

Abstract
Background
Injuries are a significant public health burden and alcohol intoxication is recognised as a risk factor for injuries. Increasing attention is being paid to supply‐side interventions that aim to modify the environment and context within which alcohol is supplied and consumed.
Objectives
To quantify the effectiveness of interventions implemented in the server setting for reducing injuries.
Search methods
We searched the following electronic databases to November 2008; Cochrane Injuries Group's Specialised Register, CENTRAL, MEDLINE, EMBASE, PsycINFO, PsycEXTRA, ISI Web of Science, Conference Proceedings Citation Index ‐ Science, TRANSPORT and ETOH. We also searched reference lists of articles and contacted experts in the field.
Selection criteria
Randomised controlled trials (RCTs), non‐randomised controlled trials (NRTs) and controlled before and after studies (CBAs) of the effects of interventions administered in the server setting that attempted to modify the conditions under which alcohol is served and consumed, to facilitate sensible alcohol consumption and reduce the occurrence of alcohol‐related harm.
Data collection and analysis
Two authors independently screened search results and assessed the full texts of potentially relevant studies for inclusion. Data were extracted and methodological quality was examined. Due to variability in the types of interventions investigated, a pooled analysis was not appropriate.
Main results
Twenty‐three studies met the inclusion criteria. Overall methodological quality was poor. Five studies used an injury outcome measure; one of these studies was randomised, the remaining four where CBA studies.
The RCT targeting the alcohol server setting environment with an injury outcome compared the introduction of toughened glassware (experimental) to annealed glassware (control) on the number of bar staff injuries; a greater number of injuries were detected in the experimental group (relative risk 1.72, 95% CI 1.15 to 2.59).
One CBA study investigated server training and estimated a reduction of 23% in single‐vehicle, night‐time crashes in the experimental area (controlled for crashes in the control area). Another CBA study examined the impact of a drink driving service, and reported a reduction in injury road crashes of 15% in the experimental area, with no change in the control; no difference was found for fatal crashes. In a CBA study investigating the impact of an intervention aiming to reduce crime in drinking premises, the study authors found a lower rate of all crime in the experimental premises (rate ratio 4.6, 95% CI 1.7 to 12, P = 0.01); no difference was found for injury (rate ratio 1.1 95% CI 0.1 to 10, P = 0.093). A CBA study investigating the impact of a policy intervention reported that pre‐intervention the serious assault rate in the experimental area was 52% higher than the rate in the control area. After intervention, the serious assault rate in the experimental area was 37% lower than in the control area.
The effects of such interventions on patron alcohol consumption is inconclusive. One randomised trial found a statistically significant reduction in observed severe aggression exhibited by patrons. There is some indication of improved server behaviour but it is difficult to predict what effect this might have on injury risk.
Authors' conclusions
There is insufficient evidence from randomised controlled trials and well conducted controlled before and after studies to determine the effect of interventions administered in the alcohol server setting on injuries. Compliance with interventions appears to be a problem; hence mandated interventions may be more likely to show an effect. Randomised controlled trials, with adequate allocation concealment and blinding are required to improve the evidence base. Further well‐conducted, non‐randomised trials are also needed when random allocation is not feasible.
Plain language summary
Are interventions that are implemented in alcohol server settings (e.g. bars and pubs) effective for preventing injuries?
Injuries are a significant public health burden and alcohol intoxication (i.e. drunkenness) is recognised as a risk factor for injuries; indeed the effects of alcohol lead to a considerable proportion of all injuries. Alcohol‐associated injuries are a problem in both high‐ and low‐income countries.
Many interventions to reduce alcohol‐related injuries have a demand‐side focus and aim to reduce individuals' demand and consequently consumption of alcohol. However, there is increasing attention on supply‐side interventions, which attempt to alter the environment and context within which alcohol is supplied and consumed; the aim being to modify the drinking and/or the drinking environment so that potential harm is minimised.
This systematic review was conducted to examine the evidence for the effectiveness of interventions implemented in the alcohol server setting for reducing injuries. The authors of this systematic review examined all studies that compared server settings which received an intervention aimed at facilitating sensible alcohol consumption and/or preventing injuries, to server settings which did not receive such an intervention.
The authors found 23 studies; only five of these measured the effect on injury, the remaining 18 measured the effect on behaviour (by the patrons and/or the servers of the alcohol within the premises). The studies investigated a range of interventions involving server training, health promotion initiatives, a drink driving service, a policy intervention and interventions that targeted the server setting environment.
The authors concluded that there is insufficient high quality evidence that interventions in the alcohol server setting are effective in preventing injuries. The evidence for the effectiveness of the interventions on patron alcohol consumption was found to be inconclusive. There is conflicting evidence as to whether server behaviour is improved and it is difficult to predict what effect this might have on actual injury risk.
Lack of compliance with interventions seems to be a particular problem; hence mandated interventions or those with associated incentives for compliance, may be more likely to show an effect. The methodology of future evaluations needs to be improved. The focus of research should be broadened to investigate the effectiveness of interventions other than server training, where previous research dominates. When the collection of injury outcome data is not feasible, research is needed to identify the most useful proxy indicators.
Background
Description of the condition
Injuries are a significant global public health burden. During the year 2000, it is estimated that five million people worldwide died from injuries. Globally they account for 9% of deaths and 12% of the burden of disease (Peden 2002a). This burden is predicted to worsen; by 2020 it is estimated that deaths from injuries will increase to 8.4 million per year (Murray 1997a). Injuries rank among the leading causes of mortality and burden of disease in all regions, affecting people of all ages and income groups (Peden 2002b).
Injuries can be caused by a number of factors, alcohol being just one. Hence, when considering the public health burden, it is useful to refer to the proportion of all injuries that can be attributed to alcohol. The 'attributable fraction' represents the extent to which injury rates would fall if alcohol use was eliminated. By conducting a meta‐analysis of epidemiological research (primarily case‐control and case‐series studies) English et al (English 1996) estimated the alcohol‐attributable fractions for a range of disorders. Britton 2001 used the figures from English 1996 and estimated that for England & Wales in 1996, alcohol was responsible for: approximately 75,000 of premature life years lost, 99 of 210 (47%) deaths from assaults, 66 of 174 (38%) deaths from accidental drowning, 1176 of 3616 (33%) deaths from accidental falls, 178 of 405 (44%) deaths from fire‐related injuries, 758 of 2948 (26%) deaths from motor vehicle crashes, and 997 of 3442 (29%) suicides. However, it should be noted that all estimates of attributable fractions assume causality and can only be as accurate as the studies upon which they are based. The influence of bias, such as confounding, may lead to less accurate estimates and should be considered. Nevertheless, alcohol can be considered to cause a considerable proportion of all injuries.
Evidence that alcohol consumption has some beneficial health effects complicates public health policy in this area. Research has indicated that alcohol, consumed in moderation, is protective against coronary heart disease (CHD) and ischaemic stroke, particularly in the middle‐aged and elderly population (Britton 2001). Injuries resulting from alcohol tend to affect drinkers at younger ages, especially in the 15 to 29 years age group, which results in greater years of potential life lost and disability over the proposed life span (WHO 1999). CHD is rare in those younger than 50 years; hence most of the averted deaths are amongst the older ages. Thus, in terms of years of life lost, the adverse effects of drinking may outweigh any protection alcohol offers against CHD (Jernigan 2000).
The problems of alcohol and injury are not confined to developed countries. Indeed, the situation is particularly alarming in lower and middle‐income countries, where alcohol consumption is increasing, injury rates are high, and appropriate public health policies have not been implemented (Poznyak 2001). Most of the increase in global alcohol consumption has occurred in developing countries (WHO 2002). In sub‐Saharan Africa, where ischaemic heart disease is rare, the protective effects of alcohol are only of marginal public health importance while alcohol is a major cause of death and disability from injury (Murray 1997b).
How the intervention might work
Traditionally, injuries were perceived as random, unavoidable 'accidents', but in recent decades perceptions have altered and injuries are increasingly considered as preventable, non‐random events (Peden 2002b).
In the past, many interventions and much of the intervention research focused on individuals, targeting those considered at highest risk of alcohol‐related problems. However, it has been suggested that such a focus on 'problem drinkers' is unlikely to result in a sustained decrease in problems at the population level, because the majority of alcohol‐related problems are attributable to the substantial number of moderate drinkers who occasionally drink to intoxication (Babor 2003). It is alcohol intoxication (i.e. drunkenness) that is recognised as a strong risk factor for injury, as opposed to long‐term exposure to alcohol; thus preventing alcohol intoxication is a potentially effective approach for reducing the harm arising from alcohol (Babor 2003). Interventions that target all drinkers often have a demand‐side focus, aiming to reduce individuals' demands and consequently consumption of alcohol, mainly through educational interventions. An alternative is to take a 'supply‐side' approach. The principle of a supply‐side approach is to implement interventions that modify the environment within which alcohol is supplied, and the drinking context. Observational research has suggested that the environment of alcohol serving premises can impact on the risk of injury. Specifically relating to violence, factors such as a lack of seating, loud music, overcrowding, lack of available food are considered risk factors (Graham 1997; Homel 1992; Homel 2001; Rehm 2003).
Implementation of interventions in the server setting (e.g. bars, pubs, retailers) has the potential to maximise exposure; every alcohol consumer has contact with the industry in one form or another, while only a small proportion of these consumers come into contact with government services because of their alcohol consumption (Strategy Unit 2004). O'Donnell 1985 estimated that approximately 50% of alcohol‐related traffic crashes involve the prior consumption of alcohol on licensed premises, and a strong association between public violence and drinking on licensed premises is documented (Stockwell 2001). Hence, when such risky consumption occurs in server settings, it makes them a logical focus for prevention efforts.
Efforts applied to the server setting imply a level of acceptance that alcohol consumption will occur but aim to modify the drinking and/or the drinking environment so that potential harm is prevented. Interventions within server settings can range from the way alcohol is packaged, promoted and sold, to the overall management and policy of the establishment within which it is consumed. Such interventions include server training, use of alternatives to standard drinking glassware (for example, toughened glass, plastic containers), discontinuation of alcoholic drink promotions (for example, 'happy hours'), using server settings as sites for health promotion initiatives amongst others, which may be implemented individually or in combination.
Why it is important to do this review
Reviews of research are essential tools for health care workers, researchers, consumers and policy‐makers who want to keep up to date with evidence in their field. Systematic reviews enable a more objective appraisal of the evidence than traditional narrative reviews, and are important in demonstrating areas where the available evidence is insufficient and where further good quality trials are required (Egger 2001).
It is important that the effectiveness of interventions in the server setting is evaluated to aid policy decision‐making and priority setting. Graham 2000 published a comprehensive narrative literature review of preventive approaches for on‐premise drinking, and Shults 2001 conducted a systematic review to examine the effectiveness of server education specifically for preventing drink driving. However, no other systematic review attempting to quantify the effectiveness of all interventions delivered in the server setting on reducing all forms of injury has been identified. The purpose of this systematic review is to critically review the current evidence for the use of interventions delivered in the server setting for preventing injury.
Objectives
To quantify the effectiveness of interventions in the alcohol server setting for reducing injuries.
Methods
Criteria for considering studies for this review
Types of studies
The following randomised and non‐randomised study designs were eligible.
Randomised controlled trials
Participants are randomly allocated to intervention or control groups and followed up over time to assess any differences in outcomes.
Cluster randomised controlled trials
Groups of participants are randomly allocated to intervention or control groups and followed up over time to assess any differences in outcomes.
Non‐randomised controlled trials
The investigator has control over the allocation of participants to groups but does not use randomisation.
Controlled before and after studies
A follow‐up study of participants who have received an intervention and those who have not, measuring the outcome variable at both baseline and after the intervention period, comparing either final values if the groups are comparable at baseline, or change scores.
(Definitions adapted from those cited in Deeks 2003.)
Despite being more prone to bias than studies using random allocation, we decided to include non‐randomised controlled designs, in light of the practical constraints of conducting RCTs in this area.
Types of participants
Workers in licensed alcohol serving premises (e.g. bar staff, shop workers)
Owners and managers of alcohol serving premises
Patrons in licensed alcohol serving premises
Licensed alcohol serving outlets (e.g. retailers, pubs, bars, clubs, restaurants) including 'off‐licences' (i.e. premises which do not have a licence for on‐premise consumption, but sell alcohol for off‐premise consumption)
Areas of multiple licensed alcohol serving outlets (e.g. towns)
Types of interventions
Eligible interventions were those administered in the server setting that attempted to modify the conditions under which alcohol was served and consumed, to facilitate sensible alcohol consumption and reduce the occurrence of alcohol‐related harm. Studies of server interventions that were administered in a programme involving other ineligible (that is, not in the server setting) interventions were considered if outcomes attributed to the eligible server‐intervention component could be distinguished.
Legislative interventions such as server liability, licensing/opening hours, and advertising restrictions were not eligible.
Types of outcome measures
Primary outcomes
Fatal injuries
Non‐fatal injuries
(Data on all alcohol‐related injuries was considered, irrespective of whether the injured individual had consumed alcohol or not.)
Secondary outcomes
Behaviour change (e.g. change in amount of alcohol consumed)
Knowledge change
Search methods for identification of studies
Searches were not restricted by date, language or publication status.
Electronic searches
We searched the following electronic databases;
Cochrane Injuries Group's Specialised Register (searched November 2008),
Cochrane Central Register of Controlled Trials (The Cochrane Library 2008, Issue 4),
MEDLINE (January 1966 to November 2008),
EMBASE (1980 to November 2008),
PsycINFO (1806 to November 2008),
PsycEXTRA (1908 to November 2008),
ISI Web of Science: Science Citation Index Expanded (SCI‐EXPANDED) (1970 to November 2008),
Social Sciences Citation Index (SSCI) (1970 to November 2008), Conference Proceedings Citation Index‐ Science (CPCI‐S) (1990 to November 2008),
TRANSPORT (1988 to 2007/06),
ETOH (The Alcohol and Alcohol Problems Science Database; produced by the National Institute on Alcohol Abuse and Alcoholism (NIAAA); historic alcohol‐related research information covering the period from (1972 to 2003),
SIGLE (1980 to 2004/06),
SPECTR (September 2004),
Zetoc (1993 to September 2004),
National Research Register (issue 3/2004).
The original search strategy is presented in Appendix 1. The search strategy for the latest update is presented in Appendix 2.
Searching other resources
We searched the Internet, checked the reference lists of relevant studies and, where possible, contacted the first author of each included study to identify further potentially eligible articles.
Data collection and analysis
Selection of studies
We independently examined titles, abstracts, and keywords of citations from electronic databases for eligibility. We obtained the full text of all relevant records and independently assessed whether each met the pre‐defined inclusion criteria. We resolved disagreement by discussion.
Data extraction and management
We extracted data from each eligible study using a standard form that we had developed specifically for this review. We extracted data on the following:
study date and setting;
sample size;
study design;
method of allocation;
blinding of outcome assessment;
characteristics of intervention and control groups;
characteristics of intervention;
the outcomes evaluated;
results;
duration of follow up;
loss to follow up;
intention to treat.
Where necessary and possible, we sought additional information from researchers involved in the original studies.
We were not blinded to the names of the authors, institutions, journal of publication, or results of the trials, because evidence for the value of this is inconclusive (Berlin 1997).
Assessment of risk of bias in included studies
The Health Technology Assessment report, 'Evaluating non‐randomised intervention studies' (Deeks 2003), contains a systematic review of quality assessment tools used for non‐randomised studies and identifies six judged to be potentially useful for use in systematic reviews. For the present review, from these six, we selected a tool developed by the Effective Public Health Practice Project (Thomas 2003) to assess methodological quality of all the study designs. A modified framework of the Thomas 2003 quality tool was used to describe each of the included studies against the following criteria as available from the report;
Allocation bias (for example, was allocation to the experimental and control groups random and adequately concealed?)
Confounders (for example, did the groups under study differ in terms of distribution of potential confounders?)
Blinding (for example, were the outcome assessors blind to the allocation status of the participants?)
Data collection methods (for example, were outcome data collected through self‐report methods or more objective methods such as researcher observation or extracted from official records?)
Withdrawals and dropouts (for example, how many participants failed to complete the study and/or were lost to follow‐up?)
Intervention compliance (for example, what proportion of participants received the allocation intervention?)
Duration of follow‐up (for example, how long was/were the data collection period(s)?)
For the June 2010 update the above quality domains were incorporated into an assessment of the included studies risk of bias in accordance with the recommended approach presented in the Cochrane Handbook for Systematic Review of Interventions (Higgins 2008). We completed a risk of bias table for each study, incorporating a description of the study's performance against each of the above domains and our overall judgment of the risk of bias for each entry, as follows: 'Yes' indicates low risk of bias, 'Unclear' indicates unclear or unknown risk of bias, 'No' indicates high risk of bias.
Data synthesis
On inspection of the eligible studies, it was clear that there was a high degree of heterogeneity in terms of participants, interventions and outcomes (that is, clinical heterogeneity) which meant that a pooled analysis would not be appropriate. Therefore data were reviewed qualitatively for each study, presenting effect estimates, precision and statistical significance as reported. We calculated odds ratios (OR) and the mean difference (MD) for the RCTs where possible.
Results
Description of studies
Results of the search
The combined search strategy identified approximately 3,550 studies, of which 71 were deemed to be potentially relevant based on title or abstract. After a full text review, 23 studies were judged to meet the inclusion criteria.
Included studies
The studies had been conducted in six countries; five in Australia, twelve in the USA, two in Canada, two in Sweden, one in South Africa and one in the UK, published over a 21‐year period (1987 to 2008).
Eight were randomised controlled trials, ten were non‐randomised controlled trials and five used a controlled before and after design. Fourteen studies used individual premises as the unit of allocation; one trial used individual servers and the remaining seven used areas containing multiple serving establishments (e.g. towns).
Sixteen studies compared a responsible server training intervention with no training (or a reduced training programme). Two studies investigated the effectiveness of delivering health promotion information in serving establishments. Two studies examined interventions that targeted the server setting environment. One study focused on the management policies of serving premises, one investigated the effectiveness of a driving service for intoxicated patrons, and one looked at promotion of the use of public breathalysers.
Five studies used an injury outcome. Seventeen studies collected data on behaviour (of servers and/or of patrons) and six studies collected data on changes in knowledge.
A more detailed description of the individual studies is presented in the Characteristics of included studies table.
Risk of bias in included studies
A visual summary of the review authors' judgements about each risk of bias item for each included study is presented in Figure 1.
1.
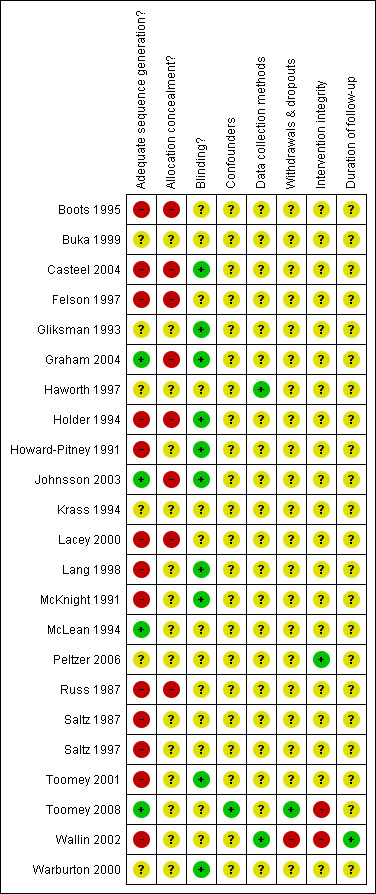
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
A summary of the quality of the trials against the quality criteria is presented below. Full details and the risk of bias judgements against each criterion are presented in the risk of bias sections of the Characteristics of included studies.
