

1. Introduction
Anxiety is an important mental health disorder during pregnancy as over half of pregnant women experience anxiety symptoms (Meades & Ayers 2011). Latinas, mainly of Mexican descent, report some of the highest levels of anxiety symptoms (20–36%) (Lara-Cinisomo, Fujimoto, Oksas, Jian, & Gharheeb 2019) compared to the general population (15–17%) (Fairbrother, Janssen, Antony, Tucker, & Young 2016). This is particularly problematic as perinatal anxiety is associated with a host of adverse maternal, birth, and infant outcomes (Davis et al. 2004; Leis, Heron, Stuart, & Mendelson 2014; O’Connor, Heron, Golding, Glover, & the 2003; Tomfohr-Madsen et al. 2019). Thus, identification of culturally relevant factors to buffer against anxiety symptoms are needed. A recent review identified religiosity, an important value of Mexican culture, as a protective factor against postpartum depression (Lara-Cinisomo, Wood, & Fujimoto 2019), but the role of religion as a protective factor in perinatal anxiety is not known.
Perinatal anxiety is common as pregnancy is a period of transition in a woman’s life in which changes in expectations and emotional distress occur (Emmanuel & Sun 2014; Lobel & M. Ibrahim 2018). This can be particularly harmful during pregnancy as anxiety is often underdiagnosed (Misri, Abizadeh, Sanders, & Swift 2015) and poses numerous health risks to both the mother and the infant, such as the increased risk for perinatal depression (Robertson, Grace, Wallington, & Stewart 2004), poor behavioral reactivity in infancy (Davis et al. 2004), shorter gestation (Tomfohr-Madsen et al. 2019), and behavioral problems in children (Leis et al. 2014; O’Connor et al. 2003). Pregnant women of Mexican descent are exposed to various psychosocial and sociocultural stressors that may predispose them to anxiety symptoms. These include being of low socioeconomic status (Bernstein 2007; Williams, Mohammed, Leavell, & Collins 2010), having lower rates of education (Stepler & Brown 2016), less access to insurance (Motel & Patten 2012; Rutledge & McLaughlin 2008), and less access to prenatal care (Osterman & Martin 2011) compared to the general population. Additionally, sociocultural stressors such as acculturative stress, the psychological distress associated with the process of adapting to a new culture (Berry 2006), have been associated with greater perinatal depressive symptoms (D’Anna-Hernandez, Aleman, & Flores 2015; Zeiders, Hoyt, & Adam 2014) and elevated anxiety trajectories across pregnancy (Preciado & D’Anna-Hernandez 2017). Thus, Mexican American women are at risk for perinatal anxiety and protective factors are needed.
Religiosity is considered a central aspect of Mexican culture and is often defined as a set of values, beliefs, and rituals (Hill & Pargament 2003; Lerman et al. 2018). In general, religiosity is linked to a lower prevalence of mental health problems (Bonelli & Koenig 2013; Wong, Rew, & Slaikeu 2006), though much of this work has focused on depression. During pregnancy, a similar protective relationship exists between religiosity and depressive symptoms (Lara-Cinisomo, Wood, et al. 2019; Mann, McKeown, Bacon, Vesselinov, & Bush 2007). However, in the general population, this relationship only existed in pregnancy (Mann et al. 2007) and not the postpartum period, but in the Mexican population, the postpartum period seemed to be the more sensitive timepoint (Lara-Cinisomo, Fujimoto, et al. 2019; Lara-Cinisomo, Wood, et al. 2019). Together these studies suggest that the effects of religiosity on depression may be temporal during the perinatal period. However, the relationship between religiosity and anxiety is less studied. One review found that 40% of the 10 studies included showed religiosity buffered against generalized anxiety in adults (Khalaf, Hebborn, Dal, & Naja 2015). Similarly, among pregnant women in the U.S. South, religiosity was associated with lower odds of anxiety symptoms and screening positive for moderate/severe anxiety (Mann, McKeown, Bacon, Vesselinov, & Bush 2008). However, others found that religiosity did not significantly predict pregnancy-specific anxiety (Arch 2013). Alternatively, among English-speaking pregnant and postpartum Latinas, religiosity was associated with greater perceived stress (Mann, Mannan, Quiñones, Palmer, & Torres 2010). Thus, more work is needed to elucidate the association between religiosity and anxiety in pregnant women of Mexican descent.
Religiosity is a salient factor in Mexican culture (Lerman et al. 2018) and adherence to traditional Mexican cultural values often buffers the adverse effects of acculturative stress on perinatal depressive symptoms (Berkel et al. 2010; Calzada & Sales 2019; D’Anna-Hernandez et al. 2015). In adults of Mexican descent, greater religious support seeking was associated with less acculturative stress (Finch & Vega 2003). However, in another study, religious involvement exacerbated the relationship between acculturative stress and depressive symptoms among adults of Mexican descent (Ellison, Finch, Ryan, & Salinas 2009). This suggests a complex and inconclusive relationship between religion and cultural stressors that needs to be explored further in the Mexican population, particularly during the perinatal period.
The goal of this study was to understand the connection between religiosity and perinatal anxiety, and how it may protect against the effects of sociocultural stressors such as acculturative stress among pregnant women of Mexican descent. We aimed to address two main questions: 1) is religiosity related to perinatal anxiety symptoms across the perinatal period? And 2) does religiosity play a protective role in the relationship between acculturative stress and mental health symptoms? We hypothesized that greater levels of religiosity would be associated with fewer perinatal anxiety symptoms, even when controlling for demographics, cultural orientation, and acculturative stress. Additionally, we predicted that higher religiosity would be associated with a lower trajectory of anxiety symptoms across the perinatal period. It was also hypothesized that religiosity would buffer the relationship between acculturative stress and perinatal anxiety symptoms.
2. Method
2.1. Sample
Two hundred and forty-three pregnant Mexican American women were recruited from a local community clinic in Southern California during their first trimester of pregnancy. To be eligible to participate in the study, women had to be of Mexican descent, at least 18 years old, non-smoking, and non-illicit drug users. Twenty-three participants withdrew from the study because they were no longer interested in participating, 12 participants were lost to follow-up, 8 participants transferred clinics, 2 were removed from the study due to no longer meeting eligibility requirements, and 1 participant had a stillbirth. A final simple of 197 mothers remained for the current study. Our rates of attrition were similar to studies with a similar sample (Lee et al. 2007), and there was no significant difference in anxiety scores between moms who dropped out of the study (M = 37.43, SD = 9.56) and those who remained (M = 35.60, SD = 10.24; t = −1.11, p = .270).
