic, rather than associated to the pathogenic variant found in the proband. Nevertheless, family history is an easily accessible information in clinical practice, and genetic testing of all relatives up to third degree is rarely available in real life.
The association between pancreatic cancer and BRCA1 is well established, with up to 10% of familial pancreatic cancer being attributable to either a BRCA1 or BRCA2 variant (27). In our study, there were 4 cases of pancreatic cancers among 20 BRCA1 and BRCA2 carriers, 2.5 times the frequency in the group with no pathogenic variants identified.
Pathogenic variants in CHEK2 have not been traditionally linked to renal cell carcinoma, but they were the most prevalent germline alteration (3.5%) in a study of 254 advanced renal cell carcinomas (28). In our study, one family out of 4 with CHEK2 variants presented two cases of renal cell carcinoma at ages 62 and 75.
Sarcoma and TP53 is another well-established association with a cumulative incidence of approximately 20% up to age 70 among carriers of TP53 pathogenic variants (29). In our study, two out of five families with a TP53 variant had a sarcoma case, one being the proband.
To our best knowledge, this is the largest series of breast cancer patients in the Brazilian population in which all subjects had NGS multigene panel testing. Palmero et al. described 229 BRCA1 and BRCA2 variants identified in 28 centers across Brazil in subjects at high risk for hereditary breast or ovarian cancer, regardless of the sequencing method (30). There are four novel variants described in this article: BRCA1 c.1071dup, BRCA1 c.5554_5555delAC, BRCA2 c.6034del, and BRCA2 c.8009C>T. Timoteo et al. reported the distribution of pathogenic variants among 157 breast cancer patients, or at high risk for hereditary breast cancer, in the state of Rio Grande do Norte. The overall prevalence was 15%, with 11 variants in BRCA1 (07%), 5 in BRCA2 (03%), 4 in ATM (03%), 1 in ATR (01%), 1 in CDH1 (01%), and 1 in MLH1 (01%) (31). Felix et al. analyzed 106 subjects at high risk for hereditary breast cancer in the state of Bahia (32). BRCA1 was completely sequenced and specific variants in BRCA2, CHEK2, and TP53 were assessed. They found 9 variants in BRCA1, and one R337H variant in TP53. Gomes et al. studied 126 patients in the state of Rio de Janeiro, with either breast or ovarian cancer, that had at least 1 NCCN criterion and no pathogenic variants in BRCA1 or BRCA2 (33). They found one variant in ATM, two in CHEK2, one in PALB2, and one in TP53.
Furthermore, this study aimed to assess predictive factors of a positive test in addition to describing variants. Even though we were not able to detect any novel predictive factor, this article sums to the body of evidence regarding the genetic germline landscape of Brazilian breast cancer patients. It is also a call for more research on the true prevalence of TP53 variants in unselected subjects, and on the elucidation of clinical implications of specific variants from Brazil.
Conclusions
Prevalence and distribution of germline pathogenic variants in this Brazilian sample of breast cancer patients are mostly similar to other populations. However, there is a trend to an overrepresentation of TP53 pathogenic variants. Future research is warranted to clarify the true prevalence and meaning of specific variants from Brazil, particularly the TP53 R337H variant. Early-onset breast cancer patients should be offered genetic counseling, particularly those with triple-negative subtype.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics Statement
The studies involving human participants were reviewed and approved by Comitê de Ética em Pesquisa em Seres Humanos do Hospital Sírio-Libanês. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
DB is the first author. MA is the senior author. ES, JP, and CQ contributed equally to data access and management. RS, BG, and BR contributed equally to data interpretation and text revision. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.743231/full#supplementary-material
References
- 1. De Oliveira Santos M. Estimativa/2020 – Incidência De Câncer No Brasil. Rev Bras Cancerol (2020) 66(1):1. doi: 10.32635/2176-9745.rbc.2020v66n1.927 [DOI] [Google Scholar]
