

Abstract
Background:
India intends to start its 1st dose of vaccination against Covid-19 on January 16th, 2021 prioritizing its frontline health care professionals with either of the two vaccines—Covaxin or Covishield. Whenever a new vaccine is launched, it is marred with controversy and myths. To understand the doubts and concerns better, this study was conducted on health care professionals working in a tertiary care hospital.
Materials and Methods:
Willing respondents, who are working in the institute, were administered the questionnaire asking their views on knowledge, beliefs, and reasons for hesitancy regarding Covid-19 immunization. A Likert scale was used to quantify the responses regarding participants’ knowledge, beliefs, and hesitancies regarding immunization with the available vaccines. Data were analyzed using MS office Excel sheets and JASP software was used to analyze the data thus obtained.
Results:
Out of 122 complete responses, we had 73 (60%) doctors, while 30 (24%) were nursing staff, the rest comprised of other health care workers, such as housekeeping staff, janitorial, etc., 66 (54%) respondents were unaware, while 25 (20%) respondents had hesitancy and 23 (18%) were having extremely negative views regarding vaccination. Some of the variables, such as age, role, marital status, gender, etc., were found to be possibly associated with these scores.
Conclusion:
Issues like concerns over vaccine safety, efficacy, reliability, etc., are deterrents for individuals and whole programme and vaccination drive across the nation. Time and again it has been seen that despite the vaccines’ contribution in breaking the transmission, concerns are making people either hesitant or unmotivated to get the vaccines. More dialogues from the authorities regarding the issues of concern may pave the way for more motivation to accept vaccination and increase the vaccination coverage.
Keywords: Belief over vaccines, coal capital of India, covid19 vaccine, health care professionals, vaccination drive, vaccine hesitancy
Introduction
Coronavirus (CoV) infection is an emerging respiratory virus that is known to cause acute respiratory diseases, ranging from the common cold, SARS, MERS to Covid-19.[1] CoV is a zoonotic agent that can be transmitted via animals to humans.[2] There have been outbreaks of multiple infectious diseases including SARS, MERS-CoV in 2002 and 2012. The outbreak of CoV disease in 2019 (Covid-19) in Wuhan City, Hubei Province, China has been declared as a global epidemic and an emerging public health issue.[3,4] The World Health Organization (WHO) announced that on January 30th, 2020, Covid-19 was an international health emergency.[5] In the very first week of March 2020, numerous new cases were reported globally, and Covid-19 was declared a major epidemic.[6] India had its first case of Covid-19 on January 30th, 2020, in Kerala and it appeared in Dhanbad district in the state of Jharkhand on April 16th, 2020.[7,8]
Earlier, In the absence of a vaccine or successful treatment, all nations around the world struggled to control the spread of the virus by introducing quarantine, lockdown, and social distancing measures, community-based use of face masks at all times, and travel restrictions. These factors greatly affected the physical and mental well-being of the people. Amidst the destruction of the pandemic, international efforts were underway to develop an effective method to control future outbreaks. There was a huge effort in developing a safe and effective Covid-19 vaccine with over 100 different candidate vaccines in different phases of development.[9,10]
India intends to have the 1st dose of vaccination against Covid-19 on January 16th, 2021, prioritizing its frontline health care workers as various countries, such as China, Russia, the US, and the UK, have started vaccinating their frontline health care workers including other population deemed fit for vaccination.[11,12,13] The Government of India has come up with a detailed guideline with details of the vaccination process, logistics, supply, and personnel requirement in the Operational Guideline for Covid-19 vaccination.[14] Health care workers across the country will be given either Covishield (ChAdOx 1 recombinant adenovirus vaccine), which is an adenovirus vector vaccine, or Covaxin (BBV152) an inactivated Covid19 vaccine starting January 16th, 2021. The vaccination program will be run in a centralized manner as health beneficiary lists will be uploaded on the Cowin App database and SMS and other necessary information will be sent to the beneficiary.[14] Health care professionals/Health Care Workers (HCWs)—such as doctors, nurses, lab assistants, operation assistants, lab technicians, dieticians, and intensive care unit (ICU) intensivists or ICU staff who are engaged in setting up the ventilators, etc.—form majority of the workforce that is directly engaged in patients and Covid-19 management, the government has prioritized them for getting the vaccine first, along with janitorial, sweeping, and housekeeping staff, who are also taking care of the ill directly.
