

Abstract
The goal of this project was to explore and to statistically evaluate the responsible gastrointestinal (GI) factors that are significant factors in explaining the systemic exposure of ibuprofen, between and within human subjects. In a previous study, we determined the solution and total concentrations of ibuprofen as a function of time in aspirated GI fluids, after oral administration of an 800 mg IR tablet (reference standard) of ibuprofen to 20 healthy volunteers in fasted state conditions. In addition, we determined luminal pH and motility pressure recordings that were simultaneously monitored along the GI tract. Blood samples were taken to determine ibuprofen plasma levels. In this work, an in-depth statistical and pharmacokinetic analysis was performed to explain which underlying GI variables are determining the systemic concentrations of ibuprofen between (inter-) and within (intra-) subjects. In addition, the obtained plasma profiles were deconvoluted to link the fraction absorbed with the fraction dissolved. Multiple linear regressions were performed to explain and quantitatively express the impact of underlying GI physiology on systemic exposure of the drug (in terms of plasma Cmax/AUC and plasma Tmax). The exploratory analysis of the correlation between plasma Cmax/AUC and the time to the first phase III contractions postdose (TMMC-III) explains ~40% of the variability in plasma Cmax for all fasted state subjects. We have experimentally shown that the in vivo intestinal dissolution of ibuprofen is dependent upon physiological variables like, in this case, pH and postdose phase III contractions. For the first time, this work presents a thorough statistical analysis explaining how the GI behavior of an ionized drug can explain the systemic exposure of the drug based on the individual profiles of participating subjects. This creates a scientifically based and rational framework that emphasizes the importance of including pH and motility in a predictive in vivo dissolution methodology to forecast the in vivo performance of a drug product. Moreover, as no extensive first-pass metabolism is considered for ibuprofen, this study demonstrates how intraluminal drug behavior is reflecting the systemic exposure of a drug.
Keywords: aspiration/motility study, in vivo dissolution, local drug concentration in the GI tract, ibuprofen, immediate release, bioequivalence, bioavailability, oral absorption, motility, manometry
Graphical Abstract
INTRODUCTION
In vivo predictive dissolution methods (iPD) should incorporate the main characteristics of the “gold standard human dissolution beaker” (i.e., the human gastrointestinal (GI) tract) into an in vitro device to achieve accurate and meaningful predictions. On the other hand, from a historical point of view, the “human beaker” has been the accepted test to demonstrate bioequivalence (BE)1,2 by comparing plasma Cmax and the area under the curve (AUC) of both reference and generic drug products in a predefined confidence interval (typically 80–125%).3 Nevertheless, one of the major causes of systemic variability in plasma Cmax after oral administration of drug products can be explained by differences in oral drug behavior along the GI tract. An iPD in vitro method aims to grasp the luminal conditions affecting in vivo dissolution and, thus, in vivo absorption. To achieve this purpose, it is necessary to gain direct insights into the in vivo dissolution behavior along the GI tract.4
BE is an integral part of FDA’s approval standard for proposed generic drug products (it helps to ensure a generic drug product works in the same way and provides the same clinical benefit as its brand-name version).
The biopharmaceutics classification system (BCS) sets forth a set of circumstances where BE may be established using in vitro studies as opposed to in vivo studies. BCS exists because in vivo dissolution is not the rate-limiting step for drug absorption in case of BCS class 1 and 3 fast dissolving drug products.5 Establishing BE with in vitro studies in accordance with BCS could be extended to class 2 and 4 drugs if an adequate in vitro dissolution methodology would be able to match in vivo dissolution. Such an iPD test coupled with a mass transport model (MTM) could become the essential tool to predict in vivo absorption and ensure BE. Obtaining drug concentrations in the GI segments after administration of a drug formulation of a class 2 drug could help to identify the physiological and physicochemical parameters that must be incorporated into the iPD test.6
The aim of this work is to explore the impact of motility events and luminal pH on the oral absorption rate of ibuprofen in the fasted state to ascertain how much of the observed variability in plasma levels is determined by the variability in luminal conditions in the GI lumen. The preliminary condition to reach any conclusion is to confirm that the experimental design (mainly the intubation procedure) is not affecting ibuprofen oral pharmacokinetics. This information will be essential to incorporate into an MTM in order to predict oral absorption from luminal levels and to improve our current gastrointestinal simulator (GIS) design.7–10
Ibuprofen is a weak acid drug (BCS class 2a; pKa ≈ 4.85) with an extremely low solubility in the stomach. This implies that the oral absorption is depending upon gastric emptying of ibuprofen in the small intestine, where dissolution and permeation will take place in the more neutral pH environment. Once it arrives in the intestine, the ibuprofen dissolution rate depends on the luminal pH and on the available small bowel volume. As ibuprofen can easily permeate the intestinal wall, its dissolution in vivo is the main limiting factor for its absorption.11
In fasted state subjects, complete gastric emptying depends on the strong burst contractions during phase III of the interdigestive migrating motor complex (MMC) propagating from stomach throughout the small intestine, thus moving the stomach content forward. The impact of the motility phase at the time of administration on gastric emptying of solids and drug formulations has been already pointed out.12–15 As subjects were dosed randomly with regard to the motility phase, the time until the next phase III contraction will also randomly vary. In consequence, the arrival of a relevant percentage of the ibuprofen dose to the intestine (where pH will drive dissolution) will be very different across subjects, adding variability to the plasma Cmax As an initial approach to delineate the relevance of the motility phase on ibuprofen absorption, the parameter selected was the time postdose to the next phase III contractions. The time of drug administration in relation to the next MMC wave could determine the arrival of most of the ibuprofen dose in the small intestine, as dissolution in the stomach is negligible.16,17
To link the intestinal variables with the observed plasma profiles, we measured ibuprofen concentrations in the stomach, duodenum, and jejunum after the oral administration of the reference standard ibuprofen to support the hypothesis of the impact of intestinal events in plasma profiles. The analysis of intestinal levels will serve to capture patterns that can be incorporated into an MTM to predict the systemic outcome of the drug product.
The clinical data analyzed in this study has been previously published. In the work of Koenigsknecht et al, data from the clinical study are presented and qualitatively described.18 Hens et al. mainly focused on buffer strength and performed a preliminary analysis, pointing out some hypotheses about relevant physiological variables.17 The present paper includes a statistical approach to identify relevant variables based on multiple-linear-correlation analyses as well as a basic mechanistic approach (i.e., fraction dissolved versus fraction absorbed) to demonstrate the in vivo dissolution versus in vivo systemic input correlation, respectively. Plasma profiles were deconvoluted to assess the fraction absorbed of ibuprofen for each individual Multiple linear regressions were performed to explain and quantitatively express the impact of underlying GI physiology on systemic exposure of the drug (in terms of plasma Cmax/AUC and plasma Tmax). With the small intestine handled as a flow-through cell, an estimation of the fraction dissolved was carried out for each individual and plotted with the corresponding fraction absorbed. In a final set of experiments, we characterized the solid state of the oral drug product that was found undissolved in the gastric, duodenal, and jejunal aspirates of subject B005-F2.
MATERIAL AND METHODS
Chemicals.
Ibuprofen tablets (800 mg, reference standard) were obtained from Dr. Reddy’s Laboratories Inc. (Shreveport, LA; IBU—Ibuprofen Tablets, USP, 800 mg, Lot no. 400603) through the University of Michigan Hospital. Phenol red was obtained from U.S. Pharmacopeia (Rockville, MD). Trifluoro-acetic acid (TFA), formic acid, methanol, and acetonitrile were obtained from Fisher Scientific Inc. (Pittsburgh, PA). All chemicals were of analytical grade or HPLC grade.
Clinical Study.
The study was held at the University of Michigan Hospital after receiving approval by the internal review board at both the University of Michigan and FDA (HUM00085066) under project number HHSF223201310144C. The study design was recently described by Hens and colleagues.17 Briefly, 13 healthy volunteers (9 men and 4 women) were recruited to explore the GI behavior of ibuprofen after oral administration of the IR tablet of ibuprofen; 7 out of 13 subjects participated in the study twice to generate intrasubject variability data. All volunteers provided written informed consent to participate in this study. After a fasting period, a multilumen GI tube from MUI Scientific (body length = 292 cm; external diameter = 7 mm; Mississauga, Ontario) was introduced via the mouth to the small intestine. The tube consisted of four independent aspiration ports located 20–30 cm apart and 16 manometry ports located proximal to the aspiration ports. Additionally, the catheter had a channel to fit a (0.035 in × 450 cm) guidewire (Boston Scientific, Marlborough, MA) as well as a channel connected to a balloon that could be filled with 7 mL of water to assist in tube placement. Finally, the end of the catheter was weighted with 7.75 g of tungsten weights.
Abdominal fluoroscopy was performed to ensure the GI tube was properly positioned in the different regions of the GI tract (i.e., stomach, duodenum, proximal and distal jejunum). The subject was asked to remain in bed while the GI tube was equilibrated by performing a baseline GI motility test for approximately 3–5 h (Medical Measurement Systems (MMS), Williston, Vermont). Prior to administration of the ibuprofen tablet, an intravenous catheter was introduced in the antecubital area of the subject for blood collection. The catheter was kept open with heparin and saline solution. The subjects were asked to empty his/her urine bladder prior to the start of the study. At approximately 4:00 AM, the subject was given a single oral dose of ibuprofen (800 mg tablet). The study drug was administered with 250 mL of water containing USP grade phenol red (0.1 mg/mL). The actual amount of water consumed was measured and recorded. Volunteers were not obliged to drink the total amount of administered water to avoid any feeling of nausea at the start of the study. After the administration of the tablet and the water, GI samples (i.e., stomach, duodenum, and jejunum) were collected at 0, 0.25, 0.5, 0.75, 1, 1.5, 2, 2.5, 3, 4, 5, 6, and 7 h. No meal was administered during the aspiration study. Plasma samples (4 mL/time point) were collected at 0, 0.167, 0.33, 0.5, 0.75, 1, 1.5, 2, 2.5, 3, 4, 5, 6, 7, 8, 12, and 28 h. The pH values of the GI fluid samples were immediately measured and recorded. The GI fluid samples were centrifuged at a speed of 17 000g for 10 min, and the supernatant was placed in the new tube for drug concentration analysis. All samples were stored in the −80 °C freezer until analysis of ibuprofen and phenol red.
Ibuprofen LC–MS/MS Analytical Method.