Allocation bias
In intervention studies, allocation should ideally be random and concealed. Allocation that is not random is likely to lead to unbalanced prognostic factors between the experimental and control groups, which will result in a biased estimate of the intervention effect. Nine studies reported using random allocation but the method used was only described in three of them; drawing lots was used in two (Graham 2004; Johnsson 2003), and a table of random numbers was used in two (McLean 1994; Toomey 2008). In none of the studies was concealment adequate.
One study (Casteel 2004) allocated the bars that agreed to participate in the study to the experimental group and those that refused to the control group. Two studies (Boots 1995; Felson 1997) allocated the intervention to an area previously identified as having a particularly high rate of alcohol‐related problems; regression‐to‐the‐mean should be considered in such instances and is described further in the 'Discussion' section.
Comparability of experimental and control groups at baseline
Baseline differences in alcohol‐related problems and/or average alcohol consumption between the experimental and control groups were reported in three studies (Boots 1995; Casteel 2004; Felson 1997). Ten studies attempted to match participants prior to allocation (Gliksman 1993; Graham 2004; Howard‐Pitney 1991; Krass 1994; Lang 1998; McKnight 1991; Peltzer 2006; Saltz 1987; Saltz 1997; Toomey 2001), although the number and type of factors matched for varied with each study. Two studies reported that the experimental and control groups had similar characteristics (Buka 1999; Lang 1998). One noted the presence of some differences (Wallin 2002). The remaining five studies did not report the presence (or absence) of baseline differences between the groups (Haworth 1997; Holder 1994; Johnsson 2003; McLean 1994; Russ 1987; Toomey 2008; Warburton 2000).
Blinding
To minimise observer bias, outcome assessors should ideally be blinded to the allocation status of participants, as they may be biased towards one group (consciously or not). Blinding of outcome assessment was used in 12 studies that used observers/interviewers to gather outcome data. The randomised controlled trial of toughened glassware (Warburton 2000) also blinded the participants to their own allocation status. Such a double‐blind design is not feasible in the other studies, due to the nature of the interventions under investigation; for example, participants cannot be blind to whether they received training or not.
Injury data (traffic crashes and violence) was collected from official records in four trials.
Data collection method
Methods by which outcome data are collected may be associated with their own biases. For example, self‐reported measures of behaviour are likely to be more prone to bias than observed behaviour.
In the seven studies with a knowledge outcome, six of these measured this in the trained servers only. All trials used a self‐completed test or questionnaire method. Response rates were high in the studies measuring knowledge immediately after the training and were lower in those with a longer follow‐up.
Behaviour was measured in two studies (Boots 1995; Buka 1999) using self‐reported data as the source of outcome data. Response rate to questionnaires tended to be low. Data on behaviour was gathered through observations by investigators in ten studies. Three (Johnsson 2003; Krass 1994; McLean 1994) out of the four studies undertaking patron interviews used a breath test to assess intoxication whilst one (Saltz 1987) collected self‐reported data on alcohol consumption. With the exception of Johnsson 2003, which achieved an extremely high response rate for patron interview (>95%), the remaining studies response rates were lower (range of 40 to 65%). One study (Haworth 1997), in which the intervention was the promotion of the use of publicly available breathalysers, used data from these devices to determine the level of usage.
All but one of the studies gathering injury outcome data used official records as the source, the exception being Warburton 2000 which used a self‐completed questionnaire.
Withdrawals and dropouts
Withdrawals and dropouts need to be minimised in any intervention study. Participants choosing to withdraw from the study are likely to be those with the worst prognosis. It is also important that participants who do not receive or complete their assigned intervention, remain in the analysis (that is, analysis is on an intention‐to‐treat basis).
Seven studies (Boots 1995; Buka 1999; Felson 1997; Holder 1994; Lacey 2000; Saltz 1997; Wallin 2002) allocated the intervention to areas of alcohol serving premises, and received a 'n/a' rating for this criterion. As the design was directed as a geographical area the percentage of participants completing, withdrawing or dropping out is not applicable.
Eight studies (Casteel 2004; Gliksman 1993; Howard‐Pitney 1991; Johnsson 2003; McKnight 1991; Russ 1987; Saltz 1987; Toomey 2008) using individual bar/premises as the unit of allocation, did not report any withdrawals, drop‐outs or loss to follow‐up.
Three studies (Krass 1994; Lang 1998; McLean 1994) reported bars refusing to participate in the patron surveys.
Four studies (Graham 2004; Peltzer 2006; Toomey 2001; Warburton 2000) reported bars withdrawing and/or lost to follow‐up; none of these studies presented outcome data for the affected bars. The information available on one study (Haworth 1997) is unclear as regards withdrawals or drop‐outs.
Intervention integrity and compliance
Eight studies examining server training reported the number of participants trained as a proportion of total servers; three reported training all staff, one trained 84% while the remaining five trained 50 to 60% of staff. In one study (Toomey 2008) 85% of intervention establishments completed their comprehensive training course but only 28% of controls completed the reduced version of the training course that had been planned for them. One of the trials (Holder 1994) was of a mandated training policy, so it is assumed that compliance was high.
Two studies examining health promotion interventions both reported that the extent of compliance with the intervention varied between premises for example, varying from displaying the information to actively distributing it, no further details are reported. The report of the study promoting breathalyser (Haworth 1997) use does not make clear whether promotion activities were completed in all premises.
The Warburton 2000 study involved replacing the bars' whole glassware supply; hence it is assumed compliance was high. The Casteel 2004 study involved making recommendations to managers to implement environmental changes to the bar, again it was reported that compliance was variable.
Follow‐up duration
In the studies assessing the change in knowledge (Boots 1995; Gliksman 1993; Howard‐Pitney 1991; Krass 1994; Lang 1998; McKnight 1991), measurements were made immediately before and after training in two studies, three months after in two, with the remaining three not specifying length of data collection periods in the report.
The timing of post observations of server behaviour to pseudo‐drunk patrons occurred within six months of administration of the intervention, with the exception of one (Wallin 2002), in which observations were made three years after. In the same study (Wallin 2002), post observations of server behaviour to patrons who appeared to be under‐age were made two and five years after. In the study in which use of breathalysers was promoted (Haworth 1997), the duration of follow‐up is unclear.
The timings of the patron interviews/surveys ranged from less than one week to three months after intervention implementation.
The length of data collection periods of injury data in the controlled before‐and‐after studies ranged from nine months to 11 years before and from three months to 15 years after. The Warburton 2000 randomised trial collected injury data for six months after.
Effects of interventions
Due to variability in the intervention types investigated by the included studies, the results have been reviewed qualitatively. The interventions have been grouped into five broad categories; server training, health promotion initiatives, drink driving service, interventions targeting the server setting environment, and policy interventions. With the exception of Graham 2004, studies in the server training category were investigating a sufficiently similar intervention to enable the studies to be presented together, with the results grouped by outcome. The focus of the training in Graham 2004 differed from the others thus has been reported separately. The results of the remaining studies in the other categories have been presented by study due to the variability of the interventions under investigation.
Server training
Fifteen studies investigated the effectiveness of server training; duration of the training interventions ranged from one to two hours to two days. All but one study involved training focusing on the responsible service of alcohol. Common training themes included raising awareness of alcohol service laws, recognition of early signs of alcohol intoxication, and tactics for dealing with intoxicated customers. Five of these reported a specific focus and/or specific training for the managers/owners in responsible alcohol service policies. In Graham 2004, the training was not targeted at responsible service, but on the prevention and management of aggression in bars.
Injury
Full results for the injury outcome are presented in Table 1.
1. Results ‐ server training (injuries).
| Buka 1999 | Not measured. |
| Gliksman 1993 | Not measured. |
| Graham 2004 | Not measured. |
| Holder 1994 | SINGLE VEHICLE NIGHT TIME (SVN) CRASHES Effect estimate = ‐0.524 (95% CI ‐0.956 to ‐0.091), t‐ratio = ‐2.40. The estimate is adjusted for seasonal fluctuations in crashes; alcohol related policy changes (changes to DUI legislation and reduction in legal driving BAL to 0.08) and for pattern of crashes in control states. Authors report the net estimated decline in SVN crashes following the implementation of the policy as: 4% after six months; 11% after 12 months; 18% after 24 months; 23% after 36 months. |
| Howard‐Pitney 1991 | Not measured. |
| Johnsson 2003 | Not measured. |
| Krass 1994 | Not measured. |
| Lang 1998 | Not measured. |
| McKnight 1991 | Not measured. |
| Russ 1987 | Not measured. |
| Saltz 1987 | Not measured. |
| Saltz 1997 | Not measured. |
| Toomey 2001 | Not measured. |
| Toomey 2008 | Not measured |
| Wallin 2003 | POLICE REPORTED VIOLENCE When adjusting for the development in the control area, the intervention parameter = ‐0.344 (se = 0.046), P < 0.001. The authors estimated this to represent a 29% reduction in police‐reported violence in the experimental area. |
Randomised controlled trials
None identified.
Non‐randomised controlled trials
None identified.
Controlled before and after studies
Holder 1994 investigated the impact of a state‐wide mandated server training policy and estimated a continued reduction in the number of single vehicle night time (SVN) crashes; after controlling for drink driving related policy changes and the trend of crashes in the control area, it was estimated that the intervention led to a reduction of 4% after six months, 11% after 12 months, 18% after 24 months, reaching 23% after 36 months.
Patron behaviour
Table 2 Patron behaviour was measured in terms of alcohol consumption in four studies (Johnsson 2003; Krass 1994; Lang 1998; Saltz 1987); three used breath tests to measure BAC, while one (Saltz 1987) used self‐reported alcohol consumption.
2. Results ‐ server training (behaviour).
| Buka 1999 | SELF‐REPORTED SERVER BEHAVIOUR Alcohol serving practices ‐ this was measured in each community using a Desired Server Behaviour Index (DSBI) (score ranged from 1 to 5). The higher the score the more desirable the behaviour. Mean DSBI (+/‐ SD) for overall server behaviour; Experimental community = 3.59 (+/‐ 0.74) Control community A = 3.59 (+/‐ 0.61) Control community B = 3.24 (+/‐ 0.65) Significance test; F=2.96, P=0.06. |
| Gliksman 1993 | OBSERVED SERVER BEHAVIOUR TO PSEUDO DRUNKS Measured using a behaviour score based on observations of six scenarios (the higher the score the more desirable the behaviour). (Exact figures are not reported in the report text, but the following estimates were read from a graph). Experimental sites behaviour score increased from ˜15 to 21.5 pre to post intervention. Control sites behaviour score changed from ˜16.5 to 16.4 pre to post intervention. Significance test; F=8.73, P<0.01. |
| Graham 2004 | OBSERVED AGGRESSION EXHIBITIED BY PATRONS (average number of incidents per observation) 1) Consistent rating of severe physical aggression by all raters, definite intent Experimental bars; decreased from 0.053 to 0.035 Control bars; increased from 0.007 to 0.060. Significance test; t= 5.23, df=28, P<0.001. 2) All severe aggression plus consistent rating of moderate physical (with or without verbal aggression), definite intent (average number of incidents per observation) Experimental bars; decreased from 0.134 to 0.101 Control bars; increased from 0.075 to 0.126. Significance test; t= 1.87, df=28, P=0.071. OBSERVED AGGRESSION EXHIBITIED BY STAFF (average number of incidents per observation) 1) Consistent rating of severe physical aggression by all raters, definite intent 'Frequencies too low for analyses. 2) All severe aggression plus consistent rating of moderate physical (with or without verbal aggression), definite intent Experimental bars; increased from 0.029 to 0.056. Control bars; increased from 0.014 to 0.053. Significance test; t= 1.19, df=28, P=0.243. |
| Holder 1994 | Not measured. |
| Howard‐Pitney 1991 | OBSERVED SERVER BEHAVIOUR Mean number of interventions made by servers were calculated for eight different responsible interventions, the overall mean for all eight interventions (the higher the mean value the more desirable the server behaviour); Experimental bars = 0.95 Control bars =1.26 Confidence intervals and results of significance test are not presented however, the authors report that 'no differences were observed between treatment and control servers on any intervention or on a sum average of eight possible interventions'. |
| Johnsson 2003 | BEHAVIOUR OF PATRONS Change in BAC(mg%) (and 95% CIs) between baseline and follow‐up; Experimental bars= ‐0.004% (‐0.012 to 0.004) Control bars = +0.007% (‐0.001 to 0.015). Mean difference in BAC between experimental and control bars = ‐0.011% (95% CI 0.022 to 0.000). In the experimental group 40% of tested patrons had a BAC greater than 0.1% before the training and 39% after. In the control group the corresponding figures were 34% before and 41% after. The difference between these changes was not significant (P = 0.12, one‐tailed, 95% CI ‐0.45 to 1.10). |
| Krass 1994 | BEHAVIOUR OF PATRONS 1) Mean BAC (mg%) of patrons This increased from 0.055 (95% CI 0.049 to 0.065) to 0.069 (95% CI 0.058 to 0.078) over the study period in the experimental sites, and increased from 0.057 (95% CI 0.050 to 0.078) to 0.058 (95% CI 0.050 to 0.066). 2) Total consumption of alcohol (gm) On experimental premises this increased from 62.4 (95% CI 50.5 to 74.4) to 69.3 (95% CI 56.9 to 81.6), and decreased from 79.0 (95% CI 82.9 to 95.1) to 67.9 (95% CI 56.7 to 79.1) in control premises. The authors report that 'no significant differences were found in mean BAC and total consumption of alcohol between experimental and control sites at pre and post level'. 3) Proportion of patrons with a BAC over 0.10mg% This increased from ˜0.17% to ˜0.27% in intervention sites and reduced from ˜0.23% to 0.2% in the control sites (exact figures are not presented in the report text, but the following estimates were read from a graph). No confidence intervals or significance test results presented for this outcome. |
| Lang 1998 | BEHAVIOUR OF PATRONS 1) Drink driving offences No quantitative data presented. The authors report that 'the downward trend in drink driving offences from intervention premises leading up to the project was continued during the evaluation period, while the figure for the control sites remained relatively unchanged. However, the number of drink driving cases from both intervention and control premises were too few to permit any meaningful evaluation'. 2) Percentage of tested patrons with a BAL(mg%)> 0.15 This reduced over the study period, with the decline greater for experimental sites (17.4% to 5.3%) than control (10.1 to 3.7%), this is not significant (P=0.389). 3) Percentage of tested patrons with a BAL>0.08 This decreased from 52% to 26.9% in experimental sites and decreased from 34.8% to 24%, this rate of decline is significantly greater (P<0.029) for the experimental than for the control group. SELF‐REPORTED SERVER BEHAVIOUR Changes in the average ratings in mean score of the adoption of responsible service policies over the pre and post periods were reported as not statistically significant (full results of significance test is not presented). Total score increased from ‐0.7 to 0.9 in intervention sites and remained unchanged at ‐1.8 in control sites (maximum possible score=+2, minimum possible score= ‐2). OBSERVED SERVER BEHAVIOUR Reported that there was no difference between experimental and control in terms of refusal of service to intoxicated pseudos. In the experimental group, 1 out of 11 visits and 3 out of 14 visits were refused service in the pre and post period respectively. In the control group, 1 out of 14 visits were refused service in both the pre and post period. Authors report that 'no further analyses were undertaken'. |
| McKnight 1991 | SELF‐REPORTED SERVER BEHAVIOUR (trained servers only) 1) Serving practices, mean score (+/‐sd); Pre = 3.13 (+/‐ 0.67) Post = 3.50 (+/‐ 0.68) Significance test; diff=0.57, t=11.90, P<0.01 2) Serving policies mean score (+/‐sd); Pre =0.58 (+/‐ 0.12) Post = 0.65 (+/‐ 0.11) Significance test; diff=0.61, t=6.65, P<0.01 OBSERVED SERVER BEHAVIOUR 1) Percentage change between pre and post server 'intervention level': a) Intervention level = 'None' (servers make no attempt to intervene); Experimental = ‐12.5% Control = ‐0.8% b) Intervention level = 'Partial' (servers provide drink requested but make some attempt at intervention); Experimental = +10.5% Control = +1.7% c) Intervention level = 'Full' (servers refuse to serve any alcoholic beverage); Experimental = +1.9% Control = ‐0.7% 2) Mean score of server intervention (the higher the score the more desirable); Mean score in experimental sites increased from 0.19 to 0.34 (diff = 0.15, F=10.42, P<0.01) between the pre and post periods. Mean score in control sites remained at 0.22 (diff = 0.00, F=0.01, P=0.97) between the pre and post periods. Significance test of the difference between the intervention effects in the experimental and control sites; F=6.70, df=1/207, P=0.01). OBSERVED 'REAL' PATRON INTOXICATION Amongst the experimental sites the mean intervention level increased from 0.03 before, to 0.22 after (F=4.27, df=1/127, P=0.04), for the comparison sites remained unchanged at 0.07 (F= 0.87, df=1/167, P=0.35) across the periods. |
| Russ 1987 | OBSERVED SERVER BEHAVIOUR Trained servers on average were reported as attempting a greater frequency of intervention than servers without training (P<0.05). BEHAVIOUR OF PATRONS The average exit BAC(%mg) for pseudo patrons served by servers who remained untrained was 0.103 (+/‐ 0.033), while those served by trained personnel had an average BAC of 0.059 (+/‐0.019). The mean difference in exit BACs between pseudopatrons served by trained versus untrained servers = 0.044 (95% CI 0.022 to 0.066). Authors report that the 'BAC levels of pseudopatrons served by trained staff were significantly lower (P<0.01) than those obtained among pseudopatrons prior to training or served by untrained servers in the post period'. |
| Saltz 1987 | BEHAVIOUR OF PATRONS 1) Per capita consumption (number of drinks) Reduced from ˜5.6 to ˜5 in experimental site and ˜6 to ˜5.5 in the comparison site. 2) Rate of consumption (drinks per hour) Reduced from ˜3.5 to ˜2.3 in the experimental site and ˜3.25 to ˜3.75 in the comparison (exact figures are not reported in the report text, but the following estimates were read from a graph). Confidence intervals or results from significance test were not reported. Authors report that 'multivariate linear and logistic regression analyses 'reveal that although absolute consumption and rate of consumption were unaffected by the program, the likelihood of a customers being intoxicated was cut in half'. |
| Saltz 1997 | SELF‐REPORTED SERVER BEHAVIOUR Self‐reported server policy of refusing service to intoxicated patrons (Mean % yes) N. Californian communities Experimental; pre = 3%, post = 19% Control; pre =8%, post = 10% S. Californian communities Experimental; pre 6%, post = 15% Control; pre =6%, post =7% S. Carolina communities Experimental; pre= 7%, post= 8% Control = pre 19%, post 17%. Authors report that 'no statistical difference was found', no further information presented. OBSERVED SERVER BEHAVIOUR Pseudo‐patron survey; responsible service assessed using an intervention score (ranging of low [=bad] of ‐2 to +2 [=good]). N. Californian communities Experimental; pre = 0.17, post = 0.21 Control = pre ‐0.15, post = ‐0.19 S. Californian communities Experimental; pre= ‐0.18, post = ‐0.17 Control = pre 0.15, post 0.16 S. Carolina communities Experimental; pre= 0.17, post= 0.07 Control; pre= ‐0.23, post= ‐0.09. Authors report that 'no statistical difference was found', no further information presented. |
| Toomey 2001 | OBSERVED SERVER BEHAVIOUR Pseudo‐intoxicated purchase attempts Pre‐intervention, the purchase rates were 68.4% and 70.1%, in the experimental and control sites respectively. Post‐intervention, the purchase rate reduced in the intervention site to 40.0% and increased to 72.9% in the control. The relative decline was reported as not statistically significant (t=‐1.17, P=0.27). Refusal of service to pseudo‐intoxicated patrons changed from 83.1% to 80.3% in experimental and from 63.0% to 54.8% in control (t=0.24, P=0.81). |
| Toomey 2008 | OBSERVED SERVER BEHAVIOUR
Pseudo‐intoxicated purchase attempts Total of purchase attempts in all participating establishments that were successful before the intervention and during two post‐intervention follow‐ups. One purchase attempt made in each establishment. Intervention Control Baseline 81/122 (66.4%) 68/109 (62.3%) 1st follow‐up 62 /111(55.9%) 67/105 (63.8%) 2nd follow‐up 73/111 (65.8%) 78/106 (73.58) Authors "observed no significant differences at follow‐up in reported policies/practices across establishments". |
| Wallin 2002 | OBSERVED SERVER BEHAVIOUR 1. Refusal rates to intoxicated patrons (Data in paper published 2003.) 55% in the experimental sites which had received training, 48% in intervention sites yet to be receive training, and 38% in the control area. The authors reported that this was not significant. No further details presented. 2. Successful attempts to buy a drink by patrons who were over 18 but appeared to be under 18. (Data in paper published 2004.) Intervention Control Baseline (1996) 129/307 (42%) 57/146 (39%) 1st follow‐up (1998) 57/146 (39%) 46/106 (43%) 2nd follow‐up (2001) 37/118 (31%) 41/120 (34%) The authors reported that differences between intervention and control groups were not significant. No further details presented |
Randomised controlled trials
In the randomised study by Johnsson 2003 the post‐intervention mean BAC levels were lower in the experimental bars (0.082%) than the control bars (0.087) (MD = ‐0.01 (95% CI ‐0.02 to 0.00). The study authors compared the change in BAC from pre to post intervention for both groups; the mean BAC in the experimental bars reduced to a greater extent than in the control bars, mean difference = ‐0.011% (95% CI 0.022 to 0.000). The odds ratio indicates a modest effect on the percentage of patrons with a BAC > 0.1 (OR 0.92, 95% CI 0.67 to 1.26), although this is compatible with the play of chance.
