

Abstract
Supernumerary teeth are dental units that appear in addition to the regular number of teeth. Their most frequent location is the anterior maxilla, especially on the maxillary midline, being called mesiodens, but also paramedian or in the position of a lateral incisor. On the other hand, the permanent canine is one of the most stable teeth regarding the number, with very few cases reported about hypo- or hyperdontia. This article reviews the few data found in the literature about the supernumerary permanent maxillary canine and also presents the case of an 8-year-old female patient with a supplemental permanent canine in the upper left maxilla. The patient was non-syndromic and did not present any other supernumerary teeth in the permanent dentition; she had only one in the temporary dentition. Using cone-beam computed tomography (CBCT) of the region, we were able to evaluate the position, structure, and shape of the supplemental canine and also to establish a treatment plan. The aim of this paper was to present this extremely rare case of a non-syndromic Romanian adult female patient with a unilateral supplemental permanent maxillary canine, and to include a literature review of the few reported such cases.
Keywords: supplemental impacted maxillary permanent canine, non-syndromic female patient
⧉ Introduction
The exceeding teeth in relation to the usual dental formula define hyperdontia or supernumerary teeth and can be found in any region of the dental arch [1]. They are located mostly in the premaxilla [2]. Their classification is made based on several criteria. Four morphological types of supernumerary teeth were described: conical, tuberculate, supplemental and odontome [3,4,5,6]. The conical tooth is a peg-shaped tooth; when it is located between the central incisors, it is called a mesiodens, and it is the most common type of hyperdontia [4, 7], appearing single or in association with other anomalies. A rare case of hypo–hyperdontia presenting mesiodens in association with agenesis of both maxillary canines has been reported [8]. The tuberculate type has a barrel shape, with an occlusal surface with several cusps, and usually remains unerupted due to its bigger size [7, 9]. The supplemental supernumerary is a duplication of a tooth from the normal dental formula and can be found both in the first and second dentition, and also in any region of the dental arch [4, 10,11]. Although odontomas are still classified by World Health Organization (WHO) as benign mixed odontogenic tumors [12], some articles suggest that, from an etiopathogenic and clinical point of view, they seem to be a manifestation of the same disturbed process [13].
Hyperdontia can be single or multiple [7], but one supernumerary tooth appears to be the most common finding [14,15]. The development of several supernumerary dental units is rare, and usually associated with systemic diseases or syndromes [16], such as cleidocranial dysplasia, cleft lip and palate, Gardner’s syndrome, Fabry–Anderson syndrome, Rothmund–Thomson syndrome, and Nance–Horan syndrome [1, 6, 17,18]. In studies on general Caucasian patients, the prevalence of supernumerary teeth reminded by Türkkahraman et al. is between 0.1% and 3.8% [19], and on Mongoloid population, the prevalence was higher than in any other racial groups [20]. In 2014, Mallineni did a literature review about supernumerary teeth and reported these numbers [1]: in primary dentition an incidence of 0.1–1.8% for Caucasians, 2.8–7.8% for Chinese children [21,22], and in permanent dentition an incidence of 0.4–2.1% for Caucasians, 2.4% for southern Chinese patients [23], with the highest incidence of 6.7% in South Africa [24]. In a radiographic study in a North Greek population, only 1.8% of patients had supernumerary teeth [25], and in a North Indian population, only 1.6% [26].
Studies about the frequency of supernumerary canines are very few. In a study that examines 152 patients with age from five to 15 years, with hyperdontia, almost 90% of the cases had the extra teeth in the premaxilla, and only 10.4% in the premolar, canine and molar area and in the lower anterior region. From these, 1.5% were in the maxillary canine region [14]. In a research conducted among 2241 Mexican children, only one case was found having a supernumerary canine [27]. Other researchers do not even mention the canine as a possible supernumerary tooth [15, 28,29]. There are also very few case reports in literature, presenting bilateral supernumerary maxillary temporary canines [30], supernumerary primary and permanent canines in the same area [31], supernumerary primary and permanent canines associated with a cleft of the alveolus [32], bilateral supernumerary permanent maxillary canines [19], bilateral supernumerary permanent mandibular canines [33], two supernumerary canines in the maxilla and two in the mandible [34].
Aim
The aim of this paper was to present this extremely rare case of a non-syndromic Romanian adult female patient with a unilateral supplemental permanent maxillary canine, and to include a literature review of the few reported such cases.
