

Abstract
To identify potential differences in racial-ethnic inequities in mortality between adults with/without intellectual and developmental disability, we compared patterns in age at death by race-ethnic status among adults who did/did not have intellectual and developmental disability reported on their death certificate in the United States. Data were from the 2005–2017 U.S. Multiple Cause-of-Death Mortality files. Average age at death by racial-ethnic status was compared between adults, age 18 and older, with/without different types of intellectual and developmental disability reported on their death certificate (N=32,760,741). A multiple descent pattern was observed among adults without intellectual or developmental disability, with age at death highest among Whites, followed by Asians, Hispanics and Blacks, then American Indians. In contrast, a bifurcated pattern was observed among adults with intellectual disability, with age at death highest among Whites, but lower and similar among all racial-ethnic minority groups. The severity of racial-ethnic inequities in age at death was most pronounced among adults with cerebral palsy. Policy makers and public health experts should be aware that racial-ethnic inequities are different for adults with intellectual and developmental disability – all minorities with intellectual and developmental disability are at greater risk of premature death than their White counterparts.
Keywords: Race-ethnicity, intellectual disability, Down syndrome, cerebral palsy, age at death, disparities, inequities, death certificates
Background
Examining differences in age at death is useful in understanding health disparities (Escarce, 2019), often revealing subpopulations that experience premature deaths (Edwards, 2011; Firebaugh et al., 2014; Tuljapurkar, 2011). In the US, there is a substantial difference in age at death for adults with intellectual and developmental disability (Landes et al., 2021; Landes et al., 2019) – conditions that occur before age 18 and are characterized by life-long impairments in mobility, language, learning, self-care, and independent living (Prasher & Janicki, 2019). Specifically, adults with intellectual and developmental disability die 13 to 25 years earlier than adults without intellectual and developmental disability, with variation associated with specific type of disability (Heslop et al., 2014; Heslop & Glover, 2015; Landes, 2017; Landes et al., 2021; Landes et al., 2019; Lauer et al., 2015). Due to lack of adequate surveillance of adults with intellectual and developmental disability across the life course (Bonardi et al., 2011; Krahn, 2019), the size of the adult population with intellectual and developmental disability in the US is unknown (Anderson et al., 2019). Based upon data from the National Health Interview Survey, it is estimated that there are 2.5 to 4 million noninstitutionalized adults with an intellectual disability in the US (Fujiura & Taylor, 2003; Larson et al., 2001). Given this, it is reasonable to assume that the US population of adults with intellectual and developmental disability is substantially larger, as it includes individuals with a more expansive group of conditions. Therefore, this age-at-death disparity affects several million adults in the US alone.
The extent to which the difference in age at death is associated with unavoidable differential prevalence in health conditions among people with/without intellectual and developmental disabilities, as opposed to an inequity related to inadequate access to social resources and health care, remains unclear (Krahn & Fox, 2014; Ouellette-Kuntz, 2005). Though some of this difference may be due to ableism and inequities within society and the healthcare system (Iezzoni et al., 2021; MENCAP, 2007), we will refer to the difference in age at death between adults with/without intellectual and developmental disability as a disparity herein given the nascent state of the evidence.
While an age-at-death disparity among adults with intellectual and developmental disability is well established, extant research has not examined whether racial-ethnic inequities in age at death are similar to those found in the general population or different among adults with/without intellectual and developmental disability (for racial-ethnic differences we intentionally use inequity as opposed to disparity; see Shavers & Shavers, 2006). In the general US population, inequities in mortality rates (frequency of occurrence of death in a defined population during a specified interval) persist for racial-ethnic minority groups despite substantial improvements in overall mortality rates throughout the twentieth century (Hummer & Hamilton, 2019). Compared to mortality rates among White Americans, Asian Americans and Pacific Islanders have similar mortality rates, Hispanic Americans have varying mortality rates based upon nativity – lower among foreign-born but higher among US-born – while Black Americans and American Indians have higher mortality rates (Hummer & Hamilton, 2019; Lariscy et al., 2015). Analysis of racial-ethnic inequities in the average age at death (mean age at death in a specific year) among the US population confirm a similar pattern, with White Americans living on average 1.4 years longer than Asians or Pacific Islanders, 7.4 to 7.8 years longer than Black or Hispanic Americans, and 11.7 years longer than American Indians (National Vital Statistics System, 2017; Xu, 2019).
Racial-ethnic inequities in mortality arise through mechanisms including, but not limited to, structural racism, racial discrimination, socioeconomic status inequities, and a lack of access to quality medical care (Hummer & Hamilton, 2019; Shavers & Shavers, 2006). Though under-researched, studies exploring racial-ethnic differences in access to care, health outcomes, and age at death suggest that inequities observed in the general population may also be present among those with intellectual and developmental disability. Several studies highlight that racial-ethnic minorities with intellectual and developmental disability experience comparatively more barriers in access to and utilization of health care than their White counterparts in the US (Bershadsky et al., 2014; Li et al., 2021; Scott & Havercamp, 2014), as well as in the UK (Robertson et al., 2019). This appears to negatively affect health outcomes for this population. For example, two studies from the US report that among people with intellectual and developmental disability, Black and Hispanic adults are more likely to report having fair or poor physical health than White adults (Li et al., 2021; Magaña et al., 2016). Recent reports from the UK provide evidence that this racial-ethnic inequity in age at death for adults with intellectual disability is not isolated to the US (Heslop et al., 2021; Heslop et al., 2019). Related, one study documents that among people with Down syndrome, one particular type of developmental disability, White Americans lived approximately 25 years longer than Black Americans in 1997 (Yang et al., 2002).