The randomised trial by Krass 1994 reported that a statistically significant difference was not found between experimental and control bars in mean patron BAC or total consumption, with values increasing for both outcomes in both groups. The mean BAC in the post intervention period was 0.069gm% (95% CI 0.058 to 0.078) in the experimental and 0.058gm% (95% CI 0.050 to 0.066) in the control. The percentage of patrons with a BAC > 0.10 in the after period was 27% in the experimental group and 20% the control; no confidence intervals or significance test were reported.
In Peltzer 2006, BAC of patrons was measured but the published data contains errors and omissions and is not usable.
Non‐randomised controlled trials
In the non‐randomised controlled trial by Lang 1998, the change in percentage of patrons with a BAC > 0.15 over the study period declined for both groups (by 12.1% in the experimental, by 6.4% in the control); the reductions were not found to be significantly different (P = 0.389). A positive intervention effect was found for the change in the percentage of patrons with a BAC > 0.08, with the percentage decline significantly greater in experimental bars (‐25.1%) than the control (‐10.8%), P < 0.029. Lang 1998 also measured subsequent drink driving offences, but detected too few offences to evaluate and no data were presented.
Controlled before and after studies
Saltz 1987 compared two Navy clubs, one of which received server training. Self‐reported data indicated no effect on overall alcohol consumption or rate of consumption of alcohol, P > 0.05. However, a positive intervention effect on the risk of having a BAC > 0.10% (as estimated from the number of drinks consumed) was found, P < 0.05.
Server behaviour
Full results for the server behaviour outcome are presented in Table 2.
Randomised controlled trials
Gliksman 1993 used a behaviour score based on observations of six scenarios (the higher the score the more desirable the behaviour). Estimates (read from a graph) showed an increase of score in the experimental sites (+6.5) and a slight decrease (‐0.1) in the control. The difference in score change was found to be statistically significant, P < 0.01.
Peltzer 2006 used a scoring system to assess the behaviour of servers in specific situations. Full details of the system are not included in the published report and only mean values of the total scores for the intervention and control groups are provided.
Toomey 2008 compared rates of successful attempts to be served by pseudo‐drunk patrons in experimental and control sites one and three months after server training had been completed. The study authors report that they found no significant differences at follow‐up in reported policies/practices across establishments.
Non‐randomised controlled trials
McKnight 1991 calculated mean scores of server intervention for each group (the higher the score the more desirable). The score in the experimental sites increased by 0.15 and remained unchanged in the control sites, between the pre and post periods. Significance testing indicated a significant difference, P = 0.01. McKnight 1991 also applied an intervention score to observed server behaviour to 'real' intoxicated patrons; the level increased significantly in the experimental bars (P = 0.04) but not in the control bars (P = 0.35) pre to post intervention.
Howard‐Pitney 1991 calculated the mean number of interventions made by servers for eight different responsible interventions. The overall mean for all eight interventions (the higher the mean value the more desirable the behaviour) was 0.95 for experimental and 1.26 for the control bars. Neither confidence intervals or P values were presented for these estimates; however, the authors reported that 'no differences were observed between treatment and control servers on any intervention or on a sum average of eight possible interventions'.
Saltz 1997 calculated a behaviour score (ranging of low [=bad] of ‐2 to +2 [=good]). In the North Californian communities the score increased by 0.04 in the experimental, and by 0.34 in the control. In the South Californian communities the score increased by 0.01 in the experimental community and by 0.01 in the control. In the South Carolina communities the score reduced by 0.1 in the experimental and increased by 0.14 in the control. The authors report that 'no statistical difference was found', no further information was presented.
The study by Russ 1987 recorded the number of observed responsible interventions made by the servers, and found that the trained servers had a higher frequency of responsible interventions than the untrained servers (P < 0.05). The exit BAC of the pseudo‐patrons was also measured, post‐test only; for the experimental group, average exit BAC = 0.103 (+/‐0.033) and for control = 0.059 (+/‐0.019), this was reported as significant, P < 0.01. Mean difference in the exit BAC of pseudo‐patrons served by experimental versus control servers = 0.044 (95% CI 0.022 to 0.066).
Three studies (Lang 1998; Toomey 2001; Wallin 2002) compared the change in the number of service refusals to pseudo‐intoxicated patrons; neither study found a significant difference between the experimental and control groups.
In Lang 1998 pseudo‐patrons were refused service, in 1/11 and 3/14 visits in the experimental group in the pre and post period, respectively. In the control group, 1/14 visits were refused in both the pre and post intervention period. The authors report that no further analyses were undertaken of this data, due to the small numbers. In the study by Toomey 2001, refusal of service to pseudo‐intoxicated patrons decreased from 83.1 to 80.3% in the experimental and from 63.0 to 54.8% in the control, the difference between the changes was not found to be significant, P = 0.81. Wallin 2002 found that, three years post intervention the refusal rates to pseudo‐intoxicated patrons was 55% in the experimental premises that had received training, 48% in the experimental sites yet to have received training and 38% in the control area. The authors reported that the differences were not significant, but exact results of the significance test were not reported.
The study by Toomey 2001 also measured server behaviour in terms of the number of successful purchase attempts by pseudo‐intoxicated patrons (that is, the lower the number of successful purchases, the more desirable the behaviour). Purchase attempts reduced from 68.4% to 40.0% and increased from 70.1% to 72.9% over the study period in the experimental and control sites, respectively. The relative decline was reported as not being statistically significant, P = 0.81.
Three studies (Buka 1999; Lang 1998; Saltz 1997) measured self‐reported server behaviour, none of which found a statistically significant difference between experimental and control.
Buka 1999 measured self‐reported server behaviour according to a Desired Server Behaviour Index (scale from 1 to 5, the higher the score the more desirable the behaviour) in the experimental and two control communities. Mean DSBI (+/‐SD) was 3.59 (+/‐0.74) in the experimental community, 3.59 (+/‐0.61) and 3.24 (+/‐0.65) in control A and B communities respectively, P = 0.06.
Lang 1998 measured server behaviour by calculation of a score, based on reported adoption of responsible service policies over the pre to post period, each bar was rated against 11 dimensions of responsible service. Average ratings of experimental sites increased in a positive direction for 4/11 dimensions, with the rest unchanged. In the control sites there was one positive, two negative and eight unchanged dimensions in the control sites. The authors report the difference not to be statistically significant but the exact results of significance test were not presented.
Saltz 1997 measured the percentage of premises reporting as having a policy of refusing service to intoxicated patrons. In the North Californian communities the percentage reporting 'yes' increased by 16% in the experimental, and by 2% in the control. In the South Californian communities the score increased by 9% in the experimental community and by 2% in the control. In the South Carolinian communities the score reduced by 1% in the experimental and decreased by 2% in the control. The authors report that 'no statistical difference was found', but no further information was presented.
Controlled before and after studies
None identified.
Knowledge
Full results for the knowledge outcome are presented in Table 3.
3. Results ‐ server training (knowledge).
| Buka 1999 | Not measured. |
| Gliksman 1993 | KNOWLEDGE OF SERVERS This was measured in the trained servers only. Results for the true/false section increased significantly pre to post test, t=‐12.5, P<0.001. Results for the open‐ended question section increased significantly pre to post test, mean score increased from 1.3 to 5.29, t=‐10.89, P<0.001. |
| Graham 2004 | Not measured. |
| Holder 1994 | Not measured. |
| Howard‐Pitney 1991 | KNOWLEDGE OF SERVERS This was measured in trained group only. Formal measures of effect and confidence intervals are not presented however, the authors report that servers and managers increased their knowledge and showed improvement in their beliefs that customers would respond favourably to responsible alcohol service and policies P<0.001, all measures'. |
| Johnsson 2003 | Not measured. |
| Krass 1994 | KNOWLEDGE OF SERVERS This was measured in trained group only. Mean total knowledge score increased from 23.98 to 30.8; t= ‐12.03, df=66, P<0.001. |
| Lang 1998 | KNOWLEDGE OF SERVERS This was measured in trained group only. The authors report a 'statistically significant (>0.05) increase in knowledge of laws regarding serving obviously drunk customers, maintained at follow‐up. Overall, however, there were only minor increases in knowledge, most of which was not retained at follow‐up'. No other quantitative data is reported. |
| McKnight 1991 | Not measured. |
| Russ 1987 | Not measured. |
| Saltz 1987 | Not measured. |
| Saltz 1997 | Not measured. |
| Toomey 2001 | Not measured. |
| Toomey 2008 | Not measured. |
| Wallin 2002 | Not measured. |
Randomised controlled trials
Gliksman 1993 and Krass 1994 reported a statistically significant improvement in knowledge after training (P < 0.05). This outcome was measured in the trained servers only. In Peltzer 2006, while a questionnaire was administered to servers to assess their knowledge and attitude, no data is available in the published report.
Non‐randomised controlled trials
Two studies (Howard‐Pitney 1991; Lang 1998) measured change in knowledge in the trained servers. Both reported a statistically significant improvement in knowledge after training (P < 0.05). This outcome was measured in the trained servers only.
Controlled before and after studies
None identified.
Server training to reduce aggression
The randomised controlled trial by Graham 2004 measured the effect of a 'safer bars' training programme on reducing observed aggression exhibited by patrons and staff, the primary outcome being the average number of incidents of severe or moderate aggression per observation.
A significant positive intervention effect (P < 0.001) was found for severe physical aggression exhibited by patrons (consistent rating by all raters; definite intent); with average number of incidents falling by 0.018 in the experimental and increasing by 0.053 in the control. A positive intervention effect was also observed when examining all severe aggression plus consistent rating of moderate physical (with or without verbal aggression; definite intent), with the average number of incidents decreasing by 0.033 in experimental and increasing by 0.051 in the control over the trial period, however this did not reach statistical significance (P = 0.071).
The number of incidents of severe physical aggression exhibited by staff (consistent rating by all raters; definite intent); was too low to enable analysis. Analysis of all severe plus consistent rating of moderate physical (with or without verbal aggression; definite intent), indicated an increase in average number of incidents by 0.027 in the experimental and an increase of 0.039 in the control bars (P = 0.243), over the trial period.
Health promotion initiatives
Full results for the health promotion interventions are presented in Table 4.
4. Results ‐ Health promotion interventions.
| Boots 1993 | |
| Injuries | Not measured. |
| Behaviour | BEHAVIOUR OF PATRONS 1) Self‐reported behaviour of drinkers For the experimental area the authors report that there was 'no significant change in attendance at 'safer' parties (i.e. those that adhered to the tips) between those who had heard of the intervention and others who had not'. a) Provision of food; chi‐squared=2.543, df=3, P=0.4675. b) Provision of alternative drinks; chi‐squared=0.823, df=3, P=0.844. c) Reduction in service to intoxication; chi‐squared=5.844, df=3, P=0.1194. d) Provision of transport; chi‐squared = 4.811, df=3, P=0.1862. In the control area is it reported that there was no significant pre‐post difference, however no quantitative data were reported. |
| Knowledge | DRINKERS' KNOWLEDGE In the experimental area there was no significant community‐wide change in safe partying knowledge resulting from the campaign; chi2=2.254, df=5, P=0.813. No significant pre‐post difference found in the control area, no other quantitative data reported. |
| McLean 1994 | |
| Injuries | Not measured. |
| Behaviour | BEHAVIOUR OF PATRONS 1) Median BAC(mg%) This was 0.030 in both the experimental and control groups (P=0.415). 2) Percentage of patrons with a BAC>0.10 This was 17.5% and 20.0% in the experimental and control groups respectively (P=0.509). 3) Percentage of patrons with a BAC>0.15 This was 7.5% and 7.8% in the experimental and control groups respectively (P=1.000). SELF‐REPORTED ALCOHOL CONSUMPTION 1) This was significantly less in the experimental group (38g) than the control (47g) with P=0.01. 2) Percentage of patrons with a measured BAC>0.05% who intended to drive This was 6.8% in experimental and 7.8% in the control group (P=0.635). |
| Knowledge | Not measured. |
Injury
No studies identified.
Patron behaviour
Randomised controlled trials
One trial was found. McLean 1994 investigated the effectiveness of the distribution and display of sensible drinking information in bars on the alcohol consumption of patrons. No statistically significant difference was found between the control and experimental bars in any of the measures of alcohol consumption used with the exception of the self‐reported data. After the intervention the median BAC(mg%) was 0.030 in both the experimental and control groups (P = 0.415); the percentage of patrons with a BAC > 0.10 was 17.5% and 20.0% in the experimental and control groups, respectively (P = 0.509). The odds ratio for the percentage of patrons with a BAC > 0.1, indicated a modest intervention effect (OR = 0.85, 95% 0.56 to 1.29; n = 18 bars), although this is compatible with the play of chance. The percentage of patrons with a BAC > 0.15 was 7.5% and 7.8% in the experimental and control groups, respectively (P = 1.000); OR = 0.96 (95% CI 0.52 to 0.77). Self‐reported alcohol consumption was significantly less in the experimental group (38g) than the control (47g) with P = 0.01; the percentage of patrons with a BAC > 0.05% who intended to drive was 6.8% in experimental and 7.8% in control group (P = 0.635).
Non‐randomised controlled trials
Boots 1995 investigated the effectiveness of the distribution cards containing 'safe‐partying' tips through liquor stores. Self‐reported data on the behaviour of drinkers were collected. Comparing pre and post intervention responses, no difference was found in the number of drinkers adhering to the tips (providing food, P = 0.4675; providing alternative drinks, P = 0.844; reducing service to intoxication, P = 0.1194; providing alternative transport, P = 0.1862). For the control town, no data is reported, however the authors state that there was no significant pre to post difference. Drinkers' knowledge of the tips promoted by the intervention was only measured in the experimental area; it was reported that there was no significant community‐wide change in safe‐partying knowledge resulting from the campaign, P = 0.813. In Haworth 1997 rates of use of public breathalysers were recorded before and after promotion activities but the published data is not usable.
Controlled before and after studies
None identified.
Drink driving service
Full results for the drink driving service are presented in Table 5.
5. Results ‐ Drink driving prevention services.
| Lacey 2000 | |
| Injuries | ROAD TRAFFIC CRASHES 1) Injury crashes These reduced by 15% in the experimental area after implementation of the programme (t=‐2.61, reported as 'highly significant'), and there was no reduction in the control areas. 2) Fatal road traffic crashes A before‐and‐after analysis of the ratio of the experimental area's fatal crashes to the comparison's fatal crashes, indicated that the ratio reduced from 0.78 to 0.60, this was reported as not being statistically significant (P=0.29). |
| Behaviour | Not measured. |
| Knowledge | Not measured. |
Injury
Randomised controlled trials
None identified.
Non‐randomised controlled trials
None identified.
Controlled before and after studies
Lacey 2000 investigated the effectiveness of a free driving home service for intoxicated drinkers. Injury crashes reduced by 15% in the experimental area after implementation of the programme (t = ‐2.61, reported as 'highly significant'), the authors report that there was no reduction in the control areas. A before‐and‐after analysis of the ratio of the experimental area's fatal crashes to the control's fatal crashes, indicated that the ratio reduced from 0.78 to 0.60, this was reported as not being statistically significant (P = 0.29).
Behaviour
None identified.
Knowledge
None identified.
Interventions targeting the server setting environment
Full results for interventions targeting the server setting environment are presented in Table 6.
