

Abstract
BACKGROUND:
Anaphylaxis is a life-threatening allergic reaction with significant risk for children with allergies. Access to potentially life-saving medication is critical for these children. This review aims to describe state laws and policies guiding stock epinephrine in schools for allergic or anaphylactic events and detail recommendations for best practices.
METHODS:
This paper is a comprehensive review of the 50 states and District of Columbia’s (DC) laws and policies for stock epinephrine at schools for children in pre-kindergarten through 12th grade.
RESULTS:
All 50 states and DC allow undesignated epinephrine in schools to use for allergic or anaphylactic reactions. A key difference arises in whether states allow (N=37) or mandate (N=14) that schools stock epinephrine. States exhibit differences in the body responsible for developing stock epinephrine policy (N=48), along with stakeholders responsible for developing procedures (N=30) and implementing them (N=19). Differences also exist in state epinephrine procurement, administration, training, and liability.
CONCLUSIONS:
This review of stock epinephrine laws and policies highlights the significant variation in state legislation despite widespread adoption. Only one-quarter of states mandate that schools have stock epinephrine available for emergency use, underscoring need for a more unified approach with consistent guidelines, comprehensive training, and possible funding for implementation.
Keywords: allergic reaction, anaphylaxis, epinephrine, food allergy, legislation, school policy
Approximately six million American school-aged children, or one in 13, have food allergies.1 This chronic, life-threatening condition carries risk of anaphylaxis upon exposure to allergen(s), most commonly milk, eggs, wheat, soy, and tree nuts.2 Research shows 40 percent of food-allergic children have experienced a serious allergic reaction,1 and 16–18 percent have had a reaction at school.3 In fact, one-quarter of first-time anaphylactic events occur at school.4
During allergic/anaphylactic reactions, immediate care is critical for best outcomes. Epinephrine auto-injectors (EAIs) can be lifesaving in the case of an allergic reaction; however, they must be readily available for use.3 Guidelines have been developed to handle allergies in and out of the healthcare setting.5 To support adoption, the federal government passed the School Access to Emergency Epinephrine Act (2013), which incentivizes states to plan for managing anaphylaxis in schools.6 As of 2018, all 50 states and the District of Columbia have had laws facilitating allergy management within schools via undesignated epinephrine (termed “stock epinephrine;” Table 1). Studies have described school district-level policies and practices,7,8 including surveys of school staff/nurses to identify specific practices and preparedness9–11 and analysis of administrative data to understand use and barriers to stock epinpehrine.12,13
Table 1.
State laws for schools to stock epinephrine
| Relevant Stakeholders | Obtaining Stock Epinephrine | Maintenance and Administration | Training | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| State Citation |
System(s) regulated | Location(s) covered | Development | Implementation | Prescription | Procurement | Allowable Price | Individual(s) who may administer | Dose | Eligible recipient(s) | Require-ments outlined | Topics |
| AL Ala. Act 2014–455 (2014), Code § 16–1-48 (2016) |
Dept. of Education | Public school campus | Physician, Board of Pharmacy | Local boards of education | School nurse, staff | Student | Yes | Yes | ||||
| AK Alaska Stat. § 17.22.010, Stat § 17.22.020 (2014) |
Dept. of Health and Social Services | 18+ individual may obtain prescription or purchase | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||||||
| AZ* Ariz. Rev. Stat. § 15–157 (2013, amended 2016) |
Dept. of Education | School, school-related events | Dept. of Health Services, Dept. of Education, medical professionals, school health professionals, school administrators, org. representing school nurses | School districts, charter schools | Standing order (Chief Medical officer of Dept. of Human Services, Chief Medical Officer of County Health Dept., physician, doctor of osteopathy) | Legislature may appropriate funds to provide for purchase of two juvenile and two adult doses, schools may accept monetary donations or grants | School nurse, staff | Four | Student, adult | Yes | Yes | |
| AR Ark. Code § 6–18-707 (2013, amended 2019) |
School district, public charter school | Physician | School nurse, staff | Student | No | No | ||||||
| CA* Cal. Educ. Code § 49414 (2014), Code § 49423 (2017) |
School, school-related events | School districts, county offices of education & charter schools | Physician | Local or mail-order pharmacies, manufacturers | May accept gifts, grants, donations from any source | School nurse, staff, volunteer | Two | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||
| CO Colo. Rev. Stat. § 22–1-119.5 (2013, amended 2018) |
Board of Education | School, school-related events | Dept. of Health & Environment | Governing authorities of schools | Physician, APN, PA | Manufacturers, TPP | FMP, reduced price, free | School nurse, staff, student | Student | Yes | Yes | |
| CT* Conn. Public Act No. 14–176 (2014) |
Board of Education | Commissioner of Public Health | Local & regional boards of education | Physician, APN, PA, optometrist, dentist | School nurse, staff, student | Student | Yes | Yes | ||||
| DE* Del. Chapter 342 (2014) |
Dept. of Education | Dept. of Public Health | Health care provider authorized to prescribe | School nurse, staff | Yes | Yes | ||||||
| DC* D.C. Act 21–259 (2016) |
Superintendent of Education, Dept. of Health | School property, school-related events | Dept. of Health | School districts | Physician, PA, NP | School nurse, staff, volunteer, student | Two | Student | Yes | Yes | ||
| FL Fla. Stat. § 381.885 (2016) |
Board of Education | School property, school-related events | Dept. of Health | School districts | Physician | Wholesale distributors | School nurse, staff, student | Student | Yes | Yes | ||