Though informative, research has not documented the full extent of racial-ethnic inequities in age at death among adults with intellectual and developmental disability in the US by disability type and in comparison to adults without intellectual and developmental disability. To fill this gap in our knowledge base, we compare average age at death for adults with intellectual disability, Down syndrome, and cerebral palsy to adults without an intellectual or developmental disability by race-ethnicity as reported on death certificates. Our expectation is that patterns in racial-ethnic inequities observed in the general population will also be present among adults with and without intellectual and developmental disability.
Methods
Data and measures
This study used 2005–2017 National Vital Statistics System US Multiple Cause of Death mortality data for residents of the 50 US states and the District of Columbia. We analyzed data on all adults, age 18 and over, who died in the US between January 1, 2005 and December 31, 2017 and had their death officially recorded on a death certificate (N=32,760,741). We used International Classification of Disease (ICD-10) codes from Parts I and II of the death certificate to create non-exclusive categories that are commonly identified as intellectual and developmental disability in the US (Boyle et al., 2011): intellectual disability (N=26,890), Down syndrome (N=23,849), and cerebral palsy (N=30,408). Disability categories and corresponding ICD-10 codes are reported in Table 1. There were an insufficient number of cases to analyze other rare types of developmental disability such as Autism, fetal alcohol syndrome, pervasive developmental disorders, and chromosomal abnormalities by race-ethnicity (combined N=3,144). We used non-exclusive categories given that intellectual disability typically or at times co-occurs with Down syndrome and cerebral palsy (Anker et al., 2020; Reid et al., 2018), but is not always reported on death certificates that include these developmental disability types. The comparison category for all analysis was decedents without intellectual disability, Down syndrome, cerebral palsy, or other rare types of developmental disability reported on their death certificate, here referred to as decedents without an intellectual or developmental disability (N=32,680,964).
Table 1:
Disability type categories and corresponding ICD-10 codes
| Disability type | ICD-10-CM diagnosis codes |
|---|---|
| Intellectual disability | F70, F71, F72, F73, F78, F79 |
| Down syndrome | Q90.0, Q90.1, Q90.2, Q90.9 |
| Cerebral palsy | G80.0, G80.1, G80.2, G80.3, G80.4, G80.8, G80.9 |
Age at death was measured in single years ranging from 18 to 126. Race-ethnicity indicates whether the decedent was Non-Hispanic White (here White), Non-Hispanic Black (here Black), Non-Hispanic American Indian or Alaskan Native (here American Indian/Alaskan Native), Non-Hispanic Asian or Pacific Islander (here Asian/Pacific Islander), or Hispanic. Country of origin is not available on US death certificates. Sex was coded dichotomously as female and male. Year indicated the year of death.
Analytic strategy
As there are no reliable estimates of population size among adults with intellectual and developmental disability in the US (Anderson et al., 2019), similar to prior studies, we analyzed average (mean) age at death (Landes et al., 2021; Landes et al., 2019). We first examined the distribution of all study variables for the entire sample, then for each disability category. We used OLS regression, with a disability by race-ethnicity interaction term, to calculate the age at death for all adults with and without the indicated disability across all racial-ethnic groups. The reference category in each model was decedents without an intellectual or developmental disability. All models control for biological sex (reference group – male), and year at death centered at the mean to ensure the accuracy of the age at death estimates. We conducted sensitivity analysis and determined that patterns in racial-ethnic differences in age at death between adults with and without intellectual and developmental disability did not vary by sex. Results from analysis by sex is not reported. We used STATA 16.0 (College Station, TX) for all analysis.
Results
The distribution of all measures across disability categories is reported in Table 2. Compared to the average unadjusted age at death for adults without an intellectual or developmental disability (74.0 years), the unadjusted age at death was 14.7 years younger for adults with intellectual disability, 19.1 years younger for adults with Down syndrome, and 24.2 years younger for adults with cerebral palsy.
Table 2:
Distributions of all study variables by disability type, 2005–2017 National Vital Statistics System US Multiple Cause of Death mortality data
| No intellectual or developmental disability | Intellectual disability | Down syndrome | Cerebral palsy | |||||
|---|---|---|---|---|---|---|---|---|
| % or M(SD) | N | % or M(SD) | N | % or M(SD) | N | % or M(SD) | N | |
| Age at death M(SD) | 73.99 (16.51) | 32,680,964 | 59.34 (16.53) | 26,890 | 54.93 (11.37) | 23,849 | 49.76 (19.81) | 30,408 |
| Race-ethnicity | ||||||||
| White | 79.87 | 26,103,567 | 79.97 | 21,505 | 83.93 | 20,016 | 75.55 | 22,972 |
| Black | 11.47 | 3,748,069 | 12.72 | 3,421 | 8.03 | 1,914 | 14.02 | 4,264 |
| American Indian | 0.60 | 196,488 | 0.61 | 163 | 0.45 | 108 | 0.88 | 269 |
| Asian or Pacific Islander | 2.14 | 698,805 | 1.21 | 325 | 1.19 | 284 | 1.42 | 431 |
| Hispanic | 5.92 | 1,934,035 | 5.49 | 1,476 | 6.40 | 1,527 | 8.13 | 2,472 |
| Sex | ||||||||
| Female | 49.95 | 16,323,769 | 45.54 | 12,246 | 48.53 | 11,575 | 44.95 | 13,668 |
| Male | 50.05 | 16,357,195 | 54.46 | 14,644 | 51.47 | 12,274 | 55.05 | 16,740 |
| Year M(SD) | 2011.18 (3.76) | 32,680,964 | 2010.45 (3.60) | 26,890 | 2011.25 (3.77) | 23,849 | 2011.60 (3.75) | 30,408 |
Note: Disability type are not mutually exclusive. M = Mean. SD = Standard deviation.
Individuals identified as Hispanic are reported only in the Hispanic race-ethnicity category.