Blood samples were added to venous blood collections tubes (K2-EDTA (spray-dried), 7.2 mg), and plasma was separated from blood samples by centrifugation and stored at −80 °C. All samples (i.e., GI fluids and plasma) were analyzed according to an accurate and precise bioanalysis LC–MS/MS method as described in detail by Hens et al.17 The reader is referred to that specific manuscript. Accuracy and precision (<15%) met the FDA requirements for bioanalytical method validation.19
Interpretation of the Phase III Motility Event after Dosing Ibuprofen to the Subject.
MMC phase III motility periods were identified from the water-perfused manometric measurements using spectral density estimation and penalized logistic regression as described in detail by Hens and colleagues.17 Briefly, motility patterns were analyzed and classified as follows: powerful antral phase III contractions were defined as the regular occurrence of at least 2 contractions per minute for a period of no less than 2 min with an average amplitude of 75 mmHg. Duodenal phase III contractions are characterized by a rate of at least 11 contractions per minute with an average amplitude of 33 mmHg lasting at least 3 min.16 The time of appearance of phase III postdose activity was an important physiological variable responsible for empty a large quantity of drug product from the stomach into the small intestine.17
pH Determination of the Aspirated GI Fluids.
Immediately after aspiration of the GI fluids, pH was measured ex vivo using a pH electrode (Mettler InLab Micro Pro, Mettler-Toledo LLC, Columbus, OH), suitable for measuring pH in small or large volumes.
Pharmacokinetic Analysis of the Individual Plasma Profiles.
Noncompartmental analysis of the individual ibuprofen plasma levels was performed in Phoenix WinNonlin Version 7 (Princeton, NJ). To perform the compartmental model analysis, intravenous (IV) ibuprofen plasma data were retrieved from the literature:
15 min IV infusion of a 360 mg dose20
5–7 min IV infusion of an 800 mg dose21
5 min IV infusion of an 800 mg dose and 30 min IV infusion of an 800 mg dose22
To predict ibuprofen pharmacokinetic disposition, one-compartment and two-compartment open models were fitted to each set of data. Curve fitting was performed in Microsoft Excel (Redmond, WA) with the PKsolver add-in macro.23 Mean parameters from the four literature IV data sets were used for deconvolution. The goodness of fit was assessed with the sum of squared residuals (SS) and the correlation coefficient (R); the model comparison was done with Akaike’s information criteria (AIC), correlation coefficient R, and Snedecor’s F value (Table S.1 of the Supporting Information).24 The intravenous plasma profiles from the literature used to obtain ibuprofen disposition parameters are represented in Figure S.1 from Supporting Information.
Deconvolution of Plasma Profiles To Determine the Fraction Absorbed.
Fractions of absorbed ibuprofen after oral administration were estimated in each subject from their plasma levels with Wagner–Nelson and Loo–Riegelman methods implemented in Microsoft Excel (Redmond, WA) with the previously estimated parameters and by numerical deconvolution in Phoenix WinNonlin Version 7 (Princeton, NJ).25 Fractional absorption rates were estimated by linear interpolation from time to time in the fraction absorbed versus time curves. The fraction absorbed (Fabs) of ibuprofen was plotted against the fraction dissolved (Fdiss) of ibuprofen in the intestinal tract for each volunteer. The Fdiss was determined by handling the small intestinal tract as a flow-through cell with a “virtual” flow of 1 mL/min. Amounts dissolved at each time interval were calculated as intestinal concentrations multiplied by the flow rate and the time interval. The flow rate of intestinal contents in the upper small intestine can be variable. However, a flow rate of 1 mL/min is reasonably well in line with the published findings in humans by Kerlin et al.26 This flow rate is used to transform concentrations into amounts in a given interval, which are accumulated and then transformed into fractions divided by the maximal concentration; thus, the fractions would have been the same regardless of the selected flow. Accumulated amounts over time were used to estimate the Fdiss in each subject. The Fdiss for the entire 7 h of sampling for each individual can be calculated by
| (1) |
Linear Correlation between Plasma Cmax/AUC and Physiological Variables.
Several multiple-linear correlations were attempted between plasma Cmax/AUC and different physiological variables summarized in Table S.2 of the Supporting Information. Predictor variables were tested individually and in combinations of two variables and their corresponding interaction. Preliminary analysis was done in Microsoft Excel (Redmond, WA), and the automatic linear modeling was executed in SPSS V.22 with a forward stepwise variable inclusion method and model selection based on Akaike’s information criteria (AIC). Analysis of variance of regression was considered significant at p < 0.05.
Polarized Optical Microscopy (POM) Studies To Evaluate the Morphology of the Oral Drug Product of Ibuprofen in Human Aspirated Fluids.
To detect solid drug product in aspirated fluids, gastric and intestinal aspirated fluids of subject B005-F2 were evaluated by polarized optical microscopy (POM).10 All microscopy studies were conducted at room temperature (22–23 °C) using an inverted optical microscope (Nikon, Diaphot-TMD, Melville, NY) with 10× and 20× Nomarski objectives. Experiments were performed in a 96-well plate by adding 300 μL of aspirated fluid. Pictures were taken to visualize solid drug product. Control experiments were performed for (i) blank fluids where oral drug product was added to the fluid and visualized by microscopy to detect the drug product (positive control) and for (ii) blank aspirated fluids (i.e., aspirated fluids containing no drug product) as such (negative control). A full wave plate filter was used in conjunction with crossed polarizers to enhance the optical features of some of the samples for image collection. Images were collected with a Spot Insight FireWire 4 Megasample Color Mosaic camera controlled with Spot software (Sterling Heights, MI).
RESULTS
The main noncompartmental pharmacokinetic parameters are summarized in Table 1. Ibuprofen intravenous plasma levels from several references were used to characterize ibuprofen disposition parameters to perform deconvolution by Wagner–Nelson and Loo–Riegelman methods and numerical deconvolution in PhoenixWinNonlin Version 7 (Princeton, NJ). Table 2 summarizes the average one- and two-compartment disposition parameters.
Table 1.
Noncompartmental Pharmacokinetic Analysisa
| Subject | terminal slope (h−1) | plasma Tmax (h) | plasma Cmax (μg/mL) | Clast (μg/mL) | AUClast (μg/mL*h) | Vz_F_obs (L) | CLF_obs (L/h) | volume intake (mL)18 |
|---|---|---|---|---|---|---|---|---|
| B003V1 | 1.5 | 78 | 59.000 | 104 | 150 | |||
| B004V1 | 0.22 | 3 | 89.7 | 0.568 | 469 | 7.81 | 1.70 | 240 |
| B004V2 | 0.26 | 4 | 61.1 | 0.424 | 448 | 6.91 | 1.78 | 249 |
| B005V1 | 0.33 | 5 | 45.2 | 0.098 | 351 | 7.01 | 2.28 | 250 |
| B005V2 | 0.29 | 4 | 38 | 0.145 | 294 | 9.28 | 2.72 | 250 |
| B006V1 | 0.31 | 2 | 68.3 | 0.067 | 292 | 8.83 | 2.74 | 250** |
| B017V1 | 0.25 | 2.5 | 77.4 | 0.143 | 252 | 12.6 | 3.16 | 209 |
| B017V2 | 0.28 | 4 | 65.1 | 0.156 | 363 | 7.79 | 2.20 | 218 |
| B042V1 | 0.25 | 2 | 67.872 | 0.100 | 284 | 11.2 | 2.81 | 239 |
| B042V2 | 0.37 | 2 | 44.7 | 2.48 | 201 | 10.3 | 3.86 | 250 |
| B044V1 | 0.27 | 3 | 61.172 | 0.069 | 275 | 10.8 | 2.91 | 305 |
| B049V1 | 0.23 | 3 | 28.1 | 3.18 | 97.9 | 31 | 7.16 | 265 |
| B049V2 | 0.22 | 4 | 31.1 | 0.074 | 138 | 25.7 | 5.77 | 250 |
| B052V1 | 0.04 | 3 | 47.4 | 9.86 | 374 | 30.4 | 1.34 | 220 |
| B053V1 | 0.22 | 2 | 63.6 | 0.157 | 268 | 13.5 | 2.98 | 250 |
| B055V1 | 0.20 | 1 | 84.3 | 0.241 | 320 | 12.3 | 2.49 | 200 |
| B055V2 | 0.18 | 1.5 | 81.2 | 0.270 | 283 | 15.6 | 2.81 | 249 |
| B063V1 | 8 | 37 | 0.084 | 217 | 3.70 | 247 | ||
| B065V1 | 0.27 | 1 | 47.5 | 0.030 | 168 | 17.4 | 4.76 | 247 |
| B065V2 | 0.23 | 3 | 48.2 | 0.067 | 179 | 19.7 | 4.45 | 247 |
| Average * | 0.25 | 2.98 | 58.2 | 0.96 ** | 269 | 14.4 | 3.24 | 239.25 |
| SD | 0.07 | 1.58 | 17.9 | 2.26 | 100 | 7.46 | 1.41 | 30.17 |
| CV% | 27.3 | 53.0 | 30.8 | 235 | 37.4 | 52.0 | 43.6 | 12.61 |
Plasma Cmax: maximum plasma concentration; Clast: last observed plasma concentration; AUClast: area under the curve from time zero up to the last observed concentration; AUCinf: area under the curve from time zero to infinity; F: oral bioavailability; CL/F: apparent oral plasma clearance; V/F: apparent oral distribution volume
average excluding B003V1 data.
additional intake of 480 mL in 30 min postdose.
Table 2.
Average Pharmacokinetic Parameters after Intravenous Administration of Ibuprofen from References 15, 16, and 17a
| parameter | value | parameter | value |
|---|---|---|---|
| k10 (1/h) (1/h) | 0.79 | k10 (1/h) | 0.63 |
| k12 (1/h) | 2.79 | V (L) | 7.51 |
| k21 (1/h) | 3.73 | CL (L/h) | 4.66 |
| Vc (L) | 5.23 | ||
| CL (L/h) | 4.06 | ||
| two-compartment parameters | one-compartment parameters | ||
k10: elimination rate constant from central compartment; k12 and k21: access and return from peripheral compartment rate constants, respectively; V: distribution volume; Vc: central compartment distribution volume; CL: plasma clearance.
Figure 1 summarizes the comparison of the plasma Cmax values obtained in this study with the average plasma Cmax values across 99 different clinical trials of immediate-release ibuprofen oral products. All plasma Cmax values are normalized by the administered dose.
Figure 1.

Comparison between the average plasma Cmax in fasted state conditions as observed in our study (20 individual data sets) versus what has been published in the literature (average of n = 99 clinical studies from ref 27), demonstrated by boxplots (corrected for 800 mg dose).27
Plasma Cmax and AUC values in each subject are depicted in Figure 2 ranked by order of magnitude. Some subjects present data from two visits. These plots allow visual evaluation of the variability between and within subjects.