2.2. Procedure
This was a longitudinal design in which participants were seen across four perinatal timepoints: early pregnancy (15–17 weeks gestation), mid-pregnancy (25–27 weeks gestation), late pregnancy (33–35 weeks gestation), and 6 weeks postpartum (45–47 weeks gestation). Participants were recruited during the first trimester of pregnancy when they were less than 15 weeks pregnant. All participants provided written informed consent at recruitment, filled out self-report measures collecting demographic information, and were drug screened. Participant visits were completed during regular prenatal care appointments as well as during scheduled home visits. Self-report questionnaires about mental health symptoms were administered during each time point. Questionnaires about cultural values and stressors were administered during early pregnancy and postpartum. All measures were provided in English and Spanish. Data were collected from June 2012 to August 2019. All procedures were approved by California State University San Marcos Institutional Review Board.
2.3. Measures
2.3.1. Religiosity
The Mexican American Cultural Values Scale (MACVS) is a 50-item measure assessing cultural values linked to Mexican Americans (Knight et al. 2010). For the current study, the 7-item religion subscale was used to assess religiosity. The items asked questions regarding spiritual beliefs and faith. Example items include: “One’s belief in God gives inner strength and meaning to life,” “Parents should teach their children to pray,” and “If everything is taken away, one still has their faith in God.” Items were scored on a 5-point scale, with higher scores indicating greater levels of religiosity. Item responses range from not at all (1) to completely (5). The measure has demonstrated good internal reliability within the current sample (α = .89-.86).
2.3.2. Acculturation status
The Acculturation Rating Scale for Mexican Americans (ARSMA-II) was used to assess levels of Mexican orientation (MO) and Anglo orientation (AO) (Cuellar, Arnold, & Maldonado 1995). The Mexican Orientation Subscale consists of 18 items, and the Anglo Orientation Subscale consists of 30 items. Scale responses range from not at all (1) to extremely often (5). Items are averaged for each subscale, with higher scores indicating greater Anglo or Mexican orientations. The measure has demonstrated good internal reliability within the current sample (MO α = .76-.83, AO α = .94-.95).
2.3.3. Acculturative stress
The Societal, Attitudinal, Environmental, and Familial Acculturative Stress Scale (SAFE) was used to measure levels of acculturative stress. The 24-item scale is rated on a 5-point scale. If the stressor had not occurred, participants indicated does not apply (0). If the stressor had occurred, participants rated their stress from not stressful (1) to extremely stressful (5). Items are summed with greater scores indicating greater levels of acculturative stress, and scores ranged from 0–120. Example items include “It bothers me that family members I am close to do not understand my new values” and “It bothers me when people pressure me to assimilate (or blend in).” The measure has demonstrated good internal reliability within the current sample (α = .90) and has been validated for use among Mexican Americans (Hovey 2000) and pregnant Mexican Americans (D’Anna-Hernandez et al. 2015).
2.3.4. Maternal anxiety symptoms
The State-Trait Anxiety Inventory for Adults (STAI) was used to measure state or current anxiety symptoms and feelings, such as worry and tenseness (Speilberger 1983). A 4-point scale was used to rate 20 state anxiety items. Examples of the items include, “I am worried” and “I feel calm.” Responses range from never (1) to very much so (4). Items are summed to obtain a total score (ranging from 20–80), with greater scores indicating greater levels of anxiety. The STAI been previously used among pregnant Mexican Americans (Lara-Cinisomo, Fujimoto, et al. 2019; Preciado & D’Anna-Hernandez 2017) and the measure has demonstrated good internal reliability within the current sample (α = .90-.89).
2.4. Statistical analysis
All statistical analyses were run in SPSS (v.24). Paired samples t-tests were used to determine if levels of religiosity changed between the prenatal (early pregnancy) and postpartum period, and to justify use of early pregnancy levels of religiosity as a relatively immutable dispositional variable. Bivariate correlations were used to assess relationships between religiosity, cultural orientation, and perinatal anxiety symptoms. To determine whether religiosity predicted lower levels of perinatal anxiety symptoms, hierarchical regression analyses were performed with religiosity entered in block one. In block two, Mexican orientation, Anglo orientation, and acculturative stress were entered as covariates, and in block 3, age, SES, and birthplace were added as covariates. This was done for each of the four time points.
A multilevel modeling analysis was performed to determine if religiosity predicted the trajectory of perinatal anxiety symptoms during pregnancy. An unconditional model was run to assess the variability of anxiety symptoms within and between participants. Perinatal timepoint (time) was entered as an independent variable in the model to predict perinatal anxiety. Time was coded as 0, 1 , 2, 3, such that early pregnancy was 0 and postpartum was 3. Additionally, time was squared and cubed to model quadratic and cubic trends, respectively, to assess the best model fit. Maternal religiosity (early pregnancy) was entered in the model as an independent variable. The interaction term time cubed x religiosity was created and entered as a predictor variable to test how religiosity predicted the trajectory of anxiety symptoms.
Given the evidence that maternal age, SES, and birthplace are associated with maternal mental health (Alhasanat & Giurgescu 2017; Ban et al. 2012; Muraca & Joseph 2014) these were included as covariates in the following analyses. To test the hypothesis that religiosity would buffer the relationship between acculturative stress and anxiety symptoms, moderation analyses using a bootstrapping approach was performed with the PROCESS computational tool for SPSS (Model 1) (Hayes 2013) with acculturative stress entered as an independent variable and maternal prenatal religiosity entered as a moderator to predict anxiety symptoms for each of the four timepoints individually.
3. Results
3.1. Sample characteristics
Maternal characteristics are shown in Table 1.
Table 1.
Maternal Characteristics (N= 197)
| Characteristic | M (SD) | N | % |
|---|---|---|---|
|
| |||
| Age | 28.26 (5.66) | ||
| ≤ 19 | 11 | 5.6 | |
| 20–29 | 106 | 53.8 | |
| 30–39 | 77 | 39.1 | |
| ≥ 40 | 3 | 1.5 | |
| Years in the US | 15.88 (7.23) | ||
| ≤ 9 | 31 | 15.7 | |
| 9–19 | 102 | 51.8 | |
| ≥ 20 | 64 | 32.5 | |
| Birthplace | |||
| Mexico | 148 | 75.1 | |
| US | 49 | 24.9 | |
| Primary language | |||
| Spanish | 143 | 72.6 | |
| English | 20 | 10.2 | |
| English/Spanish | 34 | 17.3 | |
| Parity | 1.63 (1.31) | ||
| Nulliparous | 44 | 22.3 | |
| Primiparous | 55 | 27.9 | |
| Multiparous | 98 | 49.7 | |
| Marital Status | |||
| Married to bio father | 90 | 45.7 | |
| Living with bio father | 65 | 33.0 | |
| Married to non-bio father | 2 | 1.0 | |
| Never married | 33 | 16.8 | |
| Divorced | 3 | 1.5 | |
| Separated | 4 | 2.0 | |
| Employment Status | |||
| Unemployed | 103 | 54.2 | |
| Full-time | 43 | 22.6 | |
| Part-time | 42 | 22.1 | |
| Other | 2 | 1.1 | |
| Years of Education | 10.91 (2.99) | ||
| <12 | 89 | 45.2 | |
| 12 | 63 | 32.0 | |
| >12 | 45 | 22.8 | |
| Income | 24,189.63 (11,708.00) | ||
| < 10,000 | 26 | 13.2 | |
| 11,000–20,000 | 61 | 31.0 | |
| 21,000–30,000 | 63 | 32.0 | |
| 31,000–40,000 | 32 | 16.2 | |
| > 41,000 | 15 | 7.6 | |
| SES | |||
| Hollingshead Score | 23.71 (9.10) | 172 | 87.3 |
| Unknown/ Unable to calculate | 25 | 12.7 | |
3.2. Stability of religiosity
Paired samples t-tests revealed that levels of religiosity did not significantly differ between the prenatal (early pregnancy) and the postpartum period, SE(b) = .04, t = 1.15, p =.25, suggesting that religiosity remains stable across the perinatal period.
