

ABSTRACT
Background
Recent years have shown an increased application of prospective trajectory-oriented approaches to posttraumatic stress disorder (PTSD). Although women are generally considered at increased PTSD risk, sex and gender differences in PTSD symptom trajectories have not yet been extensively studied.
Objective
To perform an in-depth investigation of differences in PTSD symptom trajectories across one-year post-trauma between men and women, by interpreting the general trends of trajectories observed in sex-disaggregated samples, and comparing within-trajectory symptom course and prevalence rates.
Method
We included N = 554 participants (62.5% men, 37.5% women) from a multi-centre prospective cohort of emergency department patients with suspected severe injury. PTSD symptom severity was assessed at 1, 3, 6, and 12 months post-trauma, using the Clinician-Administered PTSD Scale for DSM-IV. Latent growth mixture modelling on longitudinal PTSD symptoms was performed within the sex-disaggregated whole samples. Bayesian modelling with informative priors was applied for reliable model estimation, considering the imbalanced prevalence of the expected latent trajectories.
Results
In terms of general trends, the same trajectories were observed for men and women, i.e. resilient, recovery, chronic symptoms and delayed onset. Within-trajectory symptom courses were largely comparable, but resilient women had higher symptoms than resilient men. Sex differences in prevalence rates were observed for the recovery (higher in women) and delayed onset (higher in men) trajectories. Model fit for the sex-disaggregated samples was better than for the whole sample, indicating preferred application of sex-disaggregation. Analyses within the whole sample led to biased estimates of overall and sex-specific trajectory prevalence rates.
Conclusions
Sex-disaggregated trajectory analyses revealed limited sex differences in PTSD symptom trajectories within one-year post-trauma in terms of general trends, courses and prevalence rates. The observed biased trajectory prevalence rates in the whole sample emphasize the necessity to apply appropriate statistical techniques when conducting sex-sensitive research.
KEYWORDS: PTSD, sex, gender, longitudinal, course, onset, injury, latent growth mixture modelling, Bayesian
PALABRAS CLAVE: TEPT, sexo, género, longitudinal, curso, inicio, lesión, modelo de mezcla de crecimiento latente, bayesiano
HIGHLIGHTS
We investigated sex differences in PTSD symptom trajectories over one-year post-trauma.
We observed modest differences.
Symptom courses were mostly similar.
Yet, the recovering trajectory was more prevalent in women, while the delayed onset trajectory was more prevalent in men.
Short abstract
Antecedentes: Los últimos años han demostrado una mayor aplicación de enfoques prospectivos orientados a la trayectoria para el trastorno de estrés postraumático (TEPT). Aunque generalmente se considera que las mujeres tienen un mayor riesgo de TEPT, las diferencias de sexo y género en las trayectorias de los síntomas del TEPT aún no se han estudiado ampliamente.
Objetivo: Realizar una investigación en profundidad de las diferencias en las trayectorias de los síntomas del TEPT a lo largo de un año después de un trauma entre hombres y mujeres, interpretando las tendencias generales de las trayectorias observadas en muestras desagregadas por sexo, así como comparar el curso y la evolución de los síntomas dentro de la trayectoria y las tasas de prevalencia.
Método: Incluimos N = 554 participantes (62.5% hombres, 37.5% mujeres) de una cohorte prospectiva multicéntrica de pacientes del servicio de urgencias con sospecha de lesión grave. La gravedad de los síntomas del TEPT se evaluó 1, 3, 6 y 12 meses después del trauma, utilizando la Escala de TEPT administrada por un médico para el DSM-IV. Se realizó un modelo de mezcla de crecimiento latente sobre los síntomas longitudinales de TEPT en las muestras desagregadas por sexo y en la muestra completa. Se aplicó un modelo bayesiano con antecedentes informativos para una estimación confiable del modelo, considerando la prevalencia desequilibrada de las trayectorias latentes esperadas.
Resultados: En términos de tendencias generales, se observaron las mismas trayectorias para hombres y mujeres, es decir, resiliente, recuperación, síntomas crónicos y aparición tardía. Los cursos de síntomas dentro de la trayectoria fueron en gran medida comparables, pero las mujeres resilientes tenían más síntomas másque los hombres resilientes. Se observaron diferencias por sexo en las tasas de prevalencia para las trayectorias de recuperación (mayor en mujeres) y de inicio tardío (mayor en hombres). El ajuste del modelo para las muestras desagregadas por sexo fue mejor que para la muestra completa, lo que indica la aplicación preferida de la desagregación por sexo. Los análisis de la muestra completa llevaron a estimaciones sesgadas de las tasas de prevalencia de trayectorias generales y específicas por sexo.
Conclusiones: Los análisis de trayectoria desagregados por sexo revelaron diferencias limitadas entre los sexos en las trayectorias de los síntomas del TEPT durante el año posterior al trauma en términos de tendencias generales, cursos y tasas de prevalencia. Las tasas de prevalencia de trayectoria sesgada observadas en el conjunto de la muestra enfatizan la necesidad de aplicar técnicas estadísticas apropiadas al realizar investigaciones que tengan en cuenta el sexo.
Short abstract
背景: 近年来, 前瞻性轨迹导向方法在创伤后应激障碍 (PTSD) 中的应用有所增加。尽管通常认为女性 PTSD 有更高的风险, 尚未对 PTSD 症状轨迹中的性别和性别差异进行广泛研究。
目的: 通过解读在性别分类样本中观察到轨迹的一般趋势, 以及比较轨迹内症状过程和流行率, 对创伤后一年内 PTSD 症状轨迹的男女差异进行深入考查。
方法: 我们纳入了 N= 554 名参与者 (62.5% 男性, 37.5% 女性), 这些参与者来自多中心前瞻性队列疑似严重受伤的急诊科患者。在创伤后 1, 3, 6 和 12 个月, 使用DSM-IV临床用 PTSD 量表评估 PTSD 症状严重程度。在性别分类样本和整个样本中对纵向 PTSD 症状进行了潜在增长混合模型。考虑到预期潜在轨迹的流行率不平衡, 应用了具有信息先验的贝叶斯模型进行可靠模型估计。
结果: 就总体趋势而言, 男性和女性观察到相同的轨迹, 即韧性, 恢复, 慢性症状和延迟发作组。轨迹内的症状过程在很大程度上具有可比性, 但韧性组女性比韧性组男性有更高的症状。在恢复组 (女性较高) 和延迟发病组 (男性较高) 轨迹中观察到流行率的性别差异。性别分类样本的模型拟合优于整个样本, 表明首选应用性别分类。对整个样本的分析导致对总体和特定性别轨迹流行率估计有偏。
结论: 性别分类轨迹分析揭示了创伤后一年内 PTSD 症状轨迹在总体趋势, 病程和流行率方面的性别差异有限。在整个样本中观察到的有偏轨迹流行率强调了在进行性别敏感性研究时应用适当统计技术的必要性。
关键词: PTSD, 性, 性别, 纵向, 过程, 发作, 受伤, 潜在增长混合模型, 贝叶斯
1. Introduction
Sex and gender differences in prevalence rates of traumatic event exposure and posttraumatic stress disorder (PTSD) appear evident: Men experience trauma disproportionately more often, but PTSD is more prevalent in women (Gavranidou & Rosner, 2003; Olff, 2017; Shalev et al., 2019). These differences can be ascribed to both sex (i.e. biology) and gender (i.e. social identity) related factors (Kornfield, Hantsoo, & Epperson, 2018). The higher PTSD prevalence in women can be partly, but not fully, explained by the fact that they are more often exposed to interpersonal trauma and especially sexual assault, which particularly increases conditional PTSD risk (Olff, 2017; Tolin & Foa, 2006). Most studies that indicate female vulnerability for PTSD focus on endpoint PTSD. This means they differentiate individuals fulfiling the diagnostic criteria for PTSD at a specified time point from those who do not. This approach does not consider how PTSD symptoms develop over time, which may be different between women and men. Therefore, the exact temporal dynamics underlying PTSD development in men and women are still unclear.
Applying trajectory-oriented approaches may help to increase our knowledge on this matter, as they implement prognostic and longitudinal perspectives and capture PTSD symptom severity in a continuous manner. These approaches classify groups of individuals based on the severity of their symptoms and their changes over time, thus moving beyond traditional binary diagnostic categories that merely distinguish individuals with and without PTSD. Therefore, they are more suitable for investigating increases and declines of symptoms over time (Galatzer-Levy, Huang, & Bonanno, 2018). Previous studies identified various numbers and types of PTSD symptom trajectories. They differ regarding the number of trajectories identified, ranging from 2 (Armour, Shevlin, Elklit, & Mroczek, 2012; Ginzburg & Ein-Dor, 2011) up to 6 (Berntsen et al., 2012; Pietrzak et al., 2014), which is presumably due to heterogeneity in study designs, sample, trauma and outcome characteristics, as well as the chosen statistical approaches. Yet, in a comprehensive meta-analytical summary of PTSD symptom trajectories within 38 samples, Galatzer-Levy et al. (2018) found four trajectories that occurred particularly consistently. The resilience trajectory, in which individuals might suffer from some acute stress symptoms immediately after trauma but do not develop any clinically relevant PTSD symptoms, was observed in 92% of the samples. This trajectory was considered the modal response following trauma, as it occurred with a pooled prevalence rate of 70%. The recovery trajectory describes individuals who develop clinical or subclinical PTSD symptoms initially after trauma, from which they gradually recover. It was observed in 74% of the samples and had a pooled prevalence rate of 27%. The third trajectory included individuals with chronic (sub)clinical PTSD symptoms. It was observed in 61% of the samples, with a pooled prevalence rate of 10%. The fourth trajectory, clustering individuals whose (sub)clinical PTSD symptoms emerge with delayed onset, was observed in 32% of the included samples and occurred with a pooled prevalence rate of 6%. Additional trajectories have been identified, mostly further differentiating within the consistently observed trajectories. For instance, Berntsen et al. (2012) distinguished resilient individuals from extremely resilient ones and Galatzer-Levy et al. (2013) differentiated between rapidly and slowly recovering individuals. Steenkamp, Dickstein, Salters-Pedneault, Hofmann, and Litz (2012), Pietrzak et al. (2014), as well as Johannesson, Arinell, and Arnberg (2015) distinguished a highly from a moderately chronic trajectory. Steenkamp et al. (2012) further differentiated between moderate and marked recovery.
