

Abstract
The treatment of leprosy is long and complex, benefiting from the development of sterilizing, rapidly-acting drugs. Reductive evolution made Mycobacterium leprae exquisitely sensitive to Telacebec, a phase 2 drug candidate for tuberculosis. The unprecedented potency of Telacebec against M. leprae warrants further validation in clinical trials.
Keywords: Hansen disease, tuberculosis and other mycobacteria, bacteria, Mycobacterium leprae, leprosy, telacebec, QcrB inhibitors, terminal oxidase
Leprosy, also known as Hansen disease, is a chronic infectious disease caused primarily by Mycobacterium leprae and to a lesser extent by M. lepromatosis bacteria. Both species have a strong tropism for the Schwann cells; infection causes peripheral neuropathy, which leads to the characteristic deformities and disabilities. Despite successful implementation of multidrug therapies for the treatment of leprosy, >200,000 new cases were reported globally in 2019. Drug-resistant M. leprae strains, although rare, are emerging in several parts of the world (1). Therefore, newer rapidly acting bactericidal, orally bioavailable drugs are required to shorten treatment time and reduce transmission.
The high potency of drugs targeting the cytochrome bcc:aa3 terminal oxidase (also known as QcrB inhibitors) against M. ulcerans has been reported (3). Of particular importance is the finding that a single dose of the drug candidate, Telacebec (Q203) (3), eradicates infection in a mouse model of Buruli ulcer (4). The potency of drugs targeting the cytochrome bcc:aa3 terminal oxidase against M. ulcerans is explained by the absence of a functional cytochrome bd oxidase, an alternate terminal oxidase that limits the potency of telacebec in M. tuberculosis (5,6). Like M. ulcerans, M. leprae has lost the genes encoding the cytochrome bd oxidase and any other alternate terminal electron acceptors (7). Because M. leprae relies exclusively on the cytochrome bcc:aa3 terminal oxidase for respiration, Scherr et al. hypothesized that telacebec and related QcrB inhibitors could represent a new class of bactericidal drugs for leprosy (2).
The potency of telacebec was initially tested against extracellular M. leprae using a radio-respirometry assay to determine bacterial β-oxidation rate. This assay is used to assess viability of noncultivable M. leprae and measures cumulative production of CO2 by the bacilli when palmitic acid is the sole carbon source (8). Telacebec at a concentration of 0.2 nM inhibited ≈90% (p<0.001) and 2 nM inhibited ≈99.9% (p<0.0001) of M. leprae metabolic activity after 3 days of incubation (Figure, panel A). In comparison, rifampin used at 2.0 μM inhibited only ≈45% (p = 0.020) of the metabolic activity compared with untreated control in the same time frame (Figure, panel A). We observed a similar trend after 7 days of incubation (Figure, panel A); 0.2 nM of telacebec was significantly more potent than 2 μM of rifampin at all tested concentrations in this assay. Telacebec was also active against intracellular M. leprae maintained in murine bone marrow–derived macrophages (9). Telacebec at 2.0 nM inhibited ≈97% (p<0.001 vs. untreated) of the metabolic activity of intracellular M. leprae in 3 days. Telacebec was also marginally potent against intracellular M. leprae at 0.2 nM but required longer incubation; we observed a statistically nonsignificant reduction of ≈33% (p = 0.069) after 3 days’ incubation and a significant reduction of ≈40% (p = 0.034) after 7 days. Under similar experimental conditions, rifampin at 2.0 μM inhibited metabolic activity of intracellular M. leprae by ≈44% (p = 0.025) at day 3 and ≈72% (p<0.001) at day 7 compared with the untreated control group (Figure, panel B). Telacebec at 2 or 20 nM was more potent than rifampin in this assay as well.
Figure.
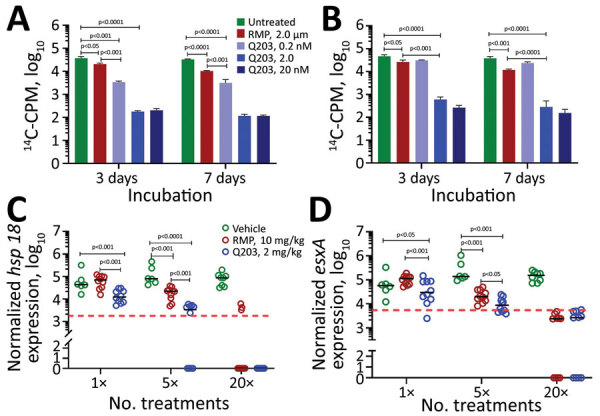
Efficacy of telacebec against Mycobacterium leprae bacteria in axenic culture (A), in murine bone marrow–derived macrophages (B), and in athymic nude mouse foot pad model (C, D). M. leprae hsp18 (C) and esxA (D) expression levels were used as a surrogate measure of viability. For panels A and B, the assays were performed in triplicate for each condition. For panels C and D, each foot pad is taken as a data point, and the red dotted lines indicate ≈99% M. leprae kill. Significance was determined by 2-tailed unpaired Student t-test. 14C, carbon 14; CPM, counts per minute; Q203, telacebec; RMP, rifampin.
