

Abstract
Introduction:
Sexual health disparities are leading causes of morbidity among youth of color in the United States. We conducted a scoping review of the literature on precursors to sexual risk-taking among young adolescents of color (ages 10-14) to assess precedents of sexual experience and their utility as measurable proximal constructs and behaviors gauging sexual risk and sexual risk prevention efforts.
Methods:
This study was conducted using the PRISMA extension for scoping reviews (PRISMA-ScR) guidelines. We searched for quantitative studies that assessed the relationships between precursors and subsequent sexual behaviors, incorporated youth of color, and specified young adolescents as the study sample. All articles were in English, however we explored both U.S. and International databases.
Results:
The database search yielded 11 studies published between 2000 and 2017. Most literature focused on youth in urban settings, and on Black and Latinx youth, while only two addressed the special circumstances of American Indian and Alaska Native youth. Sex expectancies outcomes for youth of color were likely to predict sexual risk taking and self-efficacy about sex was related to abstinence.
Conclusions:
Etiologic studies that seek to understand precursors to sexual risk taking among youth of color are limited and this paucity truncates the ability to develop sexual risk prevention programs for the age group in which prevention is most needed.
Keywords: Young adolescents, sexual risk-taking, risk prevention
Introduction
Teen pregnancy and sexually transmitted infections (STIs) are leading causes of morbidity among youth of color in the United States (Hamilton, D.T. & Morris, 2015). STIs and pregnancy during adolescence have detrimental long-term social, economic, and health effects (Hoffman, 2011; Hoffman, 2008). While rates of teen pregnancy have decreased over the past 25 years, disparities remain among youth of color. Latinx and Black adolescents report pregnancy rates over twice as high as non-Hispanic Whites (NHW) (Hamilton, B.E., Osterman, Driscoll, & Rossen, 2018). Chlamydia and gonorrhea rates are nearly five and 12 times higher, respectively, among Black youth ages 15-19 compared to NHW adolescents (Centers for Disease Control and Prevention, 2018). Latinx and Black high school students are nearly twice as likely to report not using contraception during last intercourse when compared to NHW youth (Kann et al., 2018). The epidemiological profile of American Indian and Alaska Native (AI/AN) adolescents shows similar disparities in adverse sexual health outcomes: chlamydia and gonorrhea rates are nearly three times higher, and teen birth rates are 1.7 times higher among AI/AN compared to NHW youth ages 15-19 (Dippel, Hanson, McMahon, Griese, & Kenyon, 2017; Hamilton, B. E. et al., 2018). AI/AN high school students are twice as likely to report having had more than one sexual partner and are three times less likely to use condoms (DeRavello, Everett Jones, Tulloch, Taylor, & Doshi, 2014).
These statistics make it clear that effective sexual risk prevention efforts are needed for these populations. Current approaches often target prevention efforts during teen years when many youth are already sexually active. Shifting prevention to early adolescence, ages 10-14, to intervene before the onset of sexual behaviors may be critical to mitigating disparities in adverse sexual health outcomes among youth of color.
Early adolescence is a period of rapid physical, cognitive, emotional, and social growth (Caskey & Anfara Jr, 2007). Youth develop the capacity for abstract thought, become more autonomous, transition from relying on parents as models of social norms to relying on peers, and enter puberty (Caskey & Anfara Jr, 2007; Pedlow & Carey, 2004; L. Steinberg, 2005).While most young adolescents do not engage in sexual behaviors, they may have their first romantic relationships and experiences with sexual touching during this period, behaviors that are precursors to sexual activity (Coyle, Franks, Glassman, Walker, & Charles, 2014). During this developmental stage most youth are capable of reasoning necessary for sexual risk prevention (Pedlow & Carey, 2004), and researchers have increasingly recognized this developmental period as a critical stage for sexual risk prevention (Coyle, Kirby, Marín, Gómez, & Gregorich, 2004; Siegel, Aten, & Enaharo, 2001). However, greater understanding of how early adolescent attitudes and behaviors are related to later sexual risk is needed to inform the development of our age-appropriate interventions. Critical to both understanding these links and evaluating the impact of interventions is the identification of measures of early adolescent attitudes and behaviors related to sexual risk.
There has been work to identify age-appropriate measures of sexual risk for young adolescents (Bachanas et al., 2002; Bersamin, Walker, Fisher, & Grube, 2006; Bourdeau, Grube, Bersamin, & Fisher, 2011; Coyle et al., 2014; DiIorio et al., 2001; Guilamo-Ramos et al., 2007; Holloway et al., 2012; Mathews et al., 2008; Santelli et al., 2004). An important next step is to synthesize these efforts and analyze their theoretical and empirical contributions to defining and measuring precursors to sexual risk in early adolescence. Examining the underlying theories that provided structure and guidance for the development, implementation, and assessment of precursors to sexual risk will be important, as will be examining reported associations of age-appropriate constructs with subsequent sexual risk-taking among young adolescents, particularly those of color. Findings from such a review can position future studies to better assess early sexual risk and thus better inform prevention efforts.
To achieve this goal, we conducted a scoping review of the literature on individual level precursors to sexual risk among young adolescents. We focused on behavioral and psychosocial precedents of sexual experience and their utility as measurable proximal constructs and behaviors gauging sexual risk and sexual risk prevention efforts at young ages. This approach for reviewing literature differs from traditional systematic reviews, which are useful for examining more clearly defined research questions (e.g. “Does this particular sexual risk reduction intervention reduce teen pregnancy among AI/AN teens?”) (Tricco et al., 2018). Scoping reviews allow for the assessment of broader questions to examine the potential size and scope of available research on an often-understudied research area. Scoping reviews are preliminary assessments of available research and are best utilized when a body of literature has not been comprehensively reviewed. Thus, a scoping review is appropriate here, supporting systematic synthesizing and a categorization of literature on precursors to sexual risks among young adolescents of color.
Heuristic Framework
Our review focused on proximal, individual level precursors to sexual risk-taking among young adolescents. We were interested in identifying the relationship between each construct and sexual behaviors in later adolescence to identify 1) specific non-sexual behaviors that precede subsequent sexual risk-taking and 2) developmentally appropriate measures that can be used to assess the proximal impact of sexual health interventions for young adolescents. We developed a heuristic framework to guide the review, classifying findings into two major domains of early adolescent development: 1) Cognitive and Psychological Development, and 2) Social Development and Romantic Non-sexual Experimentation.
Cognitive and Psychological Development.
