

Abstract
The variety and extent of non-pharmaceutical measures implemented by the government to control COVID-19 in Argentina were exceptional, making this country the best example to analyze the evolution of COVID-19 under the most stringent and longerlasting restrictive policies- which up to May 31st 2021 included 119 days of strict nation-wide lock-down, 304 days of less restrictive lock-downs, and 35 days of curfews. Two of the three peaks of infection correlated with the germicidal solar flux received in Argentina, suggesting a seasonal component and a role for the virus persisting in the environment. A massive public gathering crowding the presidential square in Buenos Aires, during which nearly half of those present were without face masks, did not alter the infection curve in that city. Comparative epidemiological data (standardized per million inhabitants) shows that COVID-19 in Uruguay, a neighboring country whose capital is at a similar latitude than Buenos Aires and who did not mandate lock-downs or curfews, progressed much slower (until vaccination started) than in Argentina. The number of yearly deaths caused by respiratory diseases and influenza in Argentina before the pandemic was similar to the total number of deaths attributed to COVID-19 cumulated on April 25, 2021, more than a year after the pandemic started. The failure to detect any benefit on ameliorating COVID-19 by the long and strict nation-wide lock-downs in Argentina should raise world-wide concerns about mandating costly and ineffective restrictive measures during ongoing or future pandemics.
Significance for public health.
Epidemiological data released by the Ministry of Health of Argentina was compared with the public health policies instituted by that country that have resulted among the longest, most restrictive, and more strictly enforced measures in the world intended to control COVID-19. Analysis of the data failed to detect a benefit of the public health measures instituted in Argentina when compared to a neighboring country with opposing policies. The findings reported here should be considered by Argentina as well as by other countries mandating or planning to implement long lasting stay-at-home orders and lock-downs to control COVID-19 or during future pandemics to come.
Key words: COVID-19, SARS-CoV-2, pandemic, lockdown, curfew, vaccination
Introduction
Computer modeling simulations, mainly from the Imperial College of London, predicted that 7 billion infections and 40 million deaths would occur during 2020 alone if quarantine, lockdowns and other highly restrictive measures were not enforced.1,2 These measures published by leading scientific journals and disseminated widely by the press were considered instrumental3 in justifying 1168 quarantine and lock-down policies mandated by the governments of 165 countries4 which resulted, by the first week of April 2020, in 3.9 billion people (more than half of the world’s population) in quarantine or under in-house lock-downs.5
Paralleling world-wide predictions,1,2 a local simulation study also predicted much worse consequences of the pandemic in Argentina if lock down and other restrictions were not implemented, with infection rates sharply decreasing if the number of quarantined individuals increased.6 In contrast, an earlier study of the effect of traveling (to workplace, to the pharmacy, to buy groceries or to other places) on infection by SARS-CoV-2 reported that lock-down in Argentina could be effective in reducing mobility short term but should not be effective in reducing contagion longterm. 7
Argentina was among the countries instituting early (March 19, 2020) nation-wide and strictly enforced stay-home orders while its neighbor Uruguay chose not to mandate lock-down nor quarantine, allowing free mobility.8 The measures mandated in Argentina may have not been unique but the extent and variety of restrictions imposed on the population (as detailed below) were exceptional, making this country the best example to analyze the evolution of COVID-19 under the most stringent and longer-lasting restrictive policies taken by any country. The starting assumption of the present study was that any beneficial effect of lockdowns, quarantines and curfews should be amply evident in Argentina, if such effect exists.
Design and methods
The policies implemented in Argentina to control COVID-19 were those published periodically in the Argentinean Government Official Bulletin (Boletin Oficial del Gobierno).9 The present analysis comprised COVID-19 epidemiological data released daily by the Ministry of Health of Argentina from March 3rd 2020 to May 31st 2021.10 Total infections per million inhabitants, and deaths attributed to COVID-19 per million inhabitants, were calculated using a population figure of 45.5 million.11
The compliance of mask wearing at the largest public gathering in Argentina during COVID-19 was estimated from ninetyeight different photographs taken at the funeral of ex-soccer star Diego Maradona and posted in the internet by various sources. On these photographs we could score accurately 329 persons as either wearing face mask or not. Epidemiological data for Uruguay was obtained from the country’s government daily updates.12 The epidemiological data corresponding to COVID-19 for Argentina and Uruguay were confirmed by the compilation made by the John’s Hopkins’ Center for System Sciences and Engineering.13 The germicidal solar flux received in Argentina (Buenos Aires) through the year and its virucidal effect on SARS-Co V-2 has been previously published elsewhere.14 Causes of death pre-pandemic were obtained from statistics released in 2018 by the government of Argentina.11
Results
COVID-19 policies in Argentina
The first case of COVID-19 in Argentina was reported on March 3, 2020. The federal government responded to COVID-19 with a Resolution by Need and Urgency (Decreto de Necesidad y Urgencia, DNU # 297/2020) published in the Government Official Bulletin (Boletin Oficial del Gobierno) on March 19, 2020,9 when there were 97 cases and 3 death attributed to COVID-19.10,13 This DNU declared obligatory nation-wide quarantine (Aislamiento Social Preventivo y Obligatorio or ASPO), whereby restricting the population of the whole country to their homes (known in Argentina as Phase I and indicated as region B in Figure 1) with the exceptions of essential personnel, like police. Curiously, personnel in public and private transportation (buses and taxis) were considered essential and allowed to circulate despite their main customers quarantined at home.
