

Abstract
This study examined the relationship between safety margin and force level during an isometric push task in a lateral pinch posture. Ten participants grasped an aluminum- or rubber-finished object using a lateral pinch posture and exerted 20%, 40%, 60%, 80%, and 100% of maximum push force while voluntary grip force was recorded. Then minimum required grip force was measured for each push force level. Mean safety margin, the difference between voluntary and minimum required grip forces, was 25% MVC when averaged for all push levels. Safety margin significantly increased with increasing push force for both grip surfaces. Grip force used during maximum push exertion was only 74% lateral pinch grip MVC. Possible underlying mechanisms for increasing safety margin with increasing push force are discussed as well as the implication of this finding to ergonomic analysis.
Statement of Relevance
This study demonstrates that ergonomic analyses of push tasks that involve friction force should account for safety margin and reduced grip strength during push. Failure to consider safety margin and reduced grip strength during push can result in overestimation of people’s push capability.
Keywords: safety margin, lateral pinch, hand, grip force, push
1. Introduction
Push force exertions using friction between the hand and a grasped object in a lateral pinch posture are frequently performed in daily living. Some examples are inserting a key or a plug, opening/closing zippers (Smaby et al., 2004), stabbing foodstuffs with a fork and a knife, and opening an umbrella manually. Push force exertions using hand-object friction are also performed for teleoperated microsurgery (Preising et al., 1991), propulsion of a manual wheelchair (Richter et al., 2006), and automotive assembly operations (Grieshaber and Armstrong, 2007).
During push, it is important to use sufficient grip force to secure the grip. If grip force is less than minimally required, it can result in hand slippage leading to hand injury. Malker (1991) reported that slippery handles and hands sliding onto the blades of knives were a major cause of injuries in a meat processing plant. The Department of Trade and Industry (1997) reported that consumers get injured while trying to open difficult packages using knives. To avoid such hand slippage and injury during push tasks, people may use grip force that is higher than minimally required, but low enough to prevent fatigue (Rohmert, 1973; Bystrom and Fransson-Hall, 1994) and cumulative trauma disorders (Bystrom and Kilbom, 1990; NRC, 1999; NRC and IOM, 2001). The difference between the minimum required grip force and voluntary grip force can be referred to as safety margin (Johansson and Westling, 1984).
Safety margin has previously been studied extensively in lifting tasks only. It has been shown that during lifting tasks, safety margin is affected by grip posture (McDonnell et al., 2005), anticipation (Edin et al., 1992; Flanagan and Wing, 1997; Jenmalm and Johansson, 1997; Westling and Johansson, 1984), disturbance in sensory input (Cole and Abbs, 1988; Westling and Johansson, 1984), compression or blockage of the median nerve (Cole et al., 2003; Dun et al., 2007; Lowe and Freivalds, 1999), aging (Kinoshita and Francis, 1996; Cole et al., 1999), sweat (Zackrisson et al., 2008), and neurological disorder such as stroke (Blennerhassett, et al., 2006; Hermsdorfer et al., 2003). Unfortunately, these previous studies investigated only low pinch grip forces ranging approximately from 1 to 20 N (Jenmalm et al., 1998; McDonnell et al., 2005; Kinoshita et al., 1997; Westling and Johansson, 1984). This range of pinch force is significantly lower than average maximum pinch force of 65 N (tip pinch for young healthy adults; Mathiowetz et al., 1985). Therefore, to what extent safety margins vary with force level remains unclear. Also, safety margins during high force exertions have not been examined despite its significant implication for musculoskeletal stress and injuries.
Towards this end, the present study was conducted to 1) quantify safety margin during isometric push tasks in lateral pinch, and to 2) investigate the relationship between push force level and safety margin in an isometric push task in lateral pinch. A lateral pinch was chosen for its greater utilities in daily living and work tasks compared to tip or palmar pinch. It is unknown whether people maintain a constant safety margin over a range of push force levels, or people decrease safety margin as the push force level increases to avoid overexertion. Or people may even increase safety margin with increasing push force, because potential injury from hand slipping becomes more severe for high push forces. The null hypothesis was that safety margin is constant regardless of push force level. The alternative hypothesis was that safety margin increases or decreases with increasing push force.
2. Methods
2.1. Procedure
An experiment was performed in which safety margins were measured for five different push force levels and for two grip surfaces that are prevalent in workplaces (aluminum and rubber). Voluntary grip forces and minimum required grip forces were measured separately. Then, safety margins were calculated as voluntary grip force less minimum required grip force (Johansson and Westling, 1984). All tasks were performed in the lateral pinch posture.
