

Abstract
Objective:
To evaluate the association between vertical facial morphology and overjet in untreated Class II subjects.
Materials and Methods:
The lateral cephalograms of 140 untreated Class II subjects (68 males and 72 females) between 8 and 11 years of age were divided into three groups based on their overjet value as measured on study casts: Group I normal overjet (less than 3 mm), Group II increased overjet (more than 3 mm but less than or equal to 6 mm), and Group III extreme overjet (more than 6 mm). Mean values and standard deviations of 28 variables measured on lateral cephalograms were calculated. Differences between the three groups were tested using one-way analysis of variance (ANOVA), followed by Bonferroni tests. Additionally, cephalometric differences between groups and available normal values for the Syrian population were evaluated using an independent t-test.
Results:
Subjects with normal overjet showed a horizontal facial pattern and posterior inclination of the maxilla, whereas increased overjet subjects exhibited a neutral facial pattern. In contrast, subjects with extreme overjet had a vertical facial pattern and anterior inclination of the maxilla. The mandible was retrognathic and the maxilla was normally positioned in the three groups.
Conclusions:
A positive association was found between the overjet and the tendency toward a hyperdivergent pattern.
Keywords: Class II malocclusion, Overjet, Craniofacial morphology
INTRODUCTION
An understanding of the relationship between skeletal and dental components that contribute to malocclusion is important in orthodontic treatment planning. Class II malocclusions have been described as the most frequent treatment problem in practice and one of the more difficult orthodontic problems to treat. Epidemiologic studies have shown that 20% to 30% of children have Class II malocclusions.1,2
Numerous studies have been conducted to determine the anteroposterior and vertical components of patients with Class II malocclusion.3–5 Although some studies have found that the Class II skeletal pattern is due to both maxillary protrusion and mandibular retrusion,4,6 others have found that the maxilla was in the normal position while the mandible was retrusive.5,7 Some studies have shown that the facial pattern tended to be a hyperdivergent pattern in Class II/1 and a hypodivergent pattern in Class II/2.4 Few studies have revealed no difference in vertical facial morphology between Class II/1 and Class II/2 except for the position of the maxillary incisors.6
Although the craniofacial morphology of Class II malocclusion has been analyzed in several investigations, the value of some of these investigations is limited for the following reasons: First, a clear definition of Class II malocclusion was lacking. Most investigations selected patients on the basis of Angle's classification,8 which failed to distinguish between skeletal malocclusion and anteroposterior dental relationships, and could lead to the possibility of one Class overlapping into the other.9 Second, most investigations selected dental Class II patients who may have a Class I or a Class II skeletal pattern.3,4 Few studies evaluated patients with both skeletal and dental Class II malocclusion.10,11 Third, some studies included male and female subjects in the study sample despite the fact that males and females may show a considerable degree of discrepancy in craniofacial dimensions.6 Finally, the relationship between overjet and craniofacial morphology appears to have been neglected.
Overjet is one of the parameters used to assess the sagittal relationship of the upper and lower dental arch and is considered as a good predictor of the sagittal relationship in subjects with a Class II division 1 malocclusion.12 Therefore, a better understanding of the differences in craniofacial morphology associated with different overjet magnitude may be useful in the treatment planning of Class II cases.
The aims of this study were to evaluate the association between facial morphology and overjet in untreated preadolescent Class II patients, and to identify the craniofacial characteristics of Class II patients with normal, increased, and extreme overjet in a sample of the Syrian population.
MATERIALS AND METHODS
Ethical Approval and Consent
This study was approved by the Council of the Faculty of Dentistry at Damascus University and the Scientific Research Committee of Damascus University, which provided funding for the study. Consent was obtained by asking parents to sign a form that explained the nature and purpose of the radiographic examination.
Sample Selection
The sample was derived from a larger representative sample of 1820 preadolescents attending elementary schools in the capital of Syria, Damascus. Subjects were selected according to the following primary inclusion criteria:
Dental Class II malocclusion (bilateral distal molar relationships of more than one-half cusp width)
Age range of 8 to 11 years
No missing permanent teeth
Healthy with no syndromes or history of orthodontic treatment
Examinations were carried out on the school premises under natural lighting. Of the total sample examined, 156 subjects who fulfilled the primary criteria were selected. Examinations were carried out again and lateral cephalograms were taken for selected subjects at the Department of Orthodontics, Damascus University. Of the total sample selected, 16 subjects (10.25%) were excluded because they did not have skeletal Class II (ANB angle less than 4.5 degrees). Alginate impressions were taken for 140 subjects (68 males and 72 females with a mean age of 9.9 ± 1.1 years) who met the second criteria. Impressions were poured on the same day with hard dental stone, using standard procedures for mixing and storage of impressions until they were poured. The sample was then divided into three groups on the basis of overjet values (Table 1):
Table 1.