⧉ Case presentation
An 8-year-old female patient reported in our Clinic (Ortholand Clinic, Bucharest, Romania) with the chief complaint of unerupted left permanent upper central incisor and the presence of a supernumerary deciduous lateral incisor in the left maxilla. The medical history and the initial examination did not reveal any syndrome or general disease that might be associated with the presence of supernumerary teeth. The pregnancy of the mother and the labor were normal. The family history also did not reveal the presence of a systemic disease or of supernumerary teeth, and the patient did not have siblings. The general examination showed a normal level of intelligence for the age, with good communication.
The intraoral examination showed a mixed dentition, normal for the girl’s age, with well-developed maxillary and mandibular arches. In the anterior region of the maxilla, there were present right central permanent and temporary lateral incisors, left central and lateral deciduous incisors and also a supplemental temporary lateral incisor, well aligned in the dental arch and with a shape, size, morphology and color resembling the adjacent primary lateral incisor. The occlusion was evaluated and a class II division 2 pattern was found, with increased overjet, with a full deep bite in the incisor area, and a class II canine and molar relationship according to Angle’s Classification. The upper and lower supporting zones presented inter-proximal caries, some of them treated.
A panoramic X-ray was taken one year before, and a right maxillary cone-beam computed tomography (CBCT) was recorded. The radiological examination confirmed the presence of a left lateral supplemental deciduous incisor situated distally to the normal one, with a smaller crown and root, but with similar shape. The right upper quadrant had a normal number of dental units in both dentitions (Figure 1). The CBCT revealed the presence of a supernumerary left canine in the permanent dentition (Figure 2a). Both canines had a similar shape and size, one of them being situated above the other, very high, in the maxillary bone. Comparing the hard tissues configuration, we assumed that the permanent normal canine was the one situated higher in the maxilla (Figures 1 and 2b).
Figure 1.

Initial panoramic X-ray, aspect of the left lateral supplemental deciduous incisor
Figure 2.

(a and b) Supernumerary left canine; CBCT aspect of both permanent and supernumerary canines in the left maxilla. CBCT: Cone-beam computed tomography
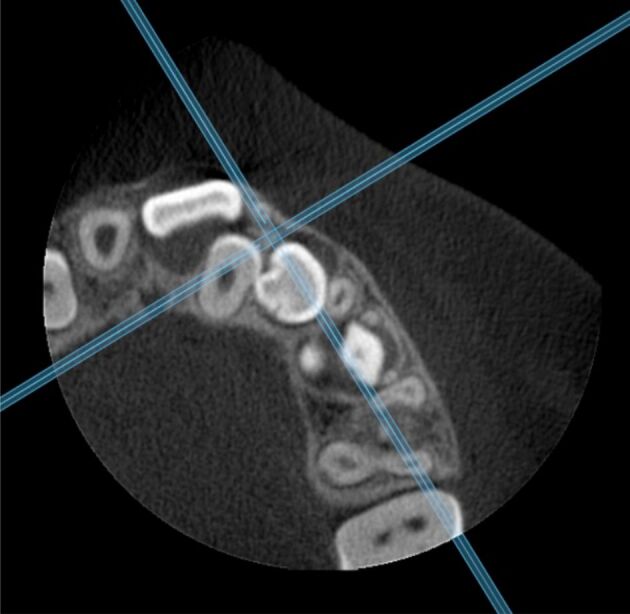
The CBCT was very carefully analyzed, to determine the normal or abnormal development of the permanent teeth, their position, and the consequences of supplemental teeth in both dentitions. The situation was not favorable, giving the fact that the formation of supernumerary teeth determined a disruption in the left maxilla. The left permanent central incisor became impacted, labially inclined and with a high position, with a coronal cyst; the left permanent lateral incisor was palatally displaced, blocked by the left deciduous lateral incisor (6.2) and also by the left supernumerary canine (Figure 3). Also, from the sagittal section, the root of the supplemental canine seemed in contact with the crown of the permanent one, which in time may lead to root resorption or tooth impaction (Figure 4a). The horizontal sections confirmed that the supplemental tooth was really a canine and not a lateral incisor, with prominent longitudinal ridges from the cusp tip down to the labial and palatal surfaces (Figures 2a, 3 and 4b). The CBCT three-dimensional (3D) reconstruction permits to visualize the complications determined by the presence of the supernumerary temporary lateral incisor and permanent canine (Figure 5).