The first domain aligns with theoretical foundations used in the majority of sexual health research studies (Bersamin et al., 2006; Bourdeau et al., 2011; Coyle & Glassman, 2016; DiIorio et al., 2001; Holloway et al., 2012; Mathews et al., 2008). Early adolescence is associated with changes in cognitive functioning that have implications for sexual risk-taking (Caskey & Anfara Jr, 2007; O’Sullivan, Cheng, Harris, & Brooks-Gunn, 2007). During this period, youth begin to develop the capacity for abstract thought processes necessary for sexual risk protective behaviors. For instance, the emergence of abstract reasoning allows youth to consider hypothetical situations and future consequences of sexual experience and sexual risks (Caskey & Anfara Jr, 2007; Pedlow & Carey, 2004; Steinberg & Morris, 2001). In addition, young adolescents gain an increased capacity for introspection, reflection, and establishment of personal goals (Caskey & Anfara Jr, 2007; L. Steinberg, 2005). As a result, youth develop personal values about sex and begin to understand the potential negative impact sexual risk-taking can have on achieving goals (Caskey & Anfara Jr, 2007; Pedlow & Carey, 2004). Finally, young adolescents develop increased capacities to reason, consider probabilities, and envision multiple behavioral alternatives (Caskey & Anfara Jr, 2007; Pedlow & Carey, 2004). Thus, they can begin to develop health-protective decision making, self-management, and problem-solving skills related to sex (Pedlow & Carey, 2004). Given the cognitive and psychological development that occurs in early adolescence, individual psychological and behavioral antecedents to sexual risk-taking are likely developmentally appropriate sexual risk precursors to measure (Bachanas et al., 2002; DiClemente et al., 2008).
Social Development and Romantic Non-sexual Experimentation.
Interventions targeting the social and relationship context common among young adolescents suggest the relevance of this second domain (Coyle et al., 2014). Concurrent with cognitive and psychological development in early adolescence, youth have an increasing need to belong to a group, peer approval becomes more important and adult approval wanes (Caskey & Anfara Jr, 2007). Young adolescents develop closer connections with peers, begin dating in groups, and engage in short-term romantic relationships (Coyle et al., 2014; Steinberg & Morris, 2001). They begin to experiment with new intimate behaviors such as holding hands, sexual touching, and romantic kissing. These behaviors have been linked to early sexual experience and risky sexual behaviors, including unprotected sex and sexual activity, putting youth at risk before they are socially or emotionally equipped (Coyle et al., 2014; Pedlow & Carey, 2004; L. Steinberg, 2005). Thus, these behaviors are likely candidates for measures of precursors of sexual risk.
These two conceptually distinct domains facilitated classification of measures and identifying relationships of measures with sexual risk-taking; they also helped identify gaps in the literature with regard to research in this age group. With this heuristic framework and the scoping review method, our review was guided by the following questions: 1) What were the conceptual and theoretical frameworks, methodologies implemented, and measures used to assess these associations? 2) Which precursors to sexual risk-taking among young adolescents have been empirically studied and shown to be associated with, or predictive of, sexual behaviors in later adolescence? 3) Can findings be used to inform our conceptualization of precursors to sexual risks among youth of color? In addition, the review assessed gender, socioeconomic status, racial group, and urban-rural differences, if available, among measures of precursors of sexual risk-taking, since distinct differences in sexual behaviors have been observed across gender, class, race groups, and geographic regions. Further, adolescents who identify as female have been shown to be more likely to refuse sex and less likely to report inconsistent condom use (Seth et al., 2012). Lower socioeconomic status (SES) has been shown to be a risk factor for teen pregnancy and STIs; likely due to limited educational and social opportunities and access to birth control and sexual health resources and services for low SES individuals when compared to high (Harling, Subramanian, Bärnighausen, & Kawachi, 2013). Last, there are observed rural-urban differences in adolescent health outcomes. Adolescents from rural geographic regions report higher rates of teen pregnancy compared to urban teens. This may be due to the limited number of providers in rural communities, the perception of a lack of confidentiality when accessing sexual health services, and the cost of healthcare services (Geske, Quevillon, Struckman-Johnson, & Hansen, 2016; Kozhimannil et al., 2015; Quine et al., 2003).
Methods
Overview
Guidelines from the PRISMA extension for Scoping Reviews (PRISMA-ScR) were used for this study. The PRISMA-ScR includes elements, both optional and required, to be included in the title, abstract, introduction, methods, results, and discussion sections of a scoping review (Tricco et al., 2018). For the first two elements we identified the manuscript as a scoping review in the title and provided a structured summary of the various components of the manuscript (e.g. introduction and results) that related to the review questions and objectives. For the introduction, we described the rationale for the review in the context of what is already known from existing literature and explained why the review questions were appropriate for a scoping review approach. The introduction explicitly provided a statement of the objectives and research questions being addressed with indication of how findings were used to conceptualize review objectives. Specific to the methods section, characteristics of sources of literature used and the inclusion and exclusion criteria were identified. In addition, the process for selecting the sources of evidence and the methods for handling and summarizing the data were described. As it relates to the results, we stated the number of sources of literature screened and included in the final review and describe reasons for exclusion in a flow chart. Also, we presented characteristics of the data with the associated citations and summarize the findings. Last, in the discussion we summarized the key results, discussed limitations, and provided a general interpretation of findings.
Retrieval
For this review, articles from peer-reviewed journals and gray literature—literature that is not scholarly, but is produced by researchers and practitioners in the field (Turner, Liddy, Bradley, & Wheatley, 2005)—published between 2000 and 2017 were identified by searching Ovid MEDLINE, PsycINFO, Google Scholar, Web of Science, and EMBASE. Search results were methodically assessed by reviewing abstracts and, if necessary, full publications to ensure that the inclusion and exclusion criteria described below were met. We searched electronic databases using variations and Boolean connections of sexual behavior terms (e.g., early sexual initiation or early initiation of sexual intercourse) and variations of various precursors within each heuristic domain (e.g., perceived susceptibility to sexual risks or perceived vulnerability to sexual risks). We also searched reviewed studies’ reference lists for additional publications.
Inclusion and Exclusion Criteria
For inclusion, articles had to: a) be published in English, but could originate from outside the United States; b) incorporate racial and ethnic minority youth; c) describe social and geographic characteristics of the sample; d) describe measures used; e) include findings based on quantitative methods only; f) clearly specify young adolescents as the study sample; g) empirically examine the relationships between a precursor that fell within the domains of the heuristic framework and subsequent sexual behaviors. Articles were excluded if they summarized research assessing pre- and post-program changes in various precursors, since our study focused on the normative relationships among precursors and subsequent sexual risk-taking. Because the goals of this review were to identify measures of precursors of sexual risk that can be used in future research and examine the associations of these measures with sexual health outcomes, we only included studies that used quantitative methods.
Data Abstraction and Synthesis
We extracted information on authorship, publication year, theoretical framework, developmental domain, precursors measured, sexual behavior outcome, timeframe during which study data were collected, sample size, demographics of sample, measures, study design and methodology, and major findings.
