

Supplemental digital content is available in the text.
Key words: health care professionals, mixed-methods systematic review, quality of care, work behavior, work motivation
Background
Health care professionals’ work motivation is assumed to be crucial for the quality of hospital care, but it is unclear which type of motivation ought to be stimulated to improve quality. Motivation and similar concepts are aligned along a motivational continuum that ranges from (intrinsic) autonomous motivation to (extrinsic) controlled motivation to provide a framework for this mixed-methods systematic review.
Purpose
This mixed-methods systematic review aims to link various types of health care professionals’ motivation directly and through their work-related behaviors to quality of care.
Methods
Six databases were searched from January 1990 to August 2016. Qualitative and quantitative studies were included if they reported on work motivation in relationship to work behavior and/or quality, and study participants were health care professionals working in hospitals in high-income countries. Study bias was evaluated using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. The review protocol was registered in the PROSPERO database (CRD42016043284).
Results
A total of 84 out of 6,525 unique records met the inclusion criteria. Results show that health care professionals’ autonomous motivation improves their quality perceptions and work-related behaviors. Controlled motivation inhibits voicing behavior, but when balanced with autonomous motivation, it stimulates core task and proactive behavior. Proactivity is associated with increased quality of care perceptions.
Practice Implications
To improve quality of care, policy makers and managers need to support health care professionals’ autonomous motivation and recognize and facilitate proactivity as an essential part of health care professionals’ jobs. Incentive-based quality improvements need to be complemented with aspects that stimulate autonomous motivation.
It is widely assumed that health care professionals’ work motivation is beneficial for the quality of patient care in hospitals (Berenson & Rice, 2015; Franco, Bennett, & Kanfer, 2002). Health care professionals’ work motivation is increasingly being investigated, as scholars draw on the positive effects of motivation on performance that were observed in the organizational literature (Cerasoli, Nicklin, & Ford, 2014; Kim, Kolb, & Kim, 2013). However, it is unclear whether these findings apply to the quality of patient care, as studies from the field of organizational research tend to focus on individual-level employee outcomes, such as performance or employee behavior, rather than on team or organizational outcomes (Kim et al., 2013). In a complex system as health care, quality follows from the performance of many independent actors working together in a connected system, which means that performance at the individual level does not necessarily predict the outcomes of the system: quality of care (Griffin, Neal, & Parker, as cited in Gagné, 2014; Hollnagel, Wears, & Braithwaite, 2015).
The inability to determine whether and how health care professionals’ motivation affects patient care is problematic, because it hampers the development of effective motivation-based policies and interventions to boost care quality. Moreover, current motivational strategies may even have unintended consequences. For example, financial incentives, which are widely popular in health care (Berenson & Rice, 2015; Flodgren et al., 2011), may improve performance on relatively simple tasks but at the same time hold the potential to “crowd out” intrinsic motivation, which determines the quality of performance on complex tasks (Cerasoli et al., 2014). Therefore, more insight is needed in the relationships between health care professionals’ work motivation, their work behaviors, and the quality of care.
Previous attempts to integrate the literature on this topic were unsuccessful in linking health care professionals’ work motivation to the quality of hospital care. In an overview of reviews, Flodgren et al. (2011) concluded that there is some but limited evidence for the effectiveness of financial incentives in changing professional practice, but no evidence to support any effects on patient outcomes. Likewise, systematic reviews on nurses’ work engagement and physicians’ occupational well-being reported positive associations with work behaviors, but the link with care outcomes was understudied (Keyko, Cummings, Yonge, & Wong, 2016; Scheepers, Boerebach, Arah, Heineman, & Lombarts, 2015).
This review aims to go beyond existing work to get more insight in the relationship between motivation and quality of care. To achieve this aim, we apply a broad approach by synthesizing the evidence from quantitative and qualitative studies on (a) the direct relationships between autonomous motivation, controlled motivation, and amotivation of all health care professionals involved in direct patient care in hospitals and the quality of hospital care, (b) the relationships between these types of work motivation and health care professionals’ core task and (c) proactive behaviors, and (d) the relationship between proactive behaviors and the quality of patient care in hospitals. To overcome a potential lack of evidence due to narrow conceptualizations of work motivation and work behavior as observed in previous reviews, we use extensive conceptualizations of these constructs by considering similar concepts, which we place within a theoretical framework to guide our systematic search for evidence and the synthesis of results. The theoretical framework and research questions are depicted in Figure 1 and will be further explained subsequently.
Figure 1.
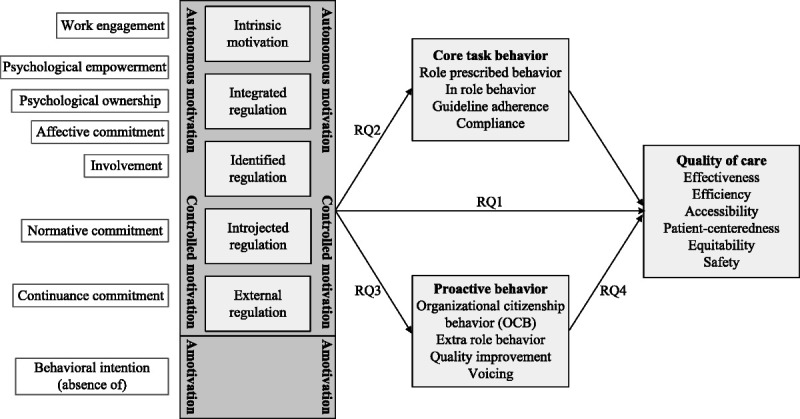
Theoretical framework: motivational continuum and Research Questions (RQ) 1–4
Background
Motivation
Work motivation is defined as “a set of energetic forces originating within and beyond an individual’s being, which determines the form, direction, intensity and duration of work- related behavior” (Pinder, as cited in Gagné, 2014, p. 38). According to the self-determination theory, various forms of work motivation exist on a continuum (Deci & Ryan, as cited in Gagné, 2014). This continuum ranges from autonomous motivation at the one end, through controlled motivation, to amotivation at the other end of the continuum. Autonomous motivation means that the reasons to engage in a behavior stem from within a person. From most autonomous to least autonomous, a behavior can be perceived as enjoyable or interesting in itself (intrinsic motivation), or as an integral part of oneself (integrated regulation), or the values underlying the behavior can be considered congruent with one’s personal goals and identity (identified regulation). Controlled motivation means that reasons to engage in a behavior stem from beyond a person. When driven by controlled motivation, a behavior is done because it has instrumental value; it helps to obtain a sense of self-worth or prevents one from feeling guilty (introjected regulation) or it leads to a separable outcome such as money or status (external regulation). Amotivation refers to not being motivated to engage in an activity (Deci & Ryan, as cited in Gagné, 2014).
