

Abstract
This case report describes the treatment of a case involving a skeletal Class II facial profile with a gummy smile. While treating a facial profile and a gummy smile, the outcome may not always be successful with orthodontic therapy alone. For this reason, surgical therapy is often chosen to gain an esthetic facial profile and a good smile. However, sometimes the patients reject surgical treatment and an alternative method must be considered. Skeletal anchorage systems such as miniscrews are now frequently used for correcting severe malocclusion that should be treated by surgical therapy. In this case report, we treated a skeletal Class II malocclusion with a convex profile and a gummy smile using miniscrews, which were placed in the upper posterior and anterior areas. The active treatment period was 3.5 years, and the patient's teeth continued to be stable after a retention period of 36 months.
Keywords: Gummy smile, Miniscrew, Facial profile
INTRODUCTION
Gummy smile is an esthetic problem for some patients and a frequent finding that can occur as a result of various intraoral or extraoral etiologies.1–5 Thus, proper diagnosis and treatment are important. If a gummy smile is characterized by overgrowth of anterior vertical maxillary excess, the outcome may not always be successful with conventional orthodontic therapy alone. In such cases, surgical therapy, such as that provided by a Le Fort impaction or maxillary gingivectomies, are often chosen to gain a good smile.6 However, if the patients are unwilling to undergo surgical treatment, an alternative method must be considered to treat the gummy smile. Miniplates7–10 and miniscrews11–16 are now frequently used for establishing absolute anchorage for orthodontic tooth movement. Surgical invasion is minimal during miniscrew insertion, compared to that associated with placement of miniplates, because mucosa should be cut and a flap is required. In this case report, we present the management of gummy smile and facial profile with skeletal Class II patients using miniscrew anchorage.
CASE REPORT
Pretreatment Evaluation
The patient, a female (age: 31 years 1 month), complained of a gummy smile. We had previously recommended orthodontic treatment with orthognathic surgery. However, the patient was not willing to undergo the surgery. The pretreatment facial photographs showed a convex profile, an acute nasolabial angle, hypermentalis activity with closed lips (Figure 1), and excessive gingival display in smiling (Figure 2). The intraoral photographs and dental casts revealed a 4.0-mm overjet and a 2.5-mm overbite. The right molar relationship was Class I and the left was full Class II; there was a little crowding in both arches. The lower dental midline coincided with the facial midline, but the upper midline was shifted to the right by 2 mm (Figure 3). A panoramic radiograph showed the existence of upper right third molars (Figure 4). As shown in the cephalometric measurements, a skeletal Class II relationship (ANB angle, 6.6°) with labial inclination of lower incisors (IMPA, 109.2°) was evident (Table 1). Based on this information, the patient was diagnosed with a skeletal Class II maxillary protrusion with a gummy smile.
Figure 1.

Pretreatment facial photographs.
Figure 2.
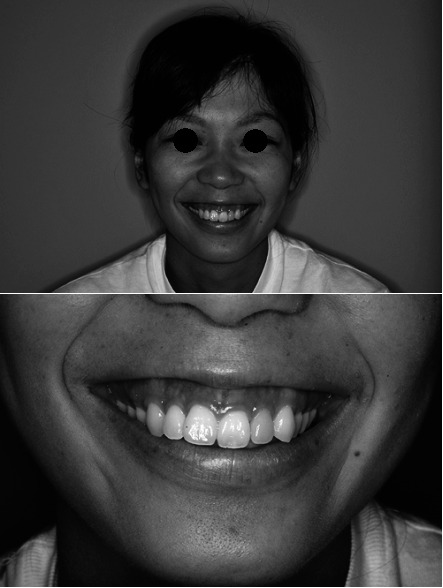
Excessive gingival display before treatment.
Figure 3.

Pretreatment intraoral photographs.
Figure 4.
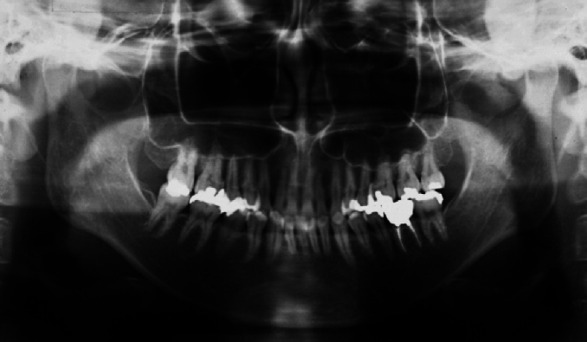
Pretreatment panoramic radiograph.
Table 1.
Summary of Cephalometric Measurements