Despite the apparent differences in prevalence rates of endpoint PTSD between women and men (Tolin & Foa, 2006), the majority of published trajectory-oriented studies have neglected sex and gender, so far. This can partly be explained by the samples’ imbalanced ratios of included men and women. Samples with military deployment-related trauma were often exclusively or predominantly male, whereas sexually abused samples were predominantly female. Previous studies with more balanced ratios mainly investigated sex or gender as predictor of trajectory membership, after specifying these trajectories within the whole sample. These studies yielded heterogeneous results. Some found that women disproportionately more often belonged to those trajectories defined by higher symptom severity. For instance, Bryant et al. (2015) found that female emergency department patients had a higher probability of belonging to the recovery, chronic or worsening trajectory, as compared to the resilient one, than men. A similar pattern was found in a sample exposed to a natural disaster: Participants within the recovering, severely chronic and moderately chronic trajectories were more likely female (Johannesson et al., 2015). Additionally, female deployed soldiers were more likely to be assigned to a trajectory with high symptoms and a significant increase over time, than one with low symptoms and little increase (Orcutt, Erickson, & Wolfe, 2004). Women’s higher risk of belonging to a non-resilient trajectory was further confirmed in another mixed-sex military sample (Berntsen et al., 2012), as well as in sample of responders to the 2001 World Trade Center attacks (Pietrzak et al., 2014). A recent consortium study (Lowe et al., 2021), pooling data of N = 3,083 emergency department patients from six large longitudinal studies, including the cohort used in the present study, also detected differences: Women had a lower probability of having low initial PTSD symptoms and being assigned to the low (resilient) symptom trajectory than men. However, despite these findings that indicate a greater female risk for long-term PTSD symptoms, other studies that investigated sex differences in the trajectories’ prevalence rates failed to confirm a greater risk for women (Galatzer-Levy et al., 2013; Galatzer-Levy, Madan, Neylan, Henn-Haase, & Marmar, 2011; Ginzburg & Ein-Dor, 2011; Hobfoll, Mancini, Hall, Canetti, & Bonanno, 2011; Le Brocque, Hendrikz, & Kenardy, 2010; Pielmaier, Milek, Nussbeck, Walder, & Maercker, 2013). Further, in their study on elderly survivors of a natural disaster, which emerged with a three-trajectory solution, Pietrzak, Van Ness, Fried, Galea, and Norris (2013) reported that women had a higher probability of belonging to the resilient or chronic dysfunction trajectory, respectively, than belonging to the delayed onset trajectory.
Thus, the question whether the prevalence rates of specific trajectories differ between men and women is not fully resolved, yet. Besides that, the question whether the same trajectories can be detected when analysing women and men separately, thus disaggregating data on PTSD symptom courses for men and women who were originally included within the same cohort has never been addressed before. Consequently, potential differences in PTSD symptom courses between women and men, in terms of initial severity and change over time within specific trajectories remain understudied to date. Raising attention towards the impact of sex and gender within trajectory-oriented approaches can provide insights into how the commonly assumed differences in endpoint PTSD between men and women emerge. Second, it allows for the future identification of potential sex- or gender-specific predictors of trajectory-membership. Together, this knowledge can be used to inform on the necessity of sex- or gender-specific screening and preventive interventions that promote resilience after trauma.
In this study, we applied latent growth mixture modelling on disaggregated data of men and women from a cohort study of patients who were admitted to an emergency department with suspected serious injury and followed up until one year afterwards. We thereby aimed to investigate the commonly observed PTSD symptom trajectories resilience, recovery, chronic and delayed onset within women and men separately. To this end, we employed Bayesian modelling with informative priors. This approach can provide reliable estimations of models with some relatively small or imbalanced latent clusters, which other statistical approaches might overlook or merge into larger, more stable clusters (van de Schoot et al., 2018). Informative priors inform on a reasonable range of values for the model parameters to be estimated (the expected number and prevalence of latent trajectories, and the expected symptom severity and change over time for a given trajectory) derived from the existing literature. It has been established that including priors with even a minor degree of information provides more accurate estimates than regular LGMM or Bayesian LGMM with non-informative priors (Smid, McNeish, Miočević, & van de Schoot, 2020). Considering the previously identified imbalanced allocations to the resilience, recovery, chronic and delayed onset trajectories, of which particularly the latter two were found to be relatively small (Galatzer-Levy et al., 2018), we considered Bayesian modelling appears to be most appropriate for our analyses.
We addressed the following research questions:
(1) Do the four expected PTSD symptom trajectories, namely, resilience, recovery, chronic and delayed onset, emerge in both men and women, if analysed separately?
(2) Do PTSD symptom courses within the respective trajectories differ between women and men?
(3) Do prevalence rates of the respective trajectories differ between men and women?
(4) Are the findings from the disaggregated models comparable with those from the whole sample? Importantly, here, the distinction between women and men was based on participants’ (biological) sex.
2. Methods
2.1. Participants and study design
Data were derived from the Trauma TIPS study, a prospective cohort study on incidence and prediction of trauma-related psychopathology (‘The Incidence, Prediction and Prevention of Post-trauma Psychopathology Study’). Adult participants were included after being transported by ambulance or helicopter with suspected severe injuries requiring specialized acute medical care to one of two level-1 Trauma Center sites (Academic Medical Center and Vrije Universiteit Medical Center) in Amsterdam, the Netherlands. Inclusion criteria were recent exposure to a potential traumatic event (DSM-IV PTSD criterion A1) and Dutch language proficiency. Exclusion criteria were: current severe psychiatric symptoms (psychosis or schizophrenia; severe personality disorders; injuries resulting from deliberate self-harm); current severe neurological disorder; moderate-severe traumatic brain injury (Glasgow Coma Scale score <13 (Teasdale & Jennett, 1974)); permanent residency outside the Netherlands. The study was approved by institutional review boards of both centres. N = 852 participants were included between September 2005 and March 2009. The larger study incorporated an embedded randomized controlled trial (RCT, ISRCTN registration number: 57754429) in 300 participants investigating the efficacy of a brief self-guided cognitive-behavioural internet intervention to prevent PTSD (Mouthaan et al., 2013; Mouthaan, Sijbrandij, Reitsma, Gersons, & Olff, 2011, 2014). Follow-up assessments occurred at 1 (T1), 3 (T2, added at the start of the RCT in September 2007), 6 (T3) and 12 months (T4) post-trauma.
At each assessment, PTSD symptom severity within the past month was determined using the validated Dutch translation of the Clinician-administered PTSD scale for DSM-IV (CAPS). This interview is the gold standard for PTSD assessment and has excellent internal consistency (Hovens et al., 1994; Weathers et al., 2004). For each DSM-IV diagnostic symptom, the CAPS measures symptom frequency and intensity (both ranges 0–4). Total symptom severity (range 0–136, higher score indicating higher symptom severity) was calculated by summing frequency and intensity scores for all 17 items, representing the re-experiencing (5 items), avoidance (7 items) and hyperarousal (5 items) clusters. Across follow-ups, CAPS scores did not differ between intervention and control conditions, see Mouthaan et al. (2013). For the current study, we selected all participants with at least two CAPS interviews across follow-up assessments to allow for reliable estimation of trajectories. This resulted in N = 554 participants (N = 346 (62.5%) men; N = 208 (37.5%) women, (biological) sex was extracted from the hospital patient records). Demographic and trauma characteristics did not differ between selected and non-selected participants, except that selected participants more commonly were from Dutch origin (84% vs 74.9%, χ2(1):9.241, p = .003, see supplementary table 1). Selected women were higher educated and more commonly experienced traffic accidents as index trauma type than selected men. Mean traumatic injury severity upon arrival at the trauma centre was significantly lower in selected women than men, while consciousness levels upon arrival at the trauma centre did not differ between men and women. There were no differences in the prevalence of endpoint PTSD at 12 months post-trauma between selected men and women, using a cut-off of CAPS total score ≥45 (Weathers, Ruscio, & Keane, 1999) (see Table 1 for demographic and trauma characteristics).
Table 1.