3.3. Relationship between cultural orientation and religiosity
Bivariate correlations indicated that levels of religiosity significantly differed according to levels of Mexican and Anglo orientation, (see Table 2). In the prenatal period, endorsing high levels of Mexican orientation was associated with higher levels of religiosity. In contrast, endorsing high levels of Anglo orientation was associated with lower levels of religiosity. This was observed during the prenatal and postpartum periods.
Table 2.
Bivariate correlations between study variables
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| 1. Prenatal Religiosity | - | ||||||||||
| 2. Prenatal Mexican-Orientation | .19** | - | |||||||||
| 3. Prenatal Anglo-Orientation | −.20** | −.13 | - | ||||||||
| 4. Prenatal Acculturative Stress | .08 | .01 | .04 | - | |||||||
| 5. Age | .22** | .20** | −.47** | .02 | - | ||||||
| 6. SES | −.16* | −.27** | .42** | −.05 | −.30** | - | |||||
| 7. Birthplace | −.15* | −.26** | .61** | −.08 | −.48** | .35** | - | ||||
| 8. Anxiety Symptoms (early pregnancy) | −.15* | −.15* | .08 | .25** | −.11 | −.01 | .06 | - | |||
| 9. Anxiety Symptoms (mid- pregnancy) | −.24* | −.16* | .09 | .23** | −.05 | −.03 | .10 | .57** | - | ||
| 10. Anxiety Symptoms (late pregnancy) | −.15* | −.11 | .09 | .19** | −.09 | −.06 | .15* | .53** | .68** | - | |
| 11. Anxiety Symptoms (postpartum) | −.05 | −.12 | .07 | .22** | −.02 | .02 | .08 | .49** | .57** | .55** | - |
indicates significance at p< .05
indicates significance at p< .01
3.4. Relationship between religiosity and anxiety symptoms
Results from the correlations indicate that higher levels of religiosity were associated with fewer anxiety symptoms during all three perinatal timepoints, but not during postpartum (see Table 2). Additionally, results from the hierarchical regressions show that when controlling for acculturation, acculturative stress, and demographics, higher levels of religiosity during early pregnancy (i.e., less than 15 weeks gestation) were associated with lower levels of anxiety symptoms during all three prenatal timepoints, but not during postpartum (see Table 3).
Table 3.
Hierarchical regression models for the prediction of perinatal anxiety symptoms by prenatal religiosity.
| Variable | Early Pregnancy Anxiety Symptoms | Mid-Pregnancy Anxiety Symptoms | Late Pregnancy Anxiety Symptoms | Postpartum Anxiety Symptoms | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ΔR2 | Adj. R 2 | β | SE | p | ΔR2 | Adj. R 2 | β | SE | p | ΔR2 | Adj. R 2 | β | SE | p | ΔR2 | Adj. R 2 | β | SE | p | |
|
| ||||||||||||||||||||
| Block 1 | ||||||||||||||||||||
| Study Variables | ||||||||||||||||||||
| Prenatal Religiosity | .02 | .02 | −.15 | 1.00 | .047 | .04 | .03 | −.19 | .91 | .012 | .03 | .02 | −.16 | .98 | .039 | .00 | .00 | −.04 | .86 | .607 |
| Block 2 | ||||||||||||||||||||
| Study Variables | ||||||||||||||||||||
| Prenatal Religiosity | .11 | .09 | −.16 | .99 | .034 | .09 | .11 | −.20 | .90 | .007 | .05 | .05 | −.17 | .99 | .032 | .06 | .04 | −.05 | .86 | .542 |
| Covariates | ||||||||||||||||||||
| Mexican Orientation | −.12 | 1.53 | .095 | −.13 | 1.38 | .081 | −.06 | 1.53 | .440 | −.12 | 1.33 | .110 | ||||||||
| Anglo Orientation | .04 | .72 | .585 | .03 | .65 | .657 | .06 | .72 | .435 | .02 | .66 | .766 | ||||||||
| Acculturative Stress | .26 | .05 | .001 | .27 | .04 | <.001 | .21 | .05 | .006 | .22 | .04 | .005 | ||||||||
| Block 3 | ||||||||||||||||||||
| Study Variables | ||||||||||||||||||||
| Prenatal Religiosity | .12 | .08 | −.16 | 1.02 | .042 | .02 | .10 | −.22 | .92 | .004 | .04 | .07 | −.20 | 1.01 | .011 | .07 | .02 | −0.59 | .89 | .462 |
| Covariates | ||||||||||||||||||||
| Mexican Orientation | −.14 | 1.62 | .076 | −.15 | 1.46 | .047 | −.06 | 1.60 | .413 | −.13 | 1.41 | .119 | ||||||||
| Anglo Orientation | .05 | .97 | .621 | .07 | .87 | .485 | .01 | .96 | .907 | .03 | .85 | .757 | ||||||||
| Acculturative Stress | .25 | .05 | .001 | .27 | .04 | <.001 | .22 | .05 | .004 | .22 | .04 | .005 | ||||||||
| Age | −.09 | .16 | .310 | .04 | .14 | .660 | .00 | .16 | .977 | .06 | .14 | .508 | ||||||||
| Socioeconomic Status | −.11 | .10 | .210 | −.13 | .09 | .118 | −.16 | .10 | .056 | −.02 | .09 | .853 | ||||||||
| Birthplace | −.01 | 2.47 | .952 | .05 | 2.22 | .603 | .19 | 2.43 | .063 | .04 | 2.15 | .727 | ||||||||
Bold indicates significance at p< .05.