Government agencies suspended in-person customer service. Social, cultural and sporting activities were cancelled and commerce closed all day. Exceptions to this policy included public and private clinics and hospitals, veterinary clinics, supermarkets and hardware stores serving to persons with documented addresses nearby (it is mandatory to carry identification documents at all times in Argentina). Persons considered at risk, including obese persons (with Grade II, body mass index 35-39.9 kg/m2), were not allowed to return to work even to perform in the exempted occupations listed above (Resolution of Ministry of Labor # 207/2020). Essential workers must carry a written or digital permit while nonessential individuals may request a temporary circulation permit for going to the doctor, hospital or caring for a sick relative. This circulation permit (called CUIDAR) holds personal data and a QR code to control legitimacy. Persons detained without proper identification or circulation permit were fined or jailed (varying with the province or circumstances) and their vehicles impounded. In addition, face masks, hand washing and social distancing of 1.5-2 meters (5-7 feet) were also required. The Argentinean Minister of Health declared on July 8, 2020 that “all bad colds are coronavirus until proven the contrary”,15 and recommended not to laugh, sing or speak loudly to reduce contagion.16 In addition, The Ministry of Health of Argentina released on April 2020, “Recomendaciones para sexo seguro” (Recommendations for safe sex) stating that to prevent COVID-19 close contacts, including sex should be avoided. 17
The measures mandated in the 1st DNU (#297/2020) were prorogated every 15 days, remaining in force until July 18, 2020 when a new decree (DNU #605/2020) partially relaxed restrictions.18 Under the measures mandated by DNU # 605/2020 (called by the government Distanciamiento Social Preventivo Obligatorio, DISPO or generally known as Phase II, depicted as Region C in Figure 1) industrial, commercial, or services activities were allowed as long as they had an operational permit approved by the provincial sanitary authority within the guidelines mandated by the national sanitary authority. Among other restrictions, the national sanitary authority limited operation of working activities to no more than 50% of the covered area of the installation. It was left to provincial sanitary authorities to rule particular days and hours for the performing of sporting, artistic or social activities as long as (by national guidelines) the number of participants remained below 10 individuals. In addition, the occupational density in close quarters (offices, restaurants, changing rooms, etc.) was limited to one worker per 2.25 square meters. These measures excluded personnel at risk, including obese individuals, from returning to work as decreed on March 19, 2020 (see above). Cinemas, theaters, cultural gatherings, and sports involving more than 10 persons or that could not preclude more than 2 meters separation between players remained prohibited. Tourism and the use of local and long-distance buses, except for personnel with proper authorization were impermissible. Social gatherings and family reunions remained prohibited regardless of numbers, except by people living in the same home.
Figure 1.
Evolution of COVID-19 in Argentina.
Restaurants were reopened (only by reservations, with 2-meter distance, and up to 4 people by table, see horizontal bars beneath the graph in Figure 1) on August 8, 2020, sometimes referred to as Phase III. On October 16, 2020, transportation between cities was allowed by car or train, and obese persons were allowed to return to work (by Resolution # 47124/2020). On October 17, 2020 the ban on urban and inter-urban public transport by school students and their tutors was lifted. On November 26, 2020 the National Government by General Decree #936/2020 authorized three days of national mourning for the death of Diego Maradona (an ex-soccer star, see Figure 1). This measure resulted in a massive gathering that government sources initially estimated to be one million but that disturbances could have reduced to little more than onehundred thousand people each of two days, crowded nearby the Presidential palace in Buenos Aires.19
On December 29, 2020 the vaccination campaign against COVID-19 began in Argentina20 (see label in Figure 1).