From this perspective, we align several related constructs that refer to energetic forces that guide behavior with this motivational continuum to guide our review. From most to least autonomous, we consider work engagement (“a positive affective-motivational state of work related well-being”; Bakker et al., as cited in Kim et al., 2013, p. 249), psychological empowerment (intrinsic task motivation due to finding the task meaningful and experiencing self-efficacy and a sense of impact; Thomas & Velthouse, as cited in Gagné, 2014), psychological ownership (being psychologically tied to an object as an extension of one’s identity, e.g., the organization, or the patient; Van Dyne & Pierce, 2004), affective commitment (“a force that binds an individual to a course of action relevant to one or more targets,” e.g., the job, organization or patient, based on values, personal involvement, and identity; Meyer & Herscovitch, as cited in Gagné, 2014, p. 34), and finally job and work involvement (the importance of one’s job or work in general; Kanungo, as cited in Gagné, 2014).
At the controlled side of the continuum, we consider normative commitment (an attachment to a target based on a perceived obligation; Meyer & Herscovitch, as cited in Gagné, 2014) and continuance commitment (an attachment to a target based on a cost–benefit analysis of maintaining versus withdrawing from the commitment; Meyer & Herscovitch, as cited in Gagné, 2014).
Finally, a construct that is often used to predict behavior is behavioral intention, which refers to a willingness to exert effort to achieve something (Ajzen, 1991). This construct can be interpreted as the absence of amotivation. To enhance readability, the concepts at the autonomous side of the continuum are referred to as autonomous motivation, and the concepts corresponding with the controlled side are referred to as controlled motivation. When relevant, specifications are given.
Quality of Care
The main aim of this review is to understand the impact of health care professionals’ work motivation on the quality of care. Quality of care encompasses more than just one type of outcome. Following the World Health Organization, quality is defined along six dimensions: effectiveness (congruent with current medical evidence and leads to improved health outcomes), efficiency (optimal and sustainable use of personnel and resources), accessibility (timeliness and skills and resources match the medical need), patient-centeredness (respects for individual needs and preferences of the patient), equitability (equality despite gender, ethnicity, or socioeconomic status), and safety (minimized risk and harm to patients; World Health Organization, 2006). This review aims to shed more light on Research Question 1: “How do autonomous motivation, controlled motivation, and amotivation relate to the six dimensions of quality of hospital care?”
Work Behaviors
Health care professionals’ actions within a hospital system are the core of patient care. For this reason, it is meaningful to consider health care professionals’ work behaviors as mediators between motivation and quality of care (Franco et al., 2002).
Work behavior can be classified into two types, namely core task behavior and proactive behavior (Kim et al., 2013; Van Dyne & Pierce, 2004). Core task behavior refers to the behaviors to fulfill formal task requirements (Crant, as cited in Gagné, 2014), which is similar to role prescribed (or in-role) behavior (behavior that is recognized by the formal reward system and that is part of the job description; Borman & Motowidlo, as cited in Kim et al., 2013). Examples of core task behaviors are guideline adherence and compliance to organizational procedures and protocols (Gagné, 2014). Studies using these concepts are included in our review in order to answer Research Question 2: “How do autonomous motivation, controlled motivation, and amotivation relate to health care professionals’ core task behaviors?”
Many core task behaviors are formalized in evidence-based guidelines and protocols, which are specific per discipline within the hospital and grounded in ample scientific evidence (Greenhalgh, Howick, & Maskrey, 2014). Consequently, the relationship between core task behaviors and quality of care is too extensive for this review. Yet, it can be argued that, although there are exceptions, exerting these behaviors contributes to care quality.
Proactive behavior, the second type of behavior, refers to challenging current circumstances and taking initiative to create new ones and is also described as going beyond one’s job or task requirements (Gagné, 2014). Similar concepts are extra-role behavior (positive and discretionary behavior that is not prescribed in formal job descriptions; Borman & Motowidlo, as cited in Kim et al., 2013) and organizational citizenship behavior, which refers “discretionary work behaviors that contribute to organizational well-being but are not part of formal job expectations” (Organ, as cited in Van Dyne & Pierce, 2004, p. 446). Examples of proactive behaviors are engaging in quality improvements and voicing concerns or speaking up in unsafe clinical situations (Gagné, 2014). We include these concepts in our review to determine their motivators, as Research Question 3 states: “How do autonomous, controlled, and amotivation relate to health care professionals’ proactive behaviors?”
Health care professionals’ proactive behaviors are indispensable for quality of care, as the complexity of the health care system can never be completely captured in guidelines and protocols (Greenhalgh et al., 2014; Hollnagel et al., 2015). However, proactive behavior may have inconsistent contributions for each of the six dimensions of quality. For example, patient-centeredness is likely to increase when health care professionals “go the extra mile” for their patients, but this may diminish efficiency. Therefore, Research Question 4 states: “How do health care professionals’ proactive behaviors relate to outcomes on the six dimensions of quality of hospital care?”
