

Abstract
Low-income parents are more likely to have a child with disruptive behaviors. Furthermore, these parents are likely to struggle with low expectations about the future, which can interfere with treatment response to even the most effective treatments. The purpose of this study was to explore correlates of low-income parents’ expectations, specifically hopelessness and optimism, in families with clinic-referred disruptive young children. Using baseline data from an intervention trial (Jones et al., 2021), we used a multi-informant approach to test whether parenting behaviors, child misbehavior, and parental daily stressors were related to parent hopelessness and optimism. Results based on the Everyday Stress Index indicated that only daily stressors, particularly those related to relationships and responsibilities, were related to parent feelings of hopelessness and optimism. Results were interpreted through transactional and ecological systems theories, particularly the Family Stress Model (Conger & Conger, 2002), as well as a low-income parent’s self-efficacy as a caregiver. Clinical implications are discussed.
Keywords: Child disruptive behaviors, Parent expectations, Low income, Stress, Parenting
Across the large, diverse population of low-income families, parents and young children are at-risk of poor physical and psychological outcomes (Brooks-Gunn & Duncan, 1997; Chaudry & Wimer, 2016; Scaramella et al., 2008; Sullivan et al., 2019, 2021), including child disruptive behaviors (Jones et al., 2016). Importantly, parent coping skills and their children’s developmental trajectories vary widely across families with limited resources (Hustedt et al., 2017). Offering insight into this variability are parent expectations. Some parents appear to have more positive expectations, including elevated levels of optimism and hope, and these positive expectations appear to translate to better parenting (Baker et al., 2005; Kashdan et al., 2002; Loh et al., 2017) and child well-being (Jones et al., 2002). Accordingly, parents who endorse higher levels of pessimism and hopelessness appear to be at-risk of poor parent and child-level problems. A systems-wide view of the complex transactions between parenting, child behavior, and stress may offer insight into what contributes to parent expectations.
The purpose of this study is to identify potential factors that are related to parent expectations in an at-risk, treatment-seeking sample of low-income families in a secondary analysis of baseline data originally collected in the context of an intervention trial (Jones et al., 2021). First, we outline how behaviors specific to parents, children, and their dyadic relationship are related to parental expectations, drawing from Bronfenbrenner’s (1977) ecological and Sameroff’s (1975) transactional theories. Then, we discuss specific expectations pertinent to low income, treatment-seeking families, as well as how such expectations may promote or impair treatment response. We hypothesized that constructs at each proposed system level (i.e., parent, child, and parent-child) will relate to parent expectations in a low income sample of parents seeking treatment for disruptive behavior in their young children.
A Transactional and Ecological Perspective on Parent Expectations
Parental expectations are likely contingent on activity across multiple different systems; parenting practices, child behavior, and external stress all play a role in the degree to which a parent is hopeful or optimistic. Bronfenbrenner (1977) originally proposed an ecological systems model wherein child development is a function of a series of interlocking contexts that vary from proximal to increasingly distal. Evolution of this theory, however, focused on the importance of “enduring forms of interaction” in shaping a child’s developmental trajectory (Bronfenbrenner & Morris, 1998, p 996). Sameroff’s (1975) seminal work complements Bronfenbrenner’s, arguing that actors in each of these systems influence the others. Taken together, processes that spur development forward are transactional and reciprocal, shaping both parent and child as they unfold. Parent-child interactions constitute one such process, and these interactions are particularly important for young children. For example, a parent may praise a child for being calm, resulting in a more even-keeled parent and a child who is more likely to engage in future calm behavior. In disruptive young children, two ways of measuring the quality of parent-child interactions are child misbehavior and parenting skills. Therefore, it is important to consider both child and parent characteristics separately, as well as behaviors and factors that link the two within a family context (e.g., stress, parenting).
In addition to parent-child interactions, Belsky (1984) highlights the critical role contextual stress plays in shaping parenting and parent expectations. Low-income parents raising a child with disruptive behavior problems are doubly at-risk. First, parents cope with stress specifically related to financial strains, including poorer living conditions and higher degrees of family instability (Evans, 2004). Second, regardless of socioeconomic status, parents of children with disruptive behavior problems report higher levels of parenting stress and family conflict than parents of non-clinic referred children (Deault, 2010; Theule et al., 2013). Coupled together, caring for a child with disruptive behaviors in the context of financial strain and associated stressors likely influences the way parents think about themselves, the world, and their parenting, translating to negative expectations.
Parental Expectations in Treatment-Seeking Families
Parental expectations are particularly critical in the context of treatment-seeking families. Behavioral Parent Training (BPT), which involves both the child and the parent as the agents of treatment, is one of the most effective evidence-based treatments for promoting child and family well-being; Comer et al., 2013; Evans et al., 2013; Higa-McMillan et al., 2016; Stoll et al., 2020). Further, recent evidence suggests BPT may be just as effective for low income families relative to families with more resources (e.g., Dedousis-Wallace et al., 2020). This effect is heartening, given that children from low income families are more likely to struggle with disruptive behavior disorders (Jones et al., 2016). However, families who are socially disadvantaged are more likely to encounter obstacles (e.g., difficulty accessing a clinic, concerns about stigma) resulting in attrition and poor engagement (Chacko et al., 2016; Jones et al., 2021; Nock & Kazdin, 2005), which may result in poor treatment response (Lundahl et al., 2006; Leijten et al., 2013; Reyno & McGrath, 2006). Accordingly, better understanding factors related to parent engagement is critical in enrolling and retaining underserved families in BPT programs–a necessary step along the path toward equitable access to evidence-based psychological services.
Research supports the role of parental expectations in explaining some of the variability in therapy outcome (e.g., Jiang et al., 2016; Kaiser et al., 2010). For example, a parent with negative expectations may view their parenting and their child’s behavior as uncontrollable and immutable, disadvantaging them from a positive outcome, before even beginning their first treatment session (Durand et al., 2009). Current treatment engagement literature focuses on parental attributions about child behavior, despite theoretical models highlighting the importance of more global parent cognitions (Pereira & Barros, 2019). Accordingly, understanding what contributes to low-income parents’ global positive and negative expectations may translate to more effective intervention among this group of underserved families.
Two contrasting, albeit related, indicators of parental expectations are hopelessness and optimism (Chang et al., 1994; Kashdan et al., 2002). Parent hopelessness, which is the anticipation of bad outcomes, engenders a sense of helplessness to control outcomes (Abramson et al., 1989; Cohen et al., 2017). In contrast to hopelessness, optimism describes a positive outlook on the future. Recent research suggests optimism is socially patterned, with people of higher socioeconomic status being more likely to report more optimistic frameworks (Boehm et al., 2015). Parental optimism is associated with more effective parenting (Jones et al., 2002), particularly when parents contend with children with disruptive behaviors (Koenig et al., 2010), and with improved long-term child behavior (Durand et al., 2009). When parenting in multiply-stressed families, such as those with low incomes and disruptive children, hopelessness may prevent, while optimism may promote, engaging with and benefiting from evidence-based treatment.