Figure 2.
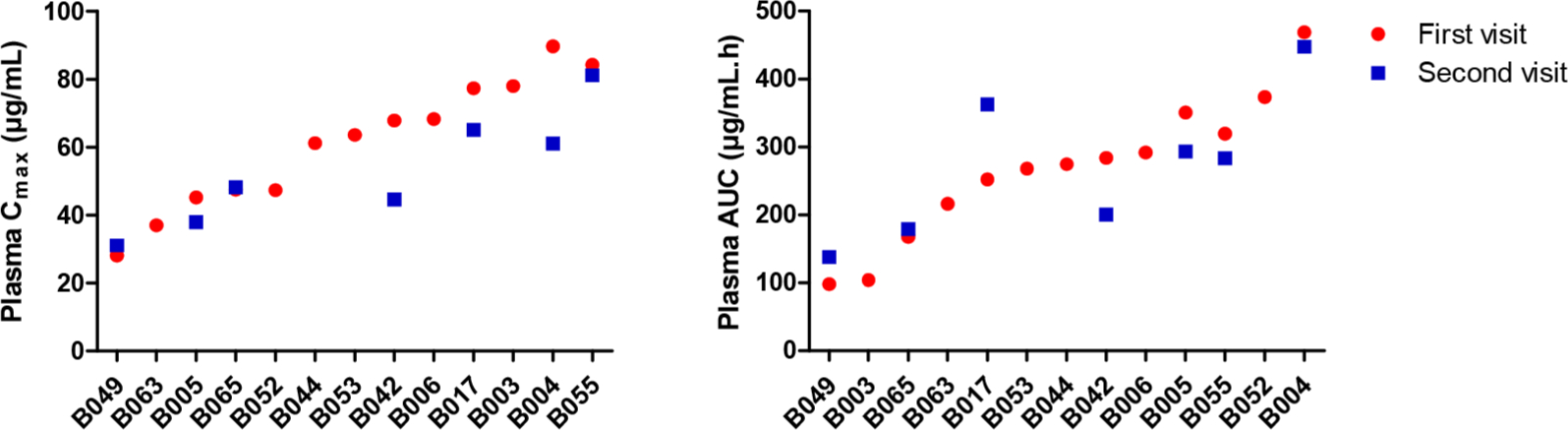
AUC0–28h and plasma Cmax in each subject. Circles represent data from the first visit, and squares display data from the second visit in the same subject (intrasubject data).
Figure 3 summarizes the average duodenal (top graph) and jejunal (bottom graph) pH values across subjects. The pH values fluctuate remarkably in the duodenum and less in the jejunum. Duodenal and jejunal ibuprofen concentrations are represented in the same plots with the pH values to explore the relationship between luminal pH and ibuprofen dissolution. These same variables are represented by the standard deviation in Figure S.2 of the Supporting Information to illustrate the interindividual variability.
Figure 3.
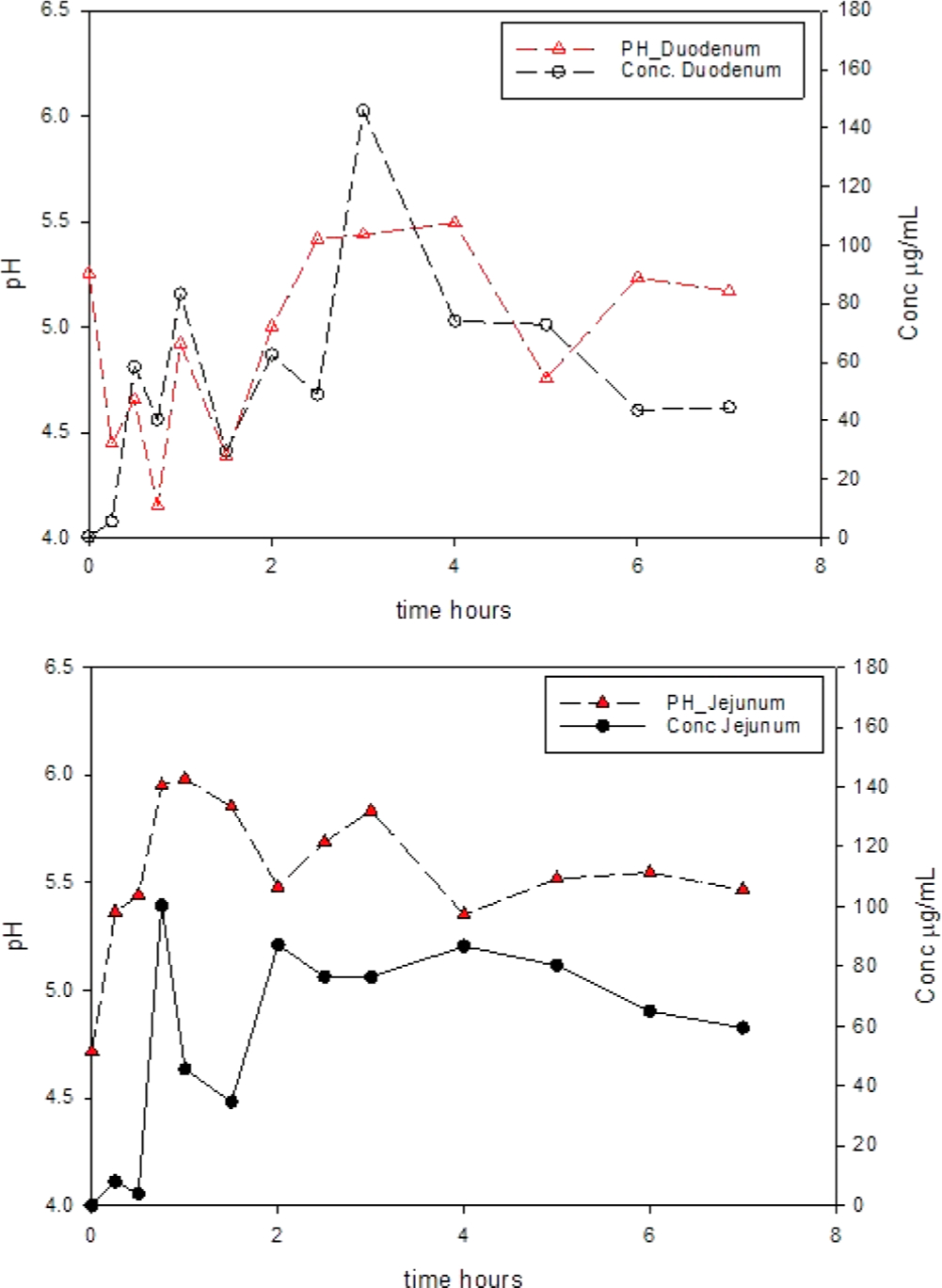
Average pH values (mean values across 19 data sets at each time point) in the duodenum (top) and jejunum (bottom) as a function of time (h) and average duodenal (top) and jejunal (bottom) ibuprofen solution concentrations (μg/mL) versus time.
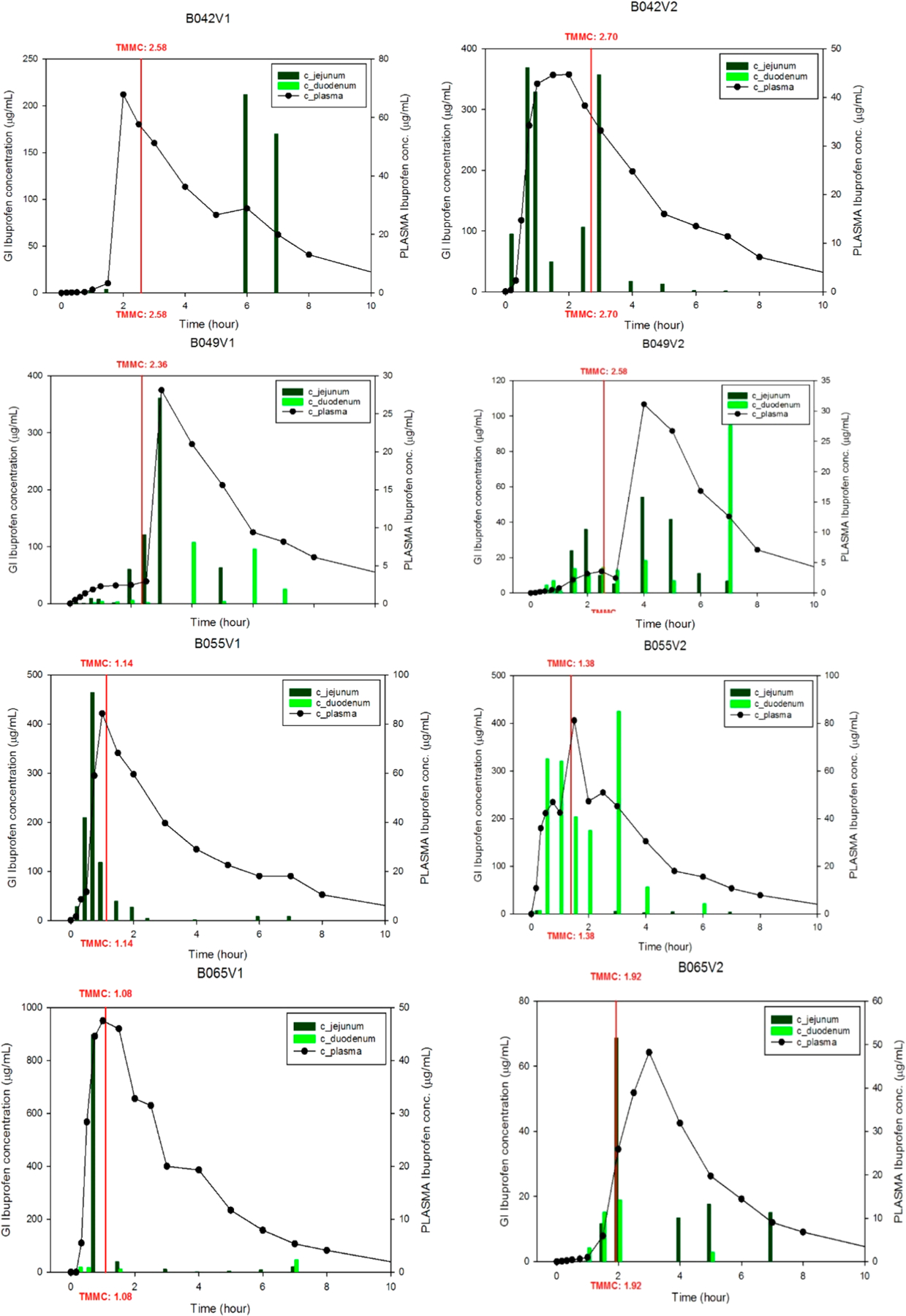
Individual ibuprofen plasma levels and luminal concentrations in the duodenum and jejunum are represented in Figures 4-1–4-3. The time to the next phase III wave postdose was plotted in each graph to show the correlation with plasma Tmax and Cmax as well as with the luminal concentrations.