The Easter holiday, when over 2 million traveled in Argentina,21 was a main reason to resume curfews on April 16, 2021 when restaurants were ordered to close at 23:00 h and the general population was placed under curfew (prohibited from circulating on the streets, often referred in Argentina as Toque de Queda) from midnight to 06:00 hours. Restaurants and industry curfews advanced to 19:00 h on May 1st, 2021. On this date by DNU # 287/2021,22 Argentina moved back to Phase I (Zone D in Figure 1), imposing the highest level of restrictions as mandated during early 2020. These stringent restrictions were prorogued until May 30th, 2021 when the country transitioned to restrictions corresponding to Phase II with closure of general businesses and restaurants after 19 h and curfew to all but essential personnel between 20 and 06 h on weekdays and curfew all day on weekends.
Progression of COVID-19 in Argentina
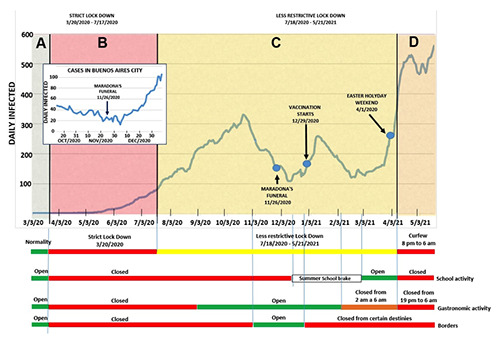
The data reported daily by the Argentinean Ministry of Health10 and summarized in Figure 1 shows the progression (in daily infections per million inhabitants) of COVID-19 from the first case in March 2020 to May 21st, 2021.
In the main panel of Figure 1 COVID-19 infections reported daily by the government of Argentina were divided by the population (in millions) and plotted as a function of date. Arrows point at dates corresponding to the funeral of Diego Maradona, the start of the vaccination campaign, and massive traveling during the Easter holiday. Below the main graph the dates of starting and ending of stay-at-home orders, curfews, schools, restaurants and international borders are indicated. The inset depicts the number of daily infections per million inhabitants in Buenos Aires in relationship to the funeral of Maradona in that city.
The data during the studied period shows that the evolution of COVID-19 in Argentina presented three main peaks separated by two intervening valleys with the following identifiable features after a basal pre-pandemic period (Zone A in Figure 1):
During the initial period of the pandemic (zone B in Figure 1) infections in Argentina remained low and relatively constant until mid-May 2020.
Infections increased rapidly with the incoming winter in spite of strict ongoing stay-at-home orders (enforced by police, Phase I) lasting until July 17, 2020.
After the first peak observed in Figure 1 at the end of October, the number of infections falls rapidly with the start of summer in spite of aperture of international borders and consequent foreign traveling. The arrow in Figure 1 indicates the starting of the funeral of Diego Maradona which resulted in a massive gathering of people in Buenos Aires.23 We downloaded and analyzed as described in the Method section the available photographs (N=98) from the funeral and determined that 46.5% of the attending persons did not wear face masks (n= 329). Daily infections (per million in the inset of Figure 1) in Buenos Aires according to local data24 remained relatively low (at or below the figures reported for the days immediately before the funeral, 40 cases/million per day) for 24 days after the funeral, until December 19, 2021, when infections begun increasing at a sustained rate.
Unexpectedly, the apparent seasonal pattern of the pandemic is broken by a second peak of infections starting at the height of summer during late December-early January 2021. Infections begun increasing after the Holidays (Christmas and New Year) which coincided with the start of the vaccination program20 (began in December 29, 2020, see arrow in Figure 1).
The second peak of infections in Argentina decreases to a valley during March 2021.
The major peak of COVID-19 in Argentina starts at the end of March 2021 (end of summer) and before extensive traveling during the Easter Holiday.21
Figure 2 compares the progression of COVID-19 (infections per million inhabitants) in Argentina with neighboring Uruguay,12,13 a country smaller and less populated than Argentina but of similar demographic composition25,26 as presented in Table 1, whose capital city, Montevideo, is nearly at the same latitude as Buenos Aires and hence with comparable germicidal solar flux throughout the year.
Epidemiological data released by both governments was standardized per million inhabitants and shown as a function of dates in red for Argentina and blue for Uruguay. Main panel shows infections per million inhabitants with arrows pointing the initiation of the respective vaccination campaigns. The inset depicts the progression of deaths attributed to COVID-19 in both countries.