Methods
In line with the broad approach of this review, a mixed-methods systematic review was conducted. Reviews can be mixed by including various types of studies, by applying mixed methods for the synthesis of studies, or by applying both theory building and theory testing modes of analysis (Harden, 2010). This systematic review was mixed in the sense that we included qualitative, quantitative, and mixed-methods studies. This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO, No. CRD42016043284) of the University of York. The data were managed using a PRISMA-based Excel workbook and ATLAS.ti, Version 8.3.2.
Sources and Search Strategy
An elaborate search string was entered into PubMed, PsycINFO, Business Source Premier, CINAHL, EMBASE, and Web of Science. Two librarians (from medical and social sciences departments) were consulted for the development of the search string, which combined three key themes: motivation/behavior (e.g., motivation OR engagement OR proactive behavior OR guideline adherence), health care professionals (e.g., nurse OR physician OR resident), and quality of care (e.g., effectiveness OR safety). The search was limited to studies published in an academic journal between January 1990 and August 2016 and written in the English language. The full search string is available from the first author on request.
The search string identified a large number of records, which included all relevant references obtained from related reviews. Consequently, it was considered appropriate to deviate from the research protocol by not performing a backward reference search.
Study Selection
To be eligible for inclusion in the systematic review, a paper had to match the following criteria: be an empirical quantitative or qualitative paper revealing information on at least one of the four research questions, study participants were health care professionals providing direct patient care, the study took place within a hospital setting and in a high-income country as classified by the World Bank (The World Bank Group, 2016), because the availability of resources is an important factor influencing care quality in middle- and low-income countries (Fritzen, 2007). Furthermore, the paper had to report on individual-level self-reported measures of work motivation, whereas the measures of health care professionals’ behaviors and quality of care could take place at either the individual or at the group level and could be either self-reported (e.g., self-reported behavior or perceived quality) or externally assessed (e.g., supervisor-assessed work behavior or outcomes derived from hospital systems).
The interrater agreement for a random selection of 10% of the screened records was unsatisfactory for both the title and abstract and full-text screening (around 0.5). Consequently, we deviated from the review protocol, which describes that the first author would screen the remaining papers. Instead, the complete title and abstract screening and the complete full-text screening were done by two independent reviewers. Inconsistencies were discussed until consensus was reached.
Risk of Bias, Data Extraction, and Synthesis of Results
The risk of bias was assessed using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers (Kmet, Cook, & Lee, 2004), with quality assessment (QA) checklists for quantitative papers (14 items) and for qualitative papers (10 items). These instruments resulted in a QA score for each paper with a possible range from 0 to 1, with 1 being the highest score. Studies were included regardless of their QA score, which is used to determine the risk of bias across studies and to differentiate between findings from low-quality and high-quality studies (with QAs below and above average, respectively).
The data extraction concerned the research method, sample size, response rate, descriptive information about the participants, definitions, and operationalizations of the concepts and research findings. The QA and data extraction were performed by two independent reviewers for 41.67% (n = 35) of the research papers, where disagreements were discussed until consensus was reached. The correlation between the QAs of the first author and the second reviewers was satisfactory (r = .61, p < .001) and the correlation between the first authors’ initial QA and the consensus decision was high (r = .89, p < .001). Therefore, it was considered appropriate to perform the risk assessment and data extraction of the remaining papers by the first author. The extracted data were entered into a spreadsheet and coded in ATLAS.ti to enable the narrative synthesis of results per research question. In the synthesis of results, we distinguished between findings based on quantitative or qualitative evidence. For mixed-methods studies, this categorization was based on the type of evidence about the research question presented.
Results
The search resulted in the identification of 6,525 unique records, of which 84 records matched the inclusion criteria. A PRISMA flow diagram of the identification and selection of records is given in Figure 2.
Figure 2.
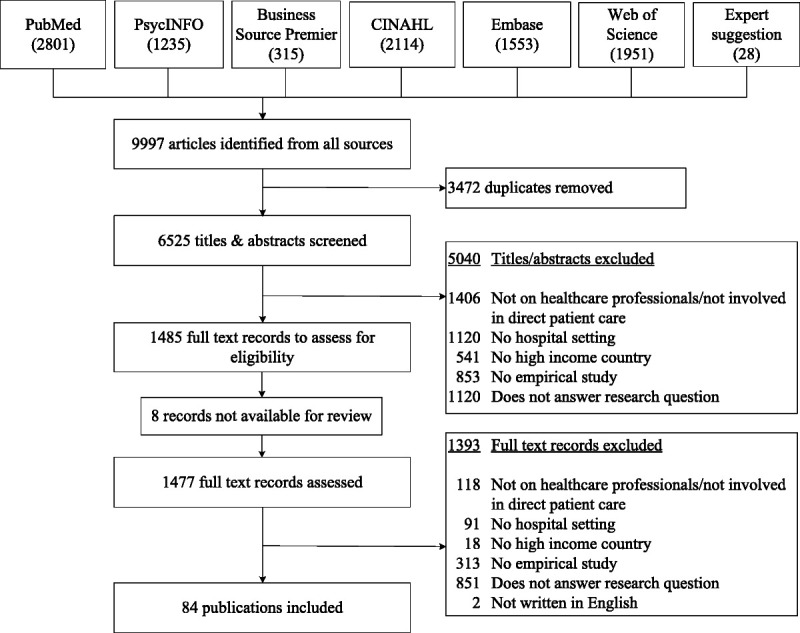
PRISMA flow diagram of the literature search
Study Characteristics and Risk of Bias
The included records on quantitative findings (n = 66) reported on four quasi-experimental studies, four time-lagged studies, four mixed-methods studies, six longitudinal studies, and 48 cross-sectional studies. Records reporting on qualitative findings (n = 18) reported on three case studies and 15 interview studies. Of all included studies, 46 focused exclusively on nurses, 13 focused exclusively on physicians, and 25 studies had participants from multiple professions, including nurses, physicians, paraprofessionals, and physician assistants. Together, the studies included over 102,500 health care professionals.