Results
Sample Characteristics
Thirty-eight publications were initially identified; 11 met criteria and represent the final sample (see Figure 1). All were retrieved from peer-reviewed journals. Tables 1 and 2 provide details for these 11 studies. Sample sizes ranged from 220 to 1,440. Most were conducted in an urban setting; study designs were both cross-sectional and longitudinal.
Figure 1.
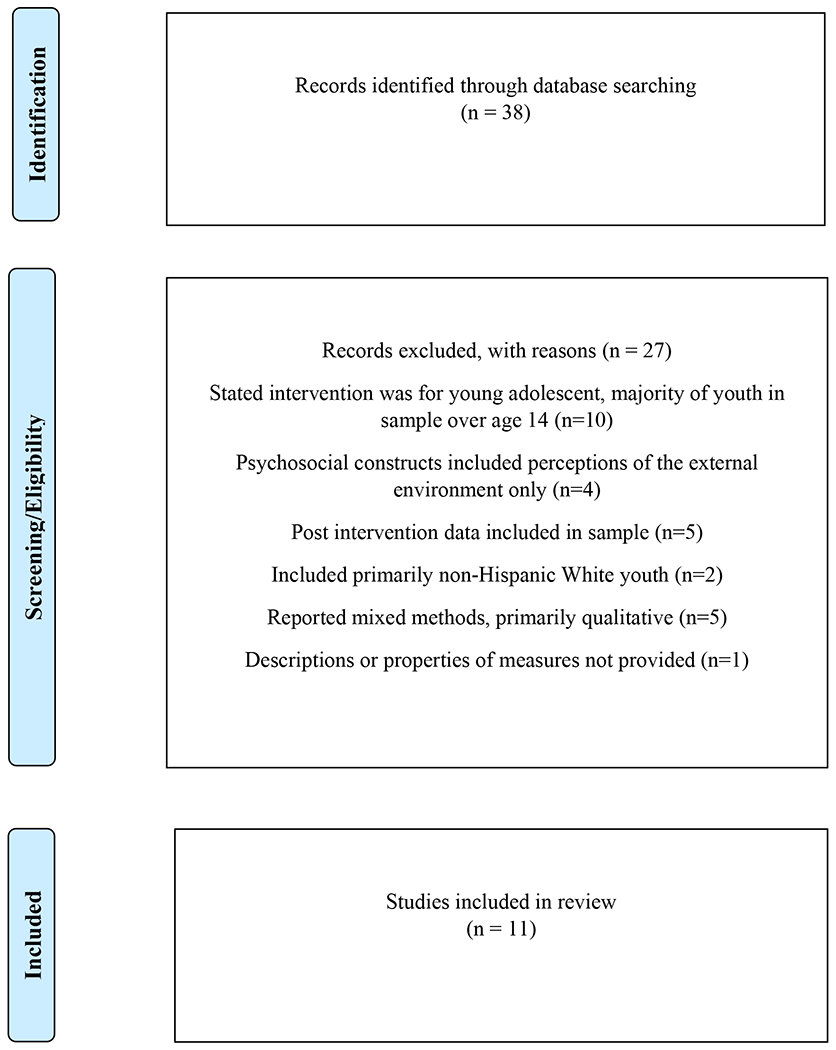
Selection process of studies included
Table 1.
Characteristics of Research Studies Included in the Final Study
| Author/Year | Domain | Sample Size | Age | Race/Ethnicity | Geographic Location | SES Status | Major Findings |
|---|---|---|---|---|---|---|---|
| Holloway 2012 [1] | Cognitive and Psychological | 223 | 11 to 13 | Black and Latinx | Urban | Low SES | Higher scores in self-evaluative and social expectancies decreased odds of engaging in sexual possibility situations. Higher scores on self-evaluative expectancy decreased odds of kissing. Self-evaluative and social expectancies decreased odds of sexual touching. |
| Bersamin 2006 [2] | Cognitive and Psychological | 1,105 | 12 to 16 | Non-White and White | Urban | Low SES | Adolescents who reported having had oral sex reported fewer negative social expectancies than adolescents who had not had oral sex. Adolescents who reported higher levels of negative social expectancies and negative physical expectancies were less likely to report having had oral sex. Negative physical expectancies were negatively associated with vaginal intercourse. |
| Boudreau 2011 [3] | Cognitive and Psychological | 1,105 | 10 to 17 | Asian American, Latinx, Black, White | Urban | Low SES | Four correlated factors capture the structure of expectancy items: social risk, social benefit, health risk, and pleasure expectancies. Only social risk expectancies were significant in predicting subsequent sexual behavior |
| DiIorio 2001 [4] | Cognitive and Psychological | 405 | 13 to 15 | Black and White | Urban | Low SES | Self-efficacy to resist sex and social outcome expectancies were not significantly associated with abstaining from sex. For those who were sexually active, self-efficacy to put on a condom, self-efficacy to refuse sex, and social outcome expectancies were significantly associated with consistent condom use. Self-efficacy to discuss sexual history, self-evaluative expectancies, and physical expectancies were not associated with consistent condom use. |
| Mathews 2008 [5] | Cognitive and Psychosocial | 1,440 | Grade 8 | South African | Urban | Low SES | The strongest predictor of sexual intentions was social outcome expectancies. Transitioning to sex decreased with increase self-efficacy related to negotiating delaying sex. Adolescence with more knowledge were less likely to make the transition to first sexual intercourse. |
| Guliamo-Ramos 2007 [6] | Cognitive and Psychological | 668 | Grades 6, 7, and 8 | Dominican, Puerto Rican, Black | Urban | Low SES | Self-evaluative and social expectancies were significantly more strongly associated with intentions to have sex for boys as opposed to girls. Social expectancies were more strongly associated with intentions to have sex for boys when compared to girls. |
| Santelli 2004 [7] | Cognitive and Psychological | 1,637 | Grades 7 and 8 | Black, Hispanic, White, and Asian | Urban | Low SES | Adolescents scoring high on self-efficacy were less likely to initiate intercourse. Knowledge was not predictive of initiation of sexual intercourse. Self-efficacy predicted initiation of sexual intercourse. |
| O’Donnell 2003 [8] | Cognitive and Psychological | 849 | Average age 12.2 | Black | Urban | Low SES | Those who reported the most positive social expectancies were most likely to have reported initiating sex at base baseline. The more positive the social expectancies, the earlier the report of sexual initiation. Refusal self-efficacy delayed sexual intercourse through 10th grade. |
| Bachanas 2004 [9] | Cognitive and Psychological | 158 | 12 to 19 | Black | Urban | Low SES | Self-efficacy was not significantly associated with teens engaging in risky sexual behaviors. |
| Coyle 2014 [10] | Emotional Development and Sexual Experimentation | 911 | Grade 7 | Black and Hispanic | Urban | Low SES | Study participants who reported ever touching private parts or being sexually touched were significantly more likely to ever have had vaginal intercourse. Among a subsample of youth who reported being in a current relationship, holding hands, kissing, cuddling, and other sexual activities were not significantly associated with vaginal intercourse. Among this subsample those who reported touching private parts were more likely to report vaginal intercourse; finding was not statistically significant. |
| Chewning 2001 [11] | Cognitive and Psychosocial | 484 | Graders 6-12 | American Indian | Rural | Low SES | Self-efficacy to abstain from sex was significantly and positively associated with never having sex and the proportion of times a condom was used during intercourse. Self-efficacy to use/get condoms was significantly and positively associated with the proportion of times a condom and birth control were used during intercourse. |
Table 2.