6. Results ‐ Interventions targeting the server setting environment.
| Casteel 2004 | |
| Injuries | Post intervention period control versus experimental stores Rate Ratios [adjusted for reported district crime] with 95% CI and P values; 1) Robbery 5.4 (95%CI 0.7‐43) P=0.11 2) Assault 3.4 (95%CI 0.7‐18) P=0.13 3) Shoplifting 5.6 (95%CI 0.9‐36) P=0.07 4) All crime 4.6 (95%CI 1.7‐12) P=0.01 5) Injury 1.1 (95%CI 0.1‐10) P=0.93 6) Police reports 2.7 (95%CI 1.3‐5.4) P=0.01. |
| Behaviour | Not measured. |
| Knowledge | Not measured. |
| Warburton 2000 | |
| Injuries | GLASSWARE RELATED INJURIES INFLICTED TO SERVING STAFF 98 staff experienced 115 injuries; 43 in control and 72 in intervention group. The ratio of number of staff injured in the experimental group to number in the control was 1.72 (95%CI 1.15, 2.59) (˜70% greater risk of injury in experimental group). Relative risk adjusted for people at risk was 1.48 (95%CI 1.02, 2.15). (˜50% greater risk of injury in experimental group). Relative risk adjusted for hours worked was 1.57 (95%CI 1.08, 2.29). (˜60% greater risk of injury in experimental group) P<0.05 (all CIs exclude the null hypothesis). Most injury, 86% and 89% in control and experimental bars respectively, was inflicted to the hands. |
| Behaviour | Not measured. |
| Knowledge | Not measured. |
Injury
Randomised controlled trials
Warburton 2000 was the only included study to be randomised and use an injury outcome. The study compared the effectiveness of two types of drinking glassware; toughened glassware (experimental) and annealed glassware (control) in reducing bar‐staff injuries. The results indicated that the experimental glass caused more injury than the control. Seventy‐two and 43 staff experienced glass injuries in the experimental and control bars, respectively. The ratio of number of staff injured in the experimental group to the number in the control = 1.72 (95% CI 1.15 to 2.59) (˜70% greater risk of injury in experimental group). The relative risk adjusted for people at risk = 1.48 (95% CI 1.02 to 2.15) (˜50% greater risk of injury in experimental group). The relative risk adjusted for hours worked = 1.57 (95% CI 1.08 to 2.29) (˜60% greater risk of injury in experimental group). All P values were < 0.05.
Non‐randomised controlled trials
None identified.
Controlled before and after studies
Casteel 2004 investigated an intervention aimed at reducing crime experienced by the drinking establishment and used a number of injury measures as outcomes, with a statistically significant intervention effect detected for two; all crime and number of police reports. Comparing the control versus experimental stores, the study authors reported rate ratios (RR) (adjusted for reported district crime) and 95% CI and P values; for robbery RR 5.4 (95% CI 0.7 to 43) P = 0.11; for assault RR 3.4 (95% CI 0.7 to 18) P = 0.13; for shoplifting RR 5.6 (95% CI 0.9 to 36) P = 0.07; for all crime RR 4.6 (95% CI 1.7 to 12) P = 0.01; for injury RR 1.1 (95% CI 0.1 to 10) P = 0.93; and for police reports RR 2.7 (95% CI 1.3 to 5.4) P = 0.01.
Behaviour
None identified.
Knowledge
None identified.
Server setting policy intervention
Full results for the policy intervention are presented in Table 7.
7. Results ‐ Server setting management/policy interventions.
| Felson 1997 | |
| Injuries | SERIOUS ASSAULT RATES The study reports that before intervention, the experimental area's serious assault rate was 52% higher than the comparison rate. |
| Knowledge | Not measured. |
| Behaviour | Not measured. |
Injury
Randomised controlled trials
None identified.
Non‐randomised controlled trials
None identified.
Controlled before and after studies
Felson 1997 investigated the impact on serious assault rate, after the introduction of a policy aimed at minimising the movement of drinkers between different bars and their alcohol consumption. The authors reported that before the policy intervention, the serious assault rate in the experimental area was 52% higher than the rate in the control area. After the intervention, the serious assault rate in the experimental area was 37% lower than in the control.
Behaviour
None identified.
Knowledge
None identified.
Discussion
Summary of main results
There is insufficient evidence from high quality intervention studies that interventions in the alcohol server setting are effective in preventing injuries. Only one randomised trial with an injury outcome was identified and this did not detect a beneficial intervention effect. Three randomised controlled trials measured patron alcohol consumption, none of which found a confident estimate of effect. One randomised trial found a statistically significant reduction in observed severe aggression exhibited by patrons. There is conflicting evidence as to whether there is an improvement in server behaviour and the extent to which this might translate into a reduction in injury risk is unknown. Interpretation of this outcome is, therefore, of limited value.
Quality of the evidence
The validity of the inferences based on a systematic review is dependent on the quality of the included studies. Overall, the methodological quality of the studies included in this review was judged to be weak.
Only eight studies used random allocation, and none of these were found to have adequate allocation concealment. Three of these studies used a cluster design and randomly allocated a very small number of clusters (Buka 1999; Gliksman 1993; Krass 1994). The benefits of randomisation are unlikely to be achieved with very small numbers. These studies have been classified as randomised trials in this systematic review however, they are likely to be as susceptible to allocation bias as the non‐randomised trials.
Attempts were made in nine of the non‐randomised designs to minimise confounding through matching of the experimental and control groups, but residual confounding remains a problem.
Ineffective and poorly concealed randomisation in the included studies, means confounding and bias are likely to have influenced the results.
Two studies allocated the intervention to an area previously identified as having a particularly high rate of alcohol‐related problems. With such an approach, regression‐to‐the‐mean should be considered. Regression‐to‐the‐mean describes the tendency for an abnormally high (or low) number of events (e.g. injuries) to return to values closer to the long term mean. Any observed abnormally high (or low) number of events is thus a result of random fluctuation. It is a particular threat to controlled‐before‐and‐after studies and has important implications when the study interest is a change in outcome. In such cases an apparent intervention effect may actually be a result of the number of events returning to the average rate after a random fluctuation. Consequently, these studies should be interpreted with caution.
Blind outcome assessment was widely used in the included studies. It was reported as being used in 11 studies during the collection of behaviour data (important when collecting data on such a subjective outcome). Additionally, the studies measuring injury outcome extracted data from official records (e.g. crash data from government statistics, crime data from police records). When using data from such external, objective sources it is reasonable to assume that outcome assessment is blind.
Questionnaires and interviews were often used to examine behaviour; the response rates were low in a number of studies. This is a source of potential bias as the non‐responders are likely to have the worst prognosis or be at most risk. Such a bias leads to an overestimation of an intervention effect. A number of studies attempted to minimise this bias in the patron interviews, by judging the intoxication level of non‐responders. Similarly, participants who withdraw from the study or are lost to follow‐up are likely to have a poorer prognosis. However, details of such withdrawals and drop‐outs were often not reported; of the few studies that did, it seemed that analysis was not on an intention‐to‐treat basis, nor was outcome data for such non‐participants presented. Cautious interpretation of such studies is needed, as it is likely that their findings over‐estimate any intervention effect.
Intervention compliance was also a problem for many of the studies. In the server training studies, the number of servers actually receiving training in the experimental groups was relatively low, often 50 to 60%. Hence, follow‐up observations of server behaviour had a good chance of being based on a number of untrained servers. In the health promotion studies, compliance was reported as 'variable'. Such a low or variable compliance is a problem for the assessment of intervention efficacy, but does indicate the effectiveness of such interventions, which is arguably of greater interest to public health intervention research.
It is difficult to quantify a sufficient length for a data collection period, but it should be long enough to account for short‐term fluctuations to provide a reliable estimate of outcome. Due to the relatively short length of follow‐up in most studies it is difficult to be confident that a change in outcome is a result of random fluctuation or if any real intervention effect lessens (or increases) over time.
A number of the included studies used a cluster design. A problem posed by cluster data arises from the fact that individuals within a cluster tend to be more similar to each other than to other members of other clusters. Failure to account for this can cause a type of 'unit of analysis error', which results in the P‐values being too small and the confidence intervals too narrow (Wears 2002), and can spuriously overestimate the significance of difference (Alderson 2002). Eight studies reported using appropriate statistical techniques to adjust for this cluster error in their analyses.
Of the variety of interventions that have the potential to be implemented in the server setting, much of the existing literature and intervention research focuses on just one: server training. Such an approach places the emphasis on the supply‐side of alcohol consumption and aims to enable servers to facilitate responsible drinking in their patrons. The approach assumes that an improvement in knowledge leads to an improvement in behaviour, which in turn will reduce the occurrence of injury. However, the appropriateness of this assumption might be questioned; behaviour is a complex concept and subject to multiple influences, knowledge being just one. For example, it is recognised that educational interventions are not effective in reducing alcohol consumption (Hope 2004), hence to assume that such an approach can change the behaviour of servers may be inappropriate.
The required large sample size is likely to be a main reason for the lack of injury outcome data in the included studies, with proxy measures such as behaviour used instead. However, it is unclear how observed behaviour is related to the occurrence of injury. Even if a causal relationship between behaviour and injury is assumed, there is no reliable effect estimates which would enable the prediction of the extent to which a given behaviour change reduces the rate of injury. For example, two of the studies of server training used server behaviour as the main outcome, reported as a behaviour score. It is difficult, however, to translate the practical implications of such a measure to injury risk and/or alcohol consumption. A previously published systematic review of primary prevention interventions for alcohol misuse in young people, by Foxcroft 2002, described the difficulty in judging relative effectiveness of different interventions, when the evaluations report different outcomes and the public health relevance of these different outcomes is unknown. Foxcroft 2002 highlighted the need for a systematic review of the evidence for subsequent alcohol‐related problems provided by such indicators, which should lead to greater clarity over the type of measures to be used in future evaluations.
The low rating of methodological quality of the included studies is undoubtedly a reflection of the numerous challenges posed by conducting research in this area; is it expected that many public health studies will never meet all of the criteria for quality (Jackson 2004). The nature of the interventions, participants and outcomes under investigation can prohibit elements of study design, such as blinding and randomisation, which are important elements for study validity. Thus our overall 'weak' rating may be unsurprising. However, it is important that researchers attempt to maximise their studies' validity, when it is feasible. For example, of the seven randomised trials included in this review, none reported using adequate allocation concealment; yet allocation concealment is always possible, irrespective of topic (Schulz 1994).
Potential biases in the review process
This systematic review addresses a focused research question using predefined inclusion criteria and methodology to select and appraise eligible studies.
As with all systematic reviews, the possibility of publication bias should be considered as a potential threat to validity. Identification of research for systematic reviews of public health interventions tends to require more complex searching than for reviews of medical interventions. The multi‐disciplinary nature of the research means that it is more widely scattered, with much published in the grey literature (Jackson 2005). In recognition of this, the search strategy for this systematic review involved searching multiple electronic databases from a range of disciplines (including two specifically of grey literature), checking of reference lists and contact with experts in the field, to identify all potentially eligible studies, published and unpublished. With such a comprehensive search strategy, the likelihood of having missed an important, relevant study is remote, thus the influence of publication bias on the findings of this systematic review can be discounted with reasonable confidence.
The included studies often used a number of outcome measures to examine intervention effectiveness; it was not possible for us to anticipate all of these when defining the inclusion criteria at the protocol stage. Therefore, for a small number of studies, we selected to report only the measures which we judge to be the most reliable and meaningful in contributing to the objectives of the review. Although these decisions were not made in reference to the results data, they are post hoc decisions and thus a potential weakness of this review.
The findings of this systematic review are limited by the overall poor methodological quality of the included studies; poorly designed and executed studies are susceptible to bias and can lead to either an over or under estimate of effect.
Several studies were conducted over a decade ago, so their relevance and generalisability to the present situation is questionable. An additional limitation is that no studies conducted in low and middle income countries were identified.
Agreements and disagreements with other studies or reviews
A previous systematic review by Shults 2001 examined the effectiveness of server training in reducing drink driving. Five controlled studies were included (Gliksman 1993; Holder 1994; Lang 1998; Russ 1987; Saltz 1987), three of which were non‐randomised designs with patron alcohol consumption as an outcome. The review concluded that 'there is sufficient evidence that face‐to‐face server training, when accompanied by strong and active management support, is effective in reducing the level of intoxication in patrons' and is 'likely to have a desirable effect on alcohol impaired driving if the affected patrons cease drinking or continue drinking in relatively safe environments after leaving the drinking establishment'. In addition to the five articles previously identified by Shults 2001, this present systematic review includes a further ten studies of server training, two of which were randomised trials measuring patron alcohol consumption as an outcome. The additional studies provide no good evidence that the intervention is effective in preventing injury or reducing patron alcohol consumption. Therefore the existence of 'sufficient evidence' for the effectiveness of server training in reducing alcohol intoxication might now be considered tentative.
Shults' review focused on trials of server training in reducing drink driving, no other systematic reviews of server setting interventions have been located to enable comparison.
Interventions such as server training, which effectively place responsibility of sensible alcohol consumption on the server, may be limited as an effective strategy due to the nature of the alcohol industry and server work. There are potential difficulties associated with interventions for which implementation is controlled by the alcohol industry; if interventions compromise profit margins, it is reasonable to suggest that the alcohol industry will resist their implementation, without the presence of incentives and/or legislation. Additionally, it should be considered that bar work is generally low paid, and is a profession with a high turnover of staff. Such a highly mobile workforce makes the process of training difficult, unless training was mandated and completion of training was a prerequisite for employment. Effective implementation amongst servers may also be resisted without financial reward for the additional responsibility placed upon them, in an already low paid and often stressful environment.
The relatively poor compliance with the interventions, particularly the server training interventions, may suggest a feeling of ambivalence or lack of belief in the benefits of intervention. Future studies should consider ways to improve uptake and intervention compliance, such as by involvement of relevant parties in the study design. Compliance with the assigned intervention is important. Non‐compliance reduces the statistical power of a trial to detect any true effect of the study intervention. In such cases it is not certain that an observed non‐significant effect is due to an ineffective intervention or to its incomplete implementation. This information also indicates the feasibility of delivering the intervention in the real life setting; if integrity of implementation in a study situation is low it is likely to be poor in practice (Jackson 2005). This apparent compliance problem may have implications for the effectiveness of policies outlined in the UK Government's 'Alcohol Harm Reduction Strategy for England' (Strategy Unit 2004), in which there is a focus on voluntary agreements with the alcohol industry in preference to a mandated approach. The findings of this systematic review suggests that it is likely that the UK Government will be required to take a firmer stance with the alcohol industry in the adoption of harm prevention policy, if any discernible effect is to be seen. However, the challenge is that usually an intervention is only likely to be made mandatory once evidence for effectiveness has been established. The Government's preference for a voluntary approach with the alcohol industry has lead to concern in regard to the lobbying influence of the industry on public policy (MacQueen 2004), which worryingly might be likened to that exhibited by the tobacco industry on anti‐smoking policy.
It is not the aim of this systematic review to make policy recommendations; policy making is a complex process in which examination of the evidence base, whilst crucial, is just one component. This review has been prepared recognising that different people interpret evidence differently; therefore the included studies have been reviewed and presented in a systematic and explicit way, so that readers are able to examine the evidence and reach their own conclusions, applicable to their own setting. A lack of evidence for effect of an approach should not necessarily prohibit its adoption; interventions in the server setting should be considered in relation to the effectiveness and cost‐effectiveness of alternative alcohol harm prevention interventions, in the context of the particular setting of interest.
Authors' conclusions
Implications for practice.
There is insufficient evidence from randomised controlled trials and well conducted non‐randomised studies to determine the effect of interventions in the alcohol server setting on injuries. Lack of compliance with the interventions seems to be a particular problem; hence mandated interventions or other incentives to improve compliance may be more likely to show an effect.
The apparent compliance problem is likely to have implications for the success of proposed strategies outlined in the Alcohol Harm Strategy for England, in which there is a preference for voluntary agreements with the alcohol industry in regard to intervention implementation. It is probable that such voluntary interventions will suffer limited uptake and thus have limited effect.
Implications for research.
The methodology of future evaluations needs to be improved. Randomised controlled trials, with adequate allocation concealment and blinding, are needed to improve the evidence base. Further well conducted non‐randomised trials are also needed, when random allocation is not feasible.
The focus of research should be broadened to investigate the effectiveness of interventions other than server training, where previous research dominates.
When the collection of injury outcome data is not feasible, research is needed to identify the most useful proxy indicators.
Finally, future studies should be designed with the aim of contributing to the evidence base, not simply as stand alone evaluations.
What's new
| Date | Event | Description |
|---|---|---|
| 15 June 2010 | New search has been performed | The searches have been updated to November 2008. Three additional studies have been added (Haworth 1997; Peltzer 2006; Toomey 2008); the text of the review has been amended accordingly. The review's main conclusions remain unchanged. |
History
Protocol first published: Issue 2, 2005 Review first published: Issue 2, 2006
| Date | Event | Description |
|---|---|---|
| 28 April 2008 | Amended | Converted to new review format. |
Acknowledgements
Thanks to Ian Roberts, Tim Collier and Julie Mytton for methodological support and Rebecca Ivers for managing the editorial processes for the review.
Thanks to Karen Blackhall for updating the databases searches for the June 2010 update.
Thanks also to the authors of the included studies for providing additional information on request, and to the peer referees for their helpful comments.
The development of this review was supported by funding from the Alcohol Education Research Council, UK.