The QA resulted in an overall mean score of 0.70 (SD = 0.21), with MQAquantitative = 0.71 (SD = 0.19) and MQAqualitative = 0.70 (SD = 0.27). The QA across studies (available from the first author on request) demonstrated that a potential risk of bias of quantitative studies are the lack of control for confounding factors and the limited definition and/or operationalization of the concepts of interest. For qualitative studies, most frequently observed shortcomings were the lack of reflexivity, the ambiguity of the sampling strategy, and data collection and/or analysis.
Seventy-one of the studies reported on one of the research questions of this review, eight studies reported on two research questions, four studies reported on three research questions, and one study reported on all four research questions. An overview of the results is depicted in Table 1. For each research question, the findings based on quantitative evidence will be described first, followed by the qualitative findings, which deepen our understanding of the relationships of interest. In the conclusions for each research question, reflections are made upon the influence of the quality of the studies.
Table 1.
Overview of findings per research question (first author and year of publication of the reporting study)
| RQ | Investigated association | Positive association | Negative association | No association |
|---|---|---|---|---|
| 1 | Intrinsic motivation – safety | Toode, 2015 | Toode, 2015 | |
| Internal work motivation – patient centeredness | Papastavrou, 2015a; Suhonen, 2014a | |||
| Work engagement – quality | Freeney, 2013a; Lowe, 2012; Shantz, 2016a; Van Bogaert, 2014a; Wong, 2010a | |||
| Work engagement – patient centeredness | Lowe, 2012 | Rathert, 2009 | ||
| Work engagement – safety | Prins, 2009a; Shantz, 2016a | Rathert, 2009 | ||
| Psychological empowerment – quality | Leggat, 2010a; Purdy, 2010a | |||
| Psychological empowerment – effectiveness | Spence Laschinger, 2014 | |||
| Ownership – patient centeredness | Harwood, 2007 a | |||
| Autonomous motivation – patient centeredness | Redfern, 1999a; Schoenfeld, 2016a | Kosmala-Anderson, 2010 | ||
| Organizational commitment – quality | De Groot, 1998; Tsai, 2011a | Johnson, 2011a | ||
| Organizational commitment – effectiveness | Freund, 2007 | |||
| Organizational commitment – efficiency | McNeese-Smith, 1999 | |||
| Organizational commitment – patient centeredness | Rathert, 2009 | |||
| Organizational commitment – safety | Vogus, 2016a,b; Rathert, 2009 | |||
| Professional commitment – quality | De Groot, 1998; Teng, 2009b | Teng, 2009b | ||
| Professional commitment – safety | Teng, 2009 | |||
| Job commitment – effectiveness | Freund, 2007 | |||
| Identified regulation – safety | Leung, 2012a; Toode, 2015 | Toode, 2015 | ||
| Motivation – quality | Khatri, 2007; Hudelson, 2008a | |||
| Motivation – accessibility | Mason, 2013 | |||
| Motivation – safety | Khatri, 2007 | |||
| Introjected regulation – safety | Toode, 2015; Toode, 2015 | |||
| External regulation – patient centeredness | Schoenfeld, 2016 a | Kosmala-Anderson, 2010 | ||
| External regulation – safety | Leung, 2012 a | Toode, 2015; Toode, 2015 | ||
| Behavioral intention – equitability | Natan, 2009 | |||
| Amotivation – quality | Redfern, 1999 a | |||
| 2 | Work engagement – core task behavior | Gordon, 2015a; Gordon, 2015a; Rodwell, 2017a; Spence Laschinger, 2009a; Spence Laschinger, 2009a | ||
| Autonomous motivation – guideline use | Neo, 2013a; van de Steeg, 2014a | |||
| Affective commitment – core task behavior | Huang, 2012a | Somers, 2000b | ||
| Organizational commitment – core task behavior | Chu, 2011a; Hsu, 2011a | Johnson, 2011a Vandenberghe, 2004a,b |
||
| Goal internalization – core task behavior | Kang, 2012a,b | |||
| Importance – compliance | Simons, 2014b | Simons, 2014b | ||
| Motivation – guideline use | Lyles, 2014; Lyles, 2014; Smith, 2005 | |||
| Motivation – providing quality care | Hudelson, 2008 a | |||
| Commitment – guideline use | Tapper, 2014b | |||
| Supervisor commitment – core task behavior | Vandenberghe, 2004a,b | |||
| Work group commitment – core task behavior | Vandenberghe, 2004a,b | |||
| Normative commitment – core task behavior | Huang, 2012a | |||
| Continuance commitment – core task behavior | Huang, 2012a | Somers, 2000b | ||
| Controlled motivation – protocol use | Neo, 2013a; van de Steeg, 2014a | |||
| Behavioral intention – compliance | O’Boyle, 2001 | Maue, 2004; Maue, 2004b; O’Boyle, 2001b | ||
| 3 | Intrinsic motivation – OCB | Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013ba; Battistelli, 2013ba; Pohl, 2012a; Pohl, 2012a | ||
| Work engagement – extra role behavior or proactive behavior | Gordon, 2015a; Gordon, 2015a; Salanova, 2011a,b; Warshawsky, 2012a | |||
| Work engagement – OCB | Rodwell, 2017a; Rodwell, 2017a | |||
| Work engagement – voicing | Wong, 2010a | |||
| Psychological empowerment – empowered behavior | Montani, 2015a; Purdy, 2010a | |||
| Psychological empowerment – proactivity | Harwood, 2007a; Kuokkanen, 2001a | |||
| Ownership – quality improvement | Harvey, 1996 | |||
| Autonomous motivation – proactivity | Redfern, 1996a; Snell, 2011 | Van de Wiel, 2013a | ||
