

Key Points
Question
What is the prevalence of polycystic ovary syndrome (PCOS) among adolescents with type 2 diabetes (T2D)?
Findings
In this systematic review and meta-analysis involving 470 girls across 6 studies, the prevalence of PCOS was 19.58%, a prevalence that is substantially higher than that of PCOS in the general adolescent population.
Meaning
These findings suggest that PCOS is a common morbidity in girls with T2D, and it is critical that active screening for PCOS in girls with T2D is initiated at diabetes diagnosis and follows international evidence-based guidelines for diagnosing PCOS in adolescents.
This systematic review and meta-analysis aims to determine the prevalence of polycystic ovary syndrome in girls with type 2 diabetes and to assess the association of obesity and race with this prevalence.
Abstract
Importance
The prevalence of pediatric type 2 diabetes (T2D) is increasing globally. Girls with T2D are at risk of developing polycystic ovary syndrome (PCOS), but the prevalence of PCOS among girls with T2D is unknown.
Objective
To determine the prevalence of PCOS in girls with T2D and to assess the association of obesity and race with this prevalence.
Data Sources
In this systematic review and meta-analysis, MEDLINE, Embase, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Web of Science: Conference Proceedings Citation Index–Science, and the gray literature were searched from inception to April 4, 2021.
Study Selection
Two reviewers independently screened for studies with observational study design that recruited 10 or more participants and reported the prevalence of PCOS in girls with T2D.
Data Extraction and Synthesis
Risk of bias was evaluated using a validated tool, and level of evidence was assessed using the Oxford Centre for Evidence-Based Medicine criteria. A random-effects meta-analysis was performed. This study follows the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guideline.
Main Outcomes and Measures
The main outcome of this systematic review was the prevalence of PCOS in girls with T2D. Secondary outcomes included assessing the associations of obesity and race with PCOS prevalence.
Results
Of 722 screened studies, 6 studies involving 470 girls with T2D (mean age at diagnosis, 12.9-16.1 years) met the inclusion criteria. The prevalence (weighted percentage) of PCOS was 19.58% (95% CI, 12.02%-27.14%; I2 = 74%; P = .002). Heterogeneity was moderate to high; however, it was significantly reduced after excluding studies that did not report PCOS diagnostic criteria, leading to a calculated prevalence (weighted percentage) of 24.04% (95% CI, 15.07%-33.01%; I2 = 0%; P = .92). Associations with obesity and race could not be determined because of data paucity.
Conclusions and Relevance
In this meta-analysis, approximately 1 in 5 girls with T2D had PCOS, but the results of this meta-analysis should be considered with caution because studies including the larger numbers of girls did not report the criteria used to diagnose PCOS, which is a challenge during adolescence. The associations of obesity and race with PCOS prevalence among girls with T2D need further evaluation to help define at-risk subgroups and implement early assessment and treatment strategies to improve management of this T2D-related comorbidity.
Introduction
Over the past 3 decades, type 2 diabetes (T2D) has made the transition from being an adult disease to being a pediatric disorder.1,2,3,4,5,6,7,8 T2D in youth is an aggressive disease with multiple associated comorbidities and poor response to current therapies; it is also associated with higher morbidity and mortality rates than adult-onset T2D.9,10,11
Polycystic ovary syndrome (PCOS) is a complex endocrine disorder that occurs in 1.14% to 11.04% of adolescent girls globally.12,13 The diagnostic criteria for PCOS during adolescence include the combination of menstrual irregularities according to time since menarche and clinical or biochemical hyperandrogenism after excluding other possible causes.14,15,16,17,18 Pelvic ultrasonography is not recommended for PCOS diagnosis in girls who are less than 8 years since menarche according to international evidence-based guidelines,18 because it is associated with overdiagnosis of PCOS.19 Insulin resistance and compensatory hyperinsulinemia are present in 44% to 70% of women with PCOS,20,21 suggesting that they are more likely to develop T2D.22,23,24
PCOS is also associated with a range of cardiometabolic diseases, including hypertension and dyslipidemia, as well as mental health disorders and future infertility.25,26,27,28 Importantly, girls with T2D and PCOS are at an increased risk of depression.29 However, although PCOS is associated with a range of conditions that are related to obesity, the association of PCOS with obesity is not well understood. PCOS is more common in adolescents with obesity,12 yet insulin resistance is at times present in patients with PCOS regardless of their body mass index (BMI).30,31,32
In addition, pediatric T2D disproportionately affects female patients, and its rates are increased among minoritized racial and ethnic groups.1,2,4,5 Determining the scale of PCOS in T2D and the association of obesity and race with PCOS genesis can inform personalized screening and treatment strategies in this population.33,34 The objectives of this systematic review and meta-analysis were to determine the prevalence of PCOS in girls with T2D and to assess the association of obesity and race with PCOS prevalence.
Methods
Systematic Review Protocol and Registration
This systematic review and meta-analysis has been registered with PROSPERO.35 Institutional review board approval and informed consent were not sought because the data were anonymous and publicly available, in accordance with 45 CFR §46. The manuscript was developed and reported in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guideline.36
Search Strategy and Eligibility Criteria
Searches in MEDLINE, Embase, CINAHL, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews were developed by a senior health sciences librarian (L.B.) (eTable 1, eTable 2, eTable 3, and eTable 4 in the Supplement). Gray literature searches were conducted in ClinicalTrials.gov, Cochrane Central Registry of Controlled Trials, and Web of Science Conference Proceedings Citation Index–Science (eTable 5 in the Supplement). In addition, we searched the reference lists of eligible articles at the full-text screening stage for additional papers that fulfill the inclusion criteria.