Demographic and trauma characteristics of included participants
| Men (n = 346) | Women (n = 208) | ||
|---|---|---|---|
| Age | 43.70 (14.76) | 44.24 (16.38) | T (552) = −0.398, p = .691 |
|
Origin Dutch Non-Dutch |
292 (84.9%) 52 (15.1%) |
170 (82.5%) 36 (17.5%) |
χ2 (1) = 0.534, p = .465 |
|
Educational level Less than secondary Secondary or greater |
81 (23.4%) 265 (76.6%) |
30 (14.6%) 176 (85.4%) |
χ2 (1) = 6.291, p = .012 |
|
Marital status Single/not living with partner Married/living with partner |
148 (42.8%) 198 (57.2%) |
99 (47.6%) 109 (52.4%) |
χ2 (1) = 1.222, p = .269 |
|
Prior trauma types experienced None Non-interpersonal trauma only Interpersonal trauma only Both types of trauma |
54 (16.7%) 105 (32.5%) 36 (11.1%) 128 (39.6%) |
40 (20.3%) 61 (31.0%) 27 (13.7%) 69 (35.0%) |
χ2 (3) = 2.308, p = .511 |
|
Index trauma type Traffic accident Other accident Assault (intentional harm) |
215 (62.2%) 116 (33.5%) 15 (4.3%) |
153 (73.6%) 50 (24.0%) 5 (2.4%) |
χ2 (2) = 7.795, p = .020 |
| Injury Severity Score upon arrival at trauma centre | 10.28 (9.56) | 8.42 (9.00) | U = 20,252, p = .012 |
| Glasgow Coma Scale total score upon arrival at trauma centre | 14.18 (2.66) | 14.08 (2.92) | U = 21,288, p = .581 |
|
Index trauma centre site Academic Medical Center Vrije Universiteit Medical Center |
257 (74.3%) 89 (25.7%) |
142 (68.3%) 66 (31.7%) |
χ2 (1) = 2.327, p = .127 |
|
Participated in embedded RCT No participation Control condition Intervention condition |
232 (67.0%) 56 (16.2%) 58 (16.8%) |
121 (58.2%) 41 (19.7%) 46 (22.1%) |
χ2 (2) = 4.512, p = .105 |
|
Endpoint PTSD probable diagnosis Yes No |
19 (7.5%) 234 (92.5%) |
10 (7.2%) 129 (92.8%) |
χ2 (2) = 0.909, p = 1.000 |
Descriptives are presented as mean (standard deviation) for continuous variables and frequency (percentage) for categorical variables. Injury Severity Score (available for N = 297 men and N = 159 women) is a standardized traumatic injury severity score made by physicians, with higher scores representing more severe injuries (range 3–75) (Baker, O'Neill, Haddon, & Long, 1974) . The Glasgow Coma Scale is used by physicians to quickly assess level of consciousness, with lower scores representing greater impairment (range 0–15) (Teasdale & Jennett, 1974). Scores were available for N = 284 men and N = 153 women.
2.2. Procedures
Potential participants were identified from hospital patient records. Patients meeting exclusion criteria based on the patient records or information from treating medical staff were not contacted. Further eligibility screening and recruitment were preferably performed within 72 hours post-trauma. At the baseline assessment, preferably scheduled approximately one week post-trauma, participants who gave written and oral informed consent were screened for psychiatric exclusion criteria (using the MINI International Neuropsychiatric Interview-Plus version 5.0 (Sheehan et al., 1998; van Vliet & de Beurs, 2007)) and completed self-report questionnaires including demographic and trauma characteristics (Mouthaan et al., 2011). If severe psychiatric symptoms meeting the exclusion criteria were disclosed during these assessments, participation was discontinued. If RCT-participants were randomized to the intervention condition, the intervention was accessible after a baseline assessment (T0). All participants were invited for follow-up assessments, irrespective of RCT participation, and had access to care as usual.
Follow-up assessments T1-T4 frequently occurred later than preferred, mostly resulting from practical issues related to participants’ medical situation. We handled this unintended variation in assessment timing by assigning collected CAPS interview data to the respective nearest assessment, which could be the originally scheduled or the adjacent assessment (i.e. T1: ≤ 60 days post-trauma; T2: 61–136 days post-trauma; T3: 137–273 days post trauma; T4 ≥ 274 days post-trauma). Ultimate sample size and timing relative to the injury for each assessment in the selected N = 554 participants with ≥2 valid CAPS interviews were: T1: n = 398, 42.15(8.75) days, range: 13–60 days; T2: n = 290, 97.15(17.22) days, range: 61–136 days; T3: n = 411, 207.18(27.40) days, range: 141–273 days; T4: n = 395, 424.9 (68.22) days, range: 288–702 days. We did not observe any significant differences in the timing of the various assessments between men and women (T1: t(396) = −0.161, p = .872; T2: t(272.96) = −1.756, p = .08; T3: t(409) = 1.437, p = .152; T4 (393): 0.242, p = .809).
2.3. Statistical analyses
2.3.1. Bayesian latent growth mixture modelling (LGMM)
We performed Bayesian LGMM with informative priors following a similar procedure as described in van de Schoot et al. (2018). In the current paper, however, we focus on sex-disaggregated models. We used square root transformed CAPS total scores, as CAPS total scores did not follow a normal distribution at all timepoints. The Bayesian results were obtained using Mplus version 8.4 (Muthen & Muthen, 2017). We present the median of the posterior distribution and its 95% higher posterior density (HPD) intervals for the parameters in the model.
The primary models included four latent trajectories with growth parameters for the intercept and linear slope. For interpretation purposes, we designated the intercept to be the first CAPS assessment (T1). The linear slope was specified as the average time in months between T1 and T2-T4, respectively. For comparison purposes between the sex-disaggregated and whole sample models, we used the same specifications and parameters for the three models, only changing them to accommodate the differences in sample sizes.
2.4. Parameter estimation priors
We used normally distributed priors for the growth parameters. The specification of the priors for the mean intercepts and linear slopes, as well as their description in terms of general trends was informed by a previously published systematic review and expert elicitation on latent PTSD trajectories (van de Schoot et al., 2018), see Table 2 and Figure 1. We used the calculated median intercept values for the four trajectories in the acute post-trauma period to derive priors for the mean intercept values, converting the standardized values into square root transformed CAPS scores, and thereafter adding or subtracting the estimated linear slope over a period of 1.5 months to this median. Additionally, we used these extracted median scores to calculate the expected end scores for each trajectory and thereafter calculated the mean slope priors for all trajectories. We used the median instead of the mean intercept values for our calculations, as PTSD symptom severity scores for European cohorts versus US cohorts are generally relatively low (Shalev et al., 2019).
Table 2.
Description and prior specification of trajectories included in the primary models. To improve interpretability, the depicted CAPS scores represent the non-transformed CAPS scores. However for the purpose of calculating the actual priors, we used the square root transformed CAPS scores in a similar manner
| Trajectory name | Description of general trend | Expected CAPS score acutely after trauma | Expected CAPS score at endpoint (T4) | Expected slope | Expected intercept (T1) | Expected relative prevalence | Expected sample size |
|---|---|---|---|---|---|---|---|
| Resilient | Continuous low symptom severity; potentially mild-moderate acute symptoms that decrease over time to low severity |
CAPS total score: 19.01 |
CAPS total score: 19.01 |
CAPS total score: 0 |
CAPS total score: 19.01 |
.616 | Men: n = 224 Women: n = 8 |
| Chronic | Continuous high symptom severity |
CAPS total score: 64.00 |
CAPS total score: 64.00 |
CAPS total score: 0 |
CAPS total score: 64.00 |
.103 | Men: n = 38 Women: n = 22 |
| Recovering | High acute symptom severity, decreasing over time to low severity, with endpoint severity similar to resilient trajectory |
CAPS total score: 55.67 |
CAPS total score: 19.01 : |
CAPS total score: (19.01–55.67)/14 = −2.62 |
CAPS total score: 55.67 + (2.62*1.5) = 51.74 |
.217 | Men: n = 79 Women: n = 45 |
| Delayed onset | Mild-moderate acute symptom severity, increasing over time to high symptom severity, with endpoint severity similar to chronic trajectory |
CAPS total score: 22.92 |
CAPS total score: 64.00 |
CAPS total score: (64.00–22.92)/14 = 2.93 |
CAPS total score: 22.92 + (2.93*1.5) = 27.32 |
.064 | Men: n = 23 Women: n = 13 |
Figure 1.
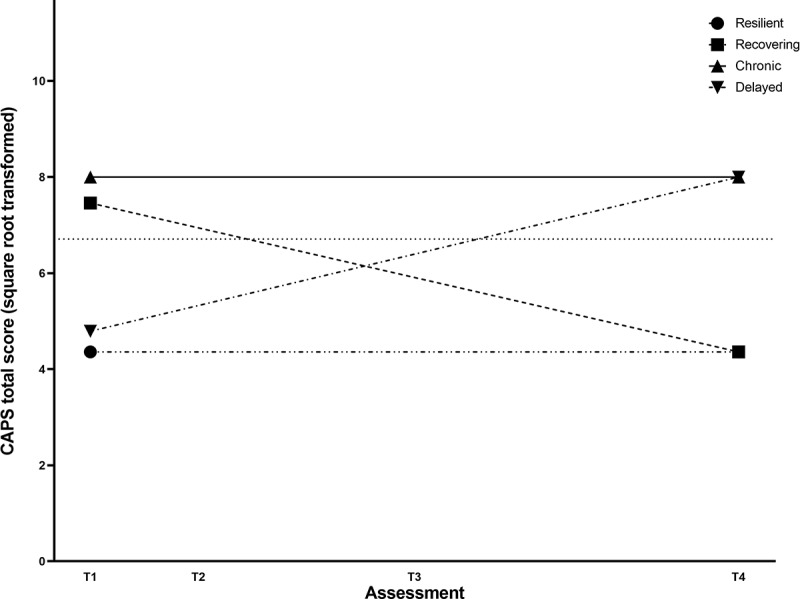
Hypothesized begin and endpoint square root transformed CAPS total scores for the four trajectories in the primary Bayesian linear growth mixture models, used to derive the mean intercept and slope priors.
The dashed line represents the square root transformed clinical cut-off for probable PTSD at CAPS total score = 45.