| Autonomous motivation – OCB | Galletta, 2012a; Galletta, 2012a | |||
| Autonomous motivation – voicing | Attree, 2007a; Brubacher, 2011; Schwappach, 2014a; Sur, 2016 | Flynn-O’Brien, 2015 | ||
| Affective commitment – OCB | Battistelli, 2013ba; Battistelli, 2013ba; Bolon, 1997b; Bolon, 1997b; Boselie, 2010a; Chênevert, 2015a; Galletta, 2012a; Galletta, 2012a; Huang, 2012a; Vogus, 2016a,b; Xerri, 2013a; Xerri, 2013a | Huang, 2012a | ||
| Affective commitment – innovative behavior | Xerri, 2013a | |||
| Organizational commitment – extra role behavior or proactive behavior | Gregersen, 1993a,b; Hsu, 2011a | Johnson, 2011a | ||
| Organizational commitment – OCB | Carson, 1998a; Chu, 2011a; Cohen, 1999; Lee, 2001a; Lee, 2001a; Lin, 2015 | Chu, 2005; Irvine, 2000a; Irvine, 2000a; Irvine, 2000a; Irvine, 2000a | ||
| Organizational commitment – quality improvement | Irvine, 2000a; Irvine, 2000a; Irvine, 2000a; Irvine, 2000a | |||
| Organizational identification – OCB | Bellou, 2006 | |||
| Importance – quality improvement | Lindgren, 2013 a | |||
| Goal internalization – extra role behavior | Kang, 2012a,b | |||
| Identified regulation – OCB | Battistelli, 2013ba | Battistelli, 2013ba | ||
| Job involvement – OCB | Cohen, 1999 | Chu, 2005 | ||
| Work involvement – OCB | Cohen, 1999 | |||
| Patient commitment – extra role behavior | Williams, 2007a | Gregersen, 1993a,b | ||
| Career/occupational commitment – OCB | Carson, 1998a; Lee, 2001a | Cohen, 1999 | Lee, 2001a | |
| Work group commitment – OCB | Gregersen, 1993a,b | Cohen, 1999 | ||
| Supervisor commitment – extra role behavior | Gregersen, 1993a,b | |||
| Management commitment – extra role behavior | Gregersen, 1993a,b | |||
| Introjected regulation – OCB | Battistelli, 2013ba | Battistelli, 2013ba | ||
| Normative commitment – OCB | Battistelli, 2013ba; Battistelli, 2013ba; Bolon, 1997b; Bolon, 1997b; Huang, 2012a; Huang, 2012a | |||
| Rewards – proactivity | Plost, 2007; Snell, 2011 | |||
| External regulation – OCB | Battistelli, 2013ba | Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013aa; Battistelli, 2013ba; Boselie, 2010a | ||
| Continuance commitment – OCB | Battistelli, 2013ba; Battistelli, 2013ba; Bolon, 1997b; Bolon, 1997b; Galletta, 2012a; Galletta, 2012a; Huang, 2012a; Huang, 2012a | |||
| Controlled motivation – voicing | Attree, 2007a; Brubacher, 2011; Schwappach, 2014a | Attree, 2007a; Brubacher, 2011; Flynn-O’Brien, 2015; Schwappach, 2014a; Sur, 2016 | ||
| Amotivation – voicing | Flynn-O’Brien, 2015; Brubacher, 2011; Sur, 2016 | |||
| 4 | Proactivity – quality | Johnson, 2011a; Redfern, 1999a,b | ||
| Proactivity – effectiveness | Campbell, 2008b | |||
| Proactivity – safety | Agnew, 2014a,b; Dearmon, 2013b; Redfern, 1999a | Dearmon, 2013b | Agnew, 2014a,b | |
| OCB – quality | D’Amato, 2008 | |||
| OCB – safety | Vogus, 2016a,b; Vogus, 2016a,b | |||
| Quality improvement – effectiveness | Ceballos, 2013e; Ogrinc, 2014a; Zimmerman, 2013 | Zimmerman, 2013 | Ceballos, 2013b; Zimmerman, 2013 | |
| Quality improvement – safety | Ceballos, 2013b; Ogrinc, 2014a | Ceballos, 2013b | ||
| Empowered behavior – quality | Purdy, 2010a | |||
| Voicing – quality | Wong, 2010a |
Note. Qualitative evidence is depicted in italics. RQ = research question; OCB = organizational citizenship behavior.
aHigh-quality study.
bExternally assessed outcome.
Each finding (positive, negative, or no association) about Research Questions 1–4 is depicted in Table 1 and papers reporting multiple research findings are represented multiple times. Full references to the included studies are given in Supplemental Digital Content 1 (http://links.lww.com/HCMR/A67). The full descriptions of the study characteristics and findings as depicted in Table 1 are available from the first author on request.
Motivation and Quality of Care
The first research question was investigated in 29 studies: 24 studies reported on quantitative evidence and 5 on qualitative evidence. The quantitative evidence showed that autonomous motivation, mostly investigated in terms of work engagement and empowerment, positively influenced overall perceptions of quality. Organizational commitment had mixed (positive and no) effects on perceived quality, and professional commitment was positively associated with three out of six patient-perceived quality indicators.
Autonomous motivation positively affected safety perceptions but had no association with the number of safety events. Work engagement was mostly positively associated with perceived safety, but one study reported no association. There was no effect of controlled motivation on perceived safety.
Autonomous motivation had mixed effects on perceived patient-centeredness, with some studies finding a positive association, one study finding no association and one study reporting a negative association. Controlled motivation was negatively associated with perceptions of patient-centeredness.
For the less investigated quality dimensions, behavioral intention was positively associated with perceptions of equitability. Autonomous motivation positively affected perceived effectiveness and efficiency of care. Furthermore, an otherwise unspecified sense of motivation was not associated with effectiveness, nor with accessibility of care.