The high nanomolar potency of telacebec against both intracellular and extracellular M. leprae prompted us to evaluate its efficacy in a mouse foot pad model of infection. We inoculated groups of 5 athymic nude mice with 3 × 107 viable M. leprae in both hind foot pads. At 8 weeks postinfection, we administered telacebec (2 mg/kg) or rifampin (10 mg/kg) by gavage as 1 dose, 5 consecutive daily doses, or 20 doses (5 days × 4 weeks). We harvested foot pads 4 weeks after completion of the drug treatment. Because M. leprae is noncultivable, we measured mycobacterial load using an established molecular method (10). We determined M. leprae hsp18 and esxA expression levels as a surrogate measure of viability (10). Bacterial hsp18 and esxA expression were significantly lower in mice receiving 1 (p<0.001) or 5 (p<0.001) consecutive doses of telacebec compared with rifampin or to the vehicle-treated control group, indicating a faster in vivo bactericidal efficacy of telacebec (Figure, panels C, D). Although >5 consecutive doses of rifampin were needed to detect a bactericidal efficacy, 1 dose of telacebec at a low dose of 2 mg/kg was sufficient to reduce the bacterial viability substantially (Figure, panels C, D).
This study demonstrates the exquisite sensitivity of M. leprae to telacebec and the potential of a shorter treatment regimen. Dose-finding studies in animals will help to determine an optimum dosing regimen for rapid bacterial eradication. Combination therapies between telacebec and first- or second-line drugs such as rifampin, clofazimine, or minocycline should be evaluated in preclinical animal models to guide the development of a potent, fast-acting, sterilizing drug combination for humans that has a low propensity for resistance development for humans. The curative promise of telacebec or other advanced QcrB inhibitors should be validated in human clinical trials.
Acknowledgments
This work was supported in part by the Lee Kong Chian School of Medicine, Nanyang Technological University Start-Up Grant (K.P.), the National Research Foundation, Singapore, under its Investigatorship Programme (grant no. NRF-NRFI06-2020-0004), and the New York Community Trust Heiser Program (grant no. P18-000248). US National Institute of Allergy and Infectious Diseases funded the provision of viable M. leprae through an interagency agreement with Health Resources and Services Administration, Healthcare Systems Bureau, National Hansen’s Disease Program (no. AAI20009-001-00000).
The views expressed in this article are solely the opinions of the authors and do not necessarily reflect the official policies of the U.S. Department of Health and Human Services or the Health Resources and Services Administration, nor does mention of the department or agency names imply endorsement by the US Government.
Biography
Dr. Lahiri is a principal investigator at the Laboratory Research Branch, National Hansen’s Disease Program, Baton Rouge, Louisiana, USA. His research focuses on understanding host pathogen relationship, developing animal models and evaluating novel therapeutic interventions in Hansen disease.
Footnotes
Suggested citation for this article: Lahiri R, Adams LB, Thomas SS, Pethe K. Sensitivity of Mycobacterium leprae to telacebec. Emerg Infect Dis. 2022 Mar [date cited]. https://doi.org/10.3201/eid2803.210394
References
- 1.Mahajan NP, Lavania M, Singh I, Nashi S, Preethish-Kumar V, Vengalil S, et al. Evidence for Mycobacterium leprae drug resistance in a large cohort of leprous neuropathy patients from India. Am J Trop Med Hyg. 2020;102:547–52. 10.4269/ajtmh.19-0390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pethe K, Bifani P, Jang J, Kang S, Park S, Ahn S, et al. Discovery of Q203, a potent clinical candidate for the treatment of tuberculosis. Nat Med. 2013;19:1157–60. 10.1038/nm.3262 [DOI] [PubMed] [Google Scholar]
- 3.Scherr N, Bieri R, Thomas SS, Chauffour A, Kalia NP, Schneide P, et al. Targeting the Mycobacterium ulcerans cytochrome bc1:aa3 for the treatment of Buruli ulcer. Nat Commun. 2018;9:5370. 10.1038/s41467-018-07804-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Thomas SS, Kalia NP, Ruf MT, Pluschke G, Pethe K. Toward a single-dose cure for Buruli ulcer. Antimicrob Agents Chemother. 2020;64:e00727–20. 10.1128/AAC.00727-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kalia NP, Hasenoehrl EJ, Ab Rahman NB, Koh VH, Ang MLT, Sajorda DR, et al. Exploiting the synthetic lethality between terminal respiratory oxidases to kill Mycobacterium tuberculosis and clear host infection. Proc Natl Acad Sci U S A. 2017;114:7426–31. 10.1073/pnas.1706139114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Moosa A, Lamprecht DA, Arora K, Barry CE III, Boshoff HIM, Ioerger TR, et al. Susceptibility of Mycobacterium tuberculosis cytochrome bd oxidase mutants to compounds targeting the terminal respiratory oxidase, cytochrome c. Antimicrob Agents Chemother. 2017;61:e01338–17. 10.1128/AAC.01338-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cole ST, Eiglmeier K, Parkhill J, James KD, Thomson NR, Wheeler PR, et al. Massive gene decay in the leprosy bacillus. Nature. 2001;409:1007–11. 10.1038/35059006 [DOI] [PubMed] [Google Scholar]
- 8.Franzblau SG, Hastings RC. Rapid in vitro metabolic screen for antileprosy compounds. Antimicrob Agents Chemother. 1987;31:780–3. 10.1128/AAC.31.5.780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bailey MA, Na H, Duthie MS, Gillis TP, Lahiri R, Parish T. Nitazoxanide is active against Mycobacterium leprae. PLoS One. 2017;12:e0184107. 10.1371/journal.pone.0184107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Davis GL, Ray NA, Lahiri R, Gillis TP, Krahenbuhl JL, Williams DL, et al. Molecular assays for determining Mycobacterium leprae viability in tissues of experimentally infected mice. PLoS Negl Trop Dis. 2013;7:e2404. 10.1371/journal.pntd.0002404 [DOI] [PMC free article] [PubMed] [Google Scholar]