The Current Study
In a sample of families with clinic-referred disruptive young children, the purpose of this study was to explore correlates of low-income parents’ expectations, specifically hopelessness and optimism. The current study drew from Bronfenbrenner’s (i.e., Bronfenbrenner & Morris, 2006) bioecological systems model to theorize how three constructs central to child and parent well-being relate to parenting expectations: child misbehavior, parenting, and daily stressors. We hypothesized that, after accounting for child and parent demographics, parenting, child behavior, and daily stressors would each explain variability in parent expectations hopelessness and optimism. Specifically, we expected that higher levels of negative parenting, child problem behaviors, and daily stressors, as well as lower levels of positive parenting, would relate to more hopelessness and less optimism.
Our operationalization of study constructs stems from the following rationale. As parents were seeking support for child disruptive behavior, we specifically measured this type of child behavior (McMahon & Forehand, 2003). We assessed both positive and negative parenting practices, as parents responded to recruitment materials to enhance their caregiving skills, and, in turn, their child’s behavior. We used both parent self-report and behavioral observations of parent-child interactions to comprehensively assess parenting, given data suggesting observations of parenting are particularly important when studying low-income families (Herbers et al., 2017). We assessed daily stressors using parent perceptions of stress, which have been reported to be better indicators than more objective measures (e.g., income) (Hustedt et al., 2017). As low-income families cope with a wide variety of stressors, we drew from previous research to evaluate two specific facets of daily stress: 1) coping with hardship (i.e., material and financial) and 2) managing relationships and responsibilities.
Method
The current study is a secondary data analysis of baseline data from a project examining strategies to increase engagement in BPT (Jones et al., 2021). The IRB approved all study procedures.
Participants
One hundred and one low-income (100–250% of Federal Poverty Guidelines) parents and their 3-to-8 year old child with clinically significant disruptive behaviors (Eyberg Child Behavior Inventory Problem score > 15 or Intensity score > 131; Eyberg & Pincus, 1999) constituted the original sample (Jones et al., 2021). Approximately 80% of these families had applied for government assistance (e.g., Medicaid, unemployment benefits, Food Stamps) in the last year. Exclusion criteria included the presence of parental child abuse/neglect, significant developmental delays of the child, and current parental psychotic or substance use disorders. Parents were also excluded if they met diagnostic criteria for a current depressive episode as defined by meeting criteria for a Major Depressive Episode on the Mini International Neuropsychiatric Interview (Sheehan et al., 1998) and had a score indicating a severe depressive episode (score > 27) on the Beck Depression Inventory (Beck et al., 1996).1 The demographic characteristics of the sample are presented under Child and Parent Characteristics in Table 1 (see Results section).
Table 1.
How Demographics and Processes Relate to Parent Expectations: Hopelessness and Optimism
| Correlating With | |||||
|---|---|---|---|---|---|
|
|
|||||
| Systems | M / % | SD | Range | Hopelessness | Optimism |
| Child Characteristics | |||||
| % female (1 =girl; 0=boy) | 44% | −.07 | .03 | ||
| Age (years) | 4.61 | 1.27 | 2.92–7.83 | .03 | .08 |
| Parent Characteristics | |||||
| Age (years) | 31.91 | 6.02 | 20–48 | −.08 | .15 |
| % female | 93.8% | −.08 | .04 | ||
| % Underrepresented | 34% | .02 | .15 | ||
| Race: | |||||
| Black or African American | 20% | ||||
| White | 69.8% | ||||
| American Indian or Alaskan Native | 1% | ||||
| More than one race | 8.3% | ||||
| Ethnicity: | |||||
| Not Hispanic/Latino | 93.8% | ||||
| Hispanic/Latino | 6.3% | ||||
| Education: | |||||
| High school or less | 8% | .03 | −.14 | ||
| Some college or vocational training | 28% | −.13 | .01 | ||
| College | 47% | .08 | .03 | ||
| Advanced degree | 17% | .03 | .06 | ||
| Parenting | |||||
| Positive | |||||
| Observed attends & rewards per min. | 1.06 | .86 | 0–4.14 | .18† | −.09 |
| Parent report1 | 49.72 | 5.70 | 36–60 | −.11 | −.03 |
| Negative | |||||
| Observed questions & instructions per min. | 3.97 | 1.95 | .79–10.22 | .02 | −.06 |
| Parent report1 | 17.38 | 3.89 | 9–27 | .05 | −.04 |
| Child Behavior | |||||
| Number of problems2 | 22.94 | 6.19 | 4–36 | .04 | .11 |
| Intensity of problems2 | 153.14 | 28.80 | 103–232 | .06 | .08 |
| Daily Stressors | 21–63 | .52* | −.31** | ||
| Hardship | .46** | −.23* | |||
| Responsibilities/Relationships | .52** | −.28** | |||
Note:
p < .001;
p = .002;
p = .08;
= Alabama Parenting Scale (Shelton et al., 1996);
= Eyberg Child Behavior Inventory (Eyberg & Pincus, 1999);
= Everyday Stressors Index (Hall et al., 1985, Hall, 1987; Hall et al., 1985)
Procedure
Families were recruited via word-of-mouth, local schools, and advertisements targeting areas (e.g., workplaces, retail outlets, & social media) with an overrepresentation of low-income parents. In addition, social service, health care, and other agencies that serve low-income families (see Jones et al., 2021, for details) were targeted for recruitment. Advertisements used phrasing such as “does your child test your limits?”, “are you having trouble finding or paying for services?”, and “get free help managing your child’s behavior” to attract low-income families with children with elevated disruptive behaviors.
Interested parents contacted a project research assistant. The research assistant then conducted a phone screen to assess key eligibility criteria. Eligible families were then invited to an in-person interview to obtain consent, confirm eligibility, and complete self-report measures. The behavioral observation task was conducted at the beginning of the next session.
Measures
Parent & Child Demographics
The parent completed a measure of demographic information about themselves (e.g., age, gender, education), the participating child (e.g., age, gender), and their family (e.g., household income).
Parenting Practices
We used behavioral observations and self-report data to assess parenting. Behavioral observations of both positive and negative parenting occurred during a parent-child clinic observation (i.e., Child’s Game) which averaged five minutes (see McMahon & Forehand, 2003). In the context of child-directed play (i.e., the Child’s Game), parental verbalizations, such as questions and instructions, detract from the focus on the child and developing positive, reinforcing interactions, whereas praise, rewards, and close attention to the child’s appropriate behavior promote the development of positive parent-child interactions (McMahon & Forehand, 2003). To capture this dynamic, four behaviors were recorded: (a) Attends (positive attention in which the parent provides an ongoing verbal description of what the child is doing; e.g., “You are stacking the blocks”), (b) Rewards (positive attention that is provided following the child’s appropriate behavior; e.g., “Good job!” “Thank you for picking up your toys!”), (c) Questions (an interrogation to which the only appropriate response is verbal), and (d) Instructions (parent-issued command toward the child). Attends and Rewards are considered “Do” Behaviors (positive behaviors to increase) and thus a facet of positive parenting, whereas Questions and Instructions in this context are labeled as “Don’t” Behaviors (negative behaviors to decrease) and associated with unhelpful (i.e., negative) parenting (Bell & Eyberg, 2002).