For the specification of the prior variances around the intercept and slope for each trajectory, we adapted the approach previously applied by van de Schoot et al. (2018) for a Bayesian LGMM of PTSD symptom severity in burn victims. We adapted their R-function to determine the optimal prior variance parameterization for the square root transformed CAPS scores given our expectations using R-package ggplot2 (Wickham, 2016) with the following specifications: for the resilient trajectory, we specified that the overlarge majority of mean intercepts (95%) would be below the commonly used cut-off of CAPS total score of 45 (Weathers et al., 1999) i.e. 6.71 for the square root transformed values, resulting in intercept variance of 2.045. Vice versa, for the chronic trajectory, we specified the overlarge majority (95%) of mean intercept would be above this clinical cut-off, resulting in intercept variance of 0.608. For the recovering trajectory, we expected the mean intercept to be lower than the mean intercept for the chronic trajectory, but allowed 95% of the mean intercepts to overlap with the intercepts for the chronic trajectory, resulting in intercept variance of 0.281. For the delayed onset trajectory, we expected the mean intercept at T1 to be higher than the mean intercept for the resilient trajectory, but allowed 95% of the mean intercepts to overlap with the intercepts for the resilient trajectory, resulting in intercept variance of 0.221.
Regarding the slope variance parameterization, we allowed 0.001% of the distribution of the slope of the recovering and delayed onset trajectories to be higher or lower than zero, respectively, as this would change the clinical interpretation of the trajectory completely. This resulted in a slope variance of 0.005 for both trajectories. For the chronic trajectory, we specified that 0.001% of the slopes could be lower than the slopes for the recovering trajectory (slope variance: 0.005), thus the symptom severity for the chronic trajectory was not allowed to decrease more than the severity in the recovering trajectory. For the resilient trajectory, we specified that 0.001% of the slopes could be higher than the slopes for the delayed onset trajectory (slope variance: 0.05), meaning that the symptom severity for the resilient trajectory was not allowed to increase more than the severity in the delayed onset trajectory.
Dirichlet priors designating the expected size of each latent trajectory were based on meta-analytic findings of the mean relative trajectory prevalence amongst prospective and longitudinal studies of latent trajectories of trauma-related psychopathology following traumatic events (Galatzer-Levy et al., 2018). As not all included studies identified exactly these four trajectories, their respective relative prevalence rates did not add up to 100%. Therefore, the estimated Dirichlet priors were adapted, using meta-regression findings on the same set of studies. The estimated relative prevalence rates of the trajectories were subsequently recalculated into expected absolute size per trajectory and incorporated into the Dirichlet priors with the delayed onset category as the reference for men and women separately (see Table 2). Default prior specifications of Mplus Version 8.4 were used for the variance-covariance parameters and residuals.
2.5. Posterior model results and sensitivity analyses
Upon specification of the statistical model and the priors, the model was estimated using one Markov Chain Monte Carlo (MCMC) chain to prevent label switching, with a fixed number of fbiterations of at least 500,000. To assess the model performance for the purpose of research question 1, posterior predictive p-values (PPP) (Meng, 1994), prior-posterior predictive p-values (PPPP) (Asparouhov, 2017; Hoijtink & van de Schoot, 2018), and entropy was appraised. Convergence was assumed if the potential scale reduction value (PSR, (Gelman, 1992) was below 1.05 for all batches of iterations post burn-in. We additionally performed a set of sensitivity analyses to assess the impact of the priors and stability of the models, applying the same seed value across models.
For a first set of sensitivity analyses, we compared the stability of the results regarding convergence and general trends to assess whether the same trajectories were obtained in terms of general trend of the trajectories between the primary models and informative models with different variances around the mean intercept priors (calculated variance: *0; *0.5; *2; *10) and mean slope priors (calculated variances: *0; *0.5; *2; *10; *100; *250). Second, we ran informative models with the same parameter specification but with a different number of trajectories estimated and compared model fit and general trends of the primary models to: a 3-class model without the informative priors specifying the delayed onset class; a 4-class model with non-informative (default) priors instead of informative priors for the delayed onset class; and a 5-class model using non-informative priors for the 5th class. Third, we compared the solution of the primary models with: a 4-class model with non-informative priors instead of informative priors; the primary 4-class model with an added quadratic slope with non-informative priors. Finally, we reran the primary model, additionally including the effects of RCT participation on the intercept and slope to preclude that the intervention provided in the embedded RCT influenced the results.
2.6. In depth exploration and sex differences in primary models
For research question 2, sex differences in the results from the primary model were explored using the 95% HPD intervals of the estimated mean intercepts and slopes for all trajectories. To further explore the primary models and their potential sex differences, we saved the participants’ estimated probabilities for each trajectory, exported these into SPSS (Version 26, IBM) and assigned each participant to one of the four trajectories based on whichever had the highest probability for the specific participant. This is the most frequently used method applied in the field of PTSD (van de Schoot, Sijbrandij, Winter, Depaoli, & Vermunt, 2017). We further explored the obtained results by plotting the mean and individual observed CAPS scores over time for each trajectory (the latter for a random subset of n = 40 men and n = 40 women assigned to the resilient trajectory and for all participants assigned to the smaller trajectories).
For research question 3, we additionally investigated sex differences in the prevalence of trajectory assignments using Bayesian Chi square tests (Bayes Factor: 01, JASP software version 0.14.1, 2020).
For research question 4, we ran the primary model on the whole sample, saved and extracted the participants estimated posterior probabilities into SPSS, assigned the participant to trajectories based on the highest probability, and compared the obtained results between the whole-sample and sex-disaggregated models. Then we performed Bayesian chi-square tests to assess potential sex differences in trajectory assignment.
3. Results
3.1. Bayesian LGMM
Addressing research question 1, we first ran the primary models in the sex-disaggregated samples. These successfully converged in both disaggregated sex-samples. Estimated CAPS scores at all assessments are provided in Figures 2A and 2B for men and women, respectively.
Figure 2.
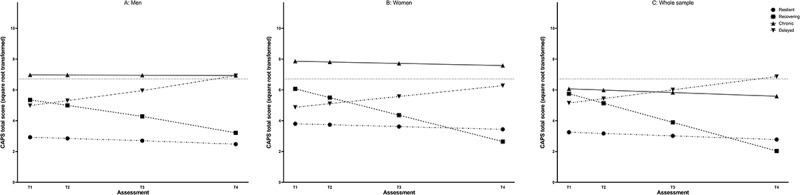
Model-estimated CAPS total scores for the trajectories in the primary Bayesian linear growth mixture models. Figure A, B, and C depict the estimated mean square root CAPS total scores obtained from the primary models for the men, women and whole sample respectively.
The dashed line represents the square root transformed clinical cut-off for probable PTSD at CAPS total score = 45.
For the male model, the PPP (.374) and PPPP (.431) were very close to .50, with an entropy of .678. For the expected resilient trajectory (estimated posterior probability: .681), estimated CAPS scores were low at baseline and significantly further decreased over time (intercept: 2.926 (95%HPD: 2.648, 3.207), slope: −0.037 (95%HPD: −0.069, −0.007)). For the expected chronic trajectory (estimated posterior probability: .081), estimated CAPS scores were continuously high (intercept: 6.975 (95%HPD: 6.073, 7.867), slope: −.003 (95%HPD: −0.085, −0.085, 0.081)). The expected recovering (estimated posterior probability: .182) and delayed onset trajectories (estimated posterior probability: .056) had comparable estimated CAPS scores at baseline (i.e. their 95%HPD intervals overlapped: recovering intercept: 5.349 (95%HPD: 4.595, 6.158), delayed onset intercept: 4.980 (95%HPD: 4.209, 5.756)), but the recovering trajectory showed a significant decrease over time (slope: −0.178 (95%HPD: −0.271, −0.08), while the delayed onset trajectory showed a significant increase over time (0.162 (95%HPD: 0.075, 0.244)).
For the female model, the PPP (.463) and PPPP (.503) were again close to .50, with an entropy of .710. The obtained solution in terms of the observed trends in the chronic (estimated posterior probability: .076, intercept: 7.859 (95%HPD: 6.801, 8.901), slope: −0.023 (95%HPD: −0.106, 0.062)) and recovering trajectories (estimated posterior probability: .205, intercept: 6.072 (95%HPD: 5.377, 6.766), slope: −0.285 (95%HPD −0.362, −0.197)) were similar to those observed in men. CAPS scores in the resilient trajectory were continuously low (estimated posterior probability: .675, intercept: 3.800 (95%HPD: 3.400, 4.217), slope: −0.300 (95%HPD: −0.068, 0.043)), without significant change over time. However, for the expected delayed onset trajectory, the 95%HPD interval for the slope did just include zero, indicating a very low probability for an increase in CAPS scores over time (estimated posterior probability: .044, intercept: 4.873 (95%HPD: 3.902, 5.837), slope: 0.117 (95%HPD: −0.001, 5.837).
3.2. Sensitivity analyses
For both men and women, the primary 4-class models were deemed stable, leading to the same results in terms of general trends when the variance around the mean intercept was increased up to twofold and when the variance around the linear slope was increased up to twofold and 10-fold for the female and male models, respectively (see supplementary table 2). For both sex-disaggregated models, the fit for the primary 4-class model was comparable to the 3-class model without the delayed onset class (see supplementary). Yet, as the delayed onset trajectory contains a clinically relevant group which would otherwise not be distinguished, we opted to maintain this solution instead of the more parsimonious 3-class model. For both primary models, model fit was superior compared to a 4-class model with non-informative priors and a 4-class model with an unspecified class instead of the delayed onset class. Within the men, the fit was comparable to a 5-class model with an unspecified additional class, but as this merely resulted in another resilient trajectory and thus had no added clinical value, the more parsimonious primary 4-class model was maintained. Within women, the fit of the primary model was better than that of the 5-class model with an unspecified additional class. The model with an added quadratic slope with non-informative priors decreased the model fit in women but increased the model fit in men. In men, this model resulted in two classes with decreasing symptoms over time, at the loss of the delayed onset class. Additional sensitivity analyses showed no significant impact of RCT participation on the estimated trajectories (see supplementary results).