Compared to the distribution of adults without an intellectual or developmental disability, other differences of note include a smaller percentage of adults with Down syndrome who were Black, and a smaller percentage of adults with intellectual disability or cerebral palsy who were female.
Results for OLS regression models are reported in Table 3. There were distinct racial-ethnic inequities in age at death for each disability category. For ease of interpretation, the mean age at death for decedents with and without each disability across all racial-ethnic groups are presented in Figure 1.
Table 3:
Logistic regression models of age at death, 2005–2017 National Vital Statistics System US Multiple Cause of Death mortality data
| Intellectual disability | Down syndrome | Cerebral palsy | ||||
|---|---|---|---|---|---|---|
| b | 95% CI | b | 95% CI | b | 95% CI | |
| IDD type (ref: No IDD) | −14.03*** | (−14.25, −13.82) | −19.50 | (−19.72, −19.28) | −22.20*** | (−22.41, −22.00) |
| Race-ethnicity (ref: White) | ||||||
| Black | −7.95*** | (−7.97,7.93) | −7.95*** | (−7.97,7.93) | −7.95*** | (−7.97,7.93) |
| American Indian | −11.78*** | (−11.85, −11.71) | −11.78*** | (−11.85, −11.71) | −11.78*** | (−11.85, −11.71) |
| Asian or Pacific Islander | −2.40*** | (−2.44, −2.36) | −2.40*** | (−2.44, −2.36) | −2.40*** | (−2.44, −2.36) |
| Hispanic | −7.48*** | (−7.50, −7.45) | −7.48*** | (−7.50, −7.45) | −7.48*** | (−7.50, −7.45) |
| Female (ref: Male) | −6.61** | (−6.62, 6.60) | −6.61*** | (−6.62, 6.60) | −6.61*** | (−6.62, 6.60) |
| Year (centered at mean) | 0.07*** | (0.07, 0.07) | 0.07*** | (0.07, 0.07) | 0.07*** | (0.07, 0.07) |
| IDD × Race-ethnicity interaction term | ||||||
| Black | 0.31 | (−0.26, 0.89) | 2.59*** | (1.84, 3.33) | −3.96*** | (−4.47, −3.44) |
| American Indian | 4.90*** | (2.46, 7.35) | 4.52** | (1.51, 7.52) | 2.00* | (0.10, 3.91) |
| Asian or Pacific Islander | −8.87*** | (−10.61, −7.13) | −5.19*** | (−7.04, −3.33) | 11.12*** | (−12.63, −9.61) |
| Hispanic | −3.45*** | (−4.29, −2.62) | 1.25*** | (0.42, 2.08) | −7.94*** | (−8.60, −7.28) |
| Intercept | 72.17*** | (72.16, 72.17) | 72.17*** | (72.16, 72.17) | 72.17*** | (72.16, 72.17) |
| N | 32,707,854 | 32,704,813 | 32,711,372 | |||
Notes:
p<.001;
p<.01;
p<.05.
No IDD = Decedents without an intellectual or developmental disability. Individuals identified as Hispanic are reported only in the Hispanic race-ethnicity category.
Figure 1:
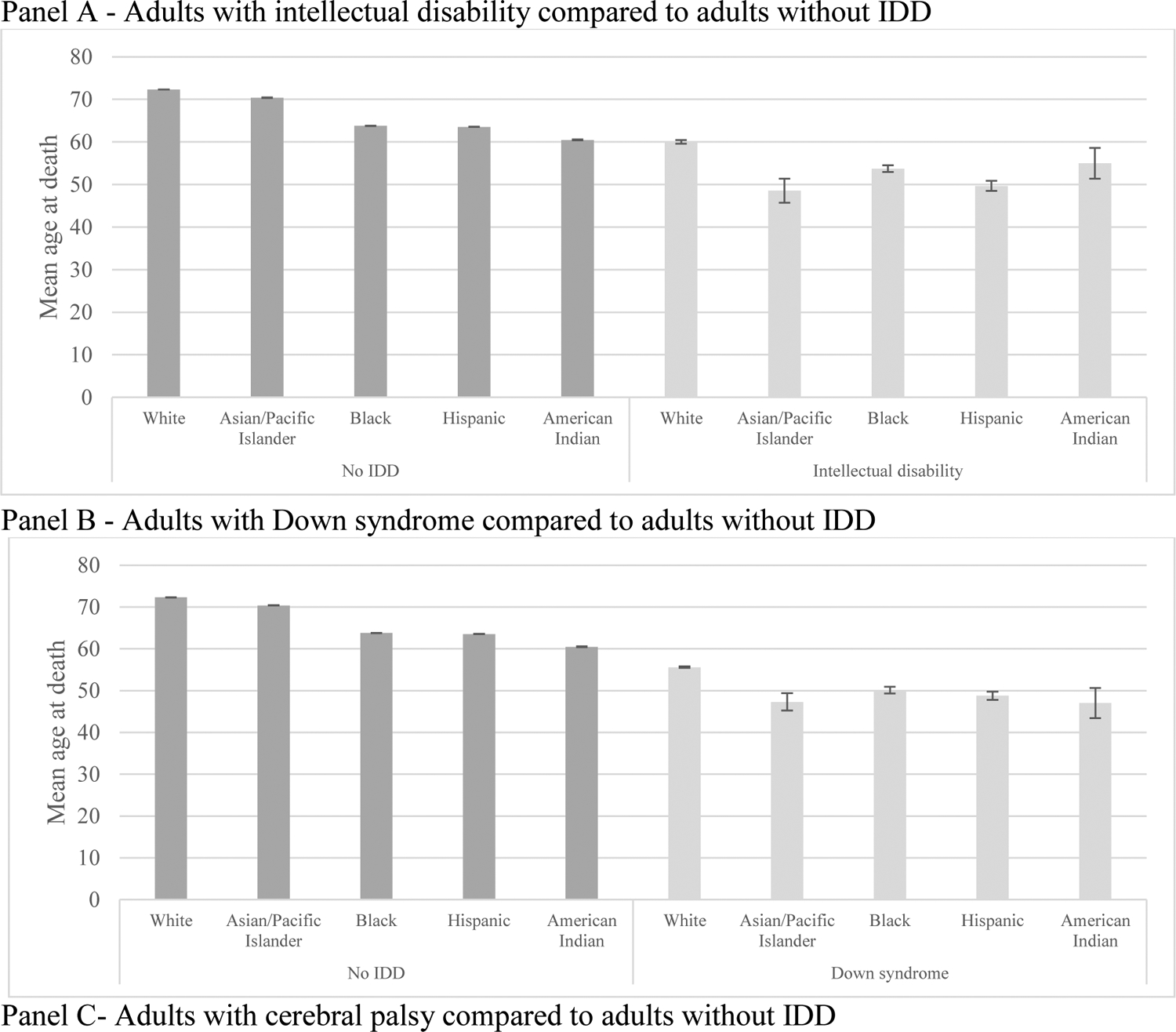
Mean age at death by disability status and race-ethnicity, 2005–2017 National Vital Statistics System US Multiple Cause of Death mortality data
Note: Individuals identified as Hispanic are reported only in the Hispanic race-ethnicity category.
