

Abstract
Objectives
The novel coronavirus outbreak required the population's compliance with public health measures yet young adults have been identified as having low risk perceptions and relatively low adherence with preventive measures. This study investigated third-level students' COVID-19 risk perception, knowledge and attitudes, and preventive behaviours between February and June 2021 to further understand young adults' beliefs and behavioural response to the COVID-19 pandemic in Ireland.
Design
Cross-sectional quantitative online survey design.
Methods
Three hundred and sixty-four university students completed an online survey which measured risk perception, preventive behaviours, knowledge of COVID-19, vaccination attitude and source of COVID-19 information.
Results
University students in Ireland reported high levels of knowledge of COVID-19 and high adherence to preventive behaviours. While risk perception levels were moderately high, students displayed higher concern for others than for themselves. High levels of risk perception significantly predicted preventive behaviours while general knowledge of the virus increased the likelihood of vaccine uptake. Over two-thirds of participants were willing to take the COVID-19 vaccine if available.
Conclusions
Vaccination hesitancy remains a concern among the young adult population requiring urgent attention from public health officials. The implication for health policymakers is that positive behavioural responses of the young population can be reinforced by targeting risk perceptions and by increasing the public's knowledge and understanding of COVID-19.
Keywords: COVID-19, Risk perception, Preventive behavior, Third-level students, Young adults
1. Introduction
Coronavirus disease 2019 (COVID-19) was first reported in the city of Wuhan, China in December 2019 and a pandemic was later declared in March 2020 (World Health Organization [WHO], 2020). As of July 2021, over 286 thousand cases have been confirmed and the virus has claimed over five thousand lives in Ireland (Department of Health, 2021a). Due to the pandemic, non-essential businesses closed temporarily and access to schools and universities was restricted (Capone et al., 2020). National measures were put in place and people were required to stay at home except for essential reasons (Citizens Information, 2021). To maximise the effectiveness of the public health response, it is critical to understand the factors influencing compliance to the established measures (Liekefett & Becker, 2020).
Risk perception has been identified as a significant factor influencing peoples' response to the coronavirus pandemic (Alicea-Planas et al., 2021). It refers to an individual's perception, evaluation and understanding of potential threats and hazards, and is influenced by beliefs, experiences, feelings, attitudes and judgements as well as social, cultural and contextual factors (Cori et al., 2020). It has three distinct dimensions: perceived likelihood (the probability that an individual will be harmed by a given hazard), perceived susceptibility (the constitutional vulnerability of an individual to a hazard) and perceived severity (the extent of harm that could be caused by a hazard) (Brewer et al., 2007; Darker, 2013).
Health behavior theories suggest that risk perception motivates engagement with preventive behaviours (De Bruin & Bennett, 2020). Theories including the Health Belief Model (Rosenstock, 1974) and Health Action Process Approach (Schwarzer, 1992) propose that high perceived risk encourages acting towards reducing potential risks (Brewer et al., 2004). Ferrer and Klein (2015) argue that although risk perceptions are key determinants of health-related behavior, understanding the nature of this association is not straightforward. Previous literature reports disparate findings including positive, negative or even no association between risk perception and health behaviours, while meta-analyses report significant but small positive effects (Brewer et al., 2007; Sadique et al., 2007). This inconsistency in findings hampers the interpretation and comparison of research focusing on risk perception and health-related behaviours.
Research proposes that young adults have lower general risk perception and consequently are inclined to take more risks (Steinberg, 2008). Some researchers claim that young adults perceive themselves as being invulnerable to the consequences of their risky behaviours and underestimate these risks, negatively influencing the initiation and maintenance of health-promoting behaviours (Kim et al., 2018). This invulnerability hypothesis has dominated the understanding of risk perception during youth for decades (McErlean & Fekete, 2018). Cohn et al. (1995), however, suggest that adolescents fail to perceive situations as risky rather than feeling invulnerable towards the risk.
Developmental neuroscience research claims that increased risk-taking during adolescence and young adulthood is due to heightened reactivity to emotions, particularly reward-seeking, and immature capacity for self-regulation, rather than risk perception (Steinberg, 2008). While adolescents have similar cognitive capacities to adults, adolescents are more impulsive and attracted to the immediate consequences of their decisions and their potential beneficial outcomes rather than the costs associated with such decisions (Reniers et al., 2016).
Moreover, males have been identified as being more impulsive and more attracted to the outcomes of risk decisions than females (Reniers et al., 2016). Recent COVID-19 studies note that male students report lower risk perception and are less likely to adopt preventive behaviours (Ding et al., 2020; Yuan et al., 2020). In addition, conditional on contracting COVID-19, males are at an increased risk of developing more severe symptoms (Jin et al., 2020) and fatality rates are higher for males (Dehingia & Raj, 2021). This increased vulnerability may be due to immunological differences (Galasso et al., 2020) but also may be due to behavioural factors, as males display higher levels of health-risk behaviours e.g., smoking, while females engage in more health-protective behaviours (Bwire, 2020).
Furthermore, recent COVID-19 studies propose that the population's risk perception increases as the pandemic progresses and more information becomes available. In Italy, for example, risk perception increased significantly during the second COVID-19 wave compared to the first wave (Rubaltelli et al., 2020). On the same note, previous literature on severe acute respiratory syndrome suggests that people are more likely to comply with health measures if they perceive a high risk of being infected and getting the disease (Commodari, 2017), for example, during a rise in disease cases.
It is vital to understand young adults' risk perception and their willingness and ability to engage in the recommended measures as Irish reports have shown consistently high infection rates among individuals aged 19–34. While this age group accounted for 28% of all confirmed cases in January 2021, rates increased to 42% in June 2021 (Health Protection Surveillance Centre, 2021). Nevertheless, studies suggest that over 80% of young people engage in preventive behaviours mainly motivated by social responsibility (78.1%) and wanting to protect others (77.9%) rather than personal perceived risk (57.8%) (Oosterhoff et al., 2020).
Other studies support the finding that young people engage in preventive behaviours predominantly to protect others. Liekefett and Becker (2020) report that 40% of German participants adhered to health recommendations for self-protection while 42% adhered to protect at-risk groups. Ding et al. (2020) found that Chinese students were more concerned for their older family members and only a minority perceived themselves to be at risk of COVID-19 infection. Similarly, Franzen and Wöhner (2021) found that Swiss students perceived the virus as being dangerous for the society but not for themselves. Taking these findings together, young people appear to have higher risk perception towards others rather than personal risk perception. However, these findings require replication to ensure generalisability across other nationalities.
WHO (2021) emphasises the importance of knowledge of COVID-19 by suggesting that the best way to curtail the spread of the virus is to be well informed about the virus, its symptoms and how it spreads. Therefore, knowledge is imperative, and research has confirmed that greater knowledge indicates higher risk perception and higher engagement in protective behaviours (Alicea-Planas et al., 2021). Iorfa et al. (2020) propose that the relationship between knowledge and preventive behaviours is mediated by risk perception and this effect is moderated by gender, with knowledge of COVID-19 being linked with higher preventive behaviours through risk perception for females but not males. This mediating role of risk perception is in agreement with the intention-behavior gap which proposes that knowledge alone does not drive behavior (Finset et al., 2020).
COVID-19 vaccinations are considered the most effective preventive measure, in tandem with other protective behaviours. Vaccination is a long-term solution with the potential of reducing morbidity and mortality while also releasing resources and pressure from the healthcare system (Orenstein & Ahmed, 2017). As COVID-19 vaccines were first made available in the final months of 2020, it is important to understand the factors hindering and facilitating the acceptance of vaccines. Dror et al. (2020) highlight that although a vaccine may become available, it does not guarantee sufficient vaccination across the population due to vaccination hesitancy. Sociodemographic variables and risk perception have been identified as key factors influencing vaccination acceptance (Graffigna et al., 2020; Nguyen et al., 2011).
Research findings suggest that young adults are more likely than other age groups to be hesitant to accept the vaccine (Soares et al., 2021). In one study, 14% of Italian university students had low intentions of getting the vaccine (Barello et al., 2020). A survey conducted in March and April 2020 indicated that in Ireland, only 65% of the population reported accepting a COVID-19 vaccine if one were to become available, while 26% were hesitant and 9% were resistant (Murphy et al., 2021). However, vaccine acceptance has been consistently increasing over time in Ireland, with acceptance rates among adults increasing from 68% in January 2021 to 76% in July 2021 (Department of Health, 2021b). Moreover, acceptance rates among those aged 18–34 have been noticeably high with 90% of individuals reporting accepting the vaccine (Department of Health, 2021b).
1.1. The current study
Ireland has been noteworthy globally due to its strict COVID-19 containment measures; it is the European country with the longest lockdown restrictions and closure of public places and businesses during the first wave of the COVID-19 pandemic (Health at a Glance, 2020). Yet there is a paucity of research investigating COVID-19 and its related factors in Ireland. With Irish reports identifying consistently high levels of COVID-19 infection among the young population, there is a need to investigate young adults' responses to the pandemic. However, a lack of consensus regarding risk perception among young adults poses difficulties in understanding their response to the current coronavirus pandemic. Recent international research proposes disparate findings regarding risk perception among young adults, with some research reporting high levels of risk perception among young adults while others report low levels of personal risk perception but higher perceived risk towards others. Research appears to agree that despite the levels of risk perception, young adults continuously report high levels of engagement with preventive behaviours, possibly motivated by the desire to protect others in the society. While a small number of international studies have explored COVID-19 related risk perception and preventive behaviours among young adults, there is a lack of research investigating these factors in an Irish context. As a large proportion of third-level students fall within the age category of young adults (18–25), third-level students were the selected sample for the current study.