3.3. Sex differences in trajectory growth parameters
With regard to research question 2, the 95%HPDs for the obtained growth parameters in the primary sex-disaggregated models indicated a difference in the intercept of the resilient trajectories between men and women, with a higher intercept (i.e. higher CAPS score at baseline) in women compared to men. All other 95%HPDs overlapped, suggesting no additional significant differences. Thus, the course of CAPS scores over time within the smaller sex-disaggregated trajectories was highly similar.
Observed mean CAPS scores at all assessments for each trajectory are provided in Figures 3A and 3B and individual CAPS scores at all assessments for each trajectory are provided in supplementary Figures 1 and 2 for men and women, respectively. General trends within these observed CAPS scores fit with the observed general trends within the growth parameters and the estimated means in the primary model.
Figure 3.
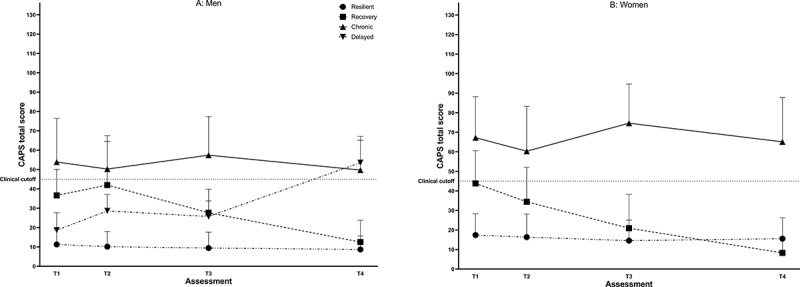
Observed non-transformed CAPS total scores for men (A) and women (B) assigned to each of the trajectories in the sex-disaggregated analyses.
CAPS total scores are depicted as mean and standard deviation. The dashed line represents the clinical cut-off for probable PTSD at CAPS total score = 45. Graph B depicts only three trajectories as no women were assigned to the delayed onset trajectory based on their highest probability for belonging to each trajectory.
3.4. Sex differences in trajectory prevalence
Addressing research question 3, that is, the relative prevalence of all trajectories, women were more often assigned to the recovering trajectory while men were more often assigned to the delayed onset trajectory (BF01(554): 6.139 in favour of the alternative hypothesis of unequal trajectory counts across sexes, see Table 3A).
Table 3.
Sex differences in prevalence of trajectories upon assignment based on highest estimated posterior probability
| Men (n = 346) | Women (n = 208) | |
|---|---|---|
| 3A: Sex-disaggregated models | ||
| Resilient | 269 (77.7%) | 160 (76.9%) |
| Recovering | 36 (10.4%) | 31 (14.9%) |
| Chronic | 29 (8.4%) | 17 (8.2%) |
| Delayed onset | 12 (3.5%) | 0 (0%) |
| 3B: Whole sample model | ||
| Resilient | 278 (80.3%) | 153 (73.6%) |
| Recovering | 14 (4%) | 18 (8.7%) |
| Chronic | 42 (12.1%) | 36 (17.3%) |
| Delayed onset | 12 (3.5%) | 1 (0.5%) |
3.5. Comparison with whole sample model
In order to answer research question 4, we repeated the primary informative 4-class model in the whole sample, combining men and women. The fit for this model in terms of PPP (.253) was lower than for the sex-disaggregated samples, while the PPPP (.500) fit was comparable to that of the female model and somewhat better than that of the male model. Entropy (.652) was lower for the whole sample than for the sex-disaggregated samples.
The general trends of the observed trajectories were highly comparable to those observed in the sex-disaggregated samples (see Figure 2C). For the expected chronic trajectory, estimated CAPS scores were continuously high (intercept: 6.975 (95%HPD: 6.073, 7.867), slope: −.003 (95%HPD: −0.085, −0.085, 0.081)). The expected recovering and delayed onset trajectories had comparable estimated CAPS scores at baseline (i.e. their 95% HPD s overlapped: recovering intercept: 5.349 (95%HPD: 4.595, 6.158), delayed onset intercept: 4.980 (95%HPD: 4.209, 5.756)). As expected, in terms of slope, the recovering trajectory showed a significant decrease over time (−0.178 (95%HPD: −0.271, −0.08)), while the delayed onset trajectory showed a significant increase over time (0.162 (95%HPD: 0.075, 0.244)). The 95%HPD intervals for the growth parameters of the whole and sex-disaggregated samples all overlapped.
There were noticeable differences in the estimated posterior probabilities of belonging to the recovering and chronic trajectories between the whole and sex-disaggregated samples. The probability for the recovering trajectory in the whole sample (.099) was about half that of the probability in the sex-disaggregated samples (men: .182, women: .205) while it was more than twice as high for the chronic trajectory (whole: .176, men: .081, women: .076). The probabilities for the resilient (whole: .671, men: .678, women: .690) and delayed onset (whole. 054, men: .056, women: .044) trajectories were comparable between samples. We observed the same pattern when assigning participants to specific trajectories based on their highest estimated posterior probabilities, with the relative prevalence of the recovering trajectory lower in the whole sample (5.8%) compared to the sex-disaggregated samples (men: 10.4%; women: 14.9%) and the relative prevalence of the chronic trajectory about twice as high (whole: 14.1%; male: 8.4%; female: 8.2%). The prevalence for the resilient trajectories was highly similar (whole: 77.8%; men: 77.7%; women: 76.9%), while that of the delayed onset trajectory (2.3%) was about the average of that in the sex-disaggregated samples (men: 3.5%, women: 0%).
Just as for the sex-disaggregated models, women were more often assigned to the recovering trajectory while men were more often assigned to the delayed onset trajectory. In contrast to the results from the sex-disaggregated samples, women were more often assigned to the chronic trajectory, while men were more often assigned to the resilient trajectory (BF01(554): 1.956; see Table 3B).
4. Discussion
We investigated sex differences in general trends, course and prevalence of PTSD symptom trajectories within one year following trauma. For this purpose, we employed Bayesian latent growth mixture modelling with informative priors on sex-disaggregated samples of emergency department patients admitted with suspected serious injury. Notably, we used the same priors for the analyses within the male and female samples. This was a forced choice, as previous literature did not provide any sex-disaggregated data to derive sex-specific priors from. Consequently, our informative priors did not pre-assume any sex differences and as such did not influence our findings. Within the sex-disaggregated samples, the four most commonly observed trajectories, i.e. resilience, recovery, chronic symptoms and delayed onset, emerged in both women and men. Within these trajectories, PTSD symptom courses, including initial symptom severity and changes in severity over time, were largely comparable between sexes. The only differences were that resilient women showed higher symptoms than resilient men. Prevalence differences emerged for two out of the four trajectories: Women were disproportionately more often assigned to the recovery trajectory than men. The delayed trajectory was more prevalent in men, with no women assigned into this trajectory, based on their highest estimated probability. Thus, our sex-disaggregated results showed limited differences in PTSD trajectory general trends, courses and prevalence rates between men and women. Women were not overrepresented within the trajectories with high PTSD symptom severity at the final assessment, i.e. the chronic and delayed trajectories. In line with this, we also did not observe a significant sex difference endpoint PTSD prevalence rates in our sample.
These findings apparently contrast previous evidence that suggested a greater PTSD risk in women. This evidence comes mostly from studies that applied the endpoint PTSD approach (Gavranidou & Rosner, 2003; Shalev et al., 2019; Tolin & Foa, 2006), but also from several studies that used trajectory-oriented approaches (Berntsen et al., 2012; Bryant et al., 2015; Johannesson et al., 2015; Lowe et al., 2021; Orcutt et al., 2004; Pietrzak et al., 2014). Our finding might be at least partially ascribed to sex differences in trauma type, which is another known moderator of endpoint PTSD (Tolin & Foa, 2006). Although all our participants were transported to the hospital for hospital evaluation because of suspected serious injuries, women’s injuries more often resulted from motor vehicle accidents, whereas men more often experienced other accidents or assault. As interpersonal trauma is associated with higher conditional PTSD risk (Kessler et al., 2017), this may have contributed to the absence of sex differences in our sample. Additionally, men had more a lower educational level compared to women, which also has been associated with higher conditional PTSD risk (Brewin, Andrews, & Valentine, 2000). Furthermore, although it was previously found that subjective rather than objective injury severity predicted subsequent PTSD symptoms after traumatic injury (Gabert-Quillen, Fallon, & Delahanty, 2011), we cannot exclude that the higher injury severity in men within our sample also impacted our results. In any case, our results seem to contradict the notion of a generally increased female vulnerability that goes over and above the impact of trauma-related and demographic factors associated with higher conditional PTSD risk.
Looking at the specific trajectories, however, it is interesting to note that the delayed onset trajectory was more prevalent in men. This is in line with the consistent emergence of this trajectory in previous trajectory-oriented studies with all- or predominantly male samples (Berntsen et al., 2012; Boasso, Steenkamp, Nash, Larson, & Litz, 2015; Dickstein, Suvak, Litz, & Adler, 2010; Eekhout, Reijnen, Vermetten, & Geuze, 2016), and the consistent absence of this trajectory in all- or predominantly female samples (Armour et al., 2012; Self-Brown, Lai, Harbin, & Kelley, 2014; Self-Brown, Lai, Thompson, McGill, & Kelley, 2013). In these previous studies, male samples were commonly exposed to trauma in a professional, mostly military, context, while the female samples included civilian populations. This makes it difficult to disentangle the effects of sex/gender and trauma population and type. Therefore, we investigated differences between women and men within a relatively homogenous population of civilians with suspected serious injury, to enable a more direct investigation of sex differences. Even though the trauma type leading to the suspected injuries warranting hospital evaluation and the injury severity differed somewhat between men and women, from our findings we tentatively conclude that male sex/gender increases the risk to belong to the delayed onset symptom trajectory over and above the effects of trauma population and type.