Age and Gender Distribution of the Sample

Group I: 46 patients (22 males and 24 females) with normal overjet (less than or equal to 3 mm)
Group II: 46 patients (22 males and 24 females) with increased overjet (more than 3 mm but less than or equal to 6 mm)
Group III: 48 patients (24 males and 24 females) with extreme overjet (more than 6 mm)
Angular and linear cephalometric parameters of 50 normal controls (26 males and 24 females) aged 8 to 11 years (9.44 ± 0.81) were obtained from a previous study conducted by one of the authors at the Department of Orthodontics, Damascus University, to investigate Syrian norms. Controls were healthy Syrian children with neutral occlusion, normal overbite and overjet, no interdental spacing or crowding, and a balanced facial profile who had not received previous orthodontic treatment.13
Methods
Overjet was measured on study casts taken from each subject as the distance from the labial surface of the mandibular central incisor to the labial surface of the most prominent maxillary incisor, with a digital caliper accurate to 0.01 held parallel to the occlusal plane.
Lateral cephalograms of subjects with Class II malocclusion were taken on the same x-ray unit at the Faculty of Dentistry, Damascus University (Arcodent, Fiad, Italy), at a film focus distance of 1.50 m (a cathode voltage of 75 to 80 kV was used depending on the age of the patient). Lateral cephalograms of subjects with normal occlusion were taken on the same x-ray unit using the same conditions previously mentioned.13
All radiographs were traced and measured manually by the same investigator (HS) under standardized conditions. Radiographs were traced randomly in a darkened room with a 0.3 mm diameter lead pencil (Figures 1 and 2). Overall, cephalometric analysis in the present study covered 19 reference angles, 7 reference lines, the facial height ratio according to Jarabak, and the sum of the sella, articular, and gonial angles according to Björk (Table 2).
Figure 1.
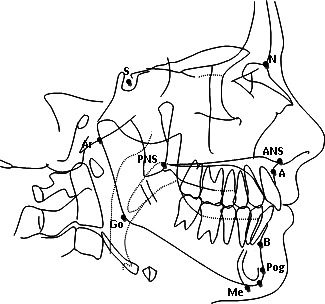
Reference points used in the study: N: nasion, S: sella, Ar: articulare, Go: gonion, Me: menton, Gn: gnathion, PNS: the intersection of posterior facial height (S-Go) and maxillary plane (Spp), A: subspinale, B: supramentale, Pog: pogonion, Ao: the point of contact of a perpendicular line drawn from point A to the bisected occlusal plane, Bo: the point of contact of a perpendicular line drawn from point B to the bisected occlusal plane, U1: upper incisor tip, and L1: lower incisor tip.
Figure 2.
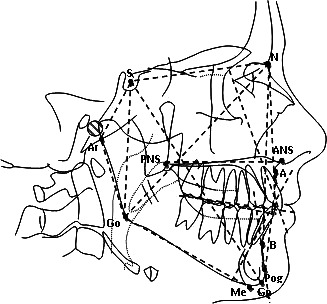
Reference lines and angles used in the present study.
Table 2.
Cephalometric Measurements Used in the Study

Statistical Analysis
An estimate of the power of the study was performed on the basis of the effect size of a relevant variable (ANB) at α = .05, with a sample size of 22 subjects in each group.14 The power of the study in each subgroup (males and females) exceeded 0.90. The Kolmogorov-Smirnov test showed that all variables were normally distributed within each group. Therefore, parametric statistics was used. The mean and standard deviation for each variable were calculated using the Statistical Package for the Social Sciences (SPSS), version 15.0 for Windows (SPSS Inc, Chicago, Ill). Differences between overjet groups were tested using one-way analysis of variance (ANOVA), followed by Bonferroni's multiple comparison post hoc tests. Differences between each malocclusion group and the normal control group were evaluated using an independent t-test. Within each group, the effect of gender was evaluated using an independent t-test. The significance level was set at P < .05.