| GA Ga. Code Ann. § 20–2-776.2 (2013) |
Board of Education | Dept. of Public Health | Physician, PA, APN | Pharmacies, manufacturers, TPP | F FMP, reduced price | School nurse, staff | Student | Yes | Yes | |||
| HI* Haw. Rev. Stat. § 302A-1164 (2019) |
Dept. of Health | Health care provider authorized to prescribe | Pharmacies, authorized health care providers | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||||
| ID Idaho Code Ann. § 33–520A (2014) |
School, school-related events | Governing authorities of schools | Physician, APN, PA | Manufacturers, TPP | FMP, reduced price, free | School nurse, staff, student | One | Student | Yes | Yes | ||
| IL 105 Ill. Comp. Stat. 5 / 22–30 (2016) |
Board of Education | School, school-related events, under supervision of school personnel, before or after normal school activities | Physician, PA, APN | School nurse, staff, volunteer, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||||
| IN Ind. Code § 20–34-4.5 (2014) |
Dept. of Education | Health care provider authorized to prescribe, pharmacist | Pharmacies | School nurse, staff, volunteer | Student, school personnel, visitor | Yes | Yes | |||||
| IA Iowa Code § 135.185 (2015) |
Dept. of Education, Board of Medicine, Board of Nursing, Board of Pharmacy | School, school-related events, under supervision of school personnel, before or after normal school activities | Org. representing school nurses | Board of directors for each school district | Health care provider, APN, PA | School nurse, staff, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | No | |||
| KS Kan. Stat. Ann. § 72–8258 (2014) |
Board of Pharmacy | School, school property, school-related event | Consultant pharmacist | Physician | Pharmacies | One | Student, school personnel | No | No | |||
| KY Ky. Rev. Stat. § 158.836 (2013) |
Dept. of Public Health | Local health depts., local clinical providers, local schools/districts | Local school boards | Donations, purchase | Volunteer | Two | Student | No | No | |||
| LA^ La. Rev. Stat. Ann. § 17.436.1 (2012) |
Governing authorities of schools | Physician | School nurse, staff | Student | Yes | No | ||||||
| ME Me. Rev. Stat. Sec. 20-A, § 6305 (2014) |
Dept. of Education | School property | Dept. of Health and Human Services | Governing bodies of schools | Physician, APN, PA | Manufacturers, TPP | FMP, reduced price, free | School nurse, staff, volunteer, student | Student | Yes | Yes | |
| MD* Md. Code., Educ. § 7–426 (2014) |
Dept. of Education, Dept. of Health and Mental Hygiene | Local boards of education | Health care provider | School nurse, staff | Student | Yes | Yes | |||||
| MA 105 Mass. Code Regs. 210.1159 (2016) |
Dept. of Public Health | School, school-related events | Board of Registration in Nursing, Board of Registration in Medicine | School districts | Shall be assessed on surcharge payers | School nurse, staff | Student | Yes | Yes | |||
| MI* Mich. Comp. Laws § 380.1178–9 (2013) |
Dept. of Education | School property | Dept. of Community Health, Assn. of School Nurses, Nurses Assn., American College of Allergy, Asthma & Immunology, Chapter of Pediatrics, School-Community Alliance of MI, other school orgs./entities | Legislature may appropriate funds to provide for purchase | School nurse, staff, student | Two | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | No | |||
| MN Minn. Stat. § 121A.2205, 121A.2207 (2018) |
District or school | School property, school-related events | Educational commissioner may develop model policy to transmit to interested schools | Interested community stakeholders | Manufacturers | FMP, reduced price, free | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||
| MS Miss. Code Ann. § 37–11-71 (2014) |
School board of each local public school district, governing body of each private or parochial school | Physician, Dept. of Health District Officers | May accept donations from public or private entities | May seek grants to obtain funding | School nurse, staff, student | Student | Yes | Yes | ||||
| MO Mo. Rev. Stat. § 196.990 (2017) |
Dept. of Elementary and Secondary Education | Any appropriate professional assn. | Physician, PA, NP | Pharmacies | School nurse, staff | Student | Yes | Yes | ||||
| MT Mont. Code Ann. § 20–5-420–21 (2013) |
School | School property, school-related events | Physician, APN, PA | Pharmacies | School nurse, staff, student | Students; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||||
| NE* Neb. Rev. Stat. § 79–224 (2016) |
School, educational service unit or program | School property, school-related events, facilities or vehicles for early childhood programs | Physicians, health care provider | Pharmacies | School nurse, staff, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | No | ||||
| NV* Nev. Rev. Stat. § 633.707 (2013) |
Each school district or governing body of each school | School property | Physician, osteopathic physician | Manufacturers, wholesalers | May accept gifts, grants and donations from any source | School nurse, staff, student | Two | Student | Yes | Yes | ||
| NH N.H. Rev. Stat. Ann. § 200:44 (2015) |
Dept. of Education | School property, school-related events, any time subject to school’s jurisdiction or supervision | Dept. of Health and Human Services | School districts | Health care provider | Pharmacies, manufacturers, TPP | FMP, reduced price, free | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |
| NJ* N.J. Stat. Ann. § 18A: 40–12.6a (2015) |
Board of education or chief school administrator | School, school-related events | Guidelines established by Dept. of Education | Physician, APN |
|
School nurse, staff, volunteer, student | Student | Yes | Yes | |||
| NM^ N.M. Stat. Ann. § 22–33-3 (2015) |
Dept. of Health | School property | School district, governing bodies of schools | Health care provider | Pharmacies, manufacturers, wholesalers | May accept gifts, grants, bequests, and donations from any source | School nurse, staff, volunteer | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||
| NY^ N.Y. Educ. Law § 3000-C (2017) |
Commissioner of education | Health care provider | Pharmacies | School provide funding | School nurse, staff | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||||