The current study is a cross-sectional quantitative online survey with the objective of investigating third-level students' COVID-19 risk perception and preventive behaviours and exploring related factors. Third-level students refer to students enrolled in either universities, institutes of technology or colleges of education (Citizens Information, 2020). To the best of our knowledge, this is the first study investigating risk perception and preventive behaviours among third-level students during COVID-19 in an Irish context. Given the variability in vaccine hesitancy rates and the potential challenges it presents to vaccine rollout, this study also aims to understand the factors influencing vaccination intentions in third-level students in Ireland. The current study sought to test the following hypotheses:
H1
Risk perception and preventive behaviours differ according to age (under vs over age of 25) and sex (females display higher risk perception and greater adoption of preventive behaviours).
H2
Higher risk perception is associated with higher levels of preventive behaviours.
H3
Greater knowledge of COVID-19 is associated with higher risk perception.
H4
Risk perception, knowledge of COVID-19 and demographic variables predict preventive behaviours, including vaccination intentions.
2. Method
2.1. Participants
The sample included 364 third-level students (77.2% females, 22.3% males) in Ireland who self-selected to take part in the study. To be eligible for participation, participants needed to be aged 18 or above, be currently enrolled in any third-level Irish institution and be fluent in the English language. Participants were invited to take part via email, social media platforms and an online research recruitment system within National University of Ireland (NUI), Galway. Participants who were recruited via the online research recruitment system were Undergraduate Psychology students in NUI, Galway who were required to participate in research in exchange for course credits. The survey also featured in one weekly student email which was forwarded to all students within NUI, Galway. The survey was also made available on social media platforms, i.e., Facebook, Twitter, LinkedIn. Participants who were recruited outside the recruitment service were given the opportunity to enter a draw for a €40 voucher.
A power calculation was conducted, using G*Power, which indicated that a sample size of a minimum of 84 third-level students was required to detect a medium effect size with an alpha level of 0.05 and a power level of 80%.
2.2. Measures
An online survey was designed to collect the data. The primary outcome measures were risk perception, knowledge of COVID-19 and preventive measures, including vaccination attitude. The secondary outcomes were demographic variables and sources of COVID-19 information. For full details of the survey, see supplementary material.
2.2.1. Demographics
Demographic information included age, sex, nationality, third-level institution, subject of study, level of degree, part/full-time enrolment and living situation. Participants were also asked to indicate if themselves, family or friends had been diagnosed with COVID-19 or had been close contacts of confirmed or suspected cases.
2.2.2. Knowledge
The measure of the level of COVID-related knowledge was adapted from previous studies (Taghrir et al., 2020; Yuan et al., 2020). The first part of this measure was based on the measure used by Taghrir et al. (2020) and was composed of statements about COVID-19 for which participants had to answer true or false. Additional statements were retrieved from Yuan et al. (2020) and a total of 16 items were included. Items included facts about COVID-19, symptoms, treatment, transmission and prevention of the virus. Examples of items include ‘COVID-19 is a respiratory infection caused by a new species of coronavirus family’, ‘the disease can be treated by usual antibiotic drugs’ and ‘the disease can be prevented through handwashing and personal hygiene’. The scoring system was consistent with that used in Taghrir et al. (2020). Participants answered with true or false and one point was assigned for each correct answer while incorrect answers were assigned no points. Reliability tests were carried out for this measure and a Cronbach's alpha of 0.80 was obtained in the original study (Taghrir et al., 2020). The second part of this measure was retrieved from Ding et al. (2020) and was composed of two items ‘what are the common symptoms of COVID-19’ and ‘who is susceptible to contracting COVID-19’. Ding et al. (2020) reported a Cronbach's alpha of 0.64 for their complete measures, however, only the above two items were used for this current study. Participants were required to tick the boxes for the correct answers. Each correct answer was assigned one point. The points for the two parts were added. Points ranged from 0 to 22. Higher scores indicated higher levels of COVID-related knowledge.
2.2.3. Preventive behaviours
A measure of self-reported preventive behaviours was adapted from a measure available from Khasawneh et al. (2020). The marking guidelines were based on the measure by Khasawneh et al. (2020) and additional items were retrieved from Taghrir et al. (2020) and were included in the measure. The preventive behaviours measure consisted of 18 items and participants responded to a 3-point Likert scale ranging from never to often/always. Examples of items included ‘I avoid meetings with friends, eating-out and sport events’ and ‘I clean and disinfect items that can be easily touched with hands (i.e., door handles, surfaces, mobile phone)’. Responses were converted to points (1 = never; 3 = often/always) and points were totalised for each participant. Points ranged from 18 to 54. Higher points indicated higher engagement with preventive behaviours. Validity and reliability tests for this measure were not available.
2.2.4. Vaccination attitude
Vaccination attitude was measured using a single question, ‘if a vaccine for COVID-19 were immediately available, what is the likelihood you would get vaccinated?’ Participants responded on a 3-point Likert scale ranging from unlikely to extremely likely. The answer ‘likely’ represented vaccine acceptance, ‘somewhat likely’ represented hesitancy, and ‘unlikely’ represented resistance. Participants who responded ‘somewhat likely’ or ‘unlikely’ were asked to tick the box(es) for the reasons for their hesitance or resistance, as obtained from Neumann-Böhme et al. (2020). Reasons included, but were not limited to, ‘I'm concerned of the potential side effects’ and ‘I don't think that COVID-19 is dangerous to my health’. No validity and reliability tests were available for this measure.
2.2.5. Risk perception
Risk perception was assessed using a measure developed by Lanciano et al. (2020). This measure contained nine items and was measured on an 11-point Likert scale ranging from 0 = not at all to 10 = very much. This measure was composed of two parts – health risk concern and health risk likelihood. These two parts were added to obtain overall risk perception. The nine items assessed participants concern for their own health, health of loved ones, return to everyday life, and estimated likelihood of contagion, death and recovery. Examples of items included ‘how worried/concerned are you about your life?’ and ‘how likely do you think it is that you might become infected with COVID-19?’. Scores ranged from 0 to 90. Higher scores indicate higher risk perception. Reliability tests for this measure reported Cronbach alpha scores of over 0.70 in the original study (Lanciano et al., 2020).
2.2.6. Source of information
Source of COVID-19 information was assessed using the measure available in Khasawneh et al. (2020). This contained 10 items and was measured on a 4-point Likert scale ranging from 1 = never to 4 = most of the time. Sources of information included social media, internet search engines, medical search engines, official sites, TV news channels, family and friends, healthcare workers, Non-Governmental Organisations (NGOs), religious leaders, and other. Participants were asked to report the frequency in which they used the above sources. Validity and reliability tests were not available for this measure.
2.3. Procedure
The online survey was created and distributed using Qualtrics, a web-based survey platform. The survey was made available from 16th February to 14th June 2021. This encompassed a period in which Ireland was facing national restrictions (16th February to 11th April) and a period in which such restrictions were eased (12th April to 14th June). Upon accessing the survey, participants were first presented with information on the study and instructed to consent to participating by ticking the consent options. Participants then completed the six sections of the survey – demographics, knowledge, preventive behaviours, vaccination attitude, risk perception and source of information. Participants who accessed the survey outside of the research recruitment service were given the option to enter their email to be included in a €40 voucher draw. Contact information for various mental health resources were made available at the end of the survey and participants were instructed to contact their GPs if concerned about their health or health of their loved ones.
2.4. Statistical analysis
Data analysis was conducted using SPSS Version 26. Descriptive statistics were used to describe demographic variables. Correlation coefficients, t-tests and multiple regression tests were used to assess the study hypotheses. Independent-samples t-tests were conducted to compare responses obtained during national restriction periods and post-restriction periods in Ireland. Correlation coefficients were used to analyse the relationship between risk perception, preventive behaviours and knowledge of COVID-19. Multiple regressions were used to determine if demographic variables, knowledge of COVID-19 and risk perception predicted general preventive behaviours and vaccination intention exclusively. t-Tests were used to analyse age and sex differences between risk perception and preventive behaviours.
2.5. Data preparation
In relation to missing data, participants' responses were considered missing data if one or more of the major sections of the survey were incomplete. Major sections included risk perception, preventive behaviours, vaccination attitude and knowledge of COVID-19, as can be viewed in Supplementary File S1. Thirty-six responses were excluded due to missing data. One participant had incomplete data for the ‘source of information’ section. However, as it was not a major section, the participant's response was still included. For data analysis purposes, total scores were calculated for knowledge of COVID-19 and preventive behaviours. Risk perception scores were calculated into overall total scores, and total scores of two distinct dimensions; health risk likelihood and health risk concern (see Supplementary Table S2).
2.6. Ethics statement
Ethical approval was received from the NUI Galway School of Psychology Research Ethics Committee.