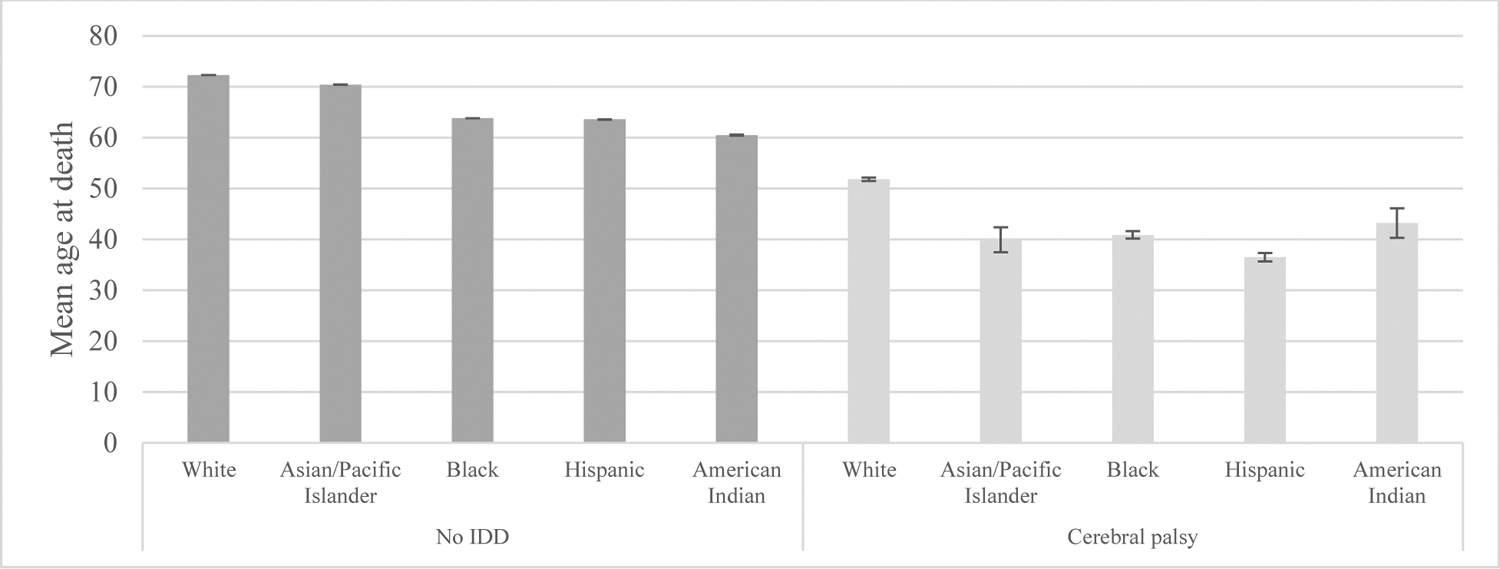
The patterns in age at death across racial-ethnic groups for decedents without intellectual or developmental disability are reported as a point of comparison in all three panels of Figure 1 (Panels A-C). Due to the size of the sample for adults without intellectual or developmental disability, confidence intervals in age at death for each racial-ethnic group were distinct. Therefore, based upon visual analysis, we describe inequities in age at death among racial-ethnic groups using a multiple descent pattern. The highest age at death was among Whites (72.3 years; 95% CI, 72.3–72.3); followed by Asians/Pacific Islanders (70.4 years; 95% CI, 70.3–70.5); Blacks (63.8; 95% CI, 63.8–63.8) and Hispanics (63.6 years; 95% CI, 63.5–63.6); then American Indians/Alaskan Natives (60.5 years; 95% CI, 60.4–60.6).
The patterns in age at death among decedents with intellectual and developmental disability were markedly different: the racial-ethnic inequities reduced to a bifurcated pattern, with distinct confidence intervals between Whites and all racial-ethnic minority decedents, but overlapping, or nearly overlapping (Hispanic and Black among adults with intellectual disability; Hispanic and all other racial-ethnic minority groups among adults with cerebral palsy), confidence intervals among the racial-ethnic minority groups.
Similar to adults without intellectual and developmental disability, among all decedents with an intellectual and developmental disability reported on their death certificate, the highest age at death was among White decedents: 60.2 years (95% CI, 60.1–60.5) for intellectual disability; 55.6 years (95% CI, 55.4–55.8) for Down syndrome; and 51.8 years (95% CI, 51.5–52.1) for cerebral palsy.