Measurement Items Used for Each Study
| Author/Year | Theoretical Framework | Study Design | Precursors Measured | Measurement Items (if available) or Constructs | Outcome Measured |
|---|---|---|---|---|---|
| Holloway 2012 [1] | Social Cognitive Theory | Cross-sectional | Sex Expectancies | Constructs: 1) Personal/Parental Expectancies, 2) Romantic/Peer Expectancies, 3) Academic/Career Expectancies |
1) Sexual possibility situations, 2) Kissing in a romantic or sexy way, 3) Sexual touching, |
| Bersamin 2006 [2] | Social Cognitive Theory | Cross-sectional | Sex Expectancies | Scale “yes” and “no” 1) I would be more popular, 2) I would feel more loved and wanted, 3) I would feel more attractive, 4) I would feel guilty, 5) I wouldget into trouble with my parents, 6) I would disappoint people who are important to me, 7) I could get pregnant/get someone pregnant, and 8) I could get an STI |
1) Oral, 2) Vaginal intercourse |
| Bourdeau 2011 [3] | Theory not specified | CFA, Longitudinal | Sex Expectancies | Scale “very unlikely”, “somewhat unlikely”, “somewhat likely”, and “very likely” 1) Get pregnant or get someone pregnant, 2) Enjoy it, 3) Get a sexually transmitted disease, 4) Feel guilty, 5) Be more popular, 6) Get into trouble with your parents, 7) Get a bad reputation, 8) Feel more loved and wanted, 9) Lose your self-respect, 10) Feel more attractive, 11) Keep your boyfriend or girlfriend from breaking up with you, 12) Feel closer to your partner, 13) Fit in more with your friends, 14) Disappoint people who are important to you, 15) Get HIV/AIDS, 16) Feel happy, 17) Have fun, 18) Feel more grown up, 19) Feel excited, 20) Feel satisfied, 21) Feel pleasure |
1) Holding hands, 2) Kissing or making out, 3) Ever engaging in oral sex, 4) Ever engaging in vaginal sex, 5) Ever engaging in anal sex |
| DiIorio 2001 [4] | Social Cognitive Theory | Cross-sectional | Self-Efficacy, Sex Expectancies | Constructs: 1) Self-efficacy to stay away from people who pressure you into having sex, 2) Self-efficacy to use a condom 3) Self-efficacy to refuse sex with a partner 4) Self-efficacy to discuss the partner’s sexual history 5) Self-evaluative expectancies with not having sex, 6) Physical expectancies with not having sex 7) Social expectancies with not having sex, 8) Self-evaluative expectancies with condom use, 9) Physical expectancies with condom use, 10) Social outcomes expectancies with condom use |
1) Delay in onset of sexual intercourse, 2) Condom use |
| Mathews 2008 [5] | Theory of Planned Behavior | Longitudinal | Knowledge, Self-Efficacy, Sex-Expectancies | Constructs: 1) HIV/AIDS knowledge, 2) Negative social outcome expectancies related to not having sex, 3) Severity of threats from consequences of unprotected sex (HIV/AIDS, STDs, and pregnancy) 4) Susceptibility to consequences of unprotected sex, 5) Self efficacy to say no to sex |
1) Intention to have sex, 2) Transition to first intercourse |
| Guliamo-Ramos 2007 [6] | Social Cognitive Theory | Cross-sectional | Sex Expectancies | “Scale ““yes”” and ““no”” 1) My mother would be embarrassed if I got pregnant. 2) It would be embarrassing for me if I got pregnant. 3) It is better to wait until I am married to have intercourse. 4) It would create money problems for my family if I got pregnant. 5) I might get HIV/AIDS. 6) I might get a sexually transmitted disease. 7) I might get a bad reputation. 8) I would feel guilty. 9) It would be morally wrong. 10) It would interfere with school. 11) I might get pregnant. 12) My boyfriend might lose respect for me. 13) I would regret not waiting until I was married. 14) It would satisfy my curiosity about sex. 15) I think I would enjoy the sex. 16) I would feel closer to the boy with whom I had intercourse. 17) It would prove to my boyfriend how much I love him. 18) I would be more popular with the boys. 19) I would feel more “grown-up.” 20) I would feel more attractive. 21) I wouldn’t feel left out. |
1) Sexual intentions |
| Santelli 2004 [7] | Social Learning Theory | Longitudinal | Self-efficacy, Knowledge, Sex Expectancies | Constructs: 1) Self-efficacy, 2) Knowledge about STD and condom use, 3) Perceived risk of STD |
1) Early initiation of sex |
| O’Donnell 2003 [8] | Social Cognitive Theory | Longitudinal | Sexual Norms and Attitudes | Constructs: 1) Sex outcome expectancies related to sexual behavior, 2) Sex refusal self-efficacy |
1) First report of sexual intercourse |
| Bachanas 2004 [9] | Risk and Protective Model | Cross-sectional | Knowledge, Self-Efficacy | Constructs: 1) Functional knowledge about HIV/AIDS, 2)Safer sex, practice self-efficacy |
1) Age first willingly had sex, 2) Number of partners in last 60 days, 3) Number of times had sex with that partner, 4) Number of times used a condom |
| Coyle 2014 [10] | Theory not specified | Cross-sectional | Romantic Non-Sexual Activities | Scale “yes” or “no” 1) We held hands, 2) We kissed, 3) We cuddled, 4) We touched each other’s private parts |
1) Had vaginal sex, 2) Touched private parts |
| Chewning 2001 [11] | Problem Behavior Theory | Cross-sectional | Self-efficacy | Specific items were not specified, but authors stated that items were obtained from three self-efficacy scales with high reliability related to sexual behaviors developed specifically for AI/AN populations by Rolf et al.(Rolf et al., 1991) | 1)Had sexual intercourse, 2)Had sexual intercourse in the past three months, 3) Proportion of times birth control was used, 4) Proportion of times condoms were use |
Cognitive and Psychological Development
Sex expectancies outcomes.
Sample description.