Appendices
Appendix 1. Original search strategy 2004
Cochrane Injuries Group Specialised Register (September 2004) (alcohol* OR beer* OR wine* OR liquor* OR spirit* OR drink* OR drunk* OR intoxicat*) AND (serve* OR serving OR pub OR pubs OR bar OR bars OR nightclub* OR restaurant* OR staff* OR shop* OR sell OR selling OR sale OR supply* OR supplier* OR supplied OR purchas* OR licens* OR licenc*)
Cochrane Central Register of Controlled Trials (The Cochrane Library 2004, Issue 3) #1 ACCIDENTS #2 WOUNDS AND INJURIES #3 CRIME #4 AUTOMOBILE DRIVING #5 (injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abuse or abusive or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*:ti) #6 (injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abuse or abusive or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*:ab) #7 (poison* near alcohol*) #8 (#1 or #2 or #3 or #4 or #5 or #6 or #7) #9ALCOHOL DRINKING #10 ALCOHOLIC BEVERAGES #11 ALCOHOLIC INTOXICATION #12 (alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*:ti) #13 (alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*:ab) #14 (problem* next drink*) #15 (bing* near alcohol*) #16 (bing* near drink*) #17 (#9 or #10 or #11 or #12 or #13 or #14 or #15 or #16) #18 (serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*:ti) #19 (serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*:ab) #20 ((industr* near alcohol) or (industr* near beer) or (industr* near brewery) or (industr* near liquor) or (industr* near wine)) #21 (#18 or #19 or #20) #22 (educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*:ti) #23 (educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*:ab) #24 (#22 or #23) #25 (#8 and #17 and #21 and #24) #26 (#25 and (not pregnan*)) #27 (#26 and (not anorexi*)) #28 (#27 and (not (drink* near water*)))
MEDLINE (January 1966 to September 2004) #1 explode accidents #2 explode wounds and injuries #3 explode crime #4 explode automobile driving #5 injur* OR death* OR mortalit* OR fatalit* OR trauma* OR fall OR falls OR falling OR burn* OR fire* OR flame* OR drown* OR abus* OR violen* OR suffocat* OR fractur* OR laceration* OR ruptur* OR wound* OR scald* OR crash* OR accident* OR suicid* OR crim* OR disorder* OR offen* OR assault* OR murder* OR homicid* OR attack* OR stab OR stabbed OR stabbing* OR danger* OR drunk* OR driv* OR impair* OR convict* OR arrest* #6 poison* near alcohol* #7 #1 OR #2 OR #3 OR #4 OR #5 OR #6 #8 explode alcohol drinking #9 explode alcoholic beverages #10 explode alcoholic intoxication #11 alcohol* OR beer* OR wine* OR liquor* OR spirit* OR drink* OR drunk* OR intoxicat* #12 problem* near1 drink* #13 bing* near3 alcohol* #14 bing* near1 drink* #15 #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 #16 serve* OR serving OR pub OR pubs OR bar OR bars OR nightclub* OR restaurant* OR staff* OR shop* OR sell OR selling OR sale OR supply* OR supplier* OR supplied OR purchas* OR licens* OR licenc* #17 industr* near (alcohol OR beer OR brewery OR liquor OR wine) #18#16 OR #17 #19 explode intervention studies #20 educat* OR train* OR promot* OR interven* OR program* OR administer* OR campaign* OR evaluat* OR assess* OR control* OR compar* OR prevent* OR safe* OR strateg* OR scheme* OR incentive* OR trial* OR environment* #21 #19 OR #20 #22 #7 AND #15 AND #18 AND #21 #23 (tg=animals) NOT ((tg=human) and (tg=animals)) #24 #22 NOT #23 #25 #24 NOT (rat or rats) #26 #25 NOT pregnan* #27 #26 NOT anorexi* #28 #27 NOT (water near1 drink*) #29 #28 in ti #30 #28 in ab #31 #29 OR #30 #31 #29 OR #30
EMBASE (1980 to 2004, wk 36) 1 exp accidents/ 2 exp injuries/ 3 exp crime/ 4 exp car driving/ 5 (injur$ or death$ or mortalit$ or fatalit$ or trauma$ or fall or falls or falling or burn$ or fire$ or flame$ or drown$ or abus$ or violen$ or suffocat$ or fractur$ or laceration$ or ruptur$ or wound$ or scald$ or crash$ or accident$ or suicid$ or crim$ or disorder$ or offen$ or assault$ or murder$ or homicid$ or attack$ or $0stab$1 or stabbed or stabbing$ or danger$ or drunk$ or driv$ or impair$ or convict$ or arrest$).ti,ab. 6 (poison$ adj3 alcohol$).mp. 7 1 or 2 or 3 or 4 or 5 or 6 8 exp alcohol drinking/ 9 exp alcoholic beverages/ 10 exp alcoholic intoxication/ 11 (alcohol$ or beer$ or wine$ or liquor$ or spirit$ or drink$ or drunk$ or intoxicat$).ti,ab. 12 (problem$ adj drink$).mp. 13 (bing$ adj3 alcohol$).mp. 14 (bing$ adj drink$).mp. 15 8 or 9 or 10 or 11 or 12 or 13 or 14 16 ($0serve$1 or $0serving or pub$1 or bars$1 or nightclub$ or restaurant$ or staff$ or shop$ or sell or selling or sale or supply$ or supplier$ or supplied or purchas$ or licens$ or licenc$).ti,ab. 17 (industr$ adj (alcohol or beer or brewery or liquor or wine)).mp. 18 16 or 17 19 exp intervention studies/ 20 (educat$ or train$ or promot$ or interven$ or program$ or administer$ or campaign$ or evaluat$ or assess$ or control$ or compar$ or prevent$ or safe$ or strateg$ or scheme$ or incentive$ or trial$ or environment$).ti,ab. 21 19 or 20 22 7 and 15 and 18 and 21 23 22 not (rat or rats).mp. 24 23 not pregnan$.mp. 25 24 not anorexi$.mp. 26 25 not (drink$ adj2 water).mp.
PsycINFO (September 2004) #1 explode "Accidents‐" in MJ,MN #2 explode "Injuries‐" in MJ,MN #3 explode "Crime‐" in MJ,MN #4 explode "Motor‐Vehicles" in MJ,MN #5 injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abus* or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest* #6 poison* near alcohol* #7 #1 or #2 or #3 or #4 or #5 or #6 #8 explode "Alcohol‐Drinking‐Attitudes" in MJ,MN #9 explode "Alcohol‐Drinking‐Patterns" in MJ,MN #10 explode "Alcohol‐Intoxication" in MJ,MN #11 explode "Alcoholic‐Beverages" in MJ,MN #12 alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat* #13 problem* near1 drink* #14 bing* near3 alcohol* #15 bing* near1 drink* #16 #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 #17 serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc* #18 industr* near (alcohol or beer or brewery or liquor or wine) #19 #17 or #18 #20 educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment* #21 #7 and #16 and #19 and #20 #22 #21 not pregnan* #23 #24 not anorexi* #24 #23 in ti #25 #23 in ab #26 #24 or #25
SIGLE (1980 to 2004/06) #1 explode "Accidents‐" / all SUBHEADINGS in MIME,MJME #2 explode " Wounds‐and‐Injuries" / all SUBHEADINGS in MIME,MJME #3 explode "Crime‐" / all SUBHEADINGS in MIME,MJME #4 explode "Automobile‐Driving" / all SUBHEADINGS in MIME,MJME #5 injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abus* or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest* #6 poison* near alcohol* #7 #1 or #2 or #3 or #4 or #5 or #6 #8 explode "Alcohol‐Drinking" / all SUBHEADINGS in MIME,MJME #9 explode ""Alcoholic‐Beverages" / all SUBHEADINGS in MIME,MJME #10 explode " Alcoholic‐Intoxication" all SUBHEADINGS in MIME,MJME #11 alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*(4521 records) #12 problem* near1 drink* #13 bing* near3 alcohol* #14 bing* near1 drink* #15 #8 or #9 or #10 or #11 or #12 or #13 or #14 #16 serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc* #17 industr* near (alcohol or beer or brewery or liquor or wine) #18 #16 or #17 #19 educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment* #20 #7 and #15 and #18 #21 #19 or #20
SPECTR (September 2004)
#2 {injur*} OR {death*} OR {mortalit*} OR {fatalit*} OR {trauma*} OR {fall} OR {falls} OR {falling} OR {burn*} OR {fire*} OR {flame*} OR {drown*} OR {abus*} OR {violen*} OR {suffocat*} OR {fractur*} OR {laceration*} OR {ruptur*} OR {wound*} OR {scald*} OR {crash*} OR {accident*} OR {suicid*} OR {crim*} OR {disorder*} OR {offen*} OR {assault*} OR {murder*} OR {homicid*} OR {attack*} OR {stab} OR {stabbed} OR {stabbing*} OR {danger*} OR {drunk*} OR {driv*} OR {impair*} OR {convict*} OR {arrest*} #3 #1 AND #2
We also searched the following databases using selected search terms from the above strategies;
ERIC (1966 to September 2004) ETOH (January 2005) National Research Register (issue 3/2004) Science (and Social Science) citation index (September 2004) TRANSPORT (1988‐2004/06) Zetoc (1993 to September 2004)
Appendix 2. Search strategy November 2008
Cochrane Injuries Group Specialised Register (searched Nov 2008) (alcohol* OR beer* OR wine* OR liquor* OR spirit* OR drink* OR drunk* OR intoxicat*) AND (serve* OR serving OR pub OR pubs OR bar OR bars OR nightclub* OR restaurant* OR staff* OR shop* OR sell OR selling OR sale OR supply* OR supplier* OR supplied OR purchas* OR licens* OR licenc*)
Cochrane Central Register of Controlled Trials (The Cochrane Library 2008, Issue 4) #1MeSH descriptor Accidents explode all trees MeSH descriptor Wounds and Injuries explode all trees #2MeSH descriptor Crime explode all trees #3MeSH descriptor Automobile Driving explode all trees #4(injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abuse or abusive or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*:ti,ab) #5(poison* near alcohol*) #6(#1 OR #2 OR #3 OR #4 OR #5 OR #6) #7MeSH descriptor Alcohol Drinking explode all trees #8MeSH descriptor Alcoholic Intoxication explode all trees #9MeSH descriptor Alcoholic Beverages explode all trees #10(alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*):ti,ab #11(problem* next drink*) #12(bing* near alcohol*) #13(bing* near drink*) #14(#8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14) #15(serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*):ti,ab #16((industr* near alcohol) or (industr* near beer) or (industr* near brewery) or (industr* near liquor) or (industr* near wine)) #17(#16 OR #17) #18(educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*):ti,ab #19(#7 AND #15 AND #18 AND #19) #20(#20 AND NOT pregnan*) #21(#21 AND NOT anorex*) #22(#22 AND NOT ( drink* NEAR/6 water* ))
MEDLINE (1950 to Nov 2008) 1.exp Accidents/ 2.exp "Wounds and Injuries"/ 3.exp Crime/ 4.exp Automobile Driving/ 5.(injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abus* or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*).ab,ti. 6.(poison* adj3 alcohol*).ab,ti. 7.1 or 2 or 3 or 4 or 5 or 6 8.exp Alcohol Drinking/ 9.exp Alcoholic Beverages/ 10.exp Alcoholic Intoxication/ 11.(alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*).ab,ti. 12.(problem* adj3 drink*).ab,ti. 13.(bing* adj3 alcohol*).ab,ti. 14.(bing* adj3 drink*).ab,ti. 15.8 or 9 or 10 or 11 or 12 or 13 or 14 16.(alcohol* and (serve* or serving or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*)).ab,ti. 17.(pub or pubs or bar or bars or nightclub* or restaurant*).ab,ti. 18.(industr* adj5 (alcohol or beer or brewery or liquor or wine)).ab,ti. 19.16 or 17 or 18 20.7 and 15 and 19 21.exp Intervention Studies/ 22.prevention & control.fs. 23.(educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*).ti. 24.21 or 22 or 23 25.20 and 24 26.exp animals/ not (exp humans/ and exp animals/) 27.(rat or rats).ab,ti,sh. 28.26 or 27 29.25 not 28 30.pregnan*.ab,ti,sh. 31.29 not 30 32.anorex*.ab,ti,sh. 33.31 not 32 34.(drink* adj2 water).ab,ti. 35.33 not 34 36.(2004* or 2005* or 2006* or 2007* or 2008*).ed. 37.35 and 36
EMBASE (1980 to Nov 2008) 1.exp accidents/ 2.exp Injury/ 3.exp Crime/ 4.exp Car Driving/ 5.(injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abus* or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab* or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*).ti,ab. 6.(poison* adj3 alcohol*).ti,ab. 7.1 or 2 or 3 or 4 or 5 or 6 8.exp Drinking Behavior/ 9.exp Alcoholic Beverage/ 10.exp Alcohol Intoxication/ 11.exp alcohol consumption/ 12.(alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*).ti,ab. 13.(problem* adj3 drink*).ti,ab. 14.(bing* adj3 alcohol*).ti,ab. 15.(bing* adj3 drink*).ti,ab. 16.8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 17.(alcohol* and (serve* or serving or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*)).ti,ab. 18.(pub* or bars* or nightclub* or restaurant*).ab,ti. 19.(industr* adj5 (alcohol or beer or brewery or liquor or wine)).ab,ti. 20.17 or 18 or 19 21.exp Intervention Study/ 22.(educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*).ti. 23.*"Prevention and Control"/ 24.exp Prevention Study/ 25.21 or 22 or 23 or 24 26.7 and 16 and 20 and 25 27.exp Animal/ not (exp Human/ and exp Animal/) 28.(rat or rats).ab,ti,sh. 29.27 or 28 30.26 not 29 31.pregnan*.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name] 32.anorex*.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name] 33.(drink* adj3 water).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name] 34.31 or 32 or 33 35.30 not 34
PsycINFO 1806 to Nov 2008 1.exp Accidents/ 2.exp PEDESTRIAN ACCIDENTS/ 3.exp HOME ACCIDENTS/ 4.exp MOTOR TRAFFIC ACCIDENTS/ 5.exp TRANSPORTATION ACCIDENTS/ 6.exp INJURIES/ 7.exp CRIME/ 8.(injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abuse or abusive or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*).ti. 9.(poison* adj3 alcohol*).ti,ab. 10.1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 11.exp Alcohol‐Drinking ‐Attitudes/ 12.exp Alcohol Drinking Patterns/ 13.exp Alcoholic Beverages/ 14.exp Alcohol Intoxication/ 15.(alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*).ab,ti. 16.(problem* adj3 drink*).ab,ti. 17.(bing* adj3 alcohol*).ab,ti. 18.(bing* adj3 drink*).ab,ti. 19.11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 20.(alcohol* and (serve* or serving or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*)).ab,ti. 21.(pub or pubs or bar or bars or nightclub* or restaurant*).ab,ti. 22.(industr* adj5 (alcohol or beer or brewery or liquor or wine)).ab,ti. 23.20 or 21 or 22 24.10 and 19 and 23 25.exp PROGRAM EVALUATION/ 26.(educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*).ti. 27.exp Treatment Effectiveness Evaluation/ 28.exp experimental design/ 29.25 or 26 or 27 or 28 30.24 and 29 31.(pregnan* or anorex* or (drink* adj3 water)).mp. [mp=title, abstract, heading word, table of contents, key concepts] 32.30 not 31 33.exp ANIMALS/ 34.(rat or rats).mp. [mp=title, abstract, heading word, table of contents, key concepts] 35.33 or 34 36.32 not 35 PsycEXTRA 1908 to Nov 2008 1.exp PEDESTRIAN ACCIDENTS/ or exp INDUSTRIAL ACCIDENTS/ or exp ACCIDENTS/ or exp HOME ACCIDENTS/ or exp TRANSPORTATION ACCIDENTS/ or exp MOTOR TRAFFIC ACCIDENTS/ 2.exp ELECTRICAL INJURIES/ or exp SPINAL CORD INJURIES/ or exp INJURIES/ or exp HEAD INJURIES/ 3.exp CRIME PREVENTION/ or exp CRIME/ or exp VIOLENT CRIME/ or exp CRIME VICTIMS/ 4.(injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abuse or abusive or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* or crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest*).mp. [mp=title, abstract, heading word, keywords] 5.(poison* adj3 alcohol*).mp. [mp=title, abstract, heading word, keywords] 6.4 or 1 or 3 or 2 or 5 7.exp Alcoholism/ or exp Alcohol Drinking Patterns/ or exp Alcohol Abuse/ 8.exp Alcoholic Beverages/ 9.exp Alcohol Intoxication/ 10.(alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*).ab,ti. 11.(problem* adj3 drink*).ab,ti. 12.(bing* adj3 alcohol*).ab,ti. 13.(bing* adj3 drink*).ab,ti. 14.7 or 8 or 9 or 10 or 11 or 12 or 13 15.(alcohol* and (serve* or serving or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*)).ab,ti. 16.(pub or pubs or bar or bars or nightclub* or restaurant*).ab,ti. 17.(industr* adj5 (alcohol or beer or brewery or liquor or wine)).ab,ti. 18.16 or 17 or 15 19.6 and 18 and 14 20.exp PROGRAM EVALUATION/ 21.(educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*).ti,ab. 22.exp Treatment Effectiveness Evaluation/ 23.exp experimental design/ 24.22 or 21 or 23 or 20 25.24 and 19 26.(pregnan* or anorex* or (drink* adj3 water)).mp. [mp=title, abstract, heading word, keywords] 27.25 not 26 28.exp ANIMALS/ 29.27 not 28 ISI Web of Science: Science Citation Index Expanded (SCI‐EXPANDED) 1970 to Nov 2008, Social Sciences Citation Index (SSCI)1970 to Nov 2008, Conference Proceedings Citation Index‐ Science (CPCI‐S) 1990 to Nov 2008 1.TI=(((serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*) or (industr* and alcohol*) or (industr* and beer) or (industr* and brewer*) or (industr* and liquor) or (industr* and wine))) AND TS=((educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*)) 2.TS=((injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or violen* or fractur* or laceration* or wound* or accident* or attack* or stab or stabbed or stabbing*) or ((drink* or drunk*) and driv*)) AND TS=((alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*) or (drink* and problem*) or (bing* and (alcohol* or drink))) NOT TS=(pregnan* or anorex* or (drink* and water)) 3.1 and 2 4.TS=(((serve* or serving or pub or pubs or bar or bars or nightclub* or restaurant* or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*) or (industr* and alcohol*) or (industr* and beer) or (industr* and brewer*) or (industr* and liquor) or (industr* and wine))) AND TS=((alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat*) or (drink* and problem*) or (bing* and (alcohol* or drink))) NOT TS=(pregnan* or anorex* or (drink* and water)) 5.TI=((injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or violen* or fractur* or laceration* or wound* or accident* or attack* or stab or stabbed or stabbing*) or ((drink* or drunk*) and driv*)) AND TS=((educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment*)) 6.4 and 5 7.3 or 6 TRANSPORT (CD) 1988 to 2007/06 #1injur* or death* or mortalit* or fatalit* or trauma* or fall or falls or falling or burn* or fire* or flame* or drown* or abus* or violen* or suffocat* or fractur* or laceration* or ruptur* or wound* or scald* or crash* or accident* or suicid* #2crim* or disorder* or offen* or assault* or murder* or homicid* or attack* or stab or stabbed or stabbing* or danger* or drunk* or driv* or impair* or convict* or arrest* #3#1 or #2 #4alcohol* or beer* or wine* or liquor* or spirit* or drink* or drunk* or intoxicat* #5problem* near drink* #6bing* near alcohol* #7bing* near drink* #8#4 or #5 or #6 or #7 #9#3 and #8 #10 pub or pubs or bar or bars or nightclub* or restaurant* #11 Alcohol* and (serve* or serving or staff* or shop* or sell or selling or sale or supply* or supplier* or supplied or purchas* or licens* or licenc*) #12 #10 or #11 #13 educat* or train* or promot* or interven* or program* or administer* or campaign* or evaluat* or assess* or control* or compar* or prevent* or safe* or strateg* or scheme* or incentive* or trial* or environment* #14 #9 and #12 and #13 #15Interlock* #16#14 NOT #15
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Boots 1995.
| Methods | Non‐randomised controlled trial, unit of allocation = town. | |
| Participants | Western Australia. Experimental = one town, Geraldton. Control = one town, Bunbury. | |
| Interventions | Health promotion intervention The 'Partysafe' campaign conducted in December 1993, for 23 days until New Year's day. Aim to encourage the responsible serving of alcohol at parties by providing 'Partysafe' Christmas cards with every purchase of takeaway liquor. The cards listed four tips for having a safe party; 1) Provide food 2) Ensure that non‐alcoholic and low alcoholic drinks are available 3) Serve alcohol responsibly 4) Consider guests' transport needs. The tips were also featured in local media. Ten licensed liquor takeaway premises in Geraldton participated in the 'Partysafe campaign'. Bunbury received no intervention. | |
| Outcomes | Drinkers' self‐reported knowledge and behaviour, collected by random telephone interviews of town residents. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | The experimental town (Geelong) was assigned to the intervention as it was at high risk for alcohol‐related problems. The control town (Bunbury) was selected on the basis of being of a similar size to the experimental town. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Unclear risk | Not reported. |
| Confounders | Unclear risk | Geelong was reported as having a high rate of per capita drinking, drink driving charges, alcohol‐related hospital admission, alcohol‐related injuries and alcohol consumption occurring in the private setting. |
| Data collection methods | Unclear risk | Knowledge and behaviour data were collected by random telephone interviews. Response rate in experimental and control area were 63% and 56% respectively. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | 10/11 licensed takeaway premises in the experimental area participated, but it is reported that the 'level of implementation varied'. |
| Duration of follow‐up | Unclear risk | Length of the data collection period is not reported. |
Buka 1999.