| NC* N.C. Gen. Stat. § 115C-375.2A (2014) |
Local school board | School, school-related events | Principals in collaboration with appropriate school personnel | Physician, PA, NP of local health dept. | School nurse, staff, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||||
| ND N.D. Admin. Code Sec. 33–37-01 (1996), Cent. Code § 23–01-05.2 (2011) |
State health officer | Physician, pharmacist | Person suffering, or believed to be suffering from anaphylaxis | No | No | |||||||
| OH Ohio Rev. Code Ann. § 3313.7110–7111, 3314.143, 3326.28, 3328.29, 4729.91, 4729.51, 4729.60, 5101.76 (2016) |
State Board of Education | School property | Superinten-dent, licensed health professional authorized to prescribe | Health care provider authorized to prescribe | Wholesalers, manufacturers | May accept donations | School nurse, staff, student | Two | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |
| OK Ok. Stat. § 70–1-116.3 (2013) |
State Board of Education | Board of Health | School districts | Physician | School nurse, staff, student | Two | Student | Yes | No | |||
| OR Or. Rev. Stat. § 339.866 (2013) |
State Board of Education | School property, school-related events | Health Authority, Board of Nursing, Board of Pharmacy | School districts | Health care provider authorized to prescribe | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||
| PA 24 Pa. Stat. Ann. § 14–1414.2 (2014) |
Physician, NP | School nurse, staff, student | Student | Yes | No | |||||||
| RI R.I. Gen. Law H8328 (2016) |
Dept. of Education, Dept. of Health | School property, school-related events, vehicle being used for school purpose | Physician, health care provider authorized to prescribe | Pharmacies | School nurse, staff | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||||
| SC S.C. Code Ann. § 59–63-95 (2013) |
Governing authorities of school districts | Dept. of Health & Environmental Control, Dept. of Education | Physician, APN, PA | Pharmacies, physicians, manufacturers, TPP | FMP, reduced price, free | School nurse, staff, volunteer, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||
| SD S.D. Codified Laws § 13–33A-4 (2014) |
State Board of Education | During school hours | Health care provider | School nurse, staff | Student | Yes | Yes | |||||
| TN Tenn. Code Ann. § 49–5-415(f) (2013) |
School board of each local public school district, governing body of each private or parochial school | Physician | School nurse, staff | Two | Student | Yes | No | |||||
| TX Tex. Educ. Code Ann. § 37.605 (2018) |
Commissioner of State Health Services | School campus, school-related events, while in transit to or from school event | Commissioner of Education, Advisory Committee (established by Commissioner of State Health Services) | School districts | Physician, health care provider authorized to prescribe | Pharmacies | May accept gifts, grants & donations, federal & local funds | School nurse, staff, volunteer | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |
| UT* Utah Code Ann. § 26–41-102 (2015) |
Dept. of Public Health | School district physician, medical director of local health dept., local emergency medical services director | Physicians, pharmacies | School nurse, staff, volunteer, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||||
| VT Vt. Stat. Ann. Tit. 16, § 1388 (2013) |
State Board of Education | School property, school-related events, school-provided transportation, school-related programs | Dept. of Public Health | Physician, APN, PA | Pharmacies, manufacturers, TPP | FMP, reduced price, free | School nurse, staff, volunteer, student | Person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | ||
| VA* Va. Code Ann. § 20–671-710 (2015) |
Dept. of Education, Dept. of Health | School property, school-related events | Local school boards, Assn. of School Nurses, Chapter of American Academy of Pediatrics, Medical Society of VA, Office of Attorney General | Physician, doctor of osteopathy, PA, NP | School nurse, staff | Two | Student | Yes | Yes | |||
| WA Wash. Rev. Code § 28A.210.383 (2013) |
Office of Superintendent of Public Instruction | School property, school-related events | Health care provider authorized to prescribe | Pharmacies | May accept donations | School nurse, staff, student | Student | Yes | Yes | |||
| WV W. Va. Code § 18–5-22c (2013) |
State Board of Education | School property, school-related events | State Health Officer | Allopathic physician, osteopathic physician | Reduced price, free | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | Yes | |||
| WI Wis. Stat. § 118.2925 (2013) |
Governing body of schools | School property, school-related events | Physician | Physician, APN, PA | School nurse, staff, student | Student; person suffering, or believed to be suffering from anaphylaxis | Yes | No | ||||
| WY Wyo. Stat. Ann. § 21–4-316 (2014) |
Dept. of Education | Dept. of Health | School districts | Health care provider authorized to prescribe | Manufacturers, TPP | FMP, reduced price, free | School nurse, staff, volunteer | Yes | Yes | |||
=State mandates stock epinephrine in schools
=Policy does not indicate that school and person administering epinephrine will have no fault if there is adverse reaction
[blank] = Not specified
Abbreviations: APN = Advanced Practiced Nurse, Assn. = Association, Dept. = Department, FMP = Fair-Market Price, NP = Nurse Practitioner, Org. = Organization, PA = Physician Assistant, TPP = Third-Party Providers
To date, no comprehensive analysis has assessed laws nationwide for stock epinephrine in schools and how they are carried out and/or enforced. Policies differ in terms of whether stock epinephrine is allowed or mandated, bodies responsible for development, types of regulated school systems, locations covered, relevant stakeholders, procurement processes, maintenance and administration, training requirements, incident documentation, and liability. This review describes these laws and considers how variation among states affects child welfare at school. This analysis holds potential to identify best practices and opportunities for improvement across states to optimally support children with food allergies.