Method Error
To determine the method error, 25 radiographs were retraced by the same examiner after 3 to 4 weeks. The method error was calculated using Dahlberg's formula: Error of method = √Σd2 /2n, where d is the difference between two measurements and n is the number of double determinations.15 The error of the method varied between 0.15 and 0.47 degrees for angular measurements and between 0.12 and 0.38 mm for linear measurements.
RESULTS
Differences Between Male and Female Subjects
Table 3 shows descriptive and comparative statistics according to gender for the three groups. No statistically significant differences were found between male and female subjects except for S-N, N-Me, SPP∶GoMe, U1-SN, and U1-Spp in Group 1, and S-Ar, S-Go, and N-Me in Group 2.
Table 3.
Comparison of Male and Female Craniofacial Morphology in Each Group

Differences Between Overjet Groups
The mean and standard deviation of each measurement for the three groups and statistical differences between groups for males, females, and total population are shown in Tables 4 to 6. Significant differences were found in skeletal and dentoalveolar measurements between the three groups.
Table 4.
Comparisons of Mean Values in Males Between the Three Groups, and Between Each Overjet Group and the Normal Occlusion Group

Table 5.
Comparisons of Mean Values in Females Between the Three Groups, and Between Each Overjet Group and the Normal Occlusion Group

Table 6.
Comparisons of Mean Values in Total Between the Three Groups, and Between Each Overjet Group and the Normal Occlusion Group

Differences Between Overjet Groups and Normal Occlusion Group
The mean and standard deviation for cephalometric variables of the normal occlusion group, as reported by Al-Salti,13 as well as statistical differences between each overjet group and the normal occlusion group for males, females, and total, are shown in Tables 4 to 6. Significant differences were found in skeletal and dentoalveolar measurements between each overjet group and the normal occlusion group.
DISCUSSION
The craniofacial morphology of Class II malocclusion has been analyzed in several cephalometric investigations,3–5 which have reported conflicting results about the characteristics of Class II malocclusion. However, no comparative data are available for Class II subjects with normal, increased, and extreme overjet. The aim of this investigation was to evaluate the association between craniofacial morphology and overjet in preadolescent Class II subjects in a sample of the Syrian population.
Skeletal Parameters
Findings of this study revealed normal anterior cranial base length (S-N), enlarged posterior cranial base length (S-Ar), and normal posterior facial height (S-Go) in all groups, except Group 1 females who had an enlarged (S-N) and (S-Go). In addition, no significant difference was found between Class II groups in (S-N, S-Ar, and S-Go), indicating the absence of a strong relationship between overjet and these measurements. In other studies, a relatively normal anterior cranial base length and decreased posterior facial height were found in Class II/1.10 On the other hand, a few previous studies reported an enlarged anterior cranial base and a decrease in posterior cranial base length in Class II/1.7,11 The divergence in findings may be attributed to ethnic differences.
The mean length of the mandibular ramus (Ar-Go) and the mandibular body (Go-Me) was significantly shorter in the extreme overjet group. Several previous studies reported a short length of the mandibular ramus and the mandibular body in Class II/1 malocclusion.7,10
Although the mean sella angle (N S Ar) tended to be increased in all groups, this was significantly different only in Group 2. However, no significant difference was noted between the three groups, indicating no relationship between the sella angle (N S Ar) and overjet. In other studies, a relatively increased sella angle was found in Class II malocclusion.7,10
The mean (S-N∶Go-Me) and (SPP∶Go-Me) angles were significantly decreased in the normal overjet group, indicating a hypodivergent pattern in this group. In contrast, the extreme overjet group showed increased (S-N∶Go-Me) and (SPP∶Go-Me) angles compared with the norms and with Groups 1 and 2, demonstrating a hyperdivergent pattern. A review of the literature reveals an increase in the (S-N∶Go-Me) angle and the (SPP∶Go-Me) angle4 in Class II/1 malocclusion, indicating a hyperdivergent pattern. In Class II/2 malocclusion patients, studies revealed a decrease in the (S-N∶Go-Me) angle6 and the (SPP∶Go-Me) angle,4,16 demonstrating a hypodivergent pattern.