There were eight studies that included sex expectancies outcomes—defined as anticipated consequences (negative or positive) of engaging in sex behaviors (Bersamin et al., 2006; Bourdeau et al., 2011; DiIorio et al., 2001; Guilamo-Ramos et al., 2007; Holloway et al., 2012; Mathews et al., 2008; L. O’Donnell, Myint-U, O’Donnell, & Stueve, 2003; Santelli et al., 2004). Among these studies, the ages within early adolescence that were included were inconsistent. Only three studies included youth ages 10 to 11—what we defined as the beginning of early adolescence (Bourdeau et al., 2011; Chewning et al., 2001; Guilamo-Ramos et al., 2007). The remaining studies (n=5) focused on youth ages 12 and older (Bersamin et al., 2006; Holloway et al., 2012; Mathews et al., 2008; L. O’Donnell et al., 2003; Santelli et al., 2004). The primary populations were Black and Latinx, and some included non-Hispanic White youth; one study specified AI/AN youth in its sample (Bourdeau et al., 2011). Most studies included racial and ethnic minority youth only, and differences in associations among precursors and subsequent sexual behaviors by race were often not assessed.
Theoretical framework and study design.
The psychosocial theories used to guide these studies, if specified, included Social Cognitive Theory (SCT) (DiIorio et al., 2001; Holloway et al., 2012) and Social Learning Theory (SLT) (L. O’Donnell et al., 2003; Santelli et al., 2004). Four studies were longitudinal (Bourdeau et al., 2011; Mathews et al., 2008; L. O’Donnell et al., 2003; Santelli et al., 2004). Four studies were cross-sectional and did not explore whether expectancies predicted later sexual behaviors (Bersamin et al., 2006; DiIorio et al., 2001; Guilamo-Ramos et al., 2007; Holloway et al., 2012). All cross-sectional studies used exploratory factor analysis. Although items were not consistent across studies, identified factors of sex expectancies were conceptually similar. Three common factors appeared across all studies, and aligned with the following types of expectancies outcomes: 1) self-evaluative expectancy outcomes (disappointment in self or perceived disappointment from parents if engaged in sexual activities), 2) social expectancy outcomes (perceived social acceptance or rejection from peers if participated in sex), and 3) physical expectancy outcomes (perceived risks of HIV, STIs, or pregnancy as a consequence of sex) (DiIorio et al., 2001). Factors across all studies were internally consistent with Cronbach’s alphas ranging from .56-.94.
Results.
Sexual health outcomes analyzed in cross-sectional studies varied. Some studies analyzed sexual behaviors as dependent variables, but others looked at behaviors more salient in this age group (Guilamo-Ramos et al., 2007; Holloway et al., 2012). The latter studies found that higher scores in constructs similar to self-evaluative and social expectancies were associated with lower odds of romantic kissing, sexual touching, situations where sexual intercourse is possible, and sexual intentions (Guilamo-Ramos et al., 2007; Holloway et al., 2012). A study looking at sexual behaviors among sexually active adolescents showed that although negative social expectancies were not significantly associated with abstaining from sex they were significantly associated with consistent condom use. In the same study, self-evaluative and physical outcome expectancies were not associated with consistent condom use (DiIorio et al., 2001). Across all cross-sectional studies, physical expectancies did not show significant associations with developmentally appropriate measures or sexual behaviors (DiIorio et al., 2001; Guilamo-Ramos et al., 2007; Holloway et al., 2012; Mathews et al., 2008).
One study examined SES, youth who reported lower SES tended to perceive fewer consequences of engaging in sexual-related behaviors and were likely to report higher non-sexual romantic behaviors, sex intentions (readiness to engage in sexual behaviors), and actual sexual behaviors (L. O’Donnell et al., 2003).
Two studies analyzed gender differences. In one, boys reported lower self-evaluative and social expectancies and higher non-romantic activities when compared to girls (Mathews et al., 2008); in another, girls reported lower self-evaluative and social expectancies and higher sexual intentions than boys (Guilamo-Ramos et al., 2007).
Among the longitudinal studies, one study found that items relevant to physical expectancies were not predictors of sexual intentions or the transition to sexual behaviors across two time points (Santelli et al., 2004). In this study, the strongest predictor of transitioning to sexual behaviors was social expectancies. Similarly, in another study, positive social expectancies to engaging in sex ((peers would approve of sexual behavior)) were associated with earlier initiation of sex (L. O’Donnell et al., 2003). The third longitudinal study sought to develop a reliable and valid standardized measure of sex expectancies, the Adolescent Sexual Expectancies Scale (ASEXS), using confirmatory factor analysis (CFA) (Bourdeau et al., 2011). In addition, the predictive ability of sex expectancies and frequency of sexual behavior over a three-year period was assessed. The CFA found four correlated factors for sexual expectancy, corresponding to expectations regarding the likelihood of social risk, social benefit, health risk, and pleasure. Social risk and benefit were conceptually similar to social expectancies, health risk was similar to physical expectancies, and pleasure was the perceived pleasure youth would experience when engaging in sexual behaviors. These factors had acceptable internal consistency (Cronbach’s alphas ranging from .74-.85). Only social risk expectancies were significantly related to subsequent sexual behavior.
Self-efficacy related to sex.
Sample description.
Six studies assessed associations between self-efficacy related to sex and sexual behaviors among young adolescents (Bachanas et al., 2002; Chewning et al., 2001; DiIorio et al., 2001; Mathews et al., 2008; L. O’Donnell et al., 2003; Santelli et al., 2004). Many of these studies were also included in the sex expectancy outcome studies mentioned above, since the majority of studies that incorporated psychosocial precursors included multiple constructs. Two studies in this category included youth younger than age 12 (Chewning et al., 2001; D. A. O’Donnell, Schwab-Stone, & Muyeed, 2002), while the remaining four included youth ages 12 or older. All studies focused on youth from economically and socially disadvantaged populations. Two of the six studies specified Latinx and Black young adolescents only (Bachanas et al., 2002; D. A. O’Donnell et al., 2002); one study specified AI/AN youth only (Chewning et al., 2001). Differences among the associations of self-efficacy related to sex and subsequent sexual behaviors were not analyzed across racial groups in these studies. SES was either controlled or was not used as a predictor of sexual behaviors and differences in associations between precursors across SES were not examined.
Theoretical framework and study design.
Five studies specified a theoretical framework; two were grounded in the SCT (DiIorio et al., 2001; L. O’Donnell et al., 2003), one incorporated the SLT (Santelli et al., 2004), another integrated the Problem Behavior Theory (PBT) (Chewning et al., 2001), the last study specified the Theory of Planned Behavior (TPB) (Mathews et al., 2008). While various theories were used, the overall concept of self-efficacy appeared to be the same across studies—one’s belief in their ability to succeed in a specific sex risk-prevention task. The types of self-efficacy analyzed varied across studies, with items focusing on sex resistance or refusal (Bachanas et al., 2002; DiIorio et al., 2001; D. A. O’Donnell et al., 2002), or negotiating delayed sex (Mathews et al., 2008). Three studies were cross-sectional (Bachanas et al., 2002; Chewning et al., 2001; DiIorio et al., 2001), and three were longitudinal (Mathews et al., 2008; L. O’Donnell et al., 2003; Santelli et al., 2004). In the cross-sectional studies, standardized items were not used to measure the various types of self-efficacy across studies.