There are some interesting parallels between the observed higher prevalence of the recovery trajectory in women within our sample and the previous evaluations of responses to trauma-focused psychotherapy that indicated stronger symptom remission in women than men (Wade et al., 2016). Trauma-focused psychotherapy promotes extinction learning, which is likely also involved in natural recovery from acute PTSD symptoms (Rothbaum & Davis, 2003), and it would be of interest to further explore sex differences in this particular neurocognitive mechanism upon traumatic stress. However, although we did find that allocation to the intervention or non-intervention condition did not impact our results, we did not evaluate the impact of and potential sex differences within additional treatment for PTSD symptoms during the study period. Therefore, increased treatment seeking behaviour of women, which is a well-documented finding across mental disorders and cultures (Wang et al., 2007), might serve as an alternative explanation of the increased recovery rates in our sample’s women.
Further mechanisms underlying the observed sex differences in prevalence of the delayed onset and recovery trajectories may be related to (culture-specific) gender-roles or gender-related psychological factors, such as attribution or coping strategies, that are influenced by differential male and female socialization (Christiansen & Berke, 2020; Norris, Perilla, Ibañez, & Murphy, 2001; Okur, Pereda, Van Der Knaap, & Bogaerts, 2019). In addition, sex differences in biological reactivity in the immediate aftermath and first weeks after the traumatic events may be involved. For example, autonomic and endocrine responses within the emergency department were previously found to differentiate between the four PTSD symptom trajectories within our cohort, as determined from self-reported symptoms within the non-sex-disaggregated samples (Schultebraucks et al., 2021). While sex differences in these responses and their association with PTSD symptom trajectories were not investigated in this study, there is increasing evidence for their existence (Seligowski et al., 2021). These potential aetiological factors should be further investigated.
The results on sex differences in the prevalence rates of PTSD symptom trajectories obtained from the sex-disaggregated samples differed from those obtained from the whole sample. The latter approach had a worse model fit and was thus not used for basing our final conclusions on. The most important difference between both approaches was that when we first specified PTSD symptom trajectories within the whole sample, we found that women were more often assigned to the chronic trajectory than men. This finding did not emerge when we investigated the difference in the prevalence rates from the respective sex-disaggregated samples. Thus, our findings based on the analyses within the whole sample actually supported the common assumption that women tend to develop chronic or clinical PTSD symptoms more often. However, this is likely a statistical artefact driven by the overrepresentation of men (62.5%) within our whole sample, which lead to inadvertent assignment of resilient women with symptoms well below (sub)clinical threshold levels into the chronic trajectory. This interpretation is supported by the results from our sex-disaggregated analyses, in which symptom levels of resilient women were significantly higher than those of resilient men, albeit clearly below (sub)clinical thresholds. Methodological research has shown that latent models estimated without the appropriate inclusion of the effects of the predictors of interest may result in biased conclusions (Vermunt, 2010). Our whole sample model was likely affected by this. However, the approach we applied in the whole sample model fits with the predominant approach within the field, as the previous studies that investigated sex-and gender-differences in PTSD trajectory prevalence rates all seem to have added sex either as a predictor of class assignment after latent model estimation (as was our whole sample approach), or as fixed regressor across classes during latent model estimation. Consequently, we tentatively assume that the observed estimation bias with regard to the trajectory prevalence rates and associated sex differences may also extend to other studies within the field, and may at least partly explain findings of increased risk for non-resilient symptom trajectories in women compared to men (Berntsen et al., 2012; Bryant et al., 2015; Johannesson et al., 2015; Lowe et al., 2021; Orcutt et al., 2004; Pietrzak et al., 2014). Thus, our in-depth analysis of sex-specific PTSD symptom trajectories, their courses and prevalence rates within the sex-disaggregated dataset holds methodological advances compared to previously applied approaches.
Additionally, by using data of emergency care patients, PTSD symptoms were clearly traceable to one specific traumatic event. However, it needs to be noted that, as all patients were treated at the emergency department because of suspected severe injury, our sample is highly specific and not representative for all traumatic event survivors, many of whom do not suffer from or are not treated for (suspected) injuries. Moreover, although our sex-disaggregated sample sizes are considered to be large enough for reliable Bayesian LGMM analyses, the resulting sample sizes of participants assigned to the smaller trajectories are modest and do not allow for further investigation of factors potentially associated with trajectory assignment that may have influenced our results, such as index trauma type and injury severity. Therefore, our results need replication in other datasets in order to increase generalizability. Such datasets would ideally include a higher number of participants, longer follow-up assessments and preferably also include individuals affected by other types of traumas. It remains an interesting question whether the prevalence of women in the delayed trajectory would be higher in studies with larger sample sizes and longer follow-up durations than in the present study.
It further needs to be mentioned that we defined overall PTSD symptom load as outcome of interest, therefore not discriminating between different symptom clusters and not taking potential sex differences in symptom presentation into account. Additionally, we used an instrument that was validated for the DSM-IV, instead of the current DSM-5. Therefore, again, further studies are needed to confirm that our results are generalizable across PTSD symptom clusters and diagnostic instruments. Additionally, we disaggregated our data based on the mere binary differentiation between men and women based on biological sex. We used existing data collected over a decade ago, and since then, sex and gender have been increasingly considered to be continuous rather than dichotomous. Hence, our use of the term sex differences may be considered an oversimplification and a more nuanced differentiation is recommended in the future. Regarding sex-specific risk factors, the impact of hormonal contraception, the menstrual cycle, and relatedly, fluctuating sex hormones on PTSD trajectories was not studied here and deserves more attention in future studies (Kornfield et al., 2018). There is previous evidence on the protective impact of hormonal contraception after trauma (Engel et al., 2019; Ferree, Wheeler, & Cahill, 2012), as well as evidence linking oestrogens to adaptive fear processing (Bierwirth, Sperl, Antov, & Stockhorst, 2021; Ferree & Cahill, 2009; Glover et al. 2012; Milad et al., 2010). Regarding gender-specific factors, it seems particularly promising to investigate the impact of psychological attribution and coping strategies that are influenced by differential male and female socializations (Christiansen & Berke, 2020; Okur et al., 2019).
Our study provides recommendations for how to design future, sex- and gender-sensitive PTSD research. First: collecting longitudinal data on PTSD symptom development and analysing trajectories seems to result in a more nuanced and dynamic picture than the endpoint PTSD approach. Second, our study provides statistical arguments for estimating trajectory-oriented models either in sex-disaggregated datasets or with appropriate inclusion of sex during initial model estimation as a class-varying regressor (Vermunt, 2010). Importantly, our findings of limited sex differences in PTSD symptom trajectories do not diminish the importance of investigating potential differences between men and women in the aetiological mechanisms underlying PTSD development, nor of investigating the potential sex-differential impact of risk and protective factors for PTSD or efficacy of preventive interventions. All these topics for future study warrant the appropriate statistical modelling of sex-specific trajectories and their respective courses. This is especially relevant when ratios between men and women within the sample are imbalanced, as in our study. The Sex and Gender Equity in Research (SAGER) guidelines (Heidari, Babor, De Castro, Tort, & Curno, 2016) also emphasize that sex and gender-sensitive research requires balanced ratios between men and women. In a recent review, this has been operationalized by a minimum of 40% for the underrepresented sex or gender (Rechlin, Splinter, Hodges, Albert, & Galea, 2021). However, imbalanced sex and gender ratios are common for various trauma populations, including emergency department patients as included in our study (Lowe et al., 2021), and will likely occur in cohort studies investigating these populations, unless sex-stratified inclusion is implemented. If (such) sex- or gender-based disaggregation of the dataset or stratified inclusion results in relatively small sample sizes, Bayesian modelling can be applied to provide more precise estimations, especially when also expecting imbalanced and dynamic latent clusters.
To sum up, in this sex-disaggregated Bayesian latent growth mixture modelling analysis of PTSD symptom development in female and male emergency care patients, the same four PTSD symptom trajectories were observed in men and women. Sex differences emerged in the trajectory courses and prevalence rates. Yet, contrary to what may have been expected based on previous research, symptoms were not generally higher in women across trajectories, but only within the resilient trajectory. Further, women were not more often assigned to a trajectory with high long-term PTSD symptom severity, namely, chronic or delayed onset. Our analyses contributed to a more nuanced understanding of the temporal dynamics of PTSD symptom development in men and women. Moreover, they provide additional support for the notion that sex- and gender-sensitive research critically depends on the use of appropriate statistical techniques, to avoid biased model estimations for the underrepresented sex or gender. By applying appropriate statistical analysis techniques and investigating sex- and gender-related factors that impact traumatic event processing and subsequent PTSD symptom development, sex-sensitive approaches can yield direct, practical implications for precision medicine.
Supplementary Material
Funding Statement
This work was supported by the ZonMw, the Netherlands Organization for Health Research and Development [62300038]; Stichting Achmea Slachtoffer en Samenleving (SASS), Aid to Victims [na]; ZonMw, the Netherlands Organization for Health Research and Development [636340004].
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available on request from the corresponding author, Mirjam van Zuiden. The data are not publicly available due to their containment of information that could compromise the privacy of research participants.