POLICY REVIEW
Allow versus Mandate Stock Epinephrine in Schools
An important distinction in state laws is whether it allows or mandates that schools stock epinephrine. The latter means schools must maintain a supply of EAIs on site. Fourteen states mandate stock epinephrine in schools, while 37 allow it. The number of states with mandates has grown since 2015 (N=7).14
Body Responsible for Developing School Policy
Most state laws (N=48) outline the body responsible for developing school stock epinephrine policy; three states did not. Most commonly, state education agencies (e.g., board, department) are responsible (N=28). In 12 states, the legislation directs schools, school districts, or other local governing body (e.g., school board) to create policies. Other relevant state agencies cited as responsible include public health (N=15), pharmacy (N=2), and nursing (Kansas). Three states require multiple state agencies to oversee policy development (state education and health agencies in District of Columbia and Maryland; state education, pharmacy, and nursing agencies in Iowa).
Types of School Systems Regulated
Stock epinephrine laws regulate different types of school systems. Thirty-seven states regulate public schools, 29 private, and 16 charter. Eight states reference other school types (eg, parochial, vocational, boarding, tribal). Thirty-four states regulate more than one type of school system, and 13 states do not specify school types. Only 13 states indicate specific school or grade levels covered by the law, all citing elementary and secondary schools. Delaware specifies the law also applies to pre-kindergarten.
Locations Covered
More than half of states (N=31) outline locations where epinephrine policy is active. Most of these identify the law applies on school property (N=28). Twenty-one states also indicate the law covers school-sponsored events.
Relevant Stakeholders
Developing procedures.
Thirty states outline stakeholders responsible for developing procedures for stock epinephrine in schools. The most commonly cited stakeholders are state-level agencies, including health (N=19), education (N=5), and pharmacy (N=2). Three states listed other state-level agencies as stakeholders, including medical and school health professionals (Arizona), boards of registration for nursing and medicine (Massachusetts), and various nursing associations (Michigan). Local stakeholders specified in the laws include schools or school districts (N=5) and providers (N=5). Additional stakeholders are organizations that include school nurses (Arizona, Iowa, Michigan, Virginia) and a consultant pharmacist (Kansas).
Implementing policy/procedures.
Nineteen states identify stakeholders responsible for implementing stock epinephrine in schools. Most often, the local school district, governing authority, or board of education has implementation authority (N=18). Minnesota specifically indicates input should be included from “interested community stakeholders” prior to policy implementation.
Obtaining Stock Epinephrine
Prescription.
Most states (N=45) legislate who must prescribe undesignated epinephrine for school use. The majority of these states indicate a local healthcare provider must prescribe this medication (N=42). Twenty-three states specify a physician must prescribe the epinephrine, while one state indicates standing orders may be used (Arizona). Six states did not identify prescription responsibility.
Procurement.
About half of states (N=27) legislate how schools may obtain stock epinephrine. States specify it may be obtained from local pharmacies (N=17), manufacturers (N=13), third-party suppliers (N=8), wholesalers (N=4), mail-order pharmacies (N=1), and donation (N=1). Alaska indicates any person over 18 years can obtain a prescription and purchase epinephrine if they complete necessary training. Twenty-four states did not indicate where schools obtain epinephrine.
Price/funding.
Less than half of states (N=24) legislate allowable price or funding for procuring epinephrine. Specifically, these states approve fair market/reduced price (N=10) and regular price (N=3); seven states allow donation. Six states indicate schools/districts may seek grants to purchase epinephrine. Michigan stipulates “school boards shall attempt to obtain funds from private sources;” however, if unable, schools can apply for reimbursement from the legislature. Twenty-seven states did not detail allowable spending or funding for epinephrine.
Maintenance and Administration of Stock Epinephrine
Storage (Figure 1).
Figure 1.