Results.
There were inconsistent findings across studies of associations among self-efficacy related to sex and sexual behaviors. One study showed that youth who engaged in sex were less likely to report self-efficacy to resist sex (DiIorio et al., 2001). In addition, among those youth in the study who engaged in sex, self-efficacy to refuse sex was significantly associated with consistent condom use. Another study found sex-refusal self-efficacy to be related to abstinence (Chewning et al., 2001). In contrast, another study found that self-efficacy was not significantly related to engaging in risky sexual behaviors (Bachanas et al., 2002).
The four longitudinal studies also used measures of self-efficacy that were internally consistent (Cronbach’s alphas=.63-.86). Unlike the cross-sectional studies, the predictive ability of the various types of self-efficacy were consistent across studies. One study found that self-efficacy related to negotiating delayed sex decreased transition to first intercourse (Mathews et al., 2008). One study found that adolescents who scored higher on self-efficacy were less likely to initiate sexual intercourse (Santelli et al., 2004). In addition, a similar study showed that seventh graders who reported they could refuse sex were more likely to postpone intercourse through 10th grade (L. O’Donnell et al., 2003). Predictive models controlled for gender and did not assess gender differences in associations between self-efficacy and subsequent sexual risk.
Knowledge.
Sample description.
Knowledge about sex was analyzed in the multi-construct models (n=3) (Bachanas et al., 2002; Mathews et al., 2008; Santelli et al., 2004). As previously noted, youth older than age 12 were not included in these studies, and race and gender differences were not examined. The study samples focused on Black and Latinx youth in urban middle schools.
Theoretical framework and study design.
Two specified a theoretical framework—the TPB and SLT (Mathews et al., 2008; Santelli et al., 2004). Two studies conducted exploratory factor analysis and showed good internal consistency for knowledge constructs (Cronbach’s alphas ranged .69-.84). Although knowledge items varied, all appeared to relate to knowledge of HIV, pregnancy, and STIs. One study used an index of knowledge that consisted of 15 items; higher total score indicates greater HIV knowledge (Bachanas et al., 2002). One study was cross-sectional (Bachanas et al., 2002), and the remaining two were longitudinal.
Results.
Findings from the cross-sectional study that showed HIV/STI knowledge was not significantly associated with early initiation of sex (Bachanas et al., 2002). One longitudinal study found that young adolescents with better HIV/STI knowledge were less likely to make the transition to first intercourse (Mathews et al., 2008) and the other study showed that knowledge was not a statistically significant predictor of initiation of sex (Santelli et al., 2004).
Summary.
Sex expectancies outcomes and self-efficacy related to sex were the most common precursors examined. The measurement of these constructs was not standardized across studies. Physical expectancies were not associated with or predictive of sexual intentions or the transition to sexual behaviors. In the longitudinal studies, social expectancies and self-efficacy related to sex were predictive of sexual intentions and sexual behaviors among youth of color.
Social Development and Romantic Non-sexual Experimentation
Sample description and study design.
Only one study fell within the Social Development and Romantic Non-Sexual Experimentation domain and met the inclusion criteria for this review (Coyle et al., 2014). This study was a cross-sectional design consisting of predominately Black and Latinx seventh graders from an urban middle school.
Results.
Study participants who reported consensually ever touching private parts or being sexually touched were 9.27 times more likely to ever have had vaginal intercourse. Among a subsample of youth who reported being in a current relationship, non-sexual activities (holding hands, kissing, cuddling) were not significantly associated with vaginal intercourse but touching private parts was associated with 2.82 times greater likelihood of vaginal intercourse, although this finding was not statistically significant.
Summary
Youth reporting consensual touching of private parts or being touched were more likely to have had vaginal intercourse.
Discussion
This scoping review is the first that we know of to analyze and summarize existing literature on individual level precursors to sexual risk-taking among young adolescents of color. Our findings suggest that research related to precursors to sexual risk-taking has been largely stagnant, even while a focus on early prevention of sexual risk-taking among ethnic and racial minorities have escalated (Childs, Knight, & White, 2015; Johnson-Motoyama et al., 2016; Kaufman et al., 2010; Shegog et al., 2017). The results of the review revealed a small body of literature investigating precursors to sexual risk-taking among young adolescents of color. That only a few studies exist is disconcerting considering the relative high rates of teen pregnancy and STIs among youth of color compared to their NHW counterparts, and the associated detrimental long-term social, economic, and health outcomes (Centers for Disease Control and Prevention, 2015; S. Hoffman, 2011).
Findings from longitudinal studies showed that social expectancies and self-efficacy, both constructs of the SCT, and SES were predictive of sexual intentions and sexual behaviors among young adolescents of color. These findings align with studies that have been conducted with high school youth. Given the importance of peer group acceptance during this developmental stage, not surprisingly, anticipated social consequences influence sexual behaviors among adolescents. In addition, self-efficacy has been shown to be consistently associated with academic and other social outcomes among youth, and a negative association with SES and sexual risk taking has been observed.
Cross-sectional studies showed mixed associations between psychosocial precursors and sexual outcomes, perhaps due to different conceptual and theoretical models and measurements of precursors to sexual risks across studies, and inherent limitations of cross-sectional designs. Only one study assessed precursors within the Social Development and Romantic Non-sexual Experimentation domain. Overall, the thin base of research and the shortcomings of extant data made it challenging to identify the most relevant theoretical frameworks and measures to inform our conceptualization of precursors among youth of color.
Moving the prevention timeline to a younger developmental stage is critical. This review identified gaps to be addressed to inform future work. First, a better understanding of early social expectancies outcomes and self-efficacy related to sex using longitudinal methods is needed. Second, early adolescence begins the stage of multiple shorter relationships in which youth begin hugging, holding hands, sharing confidences, and touching sexually (Coyle et al., 2014). These behaviors may be important predictors of subsequent sexual risk-taking in later adolescence and, therefore, longitudinal studies that seek to better understand the role of these factors as precursors are critical. Understanding risk in early adolescence—that time of transition between childhood and teen years—will greatly expand our ability to design effective prevention efforts.