The databases were initially searched from inception to February 4, 2019, and updated searches were run on February 20, 2020, and April 4, 2021. There were no language restrictions, but searches were limited to human studies. Terms for pediatrics and T2D were combined with language referencing PCOS, prevalence, and observational study design. Where a conference abstract was considered for inclusion, we searched the databases for a full-text publication and contacted the principal investigator if the publication could not be located.
Studies were included if they reported PCOS in girls diagnosed with T2D at age 18 years or younger. The studies included cross-sectional, retrospective, and prospective cohort studies, with a sample size of 10 or more patients, which reported the prevalence of PCOS in patients with T2D. We included all studies reporting on PCOS regardless of whether PCOS definition was reported.
The exclusion criteria included studies of patients with gestational diabetes. When encountering studies with serial reporting of data, we planned to include the report with the largest sample size.
Study Selection, Data Abstraction, and Quality Appraisal
Title, abstract, and full-text screening, data abstraction, risk of bias, and level of evidence assessments were performed by 2 independent reviewers in 3 teams (M.C., A.N., M.H., Y.Q., S.S.J.C., and A.J.R). Disagreements were resolved through discussion, or by a third reviewer (M.C.S.) if they persisted.
Data abstractions were done using a standardized form. We collected data including study title, author name, publication year, country, study design, age at diabetes diagnosis, age at study participation, duration of diabetes, sample size, and prevalence of obesity in participants, where available. We also extracted data on PCOS definition and total and race-based prevalence of PCOS. We contacted the principal investigators to collect any missing data.
Risk of bias was evaluated using a validated tool for prevalence studies.37 The tool assesses the internal and external validity of the studies, rating overall risk of bias as low (score >8), moderate (score 6-8), or high (score ≤5).
Level of evidence was assessed using the Oxford Centre for Evidence-Based Medicine criteria.38 The scale rates the appropriateness of each study to answer the research question, taking into account study design, study quality, imprecision, indirectness, and inconsistency.38
Statistical Analysis
We performed a meta-analysis using a random-effects model when 2 or more studies reporting the prevalence of PCOS used similar design, methods, and populations.39,40 If studies could not be included in the meta-analysis, the results were reported as a narrative summary and tabulated. Prevalence values were calculated using raw proportions of the number of girls with PCOS and T2D divided by the total number of girls diagnosed with T2D. Study weights were calculated from the inverse of the variance of prevalence value. All studies were then pooled according to weight, and a pooled prevalence value was determined. Because no studies had prevalence values close to 0% or 100%, we did not use transformations in our calculations.40
The primary outcome for this review was the pooled prevalence of PCOS with a 95% CI. Both inconsistency index (I2) and χ2 test P values were used to quantify heterogeneity, with I2 > 75% and P < .10 considered as significant cutoffs for heterogeneity.41
We had originally planned to perform subgroup analyses by race if 10 or more studies were included in the meta-analysis. However, these analyses could not be completed because of the limited number of eligible studies. Because of the number of included studies that did not report PCOS diagnostic criteria, we also conducted a post hoc sensitivity analysis excluding these studies to examine their impact on prevalence and heterogeneity. The meta-analysis was conducted using the metafor package in RStudio statistical software version 1.1.383 and R statistical software version 3.4.3 (R Project for Statistical Computing).42,43,44
Results
Study Selection