Undergraduate research assistants assessed parenting behaviors from videotapes of the parent-child interactions. The coders received approximately 50 hours of training. Prior to beginning coding, undergraduate research assistants reached at least 80% agreement with expert coders on a series of training parent-child observation videos.
More than half (51%) of the videos were double coded for fidelity. When two coders failed to reach 80% agreement, they met in person and jointly coded the observation, resolving outstanding discrepancies. This occurred in 45% of the observations (agreement prior to resolving discrepancies was 70% for Attends + Rewards and 80% for Instructions + Questions). We used the resolved discrepancy scores in these analyses, effectively resulting in data with 100% agreement across coders. Behaviors are reported as a rate per minute to account for variability in interaction length.
Parents completed an abbreviated version of the Alabama Parenting Questionnaire (APQ), a self-reported measure of positive and negative parenting practices (Shelton et al., 1996). Numerous studies have since examined the APQ (e.g., Clerkin et al., 2007; Essau et al., 2006), and reported adequate reliability and validity data. Of relevance, Clerkin et al. (2007) examined the psychometric properties of the APQ in a preschool population. A three-factor solution emerged with the following factors: positive parenting, negative/inconsistent parenting, and punitive parenting. In the current study, we used the 12-item Positive Parenting subscale (e.g., You play games and do other fun things with your child; α =.81) and the seven-item Negative Parenting subscale (e.g., You threaten to punish your child and then do not actually punish him/her; α = .63). Items pertaining to punitive parenting were left out of the current study due to IRB restrictions.
Child Behavior Problems
We operationalized disruptive behavior using the quantity and intensity of problem behaviors parents endorsed on the Eyberg Child Behavior Inventory (ECBI) (Eyberg & Pincus, 1999). On this form, parents indicate whether a behavior (e.g., whining, yelling or screaming) is currently a problem, and, if so, the intensity of the behavior or how often it occurs using a Likert scale ranging from 1 (never) to 7 (always). Problem scores range from 0 to 36 and intensity scores range from 36 to 252. The ECBI has adequate reliability and validity data (Eyberg & Pincus, 1999). In this sample, reliability estimates were α = .85 for the problem subscale and α = .91 for the intensity scale.
Daily Stressors
Parents reported on their experiences of stress using the Everyday Stressors Index (ESI) (Hall, 1983, 1987; Hall et al., 1985). This instrument consists of 20 items assessing how much (ranging from [1] not at all to [4] bothered a great deal) a variety of stressors bother each parent (example item: “How much are you bothered by having too many responsibilities?”). Scores range from 20 to 80 with higher scores indicating more stress. The measure has adequate reliability and validity data (e.g., Hall et al., 1985). The alpha coefficient for the current sample was α = .85.
Parent Expectations
We operationalized expectations using two scales: the Beck Hopelessness Scale (BHS; Beck & Steer, 1990; Beck et al., 1974) and the Life Orientation Test – Revised (LOTR; Scheier et al., 1994). The BHS uses 20 items to assess hopelessness. Each item presents a statement (e.g., I don’t expect to get what I really want) to which a parent indicates True or False. The BHS has substantial reliability and validity data (e.g., Beck et al., 1974; Innamorati et al., 2013). In this study, we generated a total score, with a possible range of 0 to 20 (α = .86). Higher scores indicated higher levels of hopelessness.
The LOT-R assessed how optimistic parents felt. Parents rate the extent to which, from 0 (strongly disagree) to 4 (strongly agree), they agree with each of 6 statements (e.g., In uncertain times, I usually expect the best). This measure has substantial reliability and validity data (e.g., Scheier et al., 1994; Solberg Nes et al., 2009) (for current sample α = .74). Higher scores represent more optimism.
Results
Data Analytic Plan
First, we conducted preliminary analyses to evaluate normality, examine the extent and mechanism of missing data, and characterize the sample of parents. We then ran bivariate correlations of each independent variable with the two indicators of expectations to assess which variables were related to optimism and hopelessness. Next, we conducted two, five-block hierarchical regression analyses in SPSS to examine the relationship of parenting, child disruptive behavior, and daily stressors with caregiver expectations after controlling for child and parent demographics. We bootstrapped results 5000 times and report robust standard errors to account for skew. In the first block, we entered the child characteristics age and gender. In the second block, we created four different binary variables to represent parent education level (high school or less, some college, college, and advanced degree). We then entered dummy-coded parent education level and a binary underrepresented status variable which indicated whether or not the parent identified as Hispanic, Latino, White, Black, Native American or Alaskan Native, or more than one race. We created a binary variable (White vs. Underrepresented Minority) given that the overall prevalence of each unique ethnic or racial category was small. In the third block, we entered self-reported and observations of parenting behavior. In the fourth block, we entered parent reports of the number and intensity of child problem behaviors. Finally, in the fifth block, we included factor scores (i.e., hardship and relationships/responsibilities) representing parent reports of stress derived from the ESI (Hall, 1983, 1987; Hall et al., 1985).
Preliminary Analyses
Data inspection indicated one outlier which we eliminated from analyses.2 From the remaining sample (n = 100), one parent did not report race or ethnicity, and three were missing behavioral observation data due to video recording malfunctioning, resulting in 96 complete cases. All four missing cases identified as female and Non-Hispanic. Two identified as Black, one opted out of reporting race, and one was White. We elected to use listwise deletion, given research suggesting that cases representing fewer than 5 % of the sample are unlikely to bias findings (Graham, 2009).
The means (or percentages for categorical variables), standard deviations, and observed range of each independent variable for complete cases are presented in Table 1. Of note, slightly less than half of the children were female. About one-third of parents identified as an underrepresented minority with the great majority of participating parents being female. Behavioral observations of parenting indicated the “Don’t” (negative) behaviors occurred at a rate over 3.7 times higher than “Do” (positive) behaviors. In contrast, parents self-reported that positive parenting behaviors occurred substantially more frequently, with a positive parenting item-level mean equaling 4.14 on a one to five scale, than negative parenting behavior, with a negative parenting item-level mean equaling 2.48. On average, parents reported the occurrence of almost 23 of the possible 36 child problem behaviors, with average intensity levels well surpassing clinical cutoffs. On average, parents reported being “a little bothered” by everyday stressors (mean item score = 1.75).
Regarding our outcome constructs, on average, parents reported normal levels of hopelessness (M = 2.63, SD = 3.27), with 4 % of the sample endorsing moderate to severe levels of hopelessness (Beck & Steer, 1993). Parents endorsed levels of optimism (M = 21.56, SD = 5.27) consistent with another sample of parents with children with cancer (Fayed et al., 2011). Hopelessness and optimism were moderately negatively correlated (r[94] = −.50, p < .001).