Figure 3.
Aspect of the left central incisor presenting a coronal cyst and of the lateral incisor palatally displaced and blocked by the supernumerary canine
Figure 4.

(a and b) The relationship between the temporary canine, the supernumerary permanent canine, and the normal permanent canine; CBCT aspect of the impacted and displaced central incisor, the palatally situated lateral incisor, the supernumerary canine, the first and second premolars and first molar. CBCT: Cone-beam computed tomography
Figure 5.

The left upper maxilla: 3D reconstruction on CBCT. 3D: Three-dimensional; CBCT: Cone-beam computed tomography
In our case, the exact etiology of the supernumerary teeth could not be related to any heredity factors, as family history was not relevant. The supernumerary permanent canine was found after radiographic investigations, made to verify if the excess number of teeth in the temporary dentition had consequences in the permanent one. The treatment plan was to extract the central and lateral primary incisors, and to wait a few months to see if the removal of the obstacle will allow the permanent left incisor to erupt. At the second clinical examination, the left central incisor (2.1) was still impacted (Figure 6a), so the decision was to design an upper appliance for anchorage and to surgically expose the permanent incisor, to traction it to the dental arch. The parents asked for three more months waiting before starting the active treatment. Intraoral pictures were recorded to analyses the therapeutic options for tooth impaction and class II division 2 malocclusion, and also for comparing the clinical evolution (Figures 6b, 6c and 7).
Figure 6.

(a–c) Clinical examination – 2.1 still not erupting: frontal view; right lateral view; left lateral view
Figure 7.

Occlusal view of the upper arch
⧉ Discussions
Many studies suggest that anomalies in the deciduous dentition are frequently correlated with anomalies in the permanent dentition [35,36,37]. Fifty percent of patients with supernumerary primary teeth from one study developed an anomaly in the permanent dentition [37]. On the other hand, another survey reported only 18.2% of anomalies in the permanent dentition for subjects with primary hyperdontia [38]. In all cases, it is important to check and follow if other supernumerary teeth are present in the permanent dentition, every time we find extra teeth in the temporary dentition.
Various theories about the etiology of supernumerary teeth have been suggested, but for the moment, the main factor remains unclear [39]. Atavism is a hypothesis that promotes the return to an ancestral human dentition that was represented by a larger number of teeth [40], but this theory best describes the supplemental premolars and molars, since the ancestor mammals had three incisors, one canine, four premolars, and three molars in each jaw quadrant [41]. So, this hypothesis could not explain the supernumerary canine [42]. The tooth germ dichotomy theory suggests that, during the first stages of development, the dental lamina divides into two homogenous or heterogenous parts, resulting in two teeth with either similar size, or different size [4]. The most commonly accepted theory is that of local and independent hyperactivity of the dental lamina [14,15, 43]. If remnants from the dental lamina persist as epithelial tissues in the jaw and if induction factors stimulate them, a supplemental tooth bud appears that turns into a new odontogenic structure [40]. Genetic factors have an important role in supernumerary tooth formation. They are supposed to have an autonomic recessive inheritance [44], based on many reports that support the tendency to find more supernumerary teeth in cases were relatives of those affected also had supernumerary teeth [45], or linked to the X chromosome [1]. Many cases of supernumerary teeth have been reported in systemic diseases or syndromes [16], such as cleidocranial dysplasia, cleft lip and palate, Gardner’s syndrome, Fabry–Anderson syndrome, Rothmund–Thomson syndrome, Nance–Horan syndrome, Marfan syndrome, orofaciodigital syndrome and others [1, 6, 17,18, 46,47]. Also, a combination of environmental and genetic factors contributes to the development of supernumerary teeth [48]. Cases of various types of supernumerary teeth in the temporary and permanent dentition have been previously described in the literature. Still, our case of a female patient having a supernumerary lateral incisor in the temporary dentition and a supplemental canine in the permanent dentition is a very rare finding, due to the usual high numerical stability of the canine; this case presentation is also adding interesting data about this pathology to the existing rather scarce literature.