Figure 4–1.
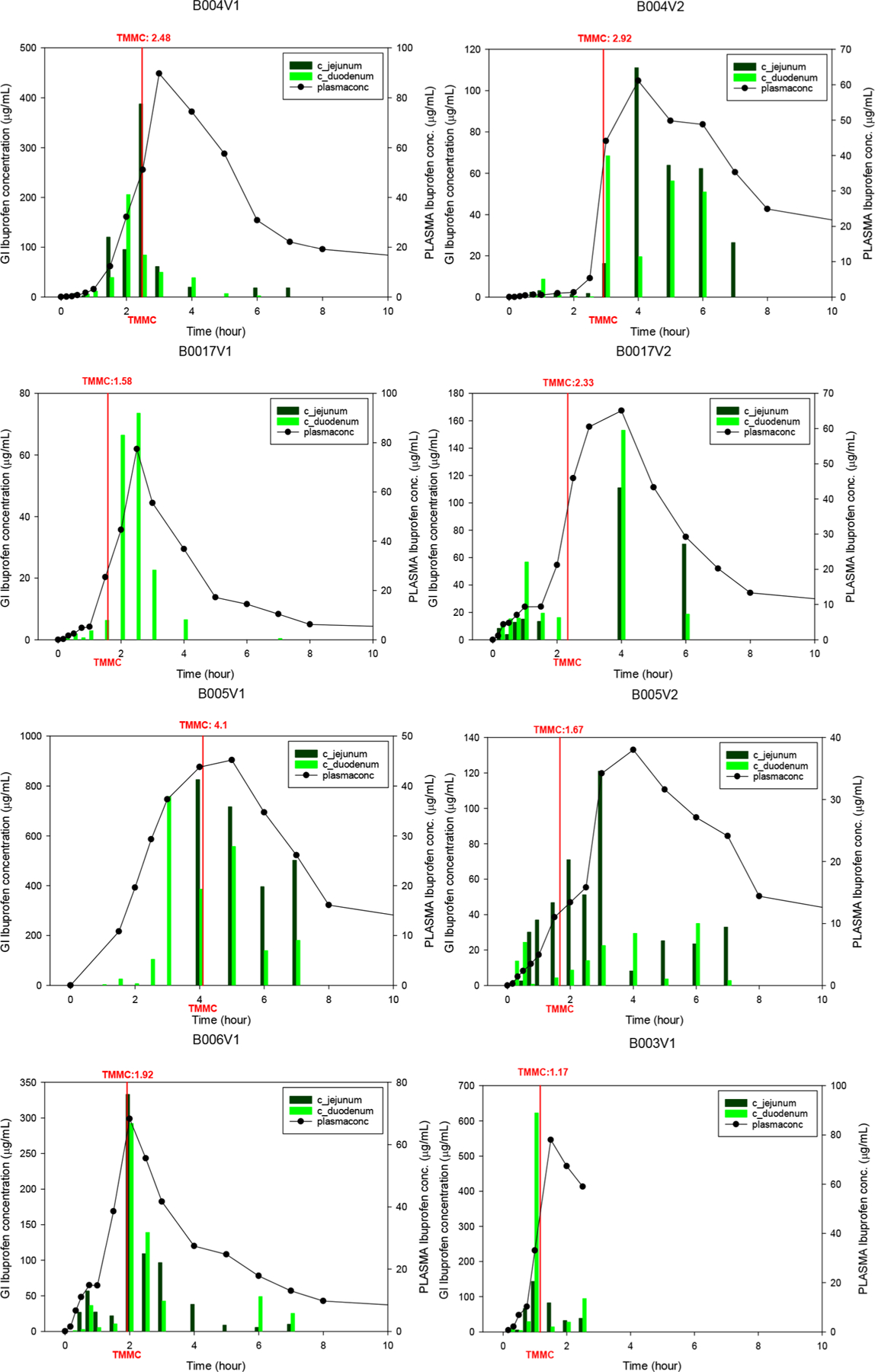
Individual ibuprofen plasma concentrations (black dots) up to 12 h, plotted with ibuprofen concentrations in the duodenum and jejunum up to 8 h. Time to phase III contractions postdose (TMMC ) is given by the red line.
Figure 4–3.
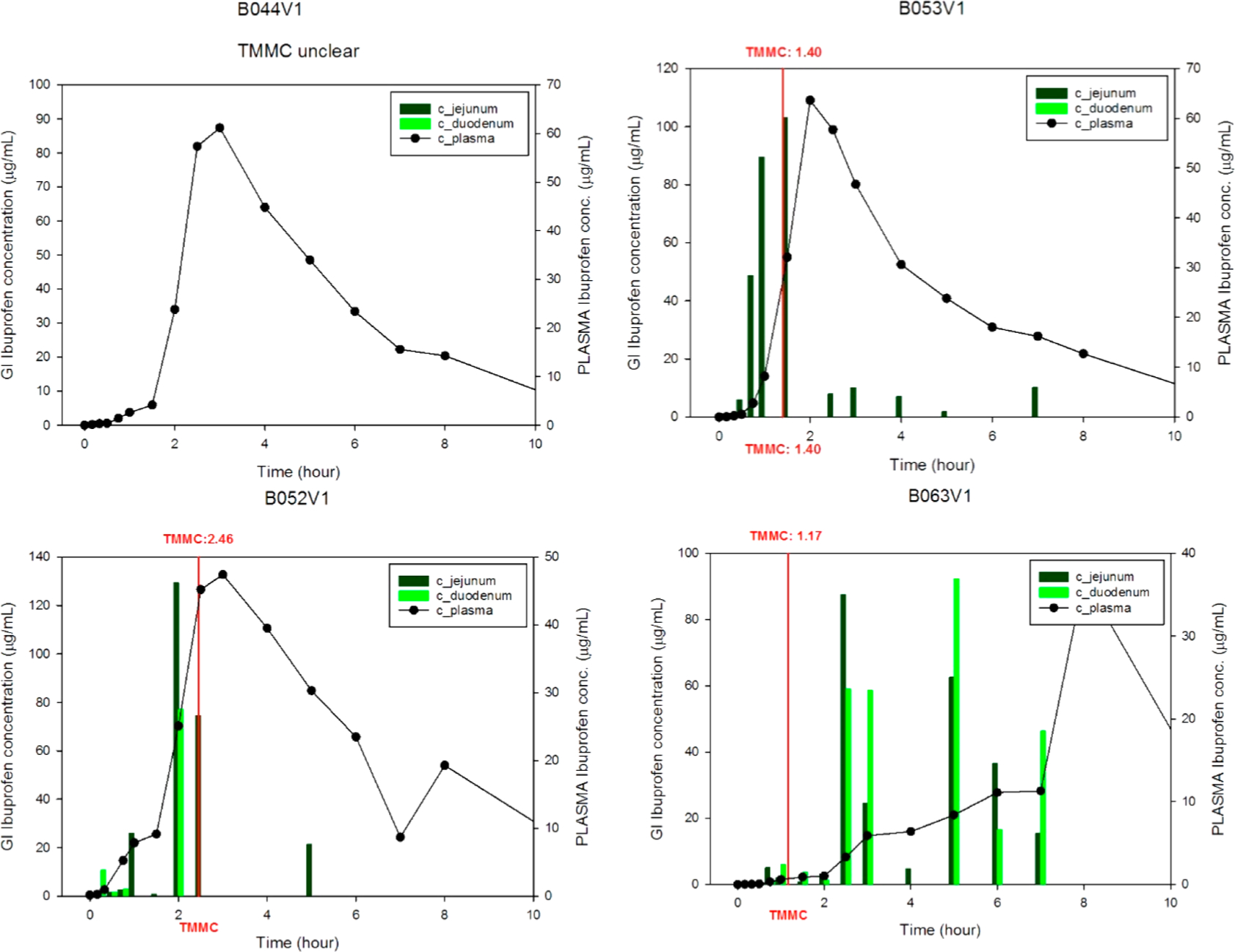
Individual ibuprofen plasma concentrations (black dots) up to 12 h, plotted with ibuprofen concentrations in the duodenum and jejunum up to 8 h. Time to phase III contractions postdose (TMMC) is given by the red line.
Figure 5 depicts the relationship between the average absorption rates (estimated from plasma levels) and the luminal concentrations. Absorption rates were estimated by linear interpolation on the fraction absorbed versus time profiles from Loo–Riegelman mass balance analysis. Figure S.3 of the Supporting Information summarizes the individual normalized absorption rates and individual normalized ibuprofen intestinal luminal concentrations to show the consistent correlation between individuals. The individual deconvoluted profiles with Wagner–Nelson or Loo–Riegelman methods are represented in Figure S.4 of the Supporting Information.
Figure 5.
