

Two distinct trajectories of dyspareunia were identified from pregnancy to 24 months postpartum; pain catastrophizing predicted inclusion in the moderate relative to minimal pain trajectory.
OBJECTIVE:
To identify distinct trajectories of dyspareunia in primiparous women and examine biopsychosocial risk factors of these trajectories.
METHODS:
This was a prospective cohort of 582 first-time mothers. Participants completed validated measures of dyspareunia at 20–24 (baseline) and 32–36 weeks of gestation and at 3, 6, 12, and 24 months postpartum. Risk factors were assessed at baseline and 3 months postpartum, with labor and delivery characteristics collected by medical record review. Latent class growth analysis was conducted to identify homogeneous subgroups with distinct trajectories of dyspareunia. Univariable and multivariable binomial logistic regressions examined whether predictors were associated with these trajectories.
RESULTS:
Overall, the prevalence of dyspareunia ranged from 31.4% at 3 months postpartum to 11.9% at 24 months. We identified two distinct classes of dyspareunia with 21% of women in the class with moderate dyspareunia and 79% in the class with minimal dyspareunia, with pain decreasing in both groups until 12 months postpartum and little change thereafter. Biomedical factors—prior chronic pain (including preexisting dyspareunia), labor epidural analgesia, induction, episiotomy, perineal laceration, mode of delivery, breastfeeding, and whether the woman had a new pregnancy during the postpartum period—did not significantly predict dyspareunia class. Greater fatigue (odds ratio [OR] 1.30; 95% CI 1.05–1.60) and depressive symptoms (OR 1.08; 95% CI 1.02–1.14) in pregnancy and fatigue (OR 1.27; 95% CI 1.04–1.56) and pain catastrophizing (OR 1.10; 95% CI 1.05–1.16) at 3 months postpartum increased the odds for the moderate relative to the minimal pain trajectory in univariable models. In a multivariable model, pain catastrophizing at 3 months postpartum (OR 1.09; 95% CI 1.04–1.15) was associated with the moderate relative to the minimal pain trajectory.
CONCLUSION:
We identified two distinct trajectories of dyspareunia across pregnancy and postpartum. One in five nulliparous women experienced moderate dyspareunia. Pain catastrophizing at 3 months postpartum was associated with experiencing moderate relative to minimal levels of dyspareunia.
Dyspareunia—pain during vaginal intercourse—is common in both pregnancy (10–62% in the first trimester, 13–44% in the second, and 17–69% in the third) and postpartum (12–62% at 3 months, 17–45% at 6 months, and 8–32% at 12–18 months).1–6 Pain negatively affects women's relationships, mental and physical health, and overall well-being,1 yet it remains underdiagnosed and untreated. The average trajectory of postpartum dyspareunia appears to decline over time, but the pain persists for a significant proportion of women.1 The wide variability in prevalence estimates may be explained by heterogeneity in trajectories of dyspareunia (ie, patterns of change over time), which have not yet been established.
Prior studies examining predictors of dyspareunia in pregnancy and postpartum have primarily been retrospective, are limited by small sample sizes and lack of long-term follow-up. Many studies have also focused on the average trajectory, which assumes that change is homogenous, and have not examined predictors of unique pain trajectories.1 Examining distinct trajectories may identify key points for earlier interventions. Prior studies have also emphasized biomedical predictors and neglected psychosocial factors, despite evidence that the latter—including depressive symptoms, fatigue, pain catastrophizing, and sexual goals (ie, motives for having sex)—are more consequential for predicting dyspareunia and postpartum sexual function.7–10 Given that only 15% of women with postpartum sexual dysfunction discuss it with their health care professional,11 enhanced knowledge of the trajectories and predictors of dyspareunia may assist clinicians in recognizing and treating this condition.
We sought to establish distinct trajectories of dyspareunia among primiparous women from mid-pregnancy to 24 months postpartum and to examine biopsychosocial predictors of the different dyspareunia trajectories.
METHODS
This study was a prospective cohort study conducted with first-time mothers recruited between 18 and 22 weeks of gestation (mean 21 weeks; range 18 to 25, SD=1.18) from the IWK Health Centre diagnostic imaging unit in Halifax, Nova Scotia, Canada, a mid-sized urban city, from August 2015 to August 2017. Research staff identified potential participants before their 20-week ultrasonogram appointment, and then on the day of their appointment, met with them to screen for eligibility and obtain informed written consent. The inclusion criteria were: 1) 18 years of age or older; 2) primiparous; 3) uncomplicated, singleton pregnancy; 4) planned delivery at the IWK Health Centre or consent for collection of birth information from the medical record if delivering elsewhere; 5) fluent in English; and 6) access to a personal email account and internet for completing surveys. Women with self-reported medical or psychiatric illnesses were eligible for inclusion if women reported the illnesses to be well-controlled.