Treatment Plan
The treatment options were discussed with the patient. The first option was traditional orthodontic treatment with Le Fort I surgery to reduce the gingival exposure and to correct maxillary protrusion. The second option involved orthodontic intrusion of the maxillary anterior region using miniscrew anchorage. Because the surgical treatment plan was declined by the patient, the treatment objectives essentially consisted of vertical control and distalization of the anterior teeth. The treatment plan involved the following steps:
Extraction of all second premolars;
Insertion of miniscrews into the buccal alveolar bone of the mesial part of the first molars;
Distal movement of the upper anterior teeth;
Extraction of the upper left second molar; and
Intrusion of the upper anterior teeth by miniscrews, which were placed above the root apices between the upper lateral incisors and canines.
Treatment Progress
Under local anesthesia, two self-drilling titanium alloy miniscrews (1.6 mm in diameter and 8 mm in length; Dual Top Auto Screw, Jeil Medical Corp, Seoul, South Korea) were inserted into the buccal alveolar bone between the upper and lower first molars and second premolars. Next, all the upper and lower second premolars were extracted, and 0.018-inch standard edgewise brackets were bonded on the upper and lower teeth. The upper first premolars were moved distally from the miniscrews with the use of elastic chain.
The lower first premolars were also distalized from the first molars (Figure 5). After 16 months, the upper left second molar was extracted and distalization of first molar began. The upper left first molar was distalized by an open coil spring from the first premolar, which was connected tightly with a miniscrew (Figure 6). After the upper left molar was distalized into a Class I relationship, retraction of the maxillary anterior teeth began. Anterior teeth retraction was carefully conducted using miniscrews to maintain the molar Class I relationship. Then, the intrusion of anterior teeth began with placement of miniscrews (1.6 mm in diameter and 8 mm in length) in the maxillary bone above the root apices between the upper lateral incisors and canines, as follows (Figure 7). Local anesthesia was administered with approximately 1.0 mL of lidocaine near the apices of the anterior teeth. The mucosa was cut and exposed bone surface and miniscrews were inserted into the maxillary bone. An 0.018-inch wire that was connected at the miniscrew head was exposed from the suture region, and the flap was closed (Figure 8). After miniscrew insertion, 50 g of intrusive force was applied from each miniscrew to the upper lateral incisors (Figure 9).
Figure 5.

Retraction of first premolars by miniscrew anchorage.
Figure 6.
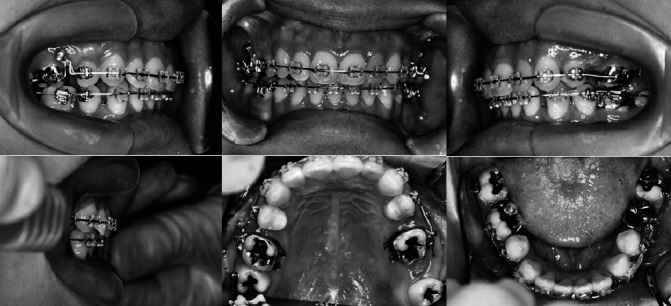
Distalization of the upper left first molar by open coil spring from first premolar, which was connected tightly with a miniscrew (upper left second molar was removed).
Figure 7.
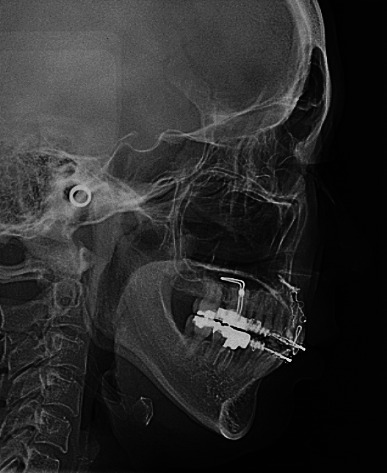
Placement of miniscrews in the maxillary bone above the root apices.
Figure 8.
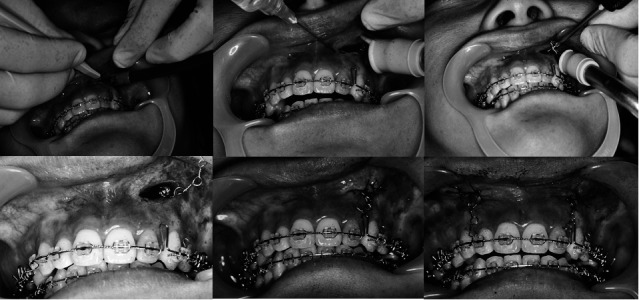
Surgical procedure for miniscrew insertion in the maxillary bone.
Figure 9.
Intrusion of upper incisors with direct miniscrew anchorage.
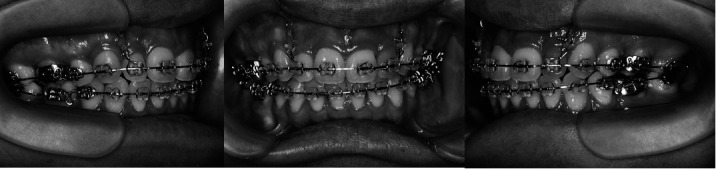
After 12 months of anterior teeth intrusion, the patient's gummy smile and overjet were fully corrected. The teeth were well aligned with a good intercuspal relation (Figure 10). The total treatment period with the fixed appliance was 3.5 years. After edgewise brackets, lingual bonded retainers were set on both the upper and lower arches between the premolars. The anterior miniscrews were left in place, and we combined them with a clear retainer at night during retention for 16 months (Figure 11), then the miniscrews were removed. The position of the teeth continued to be stable 36 months from the beginning of the retention.
Figure 10.