To measure voluntary grip forces, subjects were seated on a fixed chair with 0° shoulder abduction, 0° shoulder flexion, 90° elbow flexion, and pronated forearm for the right arm. They grasped an instrumented object with the right hand in a lateral pinch posture using the thumb pad and the lateral aspect of the middle phalange of the index finger (see Figure 1a). Then they performed isometric push exertions at five levels – maximum (100%), 80%, 60%, 40% and 20% of the maximum push force – while voluntary grip forces were measured. For sub-maximal push tasks (80%, 60%, 40%, 20%), subjects were instructed to increase their push force until their push force matched a prescribed target that was displayed on a computer screen. The grip surface of the instrumented object was covered with a smooth flat sheet of aluminum or rubber. Subjects were instructed to maintain an upright posture throughout the experiment. They were also instructed not to allow their fingers slide on the grip surface during push.
Figure 1.

Experimental apparatus: (a) Voluntary grip force during isometric push exertions in lateral pinch was measured using an instrumented object. Push force was measured using a force transducer. (b) Minimum required grip force was measured using an instrumented object at the moment the object slipped out of the fingers. The weight of the instrumented object was adjustable.
Each push exertion lasted for 5 seconds. Maximum (100%) push force was determined as an average push force during a 2-sec window in which push force was the highest. Voluntary grip force was determined as an average grip force during a 2-second window in which measured push force was closest to the target. Trials were randomized across conditions. Each condition was repeated 3 times with a 2-minute inter-trial rest.
To measure minimum required grip force, subjects grasped and lifted the aluminum- or rubber-finished instrumented object in a lateral pinch posture and slowly separated the thumb and the index finger until the object slipped out of the fingers (see Figure 1b) while grip force was recorded. Subjects were instructed to have the thumb pointing downwards while releasing the objects so that the orientations of the thumb and the index finger relative to the object were the same for the push exertions and for the minimum required grip force measurements. The wrist posture was not controlled during measure of minimum required grip forces, as minimum required grip force that is mechanically needed to lift an object (or the coefficient of friction for the fingers) is not associated with wrist posture that may influence grip force capacity or with human grip force control.
The minimum required grip force was determined to be the grip force at the moment the grip force suddenly fell, as previously described (McDonnell et al, 2005). The weight of the instrumented object was adjusted to match each subject’s five push force levels (20% to 100%) by adding or removing weights on the plate attached at the bottom of the instrumented object (see Figure 1b). Minimum required grip forces for all five push force levels were measured because the coefficient of friction may vary with grip force level (Sivamani et al., 2003; Seo et al., in press; Seo and Armstrong, in press). Trials were randomized across conditions. Each condition was repeated 3 times.
In addition to measurement of voluntary grip force and minimum required grip force, grip strength and push strength were measured in the same posture used for voluntary grip force measurement. Grip strength was measured while subjects performed maximum grip exertion (with no pushing) in the lateral pinch posture (Figure 1a). Push strength was measured while subjects placed the thumb tip and the dorsal aspect of the middle phalange (resembling the lateral pinch posture) against a vertical plate and performed maximum push exertion against the plate. Push strength measured in this manner represents push strength when the coefficient of friction is infinite, or push strength that is not limited by friction.
To eliminate possible artifacts due to contaminants, subjects washed their hands with soap and rinsed with water. Then the hands were dried with paper towels and air-dried for 10 min before the onset of the experiment. Subjects were naive about the purpose of the experiment. The entire experiment took approximately 1.5 hours.
2.2. Subjects
Ten healthy subjects (5 females and 5 males, age 18-51 years, mean age = 29) volunteered to participate in the experiment. They were right handed except one male subject. Using the non-dominant right hand, the left-handed subject did not exhibit a significant difference in safety margins compared to the nine right-handed subjects, as has been demonstrated previously (McDonnell et al., 2006; Blennerhassett et al., 2006). All subjects gave written informed consent prior to testing.
2.3. Apparatus
Push force was measured using a single-axis load cell (SM-50, Interface, Inc., Scottsdale, AZ, maximum error: ±0.03%, capacity: 222 N) that was fixed to a table (see Figure 1a). Grip force was measured using a custom developed force transducer placed between the two flat grasped surfaces (see Figure 1a and b). The two flat grip surfaces were replaceable on the instrumented object so that surface materials can be switched between rubber and aluminum on the identical locations during the experiment. With the two grip surfaces on, the grip with was 1.5 cm. The grip surfaces were 1.5 cm × 5 cm on each side (vertical × longitudinal directions in Figure 1a). For push strength measurement, the instrumented object in Figure 1a was replaced with a 10 cm × 10 cm aluminum plate facing the hand.
2.4. Statistical Analysis
Analysis of variance was performed to determine if safety margins are significantly affected by push force, grip surface material (aluminum and rubber), and interaction between the two. Statistical analysis was performed using MINITAB® Release 14 with p-value less than 0.05 being significant.