In contrast to Argentina, Uruguay did not institute lock-downs and curfews nor closed schools or restaurants through the pandemic. 8 The data in Figure 2 show that infections in Uruguay remained relatively constant and considerably lower than in Argentina from the first COVID-19 case to May 3, 2021. The number of deaths per million inhabitants follows the shape of infections per million in both countries with higher numbers in Argentina than in Uruguay until mid-May 2021 (Figure 2 inset) at which time deaths per million inhabitants become similar in both countries. Unexpectedly, infections and deaths failed to decrease after initiation of the vaccination campaigns in both countries. According to data published by the Argentinean Ministry of Health in absence of pandemic (last report for year 2018)11 more than 300,000 deaths occur yearly by identified causes. The leading cause of death in Argentina is heart and circulatory failure. Respiratory diseases, including pneumonia and influenza amounted to 61,668 in 2018 (Table 2), corresponding to 1,386 deaths per million inhabitants. After one year of pandemic since the first case (on March 3, 2020) the total number of deaths on March 3, 2021 were 52,453 (1179/million, Figure 2 inset). This number is smaller than the number of deaths caused by diseases of the respiratory system (including influenza) in Argentina during one year before the pandemic (Table 2).
The number of deaths attributed to COVID-19 (Figure 2 inset) did not reach a number similar to the number of deaths caused by respiratory diseases (including influenza) before the pandemic in Argentina (61,668 deaths or 1,386 deaths per million) until April 25, 2021, more than one year after the first death attributed to SARS-CoV-2. Although the restrictive measures mandated in Argentina failed to prevent infection by SARS-CoV-2 and progression of COVID-19 as demonstrated by at least three peaks of infections in Figure 1, the policies resulted in the economical retraction of the GDP and GDP per capita shown in Table 2 as indicated by World Bank figures.27
Discussion
Seasonal effect
Early in the pandemic, during summer up to mid May 2020, the number of daily infections in Argentina remained relatively constant and low. The strictest confinement measures in force during this period (known in Argentina as Phase 1) did not prevent the increase in infections that started during mid May, 2020 and continued until the end of October 2020 (Phase II, zone C in Figure 1). The low infection rate observed up to mid May 2020 coincides with the relatively high germicidal solar flux received in Argentina during the end of summer and fall (UVB fluxes of 0.37 and 0.24 Jm-2 min-1, respectively).14 These germicidal solar fluxes should inactivate 90% of SARS-CoV-2 in Buenos Aires after 19 or 29 minutes of exposure, respectively.14
Table 1.
Key demographic parameters in Argentina and Uruguay.
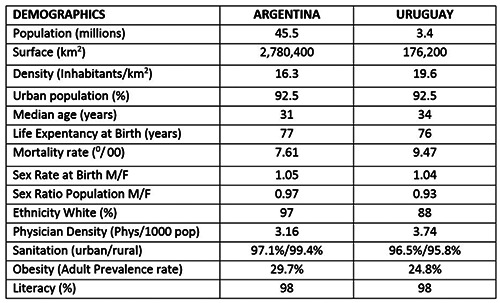
Table 2.
COVID-19 compared to other causes of death in Argentina.
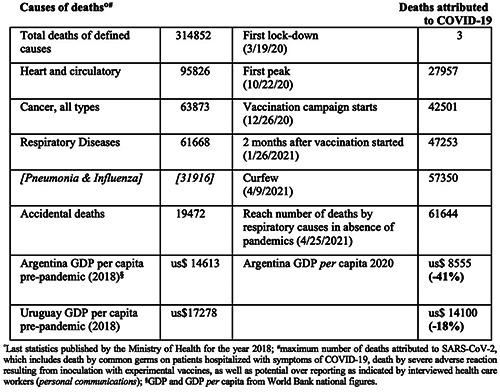
Figure 2.
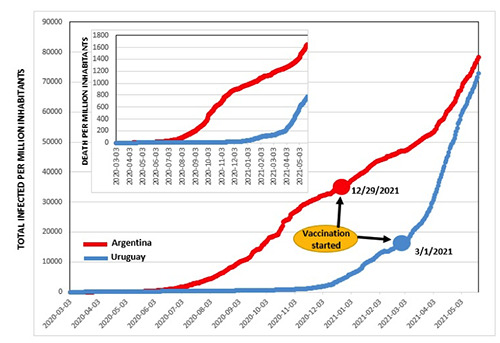
Comparison of COVID-19 in Uruguay and Argentina.