ChAdOx1 recombinant adenovirus vaccine was developed using codon-optimized S glycoprotein and synthesized with the tissue plasminogen activator (tPA) leader sequence at 5’ end. The sequence of SARS-CoV-2 coding for amino acids (2 to 1273) and the tPA leader and was propagated in the shuttle plasmid. The Adenovirus vector genome is constructed in the Bacterial Artificial Chromosome by inserting the SARS-CoV-2 S gene into the E1 locus of the ChAdOx1 adenovirus genome,[15] while Covaxin (BBV152) is a whole-virion inactivated SARS-CoV-2 vaccine formulated with an alum-adsorbed toll-like receptor (TLR) 7/8 agonist molecule (Algel-IMDG) prepared indigenously in India.[16] Surveys have been conducted in other countries on the general population, and health care workers to determine the various aspects of immunization, such as vaccine acceptance, vaccine hesitancy, and vaccine refusal, along with assessing the knowledge regarding the process of immunization and its potential benefits with varied results.[17,18,19] In all evidence quoted there is a mixed amount of acceptance and hesitancy while in some cases refusal is also evident. As of now, the government is keeping vaccinationvoluntary. As is shown in various studies, as the vaccines arrive, so arrive the misinformation, mistrust, fear, and an environment of hesitancy and refusal regarding the vaccines.[18,19]
With so much fake news, propaganda, and politicization of Covid-19 vaccines,[20] it's high time that we seek responses from the possible beneficiaries regarding their knowledge, apprehensions, and expected benefits from the vaccination.
Erstwhile Patliputra Medical College and Hospital, now renamed Shaheed Nirmal Mahto Medical College, has been the lone medical college of Dhanbad district in the state of Jharkhand and other neighboring districts like Giridih, Deoghar, Dumka, and Jamtara while neighboring district The College and Hospital is a state run medical facility catering to the health need of people living in this region. Dhanbad is also known as the Coal Capital of India, owing to its rich mineral deposit of coal.[21] The hospital is has its own immunization clinic and experts. As the vaccine for Covide-19 has arrived we intended to ascertain the awareness regarding the vaccination drive, possible benefits of getting immunized through the Covid-19 vaccine, acceptance of the vaccine, knowing the possible barriers for getting vaccinated, and reasons for refusal, if any. Our college and hospital have more than 300 health care professionals—including doctors, nurses, OT assistants, Lab technicians, ICU technicians, and dieticians—who will be given either of the two vaccines mentioned above. The study had the following objectives, (1) to ascertain the demographic and job profile of the participating health care professionals, (2) to assess the awareness regarding the vaccination program for Covid-19 vaccination, (3) to assess the acceptance regarding Covid-19 vaccines, and (4) to know the possible barriers regarding getting the vaccine.
Methods
IEC clearance
The study has proceeded after Institutional Ethical Clearance.
Study setting
The study was done in a hospital setting.
Study design
A cross-sectional study was carried out with voluntary consented anonymous participation from respondents.
Study tools
The study was conducted through an anonymous questionnaire, using semi-structured internally validated questionnaire, which was administered after piloting. The questions sought information regarding the demographic characteristics of respondents (job category, age, sex, years of clinical experience, and work area), prior exposure to Covid-19 infected patients, and whether respondents themselves had ever been infected with Covid-19. We measured HCW's readiness to obtain the Covid-19 vaccine, their awareness regarding the immunization program, their acceptance regarding the vaccination, and refusals.
Study duration
The study was conducted from January 2021 to March 2021.
Study sample size
We received and recorded responses from doctors working in the hospital and college along with nurses, lab assistants, ICU technicians, and OT assistants. Despite our best efforts to have maximum participants, we could only gather 122 complete responses.
Inclusion and exclusion criterion
All health care professionals working in the hospital and college were approached for participation in the study, after explaining the purpose of the study, those who were willing to participate were administered the questionnaire for recording the responses. Before administering the questionnaire, written consent were obtained.
Data analysis
All data were entered in Google spreadsheet templates for data analysis, continuous data values were analyzed using the descriptive statistics approach with standard deviation and mean values, while percentage values were used for dichotomous variables. A two-sampled t-test was done to evaluate the continuous values, while Chi-square test of independence was used to compare proportions. A multivariate logistic regression model was used to determine the associations between relationships of acceptance or awareness based on other parameters. Values of P < .05 were considered statistically significant. JASP free offline version was used for analyses, such as logistic regression and others.[22] A Likert scale was used to quantify the quantitative aspects like awareness, beliefs, and hesitancies. For awareness, out of the 10 questions, all correct answers were marked as 0.5 with the maximum marks of 5. While for beliefs and hesitancy all yes-answers were marked as 1 with maximum marks of 5. The following Figure illustrates the scoring scheme. [Figure 1]
Figure 1.