Of 722 screened articles, 6 studies45,46,47,48,49,50 involving 470 girls met our inclusion criteria (Figure 1). The Table reports the characteristics of the included studies. Five were retrospective cohort studies,45,46,47,48,49 and 1 was a prospective cohort study.50 The mean (SD) age at diagnosis of T2D ranged from 12.9 to 16.1 years, and the mean duration of T2D ranged from inclusion at diagnosis of T2D to 5.9 years after diagnosis.
Figure 1. Study Flow Diagram.

PCOS indicates polycystic ovary syndrome.
aThe exclusion criteria included studies of patients with gestational diabetes.
Table. Characteristics of Included Studies.
| Study | Design | Mean (SD) or mean (95% CI), y | PCOS prevalence, No. (%) | Sample size, No. | Patients, No. (%) | Risk of bias | Level of evidence | Method of PCOS assessment | US use | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age at T2D diagnosis | Age at study enrollment/measurement | Duration of T2D | Ethnic distribution | Prevalence of PCOS by ethnic group | Prevalence of obesity in female patients | ||||||||
| Amed et al,45 2012, Canada | RC | Indigenous: 12.9 (12.4-13.4)a | Indigenous: 12.9 (12.4-13.4)a | 0 | 11 (8.5) | 130 | White 36 (27.7) | White: 6 (17) | NR | Moderate | 3 | Medical records | No |
| White: 14.4 (13.8-15.1)a | White: 14.4 (13.8-15.1)a | Indigenous: 64 (49.2) | Indigenous: 1 (2) | ||||||||||
| Other ethnicity: 14.3 (13.7-14.9)a,b | Other ethnicity: 14.3 (13.7-14.9)a,b | Other: 30 (23.1)b | Other: 5 (17),b | ||||||||||
| Amutha et al,46 2012, India | RC | 16.1 (2.5)a,c | 22.2 (9.7)a,c | 5.94 (0.48)a,c | 45 (23.1) | 195 | Indian: 195 (100)d | Indian: 45 (23.1)d | NR | Moderate | 1 | Clinical symptoms (unspecified) | No |
| Balasanthiran et al,47 2012, UK | RC | 15.2 (3.34)a | 21.2 (3.19)a | 5.4 (3.09)a | 6 (22) | 27 | Bangladeshi: 11 (25) | NR | NR | Moderate | 2 | Hirsutism (documented using the Ferriman-Gallwey score) and menstrual irregularities | No |
| Black African: 4 (9) | |||||||||||||
| Black Caribbean: 4 (9) | |||||||||||||
| Indian: 7 (16) | |||||||||||||
| Pakistani: 9 (20) | |||||||||||||
| White British: 6 (14) | |||||||||||||
| Unclear: 3 (7)a | |||||||||||||
| Pérez-Perdomo et al,48 2005, Puerto Rico | RC | <10 y: 5 (7.9%) | <10 y: 5 (7.8%) | NR | 12 (21) | 58e | NR | NR | NR | High | 3 | Medical records | No |
| 10-14 y: 36 (57.1%) | 10-14 y: 29 (45.3%) | ||||||||||||
| 15-18 y: 21 (33.3%) | 15-18 y: 29 (45.3%) | ||||||||||||
| ≥19 y: 1 (1.6%) | ≥19 y: 1 (1.6%) | ||||||||||||
| Zdravkovic et al,49 2004, Canada | RC | 13.5 (2.2)a | 13.5 (2.2)a | 0 | 6 (23) | 26 | African Canadian: 11 (27) | NR | NR | Low | 2 | History of irregular menstrual periods, obesity, or biochemical evidence of hyperandrogenism | No |
| White: 6 (15) | |||||||||||||
| First Nations: 1 (2) | |||||||||||||
| Hispanic: 4 (10) | |||||||||||||
| South or East Asian: 19 (46)a | |||||||||||||
| Shield et al,50 2009, UK and Republic of Ireland | PC | 13.6 (9.9-16.8)a | 14.5 (10.8-17.8)a | 1 | 9 (26) | 34 | Black: 12 (17) | NR | NR | Low | 2 | Clinical features of PCOS including hirsutism and menstrual disturbance, supported by biochemical evidence of low sex hormone-binding globulin and luteinizing hormone predominance or US | Yes |
| Mixed or Chinese: 6 (8) | |||||||||||||
| South Asian: 13 (18) | |||||||||||||
| White: 42 (57)a | |||||||||||||
Abbreviations: NR, not reported; PC, prospective cohort; PCOS, polycystic ovary syndrome; RC, retrospective cohort; T2D, type 2 diabetes; US, ultrasonography.
Value is representative of whole cohort of the study including male patients.
The study did not specify what is meant by other race or ethnicity.
Data are mean (SE).
Ethnic distribution is assumed to match country of origin.
We subtracted from sample size girls with T2D diagnosed at age less than 10 years because they are unlikely to be pubertal and present with PCOS, and girls with T2D diagnosis at age greater than 18 years because this does not fit our inclusion criteria.
Prevalence of PCOS
The prevalence (weighted percentage) of PCOS across the included studies was 19.58% (95% CI, 12.02%-27.14%) (Figure 2).45,46,47,48,49,50 Heterogeneity was moderate to high (I2 = 74%; P = .002).
Figure 2. Forest Plot Showing Prevalence of Polycystic Ovary Syndrome in Patients With Pediatric Type 2 Diabetes.
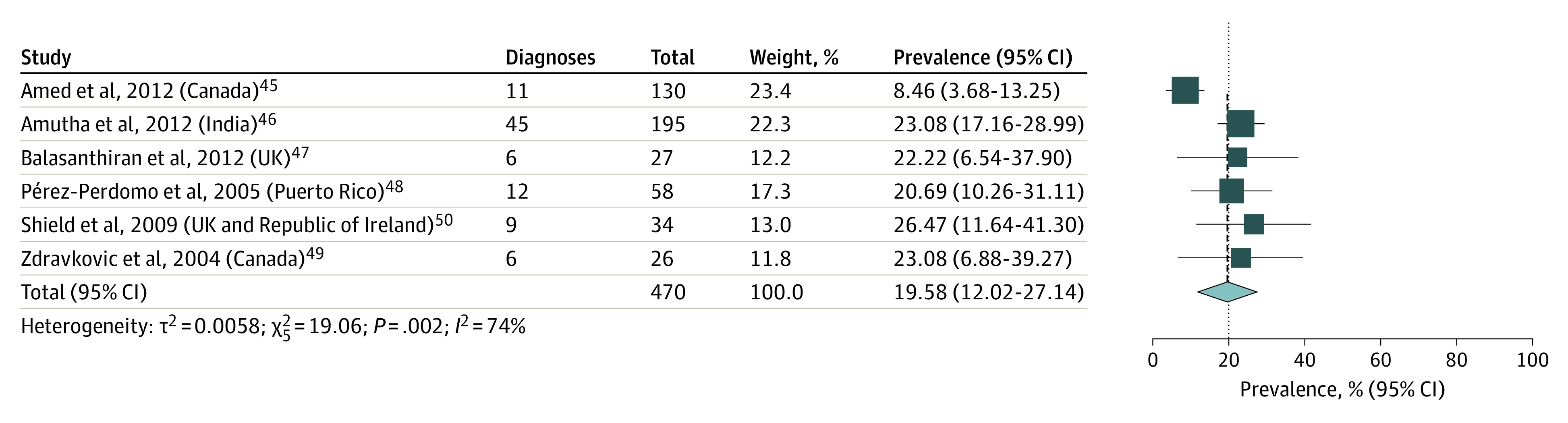
Size of boxes is proportional to weight of each study. Solid lines represent confidence interval for the prevalence value reported in each study. Dotted line represents the pooled estimate.