The increase of infections in July-October 2020, as well as the peak beginning at the end of March 2021 correlate with minimal or decreasing germicidal solar radiation received in Argentina (0.04 Jm-2 min-1 during solar noon) when 90% of SARS-CoV-2 should persist infectious during relatively long time (several hours or days) in Buenos Aires.14 After peaking in October 22, 2020, the sharp decrease in daily infections during November, 2020 correlates with the solar transit to the Tropic of Capricorn with increasing solar flux in Argentina and relatively rapid inactivation of SARS-Co V-2 (90% in 19 min of noon sunlight in Buenos Aires) reaching a minimum of infections through the summer (December 2020 in Figure 1). The positive correlation between daily infections and germicidal solar flux in at last two of the infection peaks in Argentina indicates that inactivation of SARS-CoV-2 plays a role in the evolution of the pandemic. The present finding of seasonality of COVID-19 in Argentina agrees with previous studies suggesting a role of virus persisting in the environment during COVID-19 since direct person-to-person transmission does not afford enough time for viral inactivation by solar radiation (requiring several minutes exposure).28
However, one of the three peaks in infections initiated in summer 2021 when solar radiation was abundant (Figure 1). This particular unseasonable raise in infections not correlated with solar flux begun increasing at the end of December 2020 and peaked approximately on January 11, 2021. This summer peak could be explained by infections at family gatherings during the Holydays (Christmas and New Year). However, two large national gatherings in Argentina did not affect the infection curve. Infections remained low after more than 200,000 people gathered at the funeral of Maradona and traveling of over 2 million during Easter did not alter the increasing slope of the third peak presented in Figure 1. Thus, gathering of people during a previous large event and a later Holiday do not support increased infections during celebration of Christmas and New Year in Argentina.
The increase of infections in summer reach its peak approximately 15 days after initiation of the vaccination campaign in Argentina (Figure 1). Similarly, Uruguay, having had relatively fewer infections per million than Argentina, shows a steep increasing slope of infections at the start of vaccinations in that country (Figure 2). We present no conclusive data nor are implying a cause-effect relationship between infections and vaccination. Any potential correlation between vaccination and infection in Argentina, as well as in Uruguay, is well beyond the scope of the present analysis but the observation deserves further study and elucidation.
Travel and social distancing
The funeral of Diego Maradona (an ex-soccer star worshiped in Argentina) appears to have been the largest gathering of people during COVID-19 anywhere in the world, which allows one to draw unique conclusions. Daily infections remained relatively low in Buenos Aires during 24 days after the funeral (Figure 1 inset). Considering that 97.5% of the symptoms caused by SARS-CoV-2 develop within 8.2 to 15.6 days of infection;29 the 24-day period following Maradona’s funeral provided ample time for COVID-19 to flare up if significant contagion would have proliferated amongst the crowded mourners. That a gathering of approximately 200,000 people, approximately half of which did not wear face masks (see Results) and all crowded within a relatively small area (within the square across the government palace and few surrounding streets), failed to fuel COVID-19 infections (at the end of December 2020, in Figure 1, inset) may not be definitive evidence but warrants further research about any beneficial effect of social distancing (and mask wearing) during the pandemic.
To the mobility of over two-million travelers in Argentina during the Easter holiday (1-7 April 2021),21 the national government responded with strict curfews.22 These curfews however, failed to alter the peak of infection that started approximately on March 25, 2021. Thus, epidemiological data (released by the government) presented in Figure 1 indicates that domestic traveling had no detectable effect on COVID-19 in Argentina.
Closing international borders did not prevent the infection peak occurring in October 2020 (in Zone C of Figure 1) and opening borders in November 2020 was followed by a decrease in infections. Similarly, closing and opening schools or restaurants (at the dates indicated at the bottom of Figure 1) showed no effect on infections.
Lack of effect of restrictions
Infections in Argentina increased in spite of strict confinement during Phase I (zone B in Figure 1) and peaks of infection still occurred during partial restrictions in Phase II (zone C in Figure 1). Infections nearly doubled after instituting curfew on May 1st, 2021 that by police’s strict enforcement prevented total displacement of the general population (except essential personnel with official written authorization).22 The increase in infections during strict lock-down and curfews agrees with a previous study suggesting that forcing people to remain indoors, at home or in nursing homes, should increase (or assure) contagion among same household dwellers and among patients and personnel inside the same hospital or geriatric facilities.14
To justify the high cost of lock-downs, any positive effect should have clearly surfaced in the present study above any potential effect of co-founding variables (curfew compliance, mask wearing, obesity, urbanization, demographics, etc.). Any limitations assigned to the accuracy of the data reported here should equally affect Argentina and Uruguay (with and without lockdowns, respectively), as well as many other countries of the world,28 thus having little bearing on the conclusions being presented.
