

Abstract
Background:
Middle cerebral artery (MCA) has a significantly lower incidence of anatomical variations than other intracranial arteries. We present an extremely rare case of unruptured aneurysms with the segmental duplicated MCA (d-MCA) formed a fenestrated structure at origin.
Case Description:
A 55-year-old female underwent direct surgery for the unruptured aneurysms at the top of the right internal cerebral artery with d-MCA. The d-MCA branches separated at the right internal cerebral artery top and had comparable with that of the main MCA trunk. Moreover, there was an anastomosis between the d-MCA branches. We diagnosed this anastomosis as segmental d-MCA. Two aneurysmal domes were identified during surgery at the origin of the d-MCA, which the main dome protruding backward was wide necked and another small one was collapsed or thrombosed protruding forward. We used a fenestrated clip for the posterior projecting dome, and the aneurysms were successfully obliterated.
Conclusion:
Although cerebral aneurysms associated with d-MCA are rare, there are technical difficulties in the surgical management. A fenestrated clip might be most reasonable to obtain patency of the parent arteries for the posterior projecting aneurysms if the perforators can be avoided.
Keywords: Anastomosis, Cerebral aneurysm, Fenestrated clip, Segmental duplicated middle cerebral artery
INTRODUCTION
Anomalies of the middle cerebral artery (MCA) occur less frequently than those of other major intracranial arteries.[1,3,10] The duplicated MCA (d-MCA) arises from the internal carotid artery (ICA) and the incidence is relatively low.[2,3,8] The association of cerebral aneurysms with d-MCA is rare. Due to rarity of aneurysms located at carotid trifurcation, the technical difficulties in the surgical management are dictated by the location, size, shape, and direction of aneurysmal projection.[5] We present an extremely rare case of aneurysms with the segmental d-MCA formed a fenestrated structure at origin.
CASE DESCRIPTION
A 55-year-old woman, right handed with hypertension presented with chronic headache. The patient was smoker and had no family history of stroke. Magnetic resonance imaging suspected an unruptured aneurysm at the top of the right ICA [Figure 1]. Three-dimensional computed tomographic angiography demonstrated an aneurysm protruding backward with a diameter of 7 mm at the origin of the right d-MCA [Figure 2a-e]. There was an anastomosis between d-MCA branches at origin [Figure 2c,e]. The right frontotemporal craniotomy was performed, and we identified two aneurysmal domes. The main aneurysm was a wide-necked dome protruding backward and another one was a small and collapsed or thrombosed dome protruding forward [Figure 3]. The medial lenticulostriate arteries passed by the aneurysm protruding backward. We used a fenestrated clip for the posterior projecting dome and the two aneurysms were successfully obliterated [Figure 4]. The postoperative course was uneventful, and the patient was discharged with no neurological deficit.
Figure 1:

Magnetic resonance (MR) images show the duplicated middle cerebral artery branches (arrows) and an aneurysm (asterisk) at the top of the right internal carotid artery (a: T2-weighted imaging, b: T1-weighted imaging, c: MR angiography).
Figure 2:

Computed tomographic angiography (CTA) demonstrates an aneurysm protruding backward (asterisk) and the duplicated middle cerebral artery (d-MCA) branches (arrows). There is an anastomosis (arrowhead) between d-MCA branches at the origin (a, c-e: three-dimensional CTA, b: source imaging of CTA).
Figure 3:
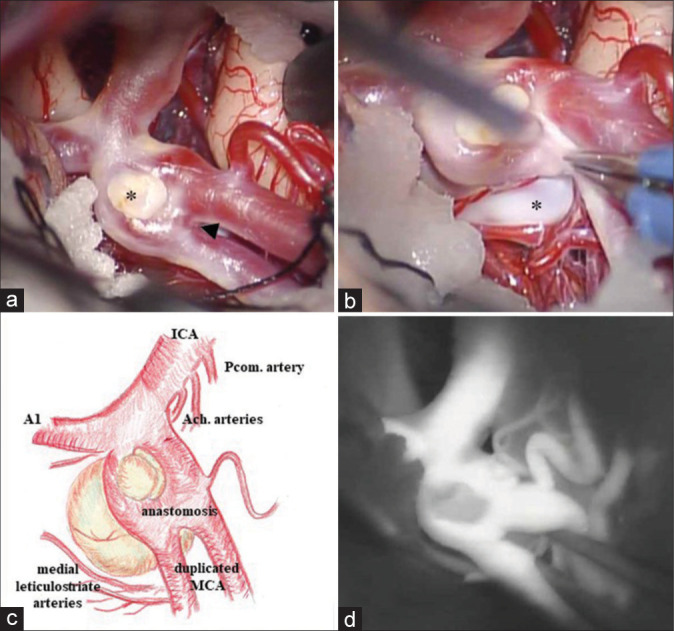
The intraoperative images reveal two aneurysmal domes (asterisk) and an anastomosis (arrowhead) between d-MCA branches. The small dome protruding forward is collapsed or thrombosed (a, b: intraoperative image, c: a sketch of operative view, d: the indocyanine green video angiography.