Then, instead of a multiple descent patten in age at death among racial-ethnic minorities, there was a bifurcated pattern with comparably lower and similar ages at death among all racial-ethnic minority groups. For adults with an intellectual disability reported on the death certificate, mean age at death was 48.6 years (95% CI, 45.8–51.4) among Asians/Pacific Islanders, 49.7 years (95% CI, 48.5–50.9) among Hispanics, 53.7 years (95% CI, 52.9–54.5) among Blacks, and 55.0 years (95% CI, 51.4–58.6) among American Indians/Alaskan Natives.
For adults with Down syndrome reported on the death certificate, mean age at death was 47.3 years (95% CI, 45.3, 49.4) among Asians/Pacific Islanders, 50.1 years (95% CI, 49.3, 51.0) among Blacks, 48.8 years (95% CI, 47.8, 49.7) among Hispanics, and 47.0 years (95% CI, 43.4, 50.6) among American Indians/Alaskan Natives.
For adults with cerebral palsy reported on the death certificate, mean age at death was 39.9 years (95% CI, 37.4, 42.4) among Asians/Pacific Islanders, 40.9 years (95% CI, 40.1, 41.6) among Blacks, 36.5 years (95% CI, 35.6, 37.4) among Hispanics, and 43.2 years (95% CI, 40.3, 16.1) among American Indians/Alaskan Natives.
As can be seen in the coefficients for the intellectual or developmental disability by race-ethnicity interaction term in Table 3, the shift in the age at death differences among racial-ethnic groups from a multiple descent to a bifurcated pattern was due to two factors. The first was a comparatively greater age-at-death inequity for Asians/Pacific Islanders than other racial-ethnic minority groups across all disability categories. The second was a comparatively reduced age-at-death inequity for American Indians/Alaskan Natives than other racial-ethnic minority groups across all disability statuses.
It is also important to note that the severity of the intersecting intellectual or developmental disability age-at-death disparity by racial-ethnic group inequity varied by disability status. As a point of comparison, the racial-ethnic age-at-death inequity among those without intellectual or developmental disability was 1.9 years for Asians/Pacific Islanders, 8.5 years for Blacks, 8.8 years for Hispanics, and 11.8 years for American Indians/Native Americans.
Among decedents with intellectual and developmental disability, the intersection of disability status increased the age-at-death inequity for Asians/Pacific Islanders: 11.6 years for intellectual disability; 8.3 years for Down syndrome; and 11.9 years for cerebral palsy. The age-at-death inequity was also comparatively greater for Hispanics with intellectual disability (10.5 years), or cerebral palsy (15.3 years), and Blacks with cerebral palsy (11.0 years). In contrast, the age-at-death inequity was comparatively lower for American Indians/Alaskan Native with intellectual disability (5.2 years), Down syndrome (8.6 years), and cerebral palsy (8.6 years); Blacks with intellectual disability (6.5 years) or Down syndrome (5.5 years); and Hispanics with Down syndrome (6.8 years).
Discussion
As expected, results from this study demonstrate that among all racial-ethnic groups, adults with intellectual disability, Down syndrome, and cerebral palsy reported on their death certificate, on average, died at younger ages than their peers without a reported intellectual or developmental disability. In addition, we provide the first evidence that while racial-ethnic disparities in age at death were present among all adults with intellectual and developmental disability, patterns were distinct from those observed among racial-ethnic groups in the general population. As documented in prior studies, we found a multiple descent pattern in age at death among adults without intellectual and developmental disability, with the highest age at death among Whites, followed by Asians/Pacific Islanders, Hispanics and Blacks, then American Indians/Alaskan Natives. In contrast, among adults with intellectual and developmental disability, the racial-ethnic inequity in age at death was reduced to a bifurcated pattern, with the highest age at death also among Whites, but then lower and similar ages at death for all racial-ethnic minorities.
The reduction of the racial-ethnic inequity in age at death from a multiple descent to a bifurcated pattern among adults with intellectual and developmental disability appears to be due to two separate distinctions among adults without an intellectual or developmental disability. First, though Asians/Pacific Islanders without intellectual and developmental disability die at ages slightly below Whites, this inequity is much more severe across all intellectual and developmental disability groups. Second, the inequity in age at death for American Indians/Alaskan Natives observed among those without intellectual and developmental disability was reduced among American Indians/Alaskan Natives with intellectual and developmental disability. Together, these two shifts reduced the multiple descent pattern to a bifurcated pattern. Though not testable with the data used in this study, these results suggest that intellectual and developmental disability has differential effects on racial-ethnic inequities in age at death, possibly exacerbating racial-ethnic inequities for Asians/Pacific Islanders, yet lessening racial-ethnic inequities for American Indian/Alaskan Natives. To better understand this finding, future research should explore whether these shifts are associated with differential causes of death between Asian/Pacific Islander and American Indian/Alaskan Native adults with/without intellectual and developmental disability, with particular attention to the prevalence of preventable causes of death.
Results from this study underscore that people with intellectual and developmental disability from racial-ethnic minority groups are experiencing a form of double-jeopardy, with reductions in age at death associated with the intersecting marginalized statuses of disability and racial-ethnic minority status (Turan et al., 2019). Though disheartening, this result is not surprising as similar double jeopardies have been reported for people with disability in educational and employment outcomes (Bisesti & Landes, 2021; Frederick & Shifrer, 2018; Maroto et al., 2019). What is surprising was the inconsistent presence of this particular form of double jeopardy for age at death. Specifically, this double jeopardy was evident for some groups but not others. For example, among people with Down syndrome, the intersecting disadvantage was only among Asians/Pacific Islanders. Among people with intellectual disability, the intersecting disadvantage was among Asians/Pacific Islanders and Hispanics. Among those with cerebral palsy, the intersecting disadvantage was among Asians/Pacific Islanders, Hispanics, and Blacks. Furthermore, the severity of the double jeopardy associated with the intersecting disability and race-ethnic disadvantage was much more pronounced among decedents with cerebral palsy than among decedents with intellectual disability or Down syndrome. Efforts to clarify differences in social determinants of health and in causes of death by disability and race-ethnic status may give further insight into the possible mechanisms informing these differences.