The number of deaths attributed to COVID-19 in Argentina could include the basal number of deaths (in absence of epidemics) caused by common and recurrent respiratory diseases. In addition, an undetermined number of COVID-19 reported deaths should have occurred due to: i) hospital infections by common germs contracted by patients hospitalized with COVID-19; and ii) to adverse reactions to vaccination. Therefore, deaths attributed to COVID-19 in Argentina could be over-reported. Regardless of the extent of over-reporting, deaths attributed to COVID-19 equaled pre-pandemic deaths by respiratory disease (including influenza) only after more than one year of pandemic. In spite of a mortality attributed to COVID-19, similar to yearly deaths by respiratory causes pre-pandemics, Argentinean society had to endure during the crisis 119 days of strict lock-down (Phase I), 304 days of less restrictive lock-downs (Phase II), and 35 days of curfews (see the Policies section above).
The progression of COVID-19 in Uruguay compared to Argentina in Figure 2 further demonstrates that lock-downs and curfews have no measurable benefit and instead, lock-downs could have accelerated the progression of COVID-19. In contrast, lockdowns and curfews seem to have a considerable impact on the economy (Table 2), with Argentina showing during 2020 a reduction in per capita GDP twice as high as that of Uruguay (were lock-downs were not mandated).
The fact that evolution of the pandemic in two neighboring countries with similar demographics and opposite policies (Uruguay and Argentina) failed to detect any obvious benefit in COVID-19 infection or mortality of long and strict nation-wide lock-downs, closures and curfews, as instituted in Argentina, should be convincing evidence, or at least rise concerns, about insisting during 2021 in mandating these costly restrictive measures. Considering the devastating effect on society and the economy, the burden of proof should fall heavily on proving a benefit of lock-downs and not on demonstrating their irrelevance.
The lack of a beneficial effect of lock-down on the progression of COVID-19 in Argentina expands and confirms the previous findings by Larrosa7 and refute predictions by computer simulations of world-wide scope1,2 as well as a local report (also based on computer simulation) that the pandemic would be controlled by lock-down, curfews and increasing restrictions.6 Lock-downs and other restrictive measures remained in place in Argentina and many other countries throughout the year 2020 and first quarter of 2021, in spite of reports indicating as early as May-August 2020 that: i) preventing healthy individuals from remaining outdoors had not resulted in significant differences (as of May 2020) on infection when compared to countries were individuals were free to stay outdoors;14,28 ii) infection rates and mortality rates fell among countries with and without lock-downs without a significant pattern;3 and iii) full lock-downs were not associated with statistical significant reductions in the number of critical cases or overall mortality.30 Any benefits of lock-downs were questioned in Germany,31 not apparent in the Republic of South Africa,32 and ruled out as responsible in any decrease of the effective epidemic reproductive rate in the UK, suggesting these authors that key predictions by computer simulation should be considered artifacts.33
Although the measures imposed in Argentina may have been extreme, the findings of the present study should apply to several other countries that implemented similar policies (albeit at a lesser degree). The findings reported here, in agreement with those noted above,3,14,28,30-33 demonstrate that virtual computer simulation could complement but never replace real epidemiological data in policy making. These findings suggest that governments should refrain from reacting to unproven and apocalyptic predictions. Instead, carefully selecting to manage the pandemic of scientific leaders with specific and documented experience (by peerreviewed publications in pertinent disciplines like field epidemiology, virology of rapid and lethal viruses, infection control, and/or immunology) seems as the best (and perhaps only) defense for avoiding the unproved measures that resulted so costly to the society and economy of Argentina as well as to those other countries adopting similar policies.
Acknowledgements
The critical review of the manuscript and valuable comments made by Dr. Amadeo Esposto are appreciated. Mrs. Francesca Zelachowski is thanked by the editorial review and corrections of the manuscript.