The qualitative evidence also supported positive associations between autonomous motivation and perceptions of quality, safety, and patient-centeredness, whereas an absence of motivation was perceived to lead to poor quality of care. An interview study found that physicians’ motivation to provide patient-centered care results from a balance between autonomous reasons (values) and controlled reasons (their own agenda based on external factors such as resources and fear of uncertainty).
When merely considering the high-quality studies, there was a positive association between autonomous motivation and perceived quality and safety. Patient-centeredness was stimulated by a balance of autonomous and controlled motivation. The studies focusing on effectiveness, equitability, and efficiency perceptions and externally assessed quality were either of low quality or reported no effect. Therefore, the effect of motivation on these outcomes remains uncertain.
Motivation and Core Task Behavior
Of the 19 studies that reported on the second research question, quantitative evidence was presented in 15 studies, and four studies presented qualitative evidence. The quantitative findings were that autonomous motivation, most often investigated in terms of work engagement and organizational commitment, positively influenced self-reported core task behavior and guideline adherence. Mixed (positive and no) results were found for the relationship between autonomous motivation and externally assessed core task behavior. One study reported that the relationship between autonomous motivation and supervisor-assessed core task behavior was mediated by commitment to the supervisor. Whereas normative commitment had a positive association with core task behavior, continuance commitment had a negative association with core task behavior. Mixed effects were reported for behavioral intention and an otherwise unspecified sense of motivation in relationship to self-reported guideline adherence. Behavioral intention did not predict observed guideline adherence.
The qualitative evidence also supported positive associations between autonomous motivation and core task behaviors. Core task behavior was reported to result from a balance between autonomous and controlled motivation, in which controlled motivation contributed to as well as inhibited this type of behavior.
When merely considering the high-quality studies, autonomous motivation was positively associated with core task behavior. Moderately controlled motivation contributed to core task behavior, but motivation at the most controlled end of the continuum did not to contribute to and even inhibited core task behavior. As the studies on behavioral intention were of low quality, its effect remains unclear.
Motivation and Proactive Behavior
The third research question was investigated in 43 studies, of which 32 presented quantitative findings and 11 presented qualitative findings. The quantitative evidence generally showed a positive relationship between autonomous motivation and proactive behavior, but findings were mixed for identified regulation, involvement, and organizational commitment. Controlled motivation had no or a negative association with self-reported proactive behavior. Furthermore, controlled motivation, commitment to patients, and goal internalization did not affect externally assessed proactive behavior. For voicing behavior, it was found that, whereas autonomous motivation stimulated voicing behavior, this behavior was discouraged by extrinsic factors (e.g., colleagues’ approval and the fear of failure).
The qualitative findings supported the positive association between autonomous motivation and proactive behavior. Nevertheless, it was observed that even if health care professionals experience a sense of ownership or find quality improvement important, this autonomous motivation may exist without actual engagement in proactive behavior. Similar to the quantitative findings, autonomous and controlled reasons simultaneously stimulated proactive behavior, quality improvements, and voicing behavior. However, for voicing behavior, controlled motivation held the potential to overrule autonomous motivation to speak up, thereby preventing this type of behavior.
Overall, autonomous motivation was positively associated with proactive behaviors. The association between controlled motivation and proactive behavior was dependent on the type of proactive behavior; whereas controlled motivation, combined with autonomous motivation, stimulated quality improvements and possibly also proactivity, controlled motivation negatively affected voicing behavior. When merely considering the high-quality studies, the results do not change.
Proactive Behavior and Quality of Care
Of the 12 studies reporting on the fourth research question, nine reported on quantitative findings and three reported on qualitative findings. The quantitative results showed that proactive behavior positively influenced perceived quality and had mixed effects on externally assessed quality and safety. Proactive behavior even had a negative effect on safety when safety was operationalized in terms of a low number of reported incidents in the hospital system. Furthermore, although proactivity among nurses stimulated nurse compliance to screening, it had no influence on the actual effectiveness of care delivered by physicians. Regarding quality improvement projects, positive effects were found on care effectiveness and safety, except when the patients were vulnerable. Voicing behavior was not associated with quality perceptions.
The qualitative evidence resembled these findings. Patients as well as nurses perceive nurses’ proactivity as an indicator of high-quality care, and nurse-reported (but not externally assessed) proactivity was indeed associated with externally assessed safety outcomes. Furthermore, interventions to stimulate proactivity or quality improvements had generally positive effects on externally assessed safety and effectiveness, but when patients were vulnerable, quality improvements had less or no effect.
When merely considering the high-quality studies, there was a positive association between self-reported proactive behavior and self-reported quality. Proactive behavior had a positive association with externally assessed safety in terms of the absence of harm to patients, but it had no or even a negative association with externally assessed safety when this was operationalized as the number of incident reports. The studies reporting on externally assessed proactive behavior, voicing behavior, or evaluations of interventions were of low quality, which limits their reliability.
Discussion
This review highlights the importance of autonomous motivation for health care professionals’ behaviors and the quality of care. We show that autonomous motivation is directly and positively associated with quality, safety, and patient-centeredness, whereas controlled motivation and amotivation are negatively associated with quality.