Recent research with the ESI suggests reliable and valid factors exist within this measure (Damron, 2016; Gissandaner et al., 2021). Thus, building from factors previous researchers have identified (i.e., Damron, 2016; Gissandaner et al., 2021), we conducted a confirmatory factor analysis to identify factors which may differentially relate to our two outcomes.
The factor measurement model of the ESI indicated two factors, moderately correlated, with six and eight items loading on the first and second factors, respectively (χ2 [74] = 76.54, p = .40, RMSEA = .019, 90% CI [.000, .061], CFI = .991, SRMR = .065, r [94] = .68, p < .001). Like previous research (Damron, 2016; Gissandaner et al., 2021), we labeled these factors as Hardship and Relationship/Responsibility, respectively. The Hardship factor assesses the extent to which parents lack resources to meet their basic needs (e.g., I have problems with having not enough money for basic necessities such as clothing, housing, food, and health care), and the Relationships/Responsibilities factor assesses how much stress results from interpersonal challenges and overwhelming daily responsibilities (e.g., I have too many responsibilities). Standardized item loadings ranged from .55 to .85 for the Hardship factor and .29 to .64 for the Relationships/Responsibilities factor.
What Constructs Relate to Parent Expectations?
Correlations between each independent and dependent variable (hopelessness & optimism) are also reported in Table 1. Daily stressors was the only variable correlated with hopelessness and optimism. In partial support of study hypotheses, as parents reported increased levels of stress, both in relation to material hardship as well as stress due to responsibilities and relationships, hopelessness increased and optimism decreased. Neither child characteristics, parent characteristics, parenting, nor child behavior was related to hopelessness or optimism.
Fig. 1 summarizes the results of the two hierarchical regression analyses for the three constructs of interest: parent behavior, child behavior, and daily stress. Congruent with the correlational analyses, regression steps including child characteristics,3 parent characteristics3, child behavior, and parenting behavior did not explain variance in hopelessness or optimism (p values for all F Δ statistics > .20). Only the fifth block, in which we entered factor scores for the Hardship and Relationships/Responsibilities factors (McNeish & Wolf, 2020), explained variance in hopelessness (R2 = .35, R2 Δ = .28, F Δ [2, 81] = 17.24, p < .001) and optimism (R2 = .20, R2 Δ = .13, F Δ [2, 81] = 6.64, p = .002).4 As presented in Table 2, parents’ self-reported stress falling under the Hardship factor was unrelated to either hopelessness or optimism; however, increased stress falling under the Relationship/Responsibilities factor was related to significantly higher levels of hopelessness and lower levels of optimism.
Fig. 1.
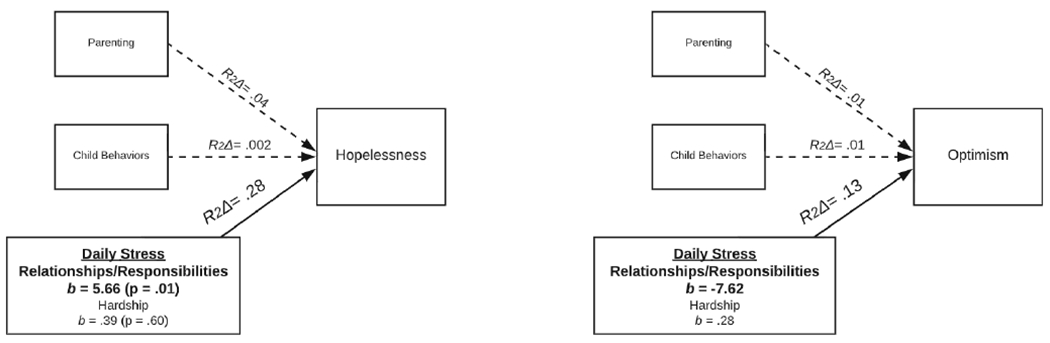
The Relationship of Each Block of Independent Variables with Hopelessness and Optimism after Controlling for Child and Parent Demographic Characteristics. Note: Solid lines indicate that R2 Δ was significant at p ≤ .002. Under the Daily Stress block, only the Relationships/Responsibilities factor was significantly related to outcomes
Table 2.
Final block of hierarchical regressions for outcomes hopelessness and optimism
| Outcome | Predictor | b | BCa 95% CI |
|---|---|---|---|
| Hopelessness | Child age | .28 | [−.21, .82] |
| Child gender | −.62 | [−2.08, .64] | |
| Parent education | |||
| High school or less | −.93 | [−3.37, 1.22] | |
| Some college or vocational school | −1.34 | [−2.86, .09] | |
| College or further | −1.12 | [−3.24, 1.18] | |
| Parent minority status | −.45 | [−1.80, 1.07] | |
| Positive parenting | |||
| Observed attends & rewards per min. | .47 | [−.50, 1.38] | |
| Parent report | .04 | [−.06, .13] | |
| Negative parenting | |||
| Observed questions & instructions per min. | .01 | [−.33, .36] | |
| Parent report | .003 | [−.12, .13] | |
| Child behavior | |||
| Number of problems | −.11 | [−.25, .03] | |
| Intensity of problems | .003 | [−.02, .03] | |
| Daily Stressors | |||
| Hardship | .39 | [−1.01, 2.13] | |
| Relationships/responsibilities | 5.66 | [2.36, 9.19] | |
| Optimism | Child age | −.06 | [−1.04, .92] |
| Child gender | .98 | [−1.18, 3.19] | |
| Parent education | |||
| High school or less | −1.42 | [−5.91, 3.59] | |
| Some college or vocational school | .34 | [−2.71, 3.21] | |
| College or further | 1.94 | [−.94, 4.51] | |
| Parent minority status | 2.15 | [−.29, 4.30] | |
| Positive parenting | |||
| Observed attends & rewards per min. | −.40 | [−1.74, 1.09] | |
| Parent report | −.12 | [−.35, .08] | |
| Negative parenting | |||
| Observed questions & instructions per min. | −.05 | [−.76, .69] | |
| Parent report | −.05 | [−.36, .23] | |
| Child behavior | |||
| Number of problems | .20 | [−.18, .55] | |
| Intensity of problems | −.001 | [−.07, .06] | |
| Daily Stressors | |||
| Hardship | .28 | [−2.40, 2.91] | |
| Relationships/responsibilities | −7.62 | [−13.10, −2.55] |
NOTE: bs are unstandardized; BCa = bias-corrected and accelerated; bolded text indicates p < .01
Discussion
In partial support of study hypotheses, findings suggested that daily stressors, specifically those pertaining to parent responsibilities and relationships, were related to parental expectations of hopelessness and optimism. Unexpectedly, after accounting for child and parent demographic factors, neither parenting skills nor child misbehavior, indicators of parent-child interactions, were associated with parent expectations. Further, stress related to financial hardship was unrelated to parent expectations.
We were surprised to find neither parenting nor child misbehavior was associated with parenting expectations, particularly as our sample consisted of parents seeking skills to better manage their child’s misbehavior. At the time of seeking treatment, it may be the case parents were less concerned about their parenting skills and severity of child misbehavior as they were actively involved in seeking support for ameliorating these specific factors. Parents are more likely to consider their child’s misbehavior as less problematic when they are receiving treatment (Johnston & Leung, 2001). Whereas parents may feel more in control of their parenting and child’s behavior, they likely still feel powerless over other stressors outside of the scope of treatment.