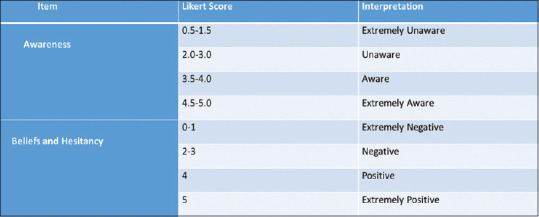
Likert Scale scoring points for Awareness and Beliefs and Hesitancy
Results
Of the 122 participants who responded with all the answers to questions, we had more doctors (76.62%) followed by nurses/ANMs (30.24%). All nurses were female, while 42 females were doctors. Mean age of 27 years suggested more participants in the younger age group. [Table 1] We noted that few participants had chronic diseases while older health care workers were not that willing to be a part of this study in general. The extent of Covid-19 prevalence in the lives of health care workers was assessed and most of the HCWs were working in close contact with Covid-19 patients, family, or relatives. [Table 2] We tried to assess the knowledge about the various aspects of vaccination from the participants and we found the belief scores were significantly associated with gender, hesitancy scores and knowledge scores were not found to be associated with gender significantly. [Table 3] The association of roles was also explored for their impact on belief, knowledge, and hesitancy scores. We found knowledge scores to be associated significantly with roles [Table 4] A t-test was applied to compare the mean scores obtained for belief, hesitancy, and knowledge gender-wise, the scores of belief were found to be highly significant statistically. [Table 4] Univariate Logistic regression analysis was done to seek out probable predictors regarding the knowledge, belief, and hesitancy scores. Marriage was found to be a significant predictor of the knowledge and belief scores. [Table 5].
Table 1.
A brief about the health care workers who participated in the study, their Marital Status, presence of any chronic disease, residence type and roles in hospital
| Demographic Varibales | Description of the varibales | Gender | Total | P | |
|---|---|---|---|---|---|
|
| |||||
| Male | Female | ||||
| Marital Status | Single/Not Married | 26 32.5% |
54 67.5% |
80 100.0%s |
0.00 |
| Married But Living Alone | 0 0.0% |
16 100.0% |
16 100.0% |
||
| Married and living with family | 20 76.9% |
6 23.1% |
26 100.0% |
||
| Age Category | 18-30 | 29 28.7% |
72 71.3% |
101 100.0% |
0.00 |
| 31-40 | 15 93.8% |
1 6.3% |
16 100.0% |
||
| 41-60 | 0 0.0% |
3 100.0% |
3 100.0% |
||
| 61-70 | 2 100.0% |
0 0.0% |
2 100.0% |
||
| Role | Doctor | 31 42.5% |
42 57.5% |
73 100.0% |
0.00 |
| Emergency Area Staff | 4 57.1% |
3 42.9% |
7 100.0% |
||
| Hospital Working Area | 4 100.0% |
0 0.0% |
4 100.0% |
||
| Nurse and ANM | 0 0.0% |
30 100.0% |
30 100.0% |
||
| Technician and Dietician | 7 87.5% |
1 12.5% |
8 100.0% |
||
| Residence | Dhanbad City | 37 41.1% |
53 58.9% |
90 100.0% |
0.254 |
| Other Blocks Dhanbad District | 2 16.7% |
10 83.3% |
12 100.0% |
||
| Other than Dhanbad District | 7 35.0% |
13 65.0% |
20 100.0% |
||
| Chronic | Yes | 4 57.1% |
3 42.9% |
7 100.0% |
0.241 |
| No | 42 36.5% |
73 63.5% |
115 100.0% |
||
| Total | 46 37.7% |
76 62.3% |
122 100.0% |
||
Table 2.