The presence of supernumerary teeth determines many complications. If they appear in the temporary dentition, extra teeth can lead to alteration of eruption or even impacted adjacent temporary or permanent teeth, alteration of position of adjacent teeth, such as rotations or ectopic positions, arch spacing, abnormal root formation, root resorption, dilacerations or even cysts formation [4, 49]. In the permanent dentition, supernumerary teeth can cause similar problems for adjacent teeth and also crowding. In a survey on 7348 people about the prevalence and features of supernumerary teeth, 29% of them caused impactions of other teeth, while 5% caused displacement of neighboring teeth. Most of the supernumerary teeth remained impacted (84%), and others developed cysts or tissue inflammation (9%) [50].
In a study on clinical repercussions of supernumerary canines, almost 70% of supernumerary teeth found were impacted, and half of them also caused the impaction of the permanent canines. Authors suggest that early diagnosis is mandatory to prevent complications and to reduce the treatment need or the complexity of the case [51]. This agrees with other studies that state that anomalies in the deciduous dentition also determine anomalies in the permanent one [36,37]. Clinical and radiographic examinations are needed in all cases where we suspect the presence of supernumerary teeth, to establish the treatment plan which might vary from extractions to orthodontic treatment for aligning the impacted teeth or correcting the malpositions, or even prosthetic solutions for obtaining a proper occlusion [52].
There are studies about the proper timing for supernumerary teeth removal. Most of them suggest the early intervention on supernumerary teeth, to minimize the damage on adjacent teeth [1, 53], while other recommend postponing the removal, if there are not associated complications [54]. Mallineni presents the opinion that, usually, if supernumerary teeth are removed, the majority of impacted permanent incisors erupt spontaneously. In contrast, the rest of them, usually the ones with high angulation, may require orthodontic traction [1, 55]. Di Biase found in his study that 75% of incisors erupted spontaneously after removal of the supernumerary tooth, and recommends only the extraction of the extra tooth, without surgical exposure of the permanent incisors [56]. Other authors found lower rates of spontaneous eruption and suggested the exposure and orthodontic attachment bonding in the same intervention as the one for the supernumerary tooth removal [57].
⧉ Conclusions
The case reported is a very unusual one, as long as the supplemental maxillary permanent canine is rarely found in healthy, non-syndromic patients. The delay of the central permanent incisor’s eruption sent the parents to our Office. Initially, the clinical examination revealed the presence of a temporary supernumerary upper lateral incisor that determined the impaction of the permanent central and lateral incisors in the same quadrant and also their malposition. The radiographic examination by CBCT determined the exact position of the permanent tooth germs and also revealed the presence of a supernumerary canine, which is a rare finding. Anomalies in the primary dentition are important due to their consequences on the succedaneum’s permanent dentition. Early diagnosis allows a good patient management and the development of an optimal treatment plan. The decision to act or not and the appropriate time to do it is important to prevent complications, and also to reduce the later treatment need. Sometimes, multidisciplinary approach is needed for managing these complications, so a good team should be prepared to step in if needed. Future statistical studies are necessary to establish the incidence of supplemental permanent maxillary canine in Romanian population.
Conflict of interest
The authors declare that they have no conflict of interests.
Authors’ contribution