Furthermore, the mean facial height ratio (S-Go/N-Me) was significantly increased in the normal overjet group, indicating a hypodivergent pattern in this group. In contrast, the extreme overjet group showed a decrease in (S-Go/N-Me), indicating a hyperdivergent pattern in this group. No significant difference was found for males, probably because of the tendency of the male pattern toward neutral in all groups, while the female pattern tends toward hypodivergent in Group 1 and hyperdivergent in Group 3. Previous studies reported a hyperdivergent pattern in patients with Class II/1.7 Siriwat and Jarabak17 found that a neutral growth pattern was dominant in Class II division I malocclusion and a hypodivergent pattern was dominant in Class II division 2.
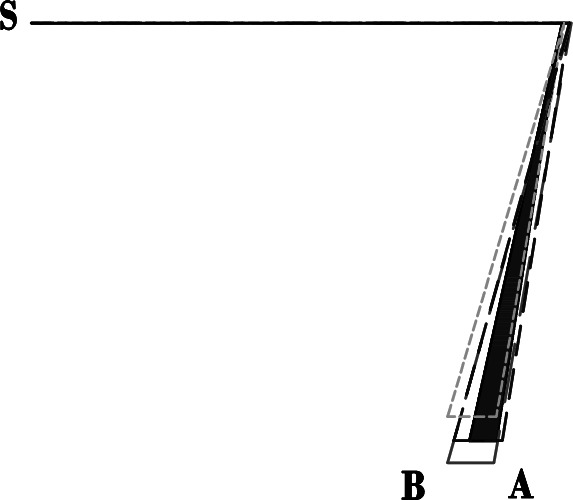
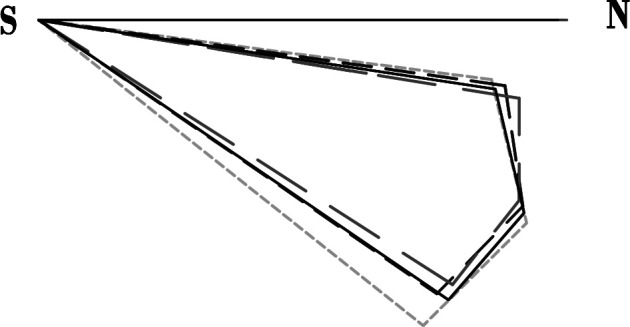
Likewise, the mean lower gonial angle (N Go Me), the Y-axis angle, and the sum of sella, articular, and gonial angles were significantly decreased in the normal overjet group, indicating a more distinctive horizontal facial pattern in this group. In contrast, the extreme overjet group showed a vertical facial pattern (Figures 3 and 4). In other studies, a vertical facial pattern was found in Class II/1 based on the sum (Björk)5,7 and on the Y-axis angle.7,10
Figure 3.
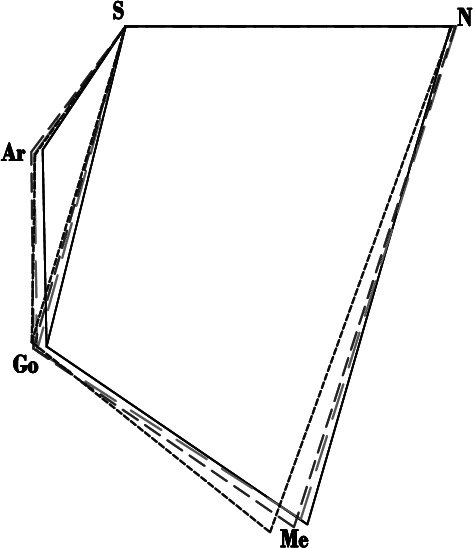
Comparison between the three groups for the Sum (Björk), (-------- Normal Occlusion, ---- ---- Group I, --- --- Group II, ----- Group III).
Figure 4.
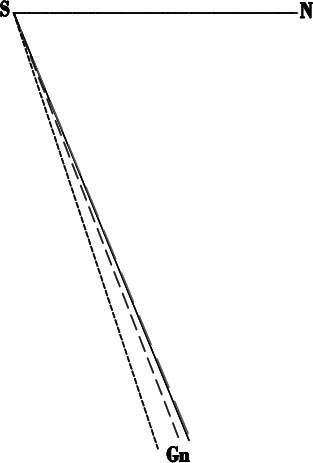
Comparison between the three groups for the N S Gn angle. (-------- Normal Occlusion, ---- ---- Group I, --- --- Group II, ----- Group III).