A snap shot of COVID19 presence In the lives of Health Care Workers in SNMMCH
| Various Questions regarding COVID19 in their lives | Yes/No or May be | Role | Total | P | ||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Doctor | Emergency Area Staff | Hospital Working Area | Nurse and ANM | Technician and Dietician | ||||
| Were you infected with COVID19 | Yes | 5 | 0 | 0 | 0 | 0 | 5 | 0.759 |
| 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | 100.0% | |||
| No | 66 | 7 | 4 | 30 | 8 | 115 | ||
| 57.4% | 6.1% | 3.5% | 26.1% | 7.0% | 100.0% | |||
| Maybe | 2 | 0 | 0 | 0 | 0 | 2 | ||
| 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | 100.0% | |||
| Are you working with someone who is infected with COVID19? | Yes | 40 | 4 | 0 | 17 | 8 | 69 | 0.022 |
| 58.0% | 5.8% | 0.0% | 24.6% | 11.6% | 100.0% | |||
| No | 33 | 3 | 4 | 13 | 0 | 53 | ||
| 62.3% | 5.7% | 7.5% | 24.5% | 0.0% | 100.0% | |||
| Are you living with any COVID19 positive family or friend? | Yes | 6 | 0 | 0 | 0 | 0 | 6 | 0.00 |
| 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | 100.0% | |||
| No | 45 | 3 | 4 | 30 | 1 | 83 | ||
| 54.2% | 3.6% | 4.8% | 36.1% | 1.2% | 100.0% | |||
| Maybe | 22 | 4 | 0 | 0 | 7 | 33 | ||
| 66.7% | 12.1% | 0.0% | 0.0% | 21.2% | 100.0% | |||
| Are you living with a COVID19 positive patient? | Yes | 27 | 4 | 0 | 2 | 0 | 33 | 0.00 |
| 81.8% | 12.1% | 0.0% | 6.1% | 0.0% | 100.0% | |||
| No | 33 | 3 | 4 | 26 | 1 | 67 | ||
| 49.3% | 4.5% | 6.0% | 38.8% | 1.5% | 100.0% | |||
| Maybe | 13 | 0 | 0 | 2 | 7 | 22 | ||
| 59.1% | 0.0% | 0.0% | 9.1% | 31.8% | 100.0% | |||
| Was you COVID19 like illness confirmed as COVID19 positive from Lab? | Yes | 5 | 0 | 3 | 4 | 0 | 12 | 0.00 |
| 41.7% | 0.0% | 25.0% | 33.3% | 0.0% | 100.0% | |||
| No | 68 | 7 | 1 | 26 | 8 | 110 | ||
| 61.8% | 6.4% | 0.9% | 23.6% | 7.3% | 100.0% | |||
| Total | 73 | 7 | 4 | 30 | 8 | 122 | ||
| 59.8% | 5.7% | 3.3% | 24.6% | 6.6% | 100.0% | |||
Table 3.
Association of various scores with the different specialties of HCWs
| The Three types of Scores | Scores obtained categorized | Role | Total | P | ||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Doctor | Emergency Area Staff | Hospital Working Area | Nurse and ANM | Technician and Dietician | ||||
| Knowledge Score | Unaware | 37 | 5 | 4 | 15 | 5 | 66 | 0.049 |
| 56.1% | 7.6% | 6.1% | 22.7% | 7.6% | 100.0% | |||
| Aware | 18 | 1 | 0 | 1 | 2 | 22 | ||
| 81.8% | 4.5% | 0.0% | 4.5% | 9.1% | 100.0% | |||
| Extremely Aware | 18 | 1 | 0 | 14 | 1 | 34 | ||
| 52.9% | 2.9% | 0.0% | 41.2% | 2.9% | 100.0% | |||
| Hesitancy Score | Extremely Negative | 16 | 0 | 1 | 6 | 0 | 23 | 0.083 |
| 69.6% | 0.0% | 4.3% | 26.1% | 0.0% | 100.0% | |||
| Non Hesitant | 44 | 3 | 3 | 20 | 4 | 74 | ||
| 59.5% | 4.1% | 4.1% | 27.0% | 5.4% | 100.0% | |||
| Hesitant | 13 | 4 | 0 | 4 | 4 | 25 | ||
| 52.0% | 16.0% | 0.0% | 16.0% | 16.0% | 100.0% | |||
| Belief Score | Extremely Negative | 13 | 3 | 1 | 5 | 1 | 23 | 0.418 |
| 56.5% | 13.0% | 4.3% | 21.7% | 4.3% | 100.0% | |||
| Negative | 11 | 0 | 0 | 3 | 0 | 14 | ||
| 78.6% | 0.0% | 0.0% | 21.4% | 0.0% | 100.0% | |||
| Positive | 40 | 4 | 3 | 15 | 7 | 69 | ||
| 58.0% | 5.8% | 4.3% | 21.7% | 10.1% | 100.0% | |||
| Extremely Positive | 9 | 0 | 0 | 7 | 0 | 16 | ||
| 56.3% | 0.0% | 0.0% | 43.8% | 0.0% | 100.0% | |||
Table 4.