3. Results
3.1. Descriptive statistics
Table 1 summarises the socio-demographic characteristics of the participants. The majority of respondents were from NUI Galway (98.9%), were completing an undergraduate degree (94%) and were enrolled on a full-time basis (96.7%). Table 2 shows participants' self-reported personal experiences with COVID-19. Descriptive statistics for risk perception, knowledge of COVID-19 and preventive behaviours are presented in Table 3 . Participants reported high levels of knowledge of COVID-19, with an overall mean score of 19.62 (SD = 1.41) out of a total score of 22. Similarly, engagement with preventive behaviours was high, with an overall mean score of 46.70 (SD = 4.75) out of a total score of 54. Risk perception was found to be moderate, with an overall mean score of 47.33 (SD = 12.61) out of a total score of 90. As regards vaccination attitude, of the 364 participants, 35 (9.6%) were unlikely to accept the vaccine, 93 (25.5%) were somewhat likely, 229 (62.9%) were extremely likely and 7 (1.9%) had already received the vaccine. Descriptive statistics for source of COVID-19 information are further presented in Table 8.
Table 1.
Characteristics of third-level students who participated in the current study (N = 364).
| Variable | Characteristic | n (%) | M (SD) | Range |
|---|---|---|---|---|
| Age (in years) | Under 25 | 339 (93.1) | 20.31 (3.88) | 18–47 |
| Over 25 | 25 (6.9) | |||
| Sex | Female | 281 (77.2) | ||
| Male | 81 (22.3) | |||
| Prefer not to say | 2 (0.5) | |||
| Nationality | Irish | 334 (91.8) | ||
| Europeana | 16 (4.4) | |||
| Other | 14 (3.8) | |||
| Living situation | Living at home | 250 (68.7) | ||
| Shared student accommodation | 73 (20.1) | |||
| Independent student accommodation | 23 (6.3) | |||
| Private accommodation | 15 (4.1) | |||
| Other | 3 (0.8) |
Includes other European countries excluding Ireland.
Table 2.
Personal COVID-19 experiences as reported by participants (N = 364).
| n | % | ||
|---|---|---|---|
| COVID-19 (have you and your family and friends been diagnosed with COVID-19 so far?) | Myself | 37 | 10.2 |
| Family/relatives | 134 | 36.8 | |
| Friends | 164 | 45.1 | |
| Other people I know | 150 | 41.2 | |
| No one I know | 61 | 16.8 | |
| COVID-19 (have you or your family or friends come into contact with a person or a suspected patient infected with COVID-19 so far?) | Myself | 118 | 32.4 |
| Family/relatives | 161 | 44.2 | |
| Friends | 165 | 45.3 | |
| Other people I know | 119 | 32.7 | |
| No close contact | 72 | 19.8 | |
Table 3.
Differences in knowledge, preventive behaviours and risk perception according to sex, age and response date (N = 364).
| Variable | Characteristic | n (%) | Knowledge of COVID-19 Range 15–22 |
Preventive behaviours Range 18–54 |
Risk perception Range 17–77 |
|||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||
| Sex | Male | 81 (22.3) | 19.60 | 1.38 | 45.27 | 5.15 | 42.73 | 12.78 |
| Female | 281 (77.2) | 19.62 | 1.43 | 47.11 | 4.57 | 48.69 | 12.20 | |
| Undisclosed | 2 (0.5) | 19.50 | 0.71 | 47.00 | 1.41 | 43.50 | 27.58 | |
| Age | Under 25 | 339 (93.1) | 19.61 | 1.41 | 46.65 | 4.75 | 47.11 | 12.31 |
| 26+ | 25 (6.9) | 19.72 | 1.51 | 47.36 | 4.75 | 50.40 | 16.22 | |
| Response date | During restrictions | 236 (64.8) | 19.64 | 1.41 | 47.16 | 4.38 | 48.34 | 12.57 |
| Post-restrictions | 128 (35.2) | 19.55 | 1.42 | 45.85 | 5.26 | 45.48 | 12.54 | |
| Overall | 364 (100%) | 19.62 | 1.41 | 46.70 | 4.75 | 47.33 | 12.61 | |
Table 8.
Sources of COVID-19 information (N = 363).
| Source | Frequency of use n (%) |
|||
|---|---|---|---|---|
| Never | Rarely | Sometimes | Most of the time | |
| Social media | 18 (4.9) | 35 (9.6) | 115 (31.6) | 195 (53.6) |
| Internet search engines | 27 (7.4) | 57 (15.7) | 141 (38.7) | 138 (37.9) |
| Academic search engines | 112 (30.8) | 137 (37.6) | 85 (23.4) | 29 (8.0) |
| Official sites | 28 (7.7) | 47 (12.9) | 122 (33.5) | 166 (45.6) |
| TV news channels | 16 (4.4) | 26 (7.1) | 91 (25.0) | 230 (63.2) |
| Family and friends | 5 (1.4) | 39 (10.7) | 165 (45.3) | 154 (42.3) |
| Healthcare workers | 80 (22.0) | 105 (28.8) | 106 (29.1) | 72 (19.8) |
| Non-governmental organisations (NGOs) | 136 (37.4) | 141 (38.7) | 68 (18.7) | 18 (4.9) |
| Religious leaders | 318 (87.4) | 33 (9.1) | 8 (2.2) | 4 (1.1) |
| Others | 257 (70.6) | 54 (14.8) | 40 (11.0) | 12 (3.3) |
Note: missing data on one participant.
3.2. Normality of variables
Histograms were inspected to determine normal distributions for risk perception, preventive behaviours and knowledge. As regards the risk perception survey section, a normal distribution was observed from the histogram and this was confirmed using a Shapiro-Wilk test, W(364) = 0.99, p = .056. As regards preventive behaviours, normal distributions were not observed from the histogram as scores were negatively skewed. A significant departure from normality was confirmed by a Shapiro-Wilk test, W(364) = 0.92, p < .001. As regards knowledge, normal distributions were not observed from the histogram as scores were also negatively skewed. A Shapiro-Wilk test, W(364) = 0.90, p < .001, confirmed a significant departure from normality. Parametric tests were still used in this study as according to the central limit theorem, the distribution of means of variables approximates normality when the sample size is sufficiently large (Kwak & Kim, 2017).
3.3. Reliability of measures
The reliability of the two primary outcomes – preventive behaviours and risk perception – and the secondary outcome, knowledge, was examined using Cronbach's Alpha. Cronbach's Alpha for the preventive behaviours section of the survey was 0.80, demonstrating excellent internal reliability for this measure. Cronbach's Alphas were calculated for overall scores (α = 0.76), total health risk concern (α = 0.66) and total health risk likelihood (α = 0.67) of the risk perception measure. As there was a small number of items in the risk perception measure, mean inter-item correlations were also calculated as advised by Pallant (2020). Mean inter-item correlation values for overall risk perception, total health risk concern and total health risk likelihood were 0.26, 0.41 and 0.26 respectively. Cronbach's Alpha for the knowledge section of the survey was 0.54, demonstrating poor internal reliability for this measure, possibly due to the fact that this measure was adapted from other measures as stated in Section 2.2.
3.4. Hypothesis 1: Risk perception and preventive behaviours differ according to age and sex
An independent-samples t-test was conducted to assess whether third-level students aged 25 or under have lower risk perception levels than those aged over 25. The independent variable was age and the dependent variable was self-reported risk perception levels. Levene's test of equality of variance was significant (F = 5.66, p = .018), suggesting that the assumption of homogeneity of variances was violated. A t-test for unequal variances was then used. The results of the t-test indicated that there was no difference between those aged 25 or under and those aged over 25 in relation to self-reported risk perception (t(362) = −1.26, p = .208).
A one-way between-subjects ANOVA was conducted to evaluate the hypothesis that risk perception levels differed according to sex. The independent variable was sex and had three levels: female, male and undisclosed. The dependent variable was self-reported risk perception levels measured on a scale ranging from 0 to 90 (0 = lowest risk perception, 90 = highest risk perception). Levene's test for homogeneity of variance was not significant (F = 1.77, p = .172), ensuring homogeneity of variance. The results of the ANOVA revealed a significant difference in sex on risk perception levels (F (2,363) = 7.36, p = .001). The mean and standard deviation scores are presented in Table 3. A Tukey HSD post hoc test was carried out to establish where the significant differences were. The post hoc test revealed a significant difference in mean risk perception scores between males and females (p < .001) with males (M = 42.73, SD = 12.78) reporting lower risk perception scores than females (M = 48.69, SD = 12.20). There were no significant differences between risk perception scores for those who preferred not to disclose their sex and males (p = .996) or females (p = .826).
A second independent-samples t-test was conducted to evaluate the hypothesis that young adults aged 25 or under engage in less preventive behaviours than adults over the age of 25. The independent variable was age, and the dependent variable was self-reported preventive behaviours. Levene's test for equality of variance was not significant (F = 0.10, p = .754), ensuring homogeneity of variance. The results of the t-test indicated that there was no significant difference between those aged under and over 25 in relation to engagement in preventive behaviours (t (362) = −0.72, p = .472).