| Methods | Non‐randomised controlled trial, unit of allocation = community. | |
| Participants | Rhode Island; USA. Three communities; one experimental and two control sites. Experimental = containing 51 bars Control site A = containing 26 bars Control site B = containing 26 bars | |
| Interventions | Server training
CAAIPP alcohol server training. Twenty‐four training courses were held, each lasting five hours, with 5‐15 servers attending each course. The training curriculum was developed from the National Highway Traffic Safety Administration. The training emphasised training by peer servers; each session was co‐facilitated by a server and an alcohol treatment/prevention professional from the community. The purpose of the training was to provide servers with the knowledge and skills required to prevent patrons from becoming intoxicated, prevent service of alcohol to minors, identify and stop service to intoxicated patrons and help prevent injuries to those individuals as well as informing servers of their legal liability if they fail to obey dram shop laws. Control communities were not exposed to CAAIPP training. |
|
| Outcomes | Self reported server behaviour, measured by a Desired Server Behaviour Index. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | Three communities, one of which was reported as being selected at random to be the experimental site and the remaining two sites were used as controls. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Unclear risk | Not reported. |
| Confounders | Unclear risk | The communities were reported as being similar in regard to vital statistics, hospital discharge data and police statistics on motor vehicle crashes and arrests. The communities were of comparable size, sociodemographic characteristics, prevalence of alcohol‐related problems and levels of institutional development and community organisation. |
| Data collection methods | Unclear risk | Self‐reported server behaviour was measured by questionnaire. From a sample of 25 premises from each control site and 50 experimental premises, three servers were randomly selected to complete the questionnaire. Response rates for questionnaires was 68% in the experimental area (31% of these were from trained servers), 72% in control A and 63% in control B. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | Of 531 servers in the experimental community, 324 (61%) completed the intervention. |
| Duration of follow‐up | Unclear risk | Data were collected four years after intervention. |
Casteel 2004.
| Methods | Controlled before and after study, unit of allocation = liquor stores | |
| Participants | Santa Monica, CA; USA Experimental = 9 liquor stores. Control = 13 liquor stores. | |
| Interventions | Environmental intervention
Based on Crime Prevention Through Environmental Design concepts (that criminal activity can be reduced by modifying the business environment). Basic elements included keeping a minimal amount of cash in the till, ensuring good visibility into and out of premises, bright interior and exterior lighting, escape routes and training of employees in how to respond to robbery and shoplifting events. From a baseline assessment, an individualised safety plan was designed. Stores also received manuals, copy of the plan and other educational materials. The Californian Occupational Safety & Health Administration implemented the intervention. Control premises received no intervention. |
|
| Outcomes | Injury (criminal activity) obtained from police records. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | After invitation to participate in the study, stores that agreed were used as the experimental group; those that refused were used as the control group. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Low risk | Outcome data were obtained from the Crime Analysis Unit of the Santa Monica Police Department. |
| Confounders | Unclear risk | Control stores were reported as being located in higher crime areas than experimental, no other information given. |
| Data collection methods | Unclear risk | Extracted from police records. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | It is reported that there was variation in the extent to which experimental stores complied with the intervention. |
| Duration of follow‐up | Unclear risk | Data were collected for 4.5 years before and 2 years after intervention implementation. |
Felson 1997.
| Methods | Controlled before and after study, unit of allocation = area. | |
| Participants | Victoria, Australia. Experimental=City of Geelong. Control=Greater Geelong and the metropolitan area of six other Victorian cities (Warrnambool, Mildura, Ballarat, Bendigo, Wangaratta, Morwell). | |
| Interventions | Policy intervention Twelve‐point policy for preventing bar‐hopping and reducing violence and other crime in and around licensed premises. Development of a policy (the Accord) for premises. The focus of the policy was to reduce the movement of patrons among bars and attempt to reduce overall alcohol consumption of patrons, and contain that consumption within safer settings. Policy provisions; 1) cover charges to entry after 11.00pm 2) denial of free re‐entry to those who had exited 3) no free drinks 4) limitations on promotions 5) no extended happy‐hours 6) uniform minimum price per drink 7) enforcing of bylaws against drinking or possession of open liquor containers on the streets 8) seizing faked, altered or borrowed ID cards misused by young people 9) issuing summons for use of illegal ID cards 10) alcohol‐free entertainment provided for underage youths on selected premises 11) calling taxis or friends for rides homes 12) uniform adherence to liquor laws by service personnel. Implementation of policy was led by the police | |
| Outcomes | Injury (serious assault rate) obtained from police records. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | The experimental city was chosen in response to a 'pub‐hopping' and associated crime problem. The metropolitan area of six other cities from the same state, used as the control. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Unclear risk | Serious assault data were obtained from police reports (NB the police took a lead in implementing intervention). |
| Confounders | Unclear risk | The pre‐intervention serious assault rate was higher in the intervention area; rate per 100,000 population, was 117 for the experimental city and 77 for the control. |
| Data collection methods | Unclear risk | Extracted from police records. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | Compliance with intervention is not reported. |
| Duration of follow‐up | Unclear risk | Data collection periods were one year pre and four years post‐intervention. |
Gliksman 1993.
| Methods | Randomised controlled trial, unit of allocation = bar. | |
| Participants | Thunder Bay, Ontario; Canada. Experimental = 4 bars Control = 4 bars | |
| Interventions | Server training
Server intervention training developed by the Addiction Research Foundation of Ontario. Managers were informed of their legal obligations and encouraged to establish policies for the sale of alcohol in their establishments. The servers were then familiarised with the new policy and instructed in responsible serving practices. The emphasis of the programme was on preventing intoxication rather than intervening once a patron has reached intoxication. Control bars received no intervention. |
|
| Outcomes | Knowledge (measured in trained only) using questionnaires. Observed server behaviour (using pseudo‐drunks). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | Four pairs of matched bars; one bar from each pair was randomly selected to receive the intervention, no further details are presented. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Low risk | Pseudo‐drunks and observers were blind to allocation status. |
| Confounders | Unclear risk | The premises were chosen to represent four types of establishment; each type represented by two bars, matched on type of liquor licence, characteristics of clientele, location, volume of business and atmosphere. |
| Data collection methods | Unclear risk | 1) Knowledge and attitudes were measured, in the trained servers only, by questionnaires. The knowledge questionnaire was completed for 55/57 and the attitudes questionnaire completed for 57/57. 2) Observations of server behaviour using pseudo‐drunks were conducted with trained actors and observers on standardised days and times using standardised forms. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | 57 servers in the experimental group received trained. |
| Duration of follow‐up | Unclear risk | 1) Knowledge and attitudes were measured immediately before and after the intervention. 2) Observations were made in all eight bars two weeks before and after the intervention. |
Graham 2004.
| Methods | Randomised controlled trial, unit of allocation = bar | |
| Participants | Toronto, Canada Experimental = 26 bars Control = 12 bars | |
| Interventions | Server training The 'Safer Bars' intervention, aim to reduce aggression in bars. Two main components; 1) risk assessment workbook (alerting environmental factors); this was drawn directly from published research on alcohol‐related aggression; alerted the bar owner to environmental factors e.g. potential problems relating to the floor plan of the bar and the role of environmental expectations. 2) three hour training programme also drawn from bar‐room research, to identify common types of incidents of aggression and staff behaviours contributing to aggression as well as staff behaviours that are effective in avoiding and defusing aggression. The training covered; i) recognising the early signs of aggression and intervening early ii) assessing the situation and planning a response iii) techniques for preventing loss of control due to anger iv) body language and non‐verbal techniques v) responding to problem situations vi) legal issues relating to managing aggression and problem behaviour Staff were paid for participation in the study. | |
| Outcomes | Observed aggression exhibited by patrons and staff. | |
| Notes | Analyses were adjusted for clustering using Hierarchical Linear Modelling (HLM). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | 26 bars were randomly assigned by drawing lots to receive the intervention, the remaining served as controls. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Low risk | Observers were blind to allocation status of the bar. Control bars were unaware of their allocation status. |
| Confounders | Unclear risk | Prior to assignment, bars were stratified according to location, type, size plus ethnicity and age of patrons. |
| Data collection methods | Unclear risk | Data were obtained from 734 pre and post observations were made by paired of trained observers. Agreement among raters found to be generally high. |
| Withdrawals & dropouts | Unclear risk | Eight bars dropped out after assignment to experimental group and were not included in the analysis. |
| Intervention integrity | Unclear risk | Participation rate in the training was 84% of staff. |
| Duration of follow‐up | Unclear risk | Observations were made six months before and after intervention. The percentage of staff that received training and were still employed at the same bar varied from 18.5% to 100% (mean 61.2%). |
Haworth 1997.
| Methods | Non‐randomised controlled trial. | |
| Participants | 29 drinking venues in Melbourne where public breathalysers were available. | |
| Interventions | Two levels of intervention to promote use of the public breathalysers, at three levels of breathalyser cost. | |
| Outcomes | Use of breathalysers by ‘intending drivers’. | |
| Notes | Published outcome data cannot be interpreted. Data shown only as bar charts and actual figures not supplied. Also it is stated that there was no promotional activity in the control venues but the outcome data for the control group is shown by promotion level. One author (Vulcan) was contacted but no longer has original data. Other authors cannot be traced. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | Hotels Association provided list of potential participants. No information provided as to how venues were allocated to the control or intervention groups. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Unclear risk | No information reported. |
| Confounders | Unclear risk | Not reported. |
| Data collection methods | Low risk | Use of breathalyser machines as recorded on these devices. |
| Withdrawals & dropouts | Unclear risk | Number of venues appears to be greater post‐intervention than pre‐intervention. |
| Intervention integrity | Unclear risk | No information reported as to whether promotion activities were completed at all interventions. |
| Duration of follow‐up | Unclear risk | From the information reported, it is not possible to determine how long data was recorded following the promotional activity. |
Holder 1994.
| Methods | Controlled before and after study, unit of allocation = US State | |
| Participants | USA Experimental = Oregon state Control = 47 remaining US states | |
| Interventions | Server training Mandated server training policy versus no mandated server training policy. The one day training course covered seven areas; 1) effect of alcohol on the body 2) interaction effects of alcohol with other drugs (prescription and illicit) 3) problem drinking and alcoholism 4) state of Oregon's service laws 5) drinking and driving laws in Oregon and legal liability issues 6) effective server intervention techniques 7) alcohol marketing practices for responsible alcohol service A standardised written test must be passed by all participants to obtain a permit to serve alcohol. | |
| Outcomes | Injury (single vehicle night‐time crashes) obtained from official records. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | US state of Oregon which had introduced a mandated responsible server training policy (in December 1986) acted as the experimental site with data from other 47 US states used as control. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Low risk | Crash data were obtained from the Oregon Highway Division and the Fatal Accident Reporting system of the US Department of Transport. |
| Confounders | Unclear risk | Not reported. |
| Data collection methods | Unclear risk | Extracted from official records. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | N/A |
| Duration of follow‐up | Unclear risk | Crash data were collected for 11 years before and two years after introduction of the policy. |
Howard‐Pitney 1991.
| Methods | Non‐randomised controlled trial, unit of allocation = bar | |
| Participants | Utah, USA. Experimental = 26 premises Control = 14 premises | |
| Interventions | Server training One‐day training session. Servers and managers attended separate programmes that taught the physical and behavioural effects of alcohol and strategies for providing a more responsible alcohol service; taught the physical and behavioural effects of alcohol, and strategies for providing more responsible alcohol service. Managers received instruction on developing company policies to change the drinking environment. | |
| Outcomes | Observed server behaviour. Knowledge (in trained group only) measured using questionnaires. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Ninety‐seven servers from 26 different establishments attended training were used as the intervention group. Control premises (n=14) were 'randomly selected'. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Low risk | The observers were blind to allocation status and the servers were unaware that they were being observed. |
| Confounders | Unclear risk | Control premises were matched on premise type and size. Any differences at baseline between the groups were not reported. |
| Data collection methods | Unclear risk | Knowledge was assessed in trained servers only using a questionnaire before and after training. Server behaviour was measured by pairs of trained observers. Observations were made in 13 of 21 establishments with trained managers and 11 of 14 control premises. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | Not reported. |
| Duration of follow‐up | Unclear risk | Length of before and after periods of administration of knowledge questionnaire was not stated. Observations took place 4‐6 weeks after intervention. |
Johnsson 2003.
| Methods | Randomised controlled trial, unit of allocation = bar. | |
| Participants | Lund University, Sweden Experimental = six student bars Control = six student bars | |
| Interventions | Server training
Training programme based on the Alcohol Skills Training Program (ASTP) and the Swedish version of the Responsible Beverage Service. Bartenders in 'key positions' attended educational programme (n=40), these participants were responsible for the total amount of alcohol served in the bar during an evening, responsible for spreading the educational programme to their colleagues, responsible for creating guidelines for serving beverages responsibly. The focus of the programme was on the servers' own reaction to alcohol. Control received no server training. |
|
| Outcomes | Patron behaviour (alcohol consumption, determined by breath tests). | |
| Notes | Not professional servers (did not receive monetary payment for service). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | Randomisation was stratified for number of members of each bar. Six of 12 student bars at Lund University were allocated by drawing lots to the intervention group, remaining six were used as the control group. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Low risk | Those conducting the breath tests were not aware of allocation status. |
| Confounders | Unclear risk | Any differences in baseline between the groups were not reported. |
| Data collection methods | Unclear risk | Patron intoxication was measured at baseline and one month after intervention, by breath test in invited and consenting patrons. 664 tests were made at baseline, one patron refused. 658 tests were made at follow‐up (360 in experimental, 298 in control), there were no refusals. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | Forty staff in 'key positions' from experimental bars were trained. |
| Duration of follow‐up | Unclear risk | Follow‐up data were collected one month after intervention. |
Krass 1994.
| Methods | Randomised controlled trial, unit of allocation = bar. | |
| Participants | Waverley, Australia. Experimental = 4 bars Control = 4 bars | |
| Interventions | Server training
Four hour training package for all staff of licensed alcohol serving establishments. The aim of which was to equip participants with the knowledge and skills necessary to comply with the Liquor Act and to develop responsible service practices within licensed premises.
Topics included in the package;
1) The New South Wales Liquor Act
2) Definition of Responsible Hospitality Practices
3) Identification of Responsible Hospitality Practices
4) Facts about alcohol
5) Responsible promotions
6) Preventing under‐age drinking
7) Recognising intoxication
8) Preventing harmful consequences of intoxication
9) Skills for the refusal or modification of requested service. Control group received no server training. |
|
| Outcomes | Behaviour of patrons (alcohol consumption, measured by breath test and interview). Knowledge (in trained group only) measured using questionnaires. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | Eight premises agreed to participate. The bars were matched into pairs and then one from each pair was assigned at random to the experimental group. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Unclear risk | Interviewers were blind to allocation status. |
| Confounders | Unclear risk | Bars were matched in pairs according to size and type of clientele prior to intervention assignment. |
| Data collection methods | Unclear risk | Knowledge was measured in the trained servers only using pre and post questionnaire, 66 completed. Exit surveys of a sample of patrons involving a breath test and interview. 233 pre‐test patron interviews were made at five sites (response rate=40%), 305 post‐test interviews at four sites (response rate=53%). Observed estimates of BAC of patrons who refused to participate were made to assess volunteer bias. |
| Withdrawals & dropouts | Unclear risk | Three bars withdrew from the baseline patron exit surveys and four withdrew from the follow‐up surveys. |
| Intervention integrity | Unclear risk | 70 servers were trained. |
| Duration of follow‐up | Unclear risk | Knowledge questionnaire administered immediately before and after training. Patron exits surveys were conducted four weeks after intervention. |
Lacey 2000.
| Methods | Controlled before and after study, unit of allocation = area. | |
| Participants | USA Experimental = Pitney County, Colorado Control = two nearby jurisdictions | |
| Interventions | Drink driving service
'Tipsy Taxi' service (operated 24 hours a day, 365 days a year) providing a free ride home for persons too intoxicated to drive. Service offered by bar employee or request made to bar employee by patron. Control areas had no such service. |
|
| Outcomes | Injury (crashes), source of data not reported. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Since 1983 Pitney County, Colorado has had a 'Tipsy Taxi' service. Two nearby comparison jurisdictions were used as controls. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Unclear risk | Not reported. |
| Confounders | Unclear risk | Comparison jurisdictions had similar socioeconomic status and DUI enforcement systems to the experimental area. |
| Data collection methods | Unclear risk | Not reported. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | N/A |
| Duration of follow‐up | Unclear risk | Crash data collected for the period 1976‐1998 (7 years before and 15 year after intervention). |
Lang 1998.
| Methods | Non‐randomised controlled trial, unit of allocation = bar. | |
| Participants | Australia Experimental = 7 premises. Control = 7 premises. | |
| Interventions | Server training Responsible service training programme, approximately 1‐2 hours long. Participants were paid their regular hourly rate to attend. Core components; 1) laws regarding the serving of juveniles and drunken people 2) recognising the signs of intoxication 3) strategies for dealing with drunken customers* 4) alcohol and its effect 5) developing responsible house policies* (*elements were not fully covered in all training workshops and in some cases omitted) | |
| Outcomes | Drink driving offences (obtained from police reports). Behaviour of patrons (alcohol consumption, measured by breath test). Self‐reported server behaviour (measured by questionnaires). Observed server behaviour (using pseudo‐drunks). Knowledge (in trained servers only) measured by questionnaires. | |
| Notes | Inconsistencies in the standard of training and coverage of topics reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Seven out of 50 bars which were eligible and agreed to participate were used as the experimental group. Seven control bars were then selected. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Low risk | Research assistants and pseudo‐patrons were not informed of the design of the study or allocation status. Drink driving data were obtained from police reports. |
| Confounders | Unclear risk | The control bars were each selected to match one of the experimental bars according to risk status, licence type and total alcohol purchases. |
| Data collection methods | Unclear risk | Knowledge questionnaire, 56.9% of the trained servers completed the follow‐up questionnaire. Observations of server behaviour using actors as pseudo‐drunks made at each site pre and post intervention, total of 78 visits made. Drink driving data were extracted from official records. Patron interviews, overall 2375/3191 of patrons consented to be surveyed (74.4%). For refusals an observed assessment of drunkenness was recorded. |
| Withdrawals & dropouts | Unclear risk | One experimental bar refused to participate in the patron exit surveys. |
| Intervention integrity | Unclear risk | 61% of available servers were trained, at follow‐up 25 of trained servers had left their job. |
| Duration of follow‐up | Unclear risk | Knowledge questionnaires were administered before and three months after intervention. Observations of server behaviour were made before (length of pre‐test period not stated) and three months after intervention. Drink driving data were collected for nine months before and three months after training. Patron behaviour through interviews. |
McKnight 1991.