Comparison of Mean scores of Knowledge, Belief and Hesitancy with relation to Gender (t-test Scores)
| Different Scores | Gender | Numbers | Mean Score | Standard Deviation | P |
|---|---|---|---|---|---|
| Knowledge Score | Male | 46 | 1.6304 | 0.82620 | 0.192 |
| Female | 76 | 1.8026 | 0.89472 | ||
| Belief Score | Male | 46 | 2.8261 | 0.56977 | 0.00 |
| Female | 76 | 2.5263 | 1.08902 | ||
| Hesitancy Score | Male | 46 | 1.9565 | 0.66522 | 0.502 |
| Female | 76 | 2.0526 | 0.60871 |
Table 5.
Logistic Regression analysis for Knowledge, Belief and Hesitancy Scores as dependents while other variables as possible predictors
| Belief Score (Believer Vs Non Believer) | Knowledge Score (Aware Vs Non Aware) | Hesitancy Score (Hesitant Vs Non Hesitant) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||||||||
| S.E. | Wald | P | 95% C.I. for Odds Ratio | S.E. | Wald | P | 95% C.I. for Odds Ratio | S.E. | Wald | P | 95% C.I. for Odds Ratio | ||||
| Age Category | 0.691 | 0.058 | 0.810 | 0.219 | 3.280 | 0.667 | 3.819 | 0.051 | 0.073 | 1.004 | 0.734 | 0.287 | 0.592 | 0.352 | 6.244 |
| Married | 0.420 | 4.403 | 0.036* | 0.182 | 0.944 | 0.520 | 5.981 | 0.014* | 1.287 | 9.892 | 0.486 | 1.047 | 0.306 | 0.234 | 1.577 |
| Having Chronic Disease | 0.991 | 0.095 | 0.758 | 0.195 | 9.478 | 1.192 | 0.848 | 0.357 | 0.032 | 3.450 | 0.902 | 3.784 | 0.052 | 0.029 | 1.013 |
| Residence | 0.267 | 0.862 | 0.353 | 0.760 | 2.160 | 0.329 | 1.460 | 0.227 | 0.781 | 2.835 | 0.442 | 2.750 | 0.097 | 0.202 | 1.143 |
| Role in Hospital | 0.148 | 0.133 | 0.715 | 0.789 | 1.412 | 0.159 | 0.128 | 0.721 | 0.692 | 1.290 | 0.168 | 0.913 | 0.339 | 0.845 | 1.631 |
| Infected from COVID19? | 1.201 | 0.202 | 0.653 | 0.163 | 18.061 | 1.095 | 0.494 | 0.482 | 0.054 | 3.963 | 1.243 | 0.001 | 0.976 | 0.084 | 11.025 |
Discussion
As the pandemic has been ravaging the world, it can be best deterred by sticking to the preventive aspects along with an effective vaccination strategy, which remains the keys to beat this pandemic. The Government of India has managed to formulate a vaccination strategy keeping its health care workers at the top for getting any of the two available vaccines at the earliest. The vaccination program has been designed in a way to cater to the population, that is at the maximum risk of exposure. First to be catered were the frontline workers including all health care workers/professionals. At the time of this manuscript being written, we have progressed with the vaccination coverage and are now ready with vaccination for the population of 18 years and above.[23,24] Vaccination coverage in India among health care workers/professionals improved starting with 35% coverage in April 2021 to 80% in June 2021.[25] This has been reported with most of the other nations as vaccine hesitancy has been encountered and reported almost from every corner of the world.[26] This still leaves a 20% chunk of unvaccinated or partially immunized high-risk individuals, leaving possibilities for exploring reasons behind the delayed vaccination. Health care professionals’ approach toward vaccine acceptance has been a major driving force in actual execution, which eventually percolates towards the general population over the years as has been seen worldwide.[27]
Recent evidence from Saudi Arabia, Palestine, and France have been pointing the problem of hesitancy among health care workers.[28,29,30] Authors in the previously discussed papers have pointed out the need for high acceptance among health care workers/professionals prior to the vaccine launch—the varied reasons for the hesitancy which are almost similar to our evidence and other quoted evidence are mentioned below.
We need not undermine the importance of the remaining 20% health care workers in India who are still not vaccinated, hindering the coverage of more than 95% of vaccinated health care workers.