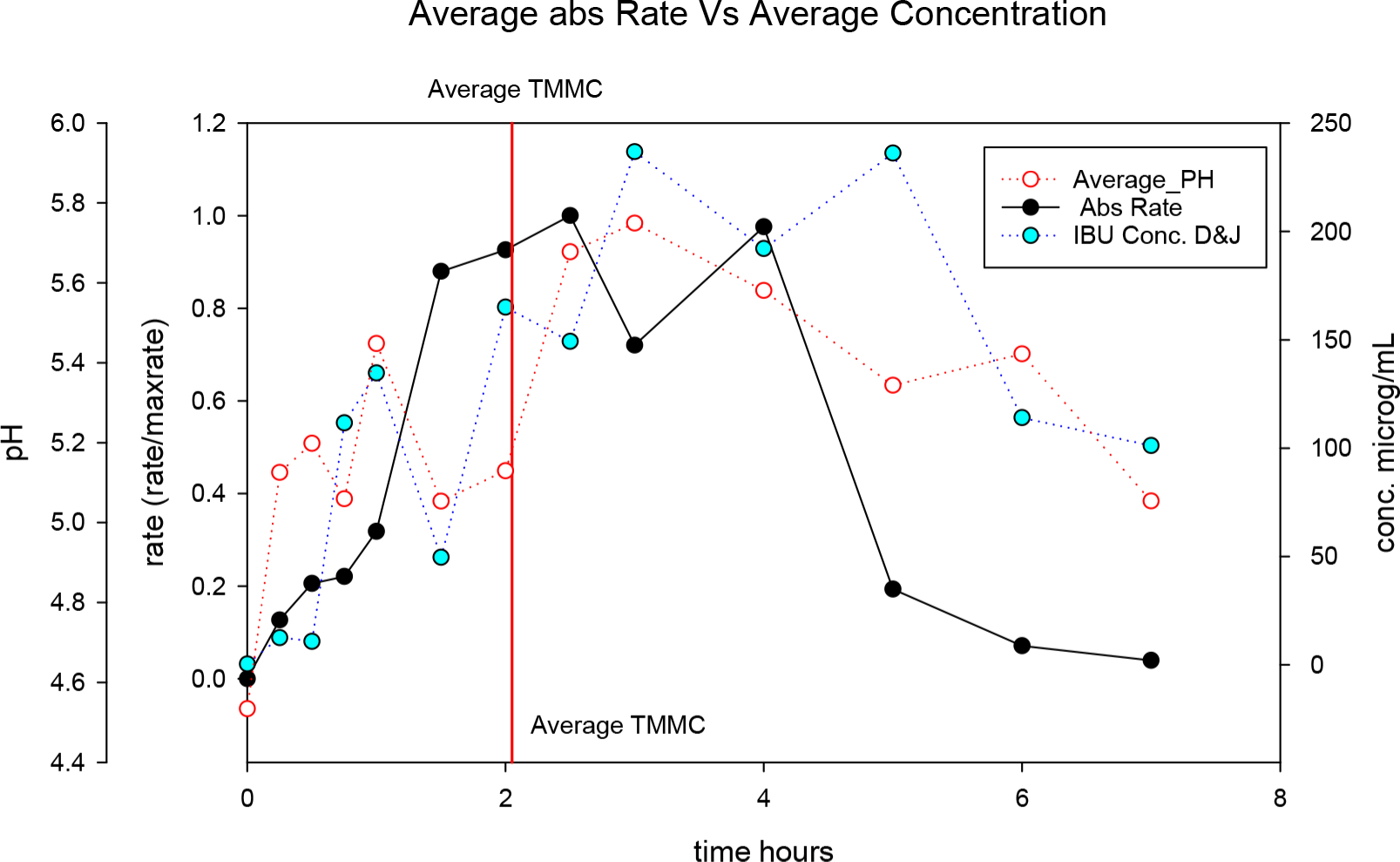
Ibuprofen absorption rates (normalized rates) versus time profile obtained from plasma levels and luminal dissolved ibuprofen concentrations (average value of duodenum and jejunum) as a function of time. Average duodenal/jejunal pH is also represented as well as the average TMMC postdose (red line).
To confirm that the intraluminal behavior of the drug is an adequate reflection of the systemic exposure, the calculated fraction absorbed, deconvoluted from the plasma concentrations at the different time points, was plotted as a function of the fraction dissolved at the different time points of aspiration. This was done for all fasted state subjects, and the outcome of the linear regression is depicted in Figure 6.
Figure 6.

Linear regression analysis of the fraction absorbed (Fabs) as a function of the fraction dissolved (Fdiss). The regression line is given by the black line.
These data clearly demonstrate how the fraction dissolved explains the fraction of ibuprofen that will be absorbed and appearing in blood (for 85%).
The only statistically significant correlation found included time to phase III contractions (TMMC) and average stomach pH from 0 to 7 h (STM_pH), with p < 0.029 and R2 = 0.45
| (2) |
Nevertheless, the slope of the STM_pH predictor was not statistically different from zero. Consequently, time to the next phase III contractions postdose (TMMC) was the physiological variable that presented a direct linear correlation with Cmax/AUC with an R2 value of 0.37, meaning nearly 40% of Cmax/AUC variability can be explained by this motility-related parameter. Following this conclusion, the relationship of TMMC and other pharmacokinetic parameters was explored.
Figure 7 summarizes an exploratory analysis of the raw experimental data. The upper left plot shows plasma Cmax versus Tmax values. The upper right plot represents the ibuprofen plasma Cmax values versus the time elapsed between drug administration and the next phase III propagating contractions in the stomach. Both linear correlations were significant (p < 0.05). The overall trend observed in the upper right plot indicated a lower plasma Cmax value whenever the next phase III contractions would appear later. The faster the drug will be removed out of the stomach with a strong burst of contractions (phase III), the faster the dissolution and absorption process can occur in the upper small intestine. This likely explains the correlation between the time to phase III contractions postdose and the appearance of the maximal concentration of ibuprofen in plasma (Cmax). The same concept is supported by the plot of plasma Tmax versus the time of phase III contractions’ appearance postdose (TMMC-III): those subjects with delayed elapsed times between drug administration and phase III contractions also have delayed plasma Tmax values. The line in the bottom plots represents the identity line for comparison. The time needed for 50% oral fraction absorbed (estimated from Wagner–Nelson plots) versus the time of phase III contractions’ appearance postdose (TMMC-III) presents a clear positive trend.
Figure 7.
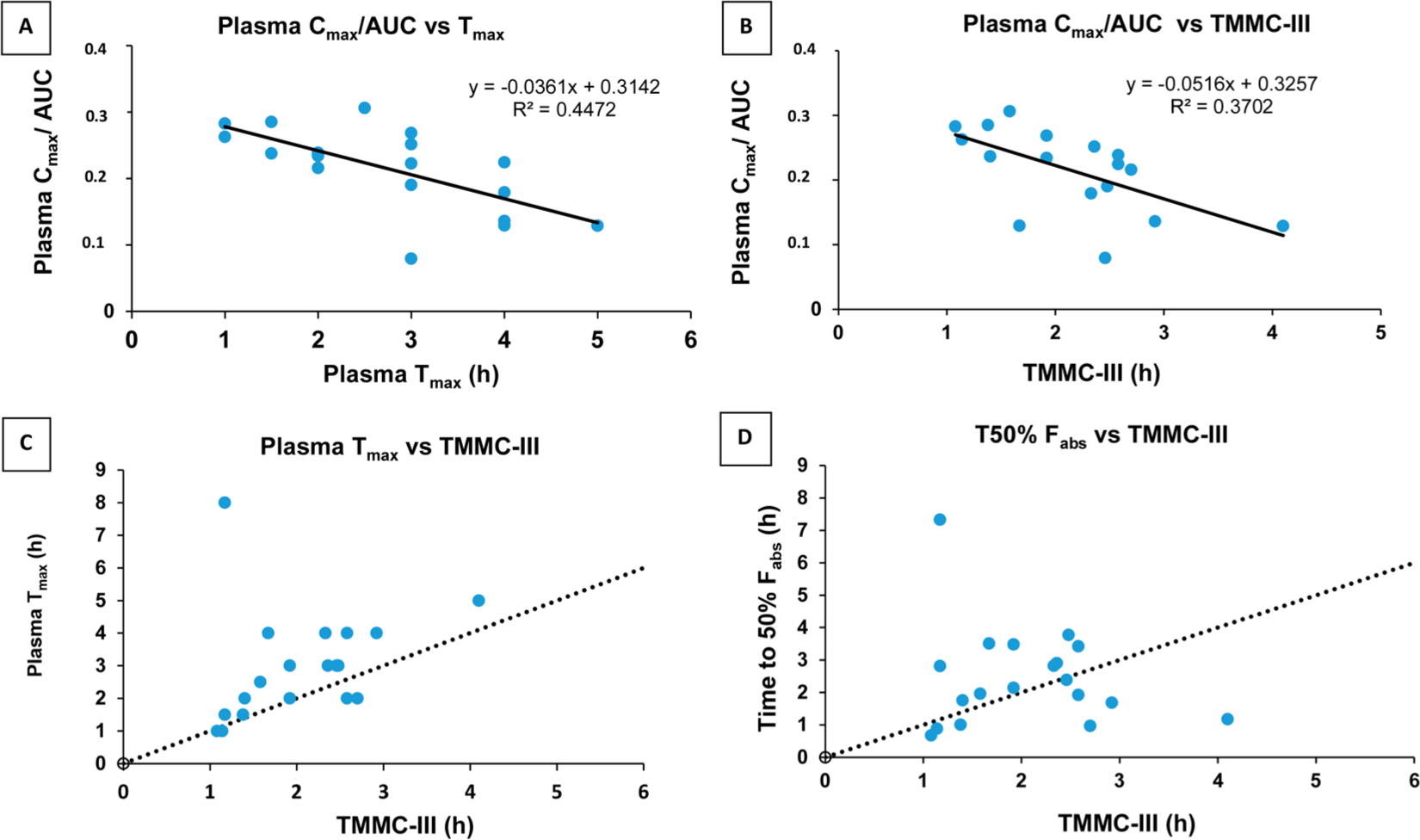
Exploratory data analysis. Top plots: Correlations between plasma Cmax (corrected by AUC) and (A) Tmax and (B) the time to the next phase III contractions postdose (TMMC-III). Bottom plots: (C) Correlation between plasma Tmax and the TMMC-III. (D) Correlation between time to 50% fraction absorbed and the TMMC-III. The dotted line in plots C and D corresponds to the identity line.
Polarized optical microscopy (POM) assisted us in visualizing the undissolved particles of drug product that were still present in the aspirated samples of subject B005-F2 (Figure 8). The shining structure is completely the same as the structure present in the IR tablet as given to the volunteers, suggesting the presence of undissolved particles of drug product in the GI fluids after tablet disintegration.
Figure 8.