Limitations
The limitations to this study relate to data. Beyond general concerns with death certificate accuracy (Lloyd-Jones et al., 1998; McGivern et al., 2017; Messite & Stellman, 1996; Nielsen et al., 1991; Wall et al., 2005), particular concern has rightly been expressed regarding use of this data to understand mortality patterns for people with intellectual disability. As summarized in a 2018 systematic literature review of death certification for people with intellectual disability by Stirton and Heslop (2018), intellectual disability is commonly underreported on death certificates. Comparing data from a registry to death certificate data, a 1998 study by Hollins et al. (1998) of two London districts report that only 46.3% of decedents known to have intellectual disability had their disability reported on the death certificate. Using a similar strategy, more recent studies from the UK clarify that underreporting of intellectual disability is more common among people with mild (9%) as opposed to moderate or severe (41%), or profound intellectual disability (58%) (Heslop et al., 2013; Heslop et al., 2014; Stirton & Heslop, 2018; Tyrer & McGrother, 2009). Underreporting does not appear to be as much of a concern for individuals with more readily-identifiable developmental disabilities such as Down syndrome or cerebral palsy (Glover & Ayub, 2010; Stirton & Heslop, 2018).
Unlike countries such as the UK (Heslop et al., 2021; Heslop et al., 2019), the US does not engage in national health surveillance of adults with intellectual and developmental disability (Krahn, 2019). As we do not have adequate estimates of population size, it is not possible to assess the degree of underreporting of intellectual and developmental disability among US death certificates. The most recent estimates of the US population of adults with intellectual disability are based upon 1990s data from the National Health Interview Survey (LaPlante & Carlson, 1996; Larson et al., 2001) or Social Security Administration (SSA) administrative data (Massey & McDermott, 1996). In addition to being dated, the authors of these studies acknowledge that the data used for the estimates do not reliably include all individuals with this disability. One more recent study used vital statistics data (live births and survival rates from death certificates) to estimate the 2010 population of adults with Down syndrome at 5.3 per 10,000, but also acknowledges this rate may be low due to underreporting (de Graaf et al., 2017). There are no estimates of the population size of adults with cerebral palsy in the US. Though recognizing this limitation, we pursued this study because efforts to understand population health patterns among people with intellectual and developmental disability in the US are dependent on maximizing understanding of trends with the data that is available (National Center on Birth Defects and Developmental Disabilities, 2009). However, it is important to underscore that the results from this study only apply to adults who had their intellectual or developmental disability reported on their death certificate.
The second limitation is the inability to calculate life expectancy as the age-specific size of the population at risk is unknown. Due to this limitation, we analyzed age at death. Though a crude measure of longevity, comparisons in age at death are often used for rare conditions for which the size of the population is unknown, and easily translate into years of life lost for those with the condition (Jannerfeldt & Hörte, 1988; Lanzkron et al., 2013; Solberg et al., 2018; Tuljapurkar, 2011). Finally, there were insufficient number of cases to examine patterns in age at death by race-ethnicity among adults with more rare types of intellectual and developmental disability. Nonetheless, this study used vital statistics from the US to provide evidence that racial-ethnic patterns in age at death vary between adults with and without intellectual and developmental disability and underscores the importance of examining subpopulation differences within the large and heterogenous population of adults with intellectual and developmental disability.
Conclusion
Adults with an intellectual and developmental disability reported on their death certificate are, on average, dying at younger ages than their peers without intellectual or developmental disability reported. Importantly, the severity of this disparity is associated with race-ethnicity. Racial-ethnic inequities in age at death are present among adults with and without intellectual and developmental disability, but with intersectional variation in patterns. While results from this and prior studies demonstrate that Asians have similar ages at death to Whites in the general population, this is not the case among those with intellectual and developmental disability. Instead, all racial-ethnic minorities with intellectual and developmental disability die at much younger ages than their White peers. It is imperative that efforts aimed at improving health outcomes among adults with intellectual and development disability take into account that racial-ethnic minorities with intellectual disability, Down syndrome, and cerebral palsy are at greater risk of premature death than their White counterparts – a double-jeopardy that is most severe among adults with cerebral palsy. Future research supporting public health efforts should examine variation in social determinants of health and cause of death by the intersecting marginalized statuses of disability and race-ethnicity to attempt to clarify the mechanisms that may be resulting in years of lost life for racial-ethnic minorities with intellectual and developmental disability.
Highlights.
Average age at death is younger for intellectual and developmental disabled adults
This disparity is more pronounced among all racial-ethnic minorities
Racial-ethnic inequities are most severe among adults with cerebral palsy
Funding statement:
Funding for this project was provided from a grant by the Tenth Decade Project, Maxwell School of Citizenship and Public Affairs, Syracuse University. Research in this paper benefitted from NIA Center grant (P30AG066583), Center for Aging Policy Studies, Syracuse University.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Study is not humans subjects research as data is publicly available and fully deidentified.