Supplementary material
Supplemental data for this article can be accessed here
References
- Armour, C., Shevlin, M., Elklit, A., & Mroczek, D. (2012, Mar). A latent growth mixture modeling approach to PTSD symptoms in rape victims. Traumatology (Tallahass Fla), 18(1), 20–16. doi: 10.1177/1534765610395627 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asparouhov, T., & Muthen, B. (2017). Prior-posterior predictive p-values. Psychological Methods, 23(3), 524–545. doi: 10.1037/met0000113 [DOI] [PubMed] [Google Scholar]
- Baker, S. P., O'Neill, B., Haddon, W., Jr, & Long, W. B. (1974). The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. Journal of Trauma and Acute Care Surgery, 14(3), 187–196. doi: 10.1097/00005373-197403000-00001 [DOI] [PubMed] [Google Scholar]
- Berntsen, D., Johannessen, K. B., Thomsen, Y. D., Bertelsen, M., Hoyle, R. H., & Rubin, D. C. (2012, Dec). Peace and war: Trajectories of posttraumatic stress disorder symptoms before, during, and after military deployment in Afghanistan. Psychological Science, 23(12), 1557–1565. doi: 10.1177/0956797612457389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bierwirth, P., Sperl, M. F. J., Antov, M. I., & Stockhorst, U. (2021, Mar 9). Prefrontal theta oscillations are modulated by estradiol status during fear recall and extinction recall. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 6(11), 1071–1080. doi: 10.1016/j.bpsc.2021.02.011 [DOI] [PubMed] [Google Scholar]
- Boasso, A. M., Steenkamp, M. M., Nash, W. P., Larson, J. L., & Litz, B. T. (2015). The relationship between course of PTSD symptoms in deployed US Marines and degree of combat exposure. Journal of Traumatic Stress, 28(1), 73–78. doi: 10.1002/jts.21988 [DOI] [PubMed] [Google Scholar]
- Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology, 68(5), 748. doi: 10.1037/0022-006X.68.5.748 [DOI] [PubMed] [Google Scholar]
- Bryant, R. A., Nickerson, A., Creamer, M., O’Donnell, M., Forbes, D., Galatzer-Levy, I., … Silove, D. (2015, May). Trajectory of post-traumatic stress following traumatic injury: 6-year follow-up. The British Journal of Psychiatry, 206(5), 417–423. doi: 10.1192/bjp.bp.114.145516 [DOI] [PubMed] [Google Scholar]
- Christiansen, D. M., & Berke, E. T. (2020). Gender-and sex-based contributors to sex differences in PTSD. Current Psychiatry Reports, 22(4), 1–9. doi: 10.1007/s11920-020-1140-y [DOI] [PubMed] [Google Scholar]
- Dickstein, B. D., Suvak, M., Litz, B. T., & Adler, A. B. (2010, Jun). Heterogeneity in the course of posttraumatic stress disorder: Trajectories of symptomatology. Journal of Trauma Stress, 23(3), 331–339. doi: 10.1002/jts.20523 [DOI] [PubMed] [Google Scholar]
- Eekhout, I., Reijnen, A., Vermetten, E., & Geuze, E. (2016, Jan). Post-traumatic stress symptoms 5 years after military deployment to Afghanistan: An observational cohort study. Lancet Psychiatry, 3(1), 58–64. doi: 10.1016/s2215-0366(15)00368-5 [DOI] [PubMed] [Google Scholar]
- Engel, S., van Zuiden, M., Frijling, J. L., Koch, S. B. J., Nawijn, L., Schumacher, S., … Olff, M. (2019, Jun 15). Patterns of recovery from early posttraumatic stress symptoms after a preventive intervention with oxytocin: Hormonal contraception use is a prognostic factor. Biological Psychiatry, 85(12), e71–e73. doi: 10.1016/j.biopsych.2019.01.014 [DOI] [PubMed] [Google Scholar]
- Ferree, N. K., & Cahill, L. (2009, Mar). Post-event spontaneous intrusive recollections and strength of memory for emotional events in men and women. Consciousness and Cognition, 18(1), 126–134. doi: 10.1016/j.concog.2008.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferree, N. K., Wheeler, M., & Cahill, L. (2012, Sep). The influence of emergency contraception on post-traumatic stress symptoms following sexual assault. Journal of Forensic Nursing, 8(3), 122–130. doi: 10.1111/j.1939-3938.2012.01134.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabert-Quillen, C. A., Fallon, W., & Delahanty, D. L. (2011). PTSD after traumatic injury: An investigation of the impact of injury severity and peritraumatic moderators. Journal of Health Psychology, 16(4), 678–687. doi: 10.1177/1359105310386823 [DOI] [PubMed] [Google Scholar]
- Galatzer-Levy, I. R., Ankri, Y., Freedman, S., Israeli-Shalev, Y., Roitman, P., Gilad, M., & Shalev, A. Y. (2013). Early PTSD symptom trajectories: Persistence, recovery, and response to treatment: Results from the Jerusalem trauma outreach and prevention study (J-TOPS). PLoS ONE, 8(8), e70084. doi: 10.1371/journal.pone.0070084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galatzer-Levy, I. R., Huang, S. H., & Bonanno, G. A. (2018, Jul). Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clinical Psychol Review, 63, 41–55. doi: 10.1016/j.cpr.2018.05.008 [DOI] [PubMed] [Google Scholar]
- Galatzer-Levy, I. R., Madan, A., Neylan, T. C., Henn-Haase, C., & Marmar, C. R. (2011, Oct). Peritraumatic and trait dissociation differentiate police officers with resilient versus symptomatic trajectories of posttraumatic stress symptoms. Journal of Trauma Stress, 24(5), 557–565. doi: 10.1002/jts.20684 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gavranidou, M., & Rosner, R. (2003). The weaker sex? Gender and post-traumatic stress disorder. Depress Anxiety, 17(3), 130–139. doi: 10.1002/da.10103 [DOI] [PubMed] [Google Scholar]
- Gelman, A. R, D. B. (1992). Inference from iterative simulation using multiple sequences. Statistical Science, 7, 457–511. doi: 10.1214/ss/1177011136 [DOI] [Google Scholar]
- Ginzburg, K., & Ein-Dor, T. (2011, Nov-Dec). Posttraumatic stress syndromes and health-related quality of life following myocardial infarction: 8-year follow-up. General Hospital Psychiatry, 33(6), 565–571. doi: 10.1016/j.genhosppsych.2011.08.015 [DOI] [PubMed] [Google Scholar]
- Glover, E. M., Fau - Mercer, J. T., B, K., Mercer Kb Fau - Kerley, K., Kerley K Fau - Bradley, B., Bradley B Fau - Ressler, K. J., Norrholm, S. D. (2012). Estrogen levels are associated with extinction deficits in women with posttraumatic stress disorder. Biological Psychiatry, 72(1), 19–24. doi: 10.1016/j.biopsych.2012.02.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heidari, S., Babor, T. F., De Castro, P., Tort, S., & Curno, M. (2016). Sex and gender equity in research: Rationale for the SAGER guidelines and recommended use. Research Integrity and Peer Review, 1(1), 1–9. doi: 10.1186/s41073-016-0006-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hobfoll, S. E., Mancini, A. D., Hall, B. J., Canetti, D., & Bonanno, G. A. (2011, Apr). The limits of resilience: Distress following chronic political violence among Palestinians. Social Science & Medicine, 72(8), 1400–1408. doi: 10.1016/j.socscimed.2011.02.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoijtink, H., & van de Schoot, R. (2018, Sep). Testing small variance priors using prior-posterior predictive p values. Psychological Methods, 23(3), 561–569. doi: 10.1037/met0000131 [DOI] [PubMed] [Google Scholar]
- Hovens, J. E., van der Ploeg, H. M., Klaarenbeek, M. T., Bramsen, I., Schreuder, J. N., & Rivero, V. V. (1994, May). The assessment of posttraumatic stress disorder: With the clinician administered PTSD scale: Dutch results. Journal of Clinical Psychology, 50(3), 325–340. doi: 10.1002/1097-4679(199405)50:3 [DOI] [PubMed] [Google Scholar]
- Johannesson, K. B., Arinell, H., & Arnberg, F. K. (2015, Dec). Six years after the wave. Trajectories of posttraumatic stress following a natural disaster. Journal of Anxiety Disorders, 36, 15–24. doi: 10.1016/j.janxdis.2015.07.007 [DOI] [PubMed] [Google Scholar]
- Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., … Koenen, K. C. (2017). Trauma and PTSD in the WHO world mental health surveys. European Journal of Psychotraumatology, 8(sup5), 1353383. 2017/October/27. 10.1080/20008198.2017.1353383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kornfield, S. L., Hantsoo, L., & Epperson, C. N. (2018, May 18). What does sex have to do with it? The role of sex as a biological variable in the development of posttraumatic stress disorder. Current Psychiatry Reports, 20(6), 39. doi: 10.1007/s11920-018-0907-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Brocque, R. M., Hendrikz, J., & Kenardy, J. A. (2010). Parental response to child injury: Examination of parental posttraumatic stress symptom trajectories following child accidental injury. Journal of Pediatric Psychology, 35(6), 646–655. doi: 10.1093/jpepsy/jsq035 [DOI] [PubMed] [Google Scholar]
- Lowe, S. R., Ratanatharathorn, A., Lai, B. S., van der Mei, W., Barbano, A. C., Bryant, R. A., … Kessler, R. C. (2021, May). Posttraumatic stress disorder symptom trajectories within the first year following emergency department admissions: Pooled results from the International Consortium to predict PTSD. Psychological Medicine, 51(7), 1129–1139. doi: 10.1017/s0033291719004008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meng, X.-L. (1994). Posterior Predictive $p$-Values. The Annals of Statistics, 22(3), 1142–1160, 1119. doi: 10.1214/aos/1176325622 [DOI] [Google Scholar]