References
- 1.Walker PGT, Whittaker C, Watson O, et al. Imperial College of London's Report 12. The global impact of COVID-19 and strategies for mitigation and suppression. 2020 Mar. Accessed: 2020. May 1. Available from: https://www.imperial.ac.uk/mrcglobal-infectious-disease-analysis/covid-19/report-12-globalimpact-covid-19/ [Google Scholar]
- 2.Flaxman S, Mishra S, Gandy A, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020;584:257-62. [DOI] [PubMed] [Google Scholar]
- 3.Sagripanti J-L. Prestige does not bring truth. How apocalyptic predictions may have altered the natural evolution of COVID- 19. CBRNe WORLD 2020 (Summer/August issue) 40-43. [Google Scholar]
- 4.Cheng C, Barceló J, Hartnett A, et al. COVID-19 Government Response Event Dataset (CoronaNet v.1.0). Nat Hum Behav 2020;4:756-68. [DOI] [PubMed] [Google Scholar]
- 5.Sandford A. Coronavirus: Half of humanity now on lockdown as 90 countries call for confinement. [Internet] Euronews 2020. Accessed: 2020 May 20. Available from: https://yournews.com/2020/04/02/1544253/coronavirus-half-of-humanity-now-on-lockdown-as-90-countries/ [Google Scholar]
- 6.Borracci RA, Giglio ND. Forecasting the effect of social distancing on COVID-19 autumn-winter outbreak in the metropolitan area of Buenos Aires. Medicina (B Aires) 2020;80:s7-15. [PubMed] [Google Scholar]
- 7.Larrosa JMC. SARS-CoV-2 in Argentina: Lockdown, mobility, and contagion. J Med Virol 2021;93:2252-61. [DOI] [PubMed] [Google Scholar]
- 8.Dunfordv D, Dale B, Stylianou N, et al. Coronavirus: The world in lockdown in maps and charts. British Broadcasting Service. 2020. Accessed: 2020 Apr 7. Available from: www.bbc.com/news/world-52103747 [Google Scholar]
- 9.Argentine Government Bulletin. [Decreto de Necesidad y Urgencia, DNU # 297/2020). Aislamiento Social y Preventivo].[In Spanish]. Accessed: 2020. Mar 19. Available from: https://www.boletinoficial.gob.ar/detalleAviso/primera/227042/20200320 [Google Scholar]
- 10.Ministry of Health of Argentina. [Sala de situacion, Comunicados diarios (COVID-19 daily reports)].[In Spanish]. March 3rd 2020 to May 31st 2021. Accessed: 2020 Mar 3. Available from: https://www.argentina.gob.ar/salud/coronavirus-COVID-19/sala-situacion [Google Scholar]
- 11.Ministry of Health of Argentina. Estadisticas Vitales. Informacion Basica (Vital Statistics. Basic information)].[In Spanish]. Serie 5 Num 62. 2018. Available from: http://www.deis.msal.gov.ar/wp-content/uploads/2020/01/Serie5Nro62.pdf [Google Scholar]
- 12.Ministry of Public Health of Uruguay. 2020-2021. [Informe de situación sobre el coronavirus COVID-19 en Uruguay (Report on the Situation about COVID-19)].[In Spanish]. Available from: https://www.gub.uy/sistema-nacional-emergencias/comunicacion/noticias/informacion-actualizada-sobre-coronavirus-covid-19-uruguay [Google Scholar]
- 13.John's Hopkins' Center for System Sciences and Engineering [Internet] Coronavirus Statistics. Stats real time. Accessed: 2020. May 7 to Dec 14. Available from: www.epidemicstats.com [Google Scholar]
- 14.Sagripanti J-L, Lytle CD. Estimated inactivation of coronaviruses by solar radiation with special reference to COVID-19. Photochem Photobiol 2020;96:731-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Blanco D. [Todo resfrío es coronavirus hasta que se demuestre lo contrario? Expertos criticaron la declaración de Carla Vizzotti. (Every cold is coronavirus unless otherwise demonstrated. Experts criticized Carla Vizzotti’s statements)].[In Spanish]. Infobae.com [Internet]. Accessed: 2020. Jul 9. Available from: https://www.infobae.com/salud/2020/07/09/las-declaraciones-de-carla-vizzotti-sobre-que-todo-resfrio-esun-coronavirus-hasta-que-se-demuestre-lo-contrario-provocola-reaccion-de-los-expertos-puede-generar-miedo-y-una-eventual-sobredemanda-del-sistema-de-salud/ [Google Scholar]
- 16.Vizzotti C.. [El Ministerio de Salud recomendó evitar “hablar fuerte, cantar o reírse” sin tapabocas en lugares cerrados (The Ministry of Health recommended not to speak louder, sing or laugh in closed rooms)].[In Spanish]. Daily reports from de Ministry of Health. Live broadcast from the Pink House. Accessed: 2020. Aug 27. Available from: https://www.youtube. com/watch?v=Mt24WINk2E8&ab_channel=CasaRosada-Rep%C3%BAblicaArgentina [Google Scholar]