In addition, the findings of this review provide nuanced insights on the role of controlled motivation and incentives. Moderately controlled motivation is positively associated with core task performance, as observed in the organizational literature. In contrast with findings from the field of organizational studies, which support a positive effect of external regulation on performance (Cerasoli et al., 2014), our findings show that motivation at the most controlled end of the continuum is not or negatively associated with health care professionals’ core task behaviors. This discrepancy might be due to differences between work motivation of health care professionals versus of employees from other types of organizations. In a study comparing the motivation of for-profit and not-for-profit employees (with the latter group including hospital employees as their organization has a social rather than a profit mission), not-for-profit employees had lower external regulations than employees working in organizations driven by monetary goals (De Cooman, De Gieter, Pepermans, & Jegers, 2011). Furthermore, studies among medical students indicate that they choose their profession out of intrinsic and identified motivation rather than extrinsic motivation (Berenson & Rice, 2015), and they maintain this high level of intrinsic motivation throughout their career (Berenson & Rice, 2015; Scheepers et al., 2015). Because of this high level of intrinsic motivation and low level of external regulation, health care professionals might not be very susceptible for extrinsic motivators. This would also provide an explanation for the finding that providing incentives does not stimulate proactive behaviors and quality improvement, unless this is combined with autonomous reasons to act. These observations challenge the emphasis on incentivizing (e.g., financial incentives) and penalizing (e.g., public reporting) as a means to extrinsically motivate health care professionals to improve quality and potentially explain why these methods have not reached their anticipated success (Berenson & Rice, 2015; Flodgren et al., 2011; Franco et al., 2002).
Furthermore, our review sheds further light on the role of proactive behavior in the health care setting. Our findings show that proactive behavior generally contributes to effectiveness, but only when the treatment is under the direct control of the proactive health care professional. In addition, proactive behavior contributes to safety, but not if safety is operationalized as the number of reported incidents. We argue that the number of reported incidents is probably not a valid measure of patient safety, which is confirmed by our finding that autonomous reasons contribute to voicing, but that this motivation can be overruled by controlled reasons to act, such as social reprimands. We state that the number of reported incidents reflects the safety culture or the learning potential of an organization; if there is a supportive safety culture, health care workers are more willing to act proactively and voice incidents (Ancarani, Di Mauro, & Giammanco, 2017). This could also explain the observed positive relationship between proactive behavior and reported incidents. Considering this point, we conclude that proactive behavior contributes to the quality and safety of care.
Practice Implications
The key policy priority to improve quality of care is to stimulate health care professionals’ autonomous work motivation. Although our review confirms that controlled motivation has its positive sides (Cerasoli et al., 2014), it negatively affects quality perceptions and voicing behavior. Therefore, current efforts to extrinsically motivate health care professionals to improve specific quality outcomes by incentivizing or penalizing need to be revised. It is recommended that these incentive-based interventions are complemented with aspects to simultaneously stimulate autonomous motivation, such as alignment with health care professionals’ drives and values, autonomy, supportive supervision, appreciation, respect and good interpersonal relationships, and growth opportunities (Berenson & Rice, 2015; Keyko et al., 2016).
Furthermore, as we observed that motivation based on normative considerations predicts core task behavior well, we suggest that, to increase compliance for specific core task behaviors, such as hand hygiene, one might want to appeal on health care professionals’ sense of professionalism; the internalized professional norms and values to act in the interest of the patient. Health care leaders can set the norm by engaging in exemplary behaviors (Ancarani et al., 2017; Berenson & Rice, 2015; Franco et al., 2002).
The next recommendation is to facilitate health care professionals’ proactive behaviors. In uncertain contexts, systems awareness, organizational learning, and continuous quality improvement are essential, and acting proactively is “part of the job” (Griffin et al., as cited in Gagné, 2014; Hollnagel et al., 2015). It is increasingly recognized that establishing quality and safety is no longer merely “avoiding that something goes wrong,” rather, it is “ensuring that as many things as possible go right” (Hollnagel et al., 2015) by acting proactively and raising concerns. In line with this thinking, we state that, to unleash the learning potential of health care organizations and to improve the quality of care, proactive behavior needs to be recognized as a fundamental part of health care professionals’ job requirements and needs to be appreciated and facilitated accordingly, for example, by allocating resources (e.g., time, equipment, training) for quality improvements, normalizing voicing behavior, and establishing a shame- and blame-free environment for raising concerns, learning, and improvement (Ancarani et al., 2017).
This review focused on the hospital setting, and our recommendations might apply beyond this setting as well. Care provision takes place within the clinical microsystem (the team of health care professionals caring for a patient; Fulop & Ramsay, 2019), and as these can be found in several settings such as primary care clinics, mental health care, and chronic care, we assume that our findings and recommendations translate to those settings as well. However, the extent to which our research translates to other health care systems outside high-income countries may be limited, as Fritzen (2007) stated that in low- and middle-income countries, there is “often a disjunction between formal responsibilities and the requisite resources to meet minimum specific standards.” In other words, the availability of resources, which varies per system, affects the extent to which health care professionals are able to act upon their motivation to provide and improve care.
It is important to note that achieving high-quality provision in hospitals is complex and influenced by intertwined factors from the organizational context and the broader environmental context. These factors include organizational characteristics (e.g., size, scale, structure, information systems, leadership, and culture) and broader environmental characteristics such as governance, regulation, and finance of the health care system (Fulop & Ramsay, 2019). These factors should be aligned to provide health care workers with the resources, including autonomous motivation, for high-quality care delivery.
Limitations and Future Research
The results of this review need be interpreted in consideration of its limitations. First, the alignment of the motivational concepts along the self-determination theory continuum may reflect an overly simplistic view of these concepts, and the list of aligned concepts might not have been exhaustive. The generalizability of this approach may therefore be limited when investigating other, but related, concepts (e.g., altruism). In addition, some studies may have been overlooked due to publication bias, not incorporating gray literature and because the search string was not exhaustive. Furthermore, we observed a suboptimal interrater agreement regarding the inclusion of the studies, which we resolved by performing the screening of all abstracts and full-text records by two independent reviewers. Future researchers might prevent this issue by stating the inclusion and exclusion criteria more explicitly, especially for ambiguously described studies (e.g., include, unless it is completely clear that an exclusion criterion applies). In addition, the extensive QA, which included questions concerning the risk of bias, may not have completely eliminated the potential influence of bias. Regarding all research questions, it is noted that most studies use self-reported measures of behavior or quality, and therefore, the evidence for the effect of motivation on externally assessed behavior and quality is limited. Finally, most studies based their conclusions on correlations or regression analyses. In the absence of sufficient longitudinal or (quasi-)experimental studies, we cannot unambiguously determine the causality of the relationships we studied.