Prevalence of PCOS by Diagnostic Criteria
There were variations in the PCOS definition in the included studies. The PCOS diagnostic criteria used in the included studies are summarized in eTable 6 in the Supplement. Common diagnostic criteria across the different guidelines included persistent oligomenorrhea and clinical and/or biochemical hyperandrogenism. Three studies used these criteria to make a PCOS diagnosis (Table).47,49,50 The remaining studies reported PCOS diagnosis according to medical records review or clinical symptoms; however, the exact criteria were not defined.45,46,48 In addition, none of the studies reported time to menarche, which is important for establishing PCOS diagnosis.14,15,16,17,18
We conducted a sensitivity analysis excluding studies that did not report PCOS diagnostic criteria (87 girls) (Figure 3). The pooled PCOS prevalence (weighted percentage) increased to 24.04% (95% CI, 15.07%-33.01%) with a substantial reduction in heterogeneity (I2 = 0%; P = .92).47,49,50
Figure 3. Forest Plot Showing Prevalence of Polycystic Ovary Syndrome (PCOS) in Patients With Pediatric Type 2 Diabetes in Studies Following PCOS Definition in Adolescence.

Size of boxes is proportional to weight of each study. Solid lines represent confidence interval for the prevalence value reported in each study. Dotted line represents the pooled estimate.
Prevalence of PCOS by Race
Only 2 studies45,46 reported the prevalence of PCOS by race. The prevalence was 17.00% in White individuals (36 girls),45 23.10% in Indian individuals (195 girls),46 and 2.00% in Indigenous individuals in Canada (64 girls).45
Obesity and PCOS Prevalence
Although we originally aimed to determine the association of obesity and PCOS, none of the included studies provided information on the prevalence of obesity. Thus, the association between PCOS and obesity could not be evaluated.
Risk of Bias
Two studies had low risk of bias,49,50 3 studies had moderate risk of bias,45,46,47 and 1 had high risk of bias (eTable 7 in the Supplement).48 In 3 studies,46,47,49 the study population was not representative of the national population, and in 3 other studies45,47,48 the sampling frame was not representative of the target population. Cases were not selected using random selection or census data in 2 studies.45,48 One study48 had nonresponse bias and it was unclear what numerator and denominator were used to calculate PCOS prevalence.
In 3 included studies,45,46,48 the diagnostic criteria used for PCOS assessment were unclear. In 1 study,48 it was not clear whether all patients were assessed for PCOS using the same methods.
Level of Evidence
Studies had a level of evidence of 1 (1 study),46 2 (3 studies),47,49,50 or 3 (2 studies).45,48 Level of evidence was rated down for studies that did not use random sampling,45,48 and for those that did not have an adequate sample size.47,49,50
Discussion
The prevalence of pediatric T2D is increasing globally, and the majority of these patients are female.6,7,51 PCOS is a comorbidity of T2D that is associated with substantial metabolic, cardiovascular, and psychological consequences.23,26,52,53,54 Thus, the timely assessment and management of PCOS in this high-risk population is critical.22 On the basis of studies with mostly moderate risk of bias, this systematic review and meta-analysis demonstrated that approximately 1 in 5 girls with T2D have PCOS. This figure is substantially higher than PCOS prevalence among the general female adolescent population, which is estimated at 1.14% to 11.04%.12,13 There was moderate-to-high heterogeneity in the results of the studies included, although most of the heterogeneity may be attributable to the inclusion of studies that did not clearly report the PCOS diagnostic criteria. The prevalence of PCOS by race was reported in single studies, which precluded generalizability, and the association of obesity with PCOS could not be estimated because of the lack of data.
The association between PCOS and T2D in adults is bidirectional.55,56,57 Insulin resistance plays a central role in the pathogenesis of PCOS, and studies in adolescents have shown that girls with PCOS have decreased insulin sensitivity and compensatory hyperinsulinemia.23,30,58 Insulin increases the sensitivity of the pituitary gland to hypothalamic gonadotropin-releasing hormone, which, in turn, stimulates the production of luteinizing hormone.59 Both insulin and luteinizing hormone act synergistically on the ovarian theca cells to upregulate androgen production,21,55 which, in turn, reduces adipose tissue adiponectin secretion and insulin sensitivity and upregulates insulin production.60 In addition, insulin increases androgen production within the subcutaneous adipose tissue via the upregulation of the aldo-keto reductase 1C3 activity.61
Another mechanism that may lead to both insulin resistance and hyperandrogenism is lipotoxicity.22 Increased ovarian exposure to fatty acids can lead to the overproduction of androgens,62,63 and the enhanced delivery of fatty acids to nonadipose tissues is key to the development of insulin resistance and T2D.64
Although earlier studies suggested that obesity-related insulin resistance and hyperinsulinemia can contribute to PCOS pathogenesis,15 insulin resistance in patients with PCOS may be present independently of BMI.30,31,32 Obesity seems to increase the risk of PCOS only slightly65 and might represent a referral bias for PCOS.12 Lipotoxicity is a potential mechanism in the development of both T2D and PCOS, and it can occur independently of obesity.15,66 In addition, adipose tissue dysfunction is seen in both PCOS and T2D,22 as women with PCOS have larger subcutaneous adipocytes for the same degree of total adiposity and BMI, and adipocyte hypertrophy is strongly correlated with insulin resistance and T2D.67,68 Further studies are needed to clarify the association of obesity with PCOS pathogenesis in girls with T2D.
Because of the scarcity of studies reporting race-specific data, we could not address the association of race with PCOS prevalence comprehensively. However, our data demonstrate that Indian girls had the highest prevalence, followed by White girls, and then Indigenous girls in Canada. In a retrospective study69 assessing PCOS prevalence in 250 adolescents without T2D, 60 patients were African American (65%) and 24 patients (26%) were White. African American patients had a higher BMI and hemoglobin A1c and less dyslipidemia compared with White individuals.69 A systematic review70 in adult women reported that Chinese women have the lowest prevalence of PCOS, followed by White, Middle Eastern, and Black women. More studies are needed to evaluate the prevalence of PCOS in girls with T2D across different racial groups to aid the development of personalized screening and management strategies.