All study variables with the exception of labor and delivery characteristics were assessed by self-report surveys completed online via an emailed link using Qualtrics Research Suite survey software. The study was preregistered on the Open Science Framework; measures can be found on the Open Science Framework page at https://osf.io/m8zyd/?view_only=8bf96eb8270f4e00a151ea8baa5b4747. Surveys were sent at six timepoints: 20–24 weeks of gestation (baseline); 32–36 weeks of gestation; and 3, 6, 12, and 24 months postpartum. The survey links expired after 4 weeks, and email and phone reminders were sent to promote participation. Participants received gift certificates to Amazon.ca ($5 for the baseline and 32-week surveys; $10 for each of the postpartum surveys). The study was approved by the ethical review board at the IWK Health Centre.
Dyspareunia was assessed at all timepoints using a visual analog scale, which evaluated average pain intensity during intercourse in the previous 4 weeks on a continuous scale from 0 (no pain at all) to 10 (worst pain ever). The visual analog scale is recommended by IMMPACT (Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials)12 and was previously adapted for dyspareunia.13 Clinically significant pain (moderate or severe) is reflected by a pain rating of 4 or greater.14 Only women who reported engaging in intercourse in the preceding 4 weeks completed this measure.
We used time-invariant predictors because these factors can be assessed at relevant timepoints and are therefore of greater clinical utility for identifying risk factors for persistent dyspareunia. For biomedical factors, previously diagnosed chronic pain conditions (eg, fibromyalgia, migraine headaches, dyspareunia) were assessed with a single self-report item at baseline and dichotomized as yes or no. Biomedical factors related to labor and delivery, including use of epidural analgesia, induction of labor, episiotomy, and degree of perineal laceration (0 [no] to 4 [fourth-degree laceration]), were collected by a research assistant via medical record review. For women who did not deliver at the IWK Health Centre (n=23), this information was obtained with permission from their outside medical records or a brief survey at 2 weeks postpartum. Mode of delivery was dummy coded as vaginal compared with instrumental and cesarean, instrumental compared with vaginal and cesarean, and cesarean compared with vaginal and instrumental. Breastfeeding status was assessed at all timepoints and was highly correlated (r=.43 and .80 for all). Breastfeeding at 3 months postpartum was associated with the highest proportion (92.6%) of women breastfeeding and was used to test for effects with dyspareunia. Finally, whether the participant became pregnant again during the study period was assessed at each postpartum timepoint.
The psychological and social variables were evaluated at both baseline and 3 months postpartum. Fatigue was assessed by participants reporting their average daily energy level on a scale ranging from 1 (high energy) to 7 (extreme fatigue).15 Depressive symptoms were assessed with the 10-item Edinburgh Postnatal Depression Scale, validated for use in pregnancy and postpartum.16,17 Participants answered each item on a scale of 0 to 3, with total scores ranging from 0 to 30 and higher scores indicative of greater depressive symptoms. This measure showed strong internal consistency in our sample (Cronbach's α=.84 and .86). Pain catastrophizing was assessed with the validated Pain Catastrophizing Scale,18 which includes 13 items measuring exaggerated negative thoughts and feelings about pain. Responses to each item range from 0 (not at all) to 4 (all the time), with a total score from 0 to 52 and higher scores reflecting greater catastrophizing. Internal consistency was strong (Cronbach's α=.94 and .91). Finally, approach and avoidance sexual goals were assessed with a 15-item measure adapted from Cooper et al19 and used previously in dyspareunia research.9 Participants rated the importance of nine approach (eg, to promote intimacy) and six avoidance (eg, to avoid disappointing a partner) goals in influencing their decision to engage in sex with a partner on a scale from 1 (not at all important) to 7 (extremely important). Higher scores indicate higher endorsement of the goals. This measure was completed only by women who reported sexual activity in the previous 4 weeks. Cronbach's α was 0.79 and 0.89 for approach goals and 0.89 and 0.89 for avoidance goals. For measures requiring calculation of a total score, maximum likelihood imputation for item-level data missing at random was used, provided that the missing data were less than 20% of the total number of items in a given measure.20
Descriptive statistics were calculated with SPSS 25.0, and all other analyses were estimated with Mplus 8.2. We used Latent Class Growth Analysis to identify unique trajectories (ie, patterns of change) of dyspareunia from pregnancy to 24 months postpartum. Latent Class Growth Analysis is a statistical method that can be used to describe “hidden groups” within a population where there are suspected differences in how individuals within the population change over time.21 Essentially, it is a statistical model that groups similar people together based on their responses. We used a freely estimated model, meaning that we did not force the trajectories to follow a specific shape (eg, linear, quadratic). This approach allowed for the shape of the trajectories to differ across the latent classes. We constrained the variance to 0 and allowed them to vary only across classes.21 There is no established method for calculating the required sample size for the current analysis.22 Nylund et al23 recommended a sample size of 500 as sufficient for detecting the correct number of latent classes using adjusted fit statistics.