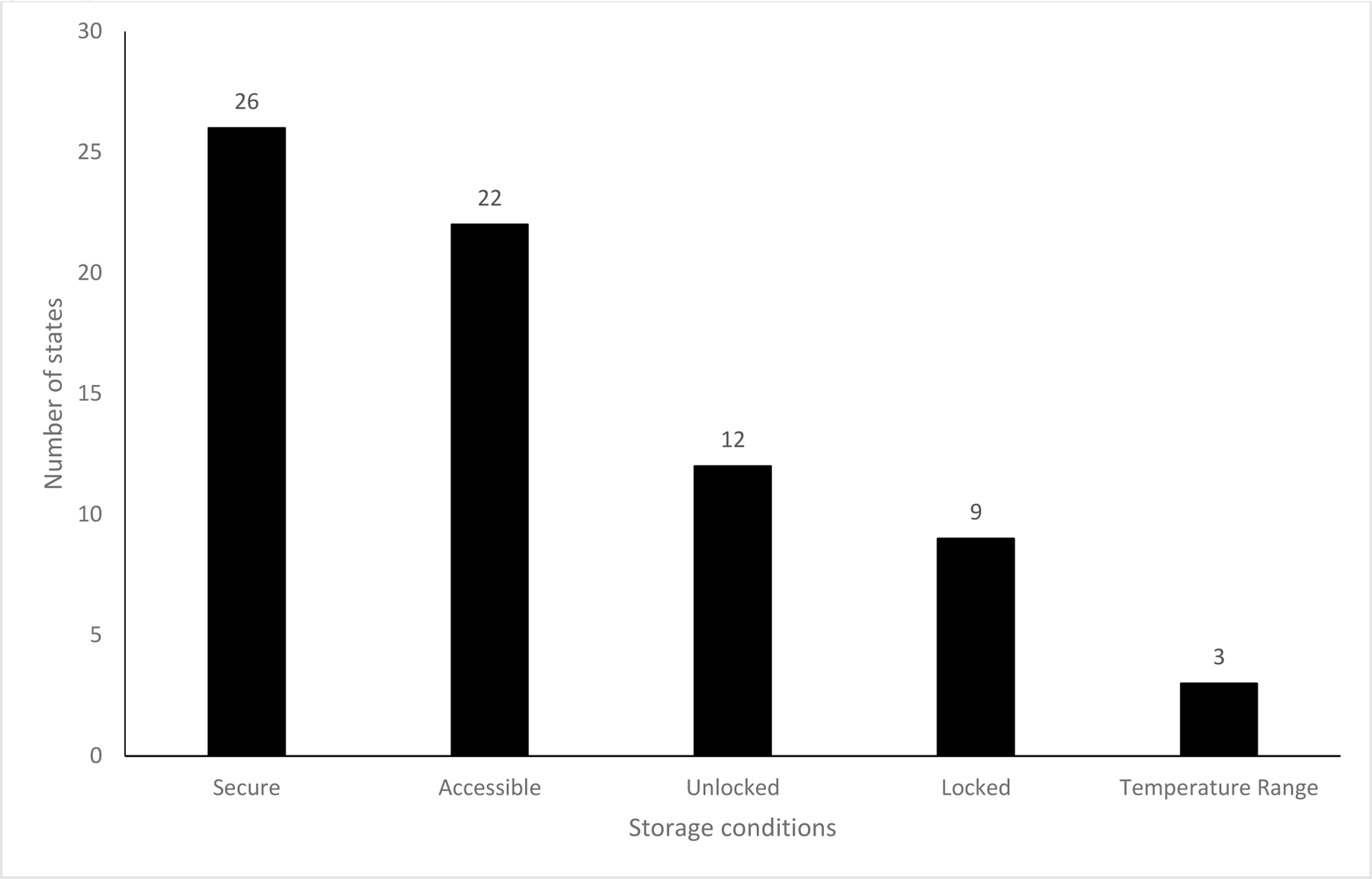
Storage conditions of stock epinephrine at school, as indicated in state laws (N=51)
Twenty-six states specify epinephrine should be stored in a secure location, and 22 indicate it should be accessible. Twelve states require storage in an unlocked location, while nine states require a locked location. Three states provide a temperature range for storage (Arkansas, Colorado, Virginia).
Administration (Figure 2).
Figure 2.
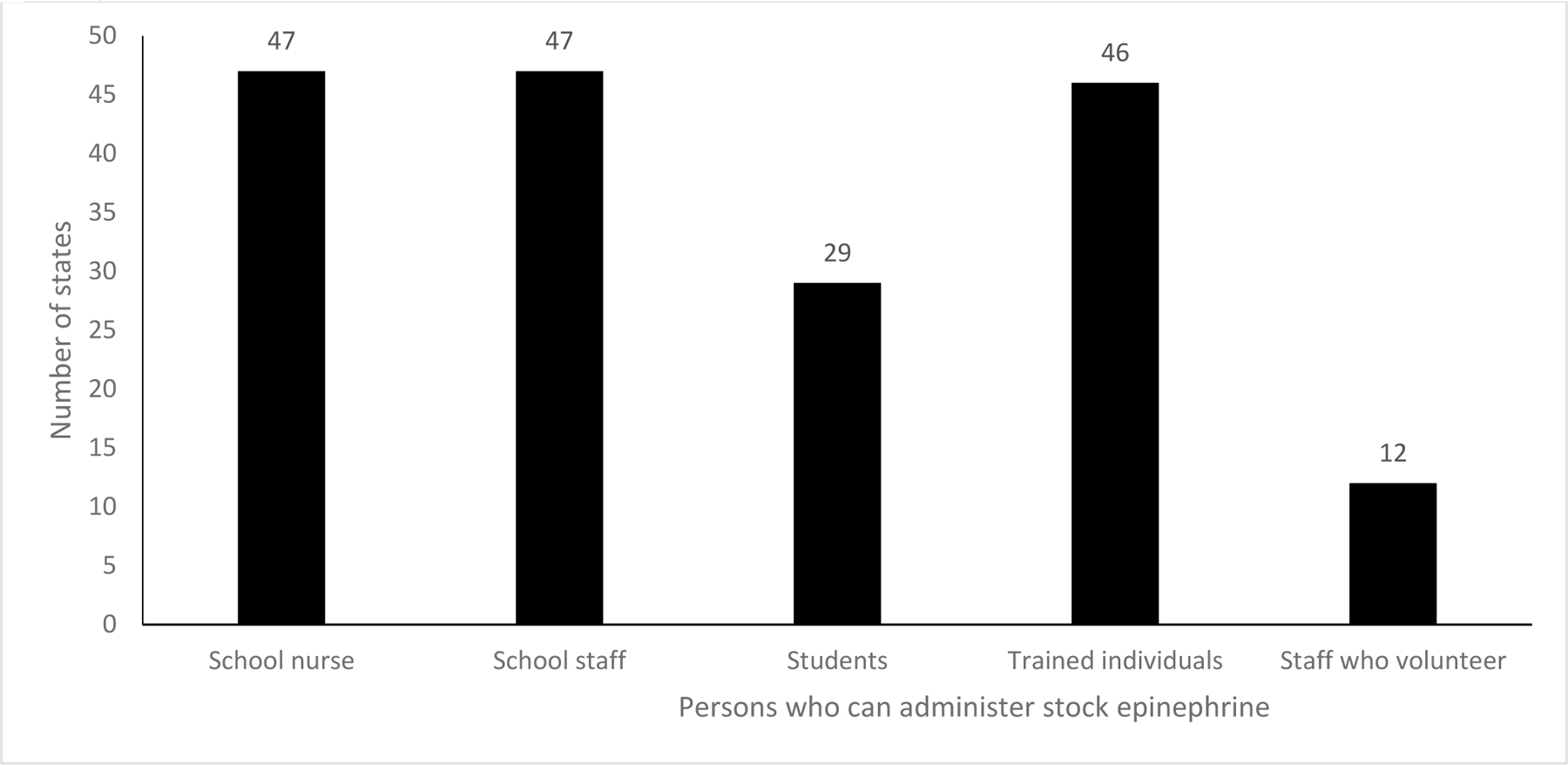
Persons who can administer stock epinephrine at school, as indicated in state laws (N=51)
Nearly all states specify the school nurse and staff can administer epinephrine (N=47). Similarly, most state laws require training for the person administering medication (N=46). Fewer states indicate staff may volunteer to administer epinephrine in school (N=12). Twenty-nine states indicate students can administer stock epinephrine themselves.