3.5. Religiosity and anxiety symptoms throughout the perinatal period
Multilevel modeling analyses for the unconditional model revealed that 54% of the variance was found between individuals, and 46% of the variance was found within individuals. The linear and quadratic trends for time were significant predictors of anxiety symptoms, but the cubic trend of time was the most parsimonious explanation of this data. Adding a cubic trend for time provided better model fit over the linear, Δχ2(2)= 17.01, p < .001, and quadratic models, Δχ2(1) = 9.31, p < .01, indicating that anxiety symptoms decreased over time in a cubic trend, b = −1.01, t(394) = −3.07, p = .002. Additionally, the main effect of religiosity was significant, b = −1.56, SE(b) = .65, t(197) = −2.39, p = .02, indicating that for every one-point increase in levels of religiosity, there was a 1.56 decrease in anxiety symptoms. Finally, the cubic time x religiosity interaction was significantly associated with anxiety symptoms, b = .07, SE(b) = .03, t(197) = 2.67, p = .01. As shown in Figure 1, women with high religiosity showed a more rapid drop in anxiety across the perinatal period, while those low in religiosity did not show drops in anxiety until postpartum.
Figure 1.
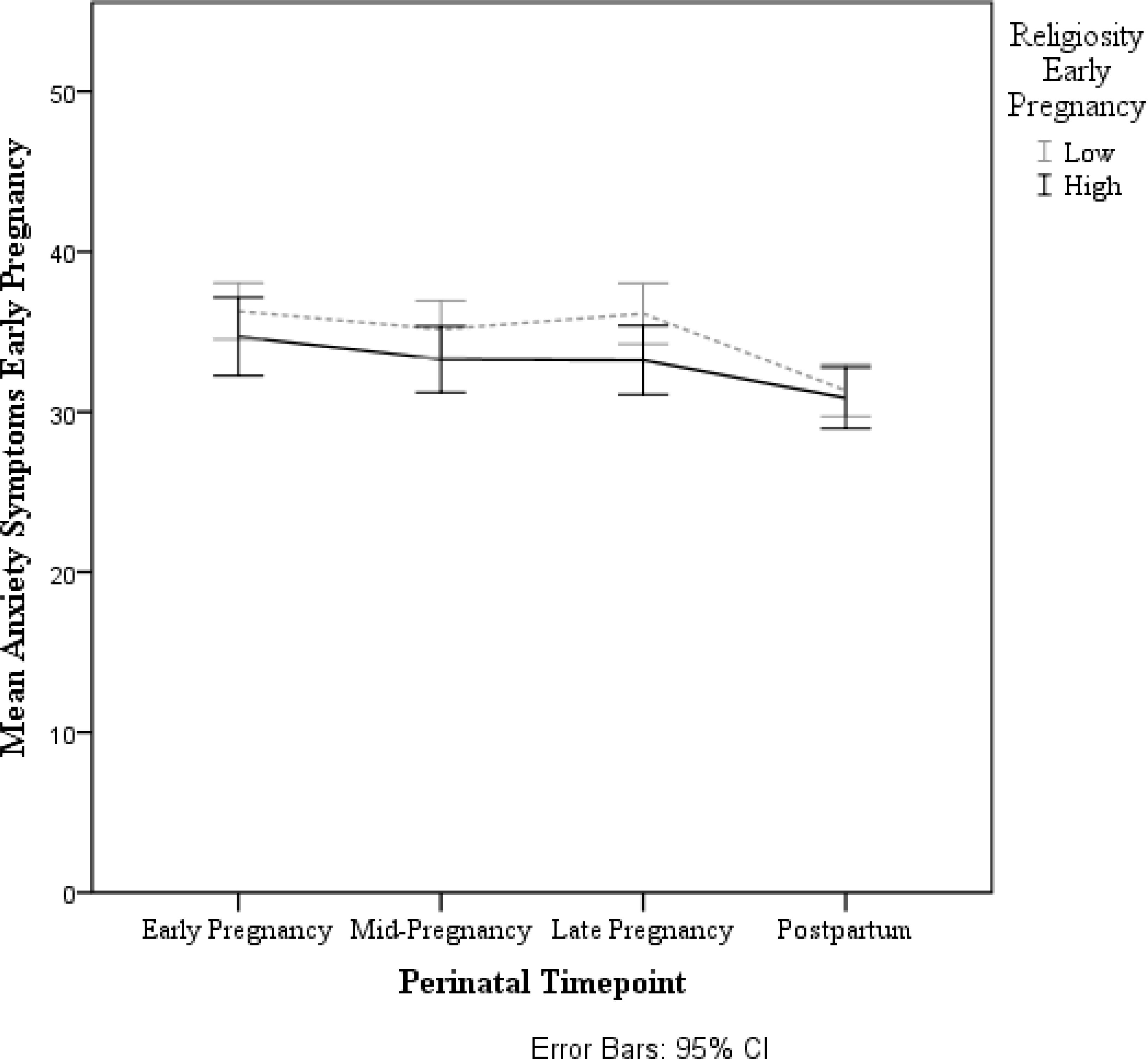
Prenatal religiosity is associated with a lower trajectory of anxiety symptoms across the perinatal period, (b = .068, SE(b) = .0255, t(197) = 2.67, p = .008).
3.6. Religiosity as a protective factor
Moderation analyses revealed that religiosity moderated the relation between acculturative stress and anxiety symptoms when controlling for age, birthplace, and SES. This was seen during early (b = −.12, SE(b) = .06, R2 = .13, R2adjusted = .09, t = −2.06, 95% CI = [−.23, −.00], p = .04), mid- (b = −.19, SE(b) = .05, R2 = .19, R2adjusted = .16, t = −3.99, 95% CI = [−.29, −.09], p < .001), and late pregnancy (b = −.13, SE(b) = .05, R2 = .14, R2adjusted = .10, t = −2.30, 95% CI = [−.23, −.02], p = .02), and postpartum (b = −.12, SE(b) = .05, R2 = .08, R2adjusted = .05, t = −2.43, 95% CI = [−.21, −.02], p = .02), see Figure 2. Conditional effects revealed that for women low in religiosity, acculturative stress was positively associated with anxiety symptoms during early, mid-, and late pregnancy, and postpartum, b = .26, SE(b) = .06, t(197) = 3.98, p < .001, 95% CI [.13, .39]; b = .31, SE(b) = .06, t(197) = 5.53 p < .001, 95% CI [.20, .43]; b = .24, SE(b) = .06, t(197) = 3.81, p < .001, 95% CI [.12, .37]; b = .22, SE(b) = .06, t(197) = 3.82, p < .001, 95% CI [.10, .33]; respectively. This relation was not significant for women who had high religiosity, b = .08, SE(b) = .06, t(197) = 1.22, p = .23, 95% CI [−.05, .20]; b = .01, SE(b) = .06, t(197) = .26, p = .80, 95% CI [−.10, .13]; b = .04, SE(b) = .06, t(197) = .71, p = .48, 95% CI [−.08, .17]; b = .03, SE(b) = .06, t(197) = .54, p = .59, 95% CI [−.08, .14], suggesting that higher levels of religiosity buffer the relationship between acculturative stress and anxiety symptoms during the perinatal period.