To determine the optimal number of classes, we followed an iterative procedure. We first ran a single class model, followed by two-, three-, four-, five-, and six-class solutions. The best-fitting classification model was determined by a combination of model fit indices: parsimony, size of classes (at least 5% of the total sample),24 and interpretability of the trajectories.23 Lower Akaike Information Criterion, lower Bayesian information criteria (BIC) value, and lower sample-size–adjusted BIC indicate better fit. Significant Lo-Mendell-Rubin likelihood ratio test and significant bootstrap likelihood ratio both test the significance of the improvement in the model when an additional class is extracted.23 Entropy values indicate how accurately the model distinguishes between the classes; these values range between 0 and 1, with values closer to 1 indicating better fit and greater precision of the individual classes. Missing data for dyspareunia in the Latent Class Growth Analysis were treated using the full information maximum likelihood function. Once the best fitting model was selected, it was re-run with 2,000 random start values to ensure it replicated without issue.
Once the best fitting model was selected, the three-step method recommended by Asparouhov and Muthén25 was used to investigate predictors of class membership. First, we performed univariable binomial logistic analyses for each of the predictors individually to examine their unique effects. We applied the Benjamini-Hochberg correction to all significance tests to control for the false discovery rate.26 The critical P-values were P=.02 for χ2 tests of proportions and independent samples median tests and P=.03 for the univariate analyses. Significant predictors from the univariate analyses were then included in a multivariate analysis. There were no issues with multicollinearity between any of our predictors (r<.63 for all). To retain the same sample size for the logistic analyses, multiple imputation was used to replace missing values of predictors only. Each missing value was imputed 10 times and the average result was used in the final analyses.
RESULTS
A total of 649 women were recruited. Forty-three women were excluded because they did not complete the baseline survey and 24 were excluded because they did not report a valid dyspareunia score at any timepoint, leaving a final sample size of 582 (Fig. 1). Women were, on average, 29 years old at the time of recruitment (range 18–45 years, SD=4.4). Most identified as heterosexual (n=539, 92.8%), were married or living with their partner (n=575, 98.8%), and reported a median relationship duration of 69.5 months (range five to 256). The majority were Canadian (n=525, 90.2%), well-educated (ie, completed a university degree(s); n=380, 65.4%), and had an annual household income of more than $60,000 (n=443, 76.6%). The number of women who reported having engaged in sexual activity in the preceding 4 weeks was 575 (99%) at baseline, 486 (83.5%) at 32 weeks of gestation, 430 (73.9%) at 3 months postpartum, 439 (75.4%) at 6 months postpartum, 432 (74.2%) at 12 months postpartum, and 405 (69.6%) at 24 months postpartum. There were no significant differences in sociodemographics between our sample of 582 women and the 24 women who were excluded. Sociodemographic information is presented in Table 1 and for all study variables in Table 2.
Fig. 1. Participant flow and response rates. *Not fluent in English, delivering outside of province, medical illness not well managed.
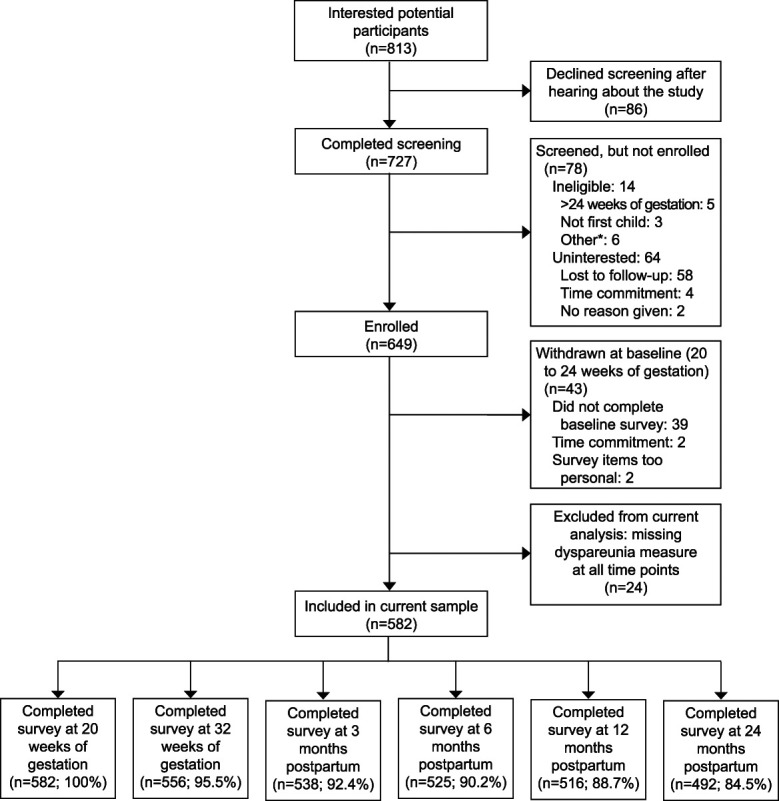
Rosen. Trajectories of Dyspareunia. Obstet Gynecol 2022 .