- 2. Buys S, Sandbach JF, Gammon A, Patel G, Kidd J, Brown K, et al. A Study of Over 35,000 Women With Breast Cancer Tested With a 25-Gene Panel of Hereditary Cancer Genes. Cancer (2017) 123(10):1721–30. doi: 10.1002/cncr.30498 [DOI] [PubMed] [Google Scholar]
- 3. King MC. “The Race” to Clone BRCA1. Sci (80-) (2014) 343(6178):1462–5. doi: 10.1126/science.1251900 [DOI] [PubMed] [Google Scholar]
- 4. Shendure J, Balasubramanian S, Church GM, Gilbert W, Rogers J, Schloss JA, et al. DNA Sequencing at 40: Past, Present and Future. Nature (2017) 550(7676):345–53. doi: 10.1038/nature24286 [DOI] [PubMed] [Google Scholar]
- 5. Couch FJ, Shimelis H, Hu C, Hart SN, Polley EC, Na J, et al. Associations Between Cancer Predisposition Testing Panel Genes and Breast Cancer. JAMA Oncol (2017) 3(9):1190–6. doi: 10.1001/jamaoncol.2017.0424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hunt KK, Euhus DM, Boughey JC, Chagpar AB, Feldman SM, Hansen NM, et al. Society of Surgical Oncology Breast Disease Working Group Statement on Prophylactic (Risk-Reducing) Mastectomy. Ann Surg Oncol (2017) (2):375–97. doi: 10.1245/s10434-016-5688-z [DOI] [PubMed] [Google Scholar]
- 7. Mann RM, Kuhl CK, Moy L. Contrast-Enhanced MRI for Breast Cancer Screening. J Magn Reson Imaging (2019) 50(2):377–90. doi: 10.1002/jmri.26654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Tutt A, Tovey H, Cheang MCU, Kernaghan S, Kilburn L, Gazinska P, et al. Carboplatin in BRCA1/2-Mutated and Triple-Negative Breast Cancer BRCAness Subgroups: The TNT Trial. Nat Med (2018) (5):628–37. doi: 10.1038/s41591-018-0009-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Robson ME, Tung N, Conte P, Im SA, Senkus E, Xu B, et al. OlympiAD Final Overall Survival and Tolerability Results: Olaparib Versus Chemotherapy Treatment of Physician’s Choice in Patients With a Germline BRCA Mutation and HER2-Negative Metastatic Breast Cancer. Ann Oncol (2019) 30(4):558–66. doi: 10.1093/annonc/mdz012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Litton JK, Rugo HS, Ettl J, Hurvitz SA, Gonçalves A, Lee KH, et al. Talazoparib in Patients With Advanced Breast Cancer and a Germline BRCA Mutation. N Engl J Med (2018) 379(8):753–63. doi: 10.1056/NEJMoa1802905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tung NM, Boughey JC, Pierce LJ, Robson ME, Bedrosian I, Dietz JR, et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J Clin Oncol (2020) 38(18):2080–106. doi: 10.1200/JCO.20.00299 [DOI] [PubMed] [Google Scholar]
- 12. Kurian AW, Hare EE, Mills MA, Kingham KE, McPherson L, Whittemore AS, et al. Clinical Evaluation of a Multiple-Gene Sequencing Panel for Hereditary Cancer Risk Assessment. J Clin Oncol (2014) 32(19):2001–9. doi: 10.1200/JCO.2013.53.6607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Simon SD, Bines J, Werutsky G, Nunes JS, Pacheco FC, Segalla JG, et al. Characteristics and Prognosis of Stage I-III Breast Cancer Subtypes in Brazil: The AMAZONA Retrospective Cohort Study. Breast (2019) 44:113–9. doi: 10.1016/j.breast.2019.01.008 [DOI] [PubMed] [Google Scholar]
- 14. Surveillance, Epidemiology, and End Results (SEER) . Program Populations (1969-2019). National Cancer Institute, DCCPS, Surveillance Research Program, released February 2021. Available at: (www.seer.cancer.gov/popdata). [Google Scholar]
- 15. Yadav S, Hu C, Hart SN, Boddicker N, Polley EC, Na J, et al. Evaluation of Germline Genetic Testing Criteria in a Hospital-Based Series of Women With Breast Cancer. J Clin Oncol (2020) 38(13):1409–18. doi: 10.1200/jco.19.02190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Oliver J, Quezada Urban R, Franco Cortés CA, Díaz Velásquez CE, Montealegre Paez AL, Pacheco-Orozco RA, et al. Latin American Study of Hereditary Breast and Ovarian Cancer LACAM: A Genomic Epidemiology Approach. Front Oncol (2019) 9:1429. doi: 10.3389/fonc.2019.01429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Li JY, Jing R, Wei H, Wang M, Xiaowei Q, Liu H, et al. Germline Mutations in 40 Cancer Susceptibility Genes Among Chinese Patients With High Hereditary Risk Breast Cancer. Int J Cancer (2019) 144(2):281–9. doi: 10.1002/ijc.31601 [DOI] [PubMed] [Google Scholar]