In line with hypotheses, parental day-to-day stress was related to parent expectations. Given the current sample of financially-strained families, we were surprised to find that only stress attributed to having too many responsibilities and too few or strained relationships, and not financial hardship, was related to hopelessness and optimism. However, for low-income families, stress may be the largest factor in determining parental hope and optimism. In contrast, parenting and child behavior may be secondary to the daily stressors of too much responsibility and insufficiently supportive relationships.
Transactional and ecological systems theories (e.g., Family Stress Model; Conger & Conger, 2002) undergird the well-established link between stress, parenting, and child behavior problems, particularly for low-income families; however, in theories such as the Family Stress Model, economic pressure and poor parental well-being are first in the chain of factors predicting poor child well-being. Whereas our use of cross-sectional data precludes examination of the sequential contributions of the independent variables we examined, evidence from the Family Stress Model provides a theoretical framework for conceptualizing their respective order. Accordingly, parenting and child problem behaviors may only contribute to expectations in the context of daily stress.
Still unclear, however, is why does stress attributed to many roles, responsibilities, and strained relationships account for variance in parental expectations, where stress attributed to final hardship does not? One aspect of this factor, strained relationships, may indicate that limited social support among low income parents of children with disruptive behaviors contributes to low parental expectations. Perceived social support is a well-documented resilience promoting factor among low-income mothers (Taylor & Conger, 2017). When systems of welfare underperform, informal social networks may provide material support when unexpected financial challenges arise (e.g., being able to borrow a friend’s car if unexpected car trouble arises, watching a friend’s child in the event of a last-minute work issue; Radey, 2018; Wadsworth, 2012). In addition to tangible aid, supportive relationships function as a coping resource for all persons, particularly those coping with stress associated with living near poverty. For instance, romantic partners can provide comfort in the context of economic pressure (Conger et al., 1999). Given the critical role supportive social networks play in the well-being of low-income families, stress in this domain may be particularly disheartening.
The literature on a construct closely related to hopelessness and optimism, parenting self-efficacy (i.e., a parent’s belief in their ability to effectively serve as a caregiver), may also offer some insight (refer to Rand, 2018 for a detailed explanation on the similarities and differences between these three constructs). Conceptually, parent self-efficacy appears to be closely tied to managing many responsibilities and having positive adult relationships. When responsibilities and relationships become overwhelming, parent self-efficacy decreases, potentially leading to poor parental and child adjustment (Albanese et al., 2019). Parents of children with disruptive behavior problems report higher levels of parenting stress and family conflict than parents of non-clinic referred children (Deault, 2010; Theule et al., 2013), and this higher level of stress relates to lower parenting self-efficacy (Jones & Prinz, 2005). As such, parents coping with elevated stress who perceive themselves as less able to fulfill their caregiver role are likely to feel less optimistic and more hopeless, and the stress associated with these concerns may outweigh stress of hardship. Finally, it is important to note that we assessed financial strain in low income families only; financial strain may emerge as a significant contributor to parental expectations in a sample of families spanning a broader range of incomes.
Limitations and Strengths
Several limitations characterized this study. Overall, hopelessness scores were low, and thus identifying a signal between potential factors and hopelessness may have been more difficult. Importantly, however, such low scores are promising from a clinical perspective, indicating that parents seeking treatment had some hope that future well-being could be better. Indeed, we anticipate the scale of study findings to only increase in an at-risk but non-treatment seeking sample, as treatment-seeking families may inherently evidence higher levels of hope, motivation, and optimism. Cross-sectional data preclude forming firm conclusions on causality and direction of effects. Additionally, one construct that we did not assess that may help explain the findings: parenting self-efficacy. Further, whereas families in this sample were low income, few met criteria for being in poverty (<100% Federal Poverty Line) and a relatively large percent reported college-level educations. Future research with a higher-risk sample of families (e.g., meet federal guidelines for poverty) should attempt to replicate these findings. Finally, there was a high degree of racial and ethnic variability both between and within families, which, in conjunction with our modest sample size, provided insufficient power to analyze whether race or ethnicity was related to parent expectations. As experiences of discrimination may be related to increased levels of hopelessness and decreased feelings of optimism for parents in various contexts, it may be the case that families who are Black, Indigenous, and people of color experienced higher levels of negative expectations than other families from non-marginalized racial and ethnic groups. Future research focusing on the relationship between discrimination and parent expectations is necessary.
This study also has several strengths. First, it is one of few studies to examine hopelessness and optimism in a sample of treatment seeking low-income families who are at-risk for child problem behavior yet underserved. Extant research on parent expectations largely consists of middle-class, White samples. As low socioeconomic status is related to negative parent expectations (e.g., Nock & Kazdin, 2001), diminished treatment engagement (Chacko et al., 2016; Jones et al., 2021; Nock & Kazdin, 2005), and possibly poor treatment outcomes (e.g., Leijten et al., 2013), an in-depth examination of these questions in a low-income sample is necessary. Extrapolating from relatively small percentages of low-income families in extant studies is insufficient for understanding the role of parental expectations in these families. Second, we examined multiple potential contributors (parent behavior, child behavior, stress) to parent expectations. Third, we used a multi-informant framework, drawing from self-reported data as well as behavioral observations.
Clinical Implications
Our findings indicate that relationship strain and stress from overwhelming responsibilities link with parent expectations, above and beyond other factors such as parenting and child misbehavior. Especially in a sample of low-income families, parent expectations are an attractive intervention avenue: they are likely much more malleable than other, external factors (i.e., parent income, living conditions; Hoza et al., 2006). As such, sensitive and responsive clinicians attuned to considerations specific to low-income families may benefit from including parental perceptions of stress, particularly those related to their relationships and responsibilities, in their case conceptualizations of disruptive child behavior. Problem solving ways to enhance relationships, and, if possible, reduce responsibilities may be beneficial. Further, parent-based interventions in populations of caregivers dealing with elevated stress may need to include a larger focus on parent coping (see Chronis-Tuscano et al., 2020). For instance, employing cognitive restructuring techniques on unhelpful expectations (e.g., my child’s behavior will never change) may facilitate increased helpful cognitions that build a better basis for connection with the child and effective discipline (e.g., my child has the ability to behave better) (Durand et al., 2013). Parenting treatment may also benefit from including caregiver affect regulation skills, drawing from treatments such as Dialectical Behavioral Therapy (Linehan, 2014) or Acceptance and Commitment Therapy (Hayes et al., 2016). Cognitive restructuring, emotional regulation, and acceptance will all aid in promoting parent cognitive flexibility and openness to change, even while coping with elevated stress levels. Finally, interventions specifically targeting parenting optimism (i.e., Durand’s, 2011 Optimistic Parenting; Durand et al., 2013) may be particularly helpful when individualizing parent training protocols for low-income populations.