Credit author statement
Scott Landes: conceptualization, methodology, data curation, formal analysis, writing – original draft and reviewing/editing, supervision
Janet Wilmoth: conceptualization, methodology, writing – original draft and reviewing/editing
Katherine McDonald: conceptualization, methodology, writing – original draft and reviewing/editing
Alyssa Smith: writing – original draft and reviewing/editing
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Anderson LL, Larson SA, MapelLentz S, & Hall-Lande J (2019). A Systematic Review of U.S. Studies on the Prevalence of Intellectual or Developmental Disabilities Since 2000. Intellectual and Developmental Disabilities, 57(5), 421–438. 10.1352/1934-9556-57.5.421 [DOI] [PubMed] [Google Scholar]
- Anker LA, Chick CF, & Hallmayer JF (2020). Chapter 17 - Aging of persons with neurodevelopmental disabilities. In Hantke N, Etkin A, & O’Hara R (Eds.), Handbook of Mental Health and Aging (Third Edition) (pp. 223–243). Academic Press. 10.1016/B978-0-12-800136-3.00017-X [DOI] [Google Scholar]
- Bershadsky J, Hiersteiner D, Fay ML, & Bradley V (2014). Race/ethnicity and the use of preventive health care among adults with intellectual and developmental disabilities. Medical Care, S25–S31. [DOI] [PubMed] [Google Scholar]
- Bisesti E, & Landes SD (2021). Racial-ethnic differences in educational trajectories for individuals with intellectual disability. Journal of Intellectual Disability Research, 65(6), 548–560. 10.1111/jir.12830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonardi A, Lauer E, Mitra M, Bershadsky J, Taub S, & Noblett C (2011). Expanding surveillance of adults with intellectual disability in the US. Center for Developmental Disabilities Evaluation and Research (CDDER), E.K. Shrive Center University of Massachusetts Medical School. [Google Scholar]
- Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, … Kogan MD (2011). Trends in the Prevalence of Developmental Disabilities in US Children, 1997–2008 [ 10.1542/peds.2010-2989]. Pediatrics, 127(6), 1034–1042. http://pediatrics.aappublications.org/content/127/6/1034.abstract [DOI] [PubMed] [Google Scholar]
- Edwards RD (2011). Changes in World Inequality in Length of Life: 1970–2000. Population and Development Review, 37(3), 499–528. 10.1111/j.1728-4457.2011.00432.x [DOI] [PubMed] [Google Scholar]
- Escarce JJ (2019). Health Inequity in the United States: A Primer. https://ldi.upenn.edu/sites/default/files/pdf/Penn%20LDI%20Health%20Inequity%20in%20the%20United%20States%20Report_5.pdf
- Firebaugh G, Acciai F, Noah AJ, Prather C, & Nau C (2014). Why Lifespans Are More Variable Among Blacks Than Among Whites in the United States. Demography, 51(6), 2025–2045. 10.1007/s13524-014-0345-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick A, & Shifrer D (2018). Race and Disability: From Analogy to Intersectionality. Sociology of Race and Ethnicity, 5(2), 200–214. 10.1177/2332649218783480 [DOI] [Google Scholar]
- Fujiura GT, & Taylor SJ (2003). Continuum of intellectual disability: Demographic evidence for the “Forgotten Generation”. Mental Retardation, 41(6), 420–429. [DOI] [PubMed] [Google Scholar]
- Heslop P, Blair PS, Fleming P, Hoghton M, Marriott A, & Russ L (2014). The Confidential Inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study. The Lancet, 383(9920), 889–895. 10.1016/S0140-6736(13)62026-7 [DOI] [PubMed] [Google Scholar]
- Heslop P, Byrne V, Calkin R, Pollard J, Sullivan B, Daly P, … Vergara E (2021). Learning Disabilities Mortality Review (LeDeR) Programme, Annual Report 2020.
- Heslop P, Calkin R, Byrne V, Huxor A, Gielnik K, & Team L (2019). Learning Disabilitiies Mortality Review (LeDeR) Programme, Annual Report 2019.
- Heslop P, & Glover G (2015). Mortality of People with Intellectual Disabilities in England: A Comparison of Data from Existing Sources. Journal of Applied Research in Intellectual Disabilities, 28(5), 414–422. 10.1111/jar.12192 [DOI] [PubMed] [Google Scholar]
- Hummer RA, & Hamilton ER (2019). Population health in America. University of California Press. [Google Scholar]
- Iezzoni LI, Rao SR, Ressalam J, Bolcic-Jankovic D, Agaronnik ND, Donelan K, … Campbell EG (2021). Physicians’ Perceptions Of People With Disability And Their Health Care. Health Affairs, 40(2), 297–306. 10.1377/hlthaff.2020.01452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jannerfeldt E, & Hörte L-G (1988). Median age at death as an indicator of premature mortality. British Medical Journal, 296(6623), 678. 10.1136/bmj.296.6623.678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krahn GL (2019). A Call for Better Data on Prevalence and Health Surveillance of People With Intellectual and Developmental Disabilities. Intellectual and Developmental Disabilities, 57(5), 357–375. 10.1352/1934-9556-57.5.357 [DOI] [PubMed] [Google Scholar]
- Krahn GL, & Fox MH (2014). Health disparities of adults with intellectual disabilities: What do we know? What do we do? Journal of Applied Research in Intellectual Disabilities, 27(5), 431–446. 10.1111/jar.12067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landes SD (2017). The Intellectual Disability Mortality Disadvantage: Diminishing With Age? American Journal on Intellectual and Developmental Disabilities, 122(2), 192–207. 10.1352/1944-7558-122.2.192 [DOI] [PubMed] [Google Scholar]
- Landes SD, McDonald KE, Wilmoth JM, & Carter Grosso E (2021). Evidence of continued reduction in the age-at-death disparity between adults with and without intellectual and/or developmental disabilities. Journal of Applied Research in Intellectual Disabilities, 34(3), 916–920. 10.1111/jar.12840 [DOI] [PubMed] [Google Scholar]