3. Results
The mean push strength was 96 N (SD = 36 N), and the mean grip strength was 87 N (SD = 26 N) for all ten subjects. Mean maximum (100%) push force in lateral pinch was 33 N (SD = 14 N) for the aluminum surface. When normalized to each subject’s push strength and expressed as a percentage of maximum voluntary contraction (%MVC), mean maximum push force for the aluminum surface was 36% MVC. Mean maximum push force for the rubber surface was 61 N (SD = 22 N) or 65% MVC. Maximum push force is greater for the rubber surface than for the aluminum surface, because the rubber surface has a higher coefficient of friction than the aluminum surface. The average coefficients of friction, the ratio of minimum required grip force to twice the pinch force (Buchholz et al., 1988; Smaby et al., 2004), were 0.5 and 0.9 for the aluminum surface and rubber surface, respectively.
Mean voluntary grip force and minimum required grip force are plotted as a function of push force for the aluminum and rubber surfaces in Figure 2. Push force and grip force are normalized to each subject’s push strength and grip strength, respectively. It can be seen in Figure 2 that voluntary grip forces are twice the minimum required grip forces. The difference between voluntary grip force and minimum required grip force is safety margin. During maximum push exertions, mean voluntary grip forces were 74% of subjects’ grip strength (grip surface, subject pooled). Voluntary grip forces used during maximum push exertions were significantly less than the subjects’ grip strength (p<0.01; grip surfaces, subject pooled).
Figure 2.
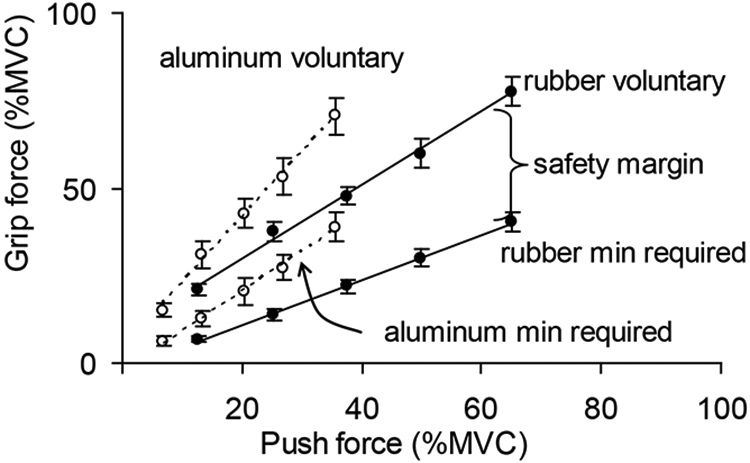
Mean ± SE voluntary grip force and minimum required grip force as a function of push force for the aluminum and rubber surfaces (10 subjects’ data pooled). The difference between the voluntary and minimum required grip forces is safety margin. Grip force and push force are normalized to each subject’s grip strength and push strength, respectively. The five different push forces correspond to 20%, 40%, 60%, 80%, and 100% of maximum push force in lateral pinch for each grip surface.
Safety margins are plotted as a function of push force in Figure 3. Push forces were normalized to each subject’s push strength in lateral pinch. Safety margins were calculated as the difference between voluntary grip force and minimum required grip force, and then normalized to each subject’s grip strength. The mean safety margin was 25% MVC (grip surface, push level, subject pooled). The mean safety margin during maximum (100%) push exertions was 3 times greater than that during 20% push exertions (material, subject pooled). Analysis of variance showed that safety margin significantly increased with increasing push force (p<0.01). Safety margin did not significantly vary with grip surface materials or with the interaction between grip surface material and push force levels (p>0.05).
Figure 3.
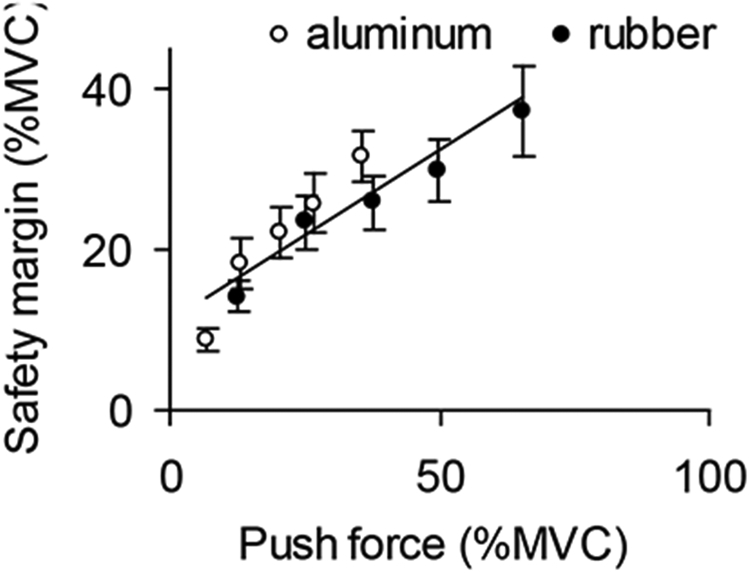
Mean ± SE safety margin as a function of push force in lateral pinch for the aluminum and rubber surfaces. Safety margins (voluntary grip force – minimum required grip force) are normalized to each subject’s grip strength. Push forces are normalized to each subject’s push strength. The five different push forces correspond to 20%, 40%, 60%, 80%, and 100% of maximum push force for each grip surface. The regression line is for both aluminum and rubber surfaces.