Dose.
Three-quarters of states (N=39) do not indicate the number of epinephrine doses that should be kept at the school. Among states that did specify, most required two doses (N=9) with a range from one (N=2) to four (N=1, Arizona). Six states detail both child and adult doses of epinephrine should be kept at school. In addition, most states (N=45) require auto-injectable epinephrine to be available at school. One state requires pre-filled syringes (Missouri). Five states do not specify the dispense method for stock epinephrine.
Eligible recipients.
Fifty states indicate who can receive stock epinephrine in school, including students (N=38), school personnel (N=4), or any person (N=26); Delaware does not specify. Nineteen states define eligible recipients as those having or reasonably believed to be experiencing anaphylaxis.
Enforcement.
Two states address epinephrine law enforcement. Alabama enforces the school stock epinephrine law only if the state provides funding. Arizona’s law specifies that each school’s governing body enforces having stock epinephrine.
Training
Requirements.
Most states (N=47) outline required training for schools to stock epinephrine and staff to administer it; four states do not discuss training. Eleven states address training frequency, mostly every one or two years. Twenty-five states’ laws identify who must administer trainings, including individuals (eg, school nurses, registered nurses, certified emergency responders, qualified personnel designated by school district physicians) or organizations (eg, health departments, nationally recognized organizations that train laypersons).
Topics (Figure 3).
Figure 3.
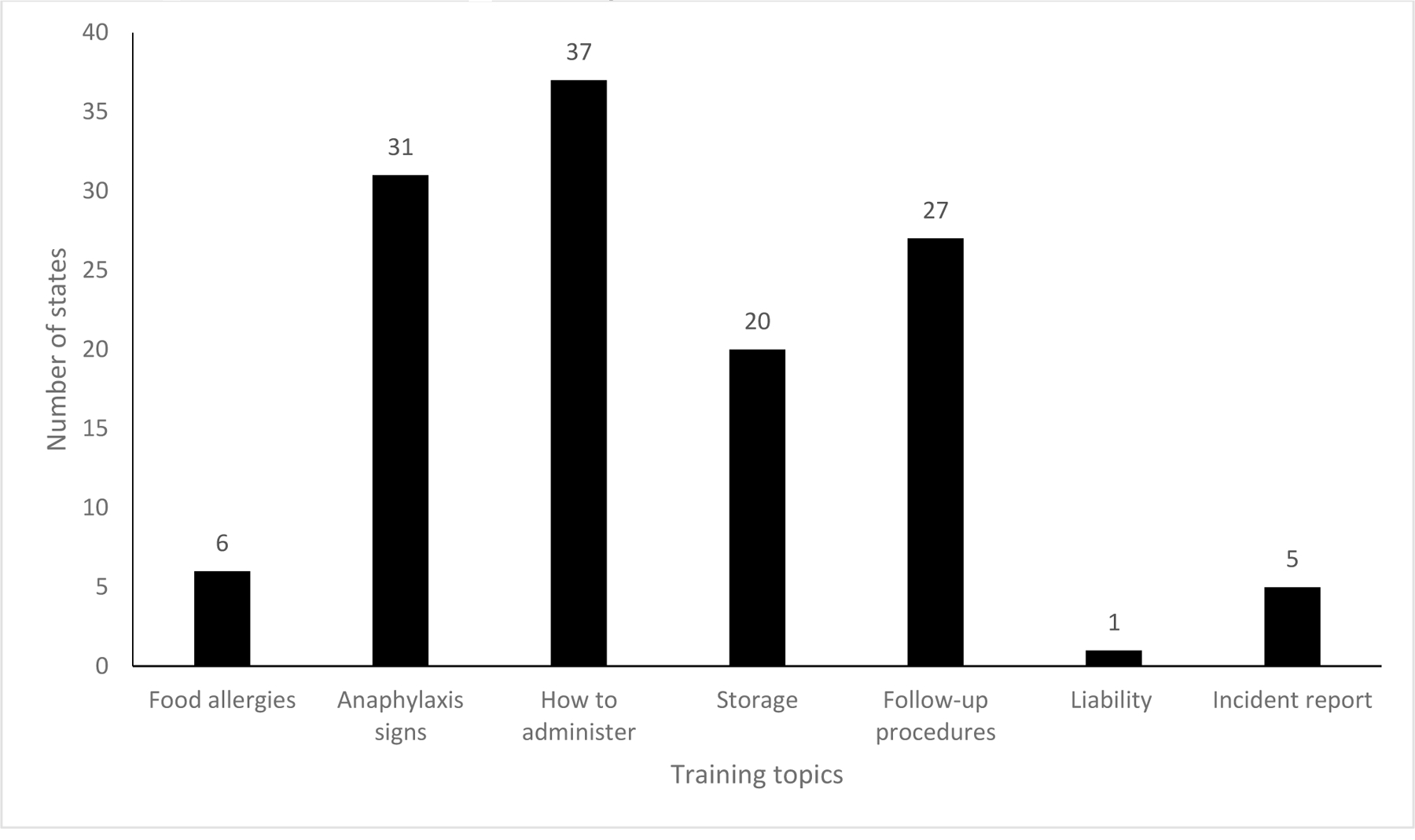
Training topics for individuals administering stock epinephrine in schools, as indicated by 39 states addressing training content
Thirty-nine states’ laws identify training topics. Most commonly, laws specify training should include how to administer epinephrine (N=37), signs/symptoms of anaphylaxis or allergic reaction (N=31), and emergency follow-up procedures (N=27). Less than half of states require training on medication storage (N=20), food allergies (N=6), incident reports (N=5), and liability coverage (N=1).