Figure 4:
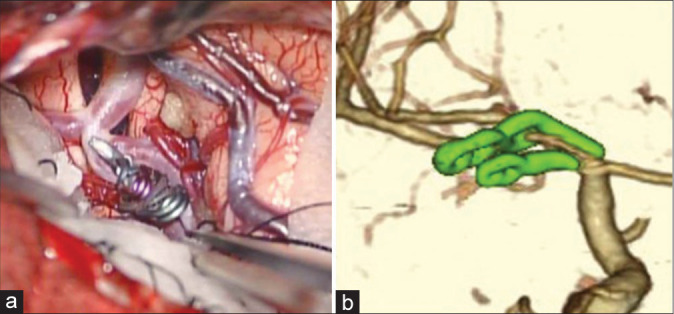
Aneurysms are completely obliterated with clips (a: intraoperative image, b: three-dimensional computed tomographic angiography).
DISCUSSION
The most frequent anatomical variations of the MCA are accessory MCA (ac-MCA), d-MCA, duplicate origin of MCA (do-MCA), MCA fenestration, and twig-like MCA.[10] Phylogenetically, the distal portion of the ICA bifurcates into cranial and caudal branches, and the anterior cerebral artery (ACA) develops from the cranial branch[7]. The MCA develops after the ACA, which can be considered its collateral branch[10]. Multiple plexiform arterial twigs develop just distally to the anterior choroidal artery (AchA).[7] These twigs fuse and regress forming lateral striate arteries and the normal MCA. The failure of these processes in embryonic stage may lead to diverse variations of the MCA.
In 1973, Teal et al. proposed the term ac-MCA as arterial branches arising from ACA or anterior communicating artery coursed with the MCA into the Sylvian fissure, and termed d-MCA as anomalous MCA arising from the ICA regardless of its size.[9] In the MCA fenestration at origin, M1 originates as a single trunk and be divided into two channels at a short segment, whereas in do-MCA, two M1 originate separately from the ICA terminal and conglutinate into a single trunk [3,10]. The d-MCA is a relatively rare anatomical branching variation from the ICA, with reported incidence of 0.2–2.9% in autopsy and 0.24–1.5% in angiography.[1,9] According to Kai et al., d-MCA can be divided into two types.[4] Type A d-MCA separates from the ICA top and has comparable with that of the main MCA trunk. Type B d-MCA originates from the ICA between the AchA and the ICA top, and its diameter is smaller than that of the main MCA trunk. The frequency of type B is twice as common as Type A.[8]
The present case is the type A d-MCA and could be actually ICA trifurcation, since the d-MCA and ACA branches had almost identical diameters.[5] Moreover, there was an anastomosis between d-MCA branches at origin. This fused d-MCA vessels cannot categorized as MCA fenestration or do-MCA because each two MCA branches arise from the ICA and these branches do not fuse into a single trunk. Stojanović et al. described this type of anastomosis between d-MCA branches as a segmental d-MCA for the first time.[8] The present case is the second report of a segmental d-MCA, and the specificity of our case is the aneurysms were on the fenestrated structure at the origin of the segmental d-MCA.
The mechanism of the development of MCA anomaly associated aneurysms is an interesting issue and some authors have suggested that hemodynamic stress at the origin of the abnormal vessel might contribute to the formation of the aneurysm.[3,8] In the previous reports, the aneurysms associated with d-MCA were all divided into Type B d-MCA, this could be result from higher hemodynamic stress due to the shape angle from the ICA than Type A.[3,4] On the other hand, hemodynamic stress in Type A d-MCA is not specific for the formation of aneurysms and this type might have congenital defect in cerebrovascular development and be prone to cerebrovascular anomalies rather than Type B.[3] Our case is extremely rare because of the aneurysms combined d-MCA applying to Type A.