In our institute, among the participants, only one individual was noted to be unvaccinated, but we did come to know the shortcomings regarding the various aspects needed to critically accept the vaccines. Knowledge, belief, and hesitancy are the three technical aspects that need to be worked upon, as we found out the mean scores for all these three aspects were on the lower side despite having maximum participants as doctors and nurses. Similar findings have been reported from one of the premier institutes of the country, Post Graduate Institute of Medical Institution and Research, Chandigarh (PGIMER), in their health care workers albeit in the early phase of the vaccination program.[31] They also showed concerns about vaccine efficacy, safety, and other possible serious side effects. Some of the studies done on antibody response and immunity provided post-vaccination have identified marriage as an important factor.[32] In recent studies done among other populations, marriage was not found to be of any statistical significance for predicting the knowledge or belief score, but in our study group we found marriage to be of importance as a predictor for knowledge and belief scores.[33] The problem of vaccine hesitancy is nothing new, it has been there since the earliest vaccines were introduced to the general public, but over the years with the eradication of smallpox, elimination of polio, elimination of neonatal tetanus, and minimizing incidences or almost cutting the chain of transmission and reduced severity of vaccine-preventable diseases, the importance of vaccines and their roles in halting the disease have been established, and even the illustrative example of H1N1 influenza vaccine is hard to be missed.[34] Somewhere the concerns and doubts raised by the HCWs in our study group resemble that of the reported attitude of Indian citizens towards Covid-19 vaccines, the study noted only 35% as having a positive sentiment towards the vaccine.[33] While another quantitative study done on health care workers concluded the need for addressing various concerns, doubts, and lack of clarity over vaccines in general.[34]
The vaccination coverage of Jharkhand till July 15th, 2021, was close to 20% of the whole population. This number is obtained when we combine the number of people taking available vaccines against Covid-19 while if we see the number of people who have been vaccinated with both doses. As per the Ministry of Health and Family Welfare data,[35] we find it to be only close to 15 lacs (~4%) against an estimated population of 38 crore people residing in the state. Since the vaccine program has started the State has seen a second wave starting in April and the decline noted in the later parts of June.[36]
Bartsch, in their seminal paper, has projected situations regarding vaccine efficacy, coverage, and possibilities of effective control of pandemic based on mathematical modeling. The evidence has been cited more than 100 times and has been largely accepted as the base for various possibilities of vaccination coverage required to curb Covid-19.[37] It largely suggests that even if the vaccine is more than 70% efficacious and is given to 70%-75% of the local population, the pandemic will be exhausted in that region.
For effective control over Covid-19, vaccination coverage should be more than 70% at a minimum in the state, as both the vaccines being administered are more than 75% effective. The same goes for the national average as well. Despite the increase in vaccination numbers, as a country, India is still nowhere close to vaccinating greater than 70% of its population. As per the latest data, India has fully vaccinated 3.5% of its population while close to 15% have received at least one dose of the available vaccines since the drive started in January.[38]
Over the years, the story has been the same, vaccines are invented to counter the surge of a disease, the public first rejects it, then as the cases increase—particularly in viral diseases as the specific treatment eludes—people tend to get the vaccines, once the disease numbers start to decrease the public appears to be losing faith on the efficiency of the vaccines and hesitancy begins to be obvious.
Limitations
One of our limitations was a small sample size and being concentrated in our institute. One refusal documented by us had morbidities and a history of severe allergic reactions.
Conclusion
Beyond doubt, vaccines play a major role in containing the spread of viral diseases but as the disease frequency starts to wane, public perception regarding vaccines too starts to wane. Hesitancy is there, and if not addressed properly, will reflect poor vaccination numbers in the context of the target population. In our opinion, we need to have more education, dialogue, and training regarding the various aspects of vaccination before it is launched, to have a better partnership between the vaccinator and vaccinated so that coverage can be on the higher side. Targeting the most vulnerable group, which could succumb to the disease, was somewhat diminished by low acceptance of the doses across the country, though in our study, the population we found there expressed enough doubts, fear, and concerns regarding the vaccine and if the doubts grow, they will definitely hamper the numbers who will be immunized. The authorities ensuring vaccination must rely on a more informative session, use of social media or newspaper, open dialogues, or capacity of conducting sessions for addressing all concerns, fear, and doubts over the vaccines. Further research in different local settings should be done to understand more about the concerns to that particular region.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors acknowledge the support provided by the staff in the vaccination center and appreciate with regards all participants for their participation.