Figure 2.
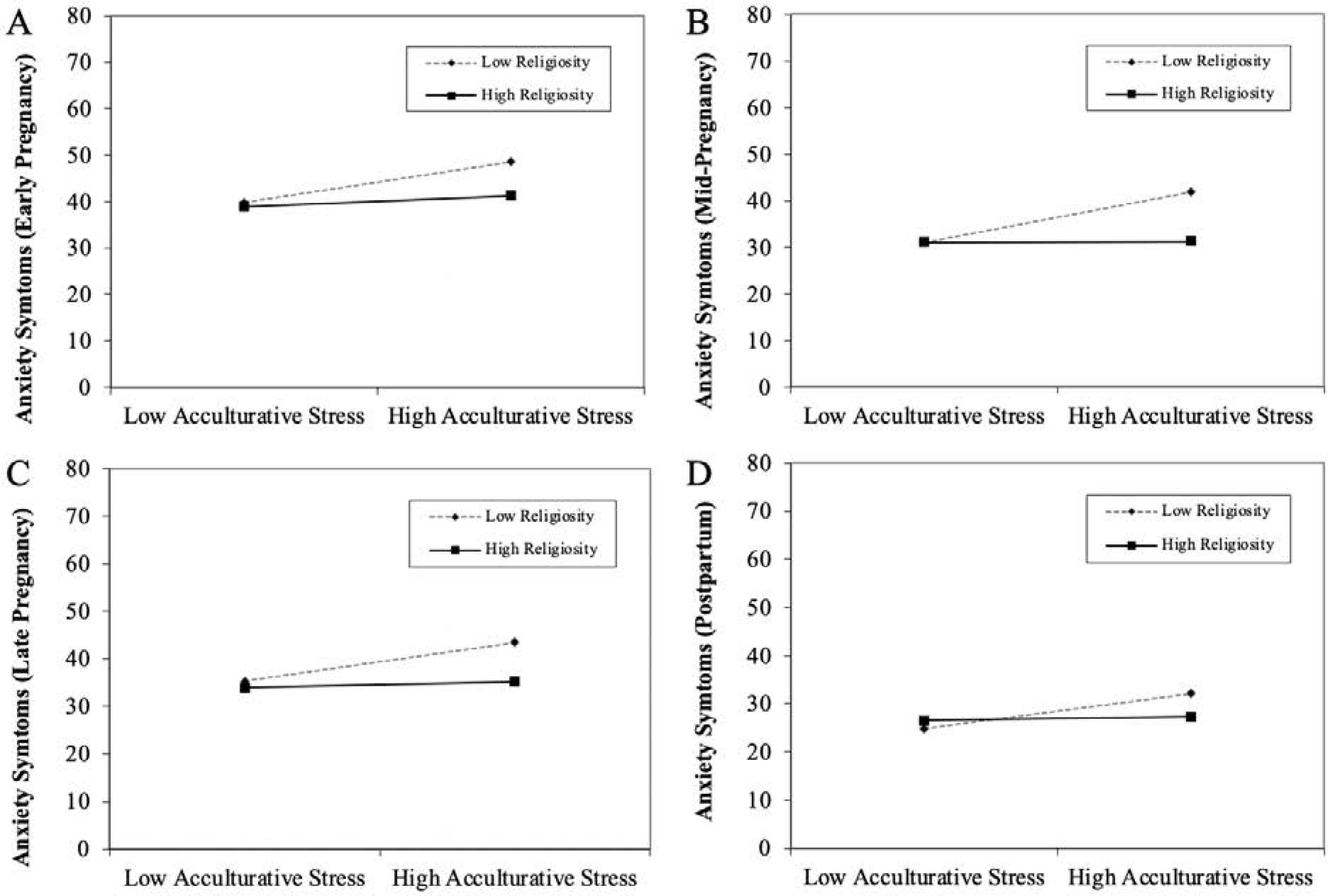
Religiosity buffered the relationship between acculturative stress and prenatal anxiety symptoms during the perinatal period. A, B, C, and D, women high in acculturative stress and high in religiosity experience lower levels of anxiety symptoms compared to women high in acculturative stress and low in religiosity, during early, mid-, and late pregnancy and postpartum (R2 = .125, b = −.115, SE(b) = .0557, p = .0411; R2 = .185, b = −.191, SE(b) = .0487, p < .001; R2 = .136, b = −.125, SE(b) = .0543, p .0225; R2 = .0845, b = −.118, SE(b) = .0483, p = .0160; respectively).
4. Discussion
A recent systematic review on religiosity and perinatal depression highlighted the need to clarify whether religiosity in Latinas was stable over the perinatal period to determine its role as a protective or risk factor for maternal mental health, including the much less studied perinatal anxiety (Lara-Cinisomo, Wood, et al. 2019). The current study addressed and expanded on this work by focusing on the association between religiosity and perinatal anxiety among pregnant women of Mexican descent from early pregnancy to 6 weeks postpartum. Given that maternal anxiety can have negative implications for the woman and her infant (Davis et al. 2004; Robertson et al. 2004) and the growth rate of Mexican-Americans is driven by birth rates and not immigration (Livingston 2019), the identification of culturally-relevant protective factors is needed. Overall religiosity was found to be associated with a more Mexican cultural orientation (less acculturation) and was protective against maternal anxiety, though only consistently during pregnancy. In addition, religiosity buffered the adverse relationship between acculturative stress and maternal anxiety, highlighting the potential protective role of religiosity during the perinatal period.
Religiosity has been suggested as an integral aspect of Mexican culture (Lerman et al. 2018). In the current study, religiosity differed by cultural orientation, with women who ascribe to a higher level of Mexican orientation reporting higher levels of religiosity than those with higher levels of Anglo orientation. Others have shown that undocumented immigrants and less acculturated Latinos are more likely to rely on religious coping compared to documented immigrants and more acculturated Latinos (Mausbach, Coon, Cardenas, & Thompson 2003; Sanchez, Dillon, Ruffin, & De La Rosa 2012). Religiosity also seems to be a stable concept as it did not vary from early pregnancy to early postpartum. Thus, this work replicates the importance of religiosity amongst Mexican pregnant women.