Table 1.
Sociodemographics of the Study Population (N=582)
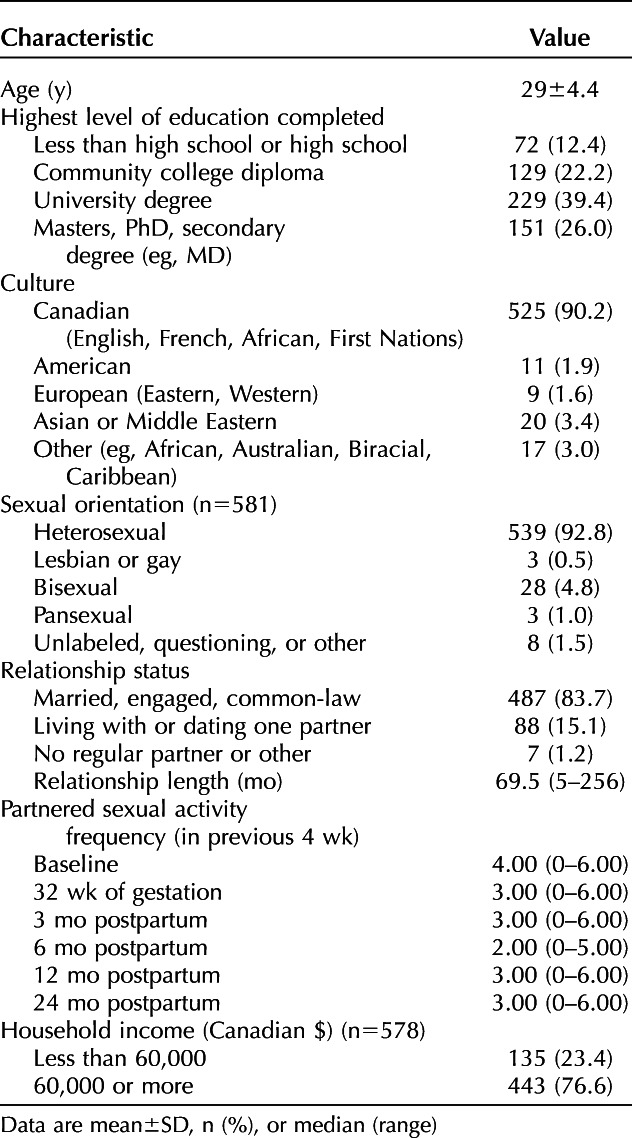
Table 2.
Measures of Primary Pain Outcome and Predictors of Dyspareunia Trajectory*

Examination of a single trajectory for the average change in dyspareunia across the full cohort revealed that the dyspareunia intercept (ie, estimated initial status at baseline, 20–24 weeks of gestation) was 1.80 (SE=0.09, P<.001), with an average decline in pain from baseline to 24 months postpartum of −0.427 (SE=0.29, P<.001). The median ratings of dyspareunia for the full cohort across timepoints are reported in Table 2. We observed significant heterogeneity in dyspareunia (see Supplemental Table 1 on the Open Science Framework page at https://osf.io/m8zyd/?view_only=8bf96eb8270f4e00a151ea8baa5b4747) for model fit indices for the six estimated Latent Class Growth Analyses. Fit indices indicated that the two-class and three-class solutions both fit the data; however, evaluation of all the indices together suggested that the two-class model was the best fitting model. In particular, the two-class solution had higher entropy (0.79), indicating more distinct separation of the classes relative to the three-class solution (0.73). The two-class solution also had a sufficient number of participants in each class and the trajectories were interpretable. Given that we allowed the means, SDs, and slope loadings to be freely estimated, we first report whether there was significant overall change in dyspareunia from baseline to 24 months postpartum, and then we describe the shape of change over time (Fig. 2).
Fig. 2. Trajectories of dyspareunia from 20 weeks of gestation to 24 months postpartum.
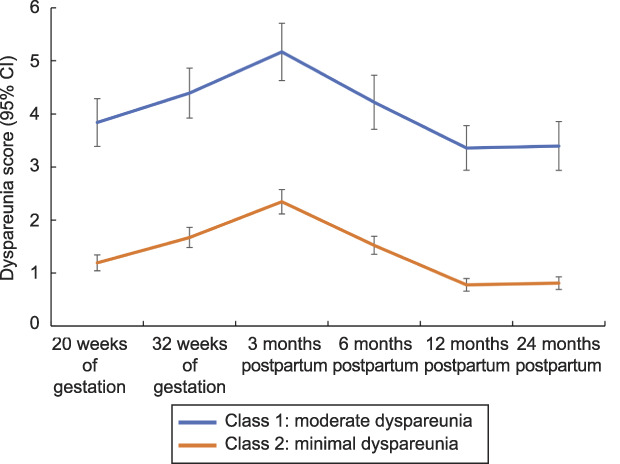
Rosen. Trajectories of Dyspareunia. Obstet Gynecol 2022.