References
- 1.Yin Y, Wunderink RG. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology. 2018;23:130–7. doi: 10.1111/resp.13196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li Q, Guan X, Wu P, Feng Z. Early transmission dynamics in Wuhan, China, of Novel Coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199–207. doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bhagavathula AS, Shehab A. The story of mysterious pneumonia and the response to deadly Novel Coronavirus (2019-nCoV): So far! NEMJ. 2020;1:7–10. [Google Scholar]
- 4.Lai C, Shih T, Ko W, Tang H, Hsueh P. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 2020;55:105924. doi: 10.1016/j.ijantimicag.2020.105924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eurosurveillance Editorial Team. Note from the editors: World Health Organization declares novel coronavirus (2019-nCoV) sixth public health emergency of international concern. Euro Surveill. 2020;25:200131e. doi: 10.2807/1560-7917.ES.2020.25.5.200131e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization. Coronavirus disease (COVID-19). Situation Report-130. 2020 May. World Health Organization. [Last accessed on 2021 Jan]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200529-covid-19-sitrep-130.pdf?sfvrsn=bf7e7f0c_4 .
- 7.Andrews MA, Areekal B, Rajesh KR, Krishnan J, Suryakala R, Krishnan B, et al. First confirmed case of COVID-19 infection in India: A case report. Indian J Med Res. 2020;151:490–2. doi: 10.4103/ijmr.IJMR_2131_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.News C, News R. Coronavirus in Dhanbad: Dhanbad is 7th district with Covid-19 case. Ranchi News-Times of India. The Times of India. 2021. [Last accessed on 2021 Jan 13]. Available from: https://timesofindia.indiatimes.com/city/ranchi/dhanbad-is-7th-district-with-covid-19-case/articleshow/75187598.cms .
- 9.World Health Organization. DRAFT landscape of COVID-19 candidate vaccines. 2020 June. World Health Organization. [Last accessed on 2021 Jan 2]. Available from: https://www.who.int/who-documents-detail/draft-landscape-of-covid-19-candidate-vaccines .
- 10.Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl Trop Dis. 2020;14:e0008961. doi: 10.1371/journal.pntd.0008961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhuyan A. India begins COVID-19 vaccination amid trial allegations. Lancet. 2021;397:264. doi: 10.1016/S0140-6736(21)00145-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Writer S. UK clears Pfizer’ s covid vaccine, first in the world. Rollout from next week. Mint. 2021. [Last accessed on 2021 Jan 14]. Available from: https://www.livemint.com/science/health/uk-clears-pfizer-s-covid-vaccine-first-in-the-world-11606893200071.html .
- 13.WHO issues its first emergency use validation for a COVID-19 vaccine and emphasizes need for equitable global access. Who.int. 2021. [Last accessed on 2021 Jan 14]. Available from: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access .
- 14.Mohfw.gov.in. 2021. [Last acessed on 2021 Jan 15]. Available from: https://www.mohfw.gov.in/pdf/COVID19VaccineOG111 Chapter 16.pdf .
- 15.Kaur SP, Gupta V. COVID-19 vaccine: A comprehensive status report. Virus Res. 2020;288:198114. doi: 10.1016/j.virusres.2020.198114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ella R, Reddy S, Jogdand H, Sarangi V, Ganneru B, Prasad S, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: Interim results from a double-blind, randomised, multicentre, phase 2 trial, and 3-month follow-up of a double-blind, randomised phase 1 trial. Lancet Infect Dis. 2021;21:950–61. doi: 10.1016/S1473-3099(21)00070-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health (Oxf) 2020 doi: 10.1093/pubmed/fdaa230. fdaa230. doi: 10.1093/pubmed/fdaa230. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Barry M, Temsah M-H, Alhuzaimi A, Alamro N, Al-Eyadhy A, Aljamaan F, et al. COVID-19 vaccine confidence and hesitancy among healthcare workers: A cross-sectional survey from a MERS-CoV experienced nation. medRxiv. doi: 10.1371/journal.pone.0244415. doi: https://doi.org/10.1101/2020.12.09.20246447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kwok KO, Li KK, Wei WI, Tang A, Wong SYS, Lee SS. Editor’ s Choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int J Nurs Stud. 2020;114:103854. doi: 10.1016/j.ijnurstu.2020.103854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Limaye RJ, Sauer M, Truelove SA. Politicizing public health: The powder keg of rushing COVID-19 vaccines. Hum Vaccin Immunother. 2021;17:1662–3. doi: 10.1080/21645515.2020.1846400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singh S, Tiwari S, Hopke PK, Zhou C, Turner JR, Panicker AS, et al. Ambient black carbon particulate matter in the coal region of Dhanbad, India. Sci Total Environ. 2018;615:955–63. doi: 10.1016/j.scitotenv.2017.09.307. [DOI] [PubMed] [Google Scholar]
- 22.JASP-A Fresh Way to Do Statistics. 2021. [Last accessed on 2021 May 31]. From: https://jasp-stats.org/
- 23.Kumar VM, Pandi-Perumal SR, Trakht I, Thyagarajan SP. Strategy for COVID-19 vaccination in India: the country with the second highest population and number of cases. NPJ Vaccines. 2021;6:60. doi: 10.1038/s41541-021-00327-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kyriakidis NC, López-Cortés A, González EV, Grimaldos AB, Prado EO. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines. 2021;6:28. doi: 10.1038/s41541-021-00292-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nearly 80% of healthcare workers, 90% frontline workers vaccinated fully: Health Ministry. The Economic Times. 2021. [Last accessed on 2021 Jul 18]. https://economictimes.indiatimes.com/news/india/nearly-80-of-healthcare-workers-90-frontline-workers-vaccinated-fully-health-ministry/videoshow/84067779.cms?from=mdr.