The d-MCA has perforating arteries to the anterior perforated substance and may contribute to the normal cerebral blood flow to the frontal lobe and the basal ganglia through the perforating arteries.[3,4,6,8] As for the surgical manipulation, avoiding damage of the d-MCA is important.[2] We were able to obliterate the aneurysm using a fenestrated clip by sparing the perforators. It is imperative to select the shortest possible clips and the optimal direction of the clip insertion so as not to catch the nearby AchA or medial lenticulostriate arteries in the blade of clips. Fenestrated clips might be most reasonable to obtain patency of the parent arteries for posterior projecting aneurysms if the perforators can be avoided because there are few possibilities of the clip shift after release of brain retraction. For the reason why we selected clipping surgery than coil embolization, the most aneurysms associated with d-MCA often have a wide neck, a sharp curved parent artery, anastomosis, and tortuous access for catheterization,[3] which might make endovascular treatment difficult and highly risky.
CONCLUSION
We experienced a rare case of the aneurysms at the origin of the segmental d-MCA. Although cerebral aneurysms associated with d-MCA are rare, there are technical difficulties in the surgical management. Fenestrated clips might be suitable to obtain patency of parent arteries.
Footnotes
How to cite this article: Shiozaki E, Kawahara I, Uchida D, Morofuji Y, Ono T, Haraguchi W, et al. Unruptured cerebral aneurysms with the segmental duplicated middle cerebral artery formed a fenestrated structure at origin. Surg Neurol Int 2022;13:33.
Contributor Information
Eri Shiozaki, Email: e.shiozaki15@gmail.com.
Ichiro Kawahara, Email: kawahara.ichiro.kr@mail.hosp.go.jp.
Daiki Uchida, Email: uchida.daiki.qg@mail.hosp.go.jp.
Yoichi Morofuji, Email: morofujiyoichi@gmail.com.
Tomonori Ono, Email: onotomon@gmail.com.
Wataru Haraguchi, Email: haraguchi.wataru.uj@mail.hosp.go.jp.
Kazuya Honda, Email: honda.kazuya.gs@mail.hosp.go.jp.
Tomoya Moritsuka, Email: moritsuka.tomoya.kd@mail.hosp.go.jp.
Keisuke Tsutsumi, Email: tsutsumi.keisuke.pn@mail.hosp.go.jp.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Crompton MR. The pathology of ruptured middle-cerebral aneurysms with special reference to the differences between the sexes. Lancet. 1962;2:421–5. doi: 10.1016/s0140-6736(62)90281-7. [DOI] [PubMed] [Google Scholar]
- 2.Elsharkawy A, Ishii K, Niemelä M, Kivisaari R, Lehto H, Hernesniemi J. Management of aneurysms at the origin of duplicated middle cerebral artery: Series of four patients with review of the literature. World Neurosurg. 2013;80:e313–8. doi: 10.1016/j.wneu.2012.10.004. [DOI] [PubMed] [Google Scholar]
- 3.Hou K, Xu K, Liu H, Li G, Yu J. The clinical characteristics and treatment considerations for intracranial aneurysms associated with middle cerebral artery anomalies: A systematic review. Front Neurol. 2020;11:564797. doi: 10.3389/fneur.2020.564797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kai Y, Hamada J, Morioka M, Yano S, Kudo M, Kuratsu J. Treatment of unruptured duplicated middle cerebral artery aneurysm: Case report. Surg Neurol. 2006;65:190–3. doi: 10.1016/j.surneu.2005.05.032. discussion 193. [DOI] [PubMed] [Google Scholar]
- 5.Kaliaperumal C, Jain N, McKinstry CS, Choudhari KA Carotid. “trifurcation” aneurysm: Surgical anatomy and management. Clin Neurol Neurosurg. 2007;109:538–40. doi: 10.1016/j.clineuro.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 6.Komiyama M, Nakajima H, Nishikawa M, Yasui T. Middle cerebral artery variations: Duplicated and accessory arteries. AJNR Am J Neuroradiol. 1998;19:45–9. [PMC free article] [PubMed] [Google Scholar]
- 7.Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol. 1948;32:205–62. [Google Scholar]
- 8.Stojanović NN, Kostić A, Mitić R, Berilažić L. Correlation between multiple cerebral aneurysms and a rare type of segmental duplication of the middle cerebral artery. BMC Neurol. 2020;20:3. doi: 10.1186/s12883-019-1588-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Teal JS, Rumbaugh CL, Bergeron RT, Segall HD. Anomalies of the middle cerebral artery: Accessory artery, duplication, and early bifurcation. Am J Roentgenol Radium Ther Nucl Med. 1973;118:567–75. doi: 10.2214/ajr.118.3.567. [DOI] [PubMed] [Google Scholar]
- 10.Uchiyama N. Anomalies of the middle cerebral artery. Neurol Med Chir (Tokyo) 2017;57:261–6. doi: 10.2176/nmc.ra.2017-0043. [DOI] [PMC free article] [PubMed] [Google Scholar]