It is important for PCOS to be diagnosed early to prevent the development of ensuing complications when untreated. PCOS in adolescence is associated with features of the metabolic syndrome, including hypertension, hyperglycemia, and dyslipidemia.26 In addition, adolescents with PCOS have higher prevalence of cardiovascular risk factors,23 including higher carotid intima thickness, β stiffness index, and reduced arterial compliance compared with patients with obesity and no PCOS.54 Psychiatric comorbidities are also prevalent in PCOS, such as anxiety (18%), depression (16%), and attention-deficit/hyperactivity disorder (9%).53 Health-related quality of life is substantially reduced in patients with PCOS, with body weight concerns, menstrual irregularity, and a sense of lack of control over health being important contributors.52,71 It is critical that PCOS in T2D is managed with a focus on biopsychosocial well-being to achieve positive health outcomes.
Limitations
The limitations of this systematic review include that none of the studies had PCOS as a primary outcome. There was also a lack of a unified approach to diagnosing PCOS across studies and no reporting of the timing of menarche, which may have contributed to the high heterogeneity observed in the meta-analysis. Two of the largest studies did not report the criteria used for PCOS diagnosis.45,46 However, this systematic review had a comprehensive search strategy across several databases, including the gray literature, which includes all available evidence to date on this outcome.
The results of this study reflect the lack of consensus and difficulty in diagnosing PCOS in adolescents. The European Society of Human Reproduction and Embryology/American Society of Reproductive Medicine, the Pediatric Endocrine Society, and the International Consortium of Paediatric Endocrinology guidelines suggest that ultrasonography showing increased ovarian size could be used to aid in diagnosis, but other guidelines are more conservative in using these findings to diagnose PCOS.14,15,16,17,18 In addition, the European Society of Human Reproduction and Embryology/American Society of Reproductive Medicine guidelines state that biochemical hyperandrogenism needs to be present, and not just clinical signs of hyperandrogenism, whereas other guidelines state that either is sufficient for diagnosing PCOS.14,15,16,17,18 There is a need for a consensus to establish the pediatric criteria for diagnosing PCOS in adolescents to ensure accurate diagnosis and lower the misclassification rates.
Given these limitations, the results should be interpreted with caution. Larger multiethnic, longitudinal cohort studies evaluating PCOS prevalence in girls with T2D and using standardized criteria for defining PCOS are urgently needed.
Conclusions
This study found that in girls with T2D, approximately 1 in 5 had PCOS. Identifying PCOS in this population is critical to allow for early screening and management of PCOS and its associated health concerns. Future studies are urgently needed to define the impact of obesity and race on PCOS prevalence in this population and to ensure the development of personalized assessment and treatment strategies.
eTable 1. Sample Search Strategy: MEDLINE
eTable 2. Sample Search Strategy: Embase
eTable 3. Search Strategy: CINAHL
eTable 4. Search Strategy: Cochrane Library—Reviews and Trials
eTable 5. Search Strategy: Web of Science—Conference Proceedings Citation Index–Science (CPCI- S), 1990-Present
eTable 6. Summary of Guidelines for Diagnosing PCOS in Adolescents
eTable 7. Risk of Bias of Included Studies
eReferences
References
- 1.Dabelea D, Mayer-Davis EJ, Saydah S, et al. ; SEARCH for Diabetes in Youth Study . Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA. 2014;311(17):1778-1786. doi: 10.1001/jama.2014.3201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nadeau K, Dabelea D. Epidemiology of type 2 diabetes in children and adolescents. Endocr Res. 2008;33(1-2):35-58. doi: 10.1080/07435800802080138 [DOI] [PubMed] [Google Scholar]
- 3.Dabelea D, Bell RA, D’Agostino RB Jr, et al. ; Writing Group for the SEARCH for Diabetes in Youth Study Group . Incidence of diabetes in youth in the United States. JAMA. 2007;297(24):2716-2724. doi: 10.1001/jama.297.24.2716 [DOI] [PubMed] [Google Scholar]
- 4.Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ. Increasing prevalence of type II diabetes in American Indian children. Diabetologia. 1998;41(8):904-910. doi: 10.1007/s001250051006 [DOI] [PubMed] [Google Scholar]
- 5.Dabelea D, Pettitt DJ, Jones KL, Arslanian SA. Type 2 diabetes mellitus in minority children and adolescents: an emerging problem. Endocrinol Metab Clin North Am. 1999;28(4):709-729. doi: 10.1016/S0889-8529(05)70098-0 [DOI] [PubMed] [Google Scholar]
- 6.Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes mellitus: present and future perspectives. Nat Rev Endocrinol. 2011;8(4):228-236. doi: 10.1038/nrendo.2011.183 [DOI] [PubMed] [Google Scholar]