Authors #1 (OCA) and #2 (MID) have equal contributions to this paper.
References
- 1.Mallineni SK. Supernumerary teeth: review of the literature with recent updates. Conf Pap Sci. 2014;2014:764050–764050. [Google Scholar]
- 2.Primosch RE. Anterior supernumerary teeth - assessment and surgical intervention in children. Pediatr Dent. 1981;3(2):204–215. [PubMed] [Google Scholar]
- 3.Mitchell L, Carter NE. An introduction to orthodontics. 1. Oxford, UK: Oxford University Press; 1996. pp. 23–25.https://www.worldcat.org/title/introduction-to-orthodontics/oclc/490069309?referer=di&ht=edition [Google Scholar]
- 4.Garvey MT, Barry HJ, Blake M. Supernumerary teeth – an overview of classification, diagnosis and management. J Can Dent Assoc. 1999;65(11):612–616. [PubMed] [Google Scholar]
- 5.Dăguci C, Burlibaşa M, Mărgărit R, Tănăsescu LA, Dăguci L, Bătăiosu M, Scrieciu M, Andrei OC. Maxillary distomolars: case reports, differential diagnosis and literature review. Rom J Morphol Embryol. 2017;58(4):1617–1622. [PubMed] [Google Scholar]
- 6.Scheiner MA, Sampson WJ. Supernumerary teeth: a review of the literature and four case reports. Aust Dent J. 1997;42(3):160–165. doi: 10.1111/j.1834-7819.1997.tb00114.x. [DOI] [PubMed] [Google Scholar]
- 7.Eigbobo JO, Osagbemiro BB. Bilateral tuberculate supernumerary teeth. Clin Pract. 2011;1(2):e30–e30. doi: 10.4081/cp.2011.e30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nirmala SVSG, Mallineni SK, Nuvvula S. Pre-maxillary hypo-hyperdontia: report of a rare case. Rom J Morphol Embryol. 2013;54(2):443–445. [PubMed] [Google Scholar]
- 9.Punathil S, Chandran N, Pai BHA, Gireesh L, Moyin S. Bilaterally erupted conical and tuberculate mesiodentes. SRM J Res Dent Sci. 2018;9(1):44–47. https://www.srmjrds.in/article.asp?issn=0976-433X;year=2018;volume=9;issue=1;spage=44;epage=47;aulast=Punathil [Google Scholar]
- 10.Andrei OC, Mărgărit R, Tănăsescu LA, Dăguci L, Farcaşiu C, Bătăiosu M, Dăguci C. A rare case of mandibulary parapremolars in siblings: case report and literature review. Rom J Morphol Embryol. 2017;58(4):1485–1490. [PubMed] [Google Scholar]
- 11.Andrei OC, Farcaşiu C, Mărgărit R, Dinescu MI, Tănăsescu LA, Dăguci L, Burlibaşa M, Dăguci C. Unilateral supplemental maxillary lateral incisor: report of three rare cases and literature review. Rom J Morphol Embryol. 2019;60(3):947–953. [PubMed] [Google Scholar]
- 12.Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumours. 2. Geneva, Switzerland: Springer-Verlag; 1992. pp. 7–9. [Google Scholar]
- 13.Pippi R. Odontomas and supernumerary teeth: is there a common origin. Int J Med Sci. 2014;11(12):1282–1297. doi: 10.7150/ijms.10501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rajab LD, Hamdan MAM. Supernumerary teeth: review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12(4):244–254. doi: 10.1046/j.1365-263x.2002.00366.x. [DOI] [PubMed] [Google Scholar]
- 15.De Oliveira Gomes C, Drummond SN, Jham BC, Abdo EN, Mesquita RA. A survey of 460 supernumerary teeth in Brazilian children and adolescents. Int J Paediatr Dent. 2008;18(2):98–106. doi: 10.1111/j.1365-263X.2007.00862.x. [DOI] [PubMed] [Google Scholar]
- 16.Umweni AA, Osunbor GEN. Non-syndrome multiple supernumerary teeth in Nigerians. Odontostomatol Trop. 2002;25(99):43–48. [PubMed] [Google Scholar]
- 17.Amarlal D, Muthu MS. Supernumerary teeth: review of literature and decision support system. Indian J Dent Res. 2013;24(1):117–122. doi: 10.4103/0970-9290.114911. [DOI] [PubMed] [Google Scholar]
- 18.Vichi M, Franchi L. Abnormalities of the maxillary incisors in children with cleft lip and palate. ASDC J Dent Child. 1995;62(6):412–417. [PubMed] [Google Scholar]
- 19.Türkkahraman H, Yilmaz HH, Cetin E. A non-syndrome case with bilateral supernumerary canines: report of a rare case. Dentomaxillofac Radiol. 2005;34(5):319–321. doi: 10.1259/dmfr/25079119. [DOI] [PubMed] [Google Scholar]
- 20.Niswander JD, Sujaku C. Congenital anomalies of teeth in Japanese children. Am J Phys Anthropol. 1963;21(4):569–574. doi: 10.1002/ajpa.1330210413. [DOI] [PubMed] [Google Scholar]