A one-way between-subjects ANOVA was conducted to evaluate the hypothesis that engagement in preventive behaviours differed according to sex. The independent variable was sex and had three levels: male, female and undisclosed. The dependent variable was self-reported preventive behaviours which was measured on a scale of 18 to 54 (18 = lowest preventive behaviours, 54 = highest preventive behaviours). Levene's test for homogeneity of variance was not significant (F = 1.87, p = .155), ensuring homogeneity of variance. A significant difference in sex on preventive behaviours was observed (F (2,363) = 4.82, p = .009). The mean and standard deviation scores are displayed in Table 3. A Tukey HSD post hoc test was carried out to establish where the significant differences were. The post hoc test revealed a significant difference between females and males in their levels of engagement in preventive behaviours (p = .006), with females (M = 47.11, SD = 4.57) engaging in higher levels of preventive behaviours than males (M = 45.27, SD = 5.15). There were no significant differences for preventive behavior levels between those who did not disclose their sex and males (p = .864) or females (p = .999).
3.4.1. Response Dates: Comparing risk perception and preventive behaviours according to response period
An independent-samples t-test was conducted to assess whether third-level students who responded to the survey during the restrictions differed in risk perception from those who responded after the restrictions were lifted. The independent variable was response date and the dependent variable was self-reported risk perception levels. Levene's test for equality of variance was not significant (F = 0.00, p = .958), ensuring homogeneity of variance. The results of the t-test indicated that there was a significant difference between those who responded during the restrictions and post-restrictions in relation to risk perception levels (t (362) = 2.08, p = .039). Students who responded during the restrictions (M = 48.34, SD = 12.57) reported higher risk perception levels than those who responded after the restrictions were lifted (M = 45.48, SD = 12.54).
A final independent-samples t-test was conducted to evaluate whether third-level students who responded to the survey during the restrictions differed in self-reported preventive behaviours from those who responded after the restrictions were lifted . The independent variable was response date, and the dependent variable was self-reported preventive behaviours. Levene's test for equality of variance was not significant (F = 0.64, p = .423), ensuring homogeneity of variance. The results of the t-test indicated that there was a significant difference between those who responded during restrictions and post-restrictions in relation to self-reported preventive behaviours (t (362) = 2.53, p = .012). Students who responded during the restrictions (M = 47.16, SD = 4.38) reported higher engagement in preventive behaviours than those who responded after the restrictions were lifted (M = 45.85, SD = 5.26).
3.5. Hypothesis 2: Risk perception and preventive behaviours
A Pearson's Product-Moment correlation coefficient was conducted to investigate if a correlation existed between risk perception and preventive behaviours. It was found that a positive moderate correlation existed (r = 0.32, p < .001), such that as risk perception increased, preventive behaviours also increased (see Fig. 1 ).
Fig. 1.
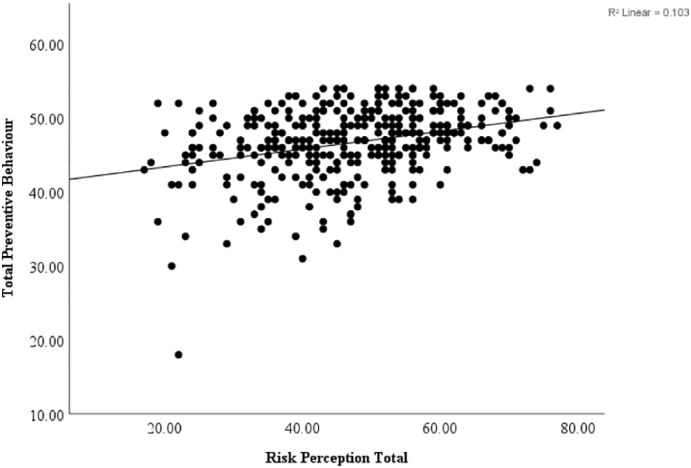
Correlation between risk perception and preventive behaviours.
3.6. Hypothesis 3: Knowlegde and risk perception
A Pearson's Product-Moment correlation coefficient was conducted to see if a correlation between risk perception and knowledge of COVID-19 existed. It was found that there was no significant correlation between risk perception and knowledge (r = −0.01, p = .841). More details on participants' knowledge of COVID-19 can be found in Supplementary Table S1.
3.7. Hypothesis 4: Predictors of preventive behaviours
A hierarchical multiple regression was conducted to examine if socio-demographic characteristics, personal COVID-19 experience, knowledge of COVID-19 and risk perception predicted preventive behaviours among third-level students in Ireland, while controlling for response date. The predictor variable, response date, was entered into the first block. The predictor variable, socio-demographic characteristics, which included age, sex, nationality and living situation, were entered into the second block. Personal COVID-19 experience, which included positive COVID-19 diagnosis for self, family, friends or others, and close contact of a positive case for self, family, friends or others, were entered into the third block. Knowledge of COVID-19 was entered into the fourth block and the remaining predictor variable, risk perception, was entered into the fifth block. The criterion variable was self-reported preventive behaviours. Means, standard deviations and frequencies for predictor and criterion variables can be found in the tables above. Further details on self-reported preventive behaviours can be found in Supplementary Table S3.
Multicollinearity was not present in the data. Pearson's Correlation statistics for predictor variables were less than 0.7, as portrayed in Table 4 . The variance inflation factor (VIF) scores were less than 10 (range = 1.03–2.02) and tolerance scores were greater than 0.1 (range = 0.50–0.97).
Table 4.
Pearson's and biserial correlations between predictors and criterion variables preventive behaviours and vaccination attitude (N = 364).
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Preventive behaviours | |||||||||||||||
| 2. Vaccination attitude - acceptance | 0.18⁎⁎ | ||||||||||||||
| 3. Age | 0.07 | −0.05 | |||||||||||||
| 4. Sex - Female | 0.16⁎ | 0.03 | −0.09 | ||||||||||||
| 5. Self - COVID-19 positive | −0.02 | −0.02 | −0.00 | −0.03 | |||||||||||
| 6. Family - COVID-19 positive | 0.02 | 0.03 | −0.07 | 0.05 | 0.08 | ||||||||||
| 7. Friends - COVID-19 positive | −0.05 | 0.03 | −0.08 | 0.06 | 0.15⁎ | 0.10 | |||||||||
| 8. Others - COVID-19 positive | 0.03 | 0.04 | −0.01 | 0.00 | 0.07 | −0.06 | 0.01 | ||||||||
| 9. No positive case identified | 0.05 | −0.09 | 0.13⁎ | −0.05 | −0.15⁎ | −0.34⁎⁎ | −0.41⁎⁎ | −0.38⁎⁎ | |||||||
| 10. Self - close contact | −0.11⁎ | −0.02 | −0.02 | 0.04 | 0.43⁎⁎ | 0.18⁎ | 0.27⁎⁎ | 0.14⁎ | −0.22⁎⁎ | ||||||
| 11. Family - close contact | 0.01 | 0.16⁎ | −0.02 | −0.07 | 0.10⁎ | 0.36⁎⁎ | 0.16⁎ | 0.04 | −0.21⁎⁎ | 0.19⁎⁎ | |||||
| 12. Friends - close contact | −0.04 | 0.09 | −0.03 | −0.04 | 0.17⁎ | 0.14⁎ | 0.49⁎⁎ | 0.16⁎ | −0.29⁎⁎ | 0.28⁎⁎ | 0.31⁎⁎ | ||||
| 13. Others - close contact | −0.02 | 0.02 | 0.07 | 0.03 | 0.13⁎ | 0.04 | 0.18⁎ | 0.49⁎⁎ | −0.23⁎⁎ | 0.17⁎ | 0.10 | 0.28⁎⁎ | |||
| 14. No close contact identified | 0.03 | −0.11⁎ | 0.07 | −0.01 | −0.14⁎ | −0.18⁎ | −0.23⁎⁎ | −0.15⁎ | 0.42⁎⁎ | −0.34⁎⁎ | −0.43⁎⁎ | −0.44⁎⁎ | −0.33⁎⁎ | ||
| 15. Knowledge of COVID-19 | 0.14⁎ | 0.12⁎ | 0.05 | 0.01 | −0.03 | 0.01 | 0.00 | 0.07 | 0.01 | 0.00 | 0.05 | 0.08 | 0.07 | −0.01 | |
| 16. Risk perception | 0.32⁎⁎ | 0.02 | 0.06 | 0.20⁎⁎ | −0.10 | 0.04 | −0.06 | 0.03 | −0.03 | −0.05 | 0.04 | 0.02 | −0.04 | −0.07 | −0.01 |
Note: associations between dichotomous variables were analysed using Chi-Square test of independence with Phi (φ).
p < .05.
p < .001.
The results of the multiple regression analysis show that the overall model was significant, accounting for 14% of the variance in self-reported preventive behaviours (F (20,343) = 3.98, p < .001, R 2 = 0.19, adjusted R 2 = 0.14), as can be seen in Table 5 .
Table 5.