4. Discussions
4.1. Safety margin during isometric push task
The present study demonstrated that subjects used higher grip force than minimally required during isometric push tasks in a lateral pinch posture (see Figure 2). This finding demonstrates that safety margin exists not only for lifting tasks as previously shown (Johansson and Westling, 1984), but also for push tasks as long as friction is involved. The safety margin observed during push tasks is presumably to secure the grip and prevent hand slippage during push.
Mean safety margin was 25% MVC in this study (see Figure 3). Safety margin values can be expressed in terms of relative safety margin to facilitate comparisons with previous studies. The relative safety margin (ratio of safety margin to voluntary grip force) was, on average, 54%. The relative safety margin seen during push tasks in this study is comparable to those observed during lifting tasks in previous studies (Edin et al., 1992; Jenmalm et al., 1998; Kinoshita, 1999; Westling and Johansson, 1984). Although it may seem the risk of slip during push tasks is less critical than dropping an object in lifting tasks, comparison between the present study and previous studies suggests that people do not necessarily use smaller safety margins for isometric push tasks compared to lifting tasks.
Comparisons between the present study and previous studies, however, could be complicated by the difference in the type of grip. The lateral aspect of the middle phalange of the index finger was used to oppose the thumb pad in the present study, whereas, in previous studies, the volar part of the index fingertip skin was used to oppose the thumb pad. The volar and the lateral aspects of the index finger may have different densities of papillary ridges and sweat glands (Peaslee, 2007), which may result in different coefficients of friction (Smith et al., 1997; Zackrisson et al., 2008) and thus different safety margins. Also, the direction of friction force relative to the finger is different between the lateral pinch (in the present study) and tip pinch (in previous studies). The stiffness of the skin varies depending on friction force direction (Nakazawa et al., 2000) and the skin coefficient of friction has an anisotropic characteristic (Bullinger, 1979). Thus different friction force directions may result in different coefficients of friction between the two grip types and thus different safety margins. Further investigations are needed to test if safety margin differs between lifting and push tasks.
4.2. Effect of push force level on safety margin
This study demonstrated that safety margin significantly increased with increasing push force (Figure 3). This increase in safety margin with increasing push force was observed for both aluminum and rubber surfaces. Mean safety margin increased four folds as push force increased from 7% MVC to 65% MVC (subject pooled). It is consistent with Kinoshita et al. (1997) that showed safety margin during lifting tasks increased 1.7 times as friction force (object weight) increased from 1.1 to 3.4 N. The present study showed that the effect of push force level on safety margin prevailed on the entire push force range for each grip surface (push force ranging from 6.3 to 61 N).
Possible underlying mechanisms for the effect of force level on safety margin were postulated. First, it could be simply a strategy to avoid slip since the consequence of slip becomes more dangerous as the push force level increases. Second, the increased safety margin seen with greater push force may have resulted from the recruitment of larger motor units, which, in turn, results in a decreased ability to finely grade force output. It has been shown that motor units that produce relatively small twitch tensions during contraction are recruited prior to motor units that produce large twitch tensions (Henneman and Mendell, 1981; Stuart and Enoka, 1984; Thomas et al., 1987). Therefore, when producing high push force (and high grip force), large motor units are recruited, which, in turn, may result in a greater safety margin compared to when producing low push force (and low grip force).
Third, increase in safety margin with increasing force level may be to compensate for greater variability in force output during high force generation. It has been shown that force variability increases with increasing force level (Enoka et al. 1999; Jones et al., 2002). For example, in Jones et al. (2002), force variability (standard deviation) increased from 0.5% MVC to 2.5% MVC as the mean force increased from 20% MVC to 70% MVC for a thumb extensor muscle. Assuming these values apply to grip force generation, to maintain grip force consistently above a minimally required level for 99.9% of times, safety margin (difference between mean voluntary grip force and minimally required grip force) should be 1.5% MVC when exerting 20% MVC grip force, and 7.7% MVC when exerting 70% MVC grip force. Therefore, 6.2% MVC increase in safety margin may be attributed to greater force variability induced by increasing grip force from 20% to 70% MVC. In summary, to ensure that grip force does not fall below the minimum required grip force, subjects may increase safety margin to account for greater grip force fluctuation during high push force exertions.