- 7.Mayer-Davis EJ, Lawrence JM, Dabelea D, et al. ; SEARCH for Diabetes in Youth Study . Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. 2017;376(15):1419-1429. doi: 10.1056/NEJMoa1610187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Divers J, Mayer-Davis EJ, Lawrence JM, et al. Trends in incidence of type 1 and type 2 diabetes among youths: selected counties and Indian reservations, United States, 2002-2015. MMWR Morb Mortal Wkly Rep. 2020;69(6):161-165. doi: 10.15585/mmwr.mm6906a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kim G, Divers J, Fino NF, et al. Trends in prevalence of cardiovascular risk factors from 2002 to 2012 among youth early in the course of type 1 and type 2 diabetes: the SEARCH for Diabetes in Youth Study. Pediatr Diabetes. 2019;20(6):693-701. doi: 10.1111/pedi.12846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reynolds K, Saydah SH, Isom S, et al. Mortality in youth-onset type 1 and type 2 diabetes: the SEARCH for Diabetes in Youth study. J Diabetes Complications. 2018;32(6):545-549. doi: 10.1016/j.jdiacomp.2018.03.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cioana M, Deng J, Hou M, et al. Prevalence of hypertension and albuminuria in pediatric type 2 diabetes: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(4):e216069. doi: 10.1001/jamanetworkopen.2021.6069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Christensen SB, Black MH, Smith N, et al. Prevalence of polycystic ovary syndrome in adolescents. Fertil Steril. 2013;100(2):470-477. doi: 10.1016/j.fertnstert.2013.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Naz MSG, Tehrani FR, Majd HA, et al. The prevalence of polycystic ovary syndrome in adolescents: a systematic review and meta-analysis. Int J Reprod Biomed. 2019;17(8):533-542. doi: 10.18502/ijrm.v17i8.4818 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fauser BCJM, Tarlatzis BC, Rebar RW, et al. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil Steril. 2012;97(1):28-38.e25. doi: 10.1016/j.fertnstert.2011.09.024 [DOI] [PubMed] [Google Scholar]
- 15.Ibáñez L, Oberfield SE, Witchel S, et al. An international consortium update: pathophysiology, diagnosis, and treatment of polycystic ovarian syndrome in adolescence. Horm Res Paediatr. 2017;88(6):371-395. doi: 10.1159/000479371 [DOI] [PubMed] [Google Scholar]
- 16.Legro RS, Arslanian SA, Ehrmann DA, et al. ; Endocrine Society . Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565-4592. doi: 10.1210/jc.2013-2350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Witchel SF, Oberfield S, Rosenfield RL, et al. The diagnosis of polycystic ovary syndrome during adolescence. Horm Res Paediatr. 2015;83:376-389. doi: 10.1159/000375530 [DOI] [PubMed] [Google Scholar]
- 18.Peña AS, Witchel SF, Hoeger KM, et al. Adolescent polycystic ovary syndrome according to the international evidence-based guideline. BMC Med. 2020;18(1):72. doi: 10.1186/s12916-020-01516-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tay CT, Hart RJ, Hickey M, et al. Updated adolescent diagnostic criteria for polycystic ovary syndrome: impact on prevalence and longitudinal body mass index trajectories from birth to adulthood. BMC Med. 2020;18(1):389. doi: 10.1186/s12916-020-01861-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Baillargeon JP, Iuorno MJ, Nestler JE. Insulin sensitizers for polycystic ovary syndrome. Clin Obstet Gynecol. 2003;46(2):325-340. doi: 10.1097/00003081-200306000-00011 [DOI] [PubMed] [Google Scholar]
- 21.Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev. 2012;33(6):981-1030. doi: 10.1210/er.2011-1034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carreau AM, Baillargeon JP. PCOS in adolescence and type 2 diabetes. Curr Diab Rep. 2015;15(1):564. doi: 10.1007/s11892-014-0564-3 [DOI] [PubMed] [Google Scholar]
- 23.Arslanian SA, Lewy VD, Danadian K. Glucose intolerance in obese adolescents with polycystic ovary syndrome: roles of insulin resistance and beta-cell dysfunction and risk of cardiovascular disease. J Clin Endocrinol Metab. 2001;86(1):66-71. doi: 10.1210/jcem.86.1.7123 [DOI] [PubMed] [Google Scholar]
- 24.Hudnut-Beumler J, Kaar JL, Taylor A, et al. Development of type 2 diabetes in adolescent girls with polycystic ovary syndrome and obesity. Pediatr Diabetes. 2021;22(5):699-706. doi: 10.1111/pedi.13206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Çoban ÖG, Tulacı ÖD, Adanır AS, Önder A. Psychiatric disorders, self-esteem, and quality of life in adolescents with polycystic ovary syndrome. J Pediatr Adolesc Gynecol. 2019;32(6):600-604. doi: 10.1016/j.jpag.2019.07.008 [DOI] [PubMed] [Google Scholar]
- 26.Fazleen NE, Whittaker M, Mamun A. Risk of metabolic syndrome in adolescents with polycystic ovarian syndrome: a systematic review and meta-analysis. Diabetes Metab Syndr. 2018;12(6):1083-1090. doi: 10.1016/j.dsx.2018.03.014 [DOI] [PubMed] [Google Scholar]
- 27.Sari SA, Celik N, Uzun Cicek A. Body perception, self-esteem, and comorbid psychiatric disorders in adolescents diagnosed with polycystic ovary syndrome. J Pediatr Adolesc Gynecol. 2020;33(6):691-696. doi: 10.1016/j.jpag.2020.08.018 [DOI] [PubMed] [Google Scholar]