- Milad, M. R., Zeidan, M. A., Contero, A., Pitman, R. K., Klibanski, A., Rauch, S. L., & Goldstein, J. M. (2010, Jul 14). The influence of gonadal hormones on conditioned fear extinction in healthy humans. Neuroscience, 168(3), 652–658. doi: 10.1016/j.neuroscience.2010.04.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mouthaan, J., Sijbrandij, M., de Vries, G. J., Reitsma, J. B., van de Schoot, R., Goslings, J. C., … Olff, M. (2013, Aug 13). Internet-based early intervention to prevent posttraumatic stress disorder in injury patients: Randomized controlled trial. The Journal of Medical Internet Research, 15(8), e165. doi: 10.2196/jmir.2460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mouthaan, J., Sijbrandij, M., Reitsma, J. B., Gersons, B. P., & Olff, M. (2011). Internet-based prevention of posttraumatic stress symptoms in injured trauma patients: Design of a randomized controlled trial. European Journal of Psychotraumatology, 2(1), 8294. doi: 10.3402/ejpt.v2i0.8294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mouthaan, J., Sijbrandij, M., Reitsma, J. B., Gersons, B. P., & Olff, M. (2014). Comparing screening instruments to predict posttraumatic stress disorder. PLoS ONE, 9(5), e97183. doi: 10.1371/journal.pone.0097183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén, L. K., and Muthén, B. O. (2017). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Norris, F. H., Perilla, J. L., Ibañez, G. E., & Murphy, A. D. (2001). Sex differences in symptoms of posttraumatic stress: Does culture play a role? Journal of Traumatic Stress, 14(1), 7–28. doi: 10.1023/A:1007851413867 [DOI] [Google Scholar]
- Okur, P., Pereda, N., Van Der Knaap, L. M., & Bogaerts, S. (2019, Apr). Attributions of blame among victims of child sexual abuse: Findings from a community sample. J Child Sex Abus, 28(3), 301–317. doi: 10.1080/10538712.2018.1546249 [DOI] [PubMed] [Google Scholar]
- Olff, M. (2017). Sex and gender differences in post-traumatic stress disorder: An update. European Journal of Psychotraumatology, 8(sup4), 1351204. 2017/November/29. 10.1080/20008198.2017.1351204 [DOI] [Google Scholar]
- Orcutt, H. K., Erickson, D. J., & Wolfe, J. (2004, Jun). The course of PTSD symptoms among Gulf War veterans: A growth mixture modeling approach. Journal of Trauma Stress, 17(3), 195–202. doi: 10.1023/B:JOTS.0000029262.42865.c2 [DOI] [PubMed] [Google Scholar]
- Pielmaier, L., Milek, A., Nussbeck, F. W., Walder, B., & Maercker, A. (2013). Trajectories of posttraumatic stress symptoms in significant others of patients with severe traumatic brain injury. Journal of Loss and Trauma, 18(6), 521–538. doi: 10.1080/15325024.2012.719342 [DOI] [Google Scholar]
- Pietrzak, R. H., Feder, A., Singh, R., Schechter, C. B., Bromet, E. J., Katz, C. L., … Southwick, S. M. (2014, Jan). Trajectories of PTSD risk and resilience in world trade center responders: An 8-year prospective cohort study. Psychological Medicine, 44(1), 205–219. doi: 10.1017/s0033291713000597 [DOI] [PubMed] [Google Scholar]
- Pietrzak, R. H., Van Ness, P. H., Fried, T. R., Galea, S., & Norris, F. H. (2013, Apr). Trajectories of posttraumatic stress symptomatology in older persons affected by a large-magnitude disaster. Journal of Psychiatric Research, 47(4), 520–526. doi: 10.1016/j.jpsychires.2012.12.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rechlin, R. K., Splinter, T. F. L., Hodges, T. E., Albert, A. Y., & Galea, L. A. M. (2021). Harnessing the power of sex differences: What a difference ten years did not make. bioRxiv. 2021-01-0100:00: 00. doi: 10.1101/2021.06.30.450396. [DOI] [Google Scholar]
- Rothbaum, B. O., & Davis, M. (2003). Applying learning principles to the treatment of post‐trauma reactions. Annals of the New York Academy of Sciences, 1008(1), 112–121. [DOI] [PubMed]
- Schultebraucks, K., Sijbrandij, M., Galatzer-Levy, I., Mouthaan, J., Olff, M., & van Zuiden, M. (2021). Forecasting individual risk for long-term posttraumatic stress disorder in emergency medical settings using biomedical data: A machine learning multicenter cohort study, Neurobiology of Stress, 14, 100297, 2021/May/01/. doi: 10.1016/j.ynstr.2021.100297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Self-Brown, S., Lai, B. S., Harbin, S., & Kelley, M. L. (2014). Maternal posttraumatic stress disorder symptom trajectories following Hurricane Katrina: An initial examination of the impact of maternal trajectories on the well-being of disaster-exposed youth. International Journal of Public Health, 59(6), 957–965. doi: 10.1007/s00038-014-0596-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Self-Brown, S., Lai, B. S., Thompson, J. E., McGill, T., & Kelley, M. L. (2013). Posttraumatic stress disorder symptom trajectories in Hurricane Katrina affected youth. Journal of Affective Disorders, 147(1–3), 198–204. doi: 10.1016/j.jad.2012.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seligowski, A. V., Steuber, E. R., Hinrichs, R., Reda, M. H., Wiltshire, C. N., Wanna, C. P., and Jovanovic, T. (2021). A prospective examination of sex differences in posttraumatic autonomic functioning, Neurobiology of Stress, Vol. 15. 100384. 10.1016/j.ynstr.2021.100384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shalev, A. Y., Gevonden, M., Ratanatharathorn, A., Laska, E., van der Mei, W. F., Qi, W., … Koenen, K. C. (2019, Feb). Estimating the risk of PTSD in recent trauma survivors: Results of the International Consortium to Predict PTSD (ICPP). World Psychiatry, 18(1), 77–87. doi: 10.1002/wps.20608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., … Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59(20), 22–33;quiz 34–57. [PubMed] [Google Scholar]
- Smid, S. C., McNeish, D., Miočević, M., & van de Schoot, R. (2020). Bayesian versus frequentist estimation for structural equation models in small sample contexts: A systematic review. Structural Equation Modeling: A Multidisciplinary Journal, 27(1), 131–161. 2020/January/02. 10.1080/10705511.2019.1577140 [DOI] [Google Scholar]
- Steenkamp, M. M., Dickstein, B. D., Salters-Pedneault, K., Hofmann, S. G., & Litz, B. T. (2012, Aug). Trajectories of PTSD symptoms following sexual assault: Is resilience the modal outcome? Journal of Trauma Stress, 25(4), 469–474. doi: 10.1002/jts.21718 [DOI] [PubMed] [Google Scholar]
- Teasdale, G., & Jennett, B. (1974). Assessment of coma and impaired consciousness: A practical scale. The Lancet, 304(7872), 81–84. doi: 10.1016/S0140-6736(74)91639-0 [DOI] [PubMed] [Google Scholar]
- Tolin, D. F., & Foa, E. B. (2006, Nov). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132(6), 959–992. doi: 10.1037/0033-2909.132.6.959 [DOI] [PubMed] [Google Scholar]
- van de Schoot, R., Sijbrandij, M., Depaoli, S., Winter, S. D., Olff, M., & van Loey, N. E. (2018, Mar-Apr). Bayesian PTSD-Trajectory analysis with informed priors based on a systematic literature search and expert elicitation. Multivariate Behavioral Research, 53(2), 267–291. doi: 10.1080/00273171.2017.1412293 [DOI] [PubMed] [Google Scholar]
- van de Schoot, R., Sijbrandij, M., Winter, S. D., Depaoli, S., & Vermunt, J. K. (2017). The GRoLTS-Checklist: Guidelines for reporting on latent trajectory studies. Structural Equation Modeling: A Multidisciplinary Journal, 24(3), 451–467. 2017/May/04. 10.1080/10705511.2016.1247646 [DOI] [Google Scholar]
- van Vliet, I. M., & de Beurs, E. (2007). The MINI-international neuropsychiatric interview. A brief structured diagnostic psychiatric interview for DSM-IV en ICD-10 psychiatric disorders. Tijdschrift voor Psychiatrie, 49(6), 393–397. [PubMed] [Google Scholar]
- Vermunt, J. K. (2010). Latent class modeling with covariates. Polit Analys, 18(4), 450. doi: 10.1093/pan/mpq025 [DOI] [Google Scholar]
- Wade, D., Varker, T., Kartal, D., Hetrick, S., O’Donnell, M., & Forbes, D. (2016). Gender difference in outcomes following trauma-focused interventions for posttraumatic stress disorder: Systematic review and meta-analysis. Psychological Trauma: Theory, Research, Practice, and Policy, 8(3), 356. doi: 10.1037/tra0000110 [DOI] [PubMed] [Google Scholar]
- Wang, P. S., Aguilar-Gaxiola, S., Alonso, J., Angermeyer, M. C., Borges, G., Bromet, E. J., … Gureje, O. (2007). Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. The Lancet, 370(9590), 841–850. doi: 10.1016/S0140-6736(07)61414-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weathers, F. W., Newman, E., Blake, D. D., Nagy, L. M., Schnurr, P. P., Kaloupek, D., & Keane, T. (2004). Clinician-administered PTSD Scale:(CAPS). Torrance, CA: Western Psychological Services. [Google Scholar]
- Weathers, F. W., Ruscio, A. M., & Keane, T. M. (1999). Psychometric properties of nine scoring rules for the clinician- administered posttraumatic stress disorder scale. Psychological Assessment, 11(2), 124–133. doi: 10.1037/1040-3590.11.2.124 [DOI] [Google Scholar]
- Wickham, H. (2016). ggplot2: Elegant graphics for data analysis. New York: Springer-Verlag. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, Mirjam van Zuiden. The data are not publicly available due to their containment of information that could compromise the privacy of research participants.