The two-class solution resulted in dyspareunia trajectories of minimal and moderate pain. In both trajectories, pain increased from mid-pregnancy to 3 months postpartum, decreased between 3 and 12 months postpartum, and appeared relatively stable between 12 and 24 months postpartum. The moderate dyspareunia class included 21% (n=125) of the women in the cohort. In this trajectory, the dyspareunia intercept was 3.84 (SE=0.30, P<.001) with a significant overall decline of −0.442 (SE=0.15, P=.004) from baseline to 24 months postpartum. In this class, median scores for dyspareunia exceeded four (eg, clinically significant pain) at 32 weeks of gestation, and at 3, 6, and 12 months postpartum (Table 2). The minimal dyspareunia class included 79% (n=457) of women in the cohort. In this class, the dyspareunia intercept was 1.19 (SE=0.12, P<.001) with a significant overall decline of −0.382 (SE=0.12, P=.002). The median pain rating in this class did not exceed four at any of the timepoints.
Odds ratios for the biopsychosocial factors in the univariable and multivariable logistic regression models are reported in Table 3. The biomedical factors—prior chronic pain condition, labor epidural analgesia, induction, episiotomy, perineal laceration, mode of delivery, breastfeeding, and second pregnancy—did not significantly predict dyspareunia trajectory at the univariable level. Reporting greater fatigue and depressive symptoms in pregnancy, and greater fatigue and pain catastrophizing at 3 months postpartum, increased the odds of being classified in the moderate pain relative to the minimal pain trajectory. Depression at 3 months postpartum and pain catastrophizing in pregnancy did not predict pain trajectory at the univariable level. Approach and avoidance sexual goals assessed in pregnancy and at 3 months postpartum similarly did not predict pain trajectory at the univariable level. When all significant psychological variables were examined together in a multivariable model and regressed simultaneously onto latent class membership, one predictor—pain catastrophizing at 3 months postpartum—was associated with inclusion in the moderate pain relative to the minimal pain trajectory.
Table 3.
Multivariate Modeling of Biopsychosocial Predictors of Dyspareunia Trajectory

DISCUSSION
In this prospective cohort of primiparous women, we found two distinct trajectories of dyspareunia from mid-pregnancy to 24 months postpartum: 21% of women were in the class with moderate dyspareunia and 79% were in the class with minimal dyspareunia. In both classes, pain increased from mid-pregnancy to 3 months postpartum, decreased between 3 and 12 months postpartum, and then was relatively stable to 24 months postpartum. The prevalence of moderate problems with dyspareunia in pregnancy and after childbirth in our study is consistent with prior studies.3,5,11,27,28 Between 45.0% and 67.9% of women in the moderate dyspareunia class reported clinically significant pain across the study period.1 No significant improvements in dyspareunia were observed after 12 months postpartum, which is indicative of pain stabilization. Ideally, self-reported pain with intercourse should be addressed by early assessment and evidence-based interventions. Although such interventions exist for various causes of dyspareunia,29 including cognitive behavioral therapy, pelvic floor physical therapy, and topical lidocaine, their efficacy in the context of the postpartum period remains unknown.
Prior research typically has found instrumental deliveries and a history of chronic pain conditions to predict more severe and persistent postpartum dyspareunia; findings for other biomedical predictors, including breastfeeding, perineal trauma, episiotomy, and mode of delivery, have been equivocal.1,5,30 None of these factors predicted dyspareunia class in the current study. Alligood et al,5 found that breastfeeding at 6 months postpartum was the strongest risk factor for dyspareunia. The current results are an important addition to the literature because prior studies, including Alligood et al,5 have not examined the associations between biomedical factors and unique trajectories of dyspareunia or the degree of change over time. The fact that biomedical factors, which are largely nonmodifiable or less modifiable, did not predict dyspareunia class may be reassuring to first-time mothers. Findings underscore the importance of a biopsychosocial approach to assessment and treatment of dyspareunia in pregnancy and postpartum,31,32 especially in light of evidence that psychosocial factors are robust predictors of dyspareunia5,33 and are amenable to intervention.