- 21.King NM, Tongkoom S, Itthagarun A, Wong HM, Lee CK. A catalogue of anomalies and traits of the primary dentition of southern Chinese. J Clin Pediatr Dent. 2008;32(2):139–146. doi: 10.17796/jcpd.32.2.w76653r22rnnn713. [DOI] [PubMed] [Google Scholar]
- 22.Huang WH, Tsai TP, Su HL. Mesiodens in the primary dentition stage: a radiographic study. ASDC J Dent Child. 1992;59(3):186–189. [PubMed] [Google Scholar]
- 23.Tsai SJ, King NM. A catalogue of anomalies and traits of the permanent dentition of southern Chinese. J Clin Pediatr Dent. 1998;22(3):185–194. [PubMed] [Google Scholar]
- 24.Van der Merwe AE, Steyn M. A report on the high incidence of supernumerary teeth in skeletal remains from a 19th century mining community from Kimberley, South Africa. SADJ. 2009;64(4):162–162; 164-166. [PubMed] [Google Scholar]
- 25.Fardi A, Kondylidou-Sidira A, Bachour Z, Parisis N, Tsirlis A. Incidence of impacted and supernumerary teeth – a radiographic study in a North Greek population. Med Oral Patol Oral Cir Bucal. 2011;16(1):e56–e61. doi: 10.4317/medoral.16.e56. [DOI] [PubMed] [Google Scholar]
- 26.Patil S, Maheshwari S. Prevalence of impacted and supernumerary teeth in the North Indian population. J Clin Exp Dent. 2014;6(2):e116–e120. doi: 10.4317/jced.51284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Salcido-García JF, Ledesma-Montes C, Hernández-Flores F, Pérez D, Garcés-Ortíz M. Frequency of supernumerary teeth in Mexican population. Med Oral Patol Oral Cir Bucal. 2004;9(5):407–409; 403–406. [PubMed] [Google Scholar]
- 28.Kara MI, Aktan AM, Ay S, Bereket C, Şener I, Bülbül M, Ezirganli Ş, Polat HB. Characteristics of 351 supernumerary molar teeth in Turkish population. Med Oral Patol Oral Cir Bucal. 2012;17(3):e395–e400. doi: 10.4317/medoral.17605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Harris EF, Clark LL. An epidemiological study of hyperdontia in American blacks and whites. Angle Orthod. 2008;78(3):460–465. doi: 10.2319/022807-104.1. [DOI] [PubMed] [Google Scholar]
- 30.Mukhopadhyay S, Biswas C, Haldar M, Roy P. Bilateral supernumerary primary maxillary canines. J Oral Res Rev. 2018;10(1):24–27. [Google Scholar]
- 31.Dos Santos APP, Ammari MM, Moliterno LFM, Júnior JC. First report of bilateral supernumerary teeth associated with both primary and permanent maxillary canines. J Oral Sci. 2009;51(1):145–150. doi: 10.2334/josnusd.51.145. [DOI] [PubMed] [Google Scholar]
- 32.Parker K, Hay N. A case report of a rare finding of supernumerary primary and permanent canines. J Int Oral Health. 2014;6(2):129–131. [PMC free article] [PubMed] [Google Scholar]
- 33.Abouei Mehrizi E, Semyari H, Eslami Amirabadi G. Bilateral mandibular supernumerary canines: a case report. J Dent Res Dent Clin Dent Prospects. 2010;4(4):140–140. doi: 10.5681/joddd.2010.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hume WJ. Supplemental canines. A case report. J Dent. 1973;1(6):261–262. doi: 10.1016/0300-5712(73)90101-2. [DOI] [PubMed] [Google Scholar]
- 35.Gellin ME. The distribution of anomalies of primary anterior teeth and their effect on the permanent successors. Dent Clin North Am. 1984;28(1):69–80. [PubMed] [Google Scholar]
- 36.Whittington BR, Durward CS. Survey of anomalies in primary teeth and their correlation with the permanent dentition. N Z Dent J. 1996;92(407):4–8. [PubMed] [Google Scholar]
- 37.Nik-Hussein NN, Abdul Majid Z. Dental anomalies in the primary dentition: distribution and correlation with the permanent dentition. J Clin Pediatr Dent. 1996;21(1):15–19. [PubMed] [Google Scholar]
- 38.Mukhopadhyay S, Mitra S. Anomalies in primary dentition: their distribution and correlation with permanent dentition. J Nat Sci Biol Med. 2014;5(1):139–143. doi: 10.4103/0976-9668.127313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kumar DK, Gopal KS. An epidemiological study on supernumerary teeth: a survey on 5,000 people. J Clin Diagn Res. 2013;7(7):1504–1507. doi: 10.7860/JCDR/2013/4373.3174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Anthonappa RP, King NM, Rabie ABM. Aetiology of supernumerary teeth: a literature review. Eur Arch Paediatr Dent. 2013;14(5):279–288. doi: 10.1007/s40368-013-0082-z. [DOI] [PubMed] [Google Scholar]