Summary of hierarchical regression model for variables predicting self-reported preventive behaviours.
| Step | Variable | β | ΔR2 | Adjusted ΔR2 | F change |
|---|---|---|---|---|---|
| 1 | Response date | −0.06 | 0.02 | 0.02 | 6.41⁎ |
| 2 | Age | 0.03 | |||
| Female vs. other sex | 0.11⁎ | ||||
| Irish vs. non-Irish | 0.03 | ||||
| Shared student accommodation vs. living at home | −0.17⁎ | ||||
| Independent student accommodation vs. living at home | −0.01 | ||||
| Other accommodation vs. living at home | −0.02 | ||||
| Private accommodation vs. living at home | 0.03 | 0.04 | 0.03 | 2.63⁎ | |
| 3 | Self - COVID-19 positive case | 0.09 | |||
| Family - COVID-19 positive case | 0.04 | ||||
| Friends - COVID-19 positive case | 0.06 | ||||
| Others - COVID-19 positive case | 0.08 | ||||
| No positive case identified | 0.08 | ||||
| Self - close contact of positive case | −0.11 | ||||
| Family - close contact of positive case | 0.01 | ||||
| Friends - close contact of positive case | −0.04 | ||||
| Others - close contact of positive case | −0.02 | ||||
| No close contact | −0.02 | 0.02 | −0.02 | 0.65 | |
| 4 | Knowledge of COVID-19 | 0.15⁎ | 0.02 | 0.01 | 6.94⁎ |
| 5 | Risk perception | 0.32⁎⁎ | 0.09 | 0.08 | 36.80⁎⁎ |
Total R2 = 0.19, adjusted R2 = 0.14.
p < .05.
p < .001.
Step one, response date, contributed significantly to the model, explaining 2% of the variance in self-reported preventive behaviours (F (1,362) = 6.41, p = .012, ΔR 2 = 0.02, adjusted ΔR 2 = 0.02). Step two, sociodemographic characteristics, contributed significantly to the model, explaining 3% of the variance in self-reported preventive behaviours (F (7,355) = 2.63, p = .012, ΔR 2 = 0.04, adjusted ΔR 2 = 0.03). Step three, personal COVID-19 experience, did not significantly contribute to the model (F (10,345) = 0.65, p = .773, ΔR 2 = 0.02, adjusted ΔR 2 = −0.02). Step four, knowledge of COVID-19, significantly contributed to the model, explaining 1% of the variance in self-reported preventive behaviours (F (1,344) = 6.94, p = .009, ΔR 2 = 0.02, adjusted ΔR 2 = 0.01). Step five, risk perception, also significantly contributed to the model, explaining 8% of the variance in self-reported preventive behaviours (F (1,343) = 36.80, p < .001, ΔR 2 = 0.09, adjusted ΔR 2 = 0.08).
Examination of the standardised beta coefficients revealed that being female (β = 0.11, p = .034), living in shared student accommodation versus living at home (β = −0.17, p = .002), knowledge of COVID-19 (β = 0.15, p = .003) and risk perception (β = 0.32, p < .001) were the only significant contributors to the variance in self-reported preventive behaviours.
3.7.1. Vaccination attitude
Participants who responded ‘unlikely’ or ‘somewhat likely’ to accepting the vaccine were classified as resistant and those who were ‘extremely likely’ or had received the vaccine were classified as accepting. A Pearson Chi-Square test of independence was carried out to see if there was an association between vaccination attitude and age. The independent variable was age with two levels; 25 years of age or under and 26 years of age or over. The dependent variable was vaccination attitude with two levels; accepting and resistant. It was found that there was no significant association between vaccination attitude and age (χ2 (1) = 0.92, p = .338). Of the participants who were aged 25 or less, 65.5% were accepting of the vaccine while among those aged 26 or older, 56% were accepting of the vaccine.
A second Pearson Chi-Square test of independence was carried out to determine if there was an association between vaccination attitude and sex. The independent variable was sex with three levels; female, male and undisclosed. The dependent variable was vaccination attitude with two levels; accepting and resistant. There was no significant association found between vaccination attitude and sex (χ2 (2) = 1.48, p = .477). Among male participants, 61.7% were accepting of the vaccine while among female participants 65.5% were accepting of the vaccine. Among those who did not disclose their sex, 100% were accepting of the vaccine.
The main reasons for resistance towards the vaccine are shown in Table 6 . Other reasons given by participants to explain vaccine resistance included allergic reactions to vaccines in general (0.5%), feeling indifferent towards vaccination, e.g. “I'm not against getting it but it wouldn't bother me if I didn't get it either” (0.3%), concerns regarding its rapid production and inadequate testing (0.3%), prioritising the more vulnerable before considering getting the vaccine (1.1%), concerns about blood clot specifically (0.3%) and uncertainty of how to register for the vaccine (0.3%).
Table 6.
Reasons for resistance towards the COVID-19 vaccine according to sex and age in percentages (n = 128).
| Reasons | Frequencies n (%) |
||||
|---|---|---|---|---|---|
| Sex |
Age |
Total | |||
| Male | Female | <25 | 26+ | ||
| I'm concerned of the potential side effects | 25 (30.9) | 86 (30.6) | 104 (30.7) | 7 (28.0) | 111 (30.5) |
| I think COVID-19 vaccine may not be safe | 14 (17.3) | 42 (14.9) | 51 (15.0) | 5 (20.0) | 56 (15.4) |
| I don't think that COVID-19 is dangerous to my health | 12 (14.8) | 22 (7.8) | 31 (9.1) | 3 (12.0) | 34 (9.3) |
| I am against vaccination in general | 0 | 4 (1.4) | 3 (0.9) | 1 (4.0) | 4 (1.1) |
| The best way is to let nature take its course | 6 (7.4) | 14 (5.0) | 19 (5.6) | 1 (4.0) | 20 (5.5) |
| I believe natural or traditional remedies | 3 (3.7) | 5 (1.8) | 6 (1.8) | 2 (8.0) | 8 (2.2) |
| I'm afraid of injections | 1 (1.2) | 17 (6.0) | 18 (5.3) | 0 | 18 (4.9) |
| Religious reasons | 2 (2.5) | 1 (0.4) | 2 (0.6) | 1 (4.0) | 3 (0.8) |
| Other reason | 5 (6.2) | 6 (2.1) | 11 (3.2) | 0 | 11 (3.0) |
A logistic regression was conducted to examine if vaccination attitude could be predicted by sociodemographic characteristics, personal COVID-19 experiences, knowledge of COVID-19 and risk perception. The dichotomous criterion variable was vaccination attitude which were recoded as accepting or resistant. The outcome of interest was vaccination acceptance which was coded as 1 while vaccination resistance was coded as 0. Sociodemographic characteristics were entered into block 1, personal COVID-19 experiences were entered into block 2, knowledge of COVID-19 was entered into block 3 and risk perception was entered into the final block.
Descriptive statistics demonstrated that 64.8% of participants were accepting of the vaccine, indicating that they were very likely to be vaccinated or had already been vaccinated. Correlation statistics for predictor variables were less than 0.7, indicating no multicollinearity in the data (Table 4).
The logistic regression model explained 11% (Nagelkerke R 2) and correctly classified 67% of participants, yet it was not statistically significant (χ2 (19) = 29.14, p = .064). Block 1 (χ2 (7) = 9.95, p = .101), block 2 (χ2 (10) = 15.04, p = .131) and block 4 (χ2 (1) = 0.01, p = .921) were also not statistically significant. Block 3, knowledge of COVID-19, was the only statistically significant block (χ2 (1) = 4.14, p = .042), explaining 11% (Nagelkerke R 2) of the variance in vaccination attitude. Results of the regression are presented in Table 7 .
Table 7.
Logistic regression for variables predicting vaccination acceptance (N = 364).
| Block | Variable | β (SE) | Wald | Exp(B) | 95% CI lower | 95% CI upper |
|---|---|---|---|---|---|---|
| 1 | Age | −0.02 (0.03) | 0.40 | 0.98 | 0.93 | 1.04 |
| Female vs. other sex | −0.11 (0.28) | 0.16 | 0.89 | 0.51 | 1.56 | |
| Shared student accommodation vs. living at home | −0.67 (0.32) | 4.35⁎ | 0.51 | 0.27 | 0.96 | |
| Independent student accommodation vs. living at home | −1.21 (0.59) | 4.23⁎ | 0.30 | 0.09 | 0.94 | |
| Other accommodation vs. living at home | 0.45 (1.27) | 0.00 | 1.05 | 0.09 | 12.58 | |
| Private accommodation vs. living at home | −0.13 (0.59) | 0.05 | 0.88 | 0.28 | 2.78 | |
| 2 | Self - COVID-19 positive case | 0.18 (0.42) | 0.18 | 1.20 | 0.52 | 2.74 |
| Family - COVID-19 positive case | 0.28 (0.29) | 0.95 | 1.32 | 0.75 | 2.32 | |
| Friends - COVID-19 positive case | 0.20 (0.31) | 0.44 | 1.22 | 0.67 | 2.23 | |
| Others - COVID-19 positive case | −0.01 (0.31) | 0.00 | 0.99 | 0.53 | 1.83 | |
| No positive case identified | 0.43 (0.43) | 1.00 | 1.54 | 0.66 | 3.56 | |
| Self - close contact of positive case | 0.40 (0.31) | 1.72 | 1.49 | 0.82 | 2.72 | |
| Family - close contact of positive case | −0.69 (0.28) | 5.94⁎ | 0.50 | 0.29 | 0.87 | |
| Friends - close contact of positive case | −0.21 (0.30) | 0.49 | 0.81 | 0.45 | 1.46 | |
| Others - close contact of positive case | 0.17 (0.31) | 0.30 | 1.18 | 0.65 | 2.17 | |
| No close contact | 0.21 (0.38) | 0.29 | 1.23 | 0.58 | 2.62 | |
| 3 | Knowledge of COVID-19 | 0.17 (0.08) | 4.12⁎ | 1.18 | 1.01 | 1.39 |
| 4 | Risk perception | 0.00 (0.01) | 0.01 | 1.00 | 0.98 | 1.02 |
Nagelkerke R2 = 0.11.
p < .05.