- 26.Roy B, Kumar V, Venkatesh A. Health Care Workers’ Reluctance to Take the Covid-19 Vaccine: A Consumer-Marketing Approach to Identifying and Overcoming Hesitancy |Catalyst non-issue content. 2021. [Last accessed on 2021 Oct 08]. from https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0676 .
- 27.Gagneux-Brunon A, Detoc M, Bruel S, Tardy B, Rozaire O, Frappe P, et al. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J Hosp Infect. 2021;108:168–73. doi: 10.1016/j.jhin.2020.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Revue E, Eyer X, Chauvin A. Why don’ t health care workers in France trust the COVID-19 vaccine? Can J Emerg Med. 2021;23:722–3. doi: 10.1007/s43678-021-00172-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Elharake JA, Galal B, Alqahtani SA, Kattan RF, Barry MA, Temsah M-H, et al. COVID-19 vaccine acceptance among health care workers in the Kingdom of Saudi Arabia. Int J Infect Dis. 2021;109:286–93. doi: 10.1016/j.ijid.2021.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Maraqa B, Nazzal Z, Rabi R, Sarhan N, Al-Shakhra K, Al-Kaila M. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev Med. 2021;149:106618. doi: 10.1016/j.ypmed.2021.106618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singhania N, Kathiravan S, Pannu AK. Acceptance of coronavirus disease 2019 vaccine among health-care personnel in India: A cross-sectional survey during the initial phase of vaccination. Clin Microbiol Infect. 2021;27:1064–6. doi: 10.1016/j.cmi.2021.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Phillips AC, Carroll D, Burns VE, Ring C, Macleod J, Drayson M. Bereavement and marriage are associated with antibody response to influenza vaccination in the elderly. Brain Behav Immun. 2006;20:279–89. doi: 10.1016/j.bbi.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 33.Praveen SV, Ittamalla R, Deepak G. Analyzing the attitude of Indian citizens towards COVID-19 vaccine-A text analytics study. Diabetes Metab Syndr. 2021;15:595–9. doi: 10.1016/j.dsx.2021.02.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kumari A, Ranjan P, Chopra S, Kaur D, Kaur T, Kalanidhi KB, et al. What Indians think of the COVID-19 vaccine: A qualitative study comprising focus group discussions and thematic analysis. Diabetes Metab Syndr. 2021;15:679–82. doi: 10.1016/j.dsx.2021.03.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mohfw.gov.in. 2021. [Last accessed on 2021 Jul 18]. https://www.mohfw.gov.in/pdf/CummulativeCovidVaccinationReport16thjuly2021.pdf.
- 36.Pioneer T. Covid-19: State sees first single-day-spike of less than 50 cases in 2nd wave. The Pioneer. 2021. [Last accessed on 2021 Jul 18]. https://www.dailypioneer.com/2021/state-editions/covid-19--state-sees-first-single-day-spike-of-less-than-50-cases-in-2nd-wave.html.
- 37.Bartsch SM, O’Shea KJ, Ferguson MC, Bottazzi ME, Wedlock PT, Strych U, et al. Vaccine efficacy needed for a COVID-19 coronavirus vaccine to prevent or stop an epidemic as the sole intervention. Am J Prev Med. 2020;59:493–503. doi: 10.1016/j.amepre.2020.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Moderna, Covovax, Biological E: What we know about India’ s new Covid vaccines. BBC News. 2021. [Last accessed on 2021 Jul 18]. https://www.bbc.com/news/world-asia-india-55748124.