Pain catastrophizing—one of the most robust psychological predictors of persistent pain34—at 3 months postpartum emerged as the only significant predictor of a moderate pain trajectory in multivariate modeling. In line with the fear-avoidance model of chronic pain34 and studies of dyspareunia outside of pregnancy and postpartum,10,35 catastrophizing leads to greater fear of pain, anxiety, hypervigilance, and avoidance of painful activities. These responses exacerbate the interpretation of pain as threatening and positively reinforce the fear-avoidance cycle, contributing to greater pain. Screening for pain catastrophizing at 3 months postpartum when sexual activity has resumed for most new parents,28 may assist clinicians in identifying who is at risk for more severe and persistent dyspareunia and should be monitored more closely to avoid the detrimental consequences of untreated pain.1
Strengths of our study include the recruitment of a nulliparous cohort in mid-pregnancy with frequent follow-up and high retention of participants to 24 months postpartum. Few studies have followed women to a period when childbirth-related injuries have healed, hormonal fluctuations have stabilized, women may have stopped breastfeeding, and sexual frequency has returned to prepregnancy levels. The study was designed to assess predictors at timepoints that reflect periods of routine appointments and opportunities for screening. The longer follow-up also allowed us to investigate the effects of a second pregnancy (41% of the sample) as a novel predictor; we did not find evidence that this factor predicted classification of dyspareunia.
An inherent limitation is that we did not have a nonpregnant control group of women to compare the observed patterns of dyspareunia over time. In addition, our core study outcome was dyspareunia and a small number of women who did not report a valid score for this measure were excluded. Therefore, women who are consistently avoiding sexual activity as a result of the pain may not be ascertained using the current study methodology. We also began our study in mid-pregnancy; future research should include an earlier assessment to investigate when the divergence of pain trajectories emerges. Although we used a validated and recommended measure of dyspareunia,12 which correlates strongly with other pain measures,31 it was a single item. Future studies should integrate a multidimensional assessment including other aspects of pain (eg, pain quality and effect), objective measurements (eg, vulvalgesiometer), and pain interference (eg, sexual function), which may exhibit different patterns of dyspareunia symptoms and risk factors.31,36 The majority of our sample were married, heterosexual, well-educated, and reported a middle-class income, limiting generalizability. We did not assess race, which is important for future research given evidence that Hispanic women report higher rates of dyspareunia as well as known racial inequities in pain treatment that negatively affect Black, Asian, and Hispanic women.37,38 We also did not collect data on use of contraception.
In a large prospective cohort of first-time mothers, we identified two distinct classes of dyspareunia trajectories. One in five participants experienced moderate pain that decreased over time but was often still present at 24 months postpartum. We also identified critical timepoints to assess pain catastrophizing to identify those at risk for moderate dyspareunia. Insufficient data concerning the health and sexual function of women during the postpartum period is a significant barrier to providing optimal care.39 This study enhances knowledge of the heterogeneity of dyspareunia across pregnancy and postpartum, which may contribute to better evaluation and treatment.
Footnotes
This project was funded by grants awarded to N. O. Rosen from the Canadian Institutes of Health Research (Funding Reference Numbers: 130338 and 152890) and Research Nova Scotia (Funding Reference Numbers: PSO-MAT-2013-8903 and PSO-EST-2016-774).
Financial Disclosure J. Chorney received funding from Lyceum Health for an unrelated study. R. George serves as an Advisory Board Consultant for OctaPharma Inc. and is an Associate Editor for the Canadian Journal of Anesthesia. N. O. Rosen is an Associate Editor of Archives of Sexual Behavior. The other authors did not report any potential conflicts of interest.
This project was approved by the IWK Health Centre Research Ethics Board (File #1018097). The authors thank Gillian Boudreau, Kayla Mooney, Megan Muise, Loriann Williams, Emily Coté, Hannah Richardson, and Lorraine Chiasson for their assistance with data collection.
This manuscript was registered with the Open Science Framework on April 21, 2021. https://osf.io/m8zyd/?view_only=8bf96eb8270f4e00a151ea8baa5b4747. All prior publications associated with this dataset are detailed in the registration.
Each author has confirmed compliance with the journal's requirements for authorship.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/C571.