- 17.Gonzalez Garcia G. Argentina’s Minister of Health [Internet]. Recommendations for safe sex [Text in spanish] [Cited 2020 Apr 16] Available from: http://www.msal.gob.ar/images/stories/ryc/graficos/0000001468cnt-covid-19_recomendacionespara-sexo-seguro.pdf [Google Scholar]
- 18.Argentine Government Bulletin. [Decreto de Necesidad y Urgencia DNU #605/2020. Distanciamiento Social Preventivo Obligatorio (Decree of Necessity and Urgency DNU #605/2020. Preventive and Mandatory Social distancing)].[In Spanish]. Accessed: 2020. Jul 18. Available from: https://www.boletinoficial.gob.ar/detalleAviso/primera/232234/20200718 [Google Scholar]
- 19.Argentine Government Bulletin. [Duelo Nacional por la muerte de Diego Maradona. Decreto 936/2020 (National mourning for the death of Diego Maradona. Decree 936/2020)].[In Spanish]. Accessed: 2020. Nov 25. Available from: https://www.boletinoficial.gob.ar/detalleAviso/primera/5237540/20201125?busqueda=2&suplemento=1 [Google Scholar]
- 20.Argentine Government Bulletin. [Plan estratégico para la vacunación contra Covid-19 en la República Argentina. Boletin Oficial de Gobierno. Resolución 2883/2020 (Strategic plan for vaccination against Covid-19 in the Argentine Republic)].[In Spanish]. Resolution 2883/2020. Accessed: 2020. Dec 29. Available from: https://www.boletinoficial.gob.ar/detalleAviso/primera/239326/20201230 [Google Scholar]
- 21.Klempert Izaguirre R. ["Antes del cierre", casi 2 millones de argentinos viajaron en Semana (Santa Easter Holiday travel 2 million travelers and reason for government restrictions)].[In Spanish]. Hoteltur 2021 [Internet]. Accessed: 2021. Apr 4. Available from: https://www.hosteltur.com/lat/143340_antesdel-cierre-casi-2-millones-de-argentinos-viajaron-en-semanasanta.html [Google Scholar]
- 22.Argentine Government Bulletin. [Medidas Generales de Prevención. DNU # 287/2021 (General Prevention Measures. DNU # 287/2021)].[In Spanish]. Accessed: 2021. Apr 30. Available from: https://www.argentina.gob.ar/normativa/nacional/decreto-287-2021-349492 [Google Scholar]
- 23.Frederic S. [Tras las denuncias, la Ciudad acusó al Gobierno de “politizar” el velorio y Frederic salió al cruce (The Government of Buenos Aires City blamed the National Government of politicizing the wake of Maradona)].[In Spanish]. Todo Noticias [Internet]. Accessed: 2020. Nov 28. Available from: https://tn.com.ar/politica/2020/11/28/la-muerte-de-diego-maradona-tras-las-denuncias-la-ciudad-acuso-algobierno-de-politizar-el-velorio-y-frederic-salio-al-cruce/ [Google Scholar]
- 24.Bourdet G. [El mapa del COVID-19 en CABA (The map of COVID en Buenos Aires City)].[In Spanish]. Diario La Nación [Internet]. Accessed: 2021 Jun 13. Available from: https://www.lanacion.com.ar/sociedad/coronavirus-cabamapa-pandemia-comuna-comuna-nid2364565/ [Google Scholar]
- 25.Country Reports [Internet]. Argentina Demographics. 2021. Accessed: 2021 Aug 20. Available from: https://www.countryreports.org/country/Argentina/population/overview.htm [Google Scholar]
- 26.Country Reports [Internet]. Uruguay Demographics. 2021. Accessed: 2021 Aug 20.Available from: https://www.countryreports.org/country/Uruguay/population.htm [Google Scholar]
- 27.Statistics Times [Internet]. GDP per capita of Argentina. Current World Bank figures. 2021. Accessed: 2021 Jan 01. Available from: https://www.statisticstimes.com/economy/country/argentina-gdp-per-capita.php [Google Scholar]
- 28.Sagripanti J-L. Seasonality and progression of COVID-19 among countries with or without lock-downs. Open J Epidemiol 2021;11:303-25. [Google Scholar]
- 29.Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann Intern Med 2020;172:577-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chaudhry R, Dranitsaris G, Mubashir T, et al. A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. eClin Med 2020;25:100464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wieland T. A phenomenological approach to assessing the effectiveness of COVID-19 related nonpharmaceutical interventions in Germany. Saf Sci 2020;131:104924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Broadbent A, Combrink H, Smart B. COVID-19 in South Africa. Glob Epidemiol 2020;2:100034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kuhbandner C, Homburg S. Commentary: Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Front Med 2020;7:761. [DOI] [PMC free article] [PubMed] [Google Scholar]