Funding
This research was supported by the National Institute of Child Health and Human Development (grant F31HD098825 to A. S.) and the National Institute of Mental Health (R01MH100377 NCT01367847; R21MH113887; ClinicalTrials.gov Identifier: NCT03597789). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Conflicts of Interest Alexandra D. W. Sullivan, Kat L. Wright, Nicole Breslend, April Highlander, Rex Forehand and Deborah J. Jones have no relevant financial or non-financial interests to disclose.
Code Availability Not applicable.
Ethics Approval: Research Involving Human Subjects Institutional IRBs approved all study procedures and materials.
Informed Consent & Consent for Publication Informed consent was obtained from parents. Parents (i.e., legal guardians) provided informed consent for their children.
Experiment Participants Parents provided informed consent for themselves and their children.
Given our aim to better understand parent expectations as they relate to intervention for child disruptive behaviors, we excluded parents who were currently experiencing a depressive or psychotic episode, or who were actively engaging in substance use. The presence of depression, psychosis, or substance abuse in a parent may call for a differing treatment approach that prioritizes individual treatment for the parent (Forehand & Sullivan, 2017).
For this caregiver, observations identified atypically high levels of attends and rewards (>5 SDs above the mean) and atypically low numbers (i.e., zero) of questions and instructions during the parent-child interaction.
We excluded child and parent characteristics from Figure 1 as they were not primary constructs of interest.
Given the low factor loadings of two items on the Relationship/Responsibilities factor, we reran the model with the two lowest loading factors dropped (.29 & .30). Results were consistent with the model including the original items.
Data Availability:
Work with data is ongoing and have thus not yet been deposited. Data are available upon request with approval.
References
- Abramson LY, Metalsky GI, & Alloy LB (1989). Hopelessness depression: A theory-based subtype of depression. Psychological Review, 96(2), 358–372. 10.1037/0033-295X.96.2.358. [DOI] [Google Scholar]
- Albanese AM, Russo GR, & Geller PA (2019). The role of parental self-efficacy in parent and child well-being: A systematic review of associated outcomes. Child: Care, Health and Development, 45(3), 333–363. 10.1111/cch.12661. [DOI] [PubMed] [Google Scholar]
- Baker BL, Blacher J, & Olsson MB (2005). Preschool children with and without developmental delay: Behavior problems, parents’ optimism and well-being. Journal of Intellectual Disability Research, 49(8), 575–590. 10.lll/j.1365-2788.2005.00691.x. [DOI] [PubMed] [Google Scholar]
- Beck AT, & Steer RA (1990). Manual for the Beck anxiety inventory. The Psychological Corporation. [Google Scholar]
- Beck AT, & Steer RA (1993). Manual for the Beck Hopelessness Scale. San Antonio, TX: Psychological Corporation. [Google Scholar]
- Beck AT, Steer RA, & Brown GK (1996). Manual for the Beck depression inventory-II. Psychological Corporation. [Google Scholar]
- Beck AT, Weissman A, Lester D, & Trexler L (1974). The measurement of pessimism: The hopelessness scale. Journal of Consulting and Clinical Psychology, 42, 861–865. 10.1037/h0037562. [DOI] [PubMed] [Google Scholar]
- Bell SK, & Eyberg SM (2002). Parent–child interaction therapy: A dyadic intervention for the treatment of young children with conduct problems. In Vandecreek L & Jackson TL (Eds.), Innovations in clinical practice: A source book (Vol. 20, pp. 57–74). Sarasota: Professional Resource Exchange. [Google Scholar]
- Belsky J (1984). The determinants of parenting: A process model. Child Development, 55, 83–96. 10.2307/1129836. [DOI] [PubMed] [Google Scholar]
- Boehm JK, Chen Y, Williams DR, Ryff C, & Kubzansky LD (2015). Unequally distributed psychological assets: Are there social disparities in optimism, life satisfaction, and positive affect? PLoS One, 10(2), e0118066. 10.1371/joumal.pone.0118066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bronfenbrenner U (1977). Toward an experimental ecology of human development. American Psychologist, 32, 513–531. 10.1037/0003-066X.32.7.513. [DOI] [Google Scholar]
- Bronfenbrenner U, & Morris PA (2006). The Bioecological Model of Human Development. In Lerner RM & Damon W (Eds.), Handbook of child psychology: Theoretical models of human development (p. 793–828). John Wiley & Sons Inc. [Google Scholar]
- Bronfenbrenner U, & Morris PA (1998). The ecology of developmental processes. In Damon W & Lerner RM (Eds.), Handbook of child psychology, Vol. 1: Theoretical models of human development (5th ed., pp. 993–1023). New York: Wiley. [Google Scholar]
- Brooks-Gunn J, & Duncan G (1997). The effects of poverty on children. The Future of Children, 7(2), 55–71. [PubMed] [Google Scholar]
- Chacko A, Jensen SA, Lowry LS, Cornwell M, Chimklis A, Chan E, Lee D, & Pulgarin B (2016). Engagement in Behavioral Parent Training: Review of the literature and implications for practice. Clinical Child and Family Psychology Review, 19(3), 204–215. 10.1007/sl0567-016-0205-2. [DOI] [PubMed] [Google Scholar]
- Chang EC, D’Zurilla TJ, & Maydeu-Olivares A (1994). Assessing the dimensionality of optimism and pessimism using a multimeasure approach. Cognitive Therapy and Research, 18(2), 143–160. 10.1007/BF02357221. [DOI] [Google Scholar]
- Chaudry A & Wimer C (2016). Poverty is not just an indicator: The relationship between income, poverty, and child well-being. Academic Pediatrics, 16(3), 23–29. Poverty is not just an indicator: The relationship between income, poverty, and child well-being. [DOI] [PubMed] [Google Scholar]
- Chronis-Tuscano A, O’Brien K, & Danko CM (2020). Supporting caregivers of children with ADHD: An integrated parenting program, Therapist Guide. Oxford University Press. [Google Scholar]
- Clerkin SM, Marks DJ, Policaro KL, & Halperin JM (2007). Psychometric properties of the Alabama parenting questionnaire-preschool revision. Journal of Clinical Child & Adolescent Psychology, 36, 19–28. 10.1080/15374410709336565. [DOI] [PubMed] [Google Scholar]
- Cohen JR, Tengsche C, Sheshko DM, Chan RCK, Hankin BL, & Abela JRZ (2017). Hopelessness. In Levesque R (Ed.), Encyclopedia of adolescence. Cham: Springer, 10.1007/978-3-319-32132-5_185-2. [DOI] [Google Scholar]
- Comer JS, Chow C, Chan PT, Cooper-Vince C, & Wilson LAS (2013). Psychosocial treatment efficacy for disruptive behavior problems in very young children: A meta- analytic examination. Journal of the American Academy of Child & Adolescent Psychiatry, 52, 26–36. 10.1016/j.jaac.2012.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger RD, & Conger KJ (2002). Resilience in Midwestern families: Selected findings from the first decade of a prospective, longitudinal study. Journal of Marriage and Family, 64(2), 361–373. [Google Scholar]