Religiosity was also associated with anxiety symptoms across the perinatal period, similar to that previously seen with perinatal depressive symptoms (Lara-Cinisomo, Fujimoto, et al. 2019). The rate at which trajectories of anxiety symptoms declined depended on the level of religiosity. There was a greater drop in anxiety for women with high adherence to religiosity across the perinatal period. However, regression analyses showed that religiosity had the greatest impact on anxiety during pregnancy rather than the postpartum period. To our knowledge, this is the first study to demonstrate that levels of religiosity have a temporal effect on anxiety symptoms. These findings have important implications because they suggest that higher levels of religiosity may provide women with coping strategies or resources that can aid in improving their mental health. Indeed, in general, others have found that higher levels of religiosity are associated with lower levels of anxiety symptoms (Ismail & Desmukh 2012; Mann et al. 2008) and better coping (Krägeloh, Chai, Shepherd, & Billington 2012). The findings also suggest that women with lower levels of religiosity are most vulnerable during the prenatal period. Given the negative effects prenatal anxiety can have on birth outcomes and maternal wellbeing (Davis et al. 2004; Leis et al. 2014; O’Connor et al. 2003; Tomfohr-Madsen et al. 2019), it is important to identify women who may benefit from additional interventions that include factors associated with religiosity.
Still, while results revealed that while religiosity buffered the effects of acculturative stress on anxiety symptoms throughout the entire perinatal period, religiosity itself only predicted anxiety symptoms during pregnancy. This could be because pregnancy is a vulnerable point in the perinatal period and is filled with many unknowns, such as uncertainty surrounding the labor and birth experience and feeling a lack of control over these events (Borrelli, Walsh, & Spiby 2018). Additionally, for women of Mexican descent, the postpartum period may be a time in which traditional expectations of motherhood culture are fulfilled (Callister & Birkhead 2002) and Mexican Orientation, and thus adherence to traditional culture values, increases in the postpartum period relative to pregnancy (Sanchez, Erika, Urbina, & D’Anna-Hernandez 2020). Mexican women report more social and intergenerational support in the postpartum period as well as familism that may contribute to less worries, stress and anxiety (Campos et al. 2008; Negron, Martin, Almog, Balbierz, & Howell 2013). For example, worries about the baby have been shown to decrease as social resources increase (Campos et al. 2008). Thus, it is possible that the support from religion is not as salient during the postpartum period relative to pregnancy for more pregnancy-related anxiety symptoms.
Few studies have addressed the potential moderating role of cultural protective factors, such as religiosity, against sociocultural stressors on maternal mental health. Previous studies have demonstrated the deleterious effects of acculturative stress on the mental health of Latinas, including Mexican-American mothers (D’Anna-Hernandez et al. 2015; Revollo, Qureshi, Collazos, Valero, & Casas 2011; Sanchez et al. 2020). Others have also shown that higher levels of acculturative stress are associated with increased anxiety symptoms during the prenatal period (Preciado & D’Anna-Hernandez 2017). This study extends these findings by performing moderations that showed that religiosity can protect women from the negative effects of acculturative stress on anxiety as early as 15 weeks of pregnancy and as late as 6 weeks postpartum. Other work has shown that religiosity and religious coping can buffer the adverse effects of acculturative stress on mental health disorders (Sanchez, Dillon, Concha, & De La Rosa 2015) while struggling with faith is a risk factor (Da Silva, Dillon, Rose Verdejo, Sanchez, & De La Rosa 2017). Though not measured in the current study, religiosity has also been associated with increased resources, social capital and social support in immigrant populations (Steffen & Merrill 2011; Stevens 2004), all which may assist and create community for new mothers. Thus, factors associated with religiosity may be protective against maternal anxiety to promote maternal/child health in the perinatal period.
Mental health professionals, providers, and other medical staff must remain secular and religiously neutral. To respect religious beliefs and practices, when mapping social support resources, if women report religion to be a source of support practitioners and researchers should keep in mind the benefits associated with religiosity, particularly among those experiencing high levels of acculturative stress. Supporting positive religious coping that matches evidence-based healthy coping behaviors similar to those used in clinical interventions may help alleviate anxiety symptoms and enable women to use the resources at their disposal. Indeed, a recent study showed that religious coping, such as reframing, can be protective (Dolcos, Hohl, Hu, & Dolcos). The findings from the current study also have important implications for future research. Religiosity is complex and can include different dimensions such as spirituality, religious practice/engagement, and religious affiliation. Future work should build on the current findings by taking into account the different dimensions of religiosity to better understand the complex role of religiosity on perinatal anxiety and extend the coping literature.
While the study provides new findings regarding the effect of religiosity on anxiety symptoms over the perinatal period in a sample of women of Mexican descent, several limitations should be noted. First, we did not assess whether religion was used as a coping strategy. Therefore, future studies should gather longitudinal data on religious coping as an approach for coping with psychological distress during the perinatal period. Additionally, we did not assess specific religious affiliation (e.g., Catholicism). Because some religions may be perceived to be more supportive of women’s mental health than others (Edgell, Tranby, & Mather 2013), future studies should gather data on religious affiliation and perceptions of emotional support. Second, the study was limited to women of Mexican descent. It is possible that other immigrant groups may exhibit different patterns of religiosity and anxiety symptoms. Therefore, future studies should include a more diverse sample of prenatal and postpartum women. Finally, the nature of this study was correlational, and thus no causal connections can be made. However, the study did yield meaningful findings regarding the complex role religiosity has on anxiety in perinatal women of Mexican descent.
5. Conclusion
This novel study examined the temporal and moderating effects of religiosity on anxiety symptoms in a sample of perinatal women of Mexican descent. Results indicate that religiosity while it is stable over time, also has a temporal effect on anxiety symptoms. The findings also revealed that the degree of religiosity influenced the extent to which anxiety symptoms improved over time. Furthermore, the results indicated that higher levels of religiosity were most beneficial on the negative effects of acculturative stress on anxiety symptoms. These findings have clinical and research implications. Women who endorse religiosity may benefit from supported religious coping. Researchers should assess the extent to which religious affiliation and perceived benefits reduce anxiety during the perinatal periods, particularly during pregnancy.