| Methods | Non‐randomised controlled trial, unit of allocation = bar. | |
| Participants | USA Experimental = 100 premises in eight sites across the USA (Lafayette, Louisiana; Washtenaw County, Michigan; York, Pennsylvania; Houston, Texas; Springfield, Massachusetts; Newark/Newcastle, Delaware; Clinton/Muscatine/Bettendorf, Iowa; Everett/Lynwood/Marysville, Washington). Control = 138 premises. | |
| Interventions | Server training
'Program of Responsible Alcohol Service' developed by the National Public Service Research Institute. Six hours in length; first three hours were intended for both servers and managers and dealt with the need for responsible alcohol service, ways of preventing customers from becoming intoxicated and methods on intervening with patrons who have already become intoxicated. The final three hours were intended for managers only and included role plays of intervention with intoxicated patrons, the formulation of policies conductive to responsible alcohol service, and guidelines for assisting managers in administering the programme to servers in their own establishments. Control establishments were not exposed to the programme. |
|
| Outcomes | Knowledge and attitudes (in trained servers only), measured by questionnaire Observed server behaviour (to pseudo‐drunks) Observed server behaviour (to 'real' patrons) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | 100 premises comprised the experimental group and 138 premises were used as control. |
| Allocation concealment? | Unclear risk | No information reported. |
| Blinding? All outcomes | Low risk | Observers were blind to allocation status and servers were not informed that observation would occur. |
| Confounders | Unclear risk | The control premises were matched according to size and characteristics to experimental premises. |
| Data collection methods | Unclear risk | Knowledge was measured in the trained servers by questionnaire. Response rates to questionnaire varied between 51 and 83% Three/four observations of server behaviour to pseudo‐drunks made in each premise before and after. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | 1079 servers were trained. |
| Duration of follow‐up | Unclear risk | Length of study period for the server observation was not reported. |
McLean 1994.
| Methods | Randomised controlled trial, unit of allocation = bar. | |
| Participants | Hobart, Tasmania; Australia Experimental = 9 bars Control = 9 bars | |
| Interventions | Health promotion intervention Distribution of '0.05 Know Your Limits' themed educational/promotional material, consistent with the immediate goal of preventing drink‐driving. Involved: 1) distribution of coasters advertising sensible drinking advice; 2) breath analyser placed in a prominent position and poster advertising its use; 3) stickers placed in toilets; 4) fact‐sheets. | |
| Outcomes | Behaviour of patrons (alcohol consumption) measured using breath tests and interviews. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | Eighteen 'hotels' in Hobart, were randomly allocated to experimental (n=9) or control groups (n=9) using a table of random numbers method. Allocation concealment was poor. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Unclear risk | Investigators were aware of the allocation status of the bars. The control bars, however, were not informed of their status. |
| Confounders | Unclear risk | Reported as being no difference. |
| Data collection methods | Unclear risk | Patrons were 'randomly' approached to be interviewed and breath tested. |
| Withdrawals & dropouts | Unclear risk | Two control bars withdrew from the patron surveys. |
| Intervention integrity | Unclear risk | Compliance with intervention varied. |
| Duration of follow‐up | Unclear risk | Intervention was implemented on the Monday of the trial week and follow‐up surveys made on the following Thursday, Friday and Saturday evenings. Response rates to the patron survey were 61% and 66% in experimental and control, respectively. |
Peltzer 2006.
| Methods | Randomised controlled trial, using matched pairs (control:intervention). | |
| Participants | Licensed and unlicensed alcohol serving establishments in Cape Town, South Africa | |
| Interventions | Server training. Course of 5‐6 hour duration provided free. Control group received the same intervention 4 months later. | |
| Outcomes | 1. knowledge, attitudes of servers based on questionnaire (measured post‐intervention only) 2. behaviour of servers when research assistants portrayed specific drinking situations 3. BAC levels of patrons. | |
| Notes | 1. Published study contains no data. 2. Only mean scores for each group are provided. 3. Data presented as numbers falling within each of three BAC categories ‐ no actual values provided. Table in which this data is provided contains arithmetical errors. Attempts to obtain data from the authors have been unsuccessful. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | 20 establishments known to brewery companies were chosen 'by a random sampling procedure'. No details given. Based on their characteristics, they were placed into matched pairs. One from each pair was 'randomly selected' (no details) to be in the intervention group and the other was a control. |
| Allocation concealment? | Unclear risk | No information provided. |
| Blinding? All outcomes | Unclear risk | Research assistants were not told which responses belonged to the experimental or the comparison group. |
| Confounders | Unclear risk | Paired establishments stated to have been matched by type, size and licensed/unlicensed. |
| Data collection methods | Unclear risk | 1. (Knowledge and attitudes of servers): questionnaire administered to 14 servers in 7 experimental establishments only. 2. (Server behaviour): research assistants assessed servers behaviour in specified situations. 3. (BAC): levels were measured in 148 patrons of experimental establishments and 161 controls. |
| Withdrawals & dropouts | Unclear risk | Report states that 3 experimental establishments closed. No information given on any closures of control establishments. |
| Intervention integrity | Low risk | All serving staff in the experimental establishments were trained. |
| Duration of follow‐up | Unclear risk | 3 months. |
Russ 1987.
| Methods | Non‐randomised controlled trial, unit of allocation = server. | |
| Participants | Rural university town, USA Experimental = 16 servers Control = 9 servers Experimental and control servers from two taverns. | |
| Interventions | Server training
Training for Intervention Procedures by Servers of Alcohol (TIPS), approximately six hours in length. During the training, servers are given information on the physiological effects of alcohol that can help them identify specific earning signs indicating when a customer is about to overindulge. Next, servers are taught a variety of tactics for dealing with intoxicated customers or those who appear to be approaching their limits. Use of role‐plays and discussion. Participants must correctly achieve at least 70% in a written test in order to become certified servers. Control servers did not receive the training. |
|
| Outcomes | Observed server behaviour (using pseudo‐patrons) Exit BAC of pseudo‐patrons. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Seventeen servers employed at two local taverns participated. 50% of serving staff at each bar attended training, reasons for non‐participation included lack of interest and inability to attend the training. The remaining untrained servers were used as the controls. |
| Allocation concealment? | High risk | Inadequate. |
| Blinding? All outcomes | Unclear risk | Pseudo‐drunks were blinded to allocation status. |
| Confounders | Unclear risk | Any differences in baseline characteristics between the two groups are not reported. |
| Data collection methods | Unclear risk | Observations used to assess server behaviour; 49 visits (24 before and 25 after) were made and interaction with server was tape recorded. |
| Withdrawals & dropouts | Unclear risk | None reported. |
| Intervention integrity | Unclear risk | All experimental servers completed training. |
| Duration of follow‐up | Unclear risk | Study period over 11 weeks. |
Saltz 1987.
| Methods | Controlled before and after study, unit of allocation = bar. | |
| Participants | Navy sites, USA Experimental = one bar Control =one bar | |
| Interventions | Server training
Development of new and revised management policies regarding the service of alcohol and an 18‐hour training course for all club personnel (five weekly sessions of 3‐4 hours each). The training curriculum was designed to embody the principles of server intervention and blend them with the new policies that employees were going to follow. Training conducted during August and beginning of September 1985. Control received no intervention. |
|
| Outcomes | Behaviour of patrons (self‐reported alcohol consumption), by interview. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Two US Navy clubs were selected, one control and one experimental. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Unclear risk | Not reported. |
| Confounders | Unclear risk | The control was selected for its operation similarity and geographical proximity to the experimental club. |
| Data collection methods | Unclear risk | Random patron interviews were used to gather outcome data. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | Not reported. |
| Duration of follow‐up | Unclear risk | Patrons were selected randomly; response rates 90% in experimental premises for both pre and post test and 90% and 87% in control respectively. Pre and post intervention periods were 4‐6 weeks in length. |
Saltz 1997.
| Methods | Non‐randomised controlled trial, unit of allocation = community. | |
| Participants | USA (Northern California, southern California, South Carolina). Experimental = 3 communities Control = 3 communities Pairs of communities located in Northern California, southern California, South Carolina. | |
| Interventions | Server training Community intervention, five components: 1) community mobilisation; 2) responsible beverage service; 3) drinking and driving (law enforcement); 4) underage drinking (reducing availability); 5) alcohol access component. The primary goal of the responsible beverage service component was to reduce the likelihood of customer intoxication at licensed on‐premise establishments through responsible beverage service practices. A second goal was for licensees to prevent already intoxicated patrons from driving or engaging in other risky behaviour when impaired. Emphasis was placed on the managers' responsibility. Training; four hour programme for servers, five hours for managers. The underlying philosophy was that of prevention (of intoxication and problems) rather than intervention (after a customer has become intoxicated or is causing problems). | |
| Outcomes | Self‐reported server behaviour (telephone survey of random sample). Observed server behaviour (using pseudo‐drunks). (a number of other outcomes were measured for the evaluation of this intervention; the data extracted for this review were restricted to the outcomes for which could be attributed to the server training component). | |
| Notes | Server training one of five strategies encompassing this community intervention. Injury data (traffic crashes) were also collected, however not used in this review as it was not possible to attribute changes in this outcome to the server training component of the intervention. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Three community pairs were selected; three experimental and three matched comparison communities. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Unclear risk | Not reported. |
| Confounders | Unclear risk | Each control community was reported as being 'matched' to an experimental community on the basis of similar local geographic area characteristics, similar industrial/agricultural bases and minority compositions. |
| Data collection methods | Unclear risk | Managers' attitudes and behaviour were assessed by telephone survey of a random sample. Pseudo‐patron survey 65 and 67 experimental premises visited at baseline and follow‐up and 67 and 69 control premises visited, respectively. |
| Withdrawals & dropouts | Unclear risk | N/A |
| Intervention integrity | Unclear risk | In the experimental communities there were 240 premises, 141 were targeted for training of which 72 (51%) attended with 276 staff trained. |
| Duration of follow‐up | Unclear risk | Response rates of survey ranged from 60‐69% and 55‐67% for the experimental communities at the pre and post periods, and 55‐62% and 54‐66% in the control, respectively. Measurements at baseline and at 'early stages' of the programme. Pseudo‐patron surveys were carried out at baseline and 3‐5 months after. |
Toomey 2001.
| Methods | Non‐randomised controlled trial, unit of allocation = bar. | |
| Participants | Licensed bars in the USA. Experimental = 5 bars Control = 9 bars | |
| Interventions | Server training Five one‐on‐one consultations (each 1‐2 hours) once a week, for owners and managers of bars. Aims: 1) develop and implement written establishment policies that encourage responsible alcohol sales; 2) inform and discuss new alcohol policies with staff. Intervention was tailored specifically to each establishment. The goal was to change those actions of alcohol establishments (sales to minors and sales to patrons already significantly impaired by alcohol) that can lead to death, injury and damage. | |
| Outcomes | Observed server behaviour (using pseudo‐drunk actors). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Five experimental bars, each with two matched control bars. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Low risk | Bars were unaware of the observation and the pseudo‐drunks were blind to allocation status. |
| Confounders | Unclear risk | Bars were matched according to bar type and location. |
| Data collection methods | Unclear risk | Observed server behaviour using pseudo‐drunks. |
| Withdrawals & dropouts | Unclear risk | One control premise was dropped from the study, therefore analysis based on five experimental and nine control bars. |
| Intervention integrity | Unclear risk | Full compliance is reported, which for this study was one bar owner/manager from each experimental bar receiving training. |
| Duration of follow‐up | Unclear risk | Pseudo‐drunks used to assess server behaviour 4‐6 weeks after intervention. |
Toomey 2008.
| Methods | Randomised controlled trial. | |
| Participants | Bars and restaurants in one US city. | |
| Interventions | A training programme for owners/managers of alcohol establishments, Alcohol Risk Management (ARM), comprising 4 sessions of 1‐2 hours each. Control group later received ‘ARM Express’, 1 session of 2 hours. | |
| Outcomes | Sales rates to ‘intoxicated’ actors making purchase attempts | |
| Notes | Data also collected on adoption by establishments of policies from a recommended list of 18 but this is not within the inclusion criteria specified in our review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | From establishments listed by state and city licensing agencies, contact was made until number agreeing to participate had reached the researchers ‘participation goal'. 231 agreed to participate. Assigned to intervention or control using a random numbers table. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Unclear risk | No information. |
| Confounders | Low risk | No details provided of any differences between intervention and control groups. |
| Data collection methods | Unclear risk | Observed server behaviour with 'intoxicated' actors. |
| Withdrawals & dropouts | Low risk | Data analysed stated to have come from all 122 (intervention) and 109 (control) establishments |
| Intervention integrity | High risk | 104/122 intervention and 31/109 controls completed training. |
| Duration of follow‐up | Unclear risk | Two follow‐ups. First approx 1 month after training completed. Second approx 3 months after training completed. |
Wallin 2002.
| Methods | Non‐randomised controlled trial, unit of allocation = area. | |
| Participants | Licensed premises in Stockholm, Sweden. Experimental area = northern part of central Stockholm (˜550 licensed premises). Control area = southern part of central Stockholm (˜270 licensed premises). | |
| Interventions | Server training 'STAD project', a multi‐component community alcohol prevention project initiated in 1996. Main categories: 1) Community mobilisation; 2) Two day responsible beverage service training course; 3) Enforcement of existing alcohol regulations. The server training course targeted restaurant owners, bartenders, servers and doormen. It covered the medical effects of alcohol consumption, information about alcohol laws, server intervention training, other drugs and group discussions. | |
| Outcomes | Observed server behaviour (using pseudo‐drunks). Observed server behaviour ‐ customers who appeared to be under 18 attempted to buy a drink. |
|
| Notes | Injury data (police reported violence) were also collected, however not used in this review as it was not possible to attribute changes in this outcome to the server training component of the intervention. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Experimental area comprised the northern part of central Stockholm (containing ˜550 licensed premises at baseline) and control comprised the southern part of central Stockholm (containing ˜270 licensed premises). |
| Allocation concealment? | Unclear risk | Inadequate. |
| Blinding? All outcomes | Unclear risk | Pseudo‐drunks and "under‐18" patrons were blind to allocation status. |
| Confounders | Unclear risk | Any differences in baseline characteristics between the two areas are not reported in pseudo‐drunk study. "Under‐18" study reports several differences; thus 23% of intervention premises were nightclubs but only 2% of control premises. |
| Data collection methods | Low risk | Observations of server behaviour to pseudo‐drunks and "under‐18s" used to assess server behaviour. Violence data were collected from police records for 48 months before and 33 months after. |
| Withdrawals & dropouts | High risk | The experimental and control areas both remained in the study. (In both intervention and control areas some premises closed and new premises opened; actual figures not supplied.) |
| Intervention integrity | High risk | Only 37 of the 61experimental bars sampled had trained their staff when the pseudo‐drunk follow‐up was done. An unspecified number had not trained their staff when the "under‐18" follow‐up was done. |
| Duration of follow‐up | Low risk | Observations conducted at the start of the intervention (1996) and at follow‐ups: pseudo‐drunks three years after intervention (1999); "under‐18s" two years (1998) and five years (2001). |
Warburton 2000.
| Methods | Randomised controlled trial, unit of randomisation = bar. | |
| Participants | Bars in South Wales, West Midlands, West of England; UK. Experimental group = 30 bars Control = 23 bars | |
| Interventions | Complete replacement of pint glasses; Experimental = toughened glassware, Control = annealed glassware. | |
| Outcomes | Injuries to bar staff, by self‐complete questionnaire. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | 53 bars were randomly assigned to experimental (n=30, toughened glassware) and control (n=30, annealed glassware) groups. Method of randomisation was not reported. |
| Allocation concealment? | Unclear risk | No information. |
| Blinding? All outcomes | Low risk | Bars did not know which glassware they were assigned to and researchers were blinded to allocation status. |
| Confounders | Unclear risk | Any differences in baseline characteristics between the two groups are not reported. |
| Data collection methods | Unclear risk | Injury data were collected over six months, by self‐completed questionnaire (distributed through bar managers), response rate is unknown. |
| Withdrawals & dropouts | Unclear risk | Four bars did not receive their allocated intervention and were excluded from the analysis. Nine bars in control and 14 in experimental were lost to follow‐up. |
| Intervention integrity | Unclear risk | Whole stock of pint glassware was replaced. |
| Duration of follow‐up | Unclear risk | Total of 1229 (653 experimental and 576 control) questionnaires were completed and returned. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Boots 1994 | Uncontrolled study. |
| Boots 1999 | Uncontrolled study. |
| Brigham 1995 | Uncontrolled study. |
| Chikritzhs 2002 | Intervention not eligible (licensing restriction). |
| Forsyth 2008 | Observational study with inadequate control group. |
| Fournier 2004 | Uncontrolled study in one university residence, involving two 'baseline parties' and two 'intervention parties'. |
| Hauritz 1998 | Uncontrolled study. |
| Hawks 1998 | Uncontrolled before‐after data. |
| Hingson 1996 | Intervention did not involve the alcohol server setting. |
| Hocking 1983 | Intervention not in the alcohol server setting. |
| Homel 2004 | Uncontrolled study. |
| Licata 2002 | Uncontrolled study. |
| Maguire 2003 | Uncontrolled study. |
| McKnight 1994 | Intervention not eligible (enhanced enforcement of legislation). |
| Molof 1995 | Two schemes, each in one US city, were evaluated. Attempts were made to control the studies but we consider the controls to be inadequate. The authors point out that they were not able to obtain all the data needed for comparison in one city and that there were confounding factors in the other city. |
| Norström 2003 | Intervention not eligible (licensing). |
| Reilly 1998 | Uncontrolled study. |
| Simons‐Morton 1997 | Uncontrolled before‐after study. |
| Treno 2007 | Uncontrolled study. |
| Wagenaar 1991 | Intervention not eligible (server liability). |
| Wagenaar 2000 | Intervention not in the alcohol server setting. |
| Wallin 2005 | Contamination of control group. This is a further follow‐up to Wallin 2002 in which (as part of the STAD intervention) training programmes were made available for bar staff in Stockholm North. However, many bars in the control area (Stodkholm South) had also trained their staff by the time of the follow up. |
| Wundersitz 2002 | Uncontrolled study. |
Characteristics of studies awaiting assessment [ordered by study ID]
South 1991.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes |
Waverley 2004.
| Methods | Controlled trial |
| Participants | Bars in Waverley, Australia |
| Interventions | A training package introduced as part of a responsible serving of alcohol project. (Other measures in the project were used in all bars, so no control.) |
| Outcomes | “....knowledge and attitudes of servers, changes in management practices and serving practices as well as changes in behaviour, (intoxication levels) of patrons”. |
| Notes | No outcome data provided in the volume of the report that we have access to. Access to a further volume will be sought. |
Contributions of authors
KK wrote the protocol, ran the searches, screened records, assessed full texts for inclusion, data extracted and wrote the review. PC screened records, assessed full texts for inclusion and helped with data extraction. PC also commented on drafts of the protocol and review.
Sources of support
Internal sources
No sources of support supplied
External sources
Cochrane Health Promotion & Public Health field, Australia.
Alcohol Education Research Council, UK.
Declarations of interest
None known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Boots 1995 {published data only}
- Boots K, Midford R. Promoting Safe Parties: Evaluation of the 1993 Geraldton Partysafe Campaign. National Centre for Research into the Prevention of Drug Abuse, Curtin University of Technology 1995.
Buka 1999 {published data only}
- Buka SL, Birdthistle IJ. Long‐term effects of a community‐wide alcohol server training intervention. Journal of Studies on Alcohol 1999;60:27‐36. [DOI] [PubMed] [Google Scholar]
Casteel 2004 {published data only}
- Casteel C, Peek‐Asa C, Howard J, Kraus JF. Effectiveness of crime prevention through environmental design in reducing criminal activity in liquor stores: a pilot study. Journal of Occupational and Environmental Medicine 2004;46:450‐8. [DOI] [PubMed] [Google Scholar]
Felson 1997 {published data only}
- Felson M, Berends R, Richardson B, Veno A. Reducing pub hopping and related crime. Criminal Justice Press 1997.