Examination of the Wald statistics indicated that living in shared student accommodation compared to living at home (Wald = 4.35, p = .037), living in independent student accommodation compared to living at home (Wald = 4.23, p = .040), having a family member who was a close contact to a positive COVID-19 case (Wald = 5.94, p = .015) and knowledge of COVID-19 (Wald = 4.12, p = .042) significantly added to the model. Living in shared student accommodation (β = −0.67) decreased the likelihood of accepting the vaccine by an odds ratio of 0.51 while living in independent student accommodation (β = −1.21) also decreased the likelihood of being compliant with the vaccine by an odds ratio of 0.30. Having a family member be a close contact of a positive case (β = −0.69) decreased the likelihood of being compliant with the vaccine by an odds ratio of 0.50 while knowledge of COVID-19 (β = 0.17) increased compliance with the vaccine by an odds ratio of 1.18.
3.8. Source of information related to COVID-19
Table 8 outlines the main sources of COVID-related information. The analysis identified social media (53.6%), official sites (45.6%), family and friends (42.3%), and TV channels (63.2%) as being the main sources of information related to COVID-19.
3.9. Risk perception
Four dependent-samples t-tests were conducted to evaluate whether there was a significant difference in personal risk perception and risk perception of others among third-level students (see Supplementary File S1, section 4; questions 1, 4, 5 and 6 covered personal risk perceptions; questions 2, 7, 8 and 9 covered perceived risk for others). A Bonferroni correction was applied to control for multiple comparisons. The alpha level was adjusted to 0.013. There was a significant difference in concerns of participants' own lives versus lives of others (t(363) = −25.58, p < .001), with participants being more concerned for the lives of others (M = 8.93, SD = 2.24) compared with their own lives (M = 5.18, SD = 2.91). There was a significant difference in concerns of infection for the self-compared to others (t(363) = −6.15, p < .001), with participants being more concerned about their loved ones being infected with the virus (M = 6.46, SD = 2.17) than about being infected themselves (M = 5.76, SD = 2.23). There was a significant difference in concerns of death due to COVID-19 (t(363) = −19.82, p < .001), with participants being more worried about the likelihood of their loved ones dying from COVID-19 (M = 5.63, SD = 2.78) than being worried about themselves (M = 2.72, SD = 1.87). There was also a significant difference in participant's perceived likelihood of recovery (t(363) = 13.29, p < .001), with participants perceiving themselves as more likely to recover from COVID-19 (M = 9.28, SD = 1.88) than their loved ones (M = 7.55, SD = 2.10). Age did not account for significant differences in risk perception as can be seen in Table 9 .
Table 9.
Results of t-tests analysing risk perceptions among third-level students (N = 364).
| Comparison | Risk perception items | Age |
Overall |
||||
|---|---|---|---|---|---|---|---|
| −25 |
26+ |
||||||
| M (SD) | t(338) | M (SD) | t(24) | M (SD) | t(363) | ||
| 1 | Concern about own life | 5.12 (2.87) | 6.12 (3.40) | 5.18 (2.91) | |||
| Concern about lives of loved ones | 8.97 (2.18) | −25.52⁎ | 8.40 (2.97) | −4.37⁎ | 8.93 (2.24) | −25.58⁎ | |
| 2 | Perceived likelihood of becoming infected | 5.73 (2.23) | 6.08 (2.29) | 5.76 (2.23) | |||
| Perceived likelihood of loved ones becoming infected | 6.42 (2.19) | −5.67⁎ | 7.04 (1.93) | −3.06⁎⁎ | 6.46 (2.17) | −6.15⁎ | |
| 3 | Perceived likelihood of own death | 2.66 (1.85) | 3.48 (2.02) | 2.72 (1.87) | |||
| Perceived likelihood of death of loved ones | 5.61 (2.76) | −19.12⁎ | 5.96 (3.02) | −5.28⁎ | 5.63 (2.78) | −19.82⁎ | |
| 4 | Perceived likelihood of own recovery | 9.30 (1.89) | 9.04 (1.74) | 9.28 (1.88) | |||
| Perceived likelihood of recovery of loved ones | 7.60 (2.08) | 12.55⁎ | 6.84 (2.27) | 4.55⁎ | 7.55 (2.10) | 13.29⁎ | |
p < .001.
p < .01.
4. Discussion
This study investigated COVID-19 risk perceptions and preventive behaviours of third-level students in Ireland. Overall, the study found that third-level students in Ireland have high levels of COVID-19 related knowledge, high engagement with preventive behaviours, and moderate levels of risk perception.
The study found that age did not influence risk perception levels or engagement in preventive behaviours with third-levels students aged 25 years or less reporting the same levels of risk perception and preventive behaviours as those over the age of 26. As for sex, the study did identify significantly higher levels of risk perception and higher levels of preventive behaviours for females as compared to males. However, the unequal distribution of respondents implies that caution is needed when interpreting these results as there were considerably fewer males than females, and fewer respondents over the age of 26, than under, within the study sample.
The present study confirmed the hypothesis of a positive relationship existing between risk perception and preventive behaviours. It was found that as risk perception increased, so did self-reported preventive behaviours. This is in accordance with previous studies which also suggest that higher risk perception indicates higher preventive behaviours (Alicea-Planas et al., 2021). Also, in accordance with previous research (Rubaltelli et al., 2020; Commodari, 2017), risk perception and preventive behaviours were found to be higher during the period of national restrictions compared to when the restrictions were lifted. Contrary to previous research (Ding et al., 2020; Iorfa et al., 2020), no association between knowledge of COVID-19 and risk perception was found in the current research. While knowledge of COVID-19 was relatively high among the current sample of third-level students, this did not have a significant influence on risk perception levels. However, as the study was conducted one year after the coronavirus outbreak, it may be that more information has been available to the public as compared to previous research, and consequently general knowledge of COVID-19 was high among the participants. Hence, there was little variation in knowledge levels among the current sample which may have led to a low probability of it being associated with risk perception levels.
The study also identified a number of predictors of preventive behaviours among third-level students. Living in shared student accommodation indicated a decrease in preventive behaviours compared to living at home during the academic term. While knowledge of COVID-19 predicted 1% of the variation in preventive behaviours, risk perception was found to be the highest independent predictor of preventive behaviours explaining 8% of the variation.
As regards to vaccination attitude, the study has highlighted the issue of vaccination resistance and hesitancy. Among third-level students, 9.6% were resistant to the vaccine while 25.5% were hesitant about being vaccinated. On the other hand, over two thirds of students were very likely to take the vaccine if offered and almost 2% had already been vaccinated when the study took place. These rates of vaccination resistance are in accordance with previous studies (Murphy et al., 2021). Given the relatively high rates of vaccination resistance and hesitancy, Irish health organisations should explore this issue and target those who are more hesitant and resistant in order to promote vaccination uptake. The high levels of vaccination hesitancy suggest that while third-level students are not completely against the vaccine, there are still some concerns that should be clarified by health organisations. As the main reason for vaccine hesitancy included concerns about the side effects, more information and clarity about the nature of side effects (for example, that they are largely short term) may be helpful to encourage this population to get vaccinated.
Contrary to findings of previous research (Dror et al., 2020; Murphy et al., 2021; Neumann-Böhme et al., 2020), this study found no significant sex differences or age differences in vaccination attitude. Males and females were equally willing to get vaccinated, with rates being 61.7% and 65.5% respectively. This was also true for students less than or over 25 years of age with compliance rates being 65.5% and 56% respectively. However, these findings should be treated with caution as there were unequal numbers of participants in each age and sex groups. The small number of participants aged over 25 and in the male group may have accounted for these findings. Another possible explanation is that individuals may be more willing with time to accept the vaccine as more information has been provided and already thousands of people have been vaccinated with no major side-effects being reported (Government of Ireland, 2021). It should also be noted that one common reason for vaccine hesitancy given by participants was the wish to prioritise the more vulnerable individuals in society before considering receiving the vaccine themselves. This can be explained by the finding that young adults had a greater perception of risk towards others than towards themselves. Third-level students were found to report greater concern for their loved ones compared to themselves in relation to health outcomes due to COVID-19.
The predictive model suggested that living in shared student accommodation or in independent student accommodation as compared to living at home decreased the likelihood of vaccine uptake. Knowledge of COVID-19, on the other hand, increased the likelihood of uptake, highlighting the importance of knowledge as an influence of preventive behaviours. While previous literature indicates a challenge of translating knowledge into behavior (Li et al., 2020), the current study proposes that knowledge can indeed translate into preventive behaviours such as receiving the vaccine.
This research found that TV channels (63.2%) and social media (53.6%) were the main sources of information related to COVID-19, followed by official sites (45.6%) and family and friends (42.3%). The importance of social media as a source of information has been previously highlighted by other studies, suggesting the need for health policy makers to disseminate accurate information via multiple media sources in order to reach the young population. The use of social media also requires attention due to large levels of ‘fake news’ regarding the coronavirus which is present in social media (Apuke & Omar, 2021). Surprisingly, TV channels were identified as the main source, a finding which has not been previously reported, as previous research has indicated that social media tended to be the dominant source of information for third-level students in particular (Khasawneh et al., 2020).