Posttreatment intraoral photographs.
Figure 11.

A clear retainer combined with the anterior miniscrews.
Treatment Results
A normal overjet and overbite were achieved and the upper and lower midlines coincided. The upper and lower dental arches were well aligned, and a Class I molar relationship was achieved. The strain of the mentalis muscle became more relaxed. The facial profile was significantly improved (Figure 12). The posttreatment panoramic radiograph showed that the all of the roots were parallel, and severe root resorption was not observed (Figure 13). On the cephalometric superimposition (pretreatment and posttreatment), the upper anterior teeth and the left first molar were distalized 5 mm (Figure 14). The anterior teeth also showed a 4-mm intrusion. IMPA changed from 109.2° to 92.5°. The ANB angle changed from 6.6° to 5.8°, and the Z-angle also changed from 56.5° to 70.0° (Table 1). Posttreatment facial smile photographs are shown in Figure 15. Gingival exposure posttreatment was dramatically reduced as a result of intrusion of the anterior teeth, and the patient obtained a good smile.
Figure 12.

Posttreatment facial photographs.
Figure 13.

Posttreatment panoramic radiograph.
Figure 14.
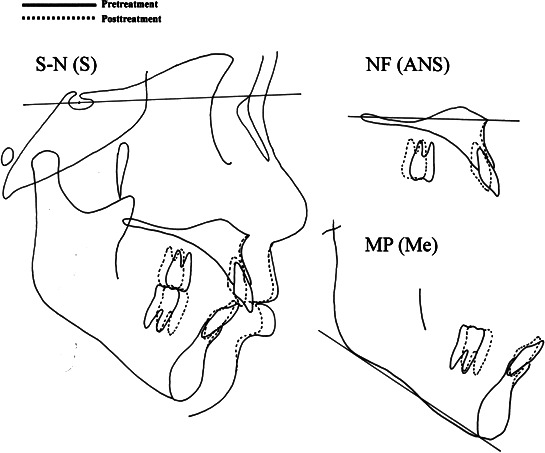
Cephalometric superimposition (pretreatment and posttreatment).
Figure 15.