The importance of this line of research in early adolescence can be exemplified in the case of AI/AN youth. We found little literature that directly speaks to this diverse group (Bourdeau et al., 2011). Two studies were perhaps the most useful and applicable to AI/AN young adolescents. First, was the longitudinal study by Bourdeau et al. (2011) that looked at expectancies among AI/AN young adolescents from an urban setting. They found that social risk expectancies were likely to predict sexual risk-taking among these youth. Second, a study about the unique cultural and protective factors related to sexual risk-taking in a rural Midwestern reservation among AIAN youth grades 6-12 found sex-refusal self-efficacy to be related to abstinence (Chewning et al., 2001). The findings of the latter study suggest that unique factors commonly present in tribal communities may influence sexual risk behaviors. For instance, stressful life events have been shown to be associated with risky behaviors among AI/AN reservation youth (Baldwin, Brown, Wayment, Nez, & Brelsford, 2011). AI/AN communities experience increased levels of stressors compared to the general population, which may magnify sexual risks for AIAN youth (Manson, Beals, Klein, Croy, & The AI-SUPERPFP Team, 2005). Also, limited access to prevention services and programs in tribal communities may likely exacerbate adverse sexual health outcomes among this population. More generally speaking, the sociocultural context of rural environments present unique challenges to adolescents when compared to youth from urban settings (Curtis, Waters, & Brindis, 2011).
Risky sexual behaviors among youth from rural communities, coinciding with barriers to health services, increase the propensity for adverse sexual health outcomes (Curtis et al., 2011). Many AI/AN youth are in low-income rural, or even remote communities. In addition, historical trauma—the loss of land, language, and traditional spiritual ways resulting in intergenerational trauma—is linked with psychological symptoms that may also negatively influence the association between stressful life events and sexual risk-taking among AI/AN youth (Anastario, FourStar, & Rink, 2013). The findings of this review support the salience of precursors to sexual risk for this group, and strongly suggest the relationships of historical context with psychosocial precursors may provide a rich foundation for prevention among AI/AN youth.
Limitations
Criteria included for this review, including a set period for publication inclusion and English-language limited the scope and may have excluded important contributions. Additionally, peer-reviewed articles not indexed in our targeted databases may have been missed. By excluding qualitative research, we may have also excluded important research. Qualitative work could be useful in informing measure development related to precursors to sexual risk-taking among this young age group. In addition, exclusively focusing on individual precursors, we have omitted the influences of external factors such as peers and family on sexual risk-taking.
Conclusions
Our interest was to better understand proximal behavioral and psychosocial precedents of sexual experience and to identify proximal measures to assess the sexual risk for younger ages. This review is a building block in further theoretical and methodological considerations of mediators or other contextual factors influencing sexual risk at young ages.
Acknowledgement:
This research and preparation of this paper were supported by grants T32AA014125 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) and F31DA043342 from the National Institute on Drug Abuse (NIDA) of the US National Institutes of Health. The contents are the sole responsibility of the authors and do not necessarily reflect the views of NIAAA, NIDA, or NIH.
References
- Anastario MP, FourStar K, & Rink E (2013). Sexual risk behavior and symptoms of historical loss in American Indian men. Journal of Community Health, 38(5), 894–899. [DOI] [PubMed] [Google Scholar]
- Bachanas PJ, Morris MK, Lewis-Gess JK, Sarett-Cuasay EJ, Sirl K, Ries JK, & Sawyer MK (2002). Predictors of risky sexual behavior in African American adolescent girls: Implications for prevention interventions. Journal of Pediatric Psychology, 27(6), 519–530. [DOI] [PubMed] [Google Scholar]
- Baldwin JA, Brown BG, Wayment HA, Nez RA, & Brelsford KM (2011). Culture and context: Buffering the relationship between stressful life events and risky behaviors in American Indian youth. Substance Use & Misuse, 46(11), 1380–1394. [DOI] [PubMed] [Google Scholar]
- Bersamin MM, Walker S, Fisher DA, & Grube JW (2006). Correlates of oral sex and vaginal intercourse in early and middle adolescence. Journal of Research on Adolescence, 16(1), 59–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bourdeau B, Grube JW, Bersamin MM, & Fisher DA (2011). The role of beliefs in sexual behavior of adolescents: Development and validation of an adolescent sexual expectancies scale. Journal of Research on Adolescence, 21(3), 639–648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caskey MM, & Anfara VA Jr. (2007). Developmental Characteristics of Young Adolescents: Research Summary. Retrieved from the Association for Middle Level Education website: https://www.amle.org/BrowsebyTopic/WhatsNew/WNDet/TabId/270/ArtMID/888/ArticleID/455/Developmental-Characteristics-of-Young-Adolescents.aspx
- Centers for Disease Control and Prevention, Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. (2015). Sexually transmitted diseases surveillance 2018. Retrieved from https://www.cdc.gov/std/stats18/toc.htm
- Chewning B, Douglas J, Kokotailo PK, LaCourt J, St Clair D, & Wilson D (2001). Protective factors associated with American Indian adolescents’ safer sexual patterns. Maternal and Child Health Journal, 5(4), 273–280. [DOI] [PubMed] [Google Scholar]
- Childs GD, Knight C, & White R (2015). Never-pregnant African American adolescent girls’ perceptions of adolescent pregnancy. Journal of Pediatric Nursing, 30(2), 310–320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coyle KK, Franks H, Glassman J, Walker JD, & Charles VE (2014). Romantic relationships: an important context for HIV/STI and pregnancy prevention programmes with young people. Sex Education, 14(5), 582–596. doi: 10.1080/14681811.2014.931278 [DOI] [Google Scholar]
- Coyle KK, & Glassman JR (2016). Exploring alternative outcome measures to improve pregnancy prevention programming in younger adolescents. American Journal of Public Health, 106(S1), S20–S22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coyle KK, Kirby DB, Marín BV, Gómez CA, & Gregorich SE (2004). Draw the line/respect the line: A randomized trial of a middle school intervention to reduce sexual risk behaviors. American Journal of Public Health, 94(5), 843–851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis AC, Waters CM, & Brindis C (2011). Rural adolescent health: The importance of prevention services in the rural community. The Journal of Rural Health, 27(1), 60–71. [DOI] [PubMed] [Google Scholar]
- DeRavello L, Everett Jones S, Tulloch S, Taylor M, & Doshi S (2014). Substance use and sexual risk behaviors among American Indian and Alaska Native high school students. Journal of School Health, 84(1), 25–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiClemente RJ, Crittenden CP, Rose E, Sales JM, Wingood GM, Crosby RA, & Salazar LF (2008). Psychosocial predictors of HIV-associated sexual behaviors and the efficacy of prevention interventions in adolescents at-risk for HIV infection: what works and what doesn’t work? Psychosomatic Medicine, 70(5), 598–605. [DOI] [PubMed] [Google Scholar]