Incident Documentation
Twenty-five states require schools have anaphylaxis action plans or protocols. Nineteen states require schools to document when stock epinephrine was administered.
School Liability
Nearly all state laws (N=48) indicate the school and person administering epinephrine will have no fault given an adverse reaction. Louisiana, New Mexico, and New York do not comment on liability protection.
IMPLICATIONS FOR SCHOOL HEALTH AND EQUITY
This review shows all states have school stock epinephrine laws in place, yet significant variation exists, creating unnecessary barriers to epinephrine access in schools. The number of children affected by food allergies and the potential of life-threatening allergic reactions warrants a more unified approach is warranted to ensure safe environments in schools.
No requirement for stock epinephrine in every school.
Most states allow stock epinephrine in schools; however, only one-quarter mandate it. Since on average two students in each classroom have food allergies, regardless of race/ethnicity or income,15 it is critical to ensure epinephrine access in every school, regardless of type. It is also critical to remove variation in epinephrine access based on school administrators or staff, particularly since administrators’ choice not to participate is a common barrier to stock epinephrine.16
The costs of caring for food allergies is often borne by families, totaling $25 billion annually.17 By mandating stock epinephrine in schools, consistent environments of care are created in a place where children spend more than half their waking hours, thus minimizing logistical and financial burdens on families to obtain additional epinephrine for school.
Inconsistent policy components.
State laws include varied information about medications, procuring, funding, training, and liability, thus creating uncertainty. A more unified approach is necessary to provide consistent guidance and support to schools while promoting equity.
A key inconsistency across states is specifications about medication types, doses, and storage. Having inadequate number of doses and locking medications for storage limits access in potentially life-saving situations. Minimum requirements should be specified to ensure easy access to adequate medication for an emergency, namely at least two auto-injectors in both child and adult doses that are stored in an unlocked location.
Another inconsistency is obtaining and funding stock epinephrine. Nearly half of states do not detail how schools can obtain stock epinephrine, and just over half provide no funding guidance, including in mandating states. Cost is cited by school nurses as a common barrier to stock epinephrine,16 and one potential concern is placing additional unfunded mandates on schools. Concrete mechanisms for funding and obtaining stock epinephrine are critical to minimize potential disparities in stock epinephrine access within schools.
A third inconsistency is training. Not all states require instruction in anaphylaxis symptoms or proper epinephrine use, both fundamental for effective treatment. Delayed or improper treatment can contribute to worse outcomes. Also, even where training is required, only one state specifies to address liability. It is important to have liability protections for those who prescribe and administer stock epinephrine and to ensure broad awareness of this protection.
Recommendations
To achieve safe environments for children with allergies at school and ensure support for personnel, it is critical that legislators, policymakers, state agencies, and schools work together to:
Optimize access of life-saving medication for all children in case of anaphylaxis or allergic reaction by mandating stock epinephrine in every state and school through laws and policies.
Maintain at least two epinephrine auto-injectors for child and adult doses to ensure appropriate anaphylaxis management in all school buildings.
Ensure epinephrine available to anyone on school grounds and easily accessible by storing in unlocked locations that are clearly marked.
Support students’ ability to self-administer epinephrine if they know proper use and have parental/guardian permission.
Update federal and state laws to delineate funding for stock epinephrine, including appropriating funds, providing flexibility for grants/donations, and regulating market prices of school-designated epinephrine.
Standardize annual training for school personnel to include key topics for safe stock epinephrine use, including anaphylaxis signs/symptoms, proper use, storage, and follow-up, both as defined in policies and within curricula offered in-person and virtually.
Ensure liability protection included in all state laws for school personnel administering stock epinephrine and train on these protections to remove barriers.
Maintain central repository of allergy and epinephrine-related resources to disseminate up-to-date state information, training materials, funding guidance, communication strategies, and best practices for effective implementation at all levels.
Collect detailed information about epinephrine use at schools for program evaluation and refinement, including analyzing individuals’ demographics and outcomes when epinephrine administrated at each school as well as at the district, local, and state level.