REFERENCES
- 1.Rosen NO, Pukall C. Comparing the prevalence, risk factors, and repercussions of postpartum genito-pelvic pain and dyspareunia. Sex Med Rev 2016;4:126–35. doi: 10.1016/j.sxmr.2015.12.003 [DOI] [PubMed] [Google Scholar]
- 2.Bartellas E, Crane JMG, Daley M, Bennett KA, Hutchens D. Sexuality and sexual activity in pregnancy. Br J Obstet Gynaecol 2000;107:964–8. doi: 10.1111/j.1471-0528.2000.tb10397.x [DOI] [PubMed] [Google Scholar]
- 3.Rossi MA, Mooney KM, Binik YM, Rosen NO. A descriptive and longitudinal analysis of pain during intercourse in pregnancy. J Sex Med 2019;16:1966–77. doi: 10.1016/j.jsxm.2019.09.011 [DOI] [PubMed] [Google Scholar]
- 4.Tennfjord MK, Hilde G, Stær-Jensen J, Ellström E, Bø K. Dysparenia and pelvic floor muscle function before and during pregnancy and after childbirth. Int Urogynecol J 2014;25:1227–35. doi: 10.1007/s00192-014-2373-2 [DOI] [PubMed] [Google Scholar]
- 5.Alligood-Peroco NR, Kjerulff KH, Repke JT. Risk factors for dyspareunia after childbirth. Obstet Gynecol 2016;128:512–8. doi: 10.1097/AOG.0000000000001590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Banaei M, Kariman N, Ozgoli G, Nasiri M, Ghasemi V, Khiabani A, et al. Prevalence of postpartum dyspareunia: a systematic review and meta-analysis. Int J Gynaecol Obstet 2020;153:14–24. doi: 10.1002/ijgo.13523 [DOI] [PubMed] [Google Scholar]
- 7.Dawson SJ, Vaillancourt-Morel M-P, Pierce M, Rosen NO. Biopsychosocial predictors of trajectories of postpartum sexual function in first-time mothers. Health Psychol 2020;39:700–10. doi: 10.1037/hea0000861 [DOI] [PubMed] [Google Scholar]
- 8.Pâquet M, Rosen NO, Steben M, Mayrand M, Santerre-Baillargeon M, Bergeron S. Daily anxiety and depressive symptoms in couples coping with vulvodynia: associations with pain, sexual function, and both partners' sexual distress Pain. 2018;19:552–61. doi: 10.1016/j.jpain.2017.12.264 [DOI] [PubMed] [Google Scholar]
- 9.Rosen NO, Muise A, Impett EA, Delisle I, Baxter M, Bergeron S. Sexual cues mediate the daily relations between interpersonal goals, pain, and wellbeing in couples coping with vulvodynia. Ann Behav Med 2018;52:216–27. doi: 10.1093/abm/kax046 [DOI] [PubMed] [Google Scholar]
- 10.Desrochers G, Bergeron S, Khalifé S, Dupuis M-J, Jodoin M. Fear avoidance and self-efficacy in relation to pain and sexual impairment in women with provoked vestibulodynia. Clin J Pain 2009;25:520–27. doi: 10.1097/AJP.0b013e31819976e3 [DOI] [PubMed] [Google Scholar]
- 11.Barrett G, Pendry E, Peacock J, Victor C, Thakar R, Manyonda I. Women's sexual health after childbirth. Br J Obstet Gynaecol 2000;107:186–95. doi: 10.1111/j.1471-0528.2000.tb11689.x [DOI] [PubMed] [Google Scholar]
- 12.Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005;113:9–19. doi: 10.1016/j.pain.2004.09.012 [DOI] [PubMed] [Google Scholar]
- 13.Pukall CF, Bergeron S, Brown C, Bachmann GA, Wesselmann U. Recommendations for self-report outcome measures in vulvodynia clinical trials. Clin J Pain 2017;33:756–65. doi: 10.1097/AJP.0000000000000453 [DOI] [PubMed] [Google Scholar]
- 14.Boonstra AM, Stewart RE, Köke AJ, Oosterwijk RFA, Swaan JL, Schreurs KMG, et al. Cut-off points for mild, moderate, and severe pain on the numeric rating scale for pain in patients with chronic musculoskeletal pain: variability and influence of sex and catastrophizing. Front Psychol 2016;7:1466. doi: 10.3389/fpsyg.2016.01466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rosen NO, Bailey K, Muise A. Degree and direction of sexual desire discrepancy are linked to sexual and relationship satisfaction in couples transitioning to parenthood. J Sex Res 2017;55:241–25. doi: 10.1080/00224499.2017.1321732 [DOI] [PubMed] [Google Scholar]
- 16.Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. B J Psychiat 1987;150:782–86. doi: 10.1192/bjp.150.6.782 [DOI] [PubMed] [Google Scholar]
- 17.Cox JL, Chapman G, Murray D, Jones PW. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in non-postnatal women. J Affect Disord 1996;39:185–89. doi: 10.1016/0165-0327(96)00008-0 [DOI] [PubMed] [Google Scholar]
- 18.Sullivan MJL, Bishop S, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess 1995;7:524–32. doi: 10.1037/1040-3590.7.4.524 [DOI] [Google Scholar]
- 19.Cooper ML, Shapiro C, Powers S. Motivations for sex and risky sexual behavior among adolescents and young adults: a functional perspective. J Pers Soc Psychol 1998;75:1528–58. doi: 10.1037/0022-3514.75.6.1528 [DOI] [PubMed] [Google Scholar]