- DiIorio C, Dudley WN, Kelly M, Soet JE, Mbwara J, & Potter JS (2001). Social cognitive correlates of sexual experience and condom use among 13-through 15-year-old adolescents. Journal of Adolescent Health, 29(3), 208–216. [DOI] [PubMed] [Google Scholar]
- Dippel EA, Hanson JD, McMahon TR, Griese ER, & Kenyon DB (2017). Applying the theory of reasoned action to understanding teen pregnancy with American Indian communities. Maternal and Child Health Journal, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geske S, Quevillon R, Struckman-Johnson C, & Hansen K (2016). Comparisons of contraceptive use between rural and urban teens. Journal of Pediatric and Adolescent Gynecology, 29(1), 33–41. [DOI] [PubMed] [Google Scholar]
- Guilamo-Ramos V, Jaccard J, Dittus P, Bouris A, Holloway I, & Casillas E (2007). Adolescent expectancies, parent-adolescent communication and intentions to have sexual intercourse among inner-city, middle school youth. Annals of Behavioral Medicine, 34(1), 56–66. [DOI] [PubMed] [Google Scholar]
- Hamilton BE, Osterman MJ, Driscoll AK, & Rossen LM (2018). Births: Provisional data for 2017. National vital statistics reports; report no 004. Hyattsville, MD:National Center for Health Statitics. 2018. [Google Scholar]
- Hamilton DT, & Morris M (2015). The racial disparities in STI in the US: Concurrency, STI prevalence, and heterogeneity in partner selection. Epidemics, 11, 56–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harling G, Subramanian S, Bärnighausen T, & Kawachi I (2013). Socioeconomic disparities in sexually transmitted infections among young adults in the United States: examining the interaction between income and race/ethnicity. Sexually Transmitted Diseases, 40(7), 575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffman SD (2013). Counting it up: The public costs of teen childbearing. Retrieved from the National Campaign to Prevent Teen and Unplanned Pregnancy website: https://powertodecide.org/what-we-do/information/resource-library/counting-it-key-data
- Hoffman SD, & Maynard RA (Eds.). (2008). Kids having kids: Economic costs & social consequences of teen pregnancy. Washington DC: The Urban Insitute. [Google Scholar]
- Holloway IW, Traube DE, Schrager SM, Levine B, Alicea S, Watson JL, McKay MM (2012). The effects of sexual expectancies on early sexualized behavior among urban minority youth. Journal of the Society for Social Work and Research, 3(1), 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson-Motoyama M, Moses M, Kann TK, Mariscal ES, Levy M, Navarro C, & Fite PJ (2016). Parent, teacher, and school stakeholder perspectives on adolescent pregnancy prevention programming for Latino youth. The Journal of Primary Prevention, 37(6), 513–525. [DOI] [PubMed] [Google Scholar]
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Queen B, Thornton J (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67(8), 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman CE, Mitchell T, Beals J, Desserich J, Wheeler C, Keane E, Sedey C (2010). Circle of life: Rationale, design, and baseline results of an HIV prevention intervention among young American Indian adolescents of the Northern Plains. Prevention Science, 11(1), 101–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozhimannil KB, Enns E, Blauer-Peterson C, Farris J, Kahn J, & Kulasingam S (2015). Behavioral and community correlates of adolescent pregnancy and Chlamydia rates in rural counties in Minnesota. Journal of Community Health, 40(3), 493–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manson SM, Beals J, Klein SA, Croy CD, & The AI-SUPERPFP Team. (2005). The social epidemiology of trauma among two American Indian reservation populations. American Journal of Public Health, 95, 851–859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathews C, Aarø LE, Flisher AJ, Mukoma W, Wubs AG, & Schaalma H (2008). Predictors of early first sexual intercourse among adolescents in Cape Town, South Africa. Health Education Research, 24(1), 1–10. [DOI] [PubMed] [Google Scholar]
- O’Donnell DA, Schwab-Stone ME, & Muyeed AZ (2002). Multidimensional resilience in urban children exposed to community violence. Child Development, 28, 2–11. [DOI] [PubMed] [Google Scholar]
- O’Donnell L, Myint-U A, O’Donnell CR, & Stueve A (2003). Long-term influence of sexual norms and attitudes on timing of sexual initiation among urban minority youth. Journal of School Health, 73(2), 68–75. [DOI] [PubMed] [Google Scholar]
- O’Sullivan LF, Cheng MM, Harris KM, & Brooks-Gunn J (2007). I wanna hold your hand: the progression of social, romantic and sexual events in adolescent relationships. Perspectives on Sexual and Reproductive Health, 39(2), 100–107. doi: 10.1363/3910007 [DOI] [PubMed] [Google Scholar]
- Pedlow CT, & Carey MP (2004). Developmentally appropriate sexual risk reduction interventions for adolescents: Rationale, review of interventions, and recommendations for research and practice. Annals of Behavioral Medicine, 27(3), 172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quine S, Bernard D, Booth M, Kang M, Usherwood T, Alperstein G, & Bennett D (2003). Health and access issues among Australian adolescents: a rural-urban comparison. Rural and Remote Health, 3(4), 245. [PubMed] [Google Scholar]
- Rolf J, Baldwin J, Trotter R, Alexander D, Denetsosie R, Tongue N, Johnson J (1991, June). AIDS prevention of youth of rural Native American tribes. Paper presented at the International Conference of AIDS. [Google Scholar]
- Santelli JS, Kaiser J, Hirsch L, Radosh A, Simkin L, & Middlestadt S (2004). Initiation of sexual intercourse among middle school adolescents: The influence of psychosocial factors. Journal of Adolescent Health, 34(3), 200–208. [DOI] [PubMed] [Google Scholar]
- Seth P, Lang DL, DiClemente RJ, Braxton ND, Crosby RA, Brown LK, … Donenberg GR (2012). Gender differences in sexual risk behaviours and sexually transmissible infections among adolescents in mental health treatment. Sexual Health, 9(3), 240–246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shegog R, Rushing SC, Gorman G, Jessen C, Torres J, Lane TL, Peskin MF (2017). NATIVE-It’s your game: Adapting a technology-based sexual health curriculum for American Indian and Alaska Native youth. The Journal of Primary Prevention, 38(1-2), 27–48. [DOI] [PubMed] [Google Scholar]
- Siegel DM, Aten MJ, & Enaharo M (2001). Long-term effects of a middle school–and high school–based human immunodeficiency virus sexual risk prevention intervention. Archives of Pediatrics & Adolescent Medicine, 155(10), 1117–1126. [DOI] [PubMed] [Google Scholar]
- Steinberg L (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74. doi: 10.1016/j.tics.2004.12.005 [DOI] [PubMed] [Google Scholar]
- Steinberg L (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74. [DOI] [PubMed] [Google Scholar]
- Steinberg L, & Morris AS (2001). Adolescent development. Annual Review of Psychology, 52(1), 83–110. [DOI] [PubMed] [Google Scholar]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Weeks L (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. [DOI] [PubMed] [Google Scholar]
- Turner AM, Liddy ED, Bradley J, & Wheatley JA (2005). Modeling public health interventions for improved access to the gray literature. Journal of the Medical Library Association, 93(4), 487. [PMC free article] [PubMed] [Google Scholar]