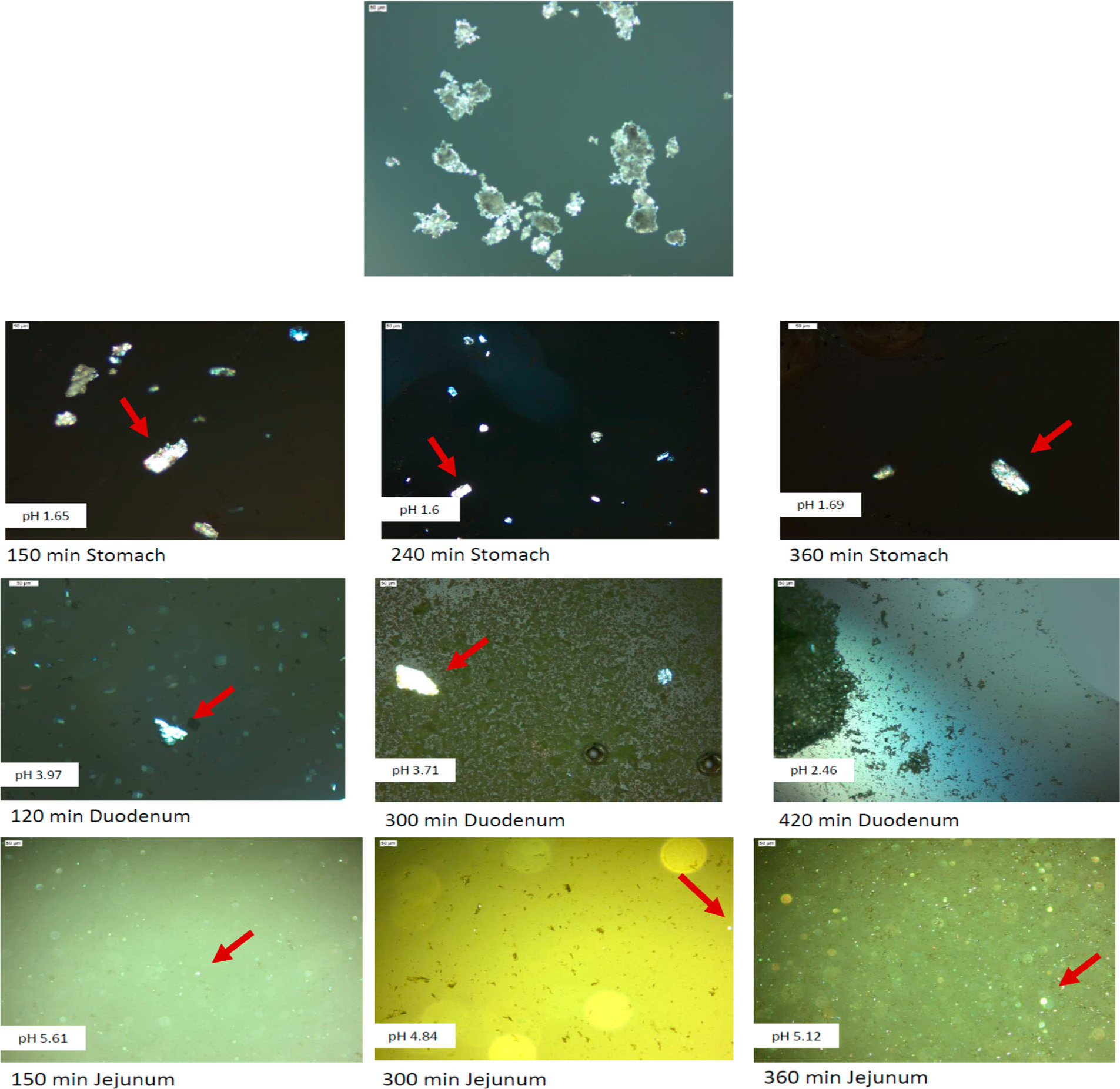
Microscopy images using polarized light to brighten up the undissolved orally administered drug product of ibuprofen (indicated by the red arrows) in human gastric, duodenal, and jejunal aspirated fluid after different time points. The top figure shows the microscopy image of the drug product itself, after crushing of the 800 mg IR Dr. Reddy’s tablet. Aspirated samples are derived from subject B005-F2.
DISCUSSION
The first question in this study is to ascertain whether the ibuprofen plasma concentrations observed in our population are consistent with other studies of the same drug and with the previously observed pharmacokinetic parameters to confirm that the intubation procedure was not affecting drug absorption and/or disposition. For instance, it is known that pain and discomfort can delay gastric emptying and thus affect the onset of drug absorption.28 In 1982, Müller-Lisner et al. already evaluated the impact of transpyloric tubes on gastric emptying, and no clinical effect was shown.29 The observed plasma Tmax values are on the range of literature values (0.4 to 4 h) for a wide range of ibuprofen doses and immediate-release formulations, even if in most studies the average value is around 2 h. Only one subject showed an extreme plasma Tmax value of 8 h; all of the other subjects presented values in the range mentioned in the literature, so a delay in plasma Tmax caused by intubation does not seem supported by the experimental data. Nevertheless, individual values can show a wide range of values in a fasted state from 0.25 to 5 h with immediate-release tablets.30 These same authors reported plasma Cmax values from 30 to 36 μg/mL for a 400 mg ibuprofen dose in line with our observed data. Apparent oral distribution volumes and clearances (V/F and CL/F, respectively) are, as well, consistent with the ranges of reported values (V/F from 7.7 to 14.7 L and CL/F from 2.87 to 3.6 L/h).27 Figure 1 summarized a comparison of plasma Cmax values from our study and a comprehensive review of 99 pharmacokinetic human studies of ibuprofen when administered as an IR oral dosage form. Additionally, inter and intrasubject variability in this study (28 and 14%, respectively) is similar to the observed variability in other BE studies.31
Moreover, Figure 1 shows that the total observed variability, between and within subjects, is remarkable. To explore which component is the predominant component, the individual plasma Cmax and AUC values are represented in Figure 2 for those individuals with repeated measurements. It is dear that the intrasubject variability is lower than the intersubject variability, as previously reported for this drug product.31
As the oral profiles obtained in this study presented reasonable similarity with other studies, IV reported data were used to perform the pharmacokinetic analysis and deconvolution of oral profiles under the assumption of similar disposition parameters. Table 2 shows the one- and two-compartment model parameters. The indexes of the goodness of fit (summarized in Table S.1 of the Supporting Information) demonstrated that a two-compartment model is better from a statistical point of view.24 Nevertheless, for the purpose of this paper, a one-compartment model was adequate and Wagner–Nelson and Loo–Riegelman deconvolution rendered similar profiles up to 5 h.
Ibuprofen is an acidic (pKa ≈ 4.85), low-solubility drug (intrinsic solubility = 68 μg/mL).32 Obviously, the dissolution rate depends on the luminal pH. As observed in Figure 3 (top), ibuprofen concentrations in the duodenum were increased when pH values were elevated. The duodenal concentration–time profile closely follows the pH versus time fluctuation. The same trend is observed in the jejunum (the bottom of Figure 3), representing the dissolved jejunal concentrations. The duodenal and jejunal concentrations did not reach ibuprofen solubility at the prevailing pH at any moment; thus, the driving force for dissolution was maintained thanks to the increase in solubility at higher pH values but also because of the ibuprofen disappearance by membrane permeation.33
Figure 4-1 summarizes the ibuprofen plasma levels in all volunteers. In each plot, the intestinal concentrations in both segments are represented. In most volunteers, the maximal luminal concentrations were observed around plasma Tmax at least in one intestinal segment (duodenum or jejunum). On the other hand, the appearance of postdose phase III contractions generally preceded plasma Cmax. These plots support the hypothesis that gastric emptying, mediated by the motility events, had a relevant impact on ibuprofen absorption, as it determines the arrival of the drug to the segment where dissolution is favored because of the higher pH values and where absorption takes place.12,13,34
Ibuprofen permeation through the intestinal membrane is driven by the drug solution concentrations in the luminal fluids (Fick’s Law).35 The absorption rate, consequently, must be higher when the luminal concentration increases. Figure 5 clearly shows the link between ibuprofen plasma levels and gastrointestinal events, which was the general purpose of this project. The absorption rates estimated from systemic ibuprofen concentrations are driven by luminal solution concentrations, the driving force for the permeation process. We have already demonstrated that individual plasma Tmax correlates well with the luminal Tmax (time at which maximal ibuprofen luminal average concentrations are observed in each subject).17 In addition, as can be observed in Figure 3, because of the weak acidic nature of the drug, luminal concentrations are determined by the luminal pH affecting the dissolution rate when the luminal pH will increase to more alkaline pH values caused by the pancreatic and mucosal secretions of bicarbonate in the upper small intestine. On top of that, the dissolution-limiting factor is the arrival of the solid drug product to the intestine, which happens slowly up to the time of phase III contractions when most of the drug is released in the intestine as observed in Figures 5 and 7.
To explore the relationship between motility expressed as the elapsed time from administration to the next phase III contractions, several correlations are depicted (Figure 6). The correlation between plasma Cmax and Tmax values is the expected correlation considering the relationship between these pharmacokinetic parameters expressed in the next equations for a one-compartmental model36
| (3) |
| (4) |
where ka represents the apparent first-order absorption rate constant, and kel represents the first-order elimination rate constant.
Assuming no change in the disposition parameter, kel, a slower absorption rate would lead to a longer plasma Tmax and consequently a lower plasma Cmax value. Correlation in the upper left plot of Figure 6 shows this trend with a reasonable variability (i.e., an R2 close to 0.5). The parameter represented is plasma Cmax over AUC to correct for the clearance variability across individuals, with the underlying assumption of a complete absorption in all of them. The plasma Cmax reflects not only the rate but also the extent of absorption and is highly correlated with the AUC. Therefore, the plasma Cmax/AUC ratio reflects better the differences in absorption rates.37In the case of ibuprofen, two factors could determine a slower apparent dissolution rate: gastric emptying has been mentioned earlier, and as it can be observed in the upper right plot, a longer TMMC seems also to be related to lower plasma Cmax values. The physiological and physicochemical explanation behind this observation would be that the dissolution of ibuprofen in the stomach is negligible, and ibuprofen needs to arrive at the small intestine with a higher prevailing pH in order to be dissolved (pH ≥ pKa). Most of the dose appears to enter the small intestine after the postdose phase III contractions, which is known as the house-keeper wave.16,38 Indeed, a good relationship is observed between plasma Tmax and TMMC. Those subjects with delayed elapsed times between drug administration and phase III contractions also have delayed plasma Tmax values. The time needed for 50% oral fraction absorbed (estimated from Wagner–Nelson plots) versus postdose phase III contractions presents the same positive correlation trend. A delayed gastric emptying is reflected in longer times to get 50% fraction absorbed. This preliminary analysis shows the clear connection between plasma levels and intestinal motility (gastric emptying). Up to 40% of Cmax variation is explained by the time to the phase III contractile wave. The house-keeper wave would likely stimulate gastric emptying of ibuprofen such that large quantities of ibuprofen enter the small intestine and dissolve. If this arrival in the small intestine is accompanied by a sufficient pH (pH ≥ pKa) to promote ibuprofen’s dissolution, we suggest that motility and pH are the major determinants for the appearance of plasma Cmax and Tmax of the drug.17 The pH variability and net fluid content could explain also partially the intersubject Cmax differences associated with the absorption process.
The observed variability in the time to appearance of postdose phase III contractions and pH values along the GI tract impacts the variability in the dissolution process of ibuprofen in the small intestine. To mimic this, the random nature/appearance of the phase III contractions postdose in relation to drug administration can be implemented in the in silico/in vitro models. In 25% of the subjects, gastric emptying follows a biphasic kinetic process.39 Gastric emptying has been recognized as the reason for variable absorption and double-peak phenomena in several pharmacokinetic profiles.40,41 However, in the current GIS, gastric emptying is mimicked following a first-order process. Obviously, this simplified approach does not capture completely the actual human variability, and some new mechanistic models have been proposed to describe gastric emptying and intestinal motility,12,14 suggesting that in some high-permeability drugs with short half-life values of gastric emptying could lead to BE Mures. The data in this work corroborate the huge variation in the appearance of postdose phase III contractions (values ranging between 1.17 and 4 h) and its impact on plasma Tmax and Cmax values.