The association between extreme overjet and a vertical facial pattern may be the result of abnormal muscle function such as altered tongue posture related to mouth breathing and tongue thrust swallowing.
No significant difference was found between the three groups in SNA, suggesting no association between the anteroposterior position of the maxilla and the overjet. In contrast, the palatal plane angle (S-N∶SPP) was significantly smaller in Group 3 than in Group 1 and the norms, indicating an upward inclination of the maxilla with extreme overjet. Various previous studies reported a normal position of the maxilla in Class II malocclusion,7,11,16 and some studies reported that maxillary protrusion is a dominant feature of Class II malocclusion.4,6 The divergent findings may be due to ethnic differences or differences in methods of identifying the maxillary position.
For the mandibular position, mean SNB and SNPog angles for the three groups were significantly less than for the norms, indicating a retrognathic mandible in the three groups. In addition, no significant difference was found between the three groups, indicating no association between the anteroposterior position of the mandible and the overjet (Figure 5). Previous studies reported that mandibular retrusion is a common feature of Class II/14,6,7,11 and Class II/2.6,16
Figure 5.
Comparison between the three groups for the ANB angle. (-------- Normal Occlusion, ---- ---- Group I, --- --- Group II, ----- Group III).
The ANB angle was significantly larger in group 3 than in group 1. Zupančič et al.12 found a positive correlation between overjet and the ANB angle. They indicated that overjet is a good predictor of the ANB angle in subjects with a Class II division 1 malocclusion.
Dentoalveolar Parameters
The upper incisors exhibited a normal inclination and position in Group 3 and were retroclined in Groups 1 and 2 (Figure 6). The position of the upper incisors in the normal overjet group was similar to Angle's description8 of Class II/2 malocclusion, which stated that the upper incisors are more retroclined in Class II/2 than in Class II/1.
Figure 6.
Comparison between the three groups for the dentoalveolar parameters. (-------- Normal Occlusion, ---- ---- Group I, --- --- Group II, ----- Group III).
The mandibular incisors exhibited a normal inclination in Groups 1 and 3 and were proclined in Group 2 (Figure 5). The incisor proclination in Group 2 and the normal inclination in Group 2 might be attributed to dentoalveolar compensation in response to mandibular retrusion in Group 2 and retroclined maxillary incisors in Group 1. In other studies, a relatively normal inclination of the mandibular incisors was found in Class II/1 and Class II/2.4,6 On the other hand, few previous studies reported protrusion of the mandibular incisors in Class II/1.4
The interincisal angle was significantly increased in the normal overjet group, reduced in the extreme overjet group, and normal in the increased overjet group because of retroclined upper incisors in the normal overjet group and proclined upper incisors in the extreme overjet group (Figure 5). A review of the literature reveals a decreased interincisal angle in Class II/1 malocclusion4,7 and an increased interincisal angle in Class II/2 malocclusion.4
The contradiction between the findings of this study and the findings of some previous studies might be due to the ethnicity, gender, age, size, and division of the study sample.
Clinical Implications
Results of this study have important clinical implications. First, because a vertical tendency was identified in extreme overjet cases, greater care is necessary to control the vertical dimension and avoid molar extrusion when treating these cases compared with increased and normal overjet cases, especially because many of the orthodontic mechanics tend to open the bite. Second, because of the skeletal and dentoalveolar characteristics of Class II patients with extreme overjet, early treatment that controls the amount and direction of mandibular growth by using functional appliances could be ideal for these patients. Finally, orthodontists could use the overjet value as a predictor of facial pattern in Class II patients. This needs to be confirmed through longitudinal studies.
CONCLUSIONS
An association was found between the overjet value and the tendency toward a hyperdivergent pattern. As the overjet increased, (S-N∶Go-Me, SPP∶Go-Me, Sum [Björk], Y-axis angle, and N Go Me) tended to increase and (S-Go/N-Me, Ar-Go, and N-Me) tended to decrease. This association was stronger in females than in males.