- 20.Newman DA. Longitudinal modeling with randomly and systematically missing data: a simulation of ad hoc, maximum likelihood, and multiple imputation techniques. Org Res Methods 2003;6:328–62. doi: 10.1177/1094428103254673 [DOI] [Google Scholar]
- 21.Grimm KJ, Ram N, Estabrook R. Growth modeling: structural equation and multilevel modeling approaches. Guilford Press; 2016. [Google Scholar]
- 22.Ferguson SL, Moore EW, Hull DM. Finding latent groups in observed data: a primer on latent profile analysis in mplus for applied researchers. Int J Behavl Dev 2020;44:458–68. doi: 10.1177/0165025419881721 [DOI] [Google Scholar]
- 23.Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equation Model 2007;14:535–69. doi: 10.1080/10705510701575396 [DOI] [Google Scholar]
- 24.Lavner JA, Bradbury TN, Karney BR. Incremental change or initial differences? testing two models of marital deterioration. J Fam Psychol 2012;26:606–16. doi: 10.1037/a0029052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Asparouhov T, Muthén BO. Auxiliary variables in mixture modeling: three-step approaches using M plus. Struct Equ Model 2014;21:329–41. doi: 10.1080/10705511.2014.915181 [DOI] [Google Scholar]
- 26.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc 1995;57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x [DOI] [Google Scholar]
- 27.Signorello LB, Harlow BL, Chekos AK, Repke JT. Postpartum sexual functioning and its relationship to perineal trauma: a retrospective cohort study. Am J Obstet Gynecol 2001;184:881–8. doi: 10.1067/mob.2001.113855 [DOI] [PubMed] [Google Scholar]
- 28.McDonald EA, Gartland D, Small R, Brown SJ. Dyspareunia and childbirth: a prospective cohort study. Br J Obstet Gynaecol 2015;122:672–9. doi: 10.1111/1471-0528.13264 [DOI] [PubMed] [Google Scholar]
- 29.Bergeron S, Corsini-Munt S, Aerts L, Rancourt K, Rosen NO. Female sexual pain disorders: a review of the literature on etiology and treatment. Cur Sex Health Rep 2015;7:159–69. doi: 10.1007/s11930-015-0053-y [DOI] [Google Scholar]
- 30.McDonald EA, Gartland D, Small R, Brown SJ. Frequency, severity and persistence of postnatal dyspareunia to 18 months postpartum: a cohort study. Midwifery 2016;34:15–20. doi: 10.1016/j.midw.2016.01.012 [DOI] [PubMed] [Google Scholar]
- 31.Rosen NO, Bergeron S, Pukall CF. Recommendations for the study of vulvar pain in women, part 1: review of assessment tools. J Sex Med 2020;17:180–94. doi: 10.1016/j.jsxm.2019.10.023 [DOI] [PubMed] [Google Scholar]
- 32.Pukall CF, Bergeron S, Rosen NO, Jackowich R. Persistent genitopelvic pain: classification, comorbidities, chronicity, and interpersonal factors. Cur Sex Health Rep 2020;12:15–23. doi: 10.1007/s11930-020-00239-7 [DOI] [Google Scholar]
- 33.Glowacka M, Rosen NO, Chorney J, Snelgrove-Clarke E, George R. Genito-pelvic pain during pregnancy and postpartum: the prospective impact of pain-related anxiety and hypervigilance to pain. J Sex Med 2014;11:3021–34. doi: 10.1111/jsm.12675 [DOI] [PubMed] [Google Scholar]
- 34.Vlaeyen JWS, Linton SJ. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012;153:1144–7. doi: 10.1016/j.pain.2011.12.009 [DOI] [PubMed] [Google Scholar]
- 35.Thomtén J, Karlsson A. Psychological factors in genital pain: the role of fear-avoidance, pain catastrophizing and anxiety sensitivity among women living in Sweden. Scand J Pain 2014;5:193–9. doi: 10.1016/j.sjpain.2014.01.003 [DOI] [PubMed] [Google Scholar]
- 36.Götz FM, Gosling SD, Rentfrow PJ. Small effects: the indispensable foundation for a cumulative psychological science. Perspect Psychol Sci 2021 Jul2. [Epub ahead of print]. doi: 10.31234/osf.io/hzrxf [DOI] [PubMed] [Google Scholar]
- 37.Nguyen RHN, Reese RL, Harlow BL. Differences in pain subtypes between Hispanic and non-Hispanic White women with chronic vulvar pain. J Womens Health 2015;24:144–50. doi: 10.1089/jwh.2014.4892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Johnson JD, Ifeyinwa A, McKenzie C, Tucker C, Tully KP, Bryant K, et al. Racial and ethnic inequities in postpartum pain evaluation and management. Obstet Gynecol 2019;134:1155–62. doi: 10.1097/AOG.0000000000003505 [DOI] [PubMed] [Google Scholar]
- 39.Kline CR, Martin DP, Deyo RA. Health consequences of pregnancy and childbirth as perceived by women and clinicians. Obstet Gynecol 1998;92:842–8. doi: 10.1016/S0029-7844(98)00251-8 [DOI] [PubMed] [Google Scholar]