Fourth, increase in hand, wrist, and arm muscle activity that is needed for increasing push force generation may have contributed to increased activity of the finger muscles that produce grip force. It has been shown that individual descending fibers project to multiple motor nuclei of more than one muscle (Asanuma et al., 1979; Fetz and Cheney, 1980; Porter, 1987; Shinoda et al., 1979). Thus an exertion in one direction in one joint is typically accompanied by exertions in other directions and in other joints (Dewald and Beer, 2001). Therefore, increasing push activity may have elevated grip activity and thus safety margin.
Fifth, increase in safety margin with increasing push force may be due to biomechanics of push. During push, friction force is applied on the finger skin towards the joints of the fingers. Friction force is parallel to the finger segment and directed proximally. This proximally-directed friction force has been shown to increase normal force without additional muscle effort (Seo et al., 2007 & 2008a,b). More specifically, friction force, Ff, on the thumb tip pad in the direction towards the thumb interphalangeal joint results in flexion moment, Ff Xf, about the interphalangeal joint, where Xf is the distance between the interphalangeal joint center and Ff. This flexion moment is in addition to the joint moment generated by muscles, Mmuscle. The total flexion moment at the joint, Mmuscle + Ff Xf, is then used to generate normal force, Fn, on the grasped object: Fn = (Mmuscle + Ff Xf ) / Xn, where Xn is the distance between the interphalangeal joint center and Fn. Therefore, increase in push force (Ff) can result in increased normal force, Fn, as long as there is no finger slip. For instance, push force of 60 N will automatically increase normal force by 27 N in an isometric condition (assuming Xn = 29 mm and Xf = 13 mm from Buchholz and colleagues (1989, 1992)).
In summary, push force can result in increased grip force independent of grip muscle effort in an isometric push task. The enhancement in grip force increases with increasing push force. It should be noted, however, that this force enhancement can be hampered by antagonistic muscle activities to stabilize the joints during force exertions. If this grip force enhancement is in fact present during push, then with the same mechanism, there will be grip force deduction during pull as the friction force generates a moment about the interphalangeal joint in the opposite direction. Future studies may investigate both push and pull tasks and quantify the contribution of this mechanism to safety margin.
4.3. Grip surface
Safety margins were not significantly different between the rubber and aluminum surfaces when push force was accounted for (see Figure 3). It is different from previous studies by Kinoshita et al. (1997) and Cole and Johansson (1993). For example, safety margin during lifting tasks increased 1.6 times as the coefficient of friction decreased from 1.6 to 0.4 for a given friction force in Kinoshita et al. (1997). It is possible that the effect of grip surface on safety margin was not seen in the present study because the coefficient of friction varied in a small range (0.5 to 0.9). The different effects of grip surface could also be attributed to the difference in the performed tasks and in the examined force range between the present study and previous studies.
4.4. Reduced maximum grip force during push
Grip force during maximum push exertions was only 74% MVC (grip surface, subject pooled; Figure 2), although mechanically push force can be maximized by using 100% MVC grip force. This submaximal grip force used for maximum push exertions may be related to “force deficit”: Previous studies (Ohtsuki, 1981a, b; Kinoshita et al., 1995; Li et al., 1998; Verdervoort et al., 1984) have reported that when several muscle groups are activated simultaneously, each muscle group’s maximum force decreases compared to that during a single muscle group exertion. As for underlying mechanisms, Ohtsuki (1981a) suggested the mutual efferent inhibition between muscle groups on the cortex level as a cause of decreased force outputs. Li et al. (1998) suggested that a central neural drive might have a certain limit that cannot be exceeded, thus limiting the overall force output.
4.5. Implication in design of consumer products and workstations
The present study presents significant implications in product/workstation design and ergonomics analysis. To ensure that users or workers are capable of performing a given push task, the first step is to make sure that the required grip force is less than people’s grip strength (Smaby et al., 2004). Safety margin and grip force reduction should also be accounted for if the task involves friction force generation. In short, required grip force plus safety margin should not exceed grip strength discounted by force deficit.
For example, if inserting a plug into a power outlet requires push force of 60 N and the coefficient of friction between the plug and the hand is 0.7, the minimum required grip force is calculated to be 43 N (minimum required grip force = push force divided by two times the coefficient of friction; equation provided in Buchholz et al. (1988) and Smaby et al. (2004)). This minimum required grip force of 43 N is less than grip strength of 87 N. Thus it may seem that people can insert the plug without difficulty. However, that is not the case when safety margin and force deficit are accounted for. Voluntary grip force may be twice the minimum required grip force (assuming the same amount of safety margin observed in the present study), which is 86 N. In addition, since this is a grip-and-push task, the maximum grip force people can generate may be 74% MVC (assuming the same amount of force deficit observed in the present study), which is 64 N. Therefore, estimated voluntary grip force (required grip force plus safety margin = 86 N) exceeds maximum grip force (grip strength discounted by force deficit = 64 N). Thus, people may struggle to insert the plug into the power outlet. It can be seen that people’s push capability can be overestimated if safety margin and grip force deficit are not accounted for during ergonomic analysis.