Similar to previous literature (Dunn et al., 2021), while third-level students reported moderate levels of risk perception, they still engage in high levels of preventive behaviours. This may be due to the fact that, while young adults perceive lower risk for themselves personally, they are still concerned about the elderly and the more vulnerable individuals in the society, and therefore engage in preventive behaviours to protect these individuals (Liekefett & Becker, 2020). One must note that many young adults do not have the opportunity to implement the many health recommendations such as remote working or avoiding contact with other people as many work in essential jobs, such as supermarkets, and/or live in shared accommodation, where avoiding personal contact is nearly impossible (Maragakis, 2020).
4.1. Limitations
The present study has a number of limitations; some of which suggest directions for future research. The main limitation of this study is its cross-sectional design which does not allow for cause-and-effect interpretations due to its reliance on correlational analysis. Cross-sectional studies using questionnaire only capture data of one point in time and cannot be used to determine cause-and-effect (Gaube et al., 2019). The use of correlations when investigating risk perception and preventive behaviours have also been suggested to not provide evidence on the meaningfulness or direction of the effect (Gaube et al., 2019). For example, high risk perception may influence higher preventive measures, however, it could also be that high engagement with preventive behaviours heightens an individual's risk perception.
Secondly, the use of online survey is also considered a limitation as participation is voluntary and respondents with biases or a particular interest in the research topic may self-select for participation, and this can potentially influence the study sample (Andrade, 2020). The use of online surveys may suggest that those who adhere with the recommendations are more willing to participate in such studies. Brewer et al. (2007) also highlight that the main limitation of using surveys to explore risk perception is that it underestimates what individuals who already plan on acting to minimise their risk would consider their risk to be without action. For example, an individual who already anticipates getting vaccinated against an illness may perceive themselves to be less likely to get the illness compared to if they did not anticipate getting the vaccine at all. For this reason, it is suggested that prospective designs and experiments manipulating risk perception are the ideal for assessing risk perception (Brewer et al., 2007). Moreover, although the questionnaires were pilot tested prior to distribution, these were not validated due to time constraints and due to COVID-19 being a recent topic requiring rapid investigation. The relatively small sample size may have been a limitation in the current study. However, due to the glut of survey research focusing on COVID-19, it was not possible to recruit more participants within the study timeframe.
Thirdly, social desirability bias may have occurred within the study as the measures were all self-reported. For example, high levels of preventive behaviours were reported by the participants, however, previous research suggest that young adults are more likely to conceal their actual COVID-19 behaviours and report inaccurate preventive measures because of shame or stigmatisation (O'Connor & Evans, 2020). Finally, the sample was relatively homogenous, particularly in terms of age, sex, nationality and university, limiting the generalizability of the results. This homogeneity also limited the ability to make valid comparisons, for example, when testing the hypothesis that those of different sex and age groups differ in risk perception levels and engagement in preventive behaviours.
4.2. Implications and conclusion
Despite these limitations, the current study presents a valuable contribution to the understanding of third-level students' response to COVID-19 in Ireland. As the study was carried out in the early months of 2021, it allowed for an indication of how young adults are responding a year since the start of the pandemic, and if preventive behaviours have been maintained compared to reports from the start of the pandemic. Given that risk perception has been found to be significantly associated with preventive behaviours, and features as an important predictor of preventive behaviours, risk perception should be addressed during health campaigns. Further research should be conducted addressing the limitations of risk perception measurement mentioned above. A variety of sociodemographic and psychological factors have been identified as influencing one's risk perception, both in the current study and previous literature. Having a better understanding of the factors contributing to risk perception and preventive behaviours allows for health policy makers to better plan educational campaigns and consequently influence positive precautionary behaviours among the population. Health policy makers and the media, therefore, should acknowledge that certain educational campaigns can be adequate for some particular groups but not for others, suggesting a need for a variety of campaigns.
Moreover, although information on COVID-19 and recommendations change according to the progress of the virus, it is crucial that health advisors be open and honest and provide the population with specific and evidence-based information. Public health advisors should also ensure young people are properly informed as youth have previously suggested gaps in public health communications which have led to common misunderstandings. This was confirmed by the current study, as one participant for example, claimed to be uncertain of how to apply for a COVID-19 vaccine due to lack of information while the majority were concerned about the potential side effects. Misinformation and lack of accurate information regarding the safety of the vaccine may potentially hinder vaccination effectiveness if not promptly and properly addressed.
CRediT authorship contribution statement
Joyce Borges: Conceptualization, Methodology, Formal analysis, Investigation, Data Curation, Writing - Original Draft, Visualization, Project administration.
Molly Byrne: Conceptualization, Writing - Review & Editing, Supervision, Project administration.
Declaration of competing interest
None.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.actpsy.2022.103535.
Appendix A. Supplementary data
Supplementary material
References
- Alicea-Planas J., Trudeau J.M., Vásquez Mazariegos W.F. COVID-19 risk perceptions and social distancing practice in Latin America. Hispanic Health Care International. 2021;1540415320985141 doi: 10.1177/1540415320985141. [DOI] [PubMed] [Google Scholar]
- Andrade C. The limitations of online surveys. Indian Journal of Psychological Medicine. 2020;42(6):575–576. doi: 10.1177/0253717620957496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Apuke O.D., Omar B. Fake news and COVID-19: Modelling the predictors of fake news sharing among social media users. Telematics and Informatics. 2021;56 doi: 10.1016/j.tele.2020.101475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barello S., Nania T., Dellafiore F., Graffigna G., Caruso R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. European Journal of Epidemiology. 2020;35:781–783. doi: 10.1007/s10654-020-00670-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewer N.T., Chapman G.B., Gibbons F.X., Gerrard M., McCaul K.D., Weinstein N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychology. 2007;26(2):136–145. doi: 10.1037/0278-6133.26.2.136. [DOI] [PubMed] [Google Scholar]
- Brewer N.T., Weinstein N.D., Cuite C.L., Herrington J.E. Risk perceptions and their relation to risk behavior. Annals of Behavioral Medicine. 2004;27:125–130. doi: 10.1207/s15324796abm2702_7. [DOI] [PubMed] [Google Scholar]
- Bwire G.M. Coronavirus: Why men are more vulnerable to Covid-19 than women? SN Comprehensive Clinical Medicine. 2020;2:874–876. doi: 10.1007/s42399-020-00341-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capone V., Caso D., Donizzetti A.R., Procentese F. University student mental well-being during COVID-19 outbreak: What are the relationships between information seeking, perceived risk and personal resources related to the academic context? Sustainability. 2020;12(17):7039. doi: 10.3390/su12177039. [DOI] [Google Scholar]
- Citizens Information Moving to Ireland for third-level education. 2020. https://www.citizensinformation.ie/en/moving_country/moving_to_ireland/studying_in_ireland/third_level_education.html
- Citizens Information COVID-19 restrictions in Ireland. 2021. https://www.citizensinformation.ie/en/covid19/living_with_covid19_plan.html#
- Cohn L.D., Macfarlane S., Yanez C., Imai W.K. Risk-perception: Differences between adolescents and adults. Health Psychology. 1995;14(3):217–222. doi: 10.1037/0278-6133.14.3.217. [DOI] [PubMed] [Google Scholar]
- Commodari E. The role of sociodemographic and psychological variables on risk perception of the flu. SAGE Open. 2017;7(3):1–10. doi: 10.1177/2158244017718890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cori L., Bianchi F., Cadum E., Anthonj C. Risk perception and COVID-19. International Journal of Environmental Research and Public Health. 2020;17(9):3114. doi: 10.3390/ijerph17093114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darker C. In: Encyclopedia of behavioral medicine. Gellman M.D., Turner J.R., editors. Springer; 2013. Risk perception; p. 110. [DOI] [Google Scholar]
- De Bruin W.B., Bennett D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: A national survey. American Journal of Preventive Medicine. 2020;59(2):157–167. doi: 10.1016/j.amepre.2020.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dehingia N., Raj A. Sex differences in COVID-19 case fatality: Do we know enough? The Lancet Global Health. 2021;9(1):e14–e15. doi: 10.1016/S2214-109X(20)30464-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department of Health . Government of Ireland; 2021. Latest updates on COVID-19 (Coronavirus)https://www.gov.ie/en/news/7e0924-latest-updates-on-covid-19-coronavirus/# [Google Scholar]