- Conger RD, Rueter MA, & Elder GH (1999). Couple resilience to economic pressure. Journal of Personality and Social Psychology, 76, 54–71. 10.1037//0022-3514.76.l.54. [DOI] [PubMed] [Google Scholar]
- Damron KR (2016). An examination of maternal stress and second-hand smoke exposure on perinatal smoking status (doctoral dissertation). University of Kentucky. [Google Scholar]
- Deault LC (2010). A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with attention-deficit/hyperactivity disorder (ADHD). Child Psychiatry and Human Development, 41, 168–192. 10.1007/sl0578-009-0159-4. [DOI] [PubMed] [Google Scholar]
- Dedousis-Wallace A, Drysdale SA, McAloon J, & Ollendick TH (2020). Parental and familial predictors and moderators of parent management treatment programs for conduct problems in youth. Clinical Child and Family Psychology Review, 24, 1–28. 10.1007/sl0567-020-00330-4. [DOI] [PubMed] [Google Scholar]
- Durand VM, Hieneman M, Clarke S, & Zona M (2009). Optimistic parenting: Hope and help for parents with challenging children. In Sailor W, Dunlap G, Sugai G, & Homer RH (Eds.), Handbook of positive behavior support (pp. 233–256). New York: Springer. [Google Scholar]
- Durand VM (2011). Optimistic parenting: Hope and help for you and your challenging child. Paul H. Brookes. [Google Scholar]
- Durand VM, Hieneman M, Clarke S, Wang M, & Rinaldi ML (2013). Positive family intervention for severe challenging behavior I: A multisite randomized clinical trial. Journal of Positive Behavior Interventions, 15(3), 133–143. 10.1177/1098300712458324. [DOI] [Google Scholar]
- Essau CA, Sasagawa S, & Frick PJ (2006). Callous-unemotional traits in a community sample of adolescents. Assessment, 13(4), 454–469. 10.1177/1073191106287354. [DOI] [PubMed] [Google Scholar]
- Eyberg S, & Pincus D (1999). Eyberg Child Behavior Inventory & Sutter-Eyberg Student Behavior Inventory- Revised: Professional manual. Psychological Assessment Resources. [Google Scholar]
- Evans GW (2004). The environment of childhood poverty. American Psychologist, 59(2), 77–92. 10.1037/0003-066X.59.2.77. [DOI] [PubMed] [Google Scholar]
- Evans SW, Owens JS, & Bunford N (2013). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 43(4), 527–551. 10.1080/15374416.2013.850700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fayed N, Klassen AF, Dix D, Klaassen R, & Sung L (2011). Exploring predictors of optimism among parents of children with cancer. Psycho-oncology, 20(4), 411–418. [DOI] [PubMed] [Google Scholar]
- Forehand R, & Sullivan AD (2017). Adult psychopathology, parenting, and children: Are there any simple answers? Clinical Psychology: Science and Practice, 24, 389–391. 10.1002/pon.l743. [DOI] [Google Scholar]
- Gissandaner TD, Schmidt AT, Mastergeorge A, Gette JA, & Littlefild AK (2021). Does stress mediate the relation between caregivers’ victimization and child behavioral outcomes? A prospective examination. Child Psychiatry and Human Development, 52, 154–165. 10.1007/sl0578-020-01000-w. [DOI] [PubMed] [Google Scholar]
- Graham JW (2009). Missing data analysis: Making it work in the real world. Annual Review of Psychology, 60, 549–576. 10.1146/annurev.psych.58.110405.085530. [DOI] [PubMed] [Google Scholar]
- Hall LA (1983). Social support, everyday stress, and maternal mental health (unpublished doctoral dissertation) Chapel Hill, NC: University of North Carolina. [Google Scholar]
- Hall LA (1987). Psychometric evaluation of the everyday stressors index (ESI). Unpublished manuscript. [Google Scholar]
- Hall LA, Williams CA, & Greenberg RS (1985). Supports, stressors, and depressive symptoms in low-income mothers of young children. American Journal of Public Health, 75(5), 518522. 10.2105/ajph.75.5.518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes SC, Strosahl KD, & Wilson KG (2016). Acceptance & Commitment Therapy: The process and practice of mindful change (2nd ed.). New York; Guilford. [Google Scholar]
- Herbers JE, Garcia EB, & Obradović J (2017). Parenting assessed by observation versus parent-report: Moderation by parent distress and family socioeconomic status. Journal of Child and Family Studies, 26, 3339–3350. 10.1007/S10826-017-0848-8. [DOI] [Google Scholar]
- Higa-McMillan CK, Francis SE, Rith-Najarian L, & Chopita BF (2016). Evidence base update: 50 years of research on treatment for child and adolescent anxiety. Journal of Clinical Child & Adolescent Psychology, 45, 91–113. 10.1080/15374416.2015.1046177. [DOI] [PubMed] [Google Scholar]
- Hoza B, Johnston C, Pillow DR, & Ascough JC (2006). Predicting treatment response for childhood attention-deficit/hyperactivity disorder: Introduction of a heuristic model to guide research. Applied and Preventive Psychology, 11(4), 215–229. 10.1016/j.appsy.2005.11.001. [DOI] [Google Scholar]
- Hustedt JT, Vu JA, Bargreen KN, Hallam RA, & Han M (2017). Early head start families’ experiences with stress: Understanding variations within a high-risk, low-income sample. Infant Mental Health Journal, 38(5), 602–616. 10.1002/imhj.21667. [DOI] [PubMed] [Google Scholar]
- Innamorati M, Lester D, Balsamo M, Erbuto D, Ricci F, Amore M, Girardi P, & Pompili M (2013). Factor validity of the Beck hopelessness scale in Italian medical patients. Journal of Psychopathology and Behavioral Assessment, 36(2), 300–307. 10.1007/s10862-013-9380-3. [DOI] [Google Scholar]
- Jiang Y, Ekono M, & Skinner C (2016). Basic facts about low-income children: Children under 18 years. National Center for Children in Poverty. [Google Scholar]
- Johnston C, & Leung DW (2001). Effects of medication, behavioral, and combined treatments on parents’ and children’s attributions for the behavior of children with attention-deficit hyperactivity disorder. Journal of Consulting and Clinical Psychology, 69(1), 67–76. 10.1037/0022-006X.69.1.67. [DOI] [PubMed] [Google Scholar]
- Jones DJ, Forehand R, Brody G, & Armisted L (2002). Positive parenting and child psychosocial adjustment in inner-city single-parent African American families: The role of maternal optimism. Behavior Modification, 26(4), 464–481. 10.1177/0145445502026004002. [DOI] [PubMed] [Google Scholar]
- Jones DJ. Anton M, Zachary C, Pittman S, Turner P, Forehand R, & Khavjou O (2016). A review of the key considerations in mental health services research: A focus on low income children and families. Couple and Family Psychology: Research and Practice, 5(4), 240–257. 10.1037/cfp0000069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones DJ, Loiselle R, Zachary CR, Georgeson A, Cline A, & Highlander A, Turner P, Youngstrom JK, Khavjou O, Anton M, Gonzalez M, Breslend NL, & Forehand R (2021). Optimizing engagement in behavioral parent training: Progress toward a technology-enhanced treatment model. Behavior Therapy, 52(2), 508–521. 10.1016/j.beth.2020.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones TL, & Prinz RJ (2005). Potential roles of parental self-efficacy in parent and child adjustment: A review. Clinical Psychology Review, 25(3), 341–363. 10.1016/j.cpr.2004.12.004. [DOI] [PubMed] [Google Scholar]