- 18. Shin H-C, Lee H-B, Yoo T-K, Lee ES, Kim RN, Park B, et al. Detection of Germline Mutations in Breast Cancer Patients With Clinical Features of Hereditary Cancer Syndrome Using a Multi-Gene Panel Test. Cancer Res Treat (2020) 52(3):697–713. doi: 10.4143/crt.2019.559 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Tung N, Lin NU, Kidd J, Allen BA, Singh N, Wenstrup RJ, et al. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients With Breast Cancer. J Clin Oncol (2016) 34(13):1460–8. doi: 10.1200/JCO.2015.65.0747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Tedaldi G, Tebaldi M, Zampiga V, Danesi R, Arcangeli V, Ravegnani M, et al. Multiple-Gene Panel Analysis in a Case Series of 255 Women With Hereditary Breast and Ovarian Cancer. Oncotarget (2017) 8(29):16791. doi: 10.18632/oncotarget.16791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lin PH, Kuo WH, Huang AC, Lu YS, Lin CH, Kuo SH, et al. Multiple Gene Sequencing for Risk Assessment in Patients With Early-Onset or Familial Breast Cancer. Oncotarget (2016) 7(7):8310–20. doi: 10.18632/oncotarget.7027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Gallardo-Alvarado LN, Tusié-Luna MT, Tussié-Luna MI, Díaz-Chávez J, Segura YX, Bargallo-Rocha E, et al. Prevalence of Germline Mutations in the TP53 Gene in Patients With Early-Onset Breast Cancer in the Mexican Population. BMC Cancer (2019) 19(1):118. doi: 10.1186/s12885-019-5312-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Achatz MI, Zambetti GP. The Inherited P53 Mutation in the Brazilian Population. Cold Spring Harb Perspect Med (2016) 6(12):a026195. doi: 10.1101/cshperspect.a026195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Ferreira AM, Brondani VB, Helena VP, Charchar HLS, Zerbini MCN, Leite LAS, et al. Clinical Spectrum of Li-Fraumeni Syndrome/Li-Fraumeni-Like Syndrome in Brazilian Individuals With the TP53 P.R337H Mutation. J Steroid Biochem Mol Biol (2019) 190:250–5. doi: 10.1016/j.jsbmb.2019.04.011 [DOI] [PubMed] [Google Scholar]
- 25. Custódio G, Parise GA, Filho N, Komechen H, Sabbaga CC, Rosati R, et al. Impact of Neonatal Screening and Surveillance for the TP53 R337H Mutation on Early Detection of Childhood Adrenocortical Tumors. J Clin Oncol (2013) 31(20):2619–26. doi: 10.1200/JCO.2012.46.3711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Shimelis H, LaDuca H, Hu C, Hart SN, Na J, Thomas A, et al. Triple-Negative Breast Cancer Risk Genes Identified by Multigene Hereditary Cancer Panel Testing. J Natl Cancer Inst (2018) 110(8):855–62. doi: 10.1093/jnci/djy106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Pilarski R. The Role of BRCA Testing in Hereditary Pancreatic and Prostate Cancer Families. Am Soc Clin Oncol Educ B (2019) 39:79–86. doi: 10.1200/edbk_238977 [DOI] [PubMed] [Google Scholar]
- 28. Carlo MI, Mukherjee S, Mandelker D, Vijai J, Kemel Y, Zhang L, et al. Prevalence of Germline Mutations in Cancer Susceptibility Genes in Patients With Advanced Renal Cell Carcinoma. JAMA Oncol (2018) 4(9). doi: 10.1001/jamaoncol.2018.1986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Mai PL, Best AF, Peters JA, DeCastro RM, Khincha PP, Loud JT, et al. Risks of First and Subsequent Cancers Among TP53 Mutation Carriers in the National Cancer Institute Li-Fraumeni Syndrome Cohort. Cancer (2016) 122(23):3673–81. doi: 10.1002/cncr.30248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Palmero EI, Carraro DM, Alemar B, Moreira MAM, Ribeiro-Dos-Santos Â, Abe-Sandes K, et al. The Germline Mutational Landscape of BRCA1 and BRCA2 in Brazil. Sci Rep (2018) 8(1):1–10. doi: 10.1038/s41598-018-27315-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. de Souza Timoteo AR, Gonçalves AÉMM, Sales LAP, Albuquerque BM, de Souza JES, de Moura PCP, et al. A Portrait of Germline Mutation in Brazilian at-Risk for Hereditary Breast Cancer. Breast Cancer Res Treat (2018) 172(3):637–46. doi: 10.1007/s10549-018-4938-0 [DOI] [PubMed] [Google Scholar]
- 32. Felix GES, Abe-Sandes C, Machado-Lopes TMB, Bomfim TF, Guindalini RS, Santos VC, et al. Germline Mutations in BRCA1, BRCA2, CHEK2 and TP53 in Patients at High-Risk for HBOC: Characterizing a Northeast Brazilian Population. Hum Genome Var (2014) 1:14012. doi: 10.1038/hgv.2014.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Gomes R, Spinola P da S, Brant AC, Matta BP, Nascimento CM, de Aquino Paes SM, et al. Prevalence of Germline Variants in Consensus Moderate-to-High-Risk Predisposition Genes to Hereditary Breast and Ovarian Cancer in BRCA1/2-Negative Brazilian Patients. Breast Cancer Res Treat (2021) 185(3):851–61. doi: 10.1007/s10549-020-05985-9 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.