Posttreatment facial smile photographs.
DISCUSSION
Excessive gingival display can be divided into several categories according to etiologic factors.17,18 Dentoalveolar excessive gingival display occurs by overgrowth of the maxillary anterior dentoalveolar heights, but it is difficult to intrude anterior sections with a normal orthodontic device. For this reason, surgical impaction of the maxillary anterior dentoalveolar region is often applied in severe gummy smile cases.19 However, surgical correction carries potential risks associated with infection, alveolar bone necrosis, and loss of tooth vitality. Moreover, since impaction of the anterior segment by Le Fort I tends to increase nasal alar width, which makes the patient's nasal profile worse, we have to decide carefully whether we will apply surgical or nonsurgical treatment.
On the other hand, implants for orthodontic anchorage, such as miniplates7–10 and miniscrews,11–16 have recently been developed. Creekmore and Eklund20 and Ohnishi et al.21 proposed the placement of a single miniscrew between the roots of the maxillary incisors, providing direct anchorage for incisor intrusion to reduce excessive gingival display. Our patient had a dentoalveolar gummy smile and the posterior teeth were in normal vertical positions. In this category, gummy smile can be corrected efficiently by intrusion of maxillary incisors. Therefore, we planned to intrude the upper incisors with miniscrews, which could provide a desirable improvement of the smile. Generally, miniscrews for intrusion of incisors are placed between the roots of the anterior teeth. In this case, we inserted the miniscrews in the maxillary bone above the root apices because the patient had sufficient space for miniscrew placement superior to the incisor apices. Miniscrew placement superior to the incisor apices has some advantages. It does not hurt the root of tooth, and it is more effective because the distance to the incisors is greater than the distance between the roots.
In the present case, we had to correct the overjet and the left molar relationship as well as the facial profile. So we also placed the miniscrews between the second premolar and first molar roots for indirect anchorage application. Because the left molar relationship was full Class II, the left second molar was removed and the first molar was distalized using a miniscrew. As a result, the patient's profile, overjet, and molar relationship were improved.
Miniscrews have many advantages in orthodontic treatment: patient cooperation is not needed to achieve maximum anchorage; the orthodontic treatment period can be shortened; undesirable side effects are avoided; and miniscrews can be inserted more easily and with less surgical damage than can miniplates. However, the long-term stability of tooth intrusion with miniscrews has not been thoroughly investigated. A 30% relapse rate for upper incisor intrusion by miniscrews was reported14 14 months after treatment.14 Baek et al.22 examined the long-term stability of anterior open-bite correction with intrusion of the maxillary posterior teeth. They showed that the maxillary first molars were intruded by 2.39 mm during treatment and erupted by 0.45 mm at the 3-year follow-up. Eighty percent of the total relapse of the intruded maxillary first molars occurred during the first year of retention. Lee and Park23 used miniscrews to intrude the maxillary molars and reported a 10.36% relapse rate for the intruded molars at 1 year posttreatment. Taken together, if an effective retention method is applied during the first year of retention, we could prevent the relapse and improve the long-term stability of the treatment. However, an effective method of retention after tooth intrusion has not been introduced. Hawley appliances can enhance the stability of orthodontic treatments, but they are inadequate for preventing relapse of intruded teeth.24 So, in this case, the anterior miniscrews were left and we combined them with a clear retainer at night during retention for 16 months to retain intruded incisors. Although the patient's teeth continued to be stable after a retention period of 36 months, periodic checkups and thorough examinations will be necessary in the future.
CONCLUSIONS
Severe gummy smile can be treated with miniscrews through intrusion of the upper incisors.
The patient's profile can be improved by correction of overjet using miniscrews.
A clear retainer attached to the anterior miniscrews is effective in preventing the eruption of intruded incisors.
Acknowledgments
We wish to thank Mrs K. Ohgushi and H. Setogawa (Pro-Seed Corp, Tokyo, Japan) for valuable information and suggestions. We also thank Dr K. Ueki for technical assistance.