- Landes SD, Stevens JD, & Turk MA (2019). Heterogeneity in age at death for adults with developmental disability. Journal of Intellectual Disability Research, 63, 1482–1487. 10.1111/jir.12672 [DOI] [PubMed] [Google Scholar]
- Lanzkron S, Carroll CP, & Haywood C (2013). Mortality Rates and Age at Death from Sickle Cell Disease: U.S., 1979–2005. Public Health Reports, 128(2), 110–116. 10.1177/003335491312800206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lariscy J, Hummer R, & Hayward M (2015). Hispanic Older Adult Mortality in the United States: New Estimates and an Assessment of Factors Shaping the Hispanic Paradox [Article]. Demography, 52(1), 1–14. 10.1007/s13524-014-0357-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson SA, Lakin KC, Anderson L, Kwak Lee N, Lee JH, & Anderson D (2001). Prevalence of mental retardation and developmental disabilities: Estimates from the 1994/1995 National Health Interview Survey Disability Supplements. American Journal on Mental Retardation, 106(3), 231–252. [DOI] [PubMed] [Google Scholar]
- Lauer E, Heslop P, & Hoghton M (2015). Identifying and addressing disparities in mortality: US and UK perspectives. International Review of Research in Developmental Disabilities, 48, 195–245. 10.1016/bs.irrdd.2015.03.002 [DOI] [Google Scholar]
- Li H, Parish SL, Magaña S, & Morales MA (2021). Racial and Ethnic Disparities in Perceived Barriers to Health Care Among U.S. Adults With Intellectual and Developmental Disabilities. Intellectual and Developmental Disabilities, 59(1), 84–94. 10.1352/1934-9556-59.1.84 [DOI] [PubMed] [Google Scholar]
- Magaña S, Parish S, Morales MA, Li H, & Fujiura G (2016). Racial and Ethnic Health Disparities Among People With Intellectual and Developmental Disabilities. Intellectual and Developmental Disabilities, 54(3), 161–172. 10.1352/1934-9556-54.3.161 [DOI] [PubMed] [Google Scholar]
- Maroto M, Pettinicchio D, & Patterson AC (2019). Hierarchies of Categorical Disadvantage: Economic Insecurity at the Intersection of Disability, Gender, and Race. Gender & Society, 33(1), 64–93. 10.1177/0891243218794648 [DOI] [Google Scholar]
- MENCAP. (2007). Death by indifference: Following up the Treat Me Right! report. Mencap. Retrieved July 13 from https://www.mencap.org.uk/sites/default/files/2016-06/DBIreport.pdf [Google Scholar]
- National Center on Birth Defects and Developmental Disabilities. (2009). U.S. surveillance of health of people with intellectual disabilities: A white paper. In. Atlanta: Centers for Disease Control and Prevention. [Google Scholar]
- National Vital Statistics System. (2017). Underlying cause of death data. Retrieved June 14 from https://wonder.cdc.gov/.
- Ouellette-Kuntz H (2005). Understanding health disparities and inequities faced by individuals with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 18(2), 113–121. 10.1111/j.1468-3148.2005.00240.x [DOI] [Google Scholar]
- Prasher VP, & Janicki MP (Eds.). (2019). Physical health of adults with intellectual and developmental disabilities (2nd ed.). Springer. [Google Scholar]
- Reid SM, Meehan EM, Arnup SJ, & Reddihough DS (2018). Intellectual disability in cerebral palsy: a population-based retrospective study. Developmental Medicine & Child Neurology, 60(7), 687–694. 10.1111/dmcn.13773 [DOI] [PubMed] [Google Scholar]
- Robertson J, Raghavan R, Emerson E, Baines S, & Hatton C (2019). What do we know about the health and health care of people with intellectual disabilities from minority ethnic groups in the United Kingdom? A systematic review. Journal of Applied Research in Intellectual Disabilities, 32(6), 1310–1334. 10.1111/jar.12630 [DOI] [PubMed] [Google Scholar]
- Scott HM, & Havercamp SM (2014). Race and Health Disparities in Adults With Intellectual and Developmental Disabilities Living in the United States. Intellectual and Developmental Disabilities, 52(6), 409–418. 10.1352/1934-9556-52.6.409 [DOI] [PubMed] [Google Scholar]
- Shavers VL, & Shavers BS (2006). Racism and health inequity among Americans. Journal of the National Medical Association, 98(3), 386–396. https://pubmed.ncbi.nlm.nih.gov/16573303 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2576116/ [PMC free article] [PubMed] [Google Scholar]
- Solberg OK, Filkuková P, Frich JC, & Feragen KJB (2018). Age at Death and Causes of Death in Patients with Huntington Disease in Norway in 1986–2015. Journal of Huntington’s Disease, 7, 77–86. 10.3233/JHD-170270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuljapurkar S (2011). 6. The Final Inequality: Variance in Age at Death. In Demography and the Economy (pp. 209–226). University of Chicago Press. [Google Scholar]
- Turan JM, Elafros MA, Logie CH, Banik S, Turan B, Crockett KB, … Murray SM (2019). Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Medicine, 17(1), 7. 10.1186/s12916-018-1246-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xu J (2019). QuickStats: Average Age at Death by Race/Hispanic Origin and Sex — National Vital Statistics System, United States, 2017. MMWR Morb Mortal Wkly Rep, 68, 690. 10.15585/mmwr.mm6831a4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang Q, Rasmussen SA, & Friedman JM (2002). Mortality associated with Down’s syndrome in the USA from 1983 to 1997: a population-based study. The Lancet, 359(9311), 1019–1025. 10.1016/S0140-6736(02)08092-3 [DOI] [PubMed] [Google Scholar]