These limitations should be addressed in future work, as well as the following recommendations. This review shows that autonomous and controlled motivation might influence behavior simultaneously. Building on studies about motivational or commitment profiles (e.g., Gagné, 2014), future (quasi-)experimental studies might aim at getting a better understanding of the “right” balance between extrinsic rewards and autonomous motivation for the provision of high-quality care. To conclude, it is strongly recommended that future studies incorporate objective and valid measures to study health care professionals’ motivation, behaviors, and the (externally assessed) quality of care dimensions.
Conclusion
To improve quality of care, policy makers and managers need to support health care professionals’ autonomously motivation and facilitate them to act proactively and “go the extra mile” for their patients. Combining autonomous and controlled motivation holds the potential to boost quality of care, but more insight is needed into how to balance these types of motivation in such a way that it does not thwart voicing behaviors.
Supplementary Material
Acknowledgments
We would like to express our gratitude to our student assistants Rick Overwijk and Marcel Schmidt for their help in the screening phases of this review. We are thankful to Helena VonVille for providing us with the Excel workbooks and advise. We are grateful to the University Medical Center Groningen and the University of Groningen as the submitted work was undertaken as part of a PhD program funded by these two institutions.
Footnotes
The authors have disclosed that they have no significant relationship with, or financial interest in, any commercial companies pertaining to this article.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s web site (www.hcmrjournal.com).
Contributor Information
Kirsten F. A. A. Dabekaussen, Email: k.f.a.a.dabekaussen@umcg.nl.
Eric Molleman, Email: h.b.m.molleman@rug.nl.
Erik Heineman, Email: e.heineman@umcg.nl.
Gera A. Welker, Email: g.a.welker@umcg.nl.
References
- Ajzen I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. [Google Scholar]
- Ancarani A. Di Mauro C., & Giammanco M. (2017). Hospital safety climate and safety behavior: A social exchange perspective. Health Care Management Review, 42(4), 341–351. [DOI] [PubMed] [Google Scholar]
- Berenson R. A., & Rice T. (2015). Beyond measurement and reward: Methods of motivating quality improvement and accountability. Health Services Research, 50, 2155–2186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerasoli C. P. Nicklin J. M., & Ford M. T. (2014). Intrinsic motivation and extrinsic incentives jointly predict performance: A 40-year meta-analysis. Psychological Bulletin, 140(4), 980–1008. 10.1037/a0035661 [DOI] [PubMed] [Google Scholar]
- De Cooman R. De Gieter S. Pepermans R., & Jegers M. (2011). A cross-sector comparison of motivation-related concepts in for-profit and not-for-profit service organizations. Nonprofit and Voluntary Sector Quarterly, 40(2), 296–317. [Google Scholar]
- Flodgren G. Eccles M. P. Shepperd S. Scott A. Parmelli E., & Beyer F. R. (2011). An overview of reviews evaluating the effectiveness of financial incentives in changing healthcare professional behaviours and patient outcomes. The Cochrane Database of Systematic Reviews, 7. 10.1002/14651858.CD009255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franco L. M. Bennett S., & Kanfer R. (2002). Health sector reform and public sector health worker motivation: A conceptual framework. Social Science & Medicine, 54(8), 1255–1266. [DOI] [PubMed] [Google Scholar]
- Fritzen S. A. (2007). Strategic management of the health workforce in developing countries: What have we learned? Human Resources for Health, 5(1), 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fulop N. J., & Ramsay A. I. G. (2019). How organisations contribute to improving the quality of healthcare. BMJ, 365, l1773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gagné M. (Ed.) (2014). The Oxford handbook of work engagement, motivation, and self-determination theory. New York, NY: Oxford University Press. [Google Scholar]
- Greenhalgh T. Howick J., & Maskrey N. (2014). Evidence based medicine: A movement in crisis? BMJ, 348, g3725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harden A. (2010). Mixed-methods systematic reviews: Integrating quantitative and qualitative findings. Focus, 2010(25), 1–8. [Google Scholar]
- Hollnagel E. Wears R. L., & Braithwaite J. (2015). From safety-I to safety-II: A white paper. The resilient health care net. Published simultaneously by the University of Southern Denmark, University of Florida, and Macquarie University. [DOI] [PubMed]
- Keyko K. Cummings G. G. Yonge O., & Wong C. A. (2016). Work engagement in professional nursing practice: A systematic review. International Journal of Nursing Studies, 61, 142–164. [DOI] [PubMed] [Google Scholar]
- Kim W. Kolb J. A., & Kim T. (2013). The relationship between work engagement and performance: A review of empirical literature and a proposed research agenda. Human Resource Development Review, 12(3), 248–276. [Google Scholar]
- Kmet L. M. Cook L. S., & Lee R. C. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton, Canada: Alberta Heritage Foundation for Medical Research. [Google Scholar]
- Scheepers R. A. Boerebach B. C. Arah O. A. Heineman M. J., & Lombarts K. M. (2015). A systematic review of the impact of physicians’ occupational well-being on the quality of patient care. International Journal of Behavioral Medicine, 22(6), 683–698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The World Bank Group . (2016). World bank list of economies (July 2016). Retrieved from https://siteresources.worldbank.org
- Van Dyne L., & Pierce J. (2004). Psychological ownership and feelings of possession: Three field studies predicting employee attitudes and organizational citizenship behavior. Journal of Organizational Behavior, 25(4), 439–459. 10.1002/job.249 [DOI] [Google Scholar]
- World Health Organization . (2006). Quality of care: A process for making strategic choices in health systems. Retrieved from http://www.who.int
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.