REFERENCES
- 1.Peck S, Peck L, Kataja M. Some vertical lineaments of lip position. Am J Orthod. 1992;101:519–524. doi: 10.1016/0889-5406(92)70126-U. [DOI] [PubMed] [Google Scholar]
- 2.Hunt O, Johnston C, Hepper P, Burden D, Stevenson M. The influence of maxillary gingival exposure on dental attractiveness ratings. Eur J Orthod. 2002;24:199–204. doi: 10.1093/ejo/24.2.199. [DOI] [PubMed] [Google Scholar]
- 3.Garber D. A, Salama M. A. The aesthetic smile: diagnosis and treatment. Periodontol 2000. 1996;11:18–28. doi: 10.1111/j.1600-0757.1996.tb00179.x. [DOI] [PubMed] [Google Scholar]
- 4.Redlich M, Mazor Z, Brezniak N. Severe high Angle Class II Division 1 malocclusion with vertical maxillary excess and gummy smile: a case report. Am J Orthod. 1999;116:317–320. doi: 10.1016/s0889-5406(99)70243-x. [DOI] [PubMed] [Google Scholar]
- 5.Polo M. Botulinum toxin type A in the treatment of excessive gingival display. Am J Orthod. 2005;127:214–218. doi: 10.1016/j.ajodo.2004.09.013. [DOI] [PubMed] [Google Scholar]
- 6.Capelozza F. L, Cardoso M. A, Reis S. A. B, Mazzottini R. Surgical-orthodontic correction of long-face syndrome. J Clin Orthod. 2006;40:323–332. [PubMed] [Google Scholar]
- 7.Sugawara J, Daimaruya T, Umemori M, Nagasaka H, Takahashi I, Kawamura H, Mitani H. Distal movement of mandibular molars in adult patients with skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004;125:130–138. doi: 10.1016/j.ajodo.2003.02.003. [DOI] [PubMed] [Google Scholar]
- 8.Umemori M, Sugawara J, Mitani H. Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop. 1999;115:166–174. doi: 10.1016/S0889-5406(99)70345-8. [DOI] [PubMed] [Google Scholar]
- 9.Erverdi N, Keles A, Nanda R. The use of skeletal anchorage in open bite treatment: a cephalometric evaluation. Angle Orthod. 2004;74:381–390. doi: 10.1043/0003-3219(2004)074<0381:TUOSAI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Sherwood K. H, Burch J. G, Thompson W. J. Closing anterior open bites by intruding molars with titanium miniplate anchorage. Am J Orthod Dentofacial Orthop. 2002;122:593–600. doi: 10.1067/mod.2002.128641. [DOI] [PubMed] [Google Scholar]
- 11.Costa A, Raffaini M, Melsen B. Miniscrews as orthodontic anchorage: a preliminary report. Int J Adult Orthod Orthognath Surg. 1998;13:201–209. [PubMed] [Google Scholar]
- 12.Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod. 1997;31:763–767. [PubMed] [Google Scholar]
- 13.Park H. S, Bae S. M, Kyung H. M, Sung J. H. Micro-implant anchorage for treatment of skeletal Class 1 bialveolar protrusion. J Clin Orthod. 2001;35:417–422. [PubMed] [Google Scholar]
- 14.Paik C. H, Woo Y. J, Boyd R. Treatment of an adult patient with vertical maxillary excess using miniscrew fixation. J Clin Orthod. 2003;37:423–428. [PubMed] [Google Scholar]
- 15.Xun C. L, Zeng X. L, Wang X. Clinical application of miniscrew implant for maximum anchorage treatment. Chin J Stomatol. 2004;39:505–508. [PubMed] [Google Scholar]
- 16.Xun C. L, Zeng X. L, Wang X. Clinical application of miniscrew implant anchorage for anterior teeth intrusion treatment. Chin J Orthod. 2004;11:29–32. [Google Scholar]
- 17.Monaco A, Streni O, Marci M. C, Marzo G, Gatto R, Giannoni M. Gummy smile: clinical parameters useful for diagnosis and therapeutic approach. J Clin Pediatr Dent. 2004;29:19–25. doi: 10.17796/jcpd.29.1.y01l3r4m06q3k2x0. [DOI] [PubMed] [Google Scholar]
- 18.Robbins J. Differential diagnosis and treatment of excess gingival display. Pract Periodontics Aesthet Dent. 1999;11:265–272. [PubMed] [Google Scholar]
- 19.Ataoglu H, Uckan S, Karaman A. I, Uyar Y. Bimaxillary orthognathic surgery in a patient with long face: a case report. Int J Adult Orthod Orthognath Surg. 1999;14:304–309. [PubMed] [Google Scholar]
- 20.Creekmore T. M, Eklund M. K. The possibility of skeletal anchorage. J Clin Orthod. 1983;17:266–269. [PubMed] [Google Scholar]
- 21.Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini-implant for orthodontic anchorage in a deep overbite case. Angle Orthod. 2005;75:444–452. doi: 10.1043/0003-3219(2005)75[444:AMFOAI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Baek M. S, Choi Y. J, Yu H. S, Lee K. J, Kwak J, Park Y. C. Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. 2010;138:396.e1–396.e9. doi: 10.1016/j.ajodo.2010.04.023. [DOI] [PubMed] [Google Scholar]
- 23.Lee H. A, Park Y. C. Treatment and posttreatment changes following intrusion of maxillary posterior teeth with miniscrew implants for open bite correction. Korean J Orthod. 2008;38:31–40. [Google Scholar]
- 24.Beckmann S. H, Segner D. Floating norms and post-treatment overbite in open bite patients. Eur J Orthod. 2002;24:379–390. doi: 10.1093/ejo/24.4.379. [DOI] [PubMed] [Google Scholar]