- 41.Weller JM. Evolution of mammalian teeth. J Paleontol. 1968;42(2):268–290. https://www.jstor.org/stable/1302214 [Google Scholar]
- 42.Babu V, Nagesh KS, Diwakar NR. A rare case of hereditary multiple impacted normal and supernumerary teeth. J Clin Pediatr Dent. 1998;23(1):59–61. [PubMed] [Google Scholar]
- 43.Levine N. The clinical management of supernumerary teeth. J Can Dent Assoc. 1962;28(5):297–303. [Google Scholar]
- 44.Batra P, Duggal R, Parkash H. Non-syndromic multiple supernumerary teeth transmitted as an autosomal dominant trait. J Oral Pathol Med. 2005;34(10):621–625. doi: 10.1111/j.1600-0714.2005.00271.x. [DOI] [PubMed] [Google Scholar]
- 45.Sedan HO, Gorlin RJ. Familial occurrence of mesiodens. Oral Surg Oral Med Oral Pathol. 1969;27(3):360–361. doi: 10.1016/0030-4220(69)90366-1. [DOI] [PubMed] [Google Scholar]
- 46.Mallineni SK, Jayaraman J, Yiu CKY, King NM. Concomitant occurrence of hypohyperdontia in a patient with Marfan syndrome: a review of the literature and report of a case. J Investig Clin Dent. 2012;3(4):253–257. doi: 10.1111/j.2041-1626.2012.00148.x. [DOI] [PubMed] [Google Scholar]
- 47.Ferrante MI, Giorgio G, Feather SA, Bulfone A, Wright V, Ghiani M, Selicorni A, Gammaro L, Scolari F, Woolf AS, Sylvie O, Bernard L, Malcolm S, Winter R, Ballabio A, Franco B. Identification of the gene for oral-facial-digital type I syndrome. Am J Hum Genet. 2001;68(3):569–576. doi: 10.1086/318802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Parolia A, Kundabala M, Dahal M, Mohan M, Thomas MS. Management of supernumerary teeth. J Conserv Dent. 2011;14(3):221–224. doi: 10.4103/0972-0707.85791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Proff P, Fanghänel J, Allegrini S, Bayerlein T, Gedrange T. Problems of supernumerary teeth, hyperdontia or dentes supernumerarii. Ann Anat. 2006;188(2):163–169. doi: 10.1016/j.aanat.2005.10.005. [DOI] [PubMed] [Google Scholar]
- 50.Demiriz L, Durmuşlar MC, Misir AF. Prevalence and characteristics of supernumerary teeth: a survey on 7348 people. J Int Soc Prev Community Dent. 2015;5(Suppl 1):S39–S43. doi: 10.4103/2231-0762.156151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Cortés-Bretón-Brinkmann J, Martínez-Rodríguez N, Barona-Dorado C, Martín-Ares M, Sanz-Alonso J, Suárez-García MJ, Prados-Frutos JC, Martínez-González JM. Clinical repercussions and epidemiological considerations of supernumerary canines: a 26 case series. Med Oral Patol Oral Cir Bucal. 2019;24(5):e615–e620. doi: 10.4317/medoral.23035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Mali S, Karjodkar FR, Sontakke S, Sansare K. Supernumerary teeth in non-syndromic patients. Imaging Sci Dent. 2012;42(1):41–45. doi: 10.5624/isd.2012.42.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Scanlan PJ, Hodges SJ. Supernumerary premolar teeth in siblings. Br J Orthod. 1997;24(4):297–300. doi: 10.1093/ortho/24.4.297. [DOI] [PubMed] [Google Scholar]
- 54.Koch H, Schwartz O, Klausen B. Indications for surgical removal of supernumerary teeth in the premaxilla. Int J Oral Maxillofac Surg. 1986;15(3):273–281. doi: 10.1016/s0300-9785(86)80085-0. [DOI] [PubMed] [Google Scholar]
- 55.Foley J. Surgical removal of supernumerary teeth and the fate of incisor eruption. Eur J Paediatr Dent. 2004;5(1):35–40. [PubMed] [Google Scholar]
- 56.Di Biase DD. The effects of variations in tooth morphology and position on eruption. Dent Pract Dent Rec. 1971;22(3):95–108. [PubMed] [Google Scholar]
- 57.Witsenburg B, Boering G. Eruption of impacted permanent upper incisors after removal of supernumerary teeth. Int J Oral Surg. 1981;10(6):423–431. doi: 10.1016/s0300-9785(81)80079-8. [DOI] [PubMed] [Google Scholar]