5. Conclusion
This paper demonstrated that 1) safety margin exists for an isometric push task in lateral pinch. Mean safety margin was 25% MVC. 2) Safety margin significantly increased with increasing push force for both aluminum and rubber surfaces. 3) Grip force used during maximum push exertion was only 74% MVC. The findings suggest that ergonomic analyses of push tasks that involve friction force should account for safety margin and reduced grip strength during push. Failure to consider safety margin and reduced grip strength during push can result in overestimation of people’s push capability.
References
- Asanuma J, Zarzecki P, Jankowska E, Hongo T, Marcus S. (1979). Projection of individual pyramidal tract neurons to lumbar motor nuclei of the monkey. Exp Brain Res 34, 73–89. [DOI] [PubMed] [Google Scholar]
- Blennerhassett JM, Carey LM, Matyas TA (2006). Grip force regulation during pinch lifts under somatosensory guidance: comparison between people with stroke and healthy controls. Archives of Physical Medicine and Rehabilitation 87, 418–29. [DOI] [PubMed] [Google Scholar]
- Buchholz B, Frederick LJ, Armstrong TJ (1988). An investigation of human palmar skin friction and the effects of materials, pinch force and moisture. Ergonomics 31 (3) Mar, 317–325. [DOI] [PubMed] [Google Scholar]
- Buchholz B (1989). A kinematic model of the human hand to evaluate its prehensile capabilities. PhD . thesis, University of Michigan, Ann Arbor. [DOI] [PubMed] [Google Scholar]
- Buchholz B, Armstrong TJ, Goldstein SA (1992). Anthropometric data for describing the kinematics of the human hand. Ergonomics 35 (3) 261–273. [DOI] [PubMed] [Google Scholar]
- Bullinger HJ, Kern P, Solf JJ (1979). Reibung Zwischen hand und griff, Forchungs bericht Nr 213. (The effects of materials and surface on the frictional behaviour between hand and handle). Bundesanstalt für Arbeitsschutz und Unfall-forscung, Dortmund, Germany. [Google Scholar]
- Bystrom S, Fransson-Hall C (1994). Acceptability of intermittent handgrip contractions based on physiological response. Human Factors 36 (1) 158–71. [DOI] [PubMed] [Google Scholar]
- Bystrom S, Kilbom A (1990). Physiological response in the forearm during and after isometric intermittent handgrip. European Journal of Applied Physiology 60, 457–466. [DOI] [PubMed] [Google Scholar]
- Cole KJ, Abbs JH (1988). Grip force adjustments evoked by load force perturbations of a grasped object, Journal of Neurophysiology, 60, 1513–1522. [DOI] [PubMed] [Google Scholar]
- Cole KJ, Johansson RS (1993). Friction in the digit-object interface scales the sensorimotor transformation for grip responses to pulling loads. Experimental Brain Research, 85, 523–532. [DOI] [PubMed] [Google Scholar]
- Cole KJ, Rotella DL, Harper JG (1999). Mechanisms for age-related changes of fingertip forces during precision gripping and lifting in adults. Journal of Neuroscience, 19 (8), 3238–3247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole KJ, Steyers CM, Graybill EK (2003). The effects of graded compression of the median nerve in the carpal canal on grip force, Experimental Brain Research, 148: 150–157. [DOI] [PubMed] [Google Scholar]
- Department of Trade and Industry (1997). Government consumer safety research: assessment of problems related to packaging size, London UK [Google Scholar]
- Dewald JPA, Beer RF (2001). Abnormal joint torque patters in the paretic upper limb of subjects with hemiparesis. Muscle and Nerve, 24, 273–283. [DOI] [PubMed] [Google Scholar]
- Dun S, Kaufmann RA, Li ZM (2007). Lower median nerve block impairs precision grip. J Electromyogr Kinesiol, 17 (3) 348–54. [DOI] [PubMed] [Google Scholar]
- Edin BB, Westling G, Johansson RS (1992). Independent control of human finger-tip forces at individual digits during precision lifting. Journal of Physiology, 450, 547–564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enoka RM, Burnett RA, Graves AE, Kornatz KW, Laidlaw DH (1999). Task- and age-dependent variations in steadiness. Progress in Brain Research, 123, 389–395. [DOI] [PubMed] [Google Scholar]
- Fetz EE, Cheney PD. (1980). Postspike facilitation of forelimb muscle activity by primate corticomotoneuronal cells. Journal of Neurophysiology 44, 751–772. [DOI] [PubMed] [Google Scholar]