References
- Alhasanat D, & Giurgescu C (2017). Acculturation and postpartum depressive symptoms among Hispanic women in the United States: systematic review. MCN: The American Journal of Maternal/Child Nursing, 42(1), 21–28. [DOI] [PubMed] [Google Scholar]
- Arch JJ (2013). Pregnancy-specific anxiety: which women are highest and what are the alcohol-related risks? Comprehensive Psychiatry, 54(3), 217–228. [DOI] [PubMed] [Google Scholar]
- Ban L, Gibson JE, West J, Fiaschi L, Oates MR, & Tata LJ (2012). Impact of socioeconomic deprivation on maternal perinatal mental illnesses presenting to UK general practice. British Journal of General Practice, 62(603), e671–e678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkel C, Knight GP, Zeiders KH, Tein J-Y, Roosa MW, Gonzales NA, & Saenz D (2010). Discrimination and adjustment for Mexican American adolescents: A prospective examination of the benefits of culturally related values. Journal of Research on Adolescence, 20(4), 893–915. doi: 10.1111/j.1532-7795.2010.00668.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein R (2007, 2007/09/06/). Minority Population Tops 100 Million, from http://www.census.gov/Press-Release/www/releases/archives/population/010048.html
- Berry J (2006). Acculturative Stress. In Wong P & Wong L (Eds.), Handbook of Multicultural Perspectives on Stress and Coping (pp. 287–298). Langley, British Columbia: Trinity Western University. [Google Scholar]
- Bonelli RM, & Koenig HG (2013). Mental disorders, religion and spirituality 1990 to 2010: a systematic evidence-based review. Journal of religion and health, 52(2), 657–673. [DOI] [PubMed] [Google Scholar]
- Borrelli SE, Walsh D, & Spiby H (2018). First-time mothers’ expectations of the unknown territory of childbirth: uncertainties, coping strategies and ‘going with the flow’. Midwifery, 63, 39–45. [DOI] [PubMed] [Google Scholar]
- Callister LC, & Birkhead A (2002). Acculturation and perinatal outcomes in Mexican immigrant childbearing women: An integrative review. Journal of Perinatal and Neonatal Nursing, 16(3), 22–38. [DOI] [PubMed] [Google Scholar]
- Calzada EJ, & Sales A (2019). Depression among Mexican-origin mothers: Exploring the immigrant paradox. Cultural Diversity and Ethnic Minority Psychology, 25(2), 288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campos B, Schetter CD, Abdou CM, Hobel CJ, Glynn LM, & Sandman CA (2008). Familialism, social support, and stress: Positive implications for pregnant Latinas. Cultural diversity & ethnic minority psychology, 14(2), 155–162. doi: 10.1037/1099-9809.14.2.155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuellar I, Arnold B, & Maldonado R (1995). Acculturation rating scale for Mexican-Americans II: A revision of the original ARSMA scale. Hispanic Journal of Behavioral Sciences, 17(3), 275–304. doi: 10.1177/07399863950173001 [DOI] [Google Scholar]
- D’Anna-Hernandez KL, Aleman B, & Flores AM (2015). Acculturative stress negatively impacts maternal depressive symptoms in Mexican-American women during pregnancy. Journal of Affective Disorders, 176, 35–42. doi: 10.1016/j.jad.2015.01.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Da Silva N, Dillon FR, Rose Verdejo T, Sanchez M, & De La Rosa M (2017). Acculturative Stress, Psychological Distress, and Religious Coping Among Latina Young Adult Immigrants. The Counseling Psychologist, 45(2), 213–236. doi: 10.1177/0011000017692111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis EP, Snidman N, Wadhwa PD, Glynn LM, Schetter CD, & Sandman CA (2004). Prenatal maternal anxiety and depression predict negative behavioral reactivity in infancy. Infancy, 6(3), 319–331. [Google Scholar]
- Dolcos F, Hohl K, Hu Y, & Dolcos S Religiosity and Resilience: Cognitive Reappraisal and Coping Self-Efficacy Mediate the Link between Religious Coping and Well-Being. Journal of religion and health, 1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edgell P, Tranby EP, & Mather DM (2013). Profiles of anticipated support: Religion’s place in the composition of Americans’ emotional support networks. Journal for the scientific study of religion, 52(2), 293–308. [Google Scholar]
- Ellison CG, Finch BK, Ryan DN, & Salinas JJ (2009). Religious involvement and depressive symptoms among Mexican-origin adults in California. Journal of Community Psychology, 37(2), 171–193. [Google Scholar]
- Emmanuel EN, & Sun J (2014). Health related quality of life across the perinatal period among Australian women. Journal of clinical nursing, 23(11–12), 1611–1619. [DOI] [PubMed] [Google Scholar]
- Fairbrother N, Janssen P, Antony MM, Tucker E, & Young AH (2016). Perinatal anxiety disorder prevalence and incidence. Journal of Affective Disorders, 200, 148–155. [DOI] [PubMed] [Google Scholar]
- Finch BK, & Vega WA (2003). Acculturation stress, social support, and self-rated health among Latinos in California. Journal of Immigrant Health, 5(3), 109–117. doi: 10.1023/a:1023987717921 [DOI] [PubMed] [Google Scholar]
- Hayes A (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Retrieved from http://www.guilford.com/p/hayes3
- Hill PC, & Pargament KI (2003). Advances in the conceptualization and measurement of religion and spirituality: Implications for physical and mental health research. American psychologist, 58(1), 64. [DOI] [PubMed] [Google Scholar]
- Hovey JD (2000). Acculturative stress, depression, and suicidal ideation in Mexican immigrants. Cultural Diversity and Ethnic Minority Psychology, 6(2), 134–151. doi: 10.1037/1099-9809.6.2.134 [DOI] [PubMed] [Google Scholar]
- Ismail Z, & Desmukh S (2012). Religiosity and psychological well-being. International Journal of Business and Social Science, 3(11). [Google Scholar]
- Khalaf DR, Hebborn LF, Dal SJ, & Naja WJ (2015). A critical comprehensive review of religiosity and anxiety disorders in adults. Journal of religion and health, 54(4), 1438–1450. [DOI] [PubMed] [Google Scholar]
- Knight G, Gonzales N, Saenz D, German M, Deardoff J, Roosav M, & Updegraff K (2010). The Mexican American Cultural Values Scale for adolescents and adults. Journal of Early Adolescence, 30(3), 444–481. doi: 10.1177/0272431609338178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krägeloh CU, Chai PPM, Shepherd D, & Billington R (2012). How religious coping is used relative to other coping strategies depends on the individual’s level of religiosity and spirituality. Journal of religion and health, 51(4), 1137–1151. [DOI] [PubMed] [Google Scholar]
- Lara-Cinisomo S, Fujimoto EM, Oksas C, Jian Y, & Gharheeb A (2019). Pilot Study Exploring Migration Experiences and Perinatal Depressive and Anxiety Symptoms in Immigrant Latinas. Maternal and Child Health Journal, 23(12), 1627–1647. [DOI] [PubMed] [Google Scholar]
- Lara-Cinisomo S, Wood J, & Fujimoto E (2019). A systematic review of cultural orientation and perinatal depression in Latina women: are acculturation, Marianismo, and religiosity risks or protective factors? Archives of Women’s Mental Health, 22(5), 557–567. [DOI] [PubMed] [Google Scholar]