- 28.Balen AH, Rutherford AJ. Managing anovulatory infertility and polycystic ovary syndrome. BMJ. 2007;335(7621):663-666. doi: 10.1136/bmj.39335.462303.80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Benson J, Severn C, Hudnut-Beumler J, et al. Depression in girls with obesity and polycystic ovary syndrome and/or type 2 diabetes. Can J Diabetes. 2020;44(6):507-513. doi: 10.1016/j.jcjd.2020.05.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lewy VD, Danadian K, Witchel SF, Arslanian S. Early metabolic abnormalities in adolescent girls with polycystic ovarian syndrome. J Pediatr. 2001;138(1):38-44. doi: 10.1067/mpd.2001.109603 [DOI] [PubMed] [Google Scholar]
- 31.Dunaif A, Finegood DT. Beta-cell dysfunction independent of obesity and glucose intolerance in the polycystic ovary syndrome. J Clin Endocrinol Metab. 1996;81(3):942-947. doi: 10.1210/jcem.81.3.8772555 [DOI] [PubMed] [Google Scholar]
- 32.Dunaif A, Segal KR, Futterweit W, Dobrjansky A. Profound peripheral insulin resistance, independent of obesity, in polycystic ovary syndrome. Diabetes. 1989;38(9):1165-1174. doi: 10.2337/diab.38.9.1165 [DOI] [PubMed] [Google Scholar]
- 33.Ibáñez L, Ong KK, López-Bermejo A, Dunger DB, de Zegher F. Hyperinsulinaemic androgen excess in adolescent girls. Nat Rev Endocrinol. 2014;10(8):499-508. doi: 10.1038/nrendo.2014.58 [DOI] [PubMed] [Google Scholar]
- 34.Teede HJ, Misso ML, Costello MF, et al. ; International PCOS Network . Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602-1618. doi: 10.1093/humrep/dey256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Samaan MC, Cioana M, Banfield L, et al. The prevalence of comorbidities in pediatric type 2 diabetes mellitus: a systematic review—PROSPERO CRD42018091127. March 19, 2018. Accessed January 5, 2022. http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018091127
- 36.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 37.Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934-939. doi: 10.1016/j.jclinepi.2011.11.014 [DOI] [PubMed] [Google Scholar]
- 38.OCEBM Levels of Evidence Working Group . The Oxford 2011 levels of evidence. Oxford Centre for Evidence-Based Medicine. 2011. Accessed January 7, 2022. http://www.cebm.net/index.aspx?o=5653
- 39.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010;1(2):97-111. doi: 10.1002/jrsm.12 [DOI] [PubMed] [Google Scholar]
- 40.Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health. 2013;67(11):974-978. doi: 10.1136/jech-2013-203104 [DOI] [PubMed] [Google Scholar]
- 41.Deeks J, Higgins J, Altman D, eds. Chapter 10: Analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. Version 6.0. Cochrane; 2019. Accessed January 5, 2022. https://training.cochrane.org/handbook/archive/v6/chapter-10 [Google Scholar]
- 42.Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1-48. doi: 10.18637/jss.v036.i03 [DOI] [Google Scholar]
- 43.RStudio : Integrated development for R version 1.1.383. RStudio, Inc; 2016. Accessed January 5, 2022. https://www.rstudio.com/
- 44.R Foundation for Statistical Computing . R: a language and environment for statistical computing, version 3.4.3. 2017. Accessed January 5, 2022. https://cran.r-project.org/bin/windows/base/old/3.4.3/
- 45.Amed S, Hamilton JK, Sellers EAC, et al. Differing clinical features in Aboriginal vs. non-Aboriginal children presenting with type 2 diabetes. Pediatr Diabetes. 2012;13(6):470-475. doi: 10.1111/j.1399-5448.2012.00859.x [DOI] [PubMed] [Google Scholar]
- 46.Amutha A, Datta M, Unnikrishnan R, Anjana RM, Mohan V. Clinical profile and complications of childhood- and adolescent-onset type 2 diabetes seen at a diabetes center in south India. Diabetes Technol Ther. 2012;14(6):497-504. doi: 10.1089/dia.2011.0283 [DOI] [PubMed] [Google Scholar]
- 47.Balasanthiran A, O’Shea T, Moodambail A, et al. . Type 2 diabetes in children and young adults in East London: an alarmingly high prevalence. Pract Diabetes. 2012;29(5):193-198a. doi: 10.1002/pdi.1689 [DOI] [Google Scholar]
- 48.Pérez-Perdomo R, Pérez-Cardona CM, Allende-Vigo M, Rivera-Rodríguez MI, Rodríguez-Lugo LA. Type 2 diabetes mellitus among youth in Puerto Rico, 2003. P R Health Sci J. 2005;24(2):111-117. [PubMed] [Google Scholar]
- 49.Zdravkovic V, Daneman D, Hamilton J. Presentation and course of type 2 diabetes in youth in a large multi-ethnic city. Diabet Med. 2004;21(10):1144-1148. doi: 10.1111/j.1464-5491.2004.01297.x [DOI] [PubMed] [Google Scholar]
- 50.Shield JPH, Lynn R, Wan KC, Haines L, Barrett TG. Management and 1 year outcome for UK children with type 2 diabetes. Arch Dis Child. 2009;94(3):206-209. doi: 10.1136/adc.2008.143313 [DOI] [PubMed] [Google Scholar]
- 51.Reinehr T. Type 2 diabetes mellitus in children and adolescents. World J Diabetes. 2013;4(6):270-281. doi: 10.4239/wjd.v4.i6.270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kaczmarek C, Haller DM, Yaron M. Health-related quality of life in adolescents and young adults with polycystic ovary syndrome: a systematic review. J Pediatr Adolesc Gynecol. 2016;29(6):551-557. doi: 10.1016/j.jpag.2016.05.006 [DOI] [PubMed] [Google Scholar]