Subjects with a normal overjet showed a horizontal facial pattern and a posterior inclination of the maxilla, whereas increased overjet subjects exhibited a neutral facial pattern with proclined lower incisors. In contrast, subjects with an extreme overjet had a vertical facial pattern, anterior inclination of the maxilla, and a short mandibular ramus.
The mandible was retrognathic and the maxilla was normally positioned in the three groups.
Acknowledgments
Part of this research was presented as an oral presentation at the 89th Annual Meeting of the International Association for Dental Research (IADR), held March 16–19, 2011, in San Diego, California. The authors are grateful to the patients and their parents for their help in this study. The authors would also like to thank Mr Greg Ogilvie, Dr Abdulsalam Aldomini, Dr Muhannad Alabdulla, and Dr Maher Hallak for their invaluable assistance.
REFERENCES
- 1.Ast D. B, Carlos J. P, Cons D. C. Prevalence and characteristics of malocclusion among senior high school students in upstate New York. Am J Orthod. 1965;51:437–445. doi: 10.1016/0002-9416(65)90241-1. [DOI] [PubMed] [Google Scholar]
- 2.Youssef M. The prevalence of dentofacial deformities in Syria. Damascus Univ J. 1996;12:151–186. [Google Scholar]
- 3.Hassan A. H. Cephalometric characteristics of Class II division 1 malocclusion in a Saudi population living in the western region. The Saudi Dental Journal. 2011;23:23–27. doi: 10.1016/j.sdentj.2010.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Khateeb E. A, Al-Khateeb S. N. Anteroposterior and vertical components of Class II division 1 and division 2 malocclusion. Angle Orthod. 2009;79:859–866. doi: 10.2319/062208-325.1. [DOI] [PubMed] [Google Scholar]
- 5.McNamara J. A., Jr Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51:177–202. doi: 10.1043/0003-3219(1981)051<0177:COCIMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Pancherz H, Zieber K, Hoyer B. Cephalometric characteristics of Class II division 1 and Class II division 2 malocclusions: a comparative study in children. Angle Orthod. 1997;67:111–120. doi: 10.1043/0003-3219(1997)067<0111:CCOCID>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 7.Al-Sairafi E. The Characteristics of Craniofacial Complex of Class II Division 1 Malocclusion Patients in the Permanent Dentition [master's thesis] Latakia, Syria: Tishreen University; 2009. [Google Scholar]
- 8.Angle E. H. Classification of malocclusion. Dental Cosmos. 1899;41:248–264. [Google Scholar]
- 9.Rinchuse D. J, Rinchuse D. J. Ambiguities of Angle's classification. Angle Orthod. 1972;59:295–298. doi: 10.1043/0003-3219(1989)059<0295:AOAC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Ishii N, Deguchi T, Hunt N. P. Craniofacial morphology of Japanese girls with Class II division 1 malocclusion. J Orthod. 2001;28:211–215. doi: 10.1093/ortho/28.3.211. [DOI] [PubMed] [Google Scholar]
- 11.Sayin Ö. Turkkaharaman H: Cephalometric evaluation of nongrowing females with skeletal and dental Class II, division 1 malocclusion. Angle Orthod. 2004;75:656–660. doi: 10.1043/0003-3219(2005)75[656:CEONFW]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Zupančič S, Pohar M, Farčnik F, Ovsenik M. Overjet as a predictor of sagittal skeletal relationships. Eur J Orthod. 2008;30:269–273. doi: 10.1093/ejo/cjm130. [DOI] [PubMed] [Google Scholar]
- 13.Al-Salti M. Craniofacial Morphology of Subjects With Neutral Occlusion in Syria [master's thesis] Damascus, Syria: Damascus University; 2000. [Google Scholar]
- 14.Cohen J. A power primer. Psychol Bull. 1992;112:155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 15.Dahlberg G. Statistical Methods for Medical and Biological Students. London, UK: George Allen & Unwin; 1940. pp. 122–132. [Google Scholar]
- 16.Karlsen A. T, Krogstad O. Morphology and growth in convex profile facial patterns: a longitudinal study. Angle Orthod. 1999;69:334–344. doi: 10.1043/0003-3219(1999)069<0334:MAGICP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Siriwat P. P, Jarabak J. R. Malocclusion and facial morphology: is there a relationship? Angle Orthod. 1985;55:127–138. doi: 10.1043/0003-3219(1985)055<0127:MAFMIT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]