- Department of Health Amárach public opinion survey – 21 June 2021. Government of Ireland. 2021. https://www.gov.ie/en/collection/6b4401-view-the-amarach-public-opinion-survey/
- Ding Y., Du X., Li Q., Zhang M., Zhang Q., Tan X., Liu Q. Risk perception of coronavirus disease 2019 (COVID-19) and its related factors among college students in China during quarantine. PloS One. 2020;15(8) doi: 10.1371/journal.pone.0237626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dror A.A., Eisenbach N., Taiber S., Morozov N.G., Mizrachi M., Zigron A., Srouji S., Sela E. Vaccine hesitancy: The next challenge in the fight against COVID-19. European Journal of Epidemiology. 2020;35:775–779. doi: 10.1007/s10654-020-00671-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn M.R., DeJonckheere M., Schuiteman S., Strome A., Herbert K., Waselewski M., Chang T. “Stay home so this can be over:” A national study of youth perspectives on social distancing during the COVID-19 pandemic. Preventive Medicine Reports. 2021;22 doi: 10.1016/j.pmedr.2021.101355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferrer R., Klein W.M. Risk perceptions and health behavior. Current Opinion in Psychology. 2015;5:85–89. doi: 10.1016/j.copsyc.2015.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finset A., Bosworth H., Butow P., Gulbrandsen P., Hulsman R.L., Pieterse A.H., Street R., Tschoetschel R., van Weert J. Effective health communication - a key factor in fighting the COVID-19 pandemic. Patient Education and Counseling. 2020;103(5):873–876. doi: 10.1016/j.pec.2020.03.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franzen A., Wöhner F. Coronavirus risk perception and compliance with social distancing measures in a sample of young adults: Evidence from Switzerland. PLoS One. 2021;16(2) doi: 10.1371/journal.pone.0247447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galasso V., Pons V., Profeta P., Becher M., Brouard S., Foucault M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proceedings of the National Academy of Sciences. 2020;117(44):27285–27291. doi: 10.1073/pnas.2012520117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaube S., Lermer E., Fischer P. In: Perceived safety. Raue M., Streicher B., Lermer E., editors. Springer; Cham: 2019. The concept of risk perception in health-related behavior theory and behavior change; pp. 101–118. [DOI] [Google Scholar]
- Government of Ireland Vaccinations. 2021. https://covid-19.geohive.ie/pages/vaccinations
- Graffigna G., Palamenghi L., Boccia S., Barello S. Relationship between citizens’ health engagement and intention to take the COVID-19 vaccine in Italy: A mediation analysis. Vaccines. 2020;8(4):576. doi: 10.3390/vaccines8040576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health at a Glance . OECDiLibrary; 2020. Chapter 1. How resilient have European health systems been to the COVID-19 crisis? [DOI] [Google Scholar]
- Health Protection Surveillance Centre COVID-19 14-day epidemiology reports- June 2021. 2021. https://www.hpsc.ie/a-z/respiratory/coronavirus/novelcoronavirus/surveillance/covid-1914-dayepidemiologyreports/
- Iorfa S.K., Ottu I.F., Oguntayo R., Ayandele O., Kolawole S.O., Gandi J.C., Dangiwa A.L., Olapegba P.O. COVID-19 knowledge, risk perception, and precautionary behavior among Nigerians: A moderated mediation approach. Frontiers in Psychology. 2020;11 doi: 10.3389/fpsyg.2020.566773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jin J.M., Bai P., He W., Wu F., Liu X.F., Han D.M., Liu S., Yang J.K. Gender differences in patients with COVID-19: Focus on severity and mortality. Frontiers in Public Health. 2020;8:152. doi: 10.3389/fpubh.2020.00152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khasawneh A.I., Humeidan A.A., Alsulaiman J.W., Bloukh S., Ramadan M., Al-Shatanawi T.N., Awad H.H., Hijazi W.Y., Al-Kammash K.R., Obeidat N., Saleh T., Kheirallah K.A. Medical students and COVID-19: Knowledge, attitudes, and precautionary measures. A descriptive study from Jordan. Frontiers. Public Health. 2020;8:253. doi: 10.3389/fpubh.2020.00253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Y., Park I., Kang S. Age and gender differences in health risk perception. Central European Journal of Public Health. 2018;26(1):54–59. doi: 10.21101/cejph.a4920. [DOI] [PubMed] [Google Scholar]
- Kwak S.G., Kim J.H. Central limit theorem: The cornerstone of modern statistics. Korean Journal of Anesthesiology. 2017;70(2):144–156. doi: 10.4097/kjae.2017.70.2.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanciano T., Graziano G., Curci A., Costadura S., Monaco A. Risk perceptions and psychological effects during the Italian COVID-19 emergency. Frontiers in Psychology. 2020;11 doi: 10.3389/fpsyg.2020.580053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li J.B., Yang A., Dou K., Wang L.X., Zhang M.C., Lin X.Q. Chinese public’s knowledge, perceived severity, and perceived controllability of COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. BMC Public Health. 2020;20:1–14. doi: 10.1186/s12889-020-09695-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liekefett L., Becker J. Compliance with governmental restrictions during the coronavirus pandemic: A matter of personal self-protection or solidarity with people in risk groups? British Journal of Social Psychology. 2020 doi: 10.1111/bjso.12439. [DOI] [PubMed] [Google Scholar]
- Maragakis L.L. John Hopkins Medicine; 2020. Coronavirus and COVID-19: Younger adults are at risk, too.https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-and-covid-19-younger-adults-are-at-risk-too [Google Scholar]
- McErlean A.R., Fekete E.M. Health-related social control and risk perceptions in emerging adults. Emerging Adulthood. 2018;6(3):206–212. doi: 10.1177/2167696817729577. [DOI] [Google Scholar]
- Murphy J., Vallières F., Bentall R.P., Shevlin M., McBride O., Hartman T.K., McKay R., Bennett K., Mason L., Gibson-Miller J., Levita L., Martinez A.P., Stocks T.V., Karatzias T., Hyland P. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. NatureCommunications. 2021;12(29) doi: 10.1038/s41467-020-20226-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neumann-Böhme S., Varghese N.E., Sabat I., Barros P.P., Brouwer W., van Exel J., Schreyögg J., Stargardt T. Once we have it, will we use it? A european survey on willingness to be vaccinated against COVID-19. The European Journal of Health Economics. 2020;21:977–982. doi: 10.1007/s10198-020-01208-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nguyen T., Henningsen K.H., Brehaut J.C., Hoe E., Wilson K. Acceptance of a pandemic influenza vaccine: A systematic review of surveys of the general public. Infection and Drug Resistance. 2011;4:197–207. doi: 10.2147/IDR.S23174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor A.M., Evans A.D. Dishonesty during a pandemic: The concealment of COVID-19 information. Journal of Health Psychology. 2020 doi: 10.1177/1359105320951603. 1359105320951603. [DOI] [PubMed] [Google Scholar]
- Oosterhoff B., Palmer C.A., Wilson J., Shook N. Adolescents' motivations to engage in social distancing during the COVID-19 pandemic: Associations with mental and social health. Journal of Adolescent Health. 2020;67(2):179–185. doi: 10.1016/j.jadohealth.2020.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orenstein W.A., Ahmed R. Simply put: Vaccination saves lives. Proceedings of the National Academy of Sciences of the United States of America. 2017;114(16):4031–4033. doi: 10.1073/pnas.1704507114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pallant J. 7th ed. Taylor & Francis Group; 2020. SPSS survival manual: A step by step guide to data analysis using IBM SPSS. [Google Scholar]
- Reniers R.L., Murphy L., Lin A., Bartolomé S.P., Wood S.J. Risk perception and risk-taking behaviour during adolescence: The influence of personality and gender. PLoS One. 2016;11(4) doi: 10.1371/journal.pone.0153842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenstock I.M. The health belief model and preventive health behavior. Health Education Monographs. 1974;2(4):354–386. doi: 10.1177/109019817400200405. [DOI] [PubMed] [Google Scholar]
- Rubaltelli E., Tedaldi E., Orabona N., Scrimin S. Environmental and psychological variables influencing reactions to the COVID-19 outbreak. British Journal of Health Psychology. 2020;25(4):1020–1038. doi: 10.1111/bjhp.12473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sadique M.Z., Edmunds W.J., Smith R.D., Meerding W.J., de Zwart O., Brug J., Beutels P. Precautionary behavior in response to perceived threat of pandemic influenza. Emerging Infectious Diseases. 2007;13(9):1307–1313. doi: 10.3201/eid1309.070372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarzer R. In: Self-efficacy: Thought control of action. Schwarzer R., editor. Taylor & Francis Group; 1992. Self-efficacy in the adoption and maintenance of health behaviors: Theoretical approaches and a new model; pp. 217–244. [DOI] [Google Scholar]
- Soares P., Rocha J.V., Moniz M., Gama A., Laires P.A., Pedro A.R., Dias S., Leite A., Nunes C. Factors associated with COVID-19 vaccine hesitancy. Vaccines. 2021;9(3):300. doi: 10.3390/vaccines9030300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L. A social neuroscience perspective on adolescent risk-taking. Developmental Review. 2008;28(1):78–106. doi: 10.1016/j.dr.2007.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taghrir M.H., Borazjani R., Shiraly R. COVID-19 and iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Archives of Iranian Medicine. 2020;23(4):249–254. doi: 10.34172/aim.2020.06. [DOI] [PubMed] [Google Scholar]
- World Health Organization WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. 2020. https://www.who.int/director-general/speeches/detail/who-dire
- World Health Organization Coronavirus. 2021. https://www.who.int/health-topics/coronavirus#tab=tab_1
- Yuan T., Liu H., Li X.D., Liu H.R. Factors affecting infection control behaviors to prevent COVID-19: An online survey of nursing students in Anhui, China in March and April 2020. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research. 2020;26 doi: 10.12659/MSM.925877. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material