Epinephrine availability in schools is a public health concern. Optimizing stock epinephrine laws creates potential for comprehensive, standardized procedures within schools and reduces disparities in epinephrine access.
Acknowledgements:
This work was partially funded through The Centers for Disease Control and Prevention, National Asthma Control Program (1NUE1EH001373–01-00). Additionally, Dr. Anna Volerman was supported by a K23 grant from the National Institutes of Health (K23 HL143128).
Footnotes
Conflict of Interest Disclosure Statement:
All authors of this article declare they have no conflicts of interest relevant to this work. Dr. Volerman serves on the Executive Board of the Chicago Asthma Consortium (unpaid). She also receives funding from the Health Resources and Services Administration.
Contributor Information
Anna Volerman, University of Chicago, 5841 S Maryland Ave, MC 2007, Chicago, IL 606037.
Claire Brindley, University of Chicago, 5841 S Maryland Ave, MC 2007, Chicago, IL 60637, Phone: 612-590-5421, Fax: 773-834-2238.
Nancy Amerson, Illinois Department of Public Health, 535 W. Jefferson St, Springfield, IL 62761, Phone: 217-558-2637, Fax: 217-782-1235.
Tiffanie Pressley, Chronic Disease Prevention and Control, Illinois Department of Public Health, 535 W. Jefferson St, Springfield, IL 62761, Phone: 217-785-5225, Fax: 217-782-1235.
Nikki Woolverton, Illinois Department of Public Health, 535 W. Jefferson St, Springfield, IL 62761, Phone: 217-557-2931, Fax: 217-782-1235.
REFERENCES
- 1.Gupta RS, Warren CM, Smith BM, Blumenstock JA, Jiang J, Davis MM, et al. The Public Health Impact of Parent-Reported Childhood Food Allergies in the United States. Pediatrics 2018;142(6):e20181235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Johns Hopkins Medicine. Food allergies in children The Johns Hopkins University, 2021. Available at https://www.hopkinsmedicine.org/health/conditions-and-diseases/food-allergies-in-children. Accessed February 8, 2021. [Google Scholar]
- 3.McIntyre CL, Sheetz AH, Carroll CR, Young MC. Administration of epinephrine for life-threatening allergic reactions in school settings. Pediatrics 2005;116(5):1134–1140. [DOI] [PubMed] [Google Scholar]
- 4.Sicherer SH, Mahr T. Management of food allergy in the school setting. Pediatrics 2010;126(6):1232–1239. [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. Voluntary Guidelines for Managing Food Allergies In Schools and Early Care and Education Programs Washington, DC: US Department of Health and Human Services; (2013). Available at https://www.hopkinsmedicine.org/health/conditions-and-diseases/food-allergies-in-children. Accessed December 14, 2020. [Google Scholar]
- 6.School Access to Emergency Epinephrine Act §399L(d), 42 USC §280g 2013. [Google Scholar]
- 7.The Network for Public Health Law. Survey of State Epinephrine Entity Stocking Laws 2016. May. [Google Scholar]
- 8.Zadikoff EH, Whyte SA, Desantiago-Cardenas L, Harvey-Gintoft B, Gupta RS. The development and implementation of the Chicago public schools emergency EpiPen® policy. J Sch Health 2014;84(5):342–347. [DOI] [PubMed] [Google Scholar]
- 9.Morris P, Baker D, Belot C, Edwards A. Preparedness for students and staff with anaphylaxis. J Sch Health 2011;81(8):471–476. [DOI] [PubMed] [Google Scholar]
- 10.Hogue SL, Muniz R, Herrem C, Silvia S, White MV. Barriers to the Administration of Epinephrine in Schools. J Sch Health 2018;88(5):396–404. [DOI] [PubMed] [Google Scholar]
- 11.Allen K, Henselman K, Laird B, Quiñones A, Reutzel T. Potential life-threatening events in schools involving rescue inhalers, epinephrine autoinjectors, and glucagon delivery devices: reports from school nurses. J Sch Nurs 2012;28(1):47–5. [DOI] [PubMed] [Google Scholar]
- 12.Tarr Cooke A, Meize-Grochowski R. Epinephrine Auto-Injectors for Anaphylaxis Treatment in the School Setting: A Discussion Paper. SAGE Open Nurs 2019;5:2377960819845246. Published 2019 May 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.DeSantiago-Cardenas L, Rivkina V, Whyte SA, Harvey-Gintoft BC, Bunning BJ, Gupta RS. Emergency epinephrine use for food allergy reactions in Chicago Public Schools. Am J Prev Med 2015;48(2):170–173. [DOI] [PubMed] [Google Scholar]
- 14.Smith A. Many States Now Require Schools to Stock Epinephrine Autoinjectors HCP Live, September 17, 2015. Available at https://www.hcplive.com/view/many-states-now-require-schools-to-stock-epinephrine-autoinjectors. Accessed December 18, 2020.
- 15.Food Allergy Research & Education. Food allergies in the classroom Available at https://www.foodallergy.org/resources/food-allergies-classroom. Accessed December 14, 2020.
- 16.Denny SA, Merryweather A, Kline JM, Stanley R. Stock epinephrine in schools: A survey of implementation, use, and barriers. J Allergy Clin Immunol Pract 2020;8(1):380–382. [DOI] [PubMed] [Google Scholar]
- 17.Gupta R, Holdford D, Bilaver L, Dyer A, Holl JL, Meltzer D. The economic impact of childhood food allergy in the United States. JAMA Pediatr 2013;167(11):1026–1031. [DOI] [PubMed] [Google Scholar]