- Lee AM, Lam SK, Lau SMSM, Chong CSY, Chui HW, & Fong DYT (2007). Prevalence, course, and risk factors for antenatal anxiety and depression. Obstetrics and Gynecology, 110(5), 1102–1112. doi: 10.1097/01.AOG.0000287065.59491.70 [DOI] [PubMed] [Google Scholar]
- Leis JA, Heron J, Stuart EA, & Mendelson T (2014). Associations between maternal mental health and child emotional and behavioral problems: does prenatal mental health matter? Journal of Abnormal Child Psychology, 42(1), 161–171. [DOI] [PubMed] [Google Scholar]
- Lerman S, Jung M, Arredondo EM, Barnhart JM, Cai J, Castañeda SF, … Molina KM (2018). Religiosity prevalence and its association with depression and anxiety symptoms among Hispanic/Latino adults. PLoS ONE, 13(2), e0185661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Livingston G (2019). Hispanic women no longer account for the majority of immigrant births in the U.S. Washington, DC: Pew Research Center. [Google Scholar]
- Lobel M, & Ibrahim M, S. (2018). Emotions and mental health during pregnancy and postpartum. Women’s Reproductive Health, 5(1), 13–19. [Google Scholar]
- Mann J, McKeown R, Bacon J, Vesselinov R, & Bush F (2008). Religiosity, spirituality and antenatal anxiety in Southern US women. Archives of Women’s Mental Health, 11(1), 19–26. [DOI] [PubMed] [Google Scholar]
- Mann JR, Mannan J, Quiñones LA, Palmer AA, & Torres M (2010). Religion, spirituality, social support, and perceived stress in pregnant and postpartum Hispanic women. Journal of Obstetric, Gynecologic & Neonatal Nursing, 39(6), 645–657. [DOI] [PubMed] [Google Scholar]
- Mann JR, McKeown RE, Bacon J, Vesselinov R, & Bush F (2007). Religiosity, spirituality, and depressive symptoms in pregnant women. The International Journal of Psychiatry in Medicine, 37(3), 301–313. [DOI] [PubMed] [Google Scholar]
- Mausbach BT, Coon DW, Cardenas V, & Thompson LW (2003). Religious coping among Caucasian and Latina dementia caregivers. Journal of Mental Health and Aging. [Google Scholar]
- Meades R, & Ayers S (2011). Anxiety measures validated in perinatal populations: a systematic review. Journal of Affective Disorders, 133(1–2), 1–15. [DOI] [PubMed] [Google Scholar]
- Misri S, Abizadeh J, Sanders S, & Swift E (2015). Perinatal generalized anxiety disorder: assessment and treatment. Journal of Women’s Health, 24(9), 762–770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Motel S, & Patten E (2012). Characteristics of the 60 largest metropolitan areas by Hispanic population. Washington, DC: Pew Hispanic Center. [Google Scholar]
- Muraca GM, & Joseph K (2014). The association between maternal age and depression. Journal of Obstetrics and Gynaecology Canada, 36(9), 803–810. [DOI] [PubMed] [Google Scholar]
- Negron R, Martin A, Almog M, Balbierz A, & Howell EA (2013). Social support during the postpartum period: mothers’ views on needs, expectations, and mobilization of support. Maternal and Child Health Journal, 1–8. doi: 10.1007/s10995-012-1037-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor TG, Heron J, Golding J, Glover V, & the ALSST (2003). Maternal antenatal anxiety and behavioural/emotional problems in children: a test of a programming hypothesis. Journal of Child Psychology and Psychiatry, 44(7), 1025–1036. doi: 10.1111/1469-7610.00187 [DOI] [PubMed] [Google Scholar]
- Osterman MJ, & Martin JA (2011). Epidural and spinal anesthesia use during labor: 27-state reporting area, 2008. [PubMed] [Google Scholar]
- Preciado A, & D’Anna-Hernandez K (2017). Acculturative stress is associated with trajectory of anxiety symptoms during pregnancy in Mexican-American women. Journal of Anxiety Disorders, 48, 28–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Revollo H-W, Qureshi A, Collazos F, Valero S, & Casas M (2011). Acculturative stress as a risk factor of depression and anxiety in the Latin American immigrant population. International Review of Psychiatry, 23(1), 84–92. [DOI] [PubMed] [Google Scholar]
- Robertson E, Grace S, Wallington T, & Stewart DE (2004). Antenatal risk factors for postpartum depression: a synthesis of recent literature. General Hospital Psychiatry, 26(4), 289–295. [DOI] [PubMed] [Google Scholar]
- Rutledge MS, & McLaughlin CG (2008). Hispanics and health insurance coverage: the rising disparity. Medical Care, 1086–1092. [DOI] [PubMed] [Google Scholar]
- Sanchez L, Erika B, Urbina E, & D’Anna-Hernandez KL (2020). Sociocultural stressors across the perinatal period and risk for postpartum depressive symptoms in women of Mexican descent. Cultural Diversity and Ethnic Minority Psychology, 26(1), 124. [DOI] [PubMed] [Google Scholar]
- Sanchez M, Dillon F, Ruffin B, & De La Rosa M (2012). The influence of religious coping on the acculturative stress of recent Latino immigrants. Journal of ethnic & cultural diversity in social work, 21(3), 10.1080/15313204.15312012.15700443. doi: 10.1080/15313204.2012.700443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanchez M, Dillon FR, Concha M, & De La Rosa M (2015). The impact of religious coping on the acculturative stress and alcohol use of recent Latino immigrants. Journal of religion and health, 54(6), 1986–2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Speilberger C (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press. [Google Scholar]
- Steffen P, & Merrill R (2011). The association between religion and acculturation in Utah Mexican immigrants. Mental Health, Religion & Culture, 14(6), 561–573. [Google Scholar]
- Stepler R, & Brown A (2016). Statistical Portrait of Hispanics in the United States. Washington, D.C.: Pew Research Center. [Google Scholar]
- Stevens WD (2004). Spreading the word: Religious beliefs and the evolution of immigrant congregations. Sociology of Religion, 65(2), 121–138. [Google Scholar]
- Tomfohr-Madsen L, Cameron EE, Dunkel Schetter C, Campbell T, O’Beirne M, Letourneau N, & Giesbrecht GF (2019). Pregnancy anxiety and preterm birth: The moderating role of sleep. Health Psychology, 38(11), 1025. [DOI] [PubMed] [Google Scholar]
- Williams DR, Mohammed SA, Leavell J, & Collins C (2010). Race, socioeconomic status and health: Complexities, ongoing challenges and research opportunities. Annals of the New York Academy of Sciences, 1186, 69–101. doi: 10.1111/j.1749-6632.2009.05339.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong YJ, Rew L, & Slaikeu KD (2006). A systematic review of recent research on adolescent religiosity/spirituality and mental health. Issues in Mental Health Nursing, 27(2), 161–183. [DOI] [PubMed] [Google Scholar]
- Zeiders KH, Hoyt LT, & Adam EK (2014). Associations between self-reported discrimination and diurnal cortisol rhythms among young adults: The moderating role of racial–ethnic minority status. Psychoneuroendocrinology, 50, 280–288. [DOI] [PMC free article] [PubMed] [Google Scholar]