- Flanagan JR, Wing AM (1997). The role of internal models in motion planning and control: evidence from grip force adjustments during movements of hand-held loads. Journal of Neoruscience, 17 (4) 1519–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grieshaber DC, Armstrong TJ (2007). Insertion loads and forearm muscle activity during flexible hose insertion tasks. Human Factors, 49 (5) 786–96. [DOI] [PubMed] [Google Scholar]
- Henneman E, Mendell LM (1981). Functional organization of the motoneuron pool and its inputs. In: Brooks VB (ed) Handbook of Physiology, The Nervous System. Washington, DC: Am. Physiol. Soc. 1981, vol. II, chapt. 11, part I, p. 423–507. [Google Scholar]
- Hermsdorfer J, Hagl E, Nowak DA, Marquardt C (2003). Grip force control during object manipulation in cerebral stroke. Clinical Neurophysiology, 114 (5) 915–929. [DOI] [PubMed] [Google Scholar]
- Jenmalm P, Johansson RS (1997). Visual and somatosensory information about object shape control manipulative finger tip forces. Journal of Neuroscience, 17, 4486–4499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jenmalm P, Goodwin AW, Johansson RS (1998). Control of grasp stability when humans lift objects with different surface curvatures. Journal of Neurophysiology, 79, 1643–1652. [DOI] [PubMed] [Google Scholar]
- Johansson RS, Westling G (1984). Roles of glabrous skin receptors and sensorimotor memory in automatic control of precision grip when lifting rougher or more slippery objects, Experimental Brain Research, 56, 550–564 [DOI] [PubMed] [Google Scholar]
- Jones KE, Hamilton AF, Wolpert DM (2002). Sources of signal-dependent noise during isometric force production. Journal of Neurophysiology, 88 (3) 1533–44. [DOI] [PubMed] [Google Scholar]
- Kinoshita H, Francis PR (1996). A comparison of prehension force control in young and elderly individuals. European Journal of Applied Physiology and Occupational Physiology, 74 (5), 450–460. [DOI] [PubMed] [Google Scholar]
- Kinoshita H, Backstrom L, Flanagan R, Johansson RS (1997). Tangential torque effects on the control of grip forces when holding objects with a precision grip. Journal of Neurophysiology, 78, 1619–1630. [DOI] [PubMed] [Google Scholar]
- Kinoshita H, Kawai S, Ikuta K (1995). Contributions and co-ordination of individual fingers in multiple finger prehension. Ergonomics, 38 (6) 1212–30. [DOI] [PubMed] [Google Scholar]
- Kinoshita H (1999). Effect of gloves on prehensile forces during lifting and holding tasks. Ergonomics, 42 (10) 1372–1385. [DOI] [PubMed] [Google Scholar]
- Li Z-M, Latash ML, Zatsiorsky VM (1998). Force sharing among fingers as a model of the redundancy problem, Experimental Brain Research, 119, 276–286 [DOI] [PubMed] [Google Scholar]
- Lowe BD, Freivalds A (1999). Effect of carpal tunnel syndrome on grip force coordination on hand tools, Ergonomics, 42 (4) 550–564. [DOI] [PubMed] [Google Scholar]
- Malker B (1991). Occupational disease and occupational accidents 1989 Official Statistics of Sweden National Board of Occupational Safety and Health, Stockholm 1991 (in Swedish) [Google Scholar]
- Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, & Rogers S (1985). Grip and Pinch Strength: Normative Data for Adults. Arch Phys Med Rehabil, 66, 69–72. [PubMed] [Google Scholar]
- McDonnell MN, Ridding MC, Flavel SC, Miles TS (2005). Effect of human grip strategy on force control in precision tasks. Experimental Brain Research, 161, 368–373. [DOI] [PubMed] [Google Scholar]
- McDonnell MN, Hillier SL, Ridding MC, Miles TS (2006). Impairments in precision grip correlate with functional measures in adult hemiplegia. Clinical Neurophysiology, 117, 1474–1480. [DOI] [PubMed] [Google Scholar]
- Nakazawa NN, Ikeura R, Innoka H (2000). Characteristics of human fingertips in the shearing direction. Biological Cybernetics, 82, 207–214. [DOI] [PubMed] [Google Scholar]
- National Research Council and Institute of Medicine (2001). Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities. Washington, DC, National Academy Press. [PubMed] [Google Scholar]
- National Research Council (1999). Work-related musculoskeletal disorders: a review of the evidence. Washington, DC, National Academy Press. [Google Scholar]