The emptying of gastric fluids is neutralized by bicarbonate in pancreatic and intestinal secretions, but this process is also affected/triggered by motility (better known as “the secreto- motor complex”).42–44 In addition, the discontinuous distribution of fluids along the intestinal tract (available pockets) can originate small fluid volumes with very different pH values at any given moment. This scenario complicates the simulation of the in vivo dissolution of ionizable drugs. The present data show in each volunteer the fluctuation of pH, suggesting that irregular gastric emptying, incomplete mixing, and back and forward fluid movement cannot be completely buffered by the residual fluids. Future magnetic resonance imaging (MRI) studies should shed fight on these mechanisms to confirm this tentative hypothesis. It was recently demonstrated that the aspirated fluids derived from this study are characterized by a low buffer capacity.17 These pH fluctuations led to a slower dissolution of ibuprofen. If the low pH value coincides with the arrival of ibuprofen particles, then the nonfavorable environment for dissolution would determine a slower dissolution/absorption and, consequently, lower plasma Cmax values and delayed plasma Tmax times. That is the reason why ibuprofen was still measured in the aspirated GI samples even 6 h postdose. The presence of solid drug product was confirmed by the difference in solution and total concentrations of ibuprofen in the specific aspirated samples of subject B005-F2, as depicted in Figure 8.
The underlying hypothesis is that (i) ibuprofen dissolution in the stomach is negligible due to the acidic pH and that (ii) the drug particles, after tablet disintegration, will slowly empty until the next phase III contractile wave.45,46 The administered water (containing 0.1 mg/mL phenol red) was rapidly emptied from the stomach into the small intestine, based on intraluminal concentrations of the nonabsorbable marker phenol red that was added to the glass of water and in MR1 measurements exploring the gastric emptying of 250 mL of water.39,47 The fast gastric emptying of the administered water, containing phenol red, has recently been investigated and reported.47 To confirm, Grimm et al. noticed the same fast transfer of water after oral administration throughout the GI tract in fasted and fed state conditions.48 The pace of gastric emptying will be faster than the complete disintegration of the ibuprofen tablet, suggesting that the phase III contractions of the MMC will be extremely important to remove the majority of drug particles out of the stomach. The observed and strong correlations between the postdose burst of phase III contractions, plasma Tmax, plasma Cmax values, and time to 50% of Fabs support these hypotheses.
This study points out that gastric emptying and motility events (phase III) are relevant determinants of ibuprofen absorption as a BCS class Ha drug. Their relevance was investigated by a statistical approach. Characterizing the range of observed values could help to implement a set of in vitro gastric emptying parameters covering them, in order to study the formulation performance under the same expected gastric emptying profiles. Further, the observed in vivo pH values can also be reflected in the different intestinal segments of a multicompartment dissolution device, confirmed by the pH profiles as observed in vivo. To the extent of our knowledge, there is no aspiration study reported in the literature that performed such an in-depth statistical/mechanical analysis as described in this paper. Although results are not surprising, it is shown, for the first time, how pH and motility affect drug behavior along the GI, tract and this work demonstrates the impact on the systemic exposure from person to person. The impact of these factors is quantified by statistical analysis.
CONCLUSION
In summary, this work presents the experimental proof that in vivo dissolution of ibuprofen (BCS class 2a) depends on luminal pH and the present motility events at the time of dosage form administration. The relationship between luminal concentrations and plasma levels indicated that the time to the next MMC phase III (house-keeper wave) determines the arrival of most of the ibuprofen dose to the small intestine. Further, ibuprofen absorption rates into plasma are clearly governed by the intestinal ibuprofen solution concentrations, as they determine the driving force for the diffusion/permeation process through the intestinal membrane. These in vivo dissolution results and the information from the relevant physiological variables can be used to refine our current prototypes of the GIS and other predictive in vitro models as well as computational in silico models to adequately predict the systemic exposure of the drug from an oral product. For the first time, within- and between-subject variability in drug exposure was explained by motility and luminal pH. Moreover, a deconvolution method was applied to extract the fraction absorbed of ibuprofen for each individual These values were positively linked with the fraction dissolved throughout the GI tract. In addition, the application of POM is a promising tool to investigate the presence of solid/undissolved drug product in aspirated fluids and can inform us to a certain extent about the solid state of the drug product.
Supplementary Material
Figure 4–2.
Individual ibuprofen plasma concentrations (black dots) up to 12 h, plotted with ibuprofen concentrations in the duodenum and jejunum up to 8 h. Time to phase III contractions postdose (TMMC) is given by the red line.
ACKNOWLEDGMENTS
This work was supported by Grant No. HHSF223201510157C and Grant No. HHSF223201310144C by the U.S. Food and Drug Administration (FDA). This report represents the scientific views of the authors and not necessarily that of the FDA. Bart Hens would like to acknowledge the Internal Funds of KU Leuven (PDM/17/164) and the Council Research of Flanders (FWO: 12R2119N).
Footnotes
The authors declare no competing financial interest.
ASSOCIATED CONTENT
Supporting Information
The Supporting Information is available free of charge on the ACS Publications website at DOI: 10.1021/acs.molpharmaceut.8b00515.
Figure S.1: Ibuprofen intravenous data from several references used to characterize its pharmacokinetic (PK) parameters; Figure S.2: Average pH and solution concentration–time profiles in the duodenum and jejunum with associated standard deviations; Figure S.3: Individual fractional absorption rates obtained by point-to-point linear interpolation in Loo–Riegelman plots and normalized ibuprofen concentrations in solution measured in the lumen (duodenum + jejunum); Figure S.4: Loo–Riegelman and Wagner–Nelson individual deconvoluted profiles; Table S.1: Statistical comparison of one-compartment versus two-compartment pharmacokinetic models for ibuprofen after intravenous administration; Table S.2: Physiological variables used in the multiple-linear correlation analysis and experimental Cmax/AUC values (PDF)
REFERENCES
- (1).Yu LX; Amidon GL; Polli JE; Zhao H; Mehta MU; Conner DP; Shah VP; Lesko LJ; Chen M-L; Lee VHL; Hussain AS Biopharmaceutics classification system: the scientific basis for biowaiver extensions. Pharm. Res. 2002, 19, 921–925. [DOI] [PubMed] [Google Scholar]
- (2).Davit BM; Conner DP; Fabian-Fritsch B; Haidar SH; Jiang X; Patel DT; Seo PRH; Suh K; Thompson CL; Yu LX Highly variable drugs: observations from bioequivalence data submitted to the FDA for new generic drug applications. AAPS J. 2008, 10, 148–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (3).Chen M-L; Shah VP; Ganes D; Midha KK; Caro J; Nambiar P; Rocci ML; Thombre AG; Abrahamsson B; Conner D; Davit B; Fackler P; Farrell C; Gupta S; Katz R; Mehta M; Preskorn SH; Sanderink G; Stavchansky S; Temple R; Wang Y; Winkle H; Yu L Challenges and opportunities in establishing scientific and regulatory standards for determining therapeutic equivalence of modified-release products: Workshop summary report. Clin. Ther. 2010, 32, 1704–1712. [DOI] [PubMed] [Google Scholar]
- (4).Hens B; Corsetti M; Spiller R; Marciani L; Vanuytsel T; Tack J; Talattof A; Amidon GL; Koziolek M; Weitschies W; et al. Exploring Gastrointestinal Variables Affecting Drug and Formulation Behavior: Methodologies, Challenges and Opportunities. Int. J. Pharm. 2017, 519, 79–97. [DOI] [PubMed] [Google Scholar]
- (5).Amidon GL; Lennemäs H; Shah VP; Crison JR A Theoretical Basis for a Biopharmaceutic Drug Classification: The Correlation of in Vitro Drug Product Dissolution and in Vivo Bioavailability. Pharm. Res. 1995, 12, 413–420. [DOI] [PubMed] [Google Scholar]
- (6).Kourentas A; Vertzoni M; Stavrinoudakis N; Symillidis A; Brouwers J; Augustijns P; Reppas C; Symilhdes M An in vitro biorelevant gastrointestinal transfer (BioGIT) system for forecasting concentrations in the fasted upper small intestine: Design, implementation, and evaluation. Eur. J. Pharm. Sci. 2016, 82, 106–114. [DOI] [PubMed] [Google Scholar]
- (7).Tsume Y; Matsui K; Searls AL; Takeuchi S; Amidon GE; Sun D; Amidon GL The impact of supersaturation level for oral absorption of BCS class IIb drugs, dipyridamole and ketoconazole, using in vivo predictive dissolution system: Gastrointestinal Simulator (GIS). Eur. J. Pharm. Sci. 2017, 102, 126–139. [DOI] [PubMed] [Google Scholar]
- (8).Tsume Y; Takeuchi S; Matsui K; Amidon GE; Amidon GL In vitro dissolution methodology, mini-Gastrointestinal Simulator (mGIS), predicts better in vivo dissolution of a weak base drug, dasatinib. Eur. J. Pharm. Sci. 2015, 76, 203–212. [DOI] [PubMed] [Google Scholar]
- (9).Matsui K; Tsume Y; Takeuchi S; Searls A; Amidon GL Utilization of Gastrointestinal Simulator, an in Vivo Predictive Dissolution Methodology, Coupled with Computational Approach To Forecast Oral Absorption of Dipyridamole. Mol. Pharmaceutics 2017, 14, 1181–1189. [DOI] [PubMed] [Google Scholar]
- (10).Hens B; Bermejo M; Tsume Y; Gonzalez-Alvarez I; Ruan H; Matsui K; Amidon GE; Cavanagh K; Kuminek G; Benninghoff G Evaluation and optimized selection of supersaturating drug delivery systems of posaconazole (BCS class 2b) in the gastrointestinal simulator (GIS): An in vitro-in silico-in vivo approach. Eur. J. Pharm. Sci. 2018, 115, 258. [DOI] [PubMed] [Google Scholar]
- (11).Tsume Y; Langguth P; Garcia-Arieta A; Amidon GL In silico prediction of drug dissolution and absorption with variation in intestinal pH for BCS class II weak acid drugs: ibuprofen and ketoprofen. Biopharm. Drug Dispos. 2012, 33, 366–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (12).Talattof A; Price JC; Amidon GL Gastrointestinal Motility Variation and Implications for Plasma Level Variation: Oral Drug Products. Mol. Pharmaceutics 2016, 13, 557–567. [DOI] [PubMed] [Google Scholar]
- (13).Higaki K; Choe SY; Löbenberg R; Welage LS; Amidon GL Mechanistic understanding of time-dependent oral absorption based on gastric motor activity in humans. Eur. J. Pharm. Biopharm. 2008, 70, 313–325. [DOI] [PubMed] [Google Scholar]
- (14).Talattof A; Amidon GL Pulse Packet Stochastic Model for Gastric Emptying in the Fasted State: A Physiological Approach. Mol. Pharmaceutics 2018, 15, 2107. [DOI] [PubMed] [Google Scholar]
- (15).Kaus LC; Gillespie WR; Hussain AS; Amidon GL The effect of in vivo dissolution, gastric emptying rate, and intestinal transit time on the peak concentration and area-under-the-curve of drugs with different gastrointestinal permeabilities. Pharm. Res. 1999, 16, 272–280. [DOI] [PubMed] [Google Scholar]
- (16).Deloose E; Janssen P; Depoortere I; Tack J The migrating motor complex: control mechanisms and its role in health and disease. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 271–285. [DOI] [PubMed] [Google Scholar]
- (17).Hens B; Tsume Y; Bermejo M; Paixao P; Koenigsknecht MJ; Baker JR; [Google Scholar]
- (18).Hasler WL; Lionberger R; Fan J; Dickens J; Shedden K; Wen B; Wysocki J; Loebenberg R; Lee A; Frances A; Amidon G; Yu A; Benninghoff G; Salehi N; Talattof A; Sun D; Amidon GL Low Buffer Capacity and Alternating Motility along the Human Gastrointestinal Tract: Implications for in Vivo Dissolution and Absorption of Ionizable Drugs. Mol. Pharmaceutics 2017, 14, 4281–4294. [DOI] [PubMed] [Google Scholar]
- (18).Koenigsknecht MJ; Baker JR; Wen B; Frances A; Zhang H; Yu A; Zhao T; Tsume Y; Pai MP; Bleske BE; Zhang X; Lionberger R; Lee A; Amidon GL; Hasler WL; Sun D Vivo Dissolution and Systemic Absorption of Immediate Release Ibuprofen in Human Gastrointestinal Tract under Fed and Fasted Conditions. Mol. Pharmaceutics 2017, 14, 4295–4304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (19).Food & Drug Administration. Bioanalytical Method Validation: Guidance for Industry; 2001.