- 53.Sadeeqa S, Mustafa T, Latif S. Polycystic ovarian syndrome-related depression in adolescent girls: a review. J Pharm Bioallied Sci. 2018;10(2):55-59. doi: 10.4103/JPBS.JPBS_1_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Patel SS, Truong U, King M, et al. Obese adolescents with polycystic ovarian syndrome have elevated cardiovascular disease risk markers. Vasc Med. 2017;22(2):85-95. doi: 10.1177/1358863X16682107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37(5):467-520. doi: 10.1210/er.2015-1104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Rosenfield RL, Mortensen M, Wroblewski K, Littlejohn E, Ehrmann DA. Determination of the source of androgen excess in functionally atypical polycystic ovary syndrome by a short dexamethasone androgen-suppression test and a low-dose ACTH test. Hum Reprod. 2011;26(11):3138-3146. doi: 10.1093/humrep/der291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Ehrmann DA, Sturis J, Byrne MM, Karrison T, Rosenfield RL, Polonsky KS. Insulin secretory defects in polycystic ovary syndrome: relationship to insulin sensitivity and family history of non-insulin-dependent diabetes mellitus. J Clin Invest. 1995;96(1):520-527. doi: 10.1172/JCI118064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Cree-Green M, Rahat H, Newcomer BR, et al. Insulin resistance, hyperinsulinemia, and mitochondria dysfunction in nonobese girls with polycystic ovarian syndrome. J Endocr Soc. 2017;1(7):931-944. doi: 10.1210/js.2017-00192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Soldani R, Cagnacci A, Yen SS. Insulin, insulin-like growth factor I (IGF-I) and IGF-II enhance basal and gonadotrophin-releasing hormone-stimulated luteinizing hormone release from rat anterior pituitary cells in vitro. Eur J Endocrinol. 1994;131(6):641-645. doi: 10.1530/eje.0.1310641 [DOI] [PubMed] [Google Scholar]
- 60.O’Connor A, Phelan N, Tun TK, Boran G, Gibney J, Roche HM. High-molecular-weight adiponectin is selectively reduced in women with polycystic ovary syndrome independent of body mass index and severity of insulin resistance. J Clin Endocrinol Metab. 2010;95(3):1378-1385. doi: 10.1210/jc.2009-1557 [DOI] [PubMed] [Google Scholar]
- 61.O’Reilly M, Gathercole L, Capper F, Arlt W, Tomlinson J. Effect of insulin on AKR1C3 expression in female adipose tissue: in-vivo and in-vitro study of adipose androgen generation in polycystic ovary syndrome. Lancet. 2015;385(1)(suppl):S16. doi: 10.1016/S0140-6736(15)60331-2 [DOI] [PubMed] [Google Scholar]
- 62.Mai K, Bobbert T, Reinecke F, et al. Intravenous lipid and heparin infusion-induced elevation in free fatty acids and triglycerides modifies circulating androgen levels in women: a randomized, controlled trial. J Clin Endocrinol Metab. 2008;93(10):3900-3906. doi: 10.1210/jc.2008-0714 [DOI] [PubMed] [Google Scholar]
- 63.Bellanger S, Battista MC, Fink GD, Baillargeon JP. Saturated fatty acid exposure induces androgen overproduction in bovine adrenal cells. Steroids. 2012;77(4):347-353. doi: 10.1016/j.steroids.2011.12.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Carpentier AC. Postprandial fatty acid metabolism in the development of lipotoxicity and type 2 diabetes. Diabetes Metab. 2008;34(2):97-107. doi: 10.1016/j.diabet.2007.10.009 [DOI] [PubMed] [Google Scholar]
- 65.Yildiz BO, Knochenhauer ES, Azziz R. Impact of obesity on the risk for polycystic ovary syndrome. J Clin Endocrinol Metab. 2008;93(1):162-168. doi: 10.1210/jc.2007-1834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.de Zegher F, Lopez-Bermejo A, Ibáñez L. Adipose tissue expandability and the early origins of PCOS. Trends Endocrinol Metab. 2009;20(9):418-423. doi: 10.1016/j.tem.2009.06.003 [DOI] [PubMed] [Google Scholar]
- 67.Villa J, Pratley RE. Adipose tissue dysfunction in polycystic ovary syndrome. Curr Diab Rep. 2011;11(3):179-184. doi: 10.1007/s11892-011-0189-8 [DOI] [PubMed] [Google Scholar]
- 68.Mannerås-Holm L, Leonhardt H, Kullberg J, et al. Adipose tissue has aberrant morphology and function in PCOS: enlarged adipocytes and low serum adiponectin, but not circulating sex steroids, are strongly associated with insulin resistance. J Clin Endocrinol Metab. 2011;96(2):E304-E311. doi: 10.1210/jc.2010-1290 [DOI] [PubMed] [Google Scholar]
- 69.Shenep L, Al-Zubeidi H. Characteristics and ethnic variations of adolescents with polycystic ovarian syndrome at a tertiary care center. J Pediatr Endocrinol. 2017;2(2):1019. Accessed January 10, 2022. http://austinpublishinggroup.com/pediatric-endocrinology/download.php?file=fulltext/jpe-v2-id1019.pdf [Google Scholar]
- 70.Ding T, Hardiman PJ, Petersen I, Wang FF, Qu F, Baio G. The prevalence of polycystic ovary syndrome in reproductive-aged women of different ethnicity: a systematic review and meta-analysis. Oncotarget. 2017;8(56):96351-96358. doi: 10.18632/oncotarget.19180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Hopkins CS, Kimble LP, Hodges HF, Koci AF, Mills BB. A mixed-methods study of coping and depression in adolescent girls with polycystic ovary syndrome. J Am Assoc Nurse Pract. 2019;31(3):189-197. doi: 10.1097/JXX.0000000000000125 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Sample Search Strategy: MEDLINE
eTable 2. Sample Search Strategy: Embase
eTable 3. Search Strategy: CINAHL
eTable 4. Search Strategy: Cochrane Library—Reviews and Trials
eTable 5. Search Strategy: Web of Science—Conference Proceedings Citation Index–Science (CPCI- S), 1990-Present
eTable 6. Summary of Guidelines for Diagnosing PCOS in Adolescents
eTable 7. Risk of Bias of Included Studies
eReferences