- Kashdan TB, Pelham WE, Lang AR, Hoza B, Jacob RG, Jennings JR, Blumenthal JD, & Gnagy EM (2002). Hope and optimism as human strengths in parents of children with externalizing disorders: Stress is in the eye of the beholder. Journal of Social and Clinical Psychology, 21(4), 441–468. 10.152l/jscp.21.4.441.22597. [DOI] [Google Scholar]
- Kaiser NM, Hinshaw SP, & Pfiffner LJ (2010). Parent cognitions and behavioral parent training: Engagement and outcomes. ADHD Report, 18(1), 6–12. 10.1521/adhd.2010.18.L6. [DOI] [Google Scholar]
- Koenig JL, Barry RA, & Kochanska G (2010). Rearing difficult children: Parents’ personality and children’s proneness to anger as predictors of future parenting. Parenting: Science and Practice, 10(4), 258–273. 10.1080/15295192.2010.492038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leijten P, Raaijmakers MA, De Castro BO, & Matthys W (2013). Does socioeconomic status matter? A meta-analysis on parent training effectiveness for disruptive child behavior. Journal of Clinical Child & Adolescent Psychology, 42(3), 384–392. 10.1080/15374416.2013.769169. [DOI] [PubMed] [Google Scholar]
- Linehan M (2014). DBT skills training manual. Guilford Publications. [Google Scholar]
- Loh J, Harms C, & Harman B (2017). Effects of parental stress, optimism, and health-prompting behaviors on the quality of life of primiparous and multiparous mothers. Nursing Research, 66(3), 231–239. 10.1097/NNR.0000000000000219. [DOI] [PubMed] [Google Scholar]
- Lundahl B, Risser HJ, & Lovejoy MC (2006). A meta-analysis of parent training: moderators and follow-up effects. Clinical Psychology Review, 26( 1), 86–104. 10.1016/j.cpr.2005.07.004 [DOI] [PubMed] [Google Scholar]
- McMahon RJ, & Forehand R (2003). Helping the non-compliant child: Family-based treatment for oppositional behavior (2nd ed.). Guilford. [Google Scholar]
- McNeish D, & Wolf MG (2020). Thinking twice about sum scores. Behavior Research Methods, 52, 2287–2305. 10.3758/sl3428-020-01398-0. [DOI] [PubMed] [Google Scholar]
- Nock MK, & Kazdin AE (2005). Randomized controlled trial of a brief intervention for increasing participation in parent management training. Journal of Consulting and Clinical Psychology, 73(5), 872–879. 10.1037/0022-006X.73.5.872. [DOI] [PubMed] [Google Scholar]
- Nock MK, & Kazdin AE (2001). Parent expectancies for child therapy: Assessment and relation to participation in treatment. Journal of Child and Family Studies, 10(2), 155–180. [Google Scholar]
- Pereira AI, & Barros L (2019). Parental cognitions and motivation to engage in psychological interventions: A systematic review. Child Psychiatry & Human Development, 50(3), 347–361. 10.1007/sl0578-018-0852-2. [DOI] [PubMed] [Google Scholar]
- Radey M (2018). Informal support among low-income mothers post welfare reform: A systematic review. Journal of Child and Family Studies, 27(12), 3782–3805. 10.1007/sl0826-018-1223-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rand KL (2018). Hope, self-efficacy, and optimism: Conceptual and empirical differences. In Gallagher MW & Lopez SJ (Eds.), The Oxford Handbook of Hope (p. 45–58). Oxford University Press. [Google Scholar]
- Reyno SM, & McGrath PJ (2006). Predictors of parent training efficacy for child externalizing behavior problems: A meta-analytic review. Journal of Child Psychology and Psychiatry, 47(1), 99–111. 10.llll/j.1469-7610.2005.01544.x. [DOI] [PubMed] [Google Scholar]
- Sameroff A (1975). Transactional models in early social relations. Human Development, 18, 65–79. 10.1159/000271476. [DOI] [Google Scholar]
- Scaramella L, Neppl TK, Ontai LL, & Conger RD (2008). Consequences of socioeconomic disadvantage across three generations: Parenting behavior and child externalizing problems. Journal of Family Psychology, 22(5), 725–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scheier MF, Carver CS, & Bridges MW (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the life orientation test. Journal of Personality and Social Psychology, 67(6), 1063–1078. [DOI] [PubMed] [Google Scholar]
- Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. (1998). The MINI-international neuropsychiatric interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59, 22–33. [PubMed] [Google Scholar]
- Shelton KK, Frick PJ, & Wootton J (1996). Assessment of parenting practices in families of elementary school-age children. Journal of Clinical Child Psychology, 25(3), 317–329. 10.1207/sl5374424jccp2503_8. [DOI] [Google Scholar]
- Solberg Nes L, Evans DR, & Segerstorm SC (2009). Optimism and college retention: Mediation by motivation, performance, and adjustment. Journal of Applied Social Psychology, 39(8), 1887–1912. 10.1111/j.1559-1816.2009.00508.x. [DOI] [Google Scholar]
- Stoll RD, Pina AA, & Schleider J (2020). Brief, non-pharmacological, interventions for pediatric anxiety: Meta-analysis and evidence base status. Journal of Clinical Child & Adolescent Psychology, 49(4), 435–459. 10.1080/15374416.2020.1738237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan AD, Benoit R, Breslend N, Compas B, Vreeland A, & Forehand R (2019). Cumulative risk of socioeconomic status factors in the context of a history of parent depression: Are there associations with child outcomes? Journal of Family Psychology, 33, 883–893. 10.1037/fam0000567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan AD, Vreeland A, Compas B, & Forehand R (2021). Does parenting explain the link between cumulative SES risk and child problems in the context of parental depression? Child Psychiatry & Human Development. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor ZE, & Conger RD (2017). Promoting strengths and resilience in single-mother families. Child Development, 88(2), 350–358. 10.1111/cdev.12741. [DOI] [PubMed] [Google Scholar]
- Theule J, Wiener J, Tannock R, & Jenkins JM (2013). Parenting stress in families of children with ADHD a meta-analysis. Journal of Emotional and Behavioral Disorders, 21(1), 3–17. 10.1177/1063426610387433. [DOI] [Google Scholar]
- Wadsworth ME (2012). Working with low-income families: Lessons learned from basic and applied research on coping with poverty-related stress. Journal of Contemporary Psychotherapy, 42 (1), 17–25. 10.1007/sl0879-011-9192-2. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Work with data is ongoing and have thus not yet been deposited. Data are available upon request with approval.