Gliksman 1993 {published data only}
- Gilksman L, McKenzie D, Single E, Douglas R, Brunet S, Moffatt K. The role of alcohol providers in prevention: an evaluation of a server intervention programme. Addiction 1993;88:1195‐203. [DOI] [PubMed] [Google Scholar]
Graham 2004 {published data only}
- Graham K, Osgood DW, Zibrowski E, Purcell J, Gliksman L, Leonard K, et al. The effect of the Safer Bars programme on physical aggression in bars: results of a randomized controlled trial. Drug and Alcohol Review 2004;23:23‐41. [DOI] [PubMed] [Google Scholar]
Haworth 1997 {published data only (unpublished sought but not used)}
- Haworth N, Bowland L, Vulcan P, Finch C. Pilot Study of Promotion of Public Breath Testing. Monash University Accident Reseach Centre; Report 117 1997.
Holder 1994 {published data only}
- Holder HD, Wagenaar AC. Mandated server training and reduced alcohol‐involved traffic crashes: a time series analysis of the Oregon experience. Accident Analysis and Prevention 1994;26(1):89‐97. [DOI] [PubMed] [Google Scholar]
Howard‐Pitney 1991 {published data only}
- Howard‐Pitney B, Johnson MD, Altman DG, Hopkins, Hammond N. Responsible alcohol service: a study of server, manager and environmental impact. American Journal of Public Health 1991;81(2):197‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Johnsson 2003 {published data only}
- Johnsson KO, Berglund M. Education of key personnel in student pubs leads to a decrease in alcohol consumption among the patrons: a randomized controlled trial. Addiction 2003;98:627‐33. [DOI] [PubMed] [Google Scholar]
Krass 1994 {published data only}
- Krass I, Flaherty B. The impact of a responsible service training on patron and server behaviour: a trial in Waverley (Sydney). Health Promotion Journal of Australia 1994;4(2):51‐8. [Google Scholar]
Lacey 2000 {published data only}
- Lacey JH, Jones RK, Anderson EW. Evaluation of a Full‐Time Ride Service Program. Aspen, Colorado's Tipsy Taxi Service. National Highway Traffic Safety Administration 2000; Vol. DOT HS 809155.
Lang 1998 {published data only}
- Lang E, Stockwell T, Rydon P, Beel A. Can training bar staff in responsible serving practices reduce alcohol‐related harm?. Drugs and Alcohol Review 1998;17:39‐50. [DOI] [PubMed] [Google Scholar]
- Stockwell T, Rydon P, Lang E, Beel A. An evaluation of the 'Freo Respects You' responsible alcohol service project. National Centre for Research into the Prevention of Drug Abuse, Curtin University, Perth, Western Australia November 1993.
McKnight 1991 {published data only}
- McKnight AJ. Factors influencing the effectiveness of server‐intervention education. Journal of Studies in Alcohol 1991;52(5):389‐97. [DOI] [PubMed] [Google Scholar]
McLean 1994 {published data only}
- McLean S, Wood L, Montgomery I, Davidson J, Jones M. Promotion of responsible drinking in hotels. Drug and Alcohol Review 1994;13:247‐55. [DOI] [PubMed] [Google Scholar]
Peltzer 2006 {published data only (unpublished sought but not used)}
- Peltzer K, Ramlagan S, Gliksman L. Responsible Alcoholic Beverages Sales and Services Training Intervention inCape Town: A Pilot Study. Journal of Psychology in Africa 2006;1:45‐52. [Google Scholar]
Russ 1987 {published data only}
- Russ NW, Geller ES. Training bar personnel to prevent drunken driving: a field evaluation. American Journal of Public Health 1987;77(8):952‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Saltz 1987 {published data only}
- Saltz RF. The roles of bars and restaurants in preventing alcohol‐impaired driving. An evaluation of server intervention. Evaluation & Health Professions 1987;10(1):5‐27. [Google Scholar]
Saltz 1997 {published data only}
- Grube JW. Preventing sales of alcohol to minors: results from a community trial. Addiction 1997;92(Suppl. 2):S251‐60. [PubMed] [Google Scholar]
- Holder HD, Gruenewald PJ, Ponicki WR, Treno AJ, Grube JW, Saltz RF, et al. Effect of community‐based interventions on high‐risk drinking and alcohol‐related injuries. JAMA 2000;284(18):2341‐7. [DOI] [PubMed] [Google Scholar]
- Holder HD, Saltz RF, Grube JW, Treno AJ, Reynolds RI, Voas RB, et al. Summing up: lessons from a comprehensive community prevention trial. Addiction 1997;92(Suppl. 2):S293‐301. [PubMed] [Google Scholar]
- Holder HD, Saltz RF, Grube JW, Voas RB, Gruenewald PJ, Treno AJ. A community prevention trial to reduce alcohol‐involved injury and death: overview. Addiction 1997;95(Suppl. 2):S155‐71. [PubMed] [Google Scholar]
- Saltz RF, Stanghetta P. A community‐wide Responsible Beverage Service program in three communities: early findings. Addiction 1997;92(Suppl. 2):S237‐49. [PubMed] [Google Scholar]
- Voas RB, Holder HD, Gruenewald PJ. The effect of drinking and driving interventions on alcohol‐involved traffic crashes within a comprehensive community trial. Addiction 1997;92(Suppl. 2):S221‐36. [PubMed] [Google Scholar]
Toomey 2001 {published data only}
- Toomey TL, Waganeer AC, Gehan JP, Kilian G, Murray DM, Perry CL. Project ARM: Alcohol risk management to prevent sales to underage and intoxicated patrons. Health Education & Behaviour 2001;28(2):186‐99. [DOI] [PubMed] [Google Scholar]
Toomey 2008 {published data only}
- Toomey, TL, Erickson DJ, Lenk KM, Kilian GR, Perry CL, Wagenaar AC. A randomized trial to evaluate a management training program to prevent illegal alcohol sales. Addiction 2008;103(3):405‐13. [DOI] [PubMed] [Google Scholar]
Wallin 2002 {published data only}
- Wallin E, Andreasson S. Can I Have a Beer Please? A Study of Alcohol Service to Young Adults on Licensed Premises in Stockholm. Prevention Science 2004;5(4):221‐9. [DOI] [PubMed] [Google Scholar]
- Wallin E, Gripenberg, Andreasson S. Too drunk for a beer? A study of overserving in Stockholm. Addiction 2002;97:901‐7. [DOI] [PubMed] [Google Scholar]
- Wallin E, Norstrom T, Andreasson S. Alcohol prevention targeting licensed premised: a study of effects on violence. Journal of Studies on Alcohol 2003;64:270‐7. [DOI] [PubMed] [Google Scholar]
Warburton 2000 {published data only}
- Warburton AL, Shepherd JP. Effectiveness of toughened glassware in terms of reducing injury in bars: a randomised controlled trial. Injury Prevention 2000;6:36‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Boots 1994 {published data only}
- Boots K. The designated driver program: an outcome evaluation. Health Promotion Journal of Australia 1994;4:1036‐73. [Google Scholar]
Boots 1999 {published data only}
- Boots K, Midford R. 'Pick‐a‐Skipper': an evaluation of a designated driver program to prevent alcohol‐related injury in a regional Australian city. Health Promotion International 1999;14(4):337‐45. [Google Scholar]
Brigham 1995 {published data only}
- Brigham TA, Meier SM, Goodner V. Increasing designated driving with a program of prompts and incentives. Journal of Applied Behaviour Analysis 1995;28:83‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chikritzhs 2002 {published data only}
- Chikritzhs T, Stockwell T. The impact of later trading hours for Australian public houses (hotels) on levels of violence. Journal of Studies on Alcohol 2002;63:591‐9. [DOI] [PubMed] [Google Scholar]
Forsyth 2008 {published data only}
- Forsyth AJM. Banning glassware from nightclubs in Glasgow (Scotland): Observed impacts, compliance and patrons views. Alcohol & Alcoholism 2008;43(1):111‐7. [DOI] [PubMed] [Google Scholar]
Fournier 2004 {published data only}
- Fournier AK, Erhart IJ, Glindemann KE, Scott Geller E. Intervening to Decrease Alcohol Abuse at University Parties. Behaviour Modification 2004;28(2):167‐81. [DOI] [PubMed] [Google Scholar]
Hauritz 1998 {published data only}
- Hauritz M, Homel R, McIlwain G, Burrows T, Townsley M (1998). Reducing Violence in Licensed Venues. Trends and Issues in Crime and Criminal Justice. Australian Institute of Criminology, no 101 ACT.
Hawks 1998 {published data only}
- Hawks D, Rydon R, Stockwell T, White M, Chikritzhs T, Townsley M (1998). The Fremantle Police‐Licensee Accord: Impact on Serving Practices, Harm and the Wider Community. Drug Trials and Tribulations: Lessons for Australian Policy, Perth WA. National Drug Research Institute, Australia.
Hingson 1996 {published data only}
- Hingson R, McGovern T, Howland J, Heeren T, Winter M, Zakocs R. Reducing alcohol‐impaired driving in Massachusetts: the Saving Lives Program. American Journal of Public Health 1996;86(6):791‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hocking 1983 {published data only}
- Hocking B. A controlled trial of supervisor training for an industrial alcohol program. Australian Alcohol/Drug Review 1983;2(2):100‐6. [Google Scholar]
Homel 2004 {published data only}
- Homel R, Carvolth R, Hauritz M, McIlwain G, Teague R. Making licensed venues safer for patrons: what environmental factors should be the focus of interventions?. Drug and Alcohol Review 2004;23:19‐29. [DOI] [PubMed] [Google Scholar]
Licata 2002 {published data only}
- Licata M, Gillham K, Campbell E. Health promotion practices of restaurant and cafés in Australia: changes from 1997 to 2000 using an annual telemarketing intervention. Health Promotion International 2002;17(3):255‐62. [DOI] [PubMed] [Google Scholar]
Maguire 2003 {published data only}
- Maguire M, Nettleton H. Reducing alcohol‐related violence and disorder: an evaluation of the 'TASC' project. Home Office Research Study 265, 2003.
McKnight 1994 {published data only}
- McKnight AJ, Streff FM. The effect of enforcement upon server of alcohol to intoxicated patrons of bars and restaurants. Accident Analysis & Prevention 1994;26(1):79‐88. [DOI] [PubMed] [Google Scholar]
Molof 1995 {published data only}
- Molof MJ, Dresser J, Ungerleider S, Kimball C, Schaefer J. Assessment of year‐round and holiday ride service programs. National Highway Traffic Safety Administration, Washington, DC 1995; Vol. DOT HS 808 203.
Norström 2003 {published data only}
- Norström T, Skog O. Saturday opening of alcohol retail shops in Sweden: an impact analysis. Journal of Studies on Alcohol 2003;64:393‐401. [DOI] [PubMed] [Google Scholar]
Reilly 1998 {published data only}
- Reilly D, Beurden E, Mitchell E, Dight R, Scott C, Beard J. Alcohol education in licensed premises using brief intervention strategies. Addiction 1998;93(3):385‐98. [DOI] [PubMed] [Google Scholar]
Simons‐Morton 1997 {published data only}
- Simons‐Morton BG, Snider Cummings S. Evaluation of a local designated driver and responsible server program to prevent drinking and driving. Journal of Drug Education 1997;27(4):321‐33. [DOI] [PubMed] [Google Scholar]
Treno 2007 {published data only}
- Treno AJ, Gruenewald PJ, Lee JP, Remer LG. The Sacramento Neighborhood Alcohol Prevention Project: outcomes from a community prevention trial. J Stud Alcohol Drugs 2007;68(2):197‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wagenaar 1991 {published data only}
- Wagenaar AC, Holder HD. Effects of alcoholic beverage server liability on traffic crash injuries. Alcoholism: Clinical and Experimental Research 1991;15(6):942‐7. [DOI] [PubMed] [Google Scholar]
Wagenaar 2000 {published data only}
- Wagenaar AC, Murray DM, Toomey TL. Communities Mobilizing for Change on Alcohol (CMCA): effects of a randomized trial on arrests and traffic crashes. Addiction 2000;95(2):209‐17. [DOI] [PubMed] [Google Scholar]
Wallin 2005 {published data only}
- Wallin E, Gripenberg J. Andreasson S. Overseeing at Licensed Premises in Stockholm: Effects of a Community Action Programme. J Stud Alcohol 2005;66:806‐14. [DOI] [PubMed] [Google Scholar]
Wundersitz 2002 {published data only}
- Wundersitz LN. An evaluation of coin‐operated breath testing machines in South Australian licensed premises. Proceedings of the 16th International Conference on Alcohol, Drugs and Traffic Safety ‐ T2002, Montréal, Québec, Canada. 2002:817‐23.
References to studies awaiting assessment
South 1991 {published data only}
- South D, Delaporte H, Nolan C. The development and evaluation of training programs in the responsible service of alcohol in Victoria. Melbourne: VicRoads 1991.
Waverley 2004 {published data only}
- Responsible serving of alcohol project: Final report. Waverley Council 2004.
Additional references
Alderson 2002
- Alderson P, Green S. Open learning material for reviewers. Cochrane Collaboration 2002.
Babor 2003
- Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, et al. Alcohol: no ordinary commodity. Oxford: Oxford University Press, 2003. [Google Scholar]
Berlin 1997
- Berlin JA. Does blinding of readers affect the results of meta‐analyses?. Lancet 1997;350:185‐6. [DOI] [PubMed] [Google Scholar]
Britton 2001
- Britton A, McPherson K. Mortality in England and Wales attributable to current alcohol consumption. Journal of Epidemiology and Community Health 2001;55:383‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deeks 2003
Egger 2001
- Egger M, Davey Smith G, O' Rouke K. Rationale, potential, and promise of systematic reviews. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. Cornwall: BMJ Publishing Group, 2001. [Google Scholar]
English 1996
- English DR, Holman CDJ, Milne E, Winter MG, Hulse GK, Codde JP, et al. The quantification of drug caused morbidity and mortality in Australia, 1995 edition. Reported in: International guide for monitoring alcohol consumption and related harm. WHO 2000.
Foxcroft 2002
- Foxcroft DR, Ireland D, Lowe G, Breen R. Primary prevention for alcohol misuse in young people. Cochrane Database of Systematic Reviews 2002, Issue 3. [Art. No.: CD003024. DOI: 10.1002/14651858.CD003024] [DOI] [PubMed] [Google Scholar]
Graham 1997
- Graham K, Homel R. Creating safer bars. In: Plant M, Single E, Stockwell T editor(s). Alcohol: Minimising the harm. New York: Free Association Books, 1997. [Google Scholar]
Graham 2000
- Graham K. Preventive interventions for on‐premise drinking: a promising but under researched area for prevention. Contemporary Drug Problems 2000;27:593‐667. [Google Scholar]
Higgins 2008
- Higgins JPT, Green S, editors. Assessment of study quality. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, 2008. [Google Scholar]
Homel 1992
- Homel R, Tomsen S. Hot spots for violence: the environment of pubs and clubs. Homicide: patterns, prevention and control: proceeding of a conference held 12‐14 May 1992, Canberra. 1992.
Homel 2001
- Homel R, McIlwain G, Carvolth R. Creating safer drinking environments. In: Heather N, Peters T, Stockwell T editor(s). International Handbook of Alcohol Dependence and Problems. Chichester: John Wiley & Sons Ltd, 2001. [Google Scholar]
Hope 2004
- Hope A. Alcohol policy and young people. The Globe 2004; Vol. http://www.ias.org.uk/publications/theglobe/04issue1,2/globe0412_p15.html.
Jackson 2004
- Jackson N, Waters E, and the Guidelines for Systematic Reviews of Health Promotion and Public Health Intervention Taskforce. The challenges of systematically reviewing public health interventions. Journal of Public Health 2004;26(3):303‐7. [DOI] [PubMed] [Google Scholar]
Jackson 2005
- Jackson N, Waters E for the Guidelines for Systematic Reviews of Health Promotion and Public Health Interventions Taskforce. Guidelines for Systematic reviews of health promotion and public health interventions. Deakin University, Australia April 2005; Vol. Version 1.2.
Jernigan 2000
- Jernigan DH, Monteiro M, Room R, Saxena S. Towards a global alcohol policy: alcohol, public health and the role of WHO. Bulletin of the World Health Organisation 2000;78(4):491‐9. [PMC free article] [PubMed] [Google Scholar]
MacQueen 2004
- MacQueen R. Alcohol evidence and policy: Harm reduction strategy is triumph of spin over substance. BMJ 2004;328:1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
Murray 1997a
- Murray CJL, Lopez AD. Alternative projections of mortality and disability by cause 1990‐2020: Global Burden of Disease Study. The Lancet 1997;349:1498‐504. [DOI] [PubMed] [Google Scholar]
Murray 1997b
- Murray CJL, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. The Lancet 1997;349:1436‐42. [DOI] [PubMed] [Google Scholar]
O'Donnell 1985
- O'Donnell M. Research on drinking locations of alcohol‐impaired drivers: implications for prevention policies. Journal of Public Health Policy 1985;6:510‐25. [PubMed] [Google Scholar]
Peden 2002a
- Peden M, McGee K, Sharma G. The injury chart book: a graphical overview of the global burden of injuries. World Health Organization 2002.
Peden 2002b
- Peden M, McGee K, Krug E (Eds). Injury: A leading cause of the global burden of disease, 2000. World Health Organization 2002.
Poznyak 2001
- Poznyak V, Peden M. WHO Collaborative Study on Alcohol and Injuries; Protocol. WHO 2001.
Rehm 2003
- Rehm J, Room R, Monteiro M, Gmel G, Graham K, Rehn N, et al. Alcohol as a risk factor for global burden of disease. European Addiction Research 2003;9:157‐64. [DOI] [PubMed] [Google Scholar]
Schulz 1994
- Schulz KF, Chalmers I, Grimes DA, Altman DG. Assessing the Quality of Randomization From Reports of Controlled Trials Published in Obstetrics and Gynecology Journals. JAMA 1994;272:125‐8. [PubMed] [Google Scholar]
Shults 2001
- Schults R, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande‐Kulis VG, et al. Reviews of Evidence Regarding Interventions to Reduce Alcohol‐Impaired Driving. American Journal of Preventive Medicine 2001;21:4S. [DOI] [PubMed] [Google Scholar]
Stockwell 2001
- Stockwell T. Responsible alcohol service: lessons from evaluations of server training and policing initiatives. Drug and Alcohol Review 2001;20:257‐65. [Google Scholar]
Strategy Unit 2004
- Strategy Unit. Alcohol harm reduction strategy for England. Prime Minister's Strategy Unit. Cabinet Office 2004.
Thomas 2003
- Thomas H. Quality assessment tool for quantitative studies. Effective Public Health Practice Project 2003.
Wears 2002
- Wears RL. Statistical methods for analyzing cluster and cluster‐randomized data. Academic Emergency Medicine 2002;9(4):330‐41. [DOI] [PubMed] [Google Scholar]
WHO 1999
- WHO. Global Status Report on Alcohol: Global Overview. World Health Organisation 1999.