- (20).Chassard D; Geneteau A; Gualano V; Brault M Bioequivalence study of two Ibuprofen formulations administered intravenously in healthy male volunteers. Clin. Drug Invest. 2004, 24, 739–747. [DOI] [PubMed] [Google Scholar]
- (21).Pavliv L; Voss B; Rock A Pharmacokinetics, safety, and tolerability of a rapid infusion of i.v. ibuprofen in healthy adults. Am. J. Health-Syst. Pharm. 2011, 68, 47–51. [DOI] [PubMed] [Google Scholar]
- (22).Smith HS; Voss B Pharmacokinetics of intravenous ibuprofen: implications of time of infusion in the treatment of pain and fever. Drugs 2012, 72, 327–337. [DOI] [PubMed] [Google Scholar]
- (23).Zhang Y; Huo M; Zhou J; Xie S PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Comput. Methods Programs Biomed 2010, 99, 306–314. [DOI] [PubMed] [Google Scholar]
- (24).Ludden TM; Beal SL; Sheiner LB Comparison of the Akaike Information Criterion, the Schwarz criterion and the F test as guides to model selection. J. Pharmacokinet. Biopharm. 1994, 22, 431–445. [DOI] [PubMed] [Google Scholar]
- (25).González-García I; Mangas-Sanjuan V; Merino-Sanjuán M; Bermejo M In vitro-in vivo correlations: general concepts, methodologies and regulatory applications. Drug Dev. Ind. Pharm. 2015, 41, 1935–1947. [DOI] [PubMed] [Google Scholar]
- (26).Kerlin P; Zinsmeister A; Phillips S Relationship of motility to flow of contents in the human small intestine. Gastroenterology 1982, 82, 701–706. [PubMed] [Google Scholar]
- (27).Davies NM Clinical pharmacokinetics of ibuprofen. The first 30 years. Clin. Pharmacokinet. 1998, 34, 101–154. [DOI] [PubMed] [Google Scholar]
- (28).Almukainzi M; Jamali F; Aghazadeh-Habashi A; Löbenberg R Disease specific modeling: Simulation of the pharmacokinetics of meloxicam and ibuprofen in disease state vs. healthy conditions. Eur. J. Pharm. Biopharm. 2016, 100, 77–84. [DOI] [PubMed] [Google Scholar]
- (29).Müller-Lissner SA; Fimmel CJ; Will N; Müller-Duysing W; Heinzel F; Blum AL Effect of gastric and transpyloric tubes on gastric emptying and duodenogastric reflux. Gastroenterology 1982, 83, 1276–1279. [PubMed] [Google Scholar]
- (30).Bienert A; Szkutnik-Fiedler D; Dyderski S; Grześkowiak E; Drobnik L; Wolc A; Slawinska U Comparative bioavailability study of two ibuprofen preparations after oral administration in healthy volunteers. Arzneim. Forsch. 2006, 56, 647–651. [DOI] [PubMed] [Google Scholar]
- (31).Wagener HH; Vögtle-Junkert U Intrasubject variability in bioequivalence studies illustrated by the example of ibuprofen. Int. J. Clin Pharmacol Ther 1996, 34, 21–31. [PubMed] [Google Scholar]
- (32).Krieg BJ; Taghavi SM; Amidon GL; Amidon GE In vivo predictive dissolution: transport analysis of the C02, bicarbonate in vivo buffer system. J. Pharm. Sci 2014, 103, 3473–3490. [DOI] [PubMed] [Google Scholar]
- (33).Miyaji Y; Fujii Y; Takeyama S; Kawai Y; Kataoka M; Takahashi M; Yamashita S Advantage of the Dissolution/Permeation System for Estimating Oral Absorption of Drug Candidates in the Drug Discovery Stage. Mol. Pharmaceutics 2016, 13, 1564–1574. [DOI] [PubMed] [Google Scholar]
- (34).Sheng JJ; Kasim NA; Chandrasekharan R; Amidon GL Solubilization and dissolution of insoluble weak acid, ketoprofen: effects of pH combined with surfactant. Eur. J. Pharm. Sci. 2006, 29, 306–314. [DOI] [PubMed] [Google Scholar]
- (35).Karpman VL [The theoretical analysis of Fick’s equation. On the centennial of the use of Fick’s principle in physiology], Z. Kardiol 1975, 64, 801–808. [PubMed] [Google Scholar]
- (36).Rowland M; Tozer TN Clinical pharmacokinetics and pharmacodynamics: concepts and applications, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, 2010. [Google Scholar]
- (37).Endrenyi L; Fritsch S; Yan W Cmax/AUC is a clearer measure than Cmax for absorption rates in investigations of bioequivalence. Int. J. Clin Pharmacol Ther Toxicol 1991, 29, 394–399. [PubMed] [Google Scholar]
- (38).Cassilly D; Kantor S; Knight LC; Maurer AH; Fisher RS; Sender J; Parkman HP Gastric emptying of a non-digestible solid: assessment with simultaneous SmartPill pH and pressure capsule, antroduodenal manometry, gastric emptying scintigraphy. Neurogastroenterol. Motil. 2008, 20, 311–319. [DOI] [PubMed] [Google Scholar]
- (39).Mudie DM; Murray K; Hoad CL; Pritchard SE; Garnett MC; Amidon GL; Gowland PA; Spiller RC; Amidon GE; Marciani L Quantification of gastrointestinal liquid volumes and distribution following a 240 mL dose of water in the fasted state. Mol. Pharmaceutics 2014, 11, 3039–3047. [DOI] [PubMed] [Google Scholar]
- (40).Oberle RL; Amidon GL The influence of variable gastric emptying and intestinal transit rates on the plasma level curve of cimetidine; an explanation for the double peak phenomenon. J. Pharmacokinet. Biopharm. 1987, 15, 529–544. [DOI] [PubMed] [Google Scholar]
- (41).Ogungbenro K; Pertinez H; Aarons L Empirical and semi-mechanistic modelling of double-peaked pharmacokinetic profile phenomenon due to gastric emptying. AAPS J. 2015, 17, 227–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (42).Vantrappen GR; Peeters TL; Janssens J The Secretory Component of the Interdigestive Migrating Motor Complex in Man. Scand. J. Gastroenterol 1979, 14, 663–667. [DOI] [PubMed] [Google Scholar]
- (43).Layer P; Chan AT; Go VL; DiMagno EP Human pancreatic secretion during phase II antral motility of the interdigestive cycle. Am. J. Physiol. 1988, 254, G249–253. [DOI] [PubMed] [Google Scholar]
- (44).Layer P; Chan AT; Go VL; Zinsmeister AR; DiMagno EP Cholinergic regulation of phase II interdigestive pancreatic secretion in humans. Pancreas 1993, 8, 181–188. [DOI] [PubMed] [Google Scholar]
- (45).Gruber P; Rubinstein A; Li VH; Bass P; Robinson J R Gastric emptying of nondigestible solids in the fasted dog. J. Pharm. Sci. 1987, 76, 117–122. [DOI] [PubMed] [Google Scholar]
- (46).Graham DY; Lacey Smith J; Jones RD; Rakhit A; Tipnis V; Hurley ME Gastroscopic localization of a microencapsulated KC1 preparation in the human stomach. Gastrointest. Enclose. 1987, 33, 220–223. [DOI] [PubMed] [Google Scholar]
- (47).Paixão P; Bermejo M; Hens B; Tsume Y; Dickens J; Shedden K; Salehi N; Koenigsknecht MJ; Baker JR; Hasler WL; Lionberger R; Fan J; Wysocki J; Wen B; Lee A; Frances A; Amidon GE; Yu A; Benninghoff G; Löbenberg R; Talattof A; Sun D; Amidon GL Gastric emptying and intestinal appearance of nonabsorbable drugs phenol red and paromomycin in human subjects: A multi-compartment stomach approach. Eur. J. Pharm. Biopharm. 2018, 129, 162–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (48).Grimm M; Scholz E; Koziolek M; Kühn J-P; Weitschies W Gastric Water Emptying under Fed State Clinical Trial Conditions Is as Fast as under Fasted Conditions. Mol. Pharmaceutics 2017, 14, 4262. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.