- Ohtsuki T (1981a). Inhibition of individual fingers during grip strength exertion, Ergonomics, 24 (1) 21–36. [DOI] [PubMed] [Google Scholar]
- Ohtsuki T (1981b). Decrease in grip strength induced by simultaneous bilateral exertion with reference to finger strength, Ergonomics, 24 (1) 37–48. [DOI] [PubMed] [Google Scholar]
- Peaslee ER (2007). Human Histology: In its relations to descriptive anatomy, physiology and pathology. Kessinger Publishing, LLC. Whitefish, MT. pp. 489. [Google Scholar]
- Porter R (1987). The Florey Lecture, corticomotoneuronal projections: synaptic events related to skilled movement. Proc R Soc Lond 231:147–168. [DOI] [PubMed] [Google Scholar]
- Preising B, Hsia TC, Mittelstadt B (1991). A literature review: Robots in medicine. IEEE Engineering in Medicine and Biology Magazine, 10, 13–22. [DOI] [PubMed] [Google Scholar]
- Richter WM, Rodriquez R, Woods KR, Karpinski AP, Axelson PW (2006). Reduced finger and wrist flexor activity during propulsion with a new flexible handrim. Archives of Physical Medicine & Rehabilitation, 87 (12) Dec 1643–1647. [DOI] [PubMed] [Google Scholar]
- Rohmert W (1973). Problems in determining rest allowances. Applied Ergonomics 4 (2) 91–95. [DOI] [PubMed] [Google Scholar]
- Seo NJ, Armstrong TJ, Chaffin DB, Ashton-Miller JA (2008a). Inward Torque and High-Friction Handles Can Reduce Required Muscle Efforts for Torque Generation. Human Factors, 50 (1) 37–48. [DOI] [PubMed] [Google Scholar]
- Seo NJ, Armstrong TJ, Chaffin DB, Ashton-Miller JA (2008b). The Effect of Handle Friction and Inward or Outward Torque on Maximum Axial Push Force. Human Factors: Journal of Human Factors and Ergonomics Society, 50 (2) 227–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seo NJ, Armstrong TJ, Ashton-Miller JA, Chaffin DB (2007). The Effect of Torque Direction and Cylindrical Handle Diameter on the Coupling between the Hand and a Cylindrical Handle. Journal of Biomechanics, 40, 3236–3243. [DOI] [PubMed] [Google Scholar]
- Seo NJ, Armstrong TJ (in press). Friction Coefficients in a Longitudinal Direction between the Finger Pad and Selected Materials for Different Normal Forces and Curvatures. Ergonomics. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seo NJ, Armstrong TJ, Drinkaus P (in press). A Comparison of Two Methods of Measuring Static Coefficient of Friction at Low Normal Forces: A Pilot Study. Ergonomics. [DOI] [PubMed] [Google Scholar]
- Shinoda Y, Zarzecki P, Asanuma H. (1979). Spinal branching of the pyramidal tract neurons in the monkey. Experimental Brain Research, 34:59–72. [DOI] [PubMed] [Google Scholar]
- Sivamani RK, Goodman J, Gitis NV, Maibach HI (2003), Friction coefficient of skin in real-time. Skin Research and Technology, 9, 235–239. [DOI] [PubMed] [Google Scholar]
- Smaby N, Johanson ME, Baker B, Kenney DE, Murray WM, Hentz VR (2004). Identification of key pinch forces required to complete functional tasks. Journal of Rehabilitation Research & Development, 41 (2) 215–224. [DOI] [PubMed] [Google Scholar]
- Smith AM, Cadoret G, St-Amour D (1997). Scopolamine increases prehensile force during object manipulation by reducing palmar sweating and decreasing skin friction. Experimental Brain Research, 114 (3) 578–83. [DOI] [PubMed] [Google Scholar]
- Stuart DG, Enoka RM Motoneurons, moto units and the size principle. In: The Clinical Neurosciences, edited by Grossman RG and Willis WD. New York: Churchill Livingstone, 1984, sect. 5. chapt. 17, p. 471–517. [Google Scholar]
- Thomas CK, Ross BH, Calancie B (1987). Human motor-unit recruitment during isometric contractions and repeated dynamic movements. Journal of Neurophysiology, 57 (1) 311–324. [DOI] [PubMed] [Google Scholar]
- Verdervoort AA, Sale DG and Moroz J (1984). Comparison of motor unit activation during unilateral and bilateral leg extension. Journal of Applied Physiology: Respir Environ Exerc Physiol 56: 46–51 [DOI] [PubMed] [Google Scholar]
- Westling G, Johansson RS (1984). Factors influencing the force control during precision grip. Experimental Brain Research, 53, 277–284. [DOI] [PubMed] [Google Scholar]
- Zackrisson T, Eriksson B, Hosseini N, Johnels B, Krogstad A-L, 2008. Patients with hyperhidrosis have changed grip force, coefficient of friction and safety margin. Acta Neurol Scand, 117, 279–284. [DOI] [PubMed] [Google Scholar]